Back to Journals » Clinical Interventions in Aging » Volume 20
Prevalence of Multiple Chronic Conditions in Older Adults with Undiagnosed Mild Cognitive Impairment and Alzheimer’s Disease and Related Dementias in Primary Care
Authors Summanwar D ![]() , Owora AH, Ben Miled Z
, Owora AH, Ben Miled Z ![]() , Dexter PR, Kulshreshtha A, Strunk S, Jiang B, Coppedge K, Disla S, Galvin JE, Boustani M
, Dexter PR, Kulshreshtha A, Strunk S, Jiang B, Coppedge K, Disla S, Galvin JE, Boustani M ![]() , Fowler NR
, Fowler NR
Received 5 June 2025
Accepted for publication 3 October 2025
Published 24 October 2025 Volume 2025:20 Pages 1799—1809
DOI https://doi.org/10.2147/CIA.S544727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Diana Summanwar,1 Arthur H Owora,2,3 Zina Ben Miled,4 Paul R Dexter,5 Ambar Kulshreshtha,6 Samuel Strunk,2 Bowen Jiang,2 Katrina Coppedge,7 Shanell Disla,8 James E Galvin,8 Malaz Boustani,5,7,9 Nicole R Fowler5,7,9
1Department of Family Medicine, Indiana University School of Medicine, Indianapolis, IN, USA; 2Translational Informatics, Biostatistics and Epidemiology Lab, Indiana University School of Medicine, Indianapolis, IN, USA; 3Center for Biomedical Informatics, Regenstrief Institute, Indianapolis, IN, USA; 4Phillip M. Drayer Department of Electrical and Computer Engineering, Lamar University, Beaumont, TX, USA; 5Regenstrief Institute, Indianapolis, IN, USA; 6Department of Family and Preventive Medicine, Emory University, Atlanta, GA, USA; 7Department of Medicine, Indiana University School of Medicine, Indianapolis, IN, USA; 8Comprehensive Center for Brain Health, Department of Neurology, University of Miami Miller School of Medicine, Boca Raton, FL, USA; 9Indiana University Center for Aging Research, Indianapolis, IN, USA
Correspondence: Diana Summanwar, Department of Family Medicine, Indiana University School of Medicine, 1040 Wishard Blvd, Indianapolis, IN, 46202, USA, Tel +1 317-278-1090, Fax +317-962-5479, Email [email protected]; [email protected]
Background: Most adults aged ≥ 65 years live with multiple chronic conditions (MCC), and nearly one in four have recognized or unrecognized Alzheimer’s disease and related dementias (ADRD), including an estimated 7.2 million Americans. Together, MCC and ADRD increase treatment complexity, medication burden, and the risk of adverse outcomes. Among patients who meet clinical criteria for mild cognitive impairment (MCI) or ADRD but lack a formal diagnosis, MCC burden remains unclear. This study examined the association between MCC burden and undiagnosed MCI and ADRD in a diverse cohort of older adults in primary care.
Methods: We conducted a cross-sectional analysis of 324 adults aged ≥ 65 from primary care clinics in Indiana and South Florida (2021– 2023), as part of a larger ADRD detection study. Patients without documented MCI or ADRD completed standardized cognitive assessments. Cognitive status (normal, MCI, ADRD) was determined by interdisciplinary consensus. Chronic conditions and medications were extracted from electronic health records. Multinomial logistic regression was used to examine the association between MCC profiles and cognitive status.
Results: Among 324 older adults, 51.9% were determined to have MCI and 8% ADRD. Patients with MCI and ADRD had more chronic conditions (mean = 5– 6) and medications (mean = 4– 5) than those with normal cognition (p < 0.001). Anticholinergic use was more common in the MCI (23.8%) and ADRD (23.1%) groups than in those with normal cognition (10.8%). In adjusted models, MCI and ADRD were associated with higher odds of having more chronic conditions. Cerebrovascular disease was associated with both MCI and ADRD; diabetes, sleep apnea, and insomnia with MCI; and ischemic heart disease and insomnia with ADRD.
Conclusion: Older adults with unrecognized MCI and ADRD experience substantial MCC and medication burden. These findings highlight the need for targeted primary care interventions that integrate cognitive screening, support MCC management, optimize self-management capacity, and promote safer prescribing.
Plain Language Summary: Many older adults live with multiple long-term health conditions and take several medications. Some also have memory or thinking problems, like mild cognitive impairment (MCI) or dementia, that have not yet been diagnosed.
In this study, we looked at older adults receiving care at primary care clinics to understand how undiagnosed memory problems are related to other health issues. We found that people with unrecognized MCI or dementia had more chronic conditions and were taking more medications than those with normal memory. Certain health problems, like stroke, diabetes, and sleep disorders, were more common in people with memory issues. We also found that medications known to affect memory (called anticholinergics) were used more often in people with memory problems, especially in younger patients.
These findings suggest that doctors and care teams should consider memory problems when treating older adults with complex health needs. By doing so, they can create safer care plans, choose better medications, and help patients manage their health more effectively.
Keywords: mild cognitive impairment, dementia, Alzheimer disease, primary health care, comorbidity, anticholinergic agents, polypharmacy, multimorbidity, Polypharmacy, geriatric assessment
Introduction
Primary care clinicians are the primary point of care for older adults living with multiple chronic conditions (MCC) and Alzheimer’s disease and other related dementias (ADRD).1,2 The Agency of Healthcare Research and Quality defines MCC as the “co-occurrence of two or more chronic physical or mental health conditions”.3 Most adults aged 65 and older live with MCC,4 and nearly one in four are affected by recognized or unrecognized ADRD.5
Delayed or missed diagnosis increases the burden on patients, families, and society.6,7 In response, multiple organizations have identified early ADRD detection as a key priority for improving the quality of care for older adults.8–10 Despite their central role, primary care clinicians face barriers to early detection, including limited time and resources, the absence of structured workflows, and insufficient training and confidence in diagnosing ADRD.11–16
Social determinants of health compound these challenges. Limited access to primary care, lower health literacy, and socioeconomic constrains contribute to delayed diagnosis, reduced engagement in follow-up care, and worse outcomes for both ADRD and MCC.1,12,16–20
Several care models have been developed to integrate cognitive screening with MCC disease management in primary care. These include comprehensive dementia care models such as the Healthy Aging Brain Cener;21 nurse-led navigation programs such as the Brain Health Navigator;22 and collaborative care initiatives such as the Guiding an Improved Dementia Experience (GUIDE) Model,23 a national program designed to support patients with ADRD and their families.
