")
Back to Journals » Hepatic Medicine: Evidence and Research » Volume 13
Approaches to the Diagnosis of Portal Hypertension: Non-Invasive or Invasive Tests?
Authors Dajti E, Alemanni LV, Marasco G, Montagnani M, Azzaroli F
Received 27 December 2020
Accepted for publication 19 February 2021
Published 18 March 2021 Volume 2021:13 Pages 25—36
DOI https://doi.org/10.2147/HMER.S278077
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Elton Dajti,1,2 Luigina Vanessa Alemanni,1,2 Giovanni Marasco,1,2 Marco Montagnani,1,2 Francesco Azzaroli1,2
1IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy; 2Department of Medical and Surgical Sciences (DIMEC), University of Bologna, Bologna, Italy
Correspondence: Francesco Azzaroli
IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy
Email [email protected]
Abstract: Portal hypertension is the main driver of complications in patients with advanced chronic liver disease (ACLD) and is defined by values of hepatic venous pressure gradient measurement (HVPG) > 5 mmHg. Values of HVPG ≥ 10 mmHg determine the presence of clinically significant portal hypertension (CSPH), the main predictor of the risk of variceal bleeding, hepatic decompensation, and mortality. However, its measurement is invasive and requires high expertise, so its routine use outside third level centers or clinical trials is limited. In the last decades, several non-invasive tests (NITs) have been developed and validated for the diagnosis of portal hypertension. Among these, liver (LSM) and spleen stiffness measurement (SSM) are the most promising tools available, as they have been proven accurate to predict CSPH, high-risk esophageal varices, decompensation, and mortality in patients with ACLD. In the last Baveno VI Consensus proceedings, LSM evaluation was recommended for the first time for diagnosis of CSPH (LSM > 20-25 kPa) and the screening of patients with a low probability of having high-risk varices (LSM < 20 kPa and platelet count > 150.000/mm3). In this review, we aimed to summarize the growing evidence supporting the use of non-invasive tests for the evaluation of portal hypertension in patients with chronic liver disease.
Keywords: liver stiffness, spleen stiffness, portal hypertension, hepatic venous pressure gradient, liver cirrhosis
Introduction
Liver cirrhosis is a major cause of morbidity and mortality worldwide and is associated with increasing health burden and costs.1 It is a very heterogeneous and dynamic condition, and at least two distinct stages should be recognized: compensated and decompensated cirrhosis.2 Decompensation includes the development of clinical events such as ascites, variceal bleeding, hepatic encephalopathy, or hepato-renal syndrome, and it is associated with a significant decrease in patient survival.3 Cirrhosis in the compensated phase, on the other hand, is associated with an up to 80% 5-year survival rate; it can be further classified according to the degree of portal hypertension, as evaluated by its gold standard,4 the hepatic venous pressure gradient (HVPG), in compensated cirrhosis without portal hypertension (HVPG <5 mmHg), with mild portal hypertension (HVPG >5 mmHg, but <10 mmHg), or clinically significant portal hypertension (CSPH, and HVPG ≥10).5 The development of CPSH is an important hallmark in the natural history of liver cirrhosis and is associated with an increased risk of gastroesophageal varices, hepatic decompensation, hepatocellular carcinoma (HCC), and mortality.5
In this view, early identification of patients with compensated cirrhosis and risk stratification according to the severity of portal hypertension is of extreme importance for the hepatologist. In the last years, several non-invasive tests have been developed and validated for these purposes, with liver (LSM) and spleen stiffness measurement (SSM) being the most promising tools available.6 In the present paper, we aim to summarize the pros and cons and the evidence supporting the use of both invasive and non-invasive tests (NITs) in the diagnosis of portal hypertension.
Part I – Invasive Evaluation of Portal Hypertension: The Hepatic Venous Pressure Gradient
It is widely recognized that patients with compensated advanced chronic liver disease (ACLD) may progress to decompensation at a rate of about 5–7% per year.7 The leading cause of decompensation is the development of portal hypertension and its complications such as variceal bleeding, hepatic encephalopathy, and ascites, thus impacting on overall patient mortality rate.8
The gold standard method used for the evaluation of portal hypertension is the measurement of HVPG, which has been widely validated also as a prognostic factor.9 Portal hypertension is defined by HVPG values> 5 mmHg; HVPG ≥10 mmHg is associated with clinically significant portal hypertension (CSPH), which is an at-risk condition for decompensation, esophageal varices, and HCC development.4,5,10 Severe PH is defined by HVPG > 12 mmHg, whereas very severe PH by HVPG >16 mmHg; these conditions are both associated with a higher risk of variceal bleeding and mortality.4 Briefly, through venous access, a catheter is introduced into the right brachial vein or the right internal jugular vein until a branch of the hepatic veins is reached, usually the median or the right vein. Afterward, a balloon is inflated occluding all the vessels below, and then the measurement of wedged hepatic vein pressure is performed.11 Subsequently, after deflating the balloon at the tip of the catheter, the free hepatic vein pressure is measured.4,11
Non-selective beta-blockers (NSBB) represent the most common therapeutic choice for the primary and secondary prophylaxis of variceal bleeding.2 HVPG measurement is also employed for the prediction of acute and chronic hemodynamic response to NSBB therapy for high-risk varices (HRV).4 According to the Baveno VI consensus, the response to NSBB is defined as the reduction of HVPG ≥10% or ≤12 mmHg after treatment.12 Moreover, HVPG may be used to assess the hemodynamic response to NSBB to guide therapy for the prevention of variceal bleeding recurrence.13
Besides, recently, the PREDESCI trial14 showed that NSBB could significantly improve decompensation-free survival in patients with compensated cirrhosis and HVPG ≥10 mmHg, with criteria similar to those adopted for assessing hemodynamic response for HRV, since these patients were those who most benefited from NSBB. Regarding HVPG prospective evaluations, one of the main applications is related to the evaluation of patency and therapeutic effectiveness after transjugular intrahepatic portosystemic shunt (TIPS) placement, which is indicated in patients with decompensated portal hypertension.15
Interestingly, dynamic HVPG changes have been prospectively reported in other settings, such as in patients with hepatitis C virus (HCV)-associated cirrhosis treated with the new direct-acting antiviral agents (DAAs), showing that sustained virologic response (SVR) was associated with a significant reduction of HVPG when compared with that assessed before treatment, thus mirroring both hemodynamic and fibrotic changes occurring after treatment.16 Also, the portal hypertension degree influences the natural history of chronic liver diseases, leading to HCC.10 Previously, an HVPG value >10mmHg has been identified as independently associated with HCC occurrence.10,17,18
Finally, HVPG value has been associated with outcomes in patients with cirrhosis undergoing elective extrahepatic surgery, allowing an accurate patients risk stratification thus improving post-surgical outcomes.19 However, HVPG use is limited by its invasiveness and is available only in highly specialized centers; thus, in the last decade, several attempts have been made to find the ideal NIT able to replace HVPG.
