")
Back to Journals » Patient Preference and Adherence » Volume 17
Are Nurse-Led Patient Consultations and Nurse-Led Dose Adjustments of Permanent Medication Acceptable for Patients with Diabetes Mellitus and Hypertension in General Practice? – Results of a Focus Group Study
Authors Weise S, Steybe T, Thiel C, Frese T
Received 10 March 2023
Accepted for publication 3 June 2023
Published 23 June 2023 Volume 2023:17 Pages 1501—1512
DOI https://doi.org/10.2147/PPA.S411902
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Solveig Weise,1 Tatjana Steybe,1 Carolin Thiel,1,2 Thomas Frese1
1Institute of General Practice and Family Medicine, Martin Luther-University Halle-Wittenberg, Halle (Saale), ST, Germany; 2SRH University of Applied Health Sciences, Gera, Thuringia, Germany
Correspondence: Solveig Weise, Institute of General Practice and Family Medicine, Medical Faculty of Martin Luther-University Halle-Wittenberg, Magdeburgerstr. 8, Halle (Saale), D-06120, Germany, Tel +49 345 557 5338, Fax +49 345 557 5340, Email [email protected]
Purpose: Practice nurse (PN)-led patient consultations and PN-led dosage adjustments of permanent medication are uncommon and not well studied in general practice (GP) in Germany. We investigated the perspectives of patients with common chronic diseases in Germany, diabetes mellitus (DM) type 2 and/or arterial hypertension (AT), on PN-led patient consultations and dosage adjustments of permanent medications in GP.
Patients and Methods: In this exploratory qualitative study, online focus groups were conducted using a semi-structured interview guide. Patients were recruited from collaborating GPs according to a predefined sampling plan. Patients were eligible for this study if they had DM or AT treated by their GP, were on at least one permanent medication and were aged 18 years or older. Focus group transcripts were analyzed using thematic analyses.
Results: Analyses of two focus groups, involving a total of 17 patients, revealed four main themes: (1) openness to the PN-led care and perceived benefits, eg because of patients’ confidence in PNs’ skills, or patients’ impression that PN-led care would better meet their needs and increase their compliance. Some patients had (2) reservations and perceived risks, especially for PN-led medication changes eg feeling that medication adjustments were a GP’s issue. Patients identified (3) reasons for encounters where they were likely to accept PN-led consultation and medication advice, eg management of DM, AT and thyroid disease. Patients also saw several important general requirements for the implementation of PN-led care in German general practice (4).
Conclusion: There is a potential for openness towards PN-led consultation and PN-led medication adjustment for permanent medication in patients with DM or AT. This study is the first qualitative study to investigate PN-led consultations and medication advice in German general practice. If the implementation of PN-led care is planned, our findings add the patients’ perspectives of acceptable reasons for encounter for PN-led care and their general requirements.
Keywords: task delegation, primary care, nurse-led care, qualitative study, patients’ perspective, team care
Introduction
Task delegation from general practitioners (GPs) to practice nurses (PNs) is considered a feasible approach to meet the current challenges facing general practice (GPc).1 Task delegation aims to empower practice teams to maintain high quality of care standards while reducing the workload on GPs.1–3 There is evidence that physician-nurse substitution in GPc leads to similar or probably better health outcomes.4,5 For example, arterial hypertension (AT) and diabetes mellitus (DM) appear to be slightly better controlled in PN-led care compared with physician-led care in GPc.4,5 In addition, mortality may be lower and patient satisfaction appears to be higher.5 International studies showed a rather good patient acceptance of PN-led care in GPc.6,7
Task delegation and team care is a common approach in GPc in many European countries6,7 and worldwide8 in primary care, but varies considerably between different countries. For example, in Australia, Canada, Ireland, the Netherlands, New Zealand, the United Kingdom and the USA task-shifting from physician to advanced practice nurse (APNs) is applied extensively.8 In these countries, APNs in primary care carry out patient consultations, diagnose conditions, order tests, manage conditions as eg high blood pressure and diabetes mellitus. This includes including changing medication dosages and prescribing medications.6,8 In other European countries as Finland, Sweden and Denmark task shifting is a little bit more limited in primary care.9 There, APN are not allowed to prescribe drugs and diagnose conditions, but perform all the other tasks listed above.8 In Austria, the Czech Republic, France and Germany task-shifting is very limited. In these countries, practice nurses (PNs) are not allowed to prescribe drugs, independently change the dose of medication, consult patients, make diagnoses or order tests in primary care.8
In Germany, PNs have a high workload and are essential in German GPc, but they perform only minor tasks (Box A1) and work under the close supervision of the GP. In recent years, PNs have increasingly undertaken additional training and qualifications.1,10 These specialised PNs were referred to as VERAH (health care assistants in family practice) or NäPa (non-physician practice assistants). VERAH/NäPa are allowed to carry out a wider range of tasks than ordinary PN, eg to carry out home visits or vaccinations independently.10 However, German GPs remain legally accountable for the health care provided in their practice. Studies have shown that task delegation from GPs to VERAH/NäPa or PNs is well accepted by patients, doctors and PNs.1,10–13
Recently, VERAH have been allowed to conduct patient consultations independently in German primary care. However, these are not widely available and not well studied. In particular, patients’ views on the scenario of PN-led patient consultations and PN-led dosage changes for permanent medication are understudied in German GPc. A nationwide German survey investigated the views of the general population on PN-led patient consultations in Germany. It included patients’ views on consultations for patients with chronic diseases in general, without focusing on specific diseases. In addition, this survey did not investigate PN-led dose adjustments for long-term medication (DCPM), nor patients’ perceived risks and benefits.1 Furthermore, this study did not focus on the attitudes of chronically ill patients, who make up the largest patient group in primary care. Although there are international surveys investigating these issues,4 the results are not transferable to German GPc due to structural differences in the health care system and differences in task-shifting in primary care.