The co-occurrence of MCC and ADRD imposes a substantial burden on patients, families, and healthcare systems.5,24 Managing MCC often involves adherence to multiple disease-specific guidelines, which frequently leads to the prescription of 10 or more medications –many with conflicting benefit-harm profiles.25–32 This high medication burden increases the complexity of disease self-management and raises the risk of drug interactions, administration errors, and adverse outcomes,33–35 particularly for individuals with ADRD.36 Among the most concerning medications are anticholinergics,37 which block acetylcholine, a neurotransmitter essential for cognitive function, and have been associated with cognitive decline and elevated ADRD risk.37–39
Prior studies have reported mixed findings regarding the relationship between MCC and cognitive status. Some have found similar MCC profiles across older adults with normal cognition, MCI, and ADRD;2,40 while others have observed greater chronic disease burden among those with cognitive impairment.41–45 Delivering effective care to patients with MCI or ADRD requires strategies that are tailored to cognitive abilities, address barriers to self-management, and actively engage care partners.46–48
This cross-sectional study examined the association between MCC profiles and undiagnosed MCI and ADRD in a diverse cohort of adults receiving primary care in Central Indiana and South Florida. We conducted neuropsychological assessments, electronic health record (EHR) reviews, and interdisciplinary clinical consensus for 324 primary care older adults without a documented diagnosis of MCI or ADRD. Based on our prior findings, we hypothesized that MCC profiles would be similar across cognitive groups. By characterizing the complexity and medication profiles of primary care patients with undetected cognitive impairment, this study aims to highlight opportunities to improve chronic disease management and prescribing practices among older adults in primary care.
Materials and Methods
Study Design and Population
We conducted a cross-sectional analysis of data collected between 2021 and 2023, as part of a larger study evaluating ADRD detection strategies in primary care. Patients were recruited from five Federally Qualified Health Centers (FQHC) affiliated with Eskenazi Health in Indianapolis, Indiana, and primary care practices affiliated with the University of Miami (UHealth) in South Florida.
Patients were eligible if they were 65 years or older, had an established primary care clinician at a participating clinic, had at least one visit within the past year, had a minimum of three years of EHRs available, and were able to provide verbal or written informed consent in English.
Patients were excluded if they had a documented diagnosis of ADRD or MCI in the EHR (identified via the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, ICD-10 codes), a history of cholinesterase inhibitor or memantine use, diagnosis of a serious mental illness (eg schizophrenia or bipolar disorder), or resided in a long-term care facility.
Data Collection and Measures
Demographic characteristics were collected through patient interviews and EHR review. Chronic conditions and prescription medications were manually extracted from the medical records.
Cognitive Status Assessment
Cognitive status was assessed using a comprehensive neuropsychological battery derived from the Uniform Data Set (UDS) 3.0 developed by the National Institute on Aging (NIA) Alzheimer’s Disease Centers.49 Global cognition was evaluated using the Montreal Cognitive Assessment (MoCA).50 Additional domains were assessed using the 15-item Multilingual Naming Test (MINT) for naming, category fluency (Animals) for verbal fluency, number span (forward and backward) for attention and working memory, Craft Story for episodic memory (immediate and delayed recall), and Trail Making Test Parts A and B for processing speed and executive attention. Mood was assessed using the Geriatric Depression Scale (GDS).
In addition, informant-based tools, including the Clinical Dementia Rating (CDR), Neuropsychiatric Inventory Questionnaire (NPI), and Functional Activities Questionnaire (FAQ), were used to evaluate cognitive, behavioral, and functional domains.
Cognitive diagnoses were made via interdisciplinary clinical consensus involving a neurologist, a geriatrician, and a neuropsychologist. This team reviewed the cognitive test results, clinical diagnoses, and medical records to categorize patients as having normal cognition, MCI, or ADRD.
Measurement of Multiple Chronic Conditions
MCC was measured using two approaches:
- Chronic conditions: We evaluated the presence of 15 common chronic conditions in older adults51–53 using clinician-coded ICD-10 diagnosis from the EHR. These conditions included ischemic heart disease, cerebrovascular disease, hyperlipidemia, diabetes, congestive heart failure, atrial fibrillation, hypertension, cancer, chronic obstructive pulmonary disease, liver disease, kidney disease, sleep apnea, insomnia, depression, and anxiety.
- Medication Use: We assessed prescription orders to quantify medication burden and exposure to medications with central anticholinergic activity and psychotropic medications, including anxiolytics, antidepressants, antipsychotics, stimulants, mood stabilizers, and sedative/hypnotics.
Statistical Analysis
Sample Size and Power Considerations
Because this was a secondary analysis of a diagnostic accuracy study, a priori sample size and power calculations were not performed. Post hoc sample considerations were based on recommended rules of thumb,54 using a conservative minimum of 10 events per variable (EPV) for the least prevalent outcome category (dementia). This approach minimized overfitting and ensured stable multinomial logistic regression estimates. Assuming a prevalence of 40% for MCI and 10% for dementia, and accounting for two covariates (continuous/dichotomous), simulations demonstrated that our sample size of 324 was adequate to detect moderate-to-large effect sizes (odds ratios 1.5–3.0) with at least 80% power (Supplemental Figure 1).
We used descriptive statistics (including proportions, means with standard deviations, and medians) to summarize participant demographic characteristics and MCC profiles across cognitive status groups (normal, MCI, and ADRD). Comparisons of patient demographic characteristics by cognitive status were conducted using Pearson’s chi-squared test, Fisher’s exact test, or Kruskal–Wallis test, as appropriate.
Multinomial logistic regression models were used to examine the relationship between patient demographic characteristics, chronic conditions, medication use and cognitive status. This approach was used to model cognitive status as an outcome variable with three nominal categories (normal cognition, MCI, or dementia), using normal cognition as the reference group. Pairwise interaction terms between patient characteristics (eg, age, sex) and chronic conditions or medications use (eg, diabetes, anticholinergic exposure) were tested to evaluate whether these characteristics moderated the relationship between cognitive status and chronic conditions/medication use.
To address model convergence issues arising from sparse data (ie, outcome and predictor categories with low counts of observations), we combined the MCI and dementia groups to create a dichotomous category: cognitive impairment versus no cognitive impairment. For this outcome, we used a binomial logistic regression model to examine whether the associations with chronic condition and medication use differed by patient demographic characteristics (eg, male vs female).
In the absence of statistically significant interaction terms, we present main effects models adjusted for age, sex, race/ethnicity, education level, and Area Deprivation Index (ADI) as potential confounders. None of the covariates were standardized, allowing regression coefficients to be interpreted in their original units.
All reported tests were 2-sided, and P <.05 was considered statistically significant. Data were analyzed using R statistical software version 4.3.0 (R Project for Statistical Computing).
Results
A total of 324 patients from both sites had complete data for analysis. The mean age was 71 years (SD = 5), and 60.5% reported their gender as female. The mean educational level was 14 years (SD = 3). The cohort was racially diverse: 53.1% identified as White non-Hispanic, 34.6% as Black non-Hispanic, 8.6% as White Hispanic, 0.6% as Black Hispanic, and 3% as other (Table 1).
