Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 17
Correlation Between Periodontal Disease and Oral, Oropharyngeal, and Parapharyngeal Cancers
Authors Daily ZA, Mohammed NB ![]() , Mohammed SM, Hussein HM
, Mohammed SM, Hussein HM ![]()
Received 8 January 2025
Accepted for publication 13 February 2025
Published 24 February 2025 Volume 2025:17 Pages 147—158
DOI https://doi.org/10.2147/CCIDE.S512557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Zina Ali Daily,1 Nawres Bahaa Mohammed,2 Samer Majeed Mohammed,2 Hashim Mueen Hussein3
1Periodontics Department, College of Dentistry, University of Al-Ameed, Karbala, Iraq; 2Maxillofacial Surgery Department, Dentistry College, University of Al-Ameed, Karbala, Iraq; 3Department of Conservative Dentistry, College of Dentistry, Mustansiriyah University, Baghdad, Iraq
Correspondence: Hashim Mueen Hussein, Department of Conservative Dentistry, College of Dentistry, Mustansiriyah University, Baghdad, Iraq, Email [email protected]; [email protected]
Background: Periodontitis is an inflammatory disease, and contributes to several inflammatory conditions, such as cancer. The relationship between periodontal disorders and different human malignancies is not well understood. The purpose of this study is to assess the association of periodontitis severity with cancers in the oral cavity, oropharyngeal and parapharyngeal regions.
Methods: The sample comprised 300 participants divided into four case groups: 75 oral, oropharyngeal, or parapharyngeal cancer patients with periodontitis (CA-with-P); 75 oral, oropharyngeal, or parapharyngeal cancer patients without periodontitis (CA-without-P); 75 periodontitis (P) patients without cancers; and a control (C) group of 75 healthy individuals. All participants were subjected to a periodontal examination that considered parameters such as bleeding on probing (BOP), plaque index (PI), probing pocket depth (PPD), and clinical attachment loss (CAL). The type of tumours was identified via a histological analysis of a biopsy sample. Saliva samples were also collected, and an enzyme-linked immunosorbent assay (ELISA) kit was used to determine interleukin 8 (IL-8) and nuclear factor kappa B (NF-κB) levels.
Results: The research findings indicated a significant increase in the number of sites with clinical observations of BOP (85.11,73.84), PI (87.23.88.14), PPD (8.03,6.82), and CAL (8.67,7.34) in groups CA-with-P and P. The CA-with-P, CA-without-P, and P groups had higher levels of salivary IL-8 (192.03, 121.89,89.22) and NF-κB (10.242, 8.172, 6.324) than the C group. Moreover, there was a significant correlation between the severity of periodontitis and the malignancies in the oral, oropharynx, and parapharyngeal regions.
Conclusion: This study assessed the mechanisms underlying the correlation between these two disorders, as elucidated by higher levels of salivary IL-8, NF-κB and an increase in clinical periodontal parameters. Periodontal bacteria, which contributes to the development of periodontal disorders, could have a major impact on the onset of oral cancers.
Keywords: periodontitis, oral malignancy, oropharyngeal malignancy, parapharyngeal cancer, IL-8, NF-κB
Introduction
Periodontal disease is a persistent inflammatory condition that impacts the bone and tissues that support the tooth. It leads to the deterioration of tissues that support the tooth, heightened tooth mobility, and, in some cases, tooth loss.1–3 The occurrence of gingival tissue damage may be attributed to a disparity between a regional infection and excessive inflammation from the host.4–6 The previous researches suggest that the impact of periodontal disease may extend beyond the mouth and have broader consequences throughout the body.7–9 Oral cancer is a complex inflammatory illness that arises from a combination of several risk factors, including genetics, socioeconomic factors, and lifestyle choices.10 Cancers of the head and neck region are characterised by a local inflammatory reaction.11 This response can trigger changes in cellular processes that facilitate the invasion and growth of cancer cells in primary oral carcinomas. Additionally, it can facilitate the spread of tumour cells to the gingival tissue, leading to the formation of secondary tumours.12 Interleukin-8 is a neutrophil-activating chemokine that is essential for neutrophil extravasation from gingival capillaries and movement to the periodontal sulcus.13 Excessive interleukin 8 (IL-8) production results in improper spreading and emigration of neutrophils to affected areas, which is linked to substantial periodontal tissue degradation.14 It has been shown that this chemokine exhibits pro-tumoral effects linked to establishing and progressing the malignancies.15–18
Tumour cells may express several cytokines and associated receptors that promote inflammation and induce cancer.19,20 Some studies showed that IL-8 expression in patients with breast cancer, malignant ovarian and osteo-carcinoma is associated with metastasis of cancer cells,21,22 advanced diseases, poor survival, and early recurrence.23–25 Nuclear factor kappa B (NF-κB) is an intracellular transcription factor that has a unique role in a number of inflammatory and cancer-related processes.26 Extrinsic stimuli, including cytokines, growth factors, oncoproteins, and stress signals, may trigger NF-κB pathways.27 Few investigations assessed the expression of NF-κB in the colonic tissue of patients with colonic polyps and colorectal cancer.28 Moreover, periodontal pathogens are correlated with the development of cancer in areas other than the gums, particularly the side edge of the tongue, which is the most common location.29 Previous studies establish the etio-pathological connections between chronic periodontitis and oral carcinoma or oropharyngeal cancer.30,31 The chemotactic cytokines have a role in host-microbiome interactions in periodontal disease and oral cancer.32 To date, no previous study has evaluated the correlation between oral, oropharyngeal, and parapharyngeal cancers with periodontitis (CA-with-P); oral, oropharyngeal, and parapharyngeal cancers without periodontitis (CA-without-P); and periodontitis (P) patients in salivary IL-8 and NF-κB levels and scores of clinical periodontal parameters detecting inflammation and periodontal pathogenies accumulation. This aspect motivated the present study, whose aim was to evaluate clinical periodontal parameters (PLI, BOP, PPD, CAL) and determine IL-8 and NF-κB levels from saliva, followed by an assessment of the correlation between periodontitis severity and oral, oropharyngeal, and parapharyngeal cancers.
Materials and Methods
This case study ranges between 2021 to 2024. The study comprised 300 participants from the Al-Hussein Medical City and Al-Hassan Al-Mujtabaa Hospital in Karbala, Iraq. The assessment was conducted on a consecutive series of 150 patients with cancer lesions divided into two groups: cancers with periodontitis (CA-with-P) and cancers without periodontitis (CA-without-P). The periodontitis (P) and control (C) groups comprised 75 individuals each. The ages of the male and female participants ranged between 40–65 years. The primary lesions of the oral cavity, oropharynx, or parapharyngeal spaces were resected surgically.
The criteria for inclusion and exclusion included: patients had to have at least 20 teeth; had not undergone any periodontal therapy in the preceding six months; had no lip malignancies, human immunodeficiency virus (HIV), or chronic inflammatory illnesses, such as rheumatoid arthritis or Crohn’s disease; had not taken any anti-inflammatory medications in the preceding three months; did not have diabetes, smoking habits, alcohol intake, or a family history of oral and oropharyngeal cancer, mento-labial region or pre-existing anomalies, grossed offensive of oral malignancies, or previously received radiation treatment for oral or oropharyngeal cancers.