Therefore, this study investigates the perspectives of chronically ill patients on PN-led patient consultations and PN-led DCPM.
Materials and Methods
Study Design and Setting
The study follows an explorative qualitative design, performed by two online focus groups using a semi-structured interview guide. In this interview guide, the researcher team first gave an impulse report about roles of PN in other countries. The research team reported that internationally, PN regularly and independently perform patient consultation for chronically ill patients in primary care. Furthermore, the researcher team explained that PN in other countries were allowed to alter the number of tablets or the dosage of the GP-prescribed medication. We explained that this specifically excludes all matters of prescription, as well as ending or starting medications. Then, participants were asked the following questions during the focus group: 1) How do you feel about a PN-led patient consultation? 2) For which diseases or health issues would you accept PN-led patient consultation? 3) Which general requirements do you think are necessary for PN-led patient consultation? 4) How do you feel about PN-led DCPM? 5) For which medications would you accept PN-led DCPM? 6) Which general requirements do you think are necessary for PN-led DCPM? 7) What benefits and risks do you see in the context of PN-led patient consultation and PN-led DCPM? 8) Would you like to add anything you felt has not been mentioned in this discussion so far?
Study Population
We applied the following inclusion criteria: Having DM type 2 and/or AT and therefore being treated in GP’s office; taking at least one permanent medication; aged over 18 years; sufficient knowledge of the German language and ability to give consent. Exclusion criteria were refusal or withdrawal of consent to the study; inadequate German language skills; being unable to give informed consent; or a severe illness that does not allow study participation. Further chronic conditions were not an exclusion criteria.
Sampling
We selected our study participants for each focus group to be as heterogeneous as possible, according to a qualitative sampling plan (Table A1). It was evidence-based concerning the criteria as practice structure (group/single practice), practice size (number of patients/physicians), patient gender and age7,14 and, additionally, on self-developed criteria based on experience of the research team as job location (city/rural) and residential area (city/rural).
Recruitment
Cooperating GPcs were selected if they matched the criteria of a predeveloped qualitative recruitment plan (eg rural or city practices, single or group practices; Table A1). We developed the qualitative recruitment plan based on literature criteria (age, gender, residential area city/rural)1 and consensus criteria in the author team (eg practice structure, practice size). Cooperating GPcs informed potential participants matching our eligibility criteria about the study. Interested patients were contacted by the research team and completed a short questionnaire on occupational and socio-demographic data in advance. Recruitment continued until a content saturation was reached. All focus group interviews were audio- and videotaped, conducted in German language and lasted between 85- and 130-mins. Interviews were transcribed and all participants were pseudonymized to ensure their anonymity. This study was performed according to the Declaration of Helsinki. Participants gave their informed consent to participate including further scientific analyses and publication of anonymized responses. This study was approved by the ethical review board of the Medical Faculty of the Martin-Luther-University Halle-Wittenberg, Germany (approval number 2020-005) prior to starting the study.
Data Analyses
We analyzed data using Thematic Analyses. Thematic Analyses aim to identify patterns or topics in qualitative data.15 In summary, it includes six framework steps of thematic analysis: 1) become familiar with the material by reading the transcripts several times; 2) start with initial coding to identify first ideas of key themes; 3) search for themes to ascertain frameworks; 4) review themes/framework; 5) define themes close to data and 6) write up and interpret themes. For Thematic Analyses, it is important to note that these steps are not linear, but researchers can move back and forth between steps. Initially, three researchers coded the transcripts completely (ST, CT, SW) ; then, coding results were discussed and compared within the author team. Finally, the themes were summarized and assessed regarding the underlying topics of the research questions. Disagreements about the data were discussed and resolved by consensus. Analysis was supported by MAXQDA 2018 (VERBI Software GmbH, Berlin, Germany). When presenting patient quotes, we use “many” when more than ten patients mentioned that aspect, “some” if five to ten when patients mentioned the topic and “few” when less than five patients expressed this opinion.
Results
We conducted two focus group interviews. A total of seventeen patients participated in these two group interviews. Their characteristics are presented in Table 1. All participants had AT (n = 14) and/or type 2 DM (n = 4; n = 3 participants had both conditions). Thematic analysis of focus group transcripts revealed four main themes regarding patients’ attitudes towards PN-led consultations and PN-led DCPM: 1) Openness and perceived benefits, 2) reservations and perceived risks, 3) reasons for encounters acceptable for PN-led care, 4) general requirements and perceived benefits. We describe each theme below, stratifying themes related to PN-led care and PN-led DCPM only where differences in themes or sub-themes occur. Additional supporting quotes for all themes beyond those presented in the results section can be found in Table A2.
