Back to Journals » Nature and Science of Sleep » Volume 17

Chin Tuck Exercise and Obstructive Sleep Apnea: A Case Report
Authors Alsaeed S ![]()
Received 12 July 2025
Accepted for publication 13 September 2025
Published 29 September 2025 Volume 2025:17 Pages 2343—2349
DOI https://doi.org/10.2147/NSS.S552879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Supplementary video of “Chin Tuck Exercise and Obstructive Sleep Apnea” [552879]
Views: 195
Suliman Alsaeed1– 3
1Preventive Dental Sciences Department, College of Dentistry, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3Health Affairs, Ministry of the National Guard, Riyadh, Saudi Arabia
Correspondence: Suliman Alsaeed, Email [email protected]
Abstract: This case report describes a patient with neck pain who was recommended by his gym coach to perform chin tuck exercises to manage his pain. After a period of 3 weeks of daily chin tuck exercise, each session consisting of 10 repetitions of a 20-second hold, performed three times per day, the patient started to experience symptoms of snoring, witnessed gasping, morning headache, and excessive daytime sleepiness. Polysomnography performed by a sleep physician confirmed the diagnosis of mild obstructive sleep apnea with an apnea-hypopnea index of 10 times/h and a significant desaturation of oxygen of 86% (BMI: 24 kg/m²). The patient was recommended to discontinue the exercise. His obstructive sleep apnea symptoms disappeared in 2 weeks, and follow-up polysomnography was conducted, which confirmed the complete resolution of obstructive sleep apnea with improved sleep parameters. To our knowledge, this is the first case report linking chin tuck exercise to the onset of obstructive sleep apnea, emphasizing the need for clinicians, physiotherapists, and fitness coaches to be aware of this potential risk.
Keywords: obstructive sleep apnea, chin tuck exercise, sleep disorder, case report
Introduction
Obstructive sleep apnea (OSA) is the most common sleep disordered breathing.1 It affects 14% of men and 5% of women and rises with increasing age.2 It is characterized by the recurrent closure of the upper airway, resulting in oxygen desaturation and sympathetic activation. The main risk factor of OSA in adults is obesity.1 However, there are neuromuscular factors that contribute to the severity of OSA.3 Most studies have focused on anatomical factors and overlooked the effects of non-anatomical factors, such as poor responsiveness of the pharyngeal dilator muscles.3
Contractibility of the pharyngeal dilator muscles has an important role during sleep. Impaired muscle activity can result in airway obstruction and subsequent reduction in inspiratory flow.4 This is mostly associated with elderly patients or patients with upper airway myopathy.5 In such cases, the airway collapses at a low pharyngeal cortical closing pressure as a result of impaired neuromuscular tone.
The chin tuck exercise is a physical therapy movement designed to strengthen specific neck and throat muscles. It is most commonly used in two main contexts: (1) rehabilitation for swallowing difficulties (dysphagia), and (2) management of neck pain and postural correction especially patients with forward head posture (FHP).6 Multiple studies have found that chin tuck exercises can be used to protect the airway from subglottic aspiration from premature food spillage, as they push the anterior pharyngeal wall backward.7,8 This results in narrowing of the upper airway entrance for airway protection, decrease in resting state distance from hyoid bone to mandible, and retraction of the tongue base.7,9
Several studies have indicated the effect of neck exercise programs—including isometric, stretching, range of motion, motor control, and strengthening exercises—on the strength of neck muscles, endurance and function, while reducing pain and disability in different samples including nursing students, office workers, and military pilots.10–13 Biomechanically, these exercises work on the deep cervical flexor muscles, which are important for postural adjustment and dynamic stabilization of the cervical spine; failure of this leads to overuse of superficial muscles which leads to increased pain and dysfunction, due to altered load distribution.11,14–16
This case report aims to highlight a potential association between chin tuck exercises and the development of obstructive sleep apnea (OSA), emphasizing the importance of recognizing exercise-related factors in the onset and resolution of sleep-disordered breathing symptoms.