Periodontal Examination
A single, qualified, and knowledgeable examiner conducted the periodontal examinations. For probing pocket depth (PPD) and clinical attachment loss (CAL), the intra-examiner reliability calibration was 95%. In line with the 2017 classification scheme to assess periodontitis severity, the participants were examined to ensure that the P and CA-with-P groups had an interdental CAL of ≥2 non-adjacent teeth or CAL of ≥3 mm on the buccal (facial) or lingual/palatal aspects, a PPD of >3 mm at more than two teeth, had stages III and IV periodontitis, and had grades B or C with unstable cases, meaning a PPD of ≥4 mm with bleeding on probing (BOP) or PPD of >5 mm with or without BOP.
Probing pocket depth (PPD), CAL, BOP, and plaque index (PI) were among the periodontal indicators. All teeth were assessed for clinical characteristics, with the exception of third molars. Probing pocket depth (PPD) and CAL were assessed at six places per tooth, whereas PI and BOP were recorded at four sites. The plaque index (PI) was regarded as either present or nonexistent.33 The presence or lack of bleeding following probing was used to identify BOP.34 A standardised periodontal probe (UNC-15) was used throughout the evaluations. At least two locations with CAL ≥6 mm and PPD ≥7 mm at the proximal sites of two distinct teeth were considered indicators of severe periodontitis.35 The C group had clinically healthy periodontium, BOP <10%, PPD ≤3 mm, and intact periodontiums.36
Tumour Examination
All patients were evaluated preoperatively through clinical examination and a radiographical assessment that included panoramic radiography and computed tomography examinations. The latter provided information about the location of the malignant sites in relation to the landmark of anatomy. Histopathological examination of the biopsy specimens was carried out by medical pathologists who specialise in evaluating tumours. The precise position of each tumour was determined using the third version of the International Classification of Diseases for Oncology.37 The present study was designed to include only medically fit patients who had oral, oropharyngeal or parapharyngeal lesions that required surgical excision prior to chemotherapy or radiotherapy. The patients were categorised into three groups based on the region requiring treatment, as demonstrated in Table 1.
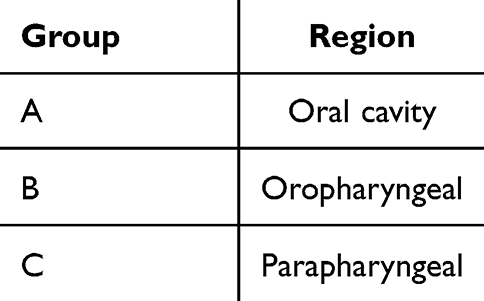 |
Table 1 Participant Division Based on Cancer Lesion Location |
Saliva Sample Collection and Analysis
The participants were encouraged to brush their teeth and floss before their saliva was collected. Unstimulated saliva samples were collected between 09:00 and 12:00. Passive drooling method of saliva collection. The patients were asked to swallow saliva first, and then allow the saliva to drain passively for five minutes over the lower lip into a clean plastic cup. A micropipette was then used to transfer 300μL of the saliva samples into an Eppendorf tube (Thermo Fisher Scientific), which was then centrifuged at 3000×g for 20 mins and stored at −20°C. The protein concentration of each biomarker was measured using an enzyme-linked immunosorbent assay (ELISA). Commercially available My BioSource ELISA kits were used to determine the levels of IL-8 and NF-κB in the saliva by following the instructions specified by the manufacturer. Antigen can be detected by sandwich ELISA. In this technique, an antibody is coated on the microtiter well. A sample containing antigen is added to the well and allowed to react with the antibody attached to the well, forming an antigen-antibody complex. After the well is washed, a second enzyme-linked antibody specific for a different epitope on the antigen is added and allowed to react with the bound antigen. Then after unbound secondary antibody is removed by washing. Finally, a substrate is added to the plate which is hydrolyzed by an enzyme to form colored products. The absorbance of all proteins was measured using a spectrophotometer plate reader. The detection limits for IL-8 and NF-κB were 2.05pg/mL and 0.15ng/mL, respectively.