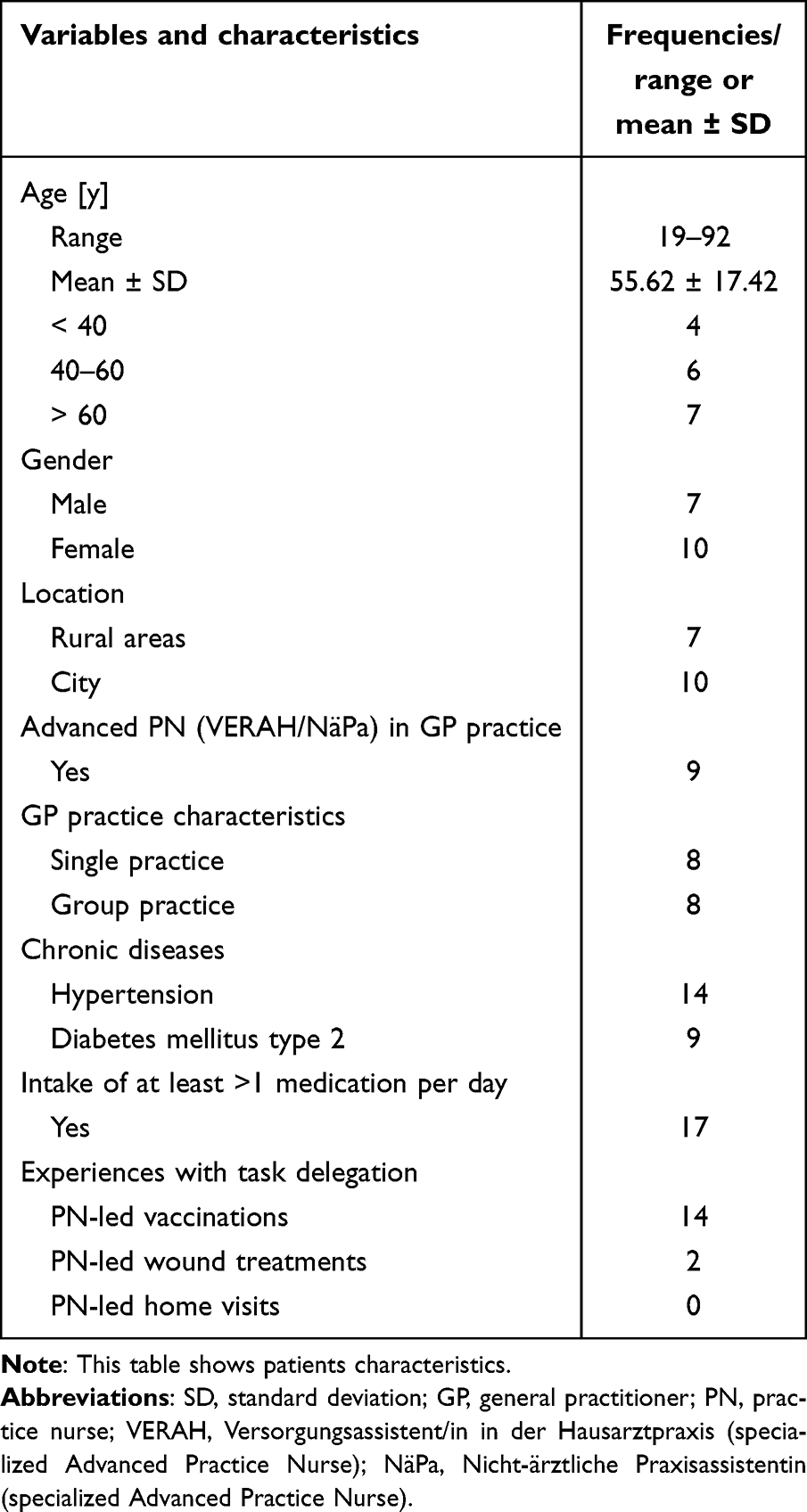 |
Table 1 Patient Characteristics |
Openness to PN-Led Care and Perceived Benefits
Many patients showed a general openness to a consultation led by a PN and some patients were open to PN-led DCPM.
New Care Concepts are Perceived as Important
For those who were generally open to the concept of PN-led care, patients explained that they were open, because they felt that new care concepts were important and necessary due to the difficult care situation in rural areas. They emphasised that PN-led care or aspects of it would be of great benefit in these circumstances.
In the city you always have the possibility to go to the GP or the GP comes to you, but in the countryside that’s not the case and I see that as a big advantage [of the concept of PN-led care][…]. (Patient P3)
Patients’ Trust in PN’s Skills
Participants mentioned that trust in healthcare providers played an important role in their openness to PN-led care. Some patients stated that they had a fundamental trust in their PN’s current skills and could therefore unreservedly see themselves being consulted by their PN:
I can see myself doing that very well, so I also have a lot of trust in my practice, the girls there are totally fit and experienced […], uh so I trust them even more than the doctor in some points. (Patient P4)
In addition, some participants felt that PNs already have a lot of knowledge but are currently not supported enough. They were open to PN-led consultations, because they felt that PNs should be given more trust and responsibility. Few respondents emphasised that PNs should be encouraged to work more independently. Many patients also expressed a positive attitude towards a PN-led DCPM:
Er, to change the dose of […] the medication that I am already taking, I wouldn’t have any concerns about that at all. (Patient P2)
Patients Perceive PN-Led Care as Beneficial
Many patients stated that they were open towards PN-led care, because they perceived this concept as beneficial.