Case Report
Patient Information
A 39-year-old male patient was referred by his sleep physician to the orthodontic clinic for consultation regarding the possible use of a mandibular advancement device (MAD) for the management of OSA. The patient reported no significant past medical history, with no known cardiovascular, metabolic, or neurological conditions. Family history was unremarkable, and no relatives were diagnosed with obstructive sleep apnea or other sleep disorders. He was a non-smoker, and reported no history of alcohol, sedative or muscle relaxant use.
Clinical Findings
The patient presented with symptoms of snoring, witnessed gasping, excessive daytime sleepiness, and morning headache. On physical examination, his body mass index (BMI) was 24 kg/m², and his Mallampati score was class II. Orthodontic examination was performed, which showed a convex profile, short chin-throat length with an obtuse chin-throat angle. He had a class I molar relationship, class II canine relationship on the left side with lower midline shift of 2 mm to the left side, and a moderate lower crowding (Figure 1). He had no posterior crossbite or mouth breathing habit. His oral hygiene was fair. No signs or symptoms of temporomandibular joint disorders were observed. There were no significant findings in the panoramic radiograph.
 |
Figure 1 Orthodontic examination showing a convex profile with short chin-throat length and obtuse chin-throat angle. Intraoral findings include Class I molar relationship, Class II canine relationship on the left side, 2 mm lower midline shift to the left, and moderate lower anterior crowding. No posterior crossbite was observed. |
During history taking, the patient reported that his symptoms of unrefreshed sleep, witnessed gasping, snoring, and morning headache started 3 weeks ago. There was no significant change in his weight during that time to justify the onset of these symptoms. Instead, the patient was maintaining heavy exercises at the fitness club during the past 3 months and carrying weights to improve his body-building regime, including shoulder shrugs and overhead presses. The patient then complained of a widespread pain over his neck and shoulders, which was managed by a specific exercise (chin tuck exercise) recommended by his personal coach to manage the pain on his neck (Supplementary Video). The exercise was performed by pressing the chin with two fingers to push the lower jaw back and head as much as possible for 20 seconds for 10 times every session (Figure 2 and Supplementary Video). This exercise was recommended to be repeated three times everyday (total of 30 times/day). During that time, the discomfort in his neck decreased but was accompanied by the start of snoring and unrefreshed sleep after 3 weeks of continuous chin tuck exercise. The patient performed this exercise until his visit to an orthodontic clinic.
 |
Figure 2 Start and end positions of Chin tuck exercise. |
Diagnostic Assessment
He had a PSG for diagnosis of OSA. The PSG report showed an AHI of 10.6/h, and all apnea events were in the supine position, indicating positional OSA. He had a significant desaturation of oxygen of 86%. His rapid eye movement (REM) sleep was markedly reduced, accounting for only 11% of total sleep time, with an overall low sleep efficiency of 72.3%. His weight was 69.4 kg with a body mass index of 24 kg/m2. There was no periodic limb movements recorded. Continuous positive airway pressure (CPAP) was initiated during the sleep study at a pressure of 4 cm H2O, which reduced the AHI to 0.7/h (Table 1).
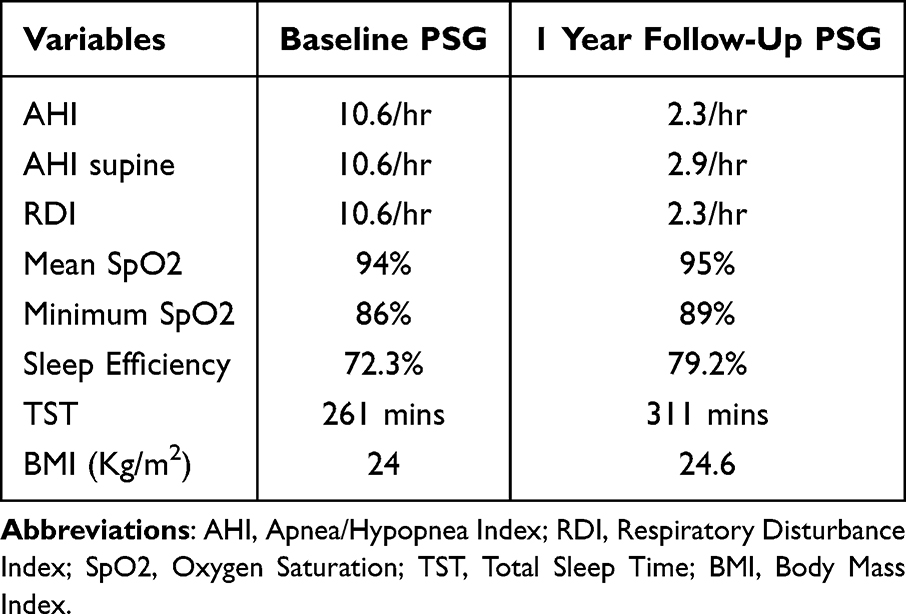 |
Table 1 Polysomnography Characteristics |
Therapeutic Intervention
Given that the patient main treatment goal was to manage his OSA and not his malocclusion, the treatment objectives were limited to treating his OSA and symptoms.