Statistical Analysis
IBM’s SPSS Statistics version 22 was used to perform chi-square and analysis of variance (ANOVA) tests for statistical evaluation. Chi-square is a statistical test that can be used to investigate the correlation between two qualitative variables. In the case of scaled variables, ANOVA tests were utilised to discover significant variations. Independent T-test for intragroup comparison. Logistic regression was used to analyse the relationship between periodontitis and malignancies affecting the oral, oropharyngeal, and parapharyngeal regions in the various variables of IL-8, NF-κB and clinical periodontal parameters. Statistical significance was set at a probability ≤ 0.05.
Results
The data of the 300 subjects enrolled in the present study were analysed. It was revealed that the mean age and gender did not significantly differ across the groups. The mean PI, BOP, PPD, and CAL of the CA-with-P and P groups were considerably higher than the C and CA-without-P groups (Table 2). The CA-with-P, CA-without-P, and P groups had higher levels of salivary IL-8 and NF-κB than the C group, as shown in Figures 1 and 2. The CA-with-P group had a higher incidence of oral cavity (A) and oropharyngeal (B) cancers than the CA-without-P group. The CA-with-P group had slightly lower incidences of parapharyngeal (C) cancers than the CA-without-P group (Table 2), as illustrated in Figure 3.
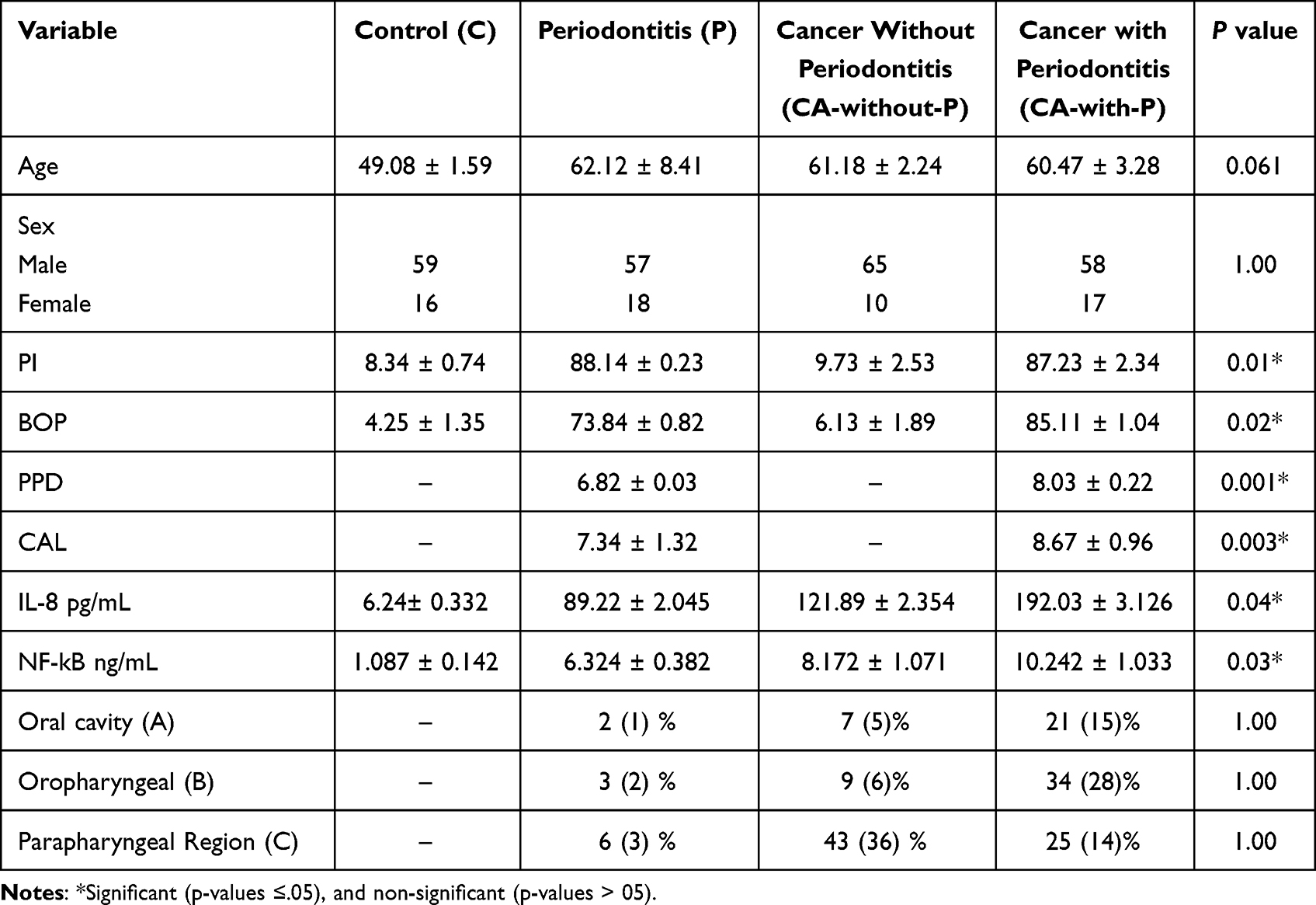 |
Table 2 The Demographic Characteristics and Clinical Periodontal Parameters of the Participants |
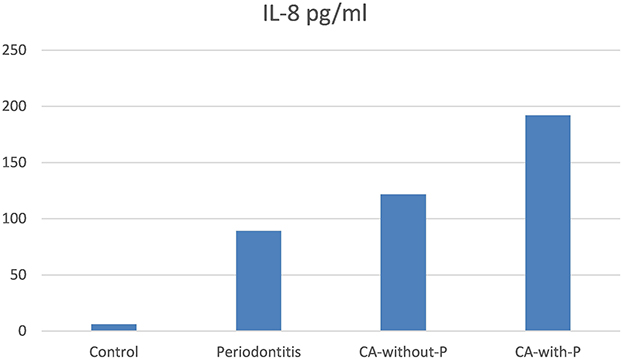 |
Figure 1 Salivary Mean of IL-8 (pg/mL) Levels in Patient Groups (Periodontitis, CA-without-P: Cancer without periodontists, CA-with-P: Cancer with Periodontitis) and Control Group. |
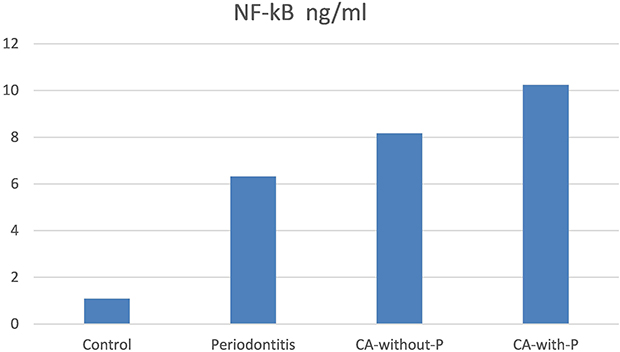 |
Figure 2 Salivary Mean of NF-kB Levels (ng/mL) in Patient Groups (Periodontitis, CA-without-P: Cancer without periodontists, CA-with-P: Cancer with Periodontitis), and Control Group. |
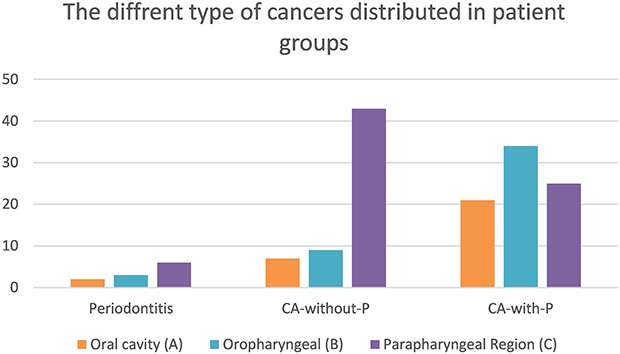 |
Figure 3 The different types of cancers according to the location distributed in patient groups (Periodontitis, CA-without-P: Cancer without periodontists, and CA-with-P: Cancer with Periodontitis). Oral cavity (A), Oropharyngeal (B), and Parapharyngeal Region (C). |
The Present Study Evaluated 150 Cancer Cases Based on Different Tissue Types and Origins (Table 3). Intragroup comparisons between subgroups of oral cavity (A), oropharyngeal (B) and parapharyngeal (C) cancers across P, CA-without-P group, and CA-with-P group are presented in (Table 4). There were significant differences (p< 0.05) between subgroups of oral cavity (A) and parapharyngeal (C) cancers and between oropharyngeal (B) and parapharyngeal (C) cancers in the CA-without-P group. Additionally, there were significant differences (p< 0.05) between subgroups of the oral cavity (A) and oropharyngeal (B) cancers in the CA-with-P group. While there were non-significant differences among sub-groups of the oral cavity (A), oropharyngeal (B) and parapharyngeal (C) cancers in the P group; between oral cavity (A) and oropharyngeal (B) cancers in the CA-without-P group. As well as between oral cavity (A) and parapharyngeal (C) cancers and between oropharyngeal (B) and parapharyngeal (C) cancers in the CA-without-P group.