Part II – Non-Invasive Evaluation of Portal Hypertension
The last decade has seen several efforts to develop tests that can replace invasive methods for the assessment of portal hypertension in patients with ACLD. Patients were routinely subjected to liver biopsies in order to establish the severity of fibrosis, and HVPG measurement is still considered the gold standard in portal hypertension evaluation.4 However, as mentioned above, these methods are invasive, not widely available, and risky for patients. Such limitations have led to the development and validation of new alternative NITs which have revolutionized the clinical approach to ACLD patients. The increasing need for NITs in patients with liver cirrhosis has also been recently highlighted by the guidelines of the European Society for the Study of the Liver (EASL).20
Novel elastographic techniques have got increasing attention through the years and today play a well-recognized role in liver disease assessment, as stated also by the last Baveno VI Consensus Workshop.2 Among ultrasound-based elastographic techniques, transient elastography (TE) is the first and the most validated method for LSM evaluation.21 Liver stiffness represents a surrogate marker of liver fibrosis; therefore, it is useful in diagnosing ACLD and its complications (Table 1). Being liver fibrosis a fundamental determinant of hepatic resistance to the portal blood flow,6 LSM application has been consequently extended to portal hypertension assessment and the prediction of esophageal varices (EV) with good results; in fact, LSM represents today a valuable non-invasive alternative to HVPG in clinical practice. One of the first pieces of evidence was produced by Carrión et al in 2006 in HCV-patients undergoing liver transplantation;22 LSM by TE technique showed a close correlation with HVPG and good accuracy (AUC=0.93) in diagnosing portal hypertension (defined as HVPG > 6 mmHg). It was followed by several studies aimed at establishing the optimal LS cut-off for portal hypertension diagnosis, obtaining controversial results. A recent meta-analysis still confirmed the good correlation between LSM and HVPG (r = 0.783).23
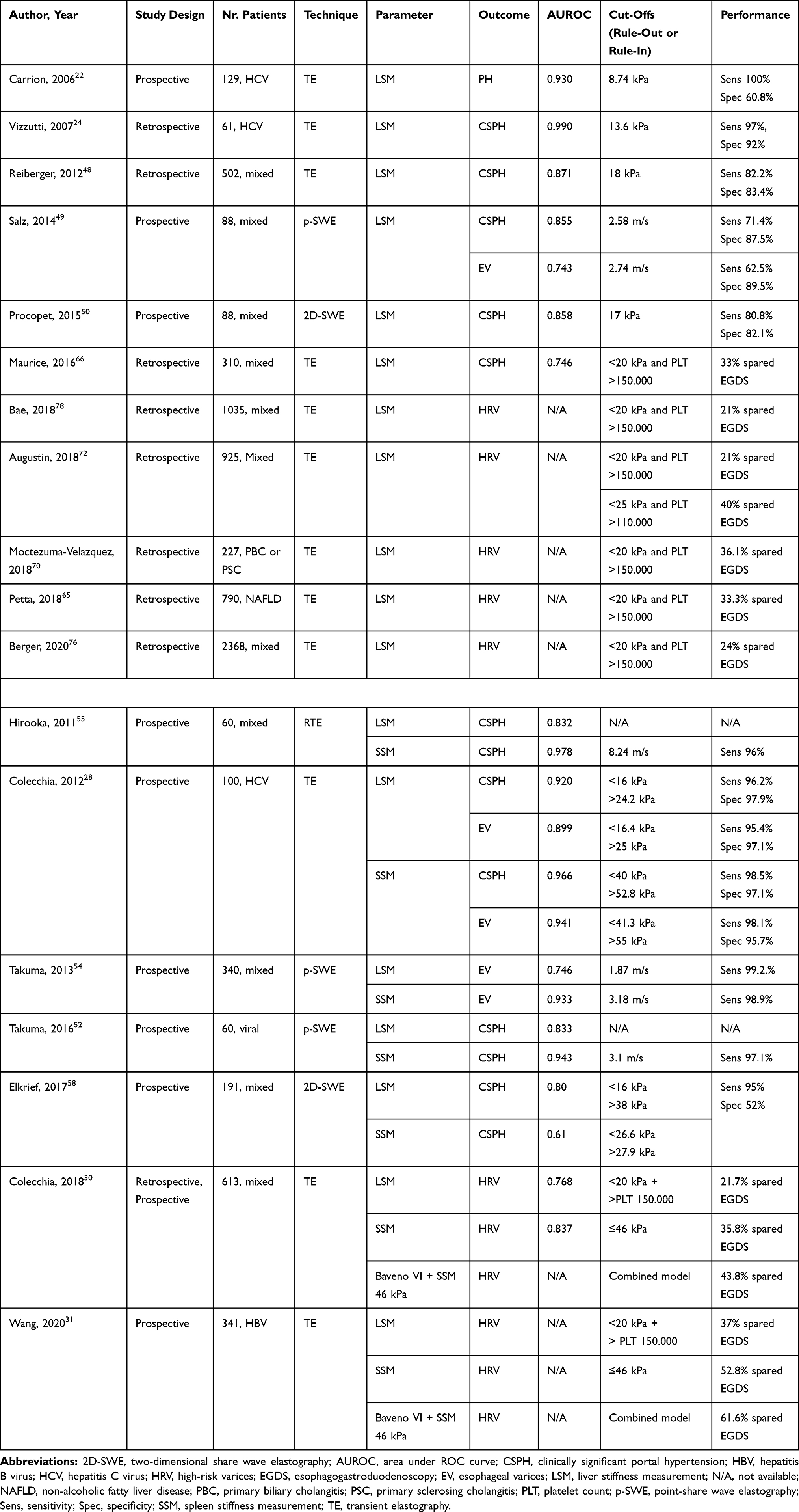 |
Table 1 Performance of Liver and Spleen Stiffness in the Diagnosis of CSPH and Gastroesophageal Varices |
However, Vizzutti et al reported that, while the correlation between LSM and HVPG values less than 10–12 mmHg was excellent (r = 0.81–0.91), it appeared to be poorer for higher HVPG values, with a non-optimal linear regression analysis (r2=0.35 for HVPG > 10 mmHg, r2=0.17 if > 12 mmHg).24 A possible explanation is that in an early phase portal hypertension is mainly linked to fibrotic modifications of liver parenchyma, but at later stages, it is determined by many hemodynamic changes driven, such as neoangiogenesis, hyperdynamic circulation, portosystemic collateral development, and splanchnic vasodilation,6 and these modifications are not captured by an indirect surrogate of portal hypertension, such as LSM.
More recently, increasing attention has been driven to the evaluation of SSM by elastosonography. It is today clear that splenomegaly does not simply reflect spleen congestion in ACLD patients, but it is determined also by structural changes and tissue hyperplasia due to fibrogenesis, angiogenesis, activation of lymphoid compartment.25–27 Consensually, SSM proved to have a strong correlation with the whole range of HVPG values, as shown in the seminal paper by Colecchia et al:28 SSM provided the strongest correlation with HVPG (r = 0.885), as compared to LSM. A recent meta-analysis confirmed the good correlation between SSM and HVPG.29 Therefore, SSM is considered today as a direct surrogate of portal hypertension that captures all of its physiopathological components, from early to the late cirrhotic stages. From a technical point of view, SSM values are obtained using the same probe used to perform LS, with the patient in a supine position with maximal abduction of the left arm and the probe positioned in an intercostal space where the spleen was correctly visualized by ultrasound. Since no specific reliability criteria have been developed for SSM, the same as those for LSM are generally applied; besides, SSM is not considered reliable if the splenic parenchymal thickness is <4 cm under the probe. The main limit of SSM is its feasibility since the rate of technical failure reported in current literature is highly variable (0–60%). However, in expert centers, this rate is usually <10%.30,31 Moreover, new devices including build-in ultrasound for spleen detection32 or fusion-methods,33 have been developed to improve SSM feasibility and accuracy in the prediction of portal hypertension.