The following treatment options were discussed with the patient:
- CPAP: CPAP is considered as the first-line treatment for OSA. In this case, CPAP with a pressure of 4 cm H2O was required to decrease the AHI to a normal level, as per the PSG report. However, the patient was not willing to use CPAP and asked for other options.
- MAD: In cases of mild-to-moderate OSA, MADs can be considered a suitable treatment option for patients who are unwilling to use CPAP. These devices work by keeping the lower jaw in a forward position during sleep while miniaturizing the patent airway.
- Discontinuation of chin tuck exercises: Given that the symptoms started after performing the chin tuck exercises, the option of discontinuations of these exercises was discussed with the patient.
A decision was made to start the treatment of this case with discontinuation of the chin tuck exercise, without the use of MADs, while working on other alternatives to manage his neck pain, such as over-the-counter analgesics (acetaminophen 500 mg as needed) and lowering the weights used in the gym.
Follow-up and Outcomes
After two weeks of discontinuing the chin tuck exercises, the patient reported significant improvement in daytime sleepiness, witnessed gasping, snoring, and morning headache. The symptoms completely disappeared after 4 to 6 weeks. A second PSG was performed after 1 year to confirm the improvement in breathing during sleep. Although the patient’s weight increased to 70.35 kg, his AHI dropped to normal levels (2.3/h). His mean saturation of oxygen during sleep improved to 95%, and sleep efficiency improved to 79% (Table 1). His PSG interpretation concluded “normal sleep onset, with overall AHI of 2.3/h.”. Timeline from the patient’s initial clinical presentation to follow-up appointments is demonstrate in Figure 3.
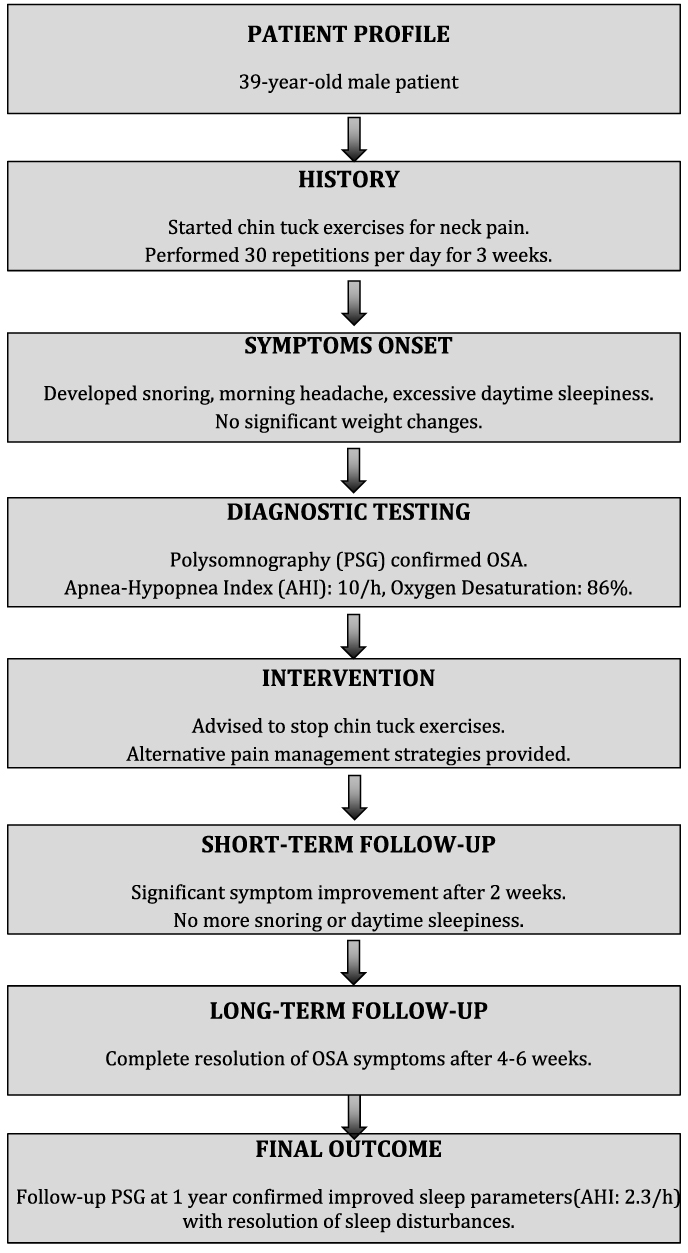 |
Figure 3 The timeline summarizes the patient’s initial presentation, symptom onset, diagnostic evaluation, intervention, and follow-up. It outlines the progression from the start of chin tuck exercises, the development of obstructive sleep apnea symptoms, diagnostic confirmation via polysomnography, treatment intervention, and subsequent resolution of symptoms. |
Discussion
Chin tuck exercise is one of the known exercises to manage FHP or neck pain.6 It was first introduced by McKenzie in 1983.6 In this study, we report a case in which the patient started to perform this exercise over a period of 3 weeks until it resulted in sudden onset of snoring, witnessed gasping during sleep, excessive daytime sleepiness, and morning headache. The patient was then diagnosed with mild OSA based on PSG. After stopping the exercises, symptoms improved immediately in 2 weeks, and sleep was significantly improved. Symptoms completely disappeared in 4 to 6 weeks, and follow-up PSG confirmed improved sleeping parameters with AHI returning to normal (2.3/h).