Lower Barrier to Contact Practice Team
As an example for benefits of a PN-led care, patients named a lower barrier for contacting their GPc. They perceived that with PN-led care the number of medical experts to contact for their complaints would increase and they would feel encouraged to contact their GP team earlier. Therefore, many patients concluded that they would receive faster treatment:
In my experience, you can get to the nurse faster than to the doctor. There would be a quicker way to get an appointment for minor medical issues. (Patient P1)
Better Communication Due to PN-Led Care
Patients felt that PN-led care would increase social satisfaction due to better communication during PN-led consultation. Few stated that they or other patients might feel better understood and better listened to. One respondent pointed out that this could be a relief, especially for chronically ill patients, as their concerns might be better addressed:
[…] In other words, the nurse could take away his worries and would have more time for this patient group […] (Patient P12)
Better Compliance Through PN-Led Care
One patient stated that PN-led care would improve patient compliance, especially with medication. In addition, this respondent felt that PN-led care and communication with the PN, would better motivate the patient to make lifestyle changes. The interviewee perceived that this could also lead to better medication adherence for patients in PN-led care:
[...] because the patient takes his tablets and is motivated to change his diet etc. by talking to the PN. [...] (Patient P8)
Time Relief for the GP
Many participants stated that PN-led care could save their GPs time and a few stated that their GP might have more time to deal with complex cases:
In this context, I think this it could be a big relief for the GP, who would then have more time for special diseases and would be more available (Patient P15)
Benefits to the Healthcare System
In addition, participants described benefits to the PN and GP workflow and to the healthcare system. Many patients concluded that PN-led consultations and PN-led DCPMs could be cheaper than GP consultations and could lead to lower healthcare costs. One patient highlighted that health care costs would be reduced due to the perceived higher quality of care provided by PN-led care.
Improving the Image of the PN Profession
Patients expressed that the PN-led consultation and DCPM would enhance the skills of PNs. Some respondents felt that this would lead to greater respect and acceptance of PNs by patients and other health care professionals, and therefore an improved image of the professional role of a PN. Patients felt that PN-led care had the potential to develop a new job profile. Furthermore, some patients indicated that this could lead to an increase in a PN’s salary.
Reservations and Perceived Risks
Patients discussed various reservations and risks when considering about PN-led patient consultation and PN-led DCPM.
Lack of PN’s Qualification and Fear of Treatment Errors
Two patients were completely opposed to the concept of PN-led care. They could not see themselves attending a PN-led consultation, because they felt that the PN was not sufficiently qualified to deal with their medical problems. Few patients could not imagine receiving medication advice from a qualified PN:
And uh like I said, I don’t see how I can let the nurse mess around with my medication. (Patient P11)
Two patients were concerned that this could also lead to treatment errors. Furthermore, few patients felt that PNs might overestimate their own skills and exceed their competence.
Lack of Information/Uncertainty
Despite their openness to PN-led consultations, few patients felt that there was a lack of clarity about how PN-led care might develop, which made them reluctant to accept the concept. However, they did make suggestions on how to address this uncertainty and to increase patient’s acceptance. For example: proof of qualification, medication guidelines predefined by the GP that the PN can use to change medication doses and continued regular contact with the GP. They underlined that a discussion with their GP would help them to clarify their questions.
Risks for the PN
Some interviewees pointed out that the PNs may be overburdened with their new tasks, both professionally and organizationally. Some interviewees also felt that there may not be enough practice staff available to cover this approach. One patient said that the PN would have to perform more tasks but might still get paid the same.
Higher Threshold for GP-Patient Consultation
Some patients expressed concern that other patients may find it difficult to tell their PN that they prefer a GP-led consultation. Some patients felt that other patients might then stop attending GP’s surgery. Some patients also feared that PN-led care might lead to less frequent GP-patient consultations and therefore to patient dissatisfaction:
For me personally, I don’t see any risks, but in general, I could imagine that a patient might feel under pressure to tell everything […] i.e. to the PN. That he might not feel safe and might have [the] impression that he is being pushed into a second-class treatment. (Patient P2)
Risks to the Healthcare System
One patient was concerned that PN-led care could lead to fewer GPs in the future:
[...] What will happen in ten years? Maybe there will be fewer GP’s surgeries, but more PNs, and we will have even fewer GPs. [...] That’s the risk. (Patient P5)
Two patients emphasised that the time advantage of PN-led care for the GP would be quickly cancelled out by, among other things, the increased time needed for supervision of practice staff (Table A2). They also felt that the concept of PN-led care involved additional coordination tasks, which would then lead to an increased workload for the practice team. One patient had doubts about the concept because she already perceived a high workload for his/her PN. Therefore, he/she she had doubts about the feasibility of this concept in everyday practice. Few patients wondered what would happen to practice staff who did not have additional qualifications and whether this would lead to tensions in the practice staff team:
[…] What happens to those [PN] who, as I said, don’t have the opportunity [to qualify] due to whatever circumstances and stay or are at that lower level? Um, how are they [PN] perceived from the outside? (Patient P13)
Doubts About the Need and Real Benefits for the Healthcare System
Few participants had reservations about PN-led care, because they doubted that there would be a real benefit for patient care, or that there was a real need in everyday practice for PN-led care. Few saw the economic interests of health insurance companies as the driving force for PN-led care, which underlined their reservations.