Besides elastography techniques, several serum biomarkers and radiological scores have been developed to non-invasively detect liver fibrosis34 and portal hypertension.35–43 For instance, the aspartate aminotransferase (AST) to Platelet Ratio Index (APRI) and Fibrosis (FIB-4) Score showed an AUROC of was 0.728 and 0.710, respectively, for the prediction of large varices in a meta-analysis.44 Several studies evaluated also more direct surrogates of portal hypertension, such as von Willebrand factor39,40 or indocyanine green clearance45,46 showing more promising results. However, the modest correlation with HVGP47 and overall suboptimal performance of the above-mentioned readily available serum biomarkers, as well as the limited evidence and availability of other more direct biomarkers, hampers the routine use of such NITs for the detection of portal hypertension and its complications in everyday clinical practice.40
Liver and Spleen Stiffness for the Diagnosis of Clinically Significant Portal Hypertension
The identification of CSPH is fundamental in ACLD since it allows to identify the patients who are at increased risk of gastroesophageal varices, decompensation, HCC, and mortality.5 With the introduction of LSM in clinical practice, many attempts have been made to establish the best LSM values to rule-in and rule-out CSPH.24,48–50 In 2017, a meta-analysis confirmed the good performance of LS in predicting CSPH (AUC=0.921) for low cut-off values of 13.6–18 kPa.23 Another meta-analysis highlighted that an LSM value <13.6 kPa assessed by TE resulted valuable to rule-out CSPH with high sensitivity (>90-95%), while the cutoff value > 22 kPa provided the overall best performance and appeared to accurately confirm CSPH (specificity > 90–95%).51 The last Baveno VI Consensus Workshop of 2015 recommended the use of LSM in clinical practice, suggesting LSM values >15 kPa as highly suggestive of cACLD and ≥20-25 kPa as sufficient to rule-in CSPH, alone or combined to platelets count and spleen size in virus-related chronic liver disease.2
Being a direct surrogate of portal hypertension, SSM showed a strong correlation with the whole range of HVPG values.28 Colecchia et al28 proposed values of 40 kPa and 52.8 kPa to respectively rule-out (sensitivity 98.5%) and rule-in CSPH (specificity 97.1%). A recent meta-analysis reported for SSM by TE a good performance in diagnosing CSPH (AUC = 0.92) and severe PH (AUC = 0.87), with elevated sensitivity (respectively 88% and 92%) and specificity (84% and 79%).29
Among other elastographic techniques, promising results have been observed as well. LSM and SSM evaluated by Acoustic Radiation Force Impulse (ARFI)52–55 were able to diagnose HVPG ≥ 10 mmHg and HVPG ≥ 12 mmHg with similarly high diagnostic performance (LSM, AUC = 0.93 and 0.87, respectively; SSM, AUC = 0.97 and 0.95).56 Promising results were found for LSM assessed by 2-dimensional shear wave elastography (2D-SWE)57,58 or Magnetic Resonance Elastography (MRE) as well,59–61 even if further evidence to better identify the optimal cutoffs for CSPH and the best application fields is needed.
Liver and Spleen Stiffness for the Diagnosis of High-Risk Esophageal Varices
One of the most relevant applications of elastometry is the identification of patients with gastroesophageal varices. Patients with ACLD require routine endoscopic surveillance in order to identify esophageal varices needing treatment (VNT), reduce upper digestive bleeding incidence and mortality. LSM is considered to have high sensitivity, but medium/low specificity in predicting esophageal varices (EV) in several studies.62–66 A meta-analysis including about 3650 patients from 18 studies, showed that LSM has a sensitivity and a specificity of 87% and 53% for any varices, and 86% and 59% for VNT.67
Regarding SSM, Stefanescu et al68 analysed its performance in chronic hepatitis patients; among cirrhotic group population, SSM resulted higher in those with EV (63.69 vs 47.48 kPa), with the best cut-off to detect EV of 52.5 kPa. In 2012, Colecchia et al28 confirmed LSM and SSM as more accurate in predicting both CSPH and EV than other NITs; moreover, they proposed a new combined logistic model using together SSM and LSM to reduce indeterminate cases.
The last Baveno VI Consensus Workshop stated that in patients with ACLD, the prevalence of VNT in patients with LSM < 20 kPa and platelet count is >150×109/L is low (< 5%), and endoscopic surveillance can be safely avoided in these patients.2 Since the postulation of these criteria in 2015, many studies have validated their safety in clinical practice. In a recent meta-analysis by Stafylidou et al69 including about 9000 patients from 30 studies, Baveno VI criteria proved to have a sensitivity of 0.97 and a specificity of 0.32 in predicting EV. Moreover, since Baveno VI criteria are originally to be applied only in patients with viral chronic liver disease, several efforts have been made for their validation in other etiologies (ie metabolic liver disease,65 cholestatic liver disease,70 after HCV-eradication71).
Nevertheless, the number of spared upper endoscopies by the application of Baveno VI criteria is relatively low (15–25%), so different attempts have been made to modify these criteria and increase the rate of spared endoscopies. Augustin et al proposed to use LSM cutoff of 25 kPa and PLT > 110 x 109/L72 (the Expanded Baveno VI), sparing up to 40–60% of upper endoscopies, as confirmed also by other authors.73–75 However, a higher rate of missed EVs has been reported, often over the safe threshold of 5%.76–78 This was confirmed also by a recent meta-analysis,69 where the Expanded Baveno VI criteria showed superior specificity (51%) for HRV, but with an increased risk of missed HRVs (up to 10%).
More recently, a new combined model30 including Baveno VI criteria and SSM (cut-off ≤ 46 kPa, assessed by TE), proved to be efficient in increasing the number of spared endoscopies without raising the rate of missed HRV. In a large cohort of almost 500 patients, this algorithm allowed to safely increase the rate of spared endoscopies to 43.8% (2% of HRV missed), as compared to Baveno VI criteria alone (21.7%); the excellent performance was then confirmed in a prospective multicenter cohort. Importantly, this combined model has been recently validated in a large prospective cohort of virally suppressed HBV patients, producing excellent results in safely ruling-out HRV.31 Similar performances were observed when combining Baveno VI criteria with SSM assessed with Supersonic Shear Imaging.79
In conclusion, non-invasive elastographic techniques are promising tools for EV prediction, and their combination will allow us to avoid unnecessary upper endoscopy in a considerable number of ACLD patients. However, which are the best criteria to apply in clinical practice is still a matter of debate, and this topic will be hopefully addressed during the upcoming Baveno VII consensus.