Neck pain is a common complaint among workers, with up to two out of three people experiencing it during their lifetime.17,18 A study on batik workers where employee were sitting in prolonged time with poor posture, chin tuck exercises were used as a self-managed intervention to reduce neck pain, muscle tension, and to improve cervical function.17,18 Although there is no evidence or clear recommendation for gym coaches to recommend chin tuck exercises for those lifting weights or using gym equipment, some coaches might recommend it aiming to relieve neck pain associated with weightlifting or to improve their posture during workouts. The exercise targets deep cervical flexor muscles, which are often weakened by forward head posture common in both sedentary workers and gym attendees.17
Although this exercise might be helpful for patients with FHP, it has different effects on the facial and neck muscles in patients with Normal Head Posture (NHP).19 A previous study was conducted to measure the biomechanical effect of the chin tuck exercise in patients with FHP versus NHP.19 It was found that NHP patients had an average muscle force of three times higher than the muscles force exerted by FHP patients while performing chin tuck exercises.19 This reflects that this exercise can result in extensive forces around the oropharynx region, especially in patients with NHP,19 who might be advised by physiotherapists to perform this exercise to manage their neck pain.
The fact that the chin tuck exercise resulted in OSA in this case, followed by the disappearance of OSA symptoms and improvement in AHI after discontinuation of exercise, reflects possible causation. This is supported by the fact that one of the possible treatment options for OSA is supervised myofunctional therapy, in which the upper airway muscle responsiveness can be improved.20 In other words, if facial exercise that is performed under supervised myofunctional therapists can improve muscle responsiveness and reduce the likelihood of oropharyngeal obstruction, then other exercises performed in the opposite direction might have opposite and negative effects on the patient’s airway. This finding encourages the need for careful assessment and investigation to identify situations in which chin tuck exercises can have a negative impact on patients’ health, especially that studies on the adverse effect of head and neck posture therapy are lacking.