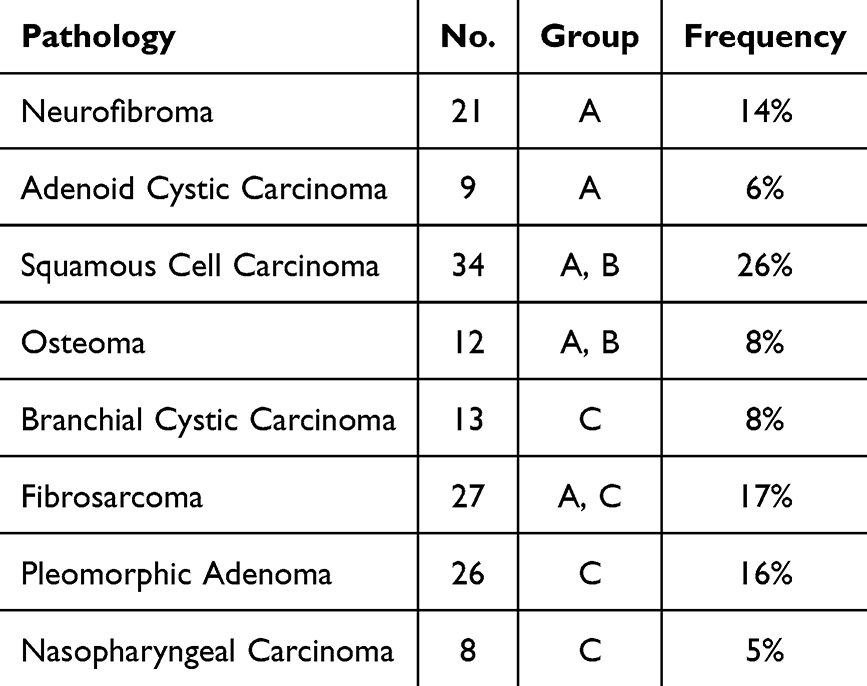 |
Table 3 The Cancer Lesion of the Participants According to the Different Types of Tissues of Origin |
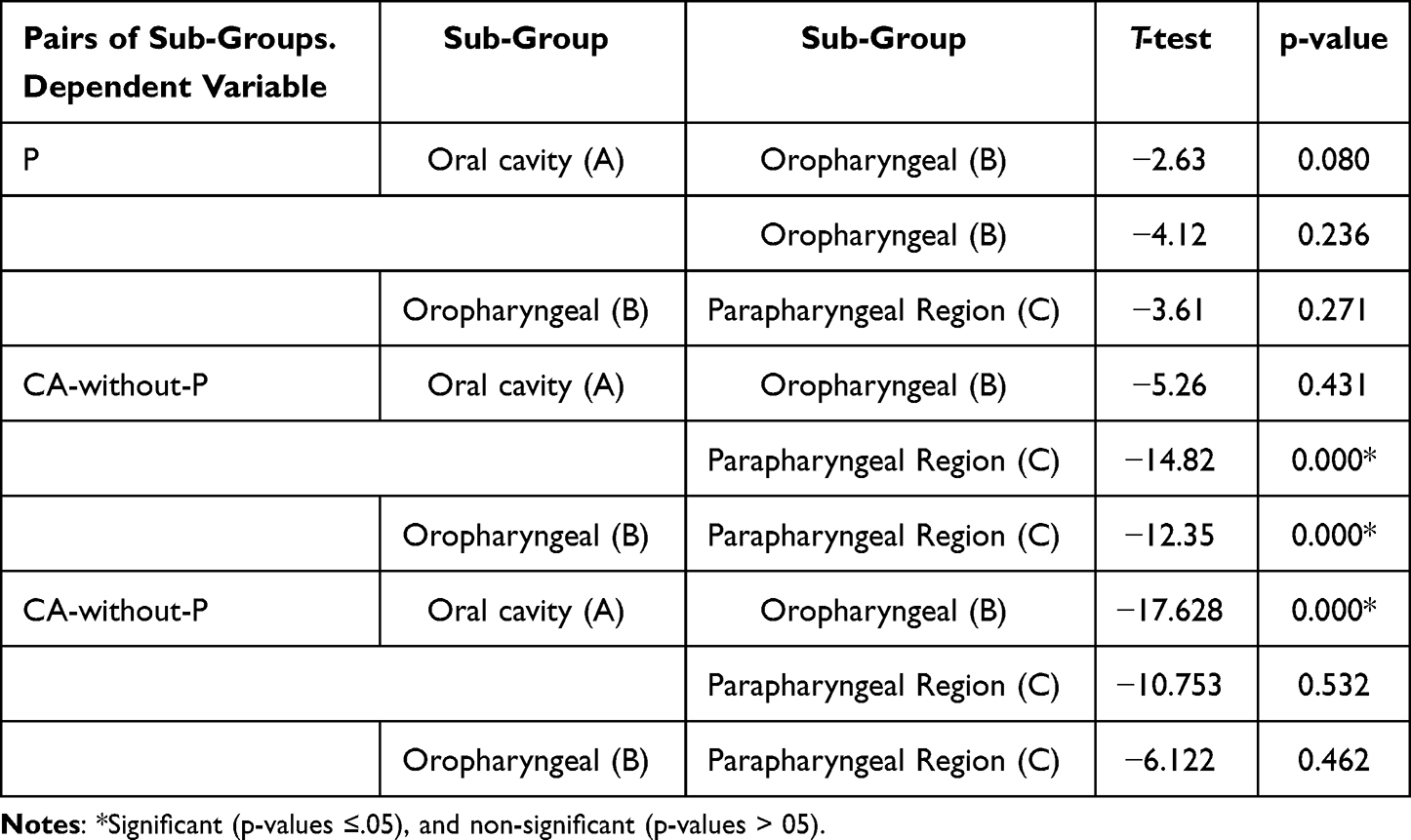 |
Table 4 Intragroup Comparisons Between Subgroups of Different Cancer Lesion Locations in the Periodontitis Group, Cancer with Periodontitis Group and Cancer with Periodontitis Group |
The correlation between periodontitis and cancers was studied using multiple logistic regression. After logistic regression models have been adjusted for age or gender. The result revealed a significant correlation between clinical periodontal parameters, lesion locations, and IL-8 and NF-κB levels with periodontitis severity and cancers (Table 5).
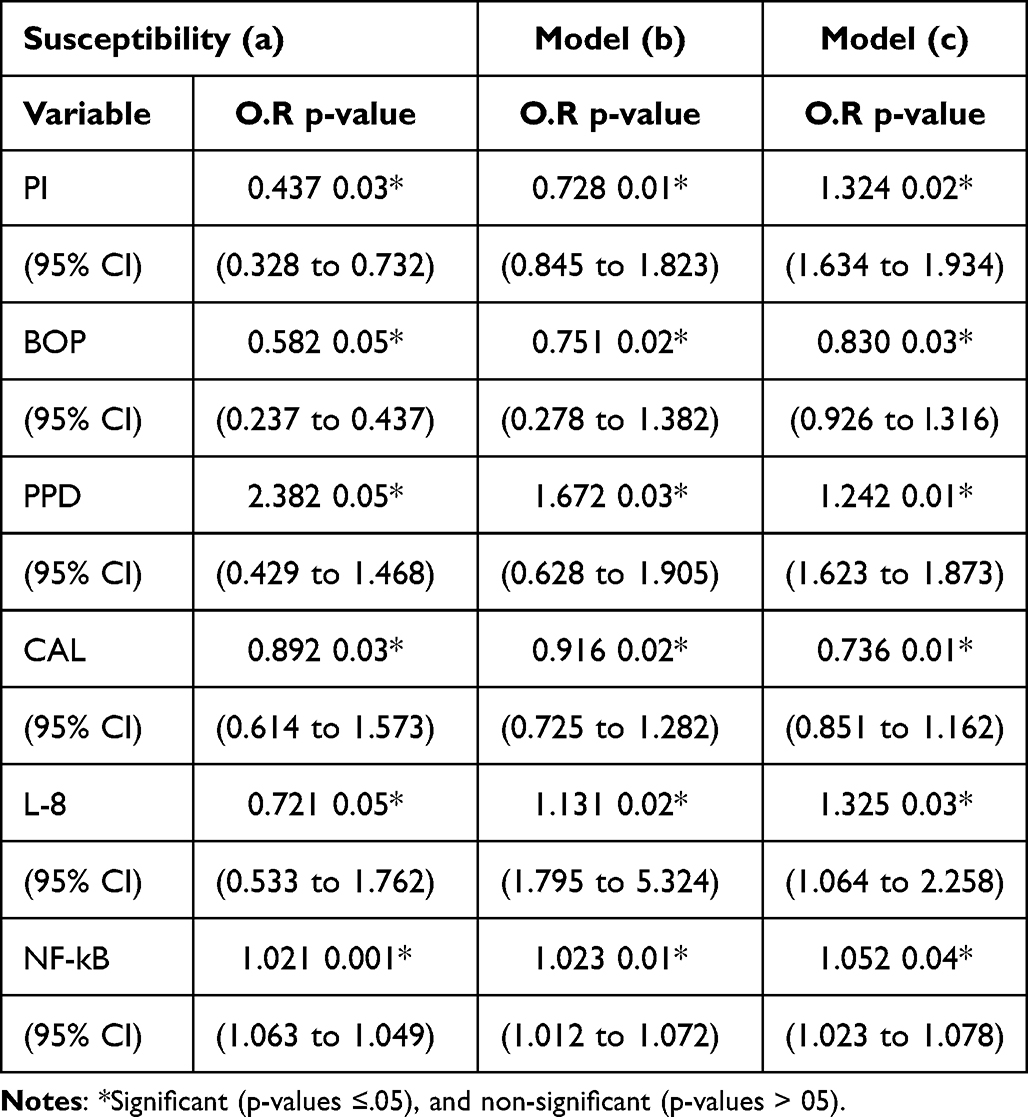 |
Table 5 The Multiple Logistic Regression Model-Based Correlations Between Periodontitis Severity and Cancers |
In logistic regression analyses, (a) represented all periodontitis and cancer cases to signify the severity of both diseases, (b) represented the controls assigned as control status and the CA-with-P and CA-without-P groups as case state in logistic regression analyses to indicate cancer lesions, and (c) represented periodontitis cases as control state in logistic regression analyses and the case state included the CA-with-P and CA-without-P groups to recognise the association between both diseases. This means the connection between periodontitis and specific cancer types is a significant association. Thus, the localized inflammation in periodontal disease with elevated periodontal parameters of inflammation (BOP, PPD, CAL), increased periodontal-pathogen accumulations (PI), and increased IL-8, NF-κB levels drive the development, propagation, and advancement of tumour formation.