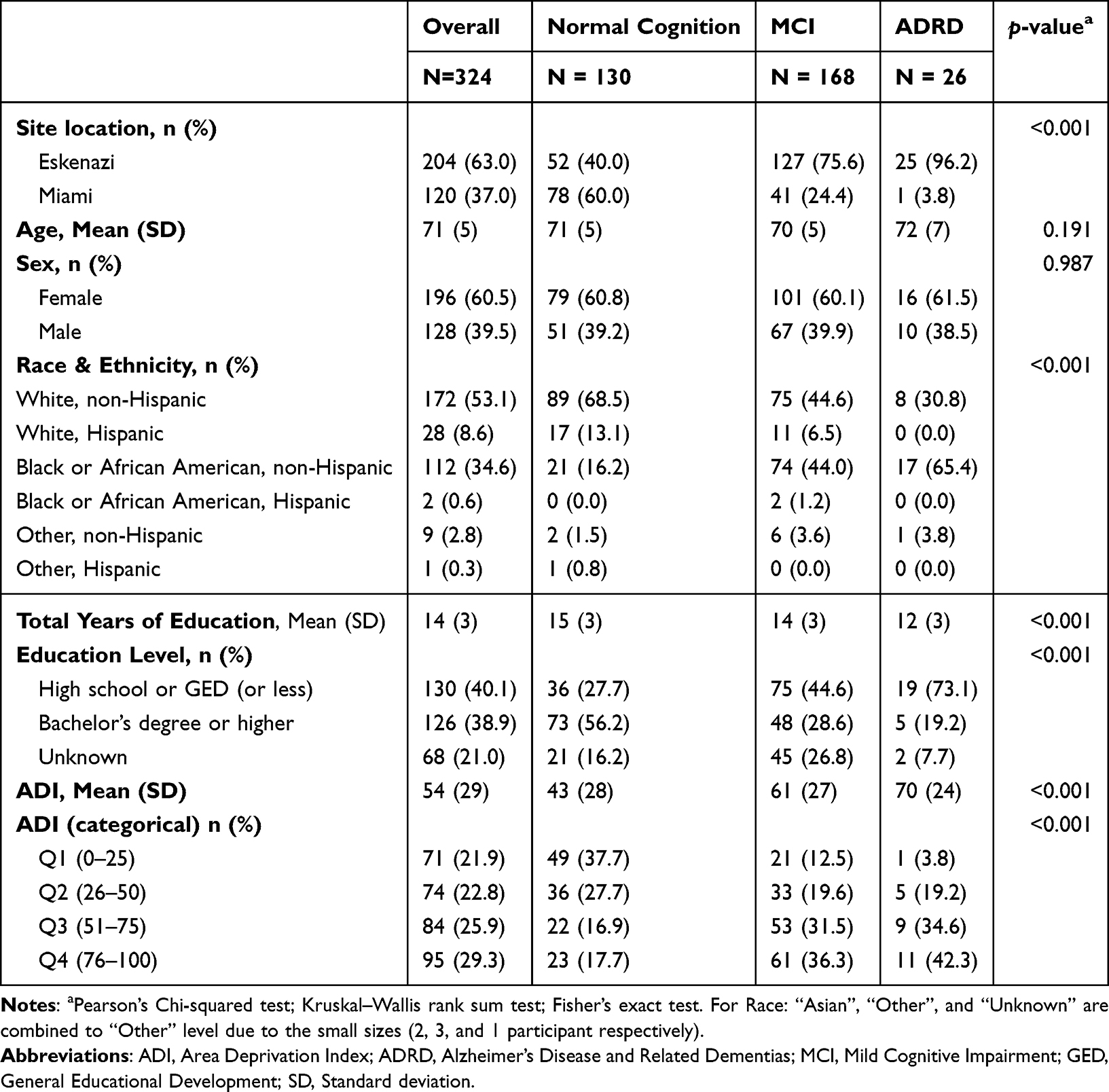 |
Table 1 Demographic Characteristics of the Study Cohort |
Most patients (59.9%, n =194) had previously undetected cognitive impairment: 51.9% (n = 168) were determined to have MCI, and 8% (n = 26) ADRD. This distribution varied by site, as most patients with MCI (n = 168) were from Indiana (75.6%, n = 127) compared with 24.4% (n = 41) from Florida. Among those with MCI, 44.6% were White non-Hispanics, and their average ADI was 61 (SD = 27). Among the patients with ADRD (n = 26), 96.2% (n = 25) were from Indiana, 3.8% (n = 1) from Florida, 65.4% were Black non-Hispanic (n = 17), and their average ADI was 70 (SD = 24).
Chronic Conditions and Medication Use
Table 2 summarizes the distribution of chronic conditions and medication use by cognitive group. Overall, patients had a mean of five chronic conditions (SD = 2), with higher counts among those with ADRD (mean = 6, SD = 2) and MCI (mean = 5, SD = 2) than among those without cognitive impairment (mean 4, SD = 2; p <0.001).
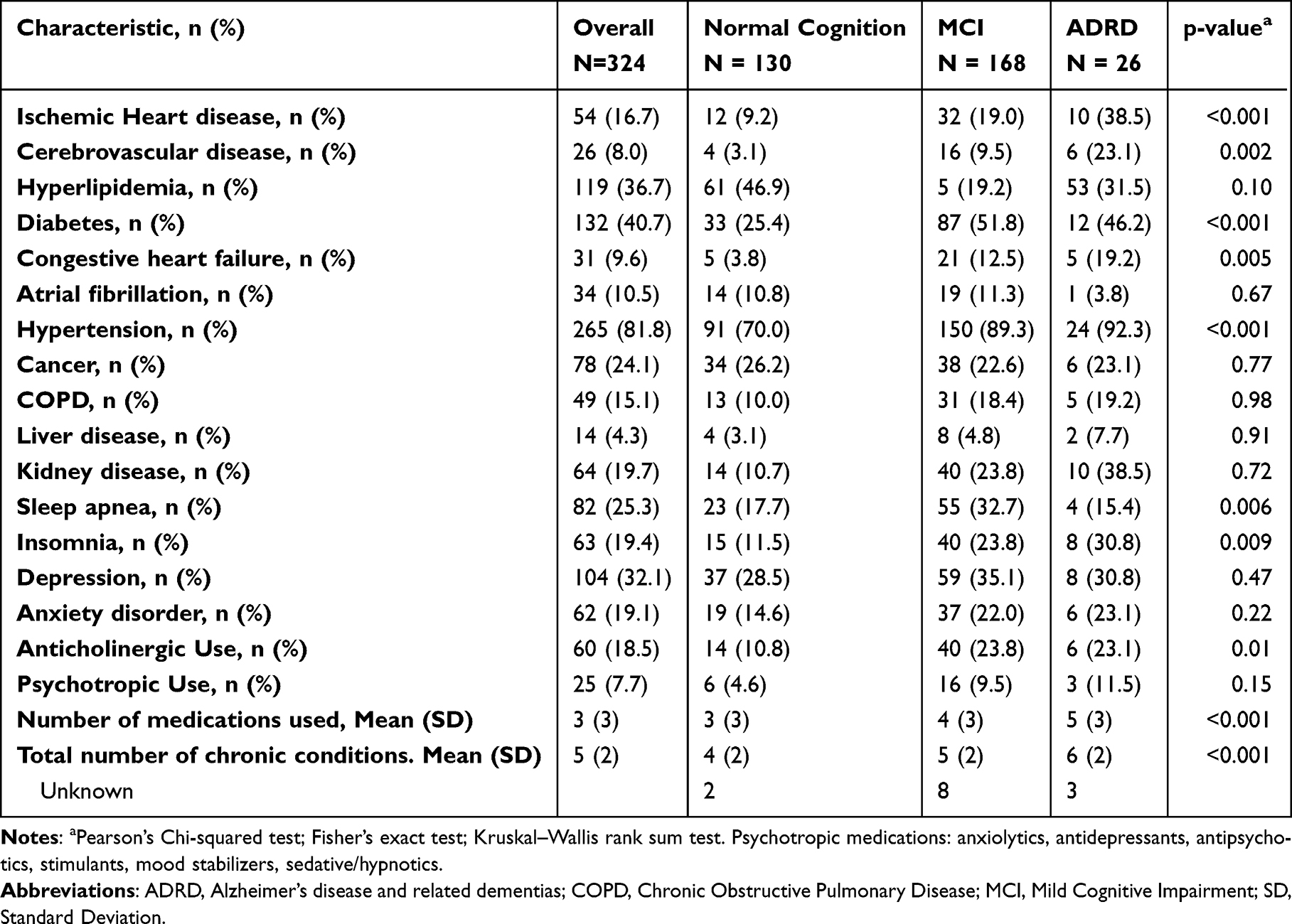 |
Table 2 Distribution of Chronic Conditions (Comorbidity Profile) and Medications Across Cognitive States |
The mean number of medications prescribed was 3 (SD = 3). Patients with ADRD (mean = 5, SD = 3) and MCI (mean = 4, SD = 3), received more prescriptions than those with normal cognition (mean = 3, SD = 3; p <0.001). Among patients with at least one prescription, 18.5% (n = 60) were