")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Arsenicism by Chronic Exposure to Mine Tailings in Peru: An Analysis of 17 Cases with Lesions on Skin and/or Annexes
Authors Ramos W , Ortega-Loayza AG, Díaz J, De La Cruz-Vargas JA , Tello M, Ronceros G, Loayza M, Gutierrez EL
Received 24 June 2022
Accepted for publication 16 September 2022
Published 8 November 2022 Volume 2022:15 Pages 2407—2414
DOI https://doi.org/10.2147/CCID.S378622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Willy Ramos,1,2 Alex G Ortega-Loayza,3 Jesús Díaz,4 Jhony A De La Cruz-Vargas,1 Mercedes Tello,5 Gerardo Ronceros,2 Manuel Loayza,1 Ericson L Gutierrez1
1Instituto de Investigaciones en Ciencias Biomédicas (INICIB), Universidad Ricardo Palma, Lima, Peru; 2Instituto de Investigaciones Clínicas, Universidad Nacional Mayor de San Marcos, Lima, Peru; 3Department of Dermatology, Oregon Health and Science University, Portland, OR, USA; 4Universidad Católica Santo Toribio de Mogrovejo, Chiclayo, Peru; 5Universidad Nacional Mayor de San Marcos, Lima, Peru
Correspondence: Ericson L Gutierrez, Instituto de Investigaciones en Ciencias Biomédicas (INICIB), Universidad Ricardo Palma, Av. Alfredo Benavides 5440, Santiago de Surco, Lima, 15039, Peru, Email [email protected]
Objective: To characterize the epidemiology and clinical manifestations of arsenicism from chronic exposure to mine tailings in people with lesions on their skin and/or annexes in two mining districts in the highlands of Peru.
Materials and Methods: In this case series study, we included 17 people that presented arsenical lesions in skin and annexes which were identified in two prior studies. We evaluated age, occupation, place of exposure, time of exposure, time of disease, manifestations on skin and annexes, location of lesions, severity, and 24-hour urine clearance of arsenic.
Results: The average time of exposure was 16.5 ± 14.7 years, and the average length of disease was 9.8 ± 8.1 years. In this study, 70.6% were men, 41.2% were farmers and 17.6% were underage. The most frequent main manifestations in skin and annexes were plantar keratosis (23.5%), palmar (11.8%), palmoplantar (11.8%) and thoracic keratosis (5.9%). Other manifestations were palmoplantar keratosis with thoracic hyperpigmentation (17.6%), Mees’ lines (17.6%) and hyper/hypopigmentation in thorax and back (11.8%). With relation to the severity of lesions, 35.3% were grade 1 (mild), 29.4 % were grade 0 (asymptomatic), 29.4 % were grade 2 (moderate), and 5.9% were grade 3 (severe). The median of 24-hour urine clearance of arsenic was 55 μg/L/24 hours. No cases of skin cancer were presented.
Conclusion: The studied cases of arsenicism with lesions on skin and/or annexes by exposure to mine tailings present with differential characteristics in comparison to other forms of arsenicism such as less severity, lower urine clearance of arsenic, and absence of skin cancer cases.
Keywords: arsenicism, mine tailings, Peru
Plain Language Summary
What is already known on this topic
The main form of worldwide-reported exposure is chronic hydroarsenicism and arsenicism by the combustion of arsenic-rich carbon. Few studies exist that evaluate the characteristics of arsenicism from exposure to mine tailings.
What this study adds
This research shows that the cases studied on arsenicism from exposure to mine tailings are presented mainly in adult males, farmers, with over a decade of exposure and residents in populated areas of the highlands. The most frequent lesions were palmar and/or plantar keratosis, of non-severe characteristic and with relatively low clearance of arsenic.
How this study might affect research, practice or policy
The identification of arsenicism cases evidence the need to implement policies to mitigate the environmental impact of mining activities, as well as the respect and supervision of existing norms.