Discussion
Periodontal disease and oral malignancies are two of the most prevalent inflammatory illnesses. Periodontal disease arises from a bacterial infection, and the bacteria contributes to the onset of cancers in the oral regions.38
The present study is the first to assess the mechanisms underlying the correlation between these two disorders, as elucidated by higher levels of salivary IL-8 and NF-κB. They positively and significantly correlate with the severity of clinical periodontal parameters. The results of the present study indicate higher mean values of clinical periodontal parameters in the CA-with-P and P groups than in the CA-without-P and C groups.
Principally, the current study’s findings indicate a considerable rise in periodontal parameter scores of PI and BOP in the P and CA-with-P groups. Periodontal bacteria, which contributes to the development of periodontal disorders, could have a major impact on the onset of oral cancers. First, the evidence indicates the involvement of bacterial infection in the development, propagation, and advancement of cancer.39 Furthermore, oral cancers may be significantly influenced by periodontal bacteria, which causes periodontal disorders.40 The majority of bacteria in plaque are part of the natural flora. Nonetheless, several bacteria found in the plaque of unhealthy periodontium have been recognised as potential pathogens. Oral neoplasms frequently harbour periodontal pathogens.41 Numerous studies have shown that people with periodontal disease have a two- to five-fold higher chance of developing oral cancers than those without the disease.42,43 Probing pocket depth (PPD) and CAL were also higher in the P and CA-with-P groups.
This lends credence to Sahingur et al’s hypothesis that oral squamous cell carcinoma (OSCC) develops in an environment conducive to periodontal disease severity and alterations in the oral microbiome.44 The present study indicates that periodontitis severity and malignancies of the mouth, throat, and parapharyngeal significantly correlate. The findings of the present study are also in agreement with Moraes et al’s findings that there was a substantial correlation between periodontitis and the incidence of oral cancers, even after adjusting for typical confounding variables, such as smoking, alcohol intake, and human papillomavirus.45 Another study discovered that periodontal disease-related tooth loss due to decreased bone mass is an additional risk variable for head and neck cancer.46 Moreover, individuals with periodontitis showed elevated levels of telomerase reverse transcriptase, an indicator of extremely selective expression of malignant cells.47 The immune-inflammatory responses play essential roles in the patient’s susceptibility to periodontal diseases and oral cancers.48 Therefore, it can be suggested that periodontitis severity may act as a hazard factor for oral, oropharyngeal, and parapharyngeal cancers. The present study indicates that there may be a reciprocal or bilateral correlation between periodontal disease and oral cancers. Also, oral cancers serve to cause or exacerbate periodontal disease and vice versa.
Oballe et al’s study discovered that rats exposed to the carcinogen 4-Nitroquinoline 1-oxide (4-NQO) developed OSCCs, indicating a significant amount of spontaneous alveolar bone loss. It contrasted with the group receiving treatment, which led to the non-development of OSCC, and the control group, which was not given 4-NQO. Consequently, the occurrence of squamous cells with malignant sites in their oral cavities may correlate with an increase in their alveolar bone loss.49 Pushalkar et al discovered that, in the same participants, the pathogenic microbial communities at tumour sites tended to be more distinct than those at non-tumour sites.50 It has been proposed that this microbial shift causes persistent inflammation in cancer locations and may aid in spreading cancer to nearby locations. This illustrates the correlation between the two illnesses and their causes. The alterations of the mouth milieu may provide circumstances conducive to the emergence of periodontal disease, oral cancers, or their combination. Interleukin 8 (IL-8) protein levels were higher in the saliva of the CA-with-P, CA-without-P, and P groups than in the C group.
Chemotactic cytokines, such as IL-8, stimulate the recruitment of inflammatory cells and increase the severity of periodontal deterioration and progression of cancers. They are produced by several cell types, including mast cells, fibroblasts, endothelial cells, macrophages, and lymphocytes that can induce immune response.51 Interestingly, this result is in agreement with studies of severe periodontal disease, illustrated by higher mean PPD at sites, which may correlate with higher salivary IL-8 levels.52,53 Neoplastic patients have higher levels of IL-8 than individuals with normal tissues. The role of IL-8 in the invasion and migration of tumour cells is crucial for tumour growth and metastasis.54 The main mediator of oral cancer-related systemic alterations is IL-8.55 Cancer tissues also show an over-expression of IL-8. It has also been linked to the metastatic phenotype and highly invasive capacity of cancer cells.56,57 Their capacity to draw in leukocytes and intensify or prolong the inflammatory response, has significant effects on periodontium illnesses like chronic periodontitis developing with tissue loss. Chronic inflammation is also becoming more recognised as a major factor in the development of tumours. Secreted substances like chemokines play a major role in mediating interactions between cancer cells and their environment and assist in augmenting the phenotypes of malignancy in oral and other cancers. IL-8 cytokines have the biological and biochemical process of chemokine acting in host-microbiome interactions in the pathophysiology of periodontitis and oral cancer.32
The CA-with-P, CA-without-P, and P groups had significantly higher levels of salivary NF-κB than the C group. Nuclear factor kappa B (NF-κB) regulates cytokine expression through numerous mechanisms. Abnormal NF-κB activity can lead to unregulated expression of interleukin in cancer metastasis and periodontal tissues.57 In mammary cancer cells, NF-κB stimulates the transcription of numerous genes encoding cytokines, receptors, and growth factors that lead to the formation and growth of cancers.58 Nuclear factor kappa B (NF-κB)’s constitutive activity correlates to aggressive cancer types, with its transcription factors linked to cancer formation and growth.58 Furthermore, NF-κB regulates IL-8 gene expression through signals, such as lipopolysaccharide and oxidative stress, resulting in optimum gene activation in cancer cells.56,58 Timing of NF-κB activation affects transcriptional responses to stimuli. NF-κB activation enhances inflammatory gene transcription, but prolonged activation changes the epigenome and affects a wider variety of genes.59 NF-κB signalling activates the family transcription factors, which bind to pro-inflammatory gene promoter regions to directly inhibit RELA and RELB function. This negative feedback loop enhances our knowledge of NF-κB signalling and offers an opportunity for treatment.60 NF-κB signalling has a key role in inflammatory reactions. Its function can be broadened to include a range of signalling pathways, biological processes, illness in humans, and therapeutic possibilities. The pathological and physiological conditions of NF-κB signalling, besides its complex roles in immune modulation, inflammation, and the malignant environment.61