Role of Elastography in the Prediction of Liver-Related Events and Response to Treatments
Prediction of Hepatic Decompensation and Mortality
Liver and spleen stiffness correlate well with HVPG measurement and can identify patients with CSPH; therefore, it has been hypothesized that they can also predict other complications driven by portal hypertension.80 A meta-analysis81 has shown that an increase of 1 kPa in LSM is associated with an increased risk of hepatic decompensation [Relative risk (RR), 1.07; 95% CI, 1.03–1.11] and mortality (RR, 1.22; 95% CI, 1.05–1.43). The proposed cut-offs for the prediction of risk of hepatic decompensation usually are >20-25 kPa,82–85 the cut-off to rule-in CSPH according to Baveno VI consensus.2 Interestingly, the accuracy of LSM (0.837) for the prediction of any decompensation was not inferior to that of HVPG (0.815).82 Since LSM cut-offs are influenced by liver etiology, numerous studies have demonstrated that LSM is an independent predictor of decompensation and other liver-related events also in large cohorts of non-alcoholic fatty liver disease (NAFLD),86,87 primary biliary cholangitis,88,89 primary sclerosing cholangitis90,91 and other etiologies.92
SSM has also been validated as an accurate NIT able to stratify for the risk of decompensation and overall mortality in ACLD patients.93–96 Colecchia et al93 showed that an SSM value of 54 kPa, evaluated by TE, could identify patients at lower risk of decompensation. Similarly, Takuma et al96 showed that SSM >3.25 and >3.43 m/s, evaluated by p-SWE, accurately predicted decompensation and mortality, respectively. Recently, the 54 kPa SSM cut-off was validated to predict decompensation after HCV eradication with direct-acting antivirals.97
In conclusion, LSM and SSM are well-validated surrogates of portal hypertension and can be used in everyday clinical practice as prognostic markers, able to stratify for the risk of decompensation and liver-related events.
Prediction of Outcomes in Patients with Hepatocellular Carcinoma
Studies with HVPG have shown that not only the degree of liver fibrosis but also that of portal hypertension can predict the risk of HCC development,10 confirming that key features of portal hypertension, such as hyperdynamic circulation, liver hypoxia, and splanchnic neoangiogenesis, play an important role in liver carcinogenesis.98,99 Similarly, LSM has been extensively shown as a valid NIT able to predict the risk of primary HCC,100 in different etiologies of liver disease87,101–103 and also after HCV eradication after DAA treatment.104 Jung et al previously reported that LSM could also predict late recurrence after liver surgery105,106 when liver disease severity is a major contributor to such complication.107 More recently, SSM was found to be the only independent predictor of late recurrence in a proof-of-concept study,108 confirming a major contribution of portal hypertension in liver carcinogenesis.
Portal hypertension is also a major determinant of morbidity and mortality in patients undergoing hepatic resection.109 Since CSPH is not to be considered an absolute contraindication to liver surgery,110,111 a correct stratification according to the severity of portal hypertension is mandatory in this context. LSM has been consistently shown to accurately predict the incidence of post-hepatectomy liver failure (PHLF)112–114 or overall complications after hepatectomy;115 interestingly, the accuracy of LSM was found not inferior to HVPG116 and superior to ICG-r15ʹ114 for this outcome. More recently, SSM has been proposed as a more accurate predictor of PHLF development,117,118 however, the number of patients included is limited and more studies are required.
Prediction of Response to Non-Selective Beta-Blockers
As mentioned above, both acute and chronic HVPG response to NSBB has been shown to correlate with a lower risk of variceal bleeding and medical prophylaxis failure.4 A similar benefit in responders was recently shown also for the prevention of the first decompensation event, mainly ascites, in the PREDESCI trial.14 With the broad administration of NSBB to all patients with CSPH, it would become even more timely and relevant to identify hemodynamical responders, the patients that truly benefit from this medical treatment, and to avoid exposure to significant adverse effects of NSBB, which are not uncommon, in non-responders. To date, no NIT has substituted HVPG in this context. Only recently a seminal paper by Kim et al119 developed and validated a model including SSM, evaluated by p-SWE, that could predict for the first time hemodynamic response with excellent accuracy (AUROC=0.848). A recent pilot study11 also demonstrated that ΔSSM after NSBB initiation, as evaluated by TE, showed excellent correlation with ΔHVPG (r= 0.784), and SSM reduction ≥10% predicted HVPG response with an AUROC of 0.973. These studies are truly preliminary, but SSM could be a very promising tool for the prediction of hemodynamic response and warrants further studies.
Prediction of Outcomes in Patients with Transjugular Intrahepatic Portosystemic Shunts
Patients with TIPS represent another setting in which monitoring with NITs can provide clinically relevant information. Firstly, an increase in LSM has been shown to correlate with systemic inflammation and independently predict mortality in patients undergoing TIPS placement;120 however, no or little correlation has been found between changes in LSM and portal pressure gradient before and after TIPS.121,122 On the other hand, ΔSSM significantly correlated with changes in portal pressure gradient after TIPS (r= 0.56–0.87),121–126 and an SSM increase during follow-up can accurately predict TIPS dysfunction (AUROC=0.81–0.87),121,124,125,127 suggesting that SSM could play a pivotal role in the non-invasive monitoring of TIPS patency and prediction of complications after its placement.
Limits of Liver and Spleen Elastography in the Prediction of Portal Hypertension and Its Complications
The evidence supporting the use of elastography in the prediction of fibrosis and portal hypertension is substantial so that its role is now recognized in numerous guidelines and these techniques are used routinely in the evaluation of patients with chronic liver disease. However, the limits of the studies supporting this role should be acknowledged, in order to be addressed and overcome by future research. The main limits of the above-mentioned papers are the retrospective nature and the inclusion of patients with mainly active viral hepatitis. Indeed, most of the studies were retrospective and lack of prospective validation in large multicenter cohorts. The selection of patients was not always adequate, as patients with previous decompensation were often included in these studies. Therefore, the prevalence of CSPH and high-risk varices was often higher than expected (ie 40–60% and 10–20%, respectively) and this clearly influenced the performance of the selected cut-offs of LSM and SSM. More importantly, most of the studies included patients either with active HCV infection or HBV infection. Despite some promising studies, it is uncertain to date whether the same cut-offs can be applied also in patients achieving SVR after DAA treatment or whether the performance of elastography is the same in this context. Moreover, NAFLD is quickly becoming the most prevalent cause of liver disease and indication to liver transplantation, so specific cut-offs for the prediction of CSPH, varices, and liver-related events are required for these patients. Cholestatic or autoimmune diseases, on the other hand, are far less frequent, and studies evaluating the predictive role for these outcomes in these specific etiologies are warranted. As for SSM, the substantial heterogeneity among the reported failure rates and the proposed cut-offs for add to the limitations of applicability of this method in everyday clinical practice.
Part III – Conclusions
The HVPG measurement is the gold standard for the evaluation of portal hypertension; however, its measurement is invasive and requires expertise, so the use in everyday clinical practice and outside third level centers is limited. In the last decade, substantial evidence supports the use of NITs, such as liver stiffness, to define CSPH and guide surveillance for varices requiring treatment in patients with ACLD. SSM has also shown excellent results in the evaluation of portal hypertension; therefore, its measurement is encouraged in all patients with cirrhosis. Future studies are needed to explore and validate the use of LSM combined with other NITs, especially SSM, to optimize the accuracy of CSPH diagnosis and increase the number of safely spared screening endoscopies. The use of SSM to monitor response to NSBB or TIPS and to predict complications after such treatments is promising and should be further explored by future prospective studies.