Introduction
Arsenic is a metalloid that is found widely distributed in nature, and humans may develop intoxication as a consequence of acute or chronic exposure. Arsenic may enter the organism through its accidental ingestion in water or food, through inhalation or percutaneous.1–3
Arsenicism is a clinical entity that is produced by environmental, occupational or medicinal exposure to arsenic. It is characterized by a variety of signs and symptoms that range from the presence of skin lesions up to cutaneous and visceral malignancy after 10–20 years of exposure. This is why signs of chronic arsenicism such as keratosis and hyper/hypopigmentation are considered as possible cutaneous markers of internal malignancy.3–7
The main form of worldwide reported exposure is chronic hydroarsenicism that is produced through the ingestion of arsenic in water with concentrations above 30 μg/L, which constitutes a public health problem mainly affecting countries such as Bangladesh,8,9 India,9,10 China,11 Argentina12 and Chile.13 Another form of arsenicism has been reported in China consistent with the use of arsenic-rich carbon (826–2578 mg/kg), which is used by the population for household cooking. The combustion of this produces arsenic emissions that contaminate indoor air and food.11,14–16 Other forms of exposure are the use of Chinese traditional medicine which includes arsenic-based components17 and seafood consumption.18
During the years 2003 and 2008, our research group reported cases of arsenicism from chronic exposure to environmental liabilities in the form of mine tailings. The first report was performed in San Mateo de Huanchor,19 a district in the province of Huarochirí (Lima-Peru) where we found that chronic exposure to mine tailings of Mayoc and Tamboraque with arsenic concentrations above 10,000 mg/kg (Figure 1A) significantly increased the rate of dermatological disease in the exposed population, which included arsenical dermatosis. A second report showed arsenicism cases from chronic exposure to the drainage fields of El Madrigal20 in the province of Caylloma (Arequipa-Peru) (Figure 1B). The zone exposed to the mine tailings of San Mateo de Huanchor was found at 3000 m.a.s.l. and its population’s main work activity was trade and in a lower scale agriculture, while Madrigal is at 3262 m.a.s.l. and its population’s work activities were agriculture, farming, and tourism. Between September 2005 and January 2006, the mine tailings of Mayoc were finally removed and relocated to the drainage fields of Tamboraque.21
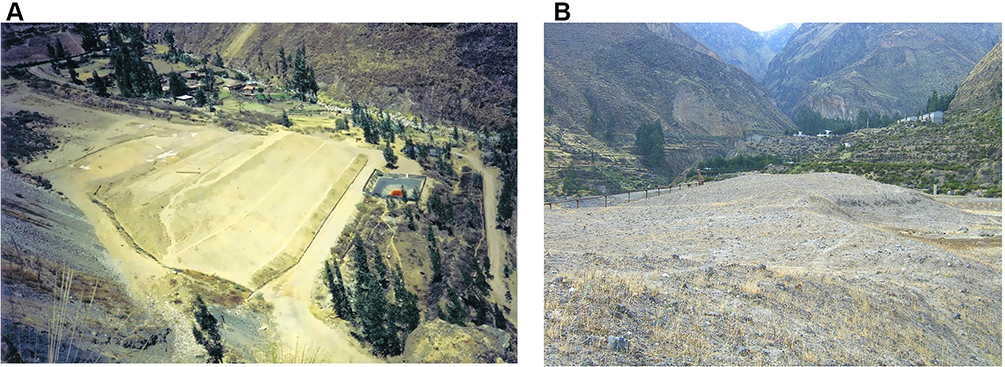 |
Figure 1 Exposure to mine tailings in sparsely populated agricultural areas in the highlands of Peru. (A) Mine tailings of Mayoc. (B) Mine tailings of El Madrigal. |
There are few studies that evaluate the characteristics of arsenicism by exposure to mine tailings in terms of exposure time, occupation, types of skin lesions, lesion severity, carcinogenicity and arsenic clearance in urine. Our clinical observations evidenced that arsenicism by exposure to mine tailings could have differential characteristics in comparison to arsenicism caused by other forms of exposure such as the consumption of water with high concentrations of arsenic, combustion of carbon mineral rich in arsenic or the use of Chinese traditional medicine. This led us to ask which are the epidemiological and clinical characteristics of arsenicism from exposure to mine tailings and if these presented relevant differences in comparison to other forms of arsenicism reported internationally.
The objective of this study was to characterize the epidemiology and clinical manifestations of arsenicism from chronic exposure to mine tailings across the analysis of 17 cases in two districts in the highlands of Peru.