In terms of the anatomical sites of the tumour, the CA-with-P group had a higher percentage of oral (A) and oropharyngeal (B) cancers than the CA-without-P group. Furthermore, oral and oropharyngeal cancer patients had higher periodontitis severity than parapharyngeal cancer patients. This could be because easier access to the oral region allows for earlier identification and diagnosis, which prevents cancer progression during oral examination.62,63 Pharyngeal cancers closely correlate with these areas as they have more blood and lymph vessels, are challenging to evaluate, and can affect the tumour’s prognosis and progression in addition to making detection and treatment more challenging.64
There is a strong correlation between cervical metastases and parapharyngeal carcinoma, with an incidence of 50–70%.65 However, due to its greater tumour dissemination, besides being located in regions difficult to visualise and diagnose.66
In head and neck squamous cell carcinomas, the oral and the oropharyngeal regions are more commonly affected.67,68 These regions are more affected in periodontitis patients as well as pathogenic periodontal microbiomes, such as Fusobacterium nucleatum and Porphyromonas gingivalis, are isolated from these sites. Apart from that, bacterial infections are known contributors to the development, advancement, and promotion of cancers.40 There are molecular pathways by which periodontal infections contribute to the development of mouth cancer. Pathogens actively interact with the host epithelium through a distinct molecular communication process to acquire cancer characteristics. Additionally, they indirectly promote the development of cancer by creating a pro-inflammatory environment and releasing carcinogenic substances. Cancer development correlates with the functional qualities of the oral microbial population rather than its compositional properties.41 The results of Shiga et al’s study indicate that the frequency of gene hypermethylation and allelic loss varies significantly across oral and pharyngeal malignancies. Although all of these tumours are identified as squamous cell carcinomas, the carcinogenesis process may change for tumours that are situated in different regions of the head and neck. Tumours in the pharynx arise from the loss of function of tumour suppressor genes caused by allelic loss, whereas carcinogenesis in the oral cavity is caused by the loss of function due to the methylation of those genes’ promoter regions.69 Moreover, in underdeveloped nations, the likelihood of oral cancer is higher than that of pharyngeal cancer.70 Cancer is exacerbated by persistent inflammation as in periodontal disease.7 Carcinogenic consequences are exacerbated by dysbacteriosis in periodontal disease.71 All of these point to an apparent correlation between periodontal disease and oral, oropharyngeal, and parapharyngeal cancers. Additionally, it implies a causal correlation between oral cancers and periodontitis severity. The influence of perio-pathogens on periodontal diseases and oral, oropharyngeal, and parapharyngeal cancer can describe the pathophysiology of oral cancers, and emphasise the oral hygiene required to prevent oral diseases, particularly oral cancers. The limitation of this study includes a lack of microbiological and biomolecular examinations owing to the need for different sample types and higher costs. The small sample size can result in a decent percentage of oral cavity (A) and oropharyngeal (B) cancers in the P group and the CA-without-P group. The CA-with-P group had slightly lower incidences of parapharyngeal (C) cancers than the CA-without-P group lacks longitudinal data because it requires more time for the study.
Conclusion
The primary finding of this study is a significant correlation between periodontitis with malignancies in the oral, oropharyngeal, and parapharyngeal regions as evidenced by higher levels of salivary IL-8 and NF-κB. This study assessed the mechanisms underlying the correlation between these two disorders, as elucidated by higher levels of salivary IL-8 and NF-κB when compared to controls. They positively and significantly correlate with the increase of clinical periodontal parameters compared with controls. The present evidence strongly suggests that periodontal disease may be an indicator of oral cancers. Owing to the periodontitis severity brought on by perio-pathogens, carcinogenesis can occur elsewhere.38 It typically manifests outside the gingiva, most frequently in the oral cavity and the oropharyngeal region.41 A microenvironment that facilitates the advancement of cancer is created by periodontal disease-related phenotypic changes and functional abnormalities in the periodontium’s immunological (IL-8, NF-κB) and stromal components.56,58 However, the tendency to recruit leukocytes and prolonged the process of inflammation may contribute to the advancement of oral illnesses such as chronic periodontitis, causing tissue damage. Furthermore, persistent inflammation is a significant factor in tumour growth. Secreted substances such as chemokines have an important role in the interaction between tumour cells and their surrounding environment, leading to the phenotype of tumours in oral and other malignancies.32 Interleukin 8 (IL-8) plays an important role in carcinogenesis as well as in immune and inflammatory response regulation. Its expression may be deregulated in cancer metastasis due to the aberrant activity of NF-κB.54,57 Nuclear factor kappa B (NF-κB) transcription factors participate in the development and growth of cancer.58 NF-κB signalling has a crucial role in physiological and pathological states, as well as its complex roles in immunological control, inflammation, and the cancerous microenvironment.61 Thus, the inflammatory environment in periodontal disease is perfect for the seeding, migration, proliferation, and escape of cancer cells. Therefore, periodontitis patients are more susceptible to malignancies affecting the oral, oropharyngeal, and parapharyngeal regions, and periodontitis severity may serve as a predictor of oral, oropharyngeal, and parapharyngeal cancers.
Ethics Approval and Consent to Participate
All procedures performed in this study involving human participants followed the Declaration of Helsinki and its later amendments for human research. The study was conducted in accordance with and approved by the Ethics Committee of the College of Dentistry, University of Al-Ameed, Iraq (number 124). All participants entered the study after they received full information about the nature, aims and processes of the study before signing an informed written consent form.
Acknowledgments
The authors would like to thank Mustansiriyah University/College of Dentistry, Baghdad – Iraq (www.uomustansiriyah.edu.iq), and the University of Al-Ameed/College of Dentistry for their support during work.
Funding
This work was supported by the This study was self-funded.
Disclosure
The authors declare no competing interests.
References
1. Könönen E, Gursoy M, Gursoy UK. Periodontitis: a multifaceted disease of tooth-supporting tissues. J Clin Med. 2019;8:1135. doi:10.3390/jcm8081135
2. Usui M, Onizuka S, Sato T, Kokabu S, Ariyoshi W, Nakashima K. Mechanism of alveolar bone destruction in Periodontitis-Periodontal bacteria and inflammation. Jpn Dent Sci Rev. 2021;57:201–208. doi:10.1016/j.jdsr.2021.09.005
3. Harbood OM, Abbas RF, Hussein HM, Hamed NA, Mahmood AA, Mahmood MS. Diagnostic ability of salivary IL-6 and MMP-9 biomarkers in different stages of periodontitis (case-control study). J Emerg Med Trauma Acute Care. 2024;2024(8):1.