In this case, there was no indication to take a lateral cephalometric radiograph or cone-beam computed tomography (CBCT) to assess the airway. Unlike the jaws and teeth, the airway is a dynamic structure, and its physiological activity cannot be measured using two-dimensional or three-dimensional radiographs. Moreover, airway measurements differ between the supine and standing positions,21–23 the position in which orthodontists take lateral cephalometric radiographs. Also, airway measurements change during sleep.24 There is no radiographic method reported to have high sensitivity or specificity to assess for the risk of OSA.2 Hence, lateral cephalometric radiographs or CBCT might lack the validity to evaluate the airway if it was aiming solely to assess for OSA.
This case report has several limitations. First, as a single-patient observation, the findings cannot be generalized, and causality between chin tuck exercise and the onset of OSA cannot be firmly established. Second, there was a difference in the time between symptom resolution and the follow up PSG, which was performed one year later due to insurance limitations. However, this may not represent a major limitation, as the symptoms of OSA, including snoring, gasping, morning headaches, and excessive daytime sleepiness were completely resolved within weeks of stopping the exercise, which reflects strong clinical evidence even before PSG confirmation. Finally, there were no dynamic endoscopic evaluation or biomechanical assessment performed to evaluate upper airway changes, which could have added further insight into the mechanism.
Conclusion
Chin tuck exercises that work on the neck and upper airway muscles may precipitate OSA in at-risk patients. In this case, the patient’s OSA symptoms completely resolved after discontinuing the exercises. Clinicians and fitness professionals should be aware of this potential risk, and further research is needed to clarify the underlying mechanisms.
Data Sharing Statement
The data supporting the findings of this case report are available from the author upon reasonable request. Due to patient confidentiality, some data cannot be shared publicly.
Ethical Consent
Written informed consent for publication of this case report and accompanying images were obtained from the patient. The case report has been prepared in accordance with the CARE guidelines.
Author Contributions
Conceptualization, Data Curation, Writing – Original Draft, Writing – Review & Editing: Suliman Alsaeed
Suliman Alsaeed approved the final version of the paper, agreed on the submission to Nature and Science of Sleep Journal, and accepts responsibility for all aspects of the work, ensuring that any questions related to accuracy or integrity are properly investigated and resolved.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
There is no conflict of interest to disclose.
References
1. Malhotra A, White DP. Obstructive sleep apnoea. Lancet. 2002;360(9328):237–245. doi:10.1016/S0140-6736(02)09464-3
2. Behrents RG, Shelgikar AV, Conley RS, et al. Obstructive sleep apnea and orthodontics: an American association of orthodontists white paper. Am J Orthodontics Dentofacial Orthopedics. 2019;156(1):13–28.e1. doi:10.1016/j.ajodo.2019.04.009
3. Aishah A, Eckert DJ. Phenotypic approach to pharmacotherapy in the management of obstructive sleep apnoea. Curr Opin Pulm Med. 2019;25(6):594–601. doi:10.1097/MCP.0000000000000628
4. Worsnop C, Kay A, Pierce R, Kim Y, Trinder J. Activity of respiratory pump and upper airway muscles during sleep onset. J Appl Physiol. 1998;85(3):908–920. doi:10.1152/jappl.1998.85.3.908
5. Kimoff RJ. Upper airway myopathy is important in the pathophysiology of obstructive sleep apnea. J Clin Sleep Med. 2007;3(6):567–569. doi:10.5664/jcsm.26964
6. McKenzie R. Treat Your Own Neck. Spinal Publications Raumati Beach; 1983.
7. Leigh J-H, Oh B-M, Seo HG, et al. Influence of the chin-down and chin-tuck maneuver on the swallowing kinematics of healthy adults. Dysphagia. 2015;30(1):89–98. doi:10.1007/s00455-014-9580-3
8. Oh D-H, Park H-S, Kim G-E. Effects of the chin-tuck maneuver on anatomical changes and angles during swallowing: a systematic review. J Korean Dysphagia Soc. 2022;12(1):1–13. doi:10.34160/jkds.2022.12.1.001
9. Welch MV, Logemann JA, Rademaker AW, Kahrilas PJ. Changes in pharyngeal dimensions effected by chin tuck. Arch Phys Med Rehabil. 1993;74(2):178–181.