Materials and Methods
Study Design and Participants
This was a case series study. In this research, we included all cases with diagnosis of arsenicism with lesions on skin and annexes identified in the studies of “dermatological diseases associated with chronic exposure to heavy metals and metalloids in mine tailings” (DHMMMT) performed in Peru.19,20 DHMMMT were cross-sectional studies carried out between the years 2003 and 2008 in the districts of San Mateo de Huanchor (Lima) and El Madrigal (Arequipa).
In this study, we included patients of all ages and sex who presented exposure to mine tailings and those who presented arsenical cutaneous lesions during the clinical examination. We excluded from the study any patient with occupational exposure to arsenic or other source different from mine tailings.
Procedures
We reviewed data bases of the DHMMMT studies obtaining the epidemiological and clinical characteristics of patients with arsenical lesions on skin and annexes exposed to mine tailings:
- Epidemiological characteristics: age, sex, origin, occupation, place of exposure and time of exposure to mine tailings.
- Clinical characteristics: length of disease, manifestations of skin and annexes, lesion location, lesion severity, arsenic in urine clearance in 24 hours and concentrations of arsenic in nails.
For study purposes, we defined chronic arsenical lesions as Mees’ lines, hyperpigmentation and/or hypopigmentation in thorax and back, palmar or plantar keratosis and non-melanoma skin cancer in areas that are not photo exposed. The severity of lesions was classified using criteria reported by Kadono14 in a prior study of chronic endemic hydroarsenicism performed in Bangladesh. DHMMMT used atomic absorption spectrophotometry for the quantification of arsenic clearance in urine and anodic stripping voltammetry to determine arsenic concentration in nails.
Statistical Analysis
The statistical analysis was carried out with the SPSS 26 program for Windows. The univariate statistics was carried out based on the collection of frequencies, percentages, central tendency and dispersion methods. The bivariate analysis was carried out with Fisher's exact test, Student’s t-test for independent samples, Pearson’s correlation and one-way analysis of variance (ANOVA). The calculations were performed with a confidence level of 95%.
Ethical Aspects
This research did not involve risks to the patients’ health since it was carried out from the information previously obtained in the studies of DHMMMT which had the approval of the ethical committees Comité de Ética del Hospital Nacional Dos de Mayo (Lima-Perú) and from Comité de Ética del Hospital Nacional Carlos Alberto Seguín Escobedo (Arequipa-Perú).
This research was approved by the Research Ethics Committee of the “Facultad de Medicina de la Universidad Ricardo Palma” (Expedited review: PI-004-2022). All participants were informed about the study, and signed informed consent was received from them. We guaranteed confidentiality of the information obtained, which was only used for the purpose of this study. The authors confirm that the guidelines outlined in the Declaration of Helsinki were followed.
Results
Epidemiological Characteristics
We diagnosed 17 cases of arsenicism with lesions on skin and/or annexes; 76.4% were male and 23.6% were female, the average age of patients was 40.8 ± 19.9 years, and the most affected age group was between 40 and 49 years of age (23.5%). Three cases corresponded to patients of pediatric age of 8, 9 and 17 years old. The most frequent occupations were farmer, student, and merchant. Cases were taken from a 2 km radius from the tailings of Mayoc (47.1%) and Tamboraque (29.4%); and a radius of 5 km from the tailings of Madrigal (23.5%). The average time of exposure was 16.5 ± 14.7 years varying between 6 and 48 years. The epidemiological characteristics of cases are shown in Table 1.