Change of Medication as a GP’s Issue
A few patients were generally sceptical about changing the DCPM through PN, stating that they did not find the concept acceptable:
But really, medication […] is a doctor’s issue for me. (Patient P4)
Reasons for Encounters Where Patients are Likely to Accept PN-Led Care
Figure 1 shows the reasons for encounters where patients would accept PN-led care. Many patients reported that PN-led care would be acceptable for DMT2/antidiabetic medications, AT/antihypertensive medications, thyroid conditions such as hypothyroidism and related medications, and seasonal upper respiratory and gastrointestinal infections (Table A2). Many patients felt that a PN-led consultation would be particularly beneficial in the management of chronic diseases, provided that the chronic disease remains stable and no major changes occur. As possible indication for PN-led care in this context, participants felt that regular consultations with time and space to talk were appropriate. In addition, some patients felt that PN-related dose changes could go beyond long-term medication. These participants considered antibiotics and medications for seasonal infectious diseases, as well as for back pain, to be amenable to PN-guided DCPM (Table A2).
 |
Figure 1 Reasons for encounters and medications for which patients reported openness to accept PN-led care. Abbreviation: PN, practice nurse. |
Reasons for Encounters Where Patients are Unlikely to Accept PN-Led Care
There were a few conditions for which some patients could not imagine consulting a PN or receiving medication advice from a PN. These included diagnoses that some patients felt were rare, complex or novel. As examples of complex conditions, many patients mentioned heart disease, genetic disorders, acquired immunodeficiency syndrome, cancer and mental health conditions.
Some participants were more cautious about the range of illnesses which they considered as serious. They generally defined serious illnesses as those affecting internal organs.
General Requirements for the Implementation of PN-Led Consultations and PN-Led DCPM
Participants discussed several different requirements that they considered important for the implementation of PN-led consultations or PN-led DCPM (Figure 2 and Table A3). In short, they valued the adequate training of the PN and the supervision of the PN’s work by the GP. For many participants, acceptability of PN-led medication advice for DCPM depended on the condition being treated and the number of different medications the patients were taking (Figure 2). Many participants emphasised the importance of an appropriately organized practice when PN-led care is provided, and some explained their views on risk reduction strategies (Tables A2 and A3).
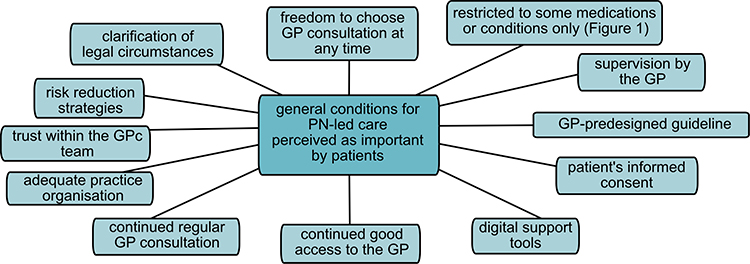 |
Figure 2 Patient’s perspective on general requirements for implementation of PN-led consultation and PN-led DCPM. Abbreviations: GP, general practitioner; PN, practice nurse; DCPM, dosage adjustments for permanent medication. |
Discussion
In this study, we investigated the perspectives of patients with DMT2 and/or AT on PN-led patient consultation and PN-led DCPM for chronically ill patients. To the best of our knowledge, this is the first qualitative study focusing on PN-led DCPM, general requirements as well as risks and benefits for both PN-led consultation and PN-led DCPM in German GPc. To address the current challenges of GPc in Germany, the implementation of PN-led care in GPc may be one solution. To support this implementation, our study adds the important aspect of the patient’s perspective.
Summary of Main Findings
In this study, many patients expressed a general openness to PN-led care, but some had reservations. Interviewees perceived many benefits: PN-led care would better meet patients’ needs better than GP-care and increase their compliance. Many patients were open to PN-led care, but only under certain conditions, eg extended training of PNs, proof of specialised certifications and a guideline for medication changes predefined by the GP. Some participants rejected the concept of PN-led care and/or expressed reservations because of perceived risks, eg treatment errors due to insufficient knowledge of the PN, or their fear of not seeing their GP often enough. Study patients saw a wide range of reasons for acceptable encounters for PN-led care, and specifically mentioned reasons for encounters for DMT2, AT, thyroid diseases, upper respiratory and gastrointestinal infections for both PN-led consultations and PN-led DCPM. From the perspective of our study patients, the most important requirements for achieving patient acceptance in the implementation of PN-led care in GPc were the patients’ informed consent to PN-led care. Also, the possibility to consult the GP at the patient’s request, adequate training of the PN and regular supervision by the GP. Therefore, this study adds important aspects to the existing literature for further research on PN-led care in German GPc and gives valuable information for practice implementation of PN-led care to reach a good patient acceptance.