Funding
No grants or other financial support.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Sepanlou SG, Safiri S, Bisignano C, et al. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(3):245–266. doi:10.1016/S2468-1253(19)30349-8
2. de Franchis R, Baveno VI Faculty. Expanding consensus in portal hypertension: report of the Baveno VI Consensus Workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63(3):743–752. doi:10.1016/j.jhep.2015.05.022
3. Angeli P, Bernardi M, Villanueva C, et al. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460. doi:10.1016/j.jhep.2018.03.024
4. Bosch J, Abraldes JG, Berzigotti A, García-Pagan JC. The clinical use of HVPG measurements in chronic liver disease. Nat Rev Gastroenterol Hepatol. 2009;6(10):573–582. doi:10.1038/nrgastro.2009.149
5. Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the Study of Liver Diseases. 2017;65(1):310–335. doi:10.1002/hep.28906
6. Berzigotti A. Non invasive evaluation of portal hypertension using ultrasound elastography. J Hepatol. 2017;67(2):399–411. doi:10.1016/j.jhep.2017.02.003
7. D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44(1):217–231. doi:10.1016/j.jhep.2005.10.013
8. D’Amico G, Morabito A, D’Amico M, et al. New concepts on the clinical course and stratification of compensated and decompensated cirrhosis. Hepatol Int. 2018;12(Suppl 1):34–43. doi:10.1007/s12072-017-9808-z
9. Procopet B, Berzigotti A. Diagnosis of cirrhosis & portal hypertension: imaging, non-invasive markers of fibrosis & liver biopsy. Gastroenterol Rep. 2017;5(2):79–89. doi:10.1093/gastro/gox012
10. Ripoll C, Groszmann RJ, Garcia-Tsao G, et al. Hepatic venous pressure gradient predicts development of hepatocellular carcinoma independently of severity of cirrhosis. J Hepatol. 2009;50(5):923–928. doi:10.1016/j.jhep.2009.01.014
11. Marasco G, Dajti E, Ravaioli F, et al. Spleen stiffness measurement for assessing the response to β-blockers therapy for high-risk esophageal varices patients. Hepatol Int. 2020;14(5):850–857. doi:10.1007/s12072-020-10062-w
12. de Franchis R, Baveno VI Faculty. Expanding consensus in portal hypertension. J Hepatol. 2015;63(3):743–752. doi:10.1016/j.jhep.2015.05.022
13. González A, Augustin S, Pérez M, et al. Hemodynamic response - Guided therapy for prevention of variceal rebleeding: an uncontrolled pilot study. Hepatology. 2006;44(4):806–812. doi:10.1002/hep.21343
14. Villanueva C, Albillos A, Genescà J, et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2019;393(10181):1597–1608. doi:10.1016/S0140-6736(18)31875-0
15. B M, Manka P, Theysohn JM, et al. Spleen stiffness is positively correlated with HVPG and decreases significantly after TIPS implantation. Dig Liver Dis. 2018;50(1):54–60. doi:10.1016/j.dld.2017.09.138
16. Lens S, Alvarado E, Mariño Z, et al. Effects of All-oral anti-viral therapy on HVPG and systemic hemodynamics in patients with Hepatitis C Virus-associated Cirrhosis. Gastroenterology. 2017;153(5):1273–1283.e1. doi:10.1053/j.gastro.2017.07.016
17. Kim MY, Baik SK, Yea CJ, et al. Hepatic venous pressure gradient can predict the development of hepatocellular carcinoma and hyponatremia in decompensated alcoholic cirrhosis. Eur J Gastroenterol Hepatol. 2009;21(11):1241–1246. doi:10.1097/MEG.0b013e32832a21c1
18. Suk KT, Kim EJ, Kim DJ, et al. Prognostic significance of hemodynamic and clinical stages in the prediction of hepatocellular carcinoma. J Clin Gastroenterol. 2016;51(3):1. doi:10.1097/MCG.0000000000000671
19. Reverter E, Cirera I, Albillos A, et al. The prognostic role of hepatic venous pressure gradient in cirrhotic patients undergoing elective extrahepatic surgery. J Hepatol. 2019;71(5):942–950. doi:10.1016/j.jhep.2019.07.007
20. Latinoamericana A. EASL-ALEH Clinical Practice Guidelines: non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol. 2015;63(1):237–264. doi:10.1016/j.jhep.2015.04.006.
21. Sandrin L, Fourquet B, Hasquenoph J-M, et al. Transient elastography: a new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med Biol. 2003;29(12):1705–1713. doi:10.1016/j.ultrasmedbio.2003.07.001
22. Carrión JA, Navasa M, Bosch J, Bruguera M, Gilabert R, Forns X. Transient elastography for diagnosis of advanced fibrosis and portal hypertension in patients with hepatitis C recurrence after liver transplantation. Liver Transpl. 2006;12(12):1791–1798. doi:10.1002/lt.20857
23. You MW, Kim KW, Pyo J, et al. A meta-analysis for the diagnostic performance of transient elastography for clinically significant portal hypertension. Ultrasound Med Biol. 2017;43(1):59–68. doi:10.1016/j.ultrasmedbio.2016.07.025
24. Vizzutti F, Arena U, Romanelli RG, et al. Liver stiffness measurement predicts severe portal hypertension in patients with HCV-related cirrhosis. Hepatology. 2007;45(5):1290–1297. doi:10.1002/hep.21665
25. Berzigotti A, Zappoli P, Magalotti D, Tiani C, Rossi V, Zoli M. Spleen enlargement on follow-up evaluation: a noninvasive predictor of complications of portal hypertension in cirrhosis. Clin Gastroenterol Hepatol. 2008;6(10):1129–1134. doi:10.1016/j.cgh.2008.05.004
26. Mejias M, Garcia-Pras E, Gallego J, Mendez R, Bosch J, Fernandez M. Relevance of the mTOR signaling pathway in the pathophysiology of splenomegaly in rats with chronic portal hypertension. J Hepatol. 2010;52(4):529–539. doi:10.1016/j.jhep.2010.01.004
27. Kondo R, Kage M, Iijima H, et al. Pathological findings that contribute to tissue stiffness in the spleen of liver cirrhosis patients. Hepatol Res. 2018;48(12):1000–1007. doi:10.1111/hepr.13195
28. Colecchia A, Montrone L, Scaioli E, et al. Measurement of spleen stiffness to evaluate portal hypertension and the presence of esophageal varices in patients with HCV-related cirrhosis. Gastroenterology. 2012;143(3):646–654. doi:10.1053/j.gastro.2012.05.035
29. Song J, Huang J, Huang H, Liu S, Luo Y. Performance of spleen stiffness measurement in prediction of clinical significant portal hypertension: a meta-analysis. Clin Res Hepatol Gastroenterol. 2018;42(3):216–226. doi:10.1016/j.clinre.2017.11.002
30. Colecchia A, Ravaioli F, Marasco G, et al. A combined model based on spleen stiffness measurement and Baveno VI criteria to rule out high-risk varices in advanced chronic liver disease. J Hepatol. 2018;69(2):308–317. doi:10.1016/j.jhep.2018.04.023