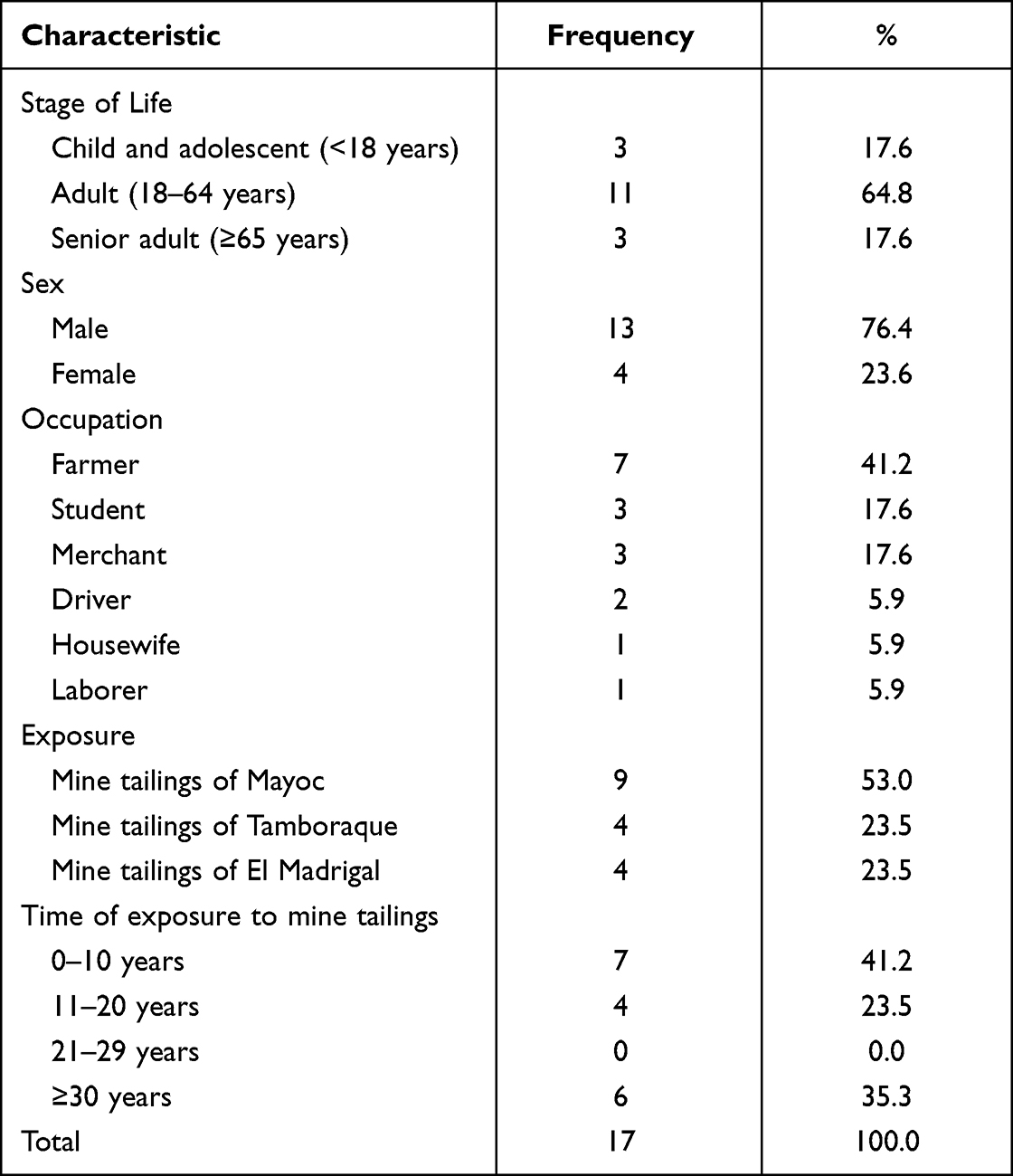 |
Table 1 Epidemiological Characteristics of Patients with Arsenicism from Chronic Exposure to Mine Tailings |
Clinical Characteristics
At the time of the dermatological examination, the average time of disease was 9.8 ± 8.1 years. The most frequent manifestations of arsenicism (Tables 2 and 3) were keratosis located in plantar of feet (23.5%), palms of hands (11.8%), palmoplantar (11.8%) and thorax (5.9%). Other manifestations were palmoplantar keratosis and hyper/hypopigmentation (17.6%), Mees’ lines (17.6%) and hyper/hypopigmentation of thorax and back (11.8%). The cases in pediatric age corresponded to plantar keratosis and Mees’ lines. There were no non-melanoma skin cancer cases in the studied population.