4. Loesche WJ, Grossman NS. Periodontal disease as a specific, albeit chronic, infection: diagnosis and treatment. Clin Microbiol Rev. 2001;14:727–752. doi:10.1128/CMR.14.4.727-752.2001
5. Daily ZA, Al‑Ghurabei BH, Al-Qarakhli AMA, Hussein HM. Association between AIM2 and pycard genes polymorphisms and susceptibility to periodontitis with coronary heart disease. J Clinic Cosme Investig Dent. 2023;15:307–320. doi:10.2147/CCIDE.S440577
6. Mahmood AA, Abbas RF. Association between caspase-1, TNF-α salivary level and their diagnostic potential to discriminate periodontitis from healthy control. Oral Health Prev Dent. 2023;16(21):61–68. doi:10.3290/j.ohpd.b3904349
7. Amar S, Han X. The impact of periodontal infection on systemic diseases. Med Sci Monit. 2003;9:291–299.
8. Oindrila P, Payal A, Michael M, Shampa C. Inflammation in periodontal disease: possible link to vascular disease. Front Physiol. 2021;11:609614. doi:10.3389/fphys.2020.609614
9. Salhi L, Rompen E, Sakalihasan N, Teughels W, Michel JB, Lambert F. Can periodontitis influence the progression of abdominal aortic aneurysm? A systematic review. Angiology. 2019;70:479–491. doi:10.1177/0003319718821243
10. Komlós G, Csurgay K, Horváth F, Pelyhe L, Németh Z. Periodontitis as a risk for oral cancer: a case–control study. BMC Oral Health. 2021;21:640. doi:10.1186/s12903-021-01998-y
11. Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int, J, Cancer. 2019;144:1941–1953. doi:10.1002/ijc.31937
12. Irani S, Barati I, Badiei M. Periodontitis and oral cancer - current concepts of the etiopathogenesis. Oncology Reviews. 2020;14(1):465. doi:10.4081/oncol.2020.465
13. Garlet GP, Martins JW, Ferreira BR, Milanezi CM, Silva JS. Patterns of chemokines and chemokine receptors expression in different forms of human periodontal disease. J Periodontal Res. 2003;38(2):210–217. doi:10.1034/j.1600-0765.2003.02012.x
14. Konopka L, Pietrzak A, Brzezińska-Błaszczyk E. Effect of scaling and root planing on interleukin-1β, interleukin-8 and MMP-8 levels in gingival crevicular fluid from chronic periodontitis patients. J Periodontal Res. 2012;47(6):681–688. doi:10.1111/j.1600-0765.2012.01480.x
15. Alfaro C, Sanmamed MF, Rodríguez-Ruiz ME, et al. Interleukin-8 in cancer pathogenesis, treatment and follow-up. Cancer Treat Rev. 2017;60:24–31. doi:10.1016/j.ctrv.2017.08.004
16. Abbas MJ, Al-Rawi NA, Al-Duboni GI. Assessment of interleukin −10 and interferon-gamma with oral squamous cell carcinoma patients compared with healthy subjects as a prediction for early detection and monitor treatment response. Mustansiria Dent J. 2019;16(1):68–77. doi:10.32828/mdj.v16i1.1026
17. Hussien GG, Ali OH. Evaluation of salivary tumor necrosis factor-alpha in patients with hypothyroidism and periodontitis: a case- control study. Mustansiria Dent J. 2023;19(1):92–106. doi:10.32828/mdj.v19i1.995
18. Abbas MJ, Al-Rawi NA, Al-Duboni GI. The role of salivary interleukin 17 as a dependent positive predictive biomarker among Iraqi patients with oral squamous cell carcinoma. J Pharm Sci Res. 2018;10(12):3149–3152.
19. Lacalle RA, Blanco R, Carmona-Rodríguez L, Martín-Leal A, Mira E, Mañes S. Chemokine receptor signaling and the hallmarks of cancer. Int Rev Cell mol Biol. 2017;331:181–244. doi:10.1016/bs.ircmb.2016.09.011
20. Daily ZA, Al‑Ghurabei BH, Al‑Qarakhli AM, Moseley R. MicroRNA‐155 (miR‑155) as an accurate biomarker of periodontal status and coronary heart disease severity: a case–control study. BMC Ora Heal J. 2023;23:868. doi:10.1186/s12903-023-03584-w
21. Zuccari DA, Leonel C, Castro R, et al. An immunohistochemical study of interleukin-8 (IL-8) in breast cancer. Acta Histochem. 2012;114(6):571–576. doi:10.1016/j.acthis.2011.10.007
22. Milovanovic J, Todorovic-Rakovic N, Abu Rabi Z. The prognostic role of interleukin-8 (IL-8) and matrix metalloproteinases −2 and −9 in lymph node-negative untreated breast cancer patients. J Balkan Union Oncol. 2013;18(4):866–873.
23. Lin Y, Huang R, Chen L, et al. Identification of interleukin-8 as estrogen receptor-regulated factor involved in breast cancer invasion and angiogenesis by protein arrays. Int, J, Cancer. 2004;109(4):507–515. doi:10.1002/ijc.11724
24. Chen Y, Chen L, Li JY, et al. ERbeta and PEA3 co-activate IL-8 expression and promote the invasion of breast cancer cells. Cancer Biol Ther. 2011;11(5):497–511. doi:10.4161/cbt.11.5.14667
25. Todorovic-Rakovic N, Milovanovic J. Interleukin-8 in breast cancer progression. J Interferon Cytokine Res. 2013;33(10):563–570. doi:10.1089/jir.2013.0023
26. Ben-Neriah Y, Karin M. Inflammation meets cancer, with NF-κB as the matchmaker. Nat Immunol. 2011;12:715–723. doi:10.1038/ni.2060
27. Patel M, Horgan PG, McMillan DC, Edwards J. NF-κB pathways in the development and progression of colorectal cancer. Transl Res. 2018;197:43–56. doi:10.1016/j.trsl.2018.02.002
28. Berkovich L, Gerber M, Katzav A, Kidron D, Avital S. NF-kappa B expression in resected specimen of colonic cancer is higher compared to its expression in inflammatory bowel diseases and polyps. Sci Rep. 2022;12:16645. doi:10.1038/s41598-022-21078-7
29. Sreenivasan PK, Prasad KVV. Distribution of dental plaque and gingivitis within the dental arches. J Int Med Res. 2017;45:1585–1596. doi:10.1177/0300060517705476
30. Karmakar S, Modak B, Solomon MC. Exploring the causal relationship between chronic periodontitis and oral cancer: an insight. Oral Oncology Reports. 2024;11:100468. doi:10.1016/j.oor.2024.100468
31. Xiong J, Liu H, Li C, Li Y, Feng J. Linking periodontitis with 20 cancers, emphasis on oropharyngeal cancer: a Mendelian randomization analysis. Sci Rep. 2024;14:12511. doi:10.1038/s41598-024-63447-4
32. Sahingur SE, Yeudall WA. Chemokine function in periodontal disease and oral cavity cancer. Front Immunol. 2015;6:214.
33. O’Leary TJ, Drake RB, Naylor JE. The plaque control record. J Periodontol. 1972;43(1):38. doi:10.1902/jop.1972.43.1.38
34. Mühlemann HR, Son S. Gingival sulcus bleeding--a leading symptom in initial gingivitis. Helv Odontol Acta. 1971;15:107–113.
35. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Periodontol. 2018;89(1):159–s172. doi:10.1002/JPER.18-0006
36. Chapple ILC, Mealey BL, Van Dyke TE, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: consensus report of workgroup 1 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Clin Periodont. 2018;45(20):S68–S77. doi:10.1111/jcpe.12940