10. Abd-Eltawab A, Shormana M, Elsherbini D, ElRazkey J. The effect of a rehabilitation neck exercise program on biomechanical head alignment, neck pain, and disability among nursing students: a randomized controlled trial. J Musculoskelet Surg Res. 2024;8:281–290. doi:10.25259/jmsr_74_2024
11. Sun X, Chai L, Huang Q, Zhou H, Liu H. Effects of exercise combined with cervicothoracic spine self-mobilization on chronic non-specific neck pain. Sci Rep. 2024;14. doi:10.1038/s41598-024-55181-8
12. Heng W, Wei F, Liu Z, et al. Physical exercise improved muscle strength and pain on neck and shoulder in military pilots. Front Physiol. 2022;13. doi:10.3389/fphys.2022.973304
13. Jones LB, Jadhakhan F, Falla D. The influence of exercise on pain, disability and quality of life in office workers with chronic neck pain: a systematic review and meta-analysis. Appl Ergon. 2024;117:104216. doi:10.1016/j.apergo.2023.104216
14. De Zoete R, Armfield N, McAuley J, Chen K, Sterling M. Comparative effectiveness of physical exercise interventions for chronic non-specific neck pain: a systematic review with network meta-analysis of 40 randomised controlled trials. Br J Sports Med. 2020;55(13):730–742. doi:10.1136/bjsports-2020-102664
15. Tsiringakis G, Dimitriadis Z, Triantafylloy E, McLean S. Motor control training of deep neck flexors with pressure biofeedback improves pain and disability in patients with neck pain: a systematic review and meta-analysis. Musculoskeletal Sci Pract. 2020;50:102220. doi:10.1016/j.msksp.2020.102220
16. Nazwar T, Bal’afif F, Wardhana D, Mustofa M. Impact of physical exercise (strength and stretching) on repairing craniovertebral and reducing neck pain: a systematic review and meta-analysis. J Craniovertebr Junction Spine. 2024;15(3):266–279. doi:10.4103/jcvjs.jcvjs_107_24
17. Hasmar W, Hadi P. Chin tuck exercise education for neck pain batik workers across Jambi City. Asian J Community Services. 2022. doi:10.55927/ajcs.v1i1.773
18. Hasmar W, Hadi P. Education on chin tuck exercises on neck pain for batik workers across the City of Jambi. Asian J Healthc Analytics. 2022. doi:10.55927/ajha.v1i2.1781
19. Han JW, Kim KH, Bae TS, Blaikie K. Biomechanical analysis of chin tuck exercise with a subject-specific neck model for the forward headed. Int J Precis Eng Manuf. 2018;19(4):587–592. doi:10.1007/s12541-018-0071-6
20. Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep. 2015;38(5):669–675. doi:10.5665/sleep.4652
21. Chubachi S, Yamada Y, Yamada M, et al. Differences in airway lumen area between supine and upright computed tomography in patients with chronic obstructive pulmonary disease. Respir Res. 2021;22(1):1–9. doi:10.1186/s12931-021-01692-1
22. Van Holsbeke CS, Verhulst SL, Vos WG, et al. Change in upper airway geometry between upright and supine position during tidal nasal breathing. J Aerosol Med Pulm Drug Deliv. 2014;27(1):51–57. doi:10.1089/jamp.2012.1010
23. Hsu WE, Wu TY. Comparison of upper airway measurement by lateral cephalogram in upright position and CBCT in supine position. J Dent Sci. 2019;14(2):185–191. doi:10.1016/j.jds.2019.01.007
24. Chuang L-P, Chen N-H, Li H-Y, et al. Dynamic upper airway changes during sleep in patients with obstructive sleep apnea syndrome. Acta oto-laryngologica. 2009;129(12):1474–1479. doi:10.3109/00016480902780242
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Uncontrolled Hypertension from Inappropriate Ventilator Settings in Obstructive Sleep Apnea: A Case Report
Tian SR, Thomas RJ, Ni YN
Nature and Science of Sleep 2026, 18:601053
Published Date: 30 May 2026