prescribed at least one anticholinergic medication. Anticholinergic use was more common among patients in the MCI (23.8%, n = 40) and ADRD groups (23.1%, n = 6) than among those with normal cognition (10.8%, n =14; p = 0.01). Psychotropic medication use was observed in 7.7% of all patients and did not differ significantly by cognitive status (normal: 4.6%, MCI: 9.5%, ADRD: 11.5%, p = 0.155).
Multivariable Associations with Cognitive Status
We used multinomial logistic regression, adjusting for patient age, sex, race/ethnicity, education level, and ADI, to assess the association between chronic conditions, medication use, and cognitive status (reference group: normal cognition; Table 3).
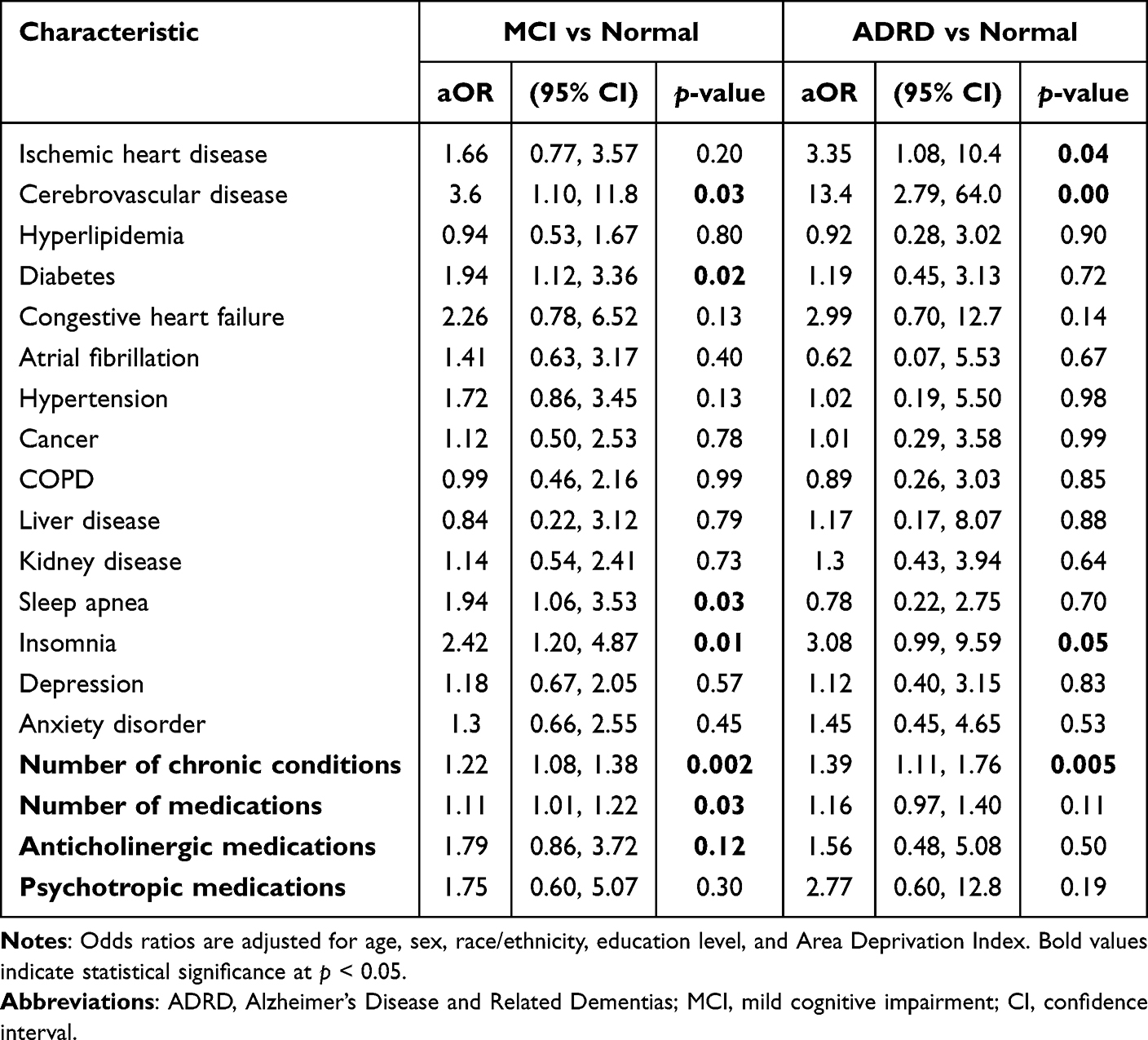 |
Table 3 Adjusted Odds Ratios from Multinomial Logistic Regression Models Examining the Association Between Chronic Conditions, Medication Use, and Cognitive Status (MCI and ADRD vs Normal Cognition) |
Patients with MCI and ADRD had higher odds of having more chronic conditions than those with normal cognition (MCI: aOR = 1.22; 95% CI: 1.08–1.38; ADRD: aOR = 1.39; 95% CI: 1.11–1.76). Cerebrovascular disease was associated with both MCI and ADRD (MCI: aOR = 3.6; 95% CI: 1.10–11.8; ADRD: aOR = 13.4; 95% CI: 2.79–64.0). Ischemic heart disease was associated with ADRD alone (aOR = 3.35; 95% CI: 1.08–10.4). Insomnia, diabetes, and sleep apnea were associated with MCI, while insomnia was associated with both MCI and ADRD.