Comparison to Other Studies
Available international studies on PN-led DCPM have focused on the patient’s perspective in relation to PN-led prescription only.14,16–20 Although this limits the comparability of our results, similar patient perspectives are evident, as described further below. In particular, international studies on PN-led care were conducted when the concept had been formally implemented into the health care system and patients gained experience with PN-led care. In contrast, our study dealt with a scenario that is still in the future for most German GP patients. Currently, PN-led dose modification of permanent medication is not legally allowed in Germany and PN-led consultations are legally allowed for “minor reasons for encounters”, but are rarely used.
Consistent with our findings, international surveys and qualitative studies have shown a general openness to PN-led consultations.1,17 The international literature highlights a general openness to PN-led DCPM,21–23 whereas only some patients in our study were open to PN-led DCPM.
As in our study, the international literature has shown that patient trust in the PN, but also in the GP, is important for openness to PN-led care.14,17,20,24 In line with these findings, patients in the UK placed more importance on trusting their long-term healthcare provider teams than on which professional (GP or PN) actually provided the consultation or gave medication advice.21 Our data showed that patients’ trust also stemmed from experiencing PNs as competent members and experts of the GPc team, an issue which was also highlighted by two British studies.14,18 Patients’ perceived benefits were another important motive for openness to PN-led care, both in our study patients and in international studies. Faster access to health care through PN-led care was frequently mentioned by our study patients and is consistent with views of Scottish patients, who felt that faster access to effective care was more important than the qualifications of the care provider.17 Patients perceive PNs as more accessible than the GPs. They consider PN-led care to be time-saving, both in our data and in the international literature.16–18 In addition, our study sample perceived that PN-led consultation would provide better patient education, better background information, and a better focus on patients’ worries and needs, which motivated them to be open to PN-led care. These motives are also supported by international studies.16–18
As a general requirement for acceptance of PN-led care, our study patients most frequently mentioned good training of PNs, including regular training after graduation. This is also shown by two British studies.18,21 Inadequate training of PNs was perceived as a risk by some interviewees in our study. This is consistent with the existing literature, where patients’ fear of potential limitations in PN training is a known pattern.14 Fear of inadequate training may be the underlying pattern why some patients in our sample felt more comfortable receiving PN-led care, if they had evidence of qualification, eg a certificate of graduation. Regular supervision of PNs by GPs was one of the most frequently mentioned general requirements for implementing PN-led care in our study and in international literature.14,21 Interestingly, other studies showed that patients did not mind waiting for supervision to take place for a change of medical advice or prescriptions, respectively, if a model with immediate supervision was chosen.21 Furthermore, our study patients highlighted that it was very important to be able to see a doctor if they felt uncomfortable with PN-led care. This could indicate that patients are open to new care concepts, but still wish to maintain influence over their own healthcare and the right to choose the kind of healthcare provider. This aspect was not explicitly described in previous literature. This may be due to differences in health system structures. In Germany patients can choose their physician freely, but in other healthcare systems as in UK, where patients have to see their GP first and cannot change GPs easily.
Our data showed that patients are open to PN-led care for a variety of reasons for encounters including chronic illnesses such as DMT2, AT and others. This study about PN-led care is the first to contain a wide variety of reasons for encounter. This is the first study, to our best knowledge, to do so in this breadth. General openness for reasons for encounter for any chronic condition was also examined by Jedro et al and showed a moderate acceptance rate but was not studied in detail.1 As in other studies,21,22,25 we could show that patients preferred GP-led consultation over consulting PNs, if they perceive their reason for encounter as a severe illness, where patients perceived a higher level of knowledge in doctors.25 In accordance with international studies,22,24 in our study patients perceived that starting a new medication, complicated or psychiatric diseases was not an issue for PN-led care.
A few patients expressed a general uncertainty and unfamiliarity regarding PN-led role in the consultation and medication advice in our study sample. This is unsurprising, as PN-led consultations are not broadly available, and PN-led DCPM is not currently available in GPc. Surprisingly, patients seem to experience uncertainties about a PN’s role even decades after implementation of PN-led care.18 As international literature17,18,21–23,26 shows, heterogenous results occur concerning how well patients understand a PNs role and responsibilities, eg what exactly would their tasks and responsibilities be.
Strengths and Limitations
This is the first study to focus on the patients’ perspective of PN-led DCPM and one of the few studies investigating patients’ perspectives on PN-led consultations in GPc in Germany. Our study provides a wide range of perspectives on issues that have not been explored as thoroughly in previous studies, such as acceptable medications for PN-led DCPM and requirements that would facilitate patients’ acceptance of the implementation of PN-led care in GPc. The qualitative focus group approach of our study allowed us to capture a wide range of attitudes and explore hidden motives, chances, reservations and concepts, which would not be possible in a quantitative approach. Patients are their own experts for how they want their care to be delivered.27 Our study focused on the views of chronically ill patients with DMT2 and AT, a highly prevalent patient group with extensive experience of care in GPc.27–31 They can add the perspective of chronically ill patients to the concept of PN-led care. This is important for further research projects, as the preferences of potential target groups can be decisive for the study design of future pilot projects.