31. Wang H, Wen B, Chang X, et al. Baveno VI criteria and spleen stiffness measurement rule out high-risk varices in virally suppressed HBV-related cirrhosis. J Hepatol. 2020. doi:10.1016/j.jhep.2020.09.034
32. Stefanescu H, Marasco G, Calès P, et al. A novel spleen-dedicated stiffness measurement by FibroScan® improves the screening of high-risk oesophageal varices. Liver Int off J Int Assoc Study Liver. 2020;40(1):175–185. doi:10.1111/liv.14228
33. Tanaka T, Hirooka M, Koizumi Y, et al. Development of a method for measuring spleen stiffness by transient elastography using a new device and ultrasound-fusion method. Lin W, ed. PLoS One. 2021;16(2):e0246315. doi:10.1371/journal.pone.0246315
34. Castera L, Chan HLY, Arrese M, et al. EASL-ALEH Clinical Practice Guidelines: non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol. 2015;63(1):237–264. doi:10.1016/j.jhep.2015.04.006
35. Giannini E, Botta F, et al. Platelet count/spleen diameter ratio: proposal and validation of a non-invasive parameter to predict the presence of oesophageal varices in patients with liver cirrhosis. Gut. 2003;52(8):1200–1205. doi:10.1136/gut.52.8.1200
36. Buck M, Garcia-Tsao G, Groszmann RJ, et al. Novel inflammatory biomarkers of portal pressure in compensated cirrhosis patients. Hepatology. 2014;59(3):1052–1059. doi:10.1002/hep.26755
37. Leeming DJ, Karsdal MA, Byrjalsen I, et al. Novel serological neo-epitope markers of extracellular matrix proteins for the detection of portal hypertension. Aliment Pharmacol Ther. 2013;38(9):1086–1096. doi:10.1111/apt.12484
38. Bureau C, Metivier S, Peron JM, et al. Transient elastography accurately predicts presence of significant portal hypertension in patients with chronic liver disease. Aliment Pharmacol Ther. 2008;27(12):1261–1268. doi:10.1111/j.1365-2036.2008.03701.x
39. La Mura V, Reverter JC, Flores-Arroyo A, et al. Von Willebrand factor levels predict clinical outcome in patients with cirrhosis and portal hypertension. Gut. 2011;60(8):1133–1138. doi:10.1136/gut.2010.235689
40. Colecchia A, Marasco G, Taddia M, et al. Liver and spleen stiffness and other noninvasive methods to assess portal hypertension in cirrhotic patients: a review of the literature. Eur J Gastroenterol Hepatol. 2015;27(9):992–1001. doi:10.1097/MEG.0000000000000393
41. Li Q, Wang R, Guo X, et al. Contrast-Enhanced CT may be a diagnostic alternative for gastroesophageal varices in cirrhosis with and without previous endoscopic variceal therapy. Gastroenterol Res Pract. 2019;2019:1–15. doi:10.1155/2019/6704673
42. Deng H, Qi X, Zhang Y, Peng Y, Li J, Guo X. Diagnostic accuracy of contrast-enhanced computed tomography for esophageal varices in liver cirrhosis: a retrospective observational study. J Evid Based Med. 2017;10(1):46–52. doi:10.1111/jebm.12226
43. Deng H, Qi X, Guo X. Computed tomography for the diagnosis of varices in liver cirrhosis: a systematic review and meta-analysis of observational studies. Postgrad Med. 2017;129(3):318–328. doi:10.1080/00325481.2017.1241664
44. Deng H, Qi X, Guo X. Diagnostic Accuracy of APRI, AAR, FIB-4, FI, King, Lok, forns, and fibroindex scores in predicting the presence of esophageal varices in liver cirrhosis: a systematic review and meta-analysis. Medicine (Baltimore). 2015;94(42):e1795. doi:10.1097/MD.0000000000001795
45. Lisotti A, Azzaroli F, Buonfiglioli F, et al. Indocyanine green retention test as a noninvasive marker of portal hypertension and esophageal varices in compensated liver cirrhosis. Hepatology. 2014;59(2):643–650. doi:10.1002/hep.26700
46. Lisotti A, Azzaroli F, Cucchetti A, et al. Relationship between indocyanine green retention test, decompensation and survival in patients with Child-Pugh A cirrhosis and portal hypertension. Liver Int. 2016;36(9):1313–1321. doi:10.1111/liv.13070
47. Verma V, Sarin SK, Sharma P, Kumar A. Correlation of aspartate aminotransferase/platelet ratio index with hepatic venous pressure gradient in cirrhosis. United Eur Gastroenterol J. 2014;2(3):226–231. doi:10.1177/2050640614527084
48. Reiberger T, Ferlitsch A, Payer BA, et al. Noninvasive screening for liver fibrosis and portal hypertension by transient elastography–a large single center experience. Wien Klin Wochenschr. 2012;124(11–12):395–402. doi:10.1007/s00508-012-0190-5
49. Salzl P, Reiberger T, Ferlitsch M, et al. Evaluation of portal hypertension and varices by acoustic radiation force impulse imaging of the liver compared to transient elastography and AST to platelet ratio index. Ultraschall Med. 2014;35(6):528–533. doi:10.1055/s-0034-1366506
50. Procopet B, Berzigotti A, Abraldes JG, et al. Real-time shear-wave elastography: applicability, reliability and accuracy for clinically significant portal hypertension. J Hepatol. 2015;62(5):1068–1075. doi:10.1016/j.jhep.2014.12.007
51. Song J, Ma Z, Huang J, et al. Comparison of three cut-offs to diagnose clinically significant portal hypertension by liver stiffness in chronic viral liver diseases: a meta-analysis. Eur Radiol. 2018;28(12):5221–5230. doi:10.1007/s00330-018-5478-z
52. Takuma Y, Nouso K, Morimoto Y, et al. Portal hypertension in patients with liver cirrhosis: diagnostic accuracy of spleen stiffness. Radiology. 2016;279(2):609–619. doi:10.1148/radiol.2015150690
53. Friedrich-Rust M, Nierhoff J, Lupsor M, et al. Performance of acoustic radiation force impulse imaging for the staging of liver fibrosis: a pooled meta-analysis. J Viral Hepat. 2012;19(2):e212–e219. doi:10.1111/j.1365-2893.2011.01537.x
54. Takuma Y, Nouso K, Morimoto Y, et al. Measurement of spleen stiffness by acoustic radiation force impulse imaging identifies cirrhotic patients with esophageal varices. Gastroenterology. 2013;144(1):92–101.e2. doi:10.1053/j.gastro.2012.09.049
55. Hirooka M, Ochi H, Koizumi Y, et al. Splenic elasticity measured with real-time tissue elastography is a marker of portal hypertension. Radiology. 2011;261(3):960–968. doi:10.1148/radiol.11110156
56. Attia D, Schoenemeier B, Rodt T, et al. Evaluation of liver and spleen stiffness with acoustic radiation force impulse quantification elastography for diagnosing clinically significant portal hypertension. Ultraschall der Medizin - Eur J Ultrasound. 2015;36(06):603–610. doi:10.1055/s-0041-107971