Medication-Specific Findings
The number of medications was associated with higher odds of MCI (aOR = 1.11; 95% CI: 1.00–1.21), but not with ADRD (OR: 1.13; 95% CI: 0.95–1.35). In medication class-specific analyses, a statistically significant interaction between age and anticholinergic use (p = 0.048) suggested that age moderated the association between anticholinergic use and cognitive status. As shown in Figure 1, the predicted anticholinergic use decreased with age among patients with cognitive impairment but increased with age among those without impairment.
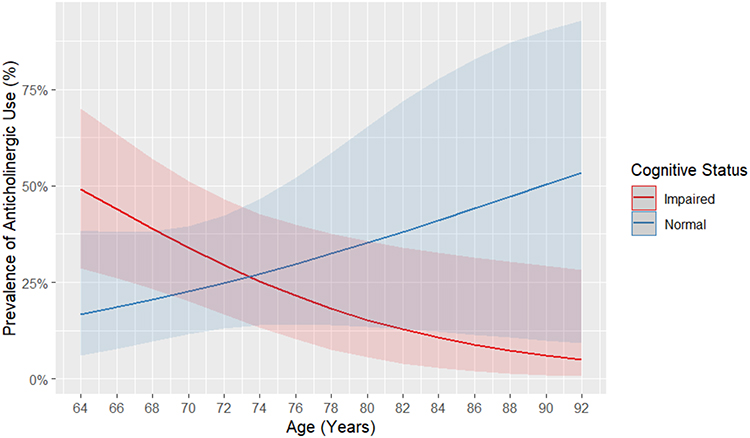 |
Figure 1 Predicted prevalence of anticholinergic medication use by age and cognitive impairment. |
Discussion
In this cross-sectional study of older primary care patients from two primary care networks in the US, patients who met the clinical criteria for MCI or ADRD had a higher burden of MCC than those with normal cognition. Among these chronic conditions, cerebrovascular disease was significantly more prevalent in patients with MCI and ADRD, consistent with prior research linking vascular pathology to cognitive decline.55–57 These findings contribute to the body of evidence that vascular risk factors play a central role in cognitive impairment and highlight the importance of cardiovascular prevention strategies in primary care.58–70
While the association between cognitive impairment and MCC is well established,41,55,56,71–73 our study contributes to the literature by focusing on undiagnosed cases of MCI and ADRD. The high prevalence of cognitive impairment in our sample may reflect the use of proactive cognitive assessments, and possibly greater underrecognized risk in underserved populations.
In addition, patients with MCI and ADRD had a higher medication burden, which in turn increases the complexity of chronic disease self-management and the risk of administration errors, drug interactions, and prescribing cascades. These medication-related risks are known to contribute to increased caregiver burden and poorer health outcomes, including hospitalization and functional decline.2,33–35,74,75
Despite well-documented associations with cognitive decline, anticholinergic medications were frequently prescribed in patients with MCI (23.8%) and ADRD (23.1%). Notably, younger individuals with cognitive impairment had higher odds of anticholinergic use, suggesting potential targets for intervention. This persistent exposure highlights the need for deprescribing interventions in primary care that prioritize medication safety and cognitive preservation.37,76,77
These findings reinforce the critical role of primary care clinicians in managing MCC in older adults with ADRD.78 Closing persistent gaps in ADRD care will require targeted, systematic interventions that support clinicians, patients, and care partners in managing MCC. Potential interventions include (1) conducting cognitive assessments to evaluate self-management capacity among patients with MCC, (2) simplifying medication regimens and adjusting treatment targets based on cognitive status and goals of care, and (3) engaging care partners earlier and consistently in developing chronic disease management plans. Together, these strategies provide a foundation for safe and more individualized primary care models that may improve outcomes for older adults.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, its cross-sectional design limits inferences about the temporal relationship between the onset of cognitive impairment and development of MCCs. It is unclear whether MCCs preceded cognitive changes or whether they emerged consequently. Second, although we adjusted for key demographic and socioeconomic factors, residual confounding is possible. Important variables, such as smoking, alcohol use, physical inactivity, obesity, and sensory impairment, may influence both cognitive status and MCC burden. Third, although we assessed the presence of MCC, we did not capture the severity and degree of clinical control, which may differ across cognitive groups. Finally, while our findings support routine cognitive screening and integrated care approaches in primary care, further implementation studies are needed to evaluate the feasibility, sustainability, and impact of these interventions in real-world primary care settings.
Conclusion
Older adults with unrecognized ADRD experience a high burden of MCC and medication exposure, including anticholinergic medications. These findings highlight the role of primary care clinicians in identifying cognitive impairment, modifying risk factors, and optimizing management of MCC. Targeted interventions, such as routine cognitive assessments, MCC prevention, simplified treatment regimens, and early engagement of care partners, may reduce medication-related risks and improve care for older adults with cognitive impairment.
Abbreviations
ADI, Area Deprivation Index; ADRD, Alzheimer’s Disease and Other Related Dementias; CDR, Clinical Dementia Rating; EHR, Electronic Health Records; FAQ, Functional Activity Questionnaire; FQHC, Federally Qualified Health Center; GDS, Geriatric Depression Scale; ICD-10, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision; MCC, Multiple Chronic Conditions; MCI, Mild Cognitive Impairment; MoCA, Montreal Cognitive Assessment; NIA, National Institute on Aging; NPI, Neuropsychiatric Inventory Questionnaire.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical standards outlined in the Declaration of Helsinki and followed all applicable institutional guidelines for research involving human participants. Ethical approval for all study procedures was obtained from the Institutional Review Board of Indiana University (number: 2008372812). Clinical trial registration was completed under the ClinicalTrials.gov identifiers: NCT06224205 and NCT05231954.
Written informed consent was obtained from all participants before enrollment. Participants were assured of the confidentiality and voluntary nature of their participation.
Author Contributions
All authors made substantial contributions to the work reported, including the conception, study design, execution, acquisition of data, and/or analysis and interpretation. All authors participated in drafting, revising, or critically reviewing the manuscript; approved the final version for publication; agreed on the journal to which the article was submitted; and accept responsibility for all aspects of the work.
Funding
This research was sponsored by the National Institute on Aging under grant number R01AG069765. The sponsor had no role in the design or conduct of the study, collection, management, analysis, or interpretation of the data, or the decision to submit the manuscript for publication.