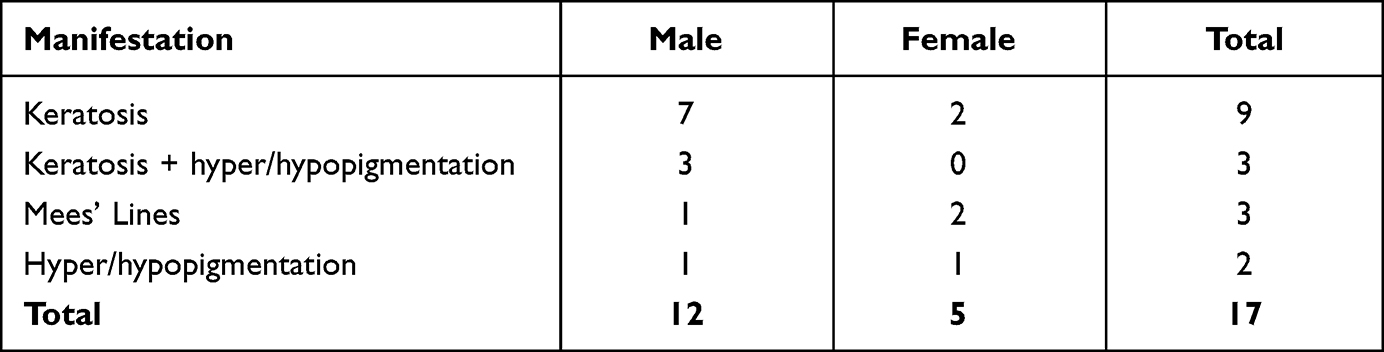 |
Table 2 Arsenicism Manifestations in Skin and Annexes from Chronic Exposure to Mine Tailings |
 |
Table 3 Epidemiological and Clinical Characteristics of Arsenicism Cases with Lesions on Skin and/or Annexes from Chronic Exposure to Mine Tailings |
Regarding the severity of lesions, 35.3% were grade 1 (mild), 29.4% were grade 0 (asymptomatic), 29.4% were grade 2 (moderate), and 5.9% were grade 3 (severe). We did not find a statistically significant relationship between age and lesion severity concentration plant operations.(ANOVA; p=0.847), there was also no statistically significant difference between the frequency of moderate-to-severe lesions in men and women (Fisher’s exact test; p=0.139).
Keratosis was most frequent in the male subjects, while in the female subjects, we did not observe a predominance of any manifestation (Table 3). We did not find cases of malnutrition associated to arsenical lesions. The average clearance of arsenic in urine of 24 hours was 51.5 ± 11.4 μg/L/24 hours (Median 55 μg/L/24 hours); while arsenic concentrations in nails of 4 patients were in average 0.85 ± 0.16 μg/g (Median 0.90 μg/g) which varied between 0.63 y 0.96 μg/g. There was no correlation between age and arsenic clearance in urine (Pearson’s correlation; R=0.071; p=0.817), there was also no statistically significant difference between arsenic clearance in urine and severity of lesions with an average clearance of 52.8 μg/L/24 hours in asymptomatic lesions, 54.8 μg/L/24 hours in mild lesions and 48.0 μg/L/24 hours in moderate-to-severe lesions (One-way ANOVA; p=0.698).
Discussion
This research shows that the cases studied on arsenicism from exposure to mine tailings with lesions on skin and/or annexes are presented mainly in adult males, farmers, with over a decade of exposure and residents in populated areas of the highlands. The most frequent lesions were palmar and/or plantar keratosis, of non-severe characteristic and with relatively low clearance of arsenic.