Although the criterion of theoretical saturation has been reached, our study sample is not representative due to the qualitative design. This limits the generalisability and transferability of our results. However, the advantages of the open setting of the focus groups in our study allowed for group interactions, reflection and an exclusive access to the specific knowledge and attitudes of the patients, which would have not been possible in a quantitative or one-on-one interview only study setting. Nevertheless, the group setting could pronounce less detailed or socially desirable responses from participating patients, when some may have felt inhibited in contributing and narrating their attitudes. However, the interviewing research team made every effort to keep the discussion as open as possible. We cannot rule out selection bias, as GPs were involved in the selection of patients, and we had to conduct online focus groups due to contact restrictions during the COVID-19 pandemic. However, we attempted to minimise selection bias by using a pre-designed qualitative sampling plan, which included a wide range of variables. We originally planned to have eight participants per focus group. Due to technical difficulties, two participants had to leave the first focus group, and one participant did turn up for the interview. Three participants were then added to the second focus group.
Conclusion
Our data shows promising results for patients' openness to the concept of PN-led patient consultation and PN-led DCPM in Germany. It shows that patients with DMT2 and AT would accept a variety of reasons for encounters with PN-led care, eg PN-led treatment of DMT2, AT, thyroid diseases and seasonal infections. The implementation of PN-led care should take into account adequate training of the PN, regular supervision by the GP, patients' informed consent and the freedom to see a GP at any time. These requirements seem to be important to increase patients’ acceptance of PN-led care. To quantify the percentage of patients who would accept or refuse PN-led DCPM, quantitative studies taking into account our qualitative study results are needed in the future. These studies should also investigate how many patients would be open to which reasons for encounter. Furthermore, the perspectives of PNs and GPs towards PN-led care should be explored. This may help in the implementation of pilot projects to ensure the reliability of primary care in rural areas.
Acknowledgments
We thank all our participating patients for their time and valuable input. We are thankful to all cooperating GPs and their practice teams. This study was funded by the Foundation for Perspectives in General Practice and supported by the General Practitioners' Association Saxony-Anhalt.
Disclosure
Dr Solveig Weise reports grants from Foundation for Perspectives in General Practice, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Jedro C, Holmberg C, Tille F, et al. The acceptability of task-shifting from doctors to allied health professionals—results from a representative telephone survey of members of the National Association of Statutory Health Insurance Physicians. Dtsch Arztebl Int. 2020;117:583–590. doi:10.3238/arztebl.2020.0583
2. Taylor MT, Wayne TD, Burrows K, Cunnington J, Lombardi A, Liou M. Qualitative study of employment of physician assistants by physicians: benefits and barriers in the Ontario health care system. Can Fam Physician. 2013;59:e507–513.
3. Lindblad E, Hallman E-B, Gillsjö C, Lindblad U, Fagerström L. Experiences of the new role of advanced practice nurses in Swedish primary health care—DASH not long? A qualitative study. Int J Nurs Pract. 2010;16(1):69–74. doi:10.1111/j.1440-172X.2009.01810.x
4. Weeks G, George J, Maclure K, Stewart D. Non-medical prescribing versus medical prescribing for acute and chronic disease management in primary and secondary care. Cochrane Database Syst Rev. 2016;11:CD011227. doi:10.1002/14651858.CD011227.pub2
5. Laurant M, van der Biezen M, Wijers N, Watananirun K, Kontopantelis E, van Vught AJ. Nurses as substitutes for doctors in primary care. Cochrane Database Syst Rev. 2018;7:CD001271. doi:10.1002/14651858.CD001271.pub3
6. Delamaire M, Lafortune G. Nurses in advanced roles: a description and evaluation of experiences in 12 developed countries. In: OECD Health Working Papers. OECD Publishing; 2010:54. doi:10.1787/5kmbrcfms5g7-en
7. Freund T, Everett C, Griffiths P, Hudon C, Naccarella L, Laurant M. Skill mix, roles and remuneration in the primary care workforce: who are the healthcare professionals in the primary care teams across the world? Int J Nurs Stud. 2015;52(3):727–743. doi:10.1016/j.ijnurstu.2014.11.014
8. Maier CB, Aiken LH. Task shifting from physicians to nurses in primary care in 39 countries: a cross-country comparative study. Eur J Public Health. 2016;26(6):927–934. doi:10.1093/eurpub/ckw098
9. Carmienke S, Freitag MH, Gensichen J, Schmidt K. Allgemeinmedizin in Dänemark: bericht von einem Hippokrates Austausch. Zeitschrift für Allgemeinmedizin. 2014;90(1):44–47.
10. Mergenthal K, Beyer M, Gerlach FM, Guethlin C. Sharing responsibilities within the general practice team - a cross-sectional study of task delegation in Germany. PLoS One. 2016;11(6):e0157248. doi:10.1371/journal.pone.0157248
11. Dini L, Gisbert Miralles J, Heintze C. Delegation in der Hausarztpraxis: Ergebnisse einer Befragung von Hausärztinnen und Hausärzten in Nordrhein-Westfalen. Bochum: Landeszentrum Gesundheit; 2018.