57. Thiele M, Hugger MB, Kim Y, et al. 2D shear wave liver elastography by Aixplorer to detect portal hypertension in cirrhosis: an individual patient data meta-analysis. Liver Int. 2020;40(6):1435–1446. doi:10.1111/liv.14439
58. Elkrief L, Ronot M, Andrade F, et al. Non-invasive evaluation of portal hypertension using shear-wave elastography: analysis of two algorithms combining liver and spleen stiffness in 191 patients with cirrhosis. Aliment Pharmacol Ther. 2018;47(5):621–630. doi:10.1111/apt.14488
59. Deng H, Qi X, Zhang T, Qi X, Yoshida EM, Guo X. Supersonic shear imaging for the diagnosis of liver fibrosis and portal hypertension in liver diseases: a meta-analysis. Expert Rev Gastroenterol Hepatol. 2018;12(1):91–98. doi:10.1080/17474124.2018.1412257
60. Suh CH, Kim KW, Park SH, et al. Shear Wave elastography as a quantitative biomarker of clinically significant portal hypertension: a systematic review and meta-analysis. Am J Roentgenol. 2018;210(5):W185–W195. doi:10.2214/AJR.17.18367
61. Ronot M, Lambert S, Elkrief L, et al. Assessment of portal hypertension and high-risk oesophageal varices with liver and spleen three-dimensional multifrequency MR elastography in liver cirrhosis. Eur Radiol. 2014;24(6):1394–1402. doi:10.1007/s00330-014-3124-y
62. Castéra L, Le BB, Roudot-Thoraval F, et al. Early detection in routine clinical practice of cirrhosis and oesophageal varices in chronic hepatitis C: comparison of transient elastography (FibroScan) with standard laboratory tests and non-invasive scores. J Hepatol. 2009;50(1):59–68. doi:10.1016/j.jhep.2008.08.018
63. Pineda JA, Recio E, Camacho Á, et al. Liver stiffness as a predictor of esophageal varices requiring therapy in HIV/hepatitis C virus-coinfected patients with cirrhosis. J Acquir Immune Defic Syndr. 2009;51(4):445–449. doi:10.1097/QAI.0b013e3181acb675
64. Fraquelli M, Giunta M, Pozzi R, et al. Feasibility and reproducibility of spleen transient elastography and its role in combination with liver transient elastography for predicting the severity of chronic viral hepatitis. J Viral Hepat. 2014;21(2):90–98. doi:10.1111/jvh.12119
65. Petta S, Sebastiani G, Bugianesi E, et al. Non-invasive prediction of esophageal varices by stiffness and platelet in non-alcoholic fatty liver disease cirrhosis. J Hepatol. 2018. doi:10.1016/j.jhep.2018.05.019
66. Maurice JB, Brodkin E, Arnold F, et al. Validation of the Baveno VI criteria to identify low risk cirrhotic patients not requiring endoscopic surveillance for varices. J Hepatol. 2016;65(5):899–905. doi:10.1016/j.jhep.2016.06.021
67. Shi KQ, Fan YC, Pan ZZ, et al. Transient elastography: a meta-analysis of diagnostic accuracy in evaluation of portal hypertension in chronic liver disease. Liver Int. 2013;33(1):62–71. doi:10.1111/liv.12003
68. Stefanescu H, Grigorescu M, Lupsor M, Procopet B, Maniu A, Badea R. Spleen stiffness measurement using Fibroscan for the noninvasive assessment of esophageal varices in liver cirrhosis patients. J Gastroenterol Hepatol. 2011;26(1):164–170. doi:10.1111/j.1440-1746.2010.06325.x
69. Stafylidou M, Paschos P, Katsoula A, et al. Performance of Baveno VI and Expanded Baveno VI criteria for excluding high-risk varices in patients with chronic liver diseases: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2019;17(9):1744–1755.e11. doi:10.1016/j.cgh.2019.04.062
70. Moctezuma-Velazquez C, Saffioti F, Tasayco-Huaman S, et al. Non-invasive prediction of high-risk varices in patients with primary biliary cholangitis and primary sclerosing cholangitis. Am J Gastroenterol. 2019;114(3):446–452. doi:10.1038/s41395-018-0265-7
71. Thabut D, Bureau C, Layese R, et al. Validation of Baveno VI criteria for screening and surveillance of esophageal varices in patients with compensated cirrhosis and a sustained response to antiviral therapy. Gastroenterology. 2019;156(4):997–1009.e5. doi:10.1053/j.gastro.2018.11.053
72. Augustin S, Pons M, Maurice JB, et al. Expanding the Baveno VI criteria for the screening of varices in patients with compensated advanced chronic liver disease. Hepatology. 2017;66(6):1980–1988. doi:10.1002/hep.29363
73. Tosetti G, Primignani M, La Mura V, et al. Evaluation of three “beyond Baveno VI” criteria to safely spare endoscopies in compensated advanced chronic liver disease. Dig Liver Dis. 2019;51(8):1135–1140. doi:10.1016/j.dld.2018.12.025
74. Chang PE, Tan CK, Cheah CC, Li W, Chow WC, Wong YJ. Validation of the Expanded Baveno-VI criteria for screening gastroscopy in asian patients with compensated advanced chronic liver disease. Dig Dis Sci. 2020. doi:10.1007/s10620-020-06334-y
75. Protopapas AA, Mylopoulou T, Papadopoulos VP, Vogiatzi K, Goulis I, Mimidis K. Validating and expanding the baveno vi criteria for esophageal varices in patients with advanced liver disease: a multicenter study. Ann Gastroenterol. 2020;33(1):87–94. doi:10.20524/aog.2019.0429
76. Berger A, Ravaioli F, Farcau O, et al. Including ratio of platelets to liver stiffness improves accuracy of screening for esophageal varices that require treatment. Clin Gastroenterol Hepatol. 2020. doi:10.1016/j.cgh.2020.06.022
77. Dajti E, Ravaioli F, Colecchia A, Marasco G, Calès P, Festi D. Are the Expanded Baveno VI Criteria really safe to screen compensated cirrhotic patients for high-risk varices? Dig Liver Dis. 2019;51(3):456–457. doi:10.1016/j.dld.2018.12.013
78. Bae J, Sinn DH, Kang W, et al. Validation of the Baveno VI and the expanded Baveno VI criteria to identify patients who could avoid screening endoscopy. Liver Int. 2018;38(8):1442–1448. doi:10.1111/liv.13732
79. Cho YS, Kim Y, Sohn JH. Application of Supersonic Shear Imaging to the Baveno VI criteria and a combination model with spleen stiffness measurement to rule out high-risk varices in compensated advanced chronic liver disease. Ultraschall der Medizin - Eur J Ultrasound. 2020. doi:10.1055/a-1168-6271
80. Berzigotti A. Non-invasive evaluation of portal hypertension using ultrasound elastography. J Hepatol. 2017;67(2):399–411. doi:10.1016/j.jhep.2017.02.003
81. Singh S, Fujii LL, Murad MH, et al. Liver stiffness is associated with risk of decompensation, liver cancer, and death in patients with chronic liver diseases: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2013;11(12):