From the epidemiological point of view, the described cases of arsenicism from mine tailings are presented in settlements of San Mateo de Huanchor (Mayoc, Daza, Tamboraque) and in the populated center of El Madrigal which constitute sparsely populated or rural Andean areas, of low socioeconomic income, in which the deposits of mine tailings have been carried out without adequate measures of environmental or technological control to mitigate the toxicity of these residues. We also found cases near a mine that did not carry out an adequate closure of its operations, leaving its environmental liabilities unattended for years and decades. In this manner, exposure to arsenic in mine tailings does not occur in a massive form such as hydroarsenicism, rather it is frequent in areas where the economy greatly depends on mining operations and where state supervision is insufficient.19,20
There are common characteristics of arsenicism from mine tailing exposure with other forms of arsenicism such as the frequent affectation in adult males, as well as the presence of keratosis and hyper/hypopigmentation type lesions. A distinctive characteristic is the severity of the lesions since the people exposed to mine tailings presented with greater rate of mild-to-moderate lesions without any cases of skin cancer observed (unlike hydroarsenicism and arsenicism from carbon combustion) despite surpassing 20 years of exposure and 15 years of disease in many cases (Table S1).3–5,7
A possible explanation for these findings is that arsenic concentrations of mine tailings are reduced with wind dispersion and as the distance from workplace or residence to the fields where the tailing deposits are located is increased.22 In this manner, people are exposed for years or decades to harmful health concentrations, enough to develop skin and/or annex lesions but not enough to cause severe lesions or skin cancer. Another possible explanation is that the mechanisms of percutaneous and inhalation toxicity were less effective than the intake to reach high concentrations of arsenic in the human body since skin as well as respiratory epithelium constitute natural barriers.23–26
This coincides with experimental studies that show the application of dust from soil rich in arsenic for pesticide use (1230–1400 mg/kg) on skin of Rhesus monkeys27 results in dermic absorption of inorganic arsenic under 1%. Likewise, studies carried out in rabbits subjected to different concentrations of inhaled arsenic trioxide 8h/day for 8 weeks, show a significant increase in its plasma metabolites only at high doses (1.1 mg/m3) in comparison to those exposed to lower doses (0.22, 0.1 and 0.05 mg/m3) that show no significant differences with the concentrations of controls.28
The lower efficiency of percutaneous and inhalation mechanisms is founded also in the comparatively inferior levels of arsenic in urine (see Table S1). If the urine clearance is low, it is probable that the blood levels of arsenic will also be low and insufficient for carcinogenesis or require greater exposure time compared to the other forms of arsenicism.29,30 Another possibility would be the existence of subjects studied on genetic polymorphism for the methylation of inorganic arsenic that favors its rapid metabolism and excretion as well as the decrease in its retention and toxic effects in the organism.31–35
Arsenic urine clearance in our study is inferior to that reported in a study carried out by the (CDC) on women of fertile age (n=194) and children from 1 to 12 years of age (n=163) from Cerro de Pasco (Peru), a mining city in the center of Peru.36 This study found that nine people had inorganic arsenic levels above 35 µg/dL with a clearance variation between 44.2 and 150.3 µg/dL. The highest levels of arsenic clearance in urine among the population of Cerro de Pasco could be explained by the greater exposure since an important percentage were not only exposed to mine tailings but also to open-pit mining and to mineral concentration plant operations. Unfortunately, the authors did not evaluate the presence of arsenical skin lesions since they were focused primarily on describing the exposure of the population to lead.36
The greater frequency of cases was among farmers. This can be explained as in the regions studied, the mine tailings are found in areas close to farmlands, which constitutes as the group with greater exposure (Figure 1). In other occupational groups, exposure to arsenic tailing dust could occur from the dispersion of such with the wind that transports it to residences and workplaces.37–39
The main limitation of this study is that there are no existing studies showing all the sources of exposure to arsenic in areas where the mine tailings are at; however, it represents that exposure to mine tailings is the primary source of exposure due to its high arsenic concentration in tailings (above 10,000 mg/kg in Mayoc),37 due to its proximity to households or workplaces of inhabitants and by the exclusion of cases related to occupational or industrial exposure, which is why from an epidemiological point of view, it is possible to attribute it as the major cause of the lesions.
Another limitation is the number of cases considered in our analysis, which is small if it is compared to reports carried out for hydroarsenicism, considering that even data collection was multicentric and included populated centers or settlements exposed to mine tailings. We must take into account that this form of arsenicism occurs in sparsely populated or rural areas, which results in the number of cases not to be so elevated. The DHMMMT studies were carried out between 2003 and 2008, the population exposure to residues or contaminants from mining activity constitutes a phenomenon currently active worldwide.
On the other hand, original studies did not carry out the arsenic dosage in nails of all patients due to the lack of financing, with the possibility in only four of them. Despite that, this data was included in the article as reference.
The identification of arsenicism cases evidences the need of implementing policies to mitigate the environmental impact of mining exploitation, as well as respect and supervision of existing norms. We consider it necessary carrying out prospective and multicentric studies that allow verification of our findings in populations exposed to environmental mining liabilities, that compromise a greater number of patients and permit to evaluate the evolution of time of arsenical lesions. It is also necessary to characterize the lesion severity, associated factors and its relationship with factors such as time exposure and arsenic clearance in urine.