Disclosure
Dr. Boustani serves as a chief Scientific Officer and co-Founder of BlueAgilis and the Chief Health Officer of Mozyne health, inc. He has equity interest in Blue Agilis, Inc and Mozyne Health, Inc. He sold his equity in Preferred Population Health Management LLC; and MyShift, Inc (previously known as RestUp, LLC). He used to be the Chief Health Officer of Digicare Realized. This company was folded early this year with no financial benefits gained by Dr. Boustani. He serves as an advisory board member or consultant for Eli Lilly and Co; Eisai, Inc; Merck & Co Inc; Biogen Inc; Genentech Inc, and NeuroX, Inc. These conflicts have been reviewed by Indiana University and has been appropriately managed to maintain objectivity.
Dr. Galvin is the creator of the Quick Dementia Rating System, for which the copyright is held by New York University. Dr. Galvin is supported by grants from the National Institutes of Health (NIH) and serves as a consultant for Beckman-Coulter, Biogen, Bristol Myers Squibb (BMS), Eisai, Eli Lilly, GE Healthcare, Lobe, and Roche. He is the Chief Scientific Officer for Cognivue, Inc., and is an investigator in clinical trials sponsored by Cognition Therapeutics, CervoMed, and CND Life Sciences. Dr. Galvin also serves on the Board of Directors for the South Florida Chapter of the Alzheimer’s Association.
The rest of the authors have no conflicts of interest to declare.
References
1. Kulshreshtha A, Parker ES, Fowler NR, et al. Prevalence of unrecognized cognitive impairment in federally qualified health centers. JAMA Network Open. 2024;7(10):e2440411. doi:10.1001/jamanetworkopen.2024.40411
2. Schubert CC, Boustani M, Callahan CM, et al. Comorbidity profile of dementia patients in primary care: are they sicker? J Am Geriatr Soc. 2006;54(1):104–109. doi:10.1111/j.1532-5415.2005.00543.x
3. Bierman AS, Wang J, O’Malley PG, Moss DK. Transforming care for people with multiple chronic conditions: agency for healthcare research and quality’s research agenda. Health Serv Res. 2021;56(Suppl 1):973–979. doi:10.1111/1475-6773.13863
4. Salive ME. Multimorbidity in older adults. Epidemiol Rev. 2013;35:75–83. doi:10.1093/epirev/mxs009
5. Alzheimer’s Association., 2024 Alzheimer’s disease facts and figures. Alzheimers Dement. 2024;20(5):3708–3821. doi:10.1002/alz.13809
6. Alzheimer’s Association., 2025 Alzheimer’s disease facts and figures. Alzheimers Dement. 2025;21(4):e70235. doi:10.1002/alz.70235
7. Ashford JW, Borson S, O’Hara R, et al. Should older adults be screened for dementia? It is important to screen for evidence of dementia! Alzheimers Dement. 2007;3(2):75–80. doi:10.1016/j.jalz.2007.03.005
8. National Academies of Sciences, Engineering, and Medicine. Preventing and Treating Alzheimer’s Disease and Related Dementias: Promising Research and Opportunities to Accelerate Progress: Proceedings of a Workshop–in Brief. The National Academies Press; 2024:13.
9. U.S. Department of Health and Human Services. National plan to address Alzheimer’s disease. Assistant Secretary for Planning and Evaluation (ASPE); [updated 2024]. Available from: https://aspe.hhs.gov/collaborations-committees-advisory-groups/napa/napa-documents/napa-national-plan.
10. Cordell CB, Borson S, Boustani M, et al. Alzheimer’s association recommendations for operationalizing the detection of cognitive impairment during the medicare annual wellness visit in a primary care setting. Alzheimers Dement. 2013;9(2):141–150. doi:10.1016/j.jalz.2012.09.011
11. Mattke S, Batie D, Chodosh J, et al. Expanding the use of brief cognitive assessments to detect suspected early-stage cognitive impairment in primary care. Alzheimers Dement. 2023;19(9):4252–4259. doi:10.1002/alz.13051
12. Harris DP, Chodosh J, Vassar SD, Vickrey BG, Shapiro MF. Primary care providers’ views of challenges and rewards of dementia care relative to other conditions. J Am Geriatr Soc. 2009;57(12):2209–2216. doi:10.1111/j.1532-5415.2009.02572.x
13. Hinton L, Franz CE, Reddy G, Flores Y, Kravitz RL, Barker JC. Practice constraints, behavioral problems, and dementia care: primary care physicians’ perspectives. J Gen Intern Med. 2007;22(11):1487–1492. doi:10.1007/s11606-007-0317-y
14. Mansfield E, Noble N, Sanson-Fisher R, Mazza D, Bryant J. Primary care physicians’ perceived barriers to optimal dementia care: a systematic review. Gerontologist. 2018;59(6):e697–e708. doi:10.1093/geront/gny067
15. Sabbagh MN, Boada M, Borson S, et al. Early detection of Mild Cognitive Impairment (MCI) in primary care. J Prev Alzheimers Dis. 2020;7(3):165–170. doi:10.14283/jpad.2020.21
16. Lang L, Clifford A, Wei L, et al. Prevalence and determinants of undetected dementia in the community: a systematic literature review and a meta-analysis. BMJ Open. 2017;7(2):e011146. doi:10.1136/bmjopen-2016-011146
17. Chin AL, Negash S, Hamilton R. Diversity and disparity in dementia: the impact of ethnoracial differences in Alzheimer disease. Alzheimer Dis Assoc Disord. 2011;25(3):187–195. doi:10.1097/WAD.0b013e318211c6c9
18. Gianattasio KZ, Prather C, Glymour MM, Ciarleglio A, Power MC. Racial disparities and temporal trends in dementia misdiagnosis risk in the United States. Alzheimers Dement. 2019;5(1):891–898. doi:10.1016/j.trci.2019.11.008
19. Cockerham WC, Hamby BW, Oates GR. The social determinants of chronic disease. Am J Prev Med. 2017;52(Supplement 1):S5–S12. doi:10.1016/j.amepre.2016.09.010
20. Shadmi E. Disparities in multiple chronic conditions within populations. J Comorb. 2013;3(2):45–50. doi:10.15256/joc.2013.3.24
21. Callahan CM, Boustani MA, Weiner M, et al. Implementing dementia care models in primary care settings: the aging brain care medical home. Aging Mental Health. 2011;15(1):5–12. doi:10.1080/13607861003801052
22. Brosch JR, Summanwar D, Fowler NR, et al. An innovative health systems approach to support early detection of cognitive impairment in primary care – the brain health navigator. BMC Prim Care. 2025;26(1):271. doi:10.1186/s12875-025-02977-w
23. Centers for Medicare & Medicaid Services. GUIDE model: guiding an improved dementia experience – fact sheet. 2023.
24. National Institute for Health and Care Research. Multiple long-term conditions – making sense of the evidence. Available from: https://www.nihr.ac.uk/blog/multiple-long-term-conditions-making-sense-evidence.