37. International Classification of Diseases for Oncology (ICD-O), 3rd Ed. 1st Revision. World Health Organization 2019.
38. Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol. 2013;62:59–94. doi:10.1111/j.1600-0757.2012.00457.x
39. Shin Y, Choung H, Lee J, Rhyu I, Kim H. Association of periodontitis with oral cancer: a case-control study. J Dent Res. 2019;98:526–533. doi:10.1177/0022034519827565
40. Al-Hebshi NN, Nasher AT, Maryoud MY, et al. Inflammatory bacteriome featuring Fusobacterium nucleatum and Pseudomonas aeruginosa identified in association with oral squamous cell carcinoma. Sci Rep. 2017;7:1834. doi:10.1038/s41598-017-02079-3
41. Li T, Hao Y, Tang Y, Liang X. Periodontal pathogens: a crucial link between periodontal diseases and oral cancer. Front Microbiol. 2022;30(13):919633. doi:10.3389/fmicb.2022.919633
42. Lafuente Ibáñez de Mendoza I, Maritxalar Mendia X, de la Fuente AM G, Quindós Andrés G, Aguirre Urizar JM. Role of porphy romonas gingivalis in oral squamous cell carcinoma development: a systematic review. J Periodontal Res. 2020;55:13–22. doi:10.1111/jre.12691
43. Javed F, Warnakulasuriya S. Is there a relationship between periodontal disease and oral cancer? A systematic review of currently available evidence. Crit Rev Oncol/Hematol. 2016;97:197–205. doi:10.1016/j.critrevonc.2015.08.018
44. Sahingur SE, Yeudall WA, Bancu I, Lauzurica-Valdemoros R, Borràs FE. Chemokine function in periodontal disease and oral cavity cancer. Front Immunol. 2015;6:6. doi:10.3389/fimmu.2015.00006
45. Moraes RC, Dias FL, Figueredo CM, Fischer RG. Association between chronic periodontitis and oral/oropharyngeal cancer. Brazil Dental J. 2016;27:261–266. doi:10.1590/0103-6440201600754
46. Shi J, Leng W, Zhao L, Deng C, Xu C, Wang J. Tooth loss and cancer risk: a dose–response meta analysis of prospective cohort studies. Oncotarget. 2018;9:15090. doi:10.18632/oncotarget.23850
47. Katarkar A, Saha A, Mukherjee S, Kundu D, Bandyopadhyay P, Chaudhuri K. Telomerase expression in individuals with chronic and aggressive periodontitis. J Periodontol. 2015;86:656–665. doi:10.1902/jop.2015.140540
48. Cavallo F, De Giovanni C, Nanni P, Forni G, Lollini PL. The immune hallmarks of cancer. Cancer Immunol Immunother. 2011;60:319–326. doi:10.1007/s00262-010-0968-0
49. Oballe H, Muniz F, Bueno CC, et al. Spontaneous alveolar bone loss after 4NQO exposure in Wistar rats. Arch Oral Biol. 2018;89:448. doi:10.1016/j.archoralbio.2018.02.001
50. Pushalkar S, Ji X, Li Y, et al. Comparison of oral microbiota in tumor and non-tumor tissues of patients with oral squamous cell carcinoma. BMC Microbiol. 2012;12:144. doi:10.1186/1471-2180-12-144
51. O’Hara AM, Bhattacharyya A, Mifflin RC, Smith MF, Ryan KA, Scott KG-E. Interleukin-8 induction by helicobacter pylori in gastric epithelial cells is dependent on apurinic/apyrimidinic endonuclease-1/redox factor-1. J Immunol. 2006;177:7990–7999. doi:10.4049/jimmunol.177.11.7990
52. Jacob PS, Nath S, Patel RP. Evaluation of interleukin-1β and 8 in gutka chewers with periodontitis among a rural Indian population. J Periodontal Implant Sci. 2014;44(3):126–133. doi:10.5051/jpis.2014.44.3.126
53. Frasheri I, Heym R, Ern C, et al. Salivary and Gingival CXCL8Correlation with periodontal status, periodontal pathogens, and smoking. Oral Dis. 2022;28(8):2267–2276. doi:10.1111/odi.13994
54. Cacev T, Radosevic S, Krizanac S, Kapitanovic S. Influence of interleukin-8 and interleukin-10 on sporadic colon cancer development and progression. Carcinogenesis. 2008;29(8):1572–1580. PubMed ID: 18628251. doi:10.1093/carcin/bgn164
55. Briukhovetska D, Dörr J, Endres S, Libby P, Dinarello CA, Kobold S. Interleukins in cancer: from biology to therapy. Nat Rev Cancer. 2021;21:481–499. doi:10.1038/s41568-021-00363-z
56. Thyagarajan A, Jiang J, Hopf A, Adamec J, Sliva D. Inhibition of oxidative stress-induced invasiveness of cancer cells by ganoderma lucidum is mediated through the suppression of interleukin-8 secretion. Int J Mol Med. 2006;18(4):657–664.
57. Malonia SK, Yadav B, Sinha S, Lazennec G, Chattopadhyay S. Chromatin remodeling protein SMAR1 regulates NF-kappaB dependent Interleukin-8 transcription in breast cancer. Int J Biochem Cell Biol. 2014;55:220–226. doi:10.1016/j.biocel.2014.09.008
58. Freund A, Chauveau C, Brouillet JP, et al. IL-8 expression and its possible relationship with estrogen-receptor-negative status of breast cancer cells. Oncogene. 2003;22(2):256–265. doi:10.1038/sj.onc.1206113
59. Cheng QJ, Ohta S, Sheu KM, et al. NF-κB dynamics determine the stimulus specificity of epigenomic reprogramming in macrophages. Science. 2021;372(6548):1349–1353. doi:10.1126/science.abc0269
60. Liu Z, Mar KB, Hanners NW, et al. A NIK–SIX signalling axis controls inflammation by targeted silencing of non-canonical NF-κB. Nature. 2019;568:249–253. doi:10.1038/s41586-019-1041-6
61. Qing Guo Q, Jin Y, Chen X, et al. Zhang J.NF-κB in biology and targeted therapy: new insights and translational implications. Signal Transduct Target The. 2024;9:53. doi:10.1038/s41392-024-01757-9
62. Moro JS, Maroneze MC, Ardenghi TM, BarinL M. DanesiC C.Oral and oropharyngeal cancer: epidemiology and survival analysis. Einseinstein. 2018;16(2):eAO4248.
63. Epstein JB, Gorsky M, Cabay RJ, Day T, Gonsalves T. Screening for and diagnosis of oral premalignant lesions and oropharyngeal squamous cell carcinoma. Can Fam Physician. 2008;54(6):870–875.
64. Massano J, Regateiro FS, Januàrio G, Ferreira A. Oral squamous cell carcinoma: review of prognostic and predictive factors. Oral Surg, Oral Med Oral Pathol Oral Radiol Endod. 2006;102(1):67–76. [Review]. doi:10.1016/j.tripleo.2005.07.038
65. Becker M. Oral cavity, oropharynx and hypopharynx. Semin Roentgenol. 2000;35(1):21–30. Review.
66. Vogel DW, Zbearen P, Thoeny CH. Cancer of the oral cavity and oropharynx. Cancer Imaging. 2010;10(1):62–72. doi:10.1102/1470-7330.2010.0008
67. Chi AC, Day TA, Neville BW. Oral cavity and oropharyngeal squamous cell carcinoma--an update. CA Cancer J Clin. 2015;65(5):401–421. doi:10.3322/caac.21293
68. Julian RS, Woo BM, Rabey EC. Oral cavity and oropharyngeal cancer: etiology, diagnosis and staging. J California Dent Assoc. 2021;49(3):163–170. doi:10.1080/19424396.2021.12222685
69. Shiga K, Ogawa T, Katagiri K, et al. Differences between oral cancer and cancers of the pharynx and larynx on a molecular level. Oncology Letter. 2011;3(1):238–243. doi:10.3892/ol.2011.451
70. Franceschi S, Bidoli E, Herrero R, Muñoz N. Comparison of cancers of the oral cavity and pharynx worldwide: etiological clues. Oral Oncol. 2000;36(1):106–115. doi:10.1016/S1368-8375(99)00070-6
71. Oveisi M, Shifman H, Fine N, et al. Novel assay to characterize neutrophil responses to oral biofilms. Infect Immun. 2019;87:e00790–18. doi:10.1128/IAI.00790-18
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.