Conclusion
In conclusion, the cases studied on arsenicism with lesions on skin and/or annexes by exposure to mine tailings present differential characteristics in comparison with other forms of arsenicism such as less severity, lower clearance of arsenic in urine and absence of skin cancer cases.
Acknowledgment
We appreciate the expertise and guidance of Dr Ferdinand de Amat Loza, who passed away in 2020.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Rehman K, Fatima F, Waheed I, et al. Prevalence of exposure of heavy metals and their impact on health consequences. J Cell Biochem. 2018;119(1):157–184. doi:10.1002/jcb.26234
2. Hughes MF, Beck BD, Chen Y, et al. Arsenic exposure and toxicology: a historical perspective. Toxicol Sci. 2011;123(2):305–332.
3. Yu HS, Liao WT, Chai CY. Arsenic carcinogenesis in the skin. J Biomed Sci. 2006;13(5):657–666.
4. Cohen SM, Chowdhury A, Arnold LL. Inorganic arsenic: a non-genotoxic carcinogen. J Environ Sci. 2016;49:28–37.
5. Sage AP, Minatel BC, Ng KW, et al. Oncogenomic disruptions in arsenic-induced carcinogenesis. Oncotarget. 2017;8(15):25736–25755.
6. Jomova K, Jenisova Z, Feszterova M, et al. Arsenic: toxicity, oxidative stress and human disease. J Appl Toxicol. 2011;31(2):95–107.
7. Frumkin H, Thun MJ. Environmental carcinogens: arsenic. CA Cancer J Clin. 2001;51:254–262.
8. Kadono T, Inaoka T, Murayama N, et al. Skin manifestations of arsenicosis in two villages in Bangladesh. Br J Dermatol. 2002;41:841–846.
9. Rahman MM, Chowdhuri UK, Mukherjee SC, et al. Chronic arsenic toxicity in Bangladesh and West Bengal-A review and commentary. Clin Toxicol. 2001;39:683–700.
10. Bhowmick S, Pramanik S, Singh P, et al. Arsenic in groundwater of West Bengal, India: a review of human health risks and assessment of possible intervention options. Sci Total Environ. 2018;612:148–169. doi:10.1016/j.scitotenv.2017.08.216
11. Liu DN, Lu XZ, Li BL, et al. Clinical analysis of 535 cases of chronic arsenic poisoning from coal burning [in Chinese]. Chin J Med. 1992;31:560–562.
12. Lepori ECV. Hidroarsenicismo crónico regional endémico en Argentina. Acta Bioquímica Clínica Latinoam. 2015;49(1):83–104.
13. Smith AH, Arroyo AP, Guha DN, et al. Arsenic-induced skin lesions among Atacameño people in Northern Chile despite good nutrition and centuries of exposure. Environ Health Perspect. 2002;108:617–620.
14. An D, Ho GY, Hu XQ. Chronic arsenic-fluorine intoxication from burning coals with high arsenic and fluorine content [in Chinese]. Chin J Prev Med. 1994;28:312–313.
15. Shraim A, Cui X, Li S, et al. Arsenic speciation in the urine and hair of individuals exposed to airborne arsenic through coal-burning in Guizhou, PR China. Toxicol Let. 2003;137:35–48. doi:10.1016/S0378-4274(02)00379-X
16. Zhao Y, Zhang J, Huang W, et al. Arsenic emission during combustion of high arsenic coals from Southwestern Guizhou, China. Energy Conver Manage. 2008;49:615–624. doi:10.1016/j.enconman.2007.07.044
17. Wong SS, Tan KC, Goh CL. Cutaneous manifestations of chronic arsenicism: review of seventeen cases. J Am Acad Dermatol. 1998;38(2 Pt 1):179–185. doi:10.1016/S0190-9622(98)70596-1
18. Taylor V, Goodale B, Raab A, et al. Human exposure to organic arsenic species from seafood. Sci Total Environ. 2017;15(580):266–282.