25. Calderón-Larrañaga A, Poblador-Plou B, González-Rubio F, Gimeno-Feliu LA, Abad-Díez JM, Prados-Torres A. Multimorbidity, polypharmacy, referrals, and adverse drug events: are we doing things well? Br J Gen Pract. 2012;62(605):e821–e826. doi:10.3399/bjgp12X659295
26. Tinetti ME, Bogardus ST, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med. 2004;351(27):2870–2874. doi:10.1056/NEJMsb042458
27. Liew TM, Lee CS, Goh SKL, Chang ZY. The prevalence and impact of potentially inappropriate prescribing among older persons in primary care settings: multilevel meta-analysis. Age Ageing. 2020;49(4):570–579. doi:10.1093/ageing/afaa057
28. Jungo KT, Streit S, Lauffenburger JC. Utilization and spending on potentially inappropriate medications by US older adults with multiple chronic conditions using multiple medications. Arch Gerontol Geriatrics. 2021;93:104326. doi:10.1016/j.archger.2020.104326
29. Huang Y, Zhang L, Huang X, Liu K, Yu Y, Xiao J. Potentially inappropriate medications in Chinese community-dwelling older adults. Int J Clin Pharm. 2020;42(2):598–603. doi:10.1007/s11096-020-00980-y
30. Pan S, Li S, Jiang S, et al. Trends in number and appropriateness of prescription medication utilization among community-dwelling older adults in the United States: 2011–2020. J Gerontol Ser A. 2024;79(7):glae108. doi:10.1093/gerona/glae108
31. Gagnon M-E, Sirois C, Simard M, Roux B, Plante C. Potentially inappropriate medications in older individuals with diabetes: a population-based study in Quebec, Canada. Prim Care Diabetes. 2020;14(5):529–537.
32. Bazargan M, Smith JL, King EO. Potentially inappropriate medication use among hypertensive older African-American adults. BMC Geriatr. 2018;18(1):238. doi:10.1186/s12877-018-0926-9
33. Dijkstra NE, Sino CGM, Schuurmans MJ, Schoonhoven L, Heerdink ER. Medication self-management: considerations and decisions by older people living at home. Res Social Adm Pharm. 2022;18(3):2410–2423. doi:10.1016/j.sapharm.2020.09.004
34. Growdon ME, Jing B, Yaffe K, et al. High-risk medication use among older adults with cognitive impairment living alone in the United States. J Am Geriatr Soc. 2024;72(12):3719–3729. doi:10.1111/jgs.19108
35. Powell C, Tomlinson J, Quinn C, Fylan B. Interventions for self-management of medicines for community-dwelling people with dementia and mild cognitive impairment and their family carers: a systematic review. Age Ageing. 2022;51(5):afac089. doi:10.1093/ageing/afac089
36. Zhao M, Chen Z, Xu T, Fan P, Tian F. Global prevalence of polypharmacy and potentially inappropriate medication in older patients with dementia: a systematic review and meta-analysis. Front Pharmacol. 2023;14:1221069. doi:10.3389/fphar.2023.1221069
37. Zheng YB, Shi L, Zhu XM, et al. Anticholinergic drugs and the risk of dementia: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2021;127:296–306. doi:10.1016/j.neubiorev.2021.04.031
38. Richardson K, Fox C, Maidment I, et al. Anticholinergic drugs and risk of dementia: case-control study. BMJ. 2018;361:k1315. doi:10.1136/bmj.k1315
39. Tan ECK, Eriksdotter M, Garcia-Ptacek S, Fastbom J, Johnell K. Anticholinergic burden and risk of stroke and death in people with different types of dementia. J Alzheimers Dis. 2018;65(2):589–596. doi:10.3233/jad-180353
40. Zekry D, Herrmann FR, Grandjean R, et al. Demented versus non-demented very old inpatients: the same comorbidities but poorer functional and nutritional status. Age Ageing. 2007;37(1):83–89. doi:10.1093/ageing/afm132
41. Bunn F, Burn A-M, Goodman C, et al. Comorbidity and dementia: a scoping review of the literature. BMC Med. 2014;12(1):192. doi:10.1186/s12916-014-0192-4
42. Poblador-Plou B, Calderón-Larrañaga A, Marta-Moreno J, et al. Comorbidity of dementia: a cross-sectional study of primary care older patients. BMC Psychiatry. 2014;14:84. doi:10.1186/1471-244x-14-84
43. Bauer K, Schwarzkopf L, Graessel E, Holle R. A claims data-based comparison of comorbidity in individuals with and without dementia. BMC Geriatr. 2014;14:10. doi:10.1186/1471-2318-14-10
44. Doraiswamy PM, Leon J, Cummings JL, Marin D, Neumann PJ. Prevalence and impact of medical comorbidity in Alzheimer’s disease. J Gerontol Ser A. 2002;57(3):M173–M177. doi:10.1093/gerona/57.3.M173
45. Clague F, Mercer SW, McLean G, Reynish E, Guthrie B. Comorbidity and polypharmacy in people with dementia: insights from a large, population-based cross-sectional analysis of primary care data. Age Ageing. 2017;46(1):33–39. doi:10.1093/ageing/afw176
46. Baird C, Woolford MH, Young C, Winbolt M, Ibrahim J. Chronic disease management and dementia: a qualitative study of knowledge and needs of staff. Aust J Prim Health. 2019;25(4):359–365. doi:10.1071/PY18197
47. Ibrahim JE, Anderson LJ, MacPhail A, Lovell JJ, Davis MC, Winbolt M. Chronic disease self-management support for persons with dementia, in a clinical setting. J Multidiscip Healthc. 2017;10:49–58. doi:10.2147/jmdh.S121626
48. Jhang KM, Wang WF, Cheng YC, Tung YC, Yen SW, Wu HH. Care need combinations for dementia patients with multiple chronic diseases. Psychol Res Behav Manag. 2023;16:179–195. doi:10.2147/prbm.S388394
49. Weintraub S, Besser L, Dodge HH, et al. Version 3 of the Alzheimer disease centers’ neuropsychological test battery in the Uniform Data Set (UDS). Alzheimer Dis Assoc Disord. 2018;32(1):10–17. doi:10.1097/wad.0000000000000223
50. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
51. Boersma P, Black LI, Ward BW. Prevalence of multiple chronic conditions among US adults, 2018. Prev Chronic Dis. 2020;17:E106.