12. Dini L, Sarganas G, Boostrom E, Ogawa S, Heintze C, Braun V. German GPs’ willingness to expand roles of physician assistants: a regional survey of perceptions and informal practices influencing uptake of health reforms in primary health care. Fam Pract. 2012;29(4):448–454. doi:10.1093/fampra/cmr12
13. Mergenthal K, Guthlin C, Beyer M, Gerlach FM, Siebenhofer A. Wie bewerten und akzeptieren Patienten die Betreuung durch Medizinische Fachangestellte in der Hausarztpraxis? Ergebnisse einer Patienten-Befragung in der HzV in Baden-Württemberg [How do patients evaluate and accept the care provided by medical assistants in the GP practice? Results of a patient survey in General Practitioner Centered Care in Baden-Württemberg]. Gesundheitswesen. 2018;80(12):1077–1083. German. doi:10.1055/s-0042-110402
14. Courtenay M, Stenner K, Carey N. The views of patients with diabetes about nurse prescribing. Diabet Med. 2010;27(9):1049–1054. doi:10.1111/j.1464-5491.2010.03051.x
15. Kiger ME, Varpio L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med Teach2020, 42(8):846–854. 10.1080/0142159X.2020.1755030
16. Barratt TN, Thomas N. Nurse practitioner consultations in primary health care: patient, carer, and nurse practitioner qualitative interpretations of communication processes. Prim Health Care Res Dev. 2019;20(42):1–9. doi:10.1017/S1463423618000798
17. Coull A, Murray I, Turner-Halliday F, Watterson A. The expansion of nurse prescribing in Scotland: an evaluation. Br J Community Nurs. 2018;18(5):234–242. doi:10.12968/bjcn.2013.18.5.234
18. Brooks N, Otway C, Rashid C, Kilty E, Maggs C. The patient’s view: the benefits and limitations of nurse prescribing. Br J Community Nurs. 2001;6(7):342–348. doi:10.12968/bjcn.2001.6.7.7066
19. Stenner KL, Courtenay M, Carey N. Consultations between nurse prescribers and patients with diabetes in primary care: A qualitative study of patient views. International Journal of Nursing Studies. 2011;48(1):37–46. doi:10.1016/j.ijnurstu.2010.06.006
20. Dhalivaal J. Patients’ perspectives on prescribing by nurses in general practice. 2022.
21. Halter M, Drennan VM, Joly LM, Gabe J, Gage H, de Lusignan S. Patients’ experiences of consultations with physician associates in primary care in England: a qualitative study. Health Expect. 2017;20(5):1011–1019. doi:10.1111/hex.12542
22. Schönenberger N, Sottas B, Merlo C, Essig S, Gysin S. Patients’ experiences with the advanced practice nurse role in Swiss family practices: a qualitative study. BMC Nursing. 2020;19(1). doi:10.1186/s12912-020-00482-2
23. Nørøxe KB, Moth G, Maindal HT, Vedsted P. Could the patient have been seen by a nurse; a questionnaire based survey of GP and patient views in Danish general practice. BMC Fam Pract. 2013;14:171. doi:10.1186/1471-2296-14-171
24. Ben Natan M, Kabaha A, Jackob N, Atallah R, Sharon I. The attitudes of patients with chronic conditions towards nurse prescribing medications. Int Nurs Rev. 2013;60(4):469–476. doi:10.1111/inr.12043
25. Redsell S, Stokes T, Jackson C, Hastings A, Baker R. Patients’ accounts of the differences in nurses’ and general practitioners’ roles in primary care. J Adv Nurs. 2007;57(2):172–180. doi:10.1111/j.1365-2648.2006.04085.x
26. van der Biezen M, Derckx E, Wensing M, Laurant M. Factors influencing decisions of general practitioners and managers to train and employ a nurse practitioner or physician assistant in primary care: a qualitative study. BMC Fam Pract. 2017;18(6):1–10. doi:10.1186/s12875-017-0587-3
27. Kennedy I. Patients are experts in their own field. BMJ. 2003;326(7402):1276–1277. doi:10.1136/bmj.326.7402.1276
28. Neuhauser H, Diederichs C, Boeing H, et al. Hypertension in Germany. Dtsch Arztebl Int. 2016;113(48):809–815. doi:10.3238/arztebl.2016.0809
29. International Diabetes Federation. IDF Diabetes Atlas.
30. Woo BFY, Lee JXY, Tam WWS. The impact of the advanced practice nursing role on quality of care, clinical outcomes, patient satisfaction, and cost in the emergency and critical care settings: a systematic review. Human Resources for Health. 2017;15(1). doi:10.1186/s12960-017-0237-9
31. Mirhoseiny S, Geelvink T, Martin S, Vollmar HC, Stock S, Redaelli M. Does task delegation to non-physician health professionals improve quality of diabetes care? Results of a scoping review. PLoS One. 2019;14(10):e0223159. doi:10.1371/journal.pone.0223159
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.