19. Ramos W, Galarza C, Ronceros G, et al. Noninfectious dermatological diseases associated with chronic exposure to mine tailings in a Peruvian district. Br J Dermatol. 2008;159:169–174. doi:10.1111/j.1365-2133.2008.08630.x
20. De Amat F, Ramos W. Enfermedades dermatológicas de tipo no infeccioso asociadas a exposición a relaves mineros en un distrito expuesto y otro no expuesto. Dermatol Peru. 2016;26(3):138–142.
21. López Pino PR. Fitorremediación en los suelos de Mayoc, San Mateo, Huarochirí-Lima [Tesis maestría]. Lima: Universidad Nacional de Ingeniería; 2011.
22. Djebbi C, Chaabani F, Font O, et al. Atmospheric dust deposition on soils around an abandoned fluorite mine (Hammam Zriba, NE Tunisia). Environ Res. 2017;158:153–166.
23. Jensen JM, Proksch E. The skin’s barrier. G Ital Dermatol Venereol. 2009;144(6):689–700.
24. Nielsen JB, Benfeldt E, Holmgaard R. Penetration through the Skin Barrier. Curr Probl Dermatol. 2016;49:103–111.
25. Celebi Sözener Z, Cevhertas L, Nadeau K, et al. Environmental factors in epithelial barrier dysfunction. J Allergy Clin Immunol. 2020;145(6):1517–1528.
26. Lee PH, Park S, Lee YG, et al. The impact of environmental pollutants on barrier dysfunction in respiratory disease. Allergy Asthma Immunol Res. 2021;13(6):850–862.
27. Lowney YW, Wester RC, Schoff RA, et al. Dermal absorption of arsenic from soils as measured in the rhesus monkey. Toxicol Sci. 2007;100:381–392.
28. Beck BD, Slayton TM, Farr CH, et al. Systemic uptake of inhaled arsenic in rabbits. Hum Exp Toxicol. 2002;21:205–215.
29. Pandey PK, Yadav S, Pandey M. Human arsenic poisoning issues in central-east Indian locations: biomarkers and biochemical monitoring. Int J Environ Res Public Health. 2007;4(1):15–22.
30. Ahsan H, Perrin M, Rahman A, et al. Associations between drinking water and urinary arsenic levels and skin lesions in Bangladesh. J Occup Environ Med. 2000;42(12):1195–1201.
31. Chen YC, Guo YL, Su HJ, et al. Arsenic methylation and skin cancer risk in southwestern Taiwan. J Occup Environ Med. 2003;45:241–248.
32. Chen YC, Su HJ, Guo YL, et al. Arsenic methylation and bladder cancer risk in Taiwan. Cancer Causes Control. 2003;14:303–310.
33. Steinmaus C, Bates MN, Yuan Y, et al. Arsenic methylation and bladder cancer risk in case-control studies in Argentina and the United States. J Occup Environ Med. 2006;48:478–488.
34. Tseng CH, Huang YK, Huang YL, et al. Arsenic exposure, urinary arsenic speciation, and peripheral vascular disease in blackfoot disease hyperendemic villages in Taiwan. Toxicol Appl Pharmacol. 2005;206:299–308.
35. Schläwicke Engström K, Broberg K, Concha G, et al. Genetic polymorphisms influencing arsenic metabolism: evidence from Argentina. Environ Health Perspect. 2007;115:599–605.
36. Conklin L, Sánchez CA, Neri A, et al. Reporte final. Exposiciones a metales pesados en niños y mujeres en edad fértil en tres comunidades mineras Cerro de Pasco, Perú 21 de Mayo – 4 de Julio de 2007. Atlanta: Centers for Disease Control and Prevention; 2008.
37. Golder Associates Perú. Investigación Geoquímica de los Relaves de Mayoc: resultados e Implicancias Para el Cierre. Lima: Golder Associates Perú; 2004.
38. Bempah CK, Ewusi A, Obiri-Yeboah S, et al. Distribution of arsenic and heavy metals from mine tailings dams at obuasi municipality of Ghana. Am J Engineer Res. 2013;2(5):61–70.
39. Martin R, Dowling K, Pearce D, et al. Health effects associated with inhalation of airborne arsenic arising from mining operations. Geosciences. 2014;4:128–175.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.