52. Erdem E. Prevalence of chronic conditions among medicare part A beneficiaries in 2008 and 2010: are medicare beneficiaries getting sicker? Prev Chronic Dis. 2014;11:E10. doi:10.5888/pcd11.130118
53. Lochner K. Prevalence of multiple chronic conditions among medicare beneficiaries, United States, 2010. Prev Chronic Dis. 2013;10:E61. doi:10.5888/pcd10.120137
54. Pate A, Riley RD, Collins GS, et al. Minimum sample size for developing a multivariable prediction model using multinomial logistic regression. Stat Methods Med Res. 2023;32(3):555–571. doi:10.1177/09622802231151220
55. Vassilaki M, Aakre JA, Cha RH, et al. Multimorbidity and risk of mild cognitive impairment. J Am Geriatr Soc. 2015;63(9):1783–1790. doi:10.1111/jgs.13612
56. Wei MY, Levine DA, Zahodne LB, Kabeto MU, Langa KM. Multimorbidity and cognitive decline over 14 years in older Americans. J Gerontol Ser A. 2019;75(6):1206–1213. doi:10.1093/gerona/glz147
57. Kalaria RN. Cerebrovascular disease and mechanisms of cognitive impairment. Stroke. 2012;43(9):2526–2534. doi:10.1161/STROKEAHA.112.655803
58. Stefanidis KB, Askew CD, Greaves K, Summers MJ. The effect of non-stroke cardiovascular disease states on risk for cognitive decline and dementia: a systematic and meta-analytic review. Neuropsychol Rev. 2018;28(1):1–15. doi:10.1007/s11065-017-9359-z
59. Clair L, Anderson H, Anderson C, Ekuma O, Prior HJ. Cardiovascular disease and the risk of dementia: a survival analysis using administrative data from Manitoba. Can J Public Health. 2022;113(3):455–464. doi:10.17269/s41997-021-00589-2
60. Wolters FJ, Segufa RA, Darweesh SKL, et al. Coronary heart disease, heart failure, and the risk of dementia: a systematic review and meta-analysis. Alzheimers Dement. 2018;14(11):1493–1504. doi:10.1016/j.jalz.2018.01.007
61. Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957–967. doi:10.1016/s0140-6736(15)01225-8
62. Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364(9435):685–696. doi:10.1016/s0140-6736(04)16895-5
63. Kitagawa K. Blood pressure management for secondary stroke prevention. Hypertens Res. 2022;45(6):936–943. doi:10.1038/s41440-022-00908-1
64. Alloubani A, Nimer R, Samara R. Relationship between hyperlipidemia, cardiovascular disease and stroke: a systematic review. Curr Cardiol Rev. 2021;17(6):52–66. doi:10.2174/1573403X16999201210200342
65. Owolabi MO, Thrift AG, Mahal A, et al. Primary stroke prevention worldwide: translating evidence into action. Lancet Public Health. 2022;7(1):e74–e85. doi:10.1016/S2468-2667(21)00230-9
66. Hewitt J, Castilla Guerra L, Fernández-Moreno MDC, Sierra C. Diabetes and stroke prevention: a review. Stroke Res Treat. 2012;2012(1):673187. doi:10.1155/2012/673187
67. Zhang J, Chen C, Hua S, et al. An updated meta-analysis of cohort studies: diabetes and risk of Alzheimer’s disease. Diabet Res Clin Pract. 2017;124:41–47. doi:10.1016/j.diabres.2016.10.024
68. Sáiz-Vazquez O, Puente-Martínez A, Pacheco-Bonrostro J, Ubillos-Landa S. Blood pressure and Alzheimer’s disease: a review of meta-analysis. Front Neurol. 2022;13:1065335. doi:10.3389/fneur.2022.1065335
69. Summanwar D, Kim H, Wei J, Boustani M, Alonso A, Kulshreshtha A. Association of cardiovascular disease with dementia: a longitudinal analysis using National Alzheimer’s Coordinating Center data. J Alzheimers Dis Reports. 2025;9:25424823251370646. doi:10.1177/25424823251370646
70. Livingston G, Huntley J, Liu KY, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet. 2024;404(10452):572–628. doi:10.1016/S0140-6736(24)01296-0
71. Chen H, Zhou Y, Huang L, Xu X, Yuan C. Multimorbidity burden and developmental trajectory in relation to later-life dementia: a prospective study. Alzheimers Dement. 2023;19(5):2024–2033. doi:10.1002/alz.12840
72. Hu H-Y, Zhang Y-R, Aerqin Q, et al. Association between multimorbidity status and incident dementia: a prospective cohort study of 245,483 participants. Transl Psychiatry. 2022;12(1):505. doi:10.1038/s41398-022-02268-3
73. Valletta M, Vetrano DL, Xia X, et al. Multimorbidity patterns and 18-year transitions from normal cognition to dementia and death: a population-based study. J Internal Med. 2023;294(3):326–335. doi:10.1111/joim.13683
74. Previdoli G, Cheong VL, Alldred D, et al. A rapid review of interventions to improve medicine self-management for older people living at home. Health Expect. 2023;26(3):945–988. doi:10.1111/hex.13729
75. Fowler NR, Perkins AJ, Park S, et al. Relationship between health-related quality of life, depression, and anxiety in older primary care patients and their family members. Aging Mental Health. 2024;28(6):910–916. doi:10.1080/13607863.2023.2285499
76. Bostock CV, Soiza RL, Mangoni AA. Association between prescribing of antimuscarinic drugs and antimuscarinic adverse effects in older people. Expert Rev Clin Pharmacol. 2010;3(4):441–452. doi:10.1586/ecp.10.34
77. Carollo M, Crisafulli S, Vitturi G, et al. Clinical impact of medication review and deprescribing in older inpatients: a systematic review and meta-analysis. J Am Geriatr Soc. 2024;72(10):3219–3238. doi:10.1111/jgs.19035
78. Ma D, Wang Y, Zhao Y, et al. How to manage comorbidities in people with dementia: a scoping review. Ageing Res Rev. 2023;88:101937. doi:10.1016/j.arr.2023.101937
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Feasibility of Deriving the Electronic Frailty Index from Australian General Practice Records
Lewis ET, Williamson M, Lewis LP, Ní Chróinín D, Dent E, Ticehurst M, Peters R, Macniven R, Cardona M
Clinical Interventions in Aging 2022, 17:1589-1598
Published Date: 3 November 2022
Current Understanding of Verbal Fluency in Alzheimer’s Disease: Evidence to Date
Wright LM, De Marco M, Venneri A
Psychology Research and Behavior Management 2023, 16:1691-1705
Published Date: 5 May 2023
Interaction Between Multimorbidity and Hip Fracture Surgery Leads to Excess Risk of Infection: A Danish Registry-Based Cohort Study of 92,599 Patients With Hip Fracture
Hansen CM, Gadgaard NR, Vandenbroucke-Grauls C, Hailer NP, Pedersen AB
Clinical Epidemiology 2025, 17:167-176
Published Date: 24 February 2025
Anticholinergic Burden and Its Association with Hospitalisation Risk and Causes of Admission in Older Adults with Mild Cognitive Impairment or Dementia
Rahoo R, Liau ZY, Low MJ, Kamaruzzaman SB, Francis B, Khor HM
Clinical Interventions in Aging 2025, 20:1661-1670
Published Date: 25 September 2025