82. Robic MA, Procopet B, Métivier S, et al. Liver stiffness accurately predicts portal hypertension related complications in patients with chronic liver disease: a prospective study. J Hepatol. 2011;55(5):1017–1024. doi:10.1016/j.jhep.2011.01.051
83. Kitson MT, Roberts SK, Colman JC, Paul E, Button P, Kemp W. Liver stiffness and the prediction of clinically significant portal hypertension and portal hypertensive complications. Scand J Gastroenterol. 2015;50(4):462–469. doi:10.3109/00365521.2014.964758
84. Merchante N, Rivero-Juárez A, Téllez F, et al. Liver stiffness predicts clinical outcome in human immunodeficiency virus/hepatitis C virus-coinfected patients with compensated liver cirrhosis. Hepatology. 2012;56(1):228–238. doi:10.1002/hep.25616
85. Wang J-H, Chuah S-K, Lu S-N, et al. Baseline and serial liver stiffness measurement in prediction of portal hypertension progression for patients with compensated cirrhosis. Liver Int. 2014;34(9):1340–1348. doi:10.1111/liv.12525
86. Mendoza Y, Cocciolillo S, Murgia G, et al. Noninvasive markers of portal hypertension detect decompensation in overweight or obese patients with compensated advanced chronic liver disease. Clin Gastroenterol Hepatol off Clin Pract J Am Gastroenterol Assoc. 2020. doi:10.1016/j.cgh.2020.04.018
87. Petta S, Sebastiani G, Viganò M, et al. Monitoring occurrence of liver-related events and survival by transient elastography in patients with nonalcoholic fatty liver disease and compensated advanced chronic liver disease. Clin Gastroenterol Hepatol. 2020. doi:10.1016/j.cgh.2020.06.045
88. Corpechot C, Carrat F, Poujol-Robert A, et al. Noninvasive elastography-based assessment of liver fibrosis progression and prognosis in primary biliary cirrhosis. Hepatology. 2012;56(1):198–208. doi:10.1002/hep.25599
89. Osman KT, Maselli DB, Idilman IS, et al. Liver stiffness measured by either magnetic resonance or transient elastography is associated with liver fibrosis and is an independent predictor of outcomes among patients with primary biliary Cholangitis. J Clin Gastroenterol. 2020. doi:10.1097/MCG.0000000000001433
90. Cazzagon N, Lemoinne S, El Mouhadi S, et al. The complementary value of magnetic resonance imaging and vibration-controlled transient elastography for risk stratification in primary sclerosing cholangitis. Am J Gastroenterol. 2019;114(12):1878–1885. doi:10.14309/ajg.0000000000000461
91. Idilman IS, Low HM, Bakhshi Z, Eaton J, Venkatesh SK. Comparison of liver stiffness measurement with MRE and liver and spleen volumetry for prediction of disease severity and hepatic decompensation in patients with primary sclerosing cholangitis. Abdom Radiol. 2020;45(3):701–709. doi:10.1007/s00261-019-02387-4
92. Israelsen M, Guerrero Misas M, Koutsoumourakis A, et al. Collagen proportionate area predicts clinical outcomes in patients with alcohol-related liver disease. Aliment Pharmacol Ther. 2020;52:11–12. doi:10.1111/apt.16111
93. Colecchia A, Colli A, Casazza G, et al. Spleen stiffness measurement can predict clinical complications in compensated HCV-related cirrhosis: a prospective study. J Hepatol. 2014;60(6):1158–1164. doi:10.1016/j.jhep.2014.02.024
94. Meister P, Dechêne A, Büchter M, et al. Spleen stiffness differentiates between acute and chronic liver damage and predicts hepatic decompensation. J Clin Gastroenterol. 2018;1. doi:10.1097/MCG.0000000000001044
95. Buechter M, Kahraman A, Manka P, et al. Spleen and liver stiffness is positively correlated with the risk of esophageal variceal bleeding. Digestion. 2016;94(3):138–144. doi:10.1159/000450704
96. Takuma Y, Morimoto Y, Takabatake H, et al. Measurement of spleen stiffness with acoustic radiation force impulse imaging predicts mortality and hepatic decompensation in patients with liver cirrhosis. Clin Gastroenterol Hepatol. 2016;15(11):1782–1790.e4. doi:10.1016/j.cgh.2016.10.041
97. Dajti E, Ravaioli F, Colecchia A, et al. Spleen stiffness measurements predict the risk of hepatic decompensation after direct-acting antivirals in HCV Cirrhotic Patients. Ultraschall Med. 2020. doi:10.1055/a-1205-0367
98. Onori P, Morini S, Franchitto A, Sferra R, Alvaro D, Gaudio E. Hepatic microvascular features in experimental cirrhosis: a structural and morphometrical study in CCl4-treated rats. J Hepatol. 2000;33(4):555–563. doi:10.1016/S0168-8278(00)80007-0
99. Rappaport AM, MacPhee PJ, Fisher MM, Phillips MJ. The scarring of the liver acini (Cirrhosis). Tridimensional and microcirculatory considerations. Virchows Arch a Pathol Anat Histopathol. 1983;402(2):107–137. doi:10.1007/BF00695054
100. Marasco G, Colecchia A, Silva G, et al. Non-invasive tests for the prediction of primary hepatocellular carcinoma. World J Gastroenterol. 2020;26(24):3326–3343. doi:10.3748/wjg.v26.i24.3326
101. Papatheodoridis GV, Sypsa V, Dalekos GN, et al. Hepatocellular carcinoma prediction beyond year 5 of oral therapy in a large cohort of Caucasian patients with chronic hepatitis B. J Hepatol. 2020;72(6):1088–1096. doi:10.1016/j.jhep.2020.01.007
102. Salmon D, Bani-Sadr F, Loko MA, et al. Insulin resistance is associated with a higher risk of hepatocellular carcinoma in cirrhotic HIV/HCV-co-infected patients: results from ANRS CO13 HEPAVIH. J Hepatol. 2012;56(4):862–868. doi:10.1016/j.jhep.2011.11.009
103. Izumi T, Sho T, Morikawa K, et al. Assessing the risk of hepatocellular carcinoma by combining liver stiffness and the controlled attenuation parameter. Hepatol Res. 2019;49(10):1207–1217. doi:10.1111/hepr.13391
104. You M, Kim KW, Shim J, Pyo J. Impact of liver‐stiffness measurement on hepatocellular carcinoma development in chronic hepatitis C patients treated with direct‐acting antivirals: a systematic review and time‐to‐event meta‐analysis. J Gastroenterol Hepatol. 2020;
105. Jung KS, Kim SU, Choi GH, et al. Prediction of recurrence after curative resection of hepatocellular carcinoma using liver stiffness measurement (FibroScan®). Ann Surg Oncol. 2012;19(13):4278–4286. doi:10.1245/s10434-012-2422-3
106. Jung KS, Kim JH, Kim SU, et al. Liver stiffness value-based risk estimation of late recurrence after curative resection of hepatocellular carcinoma: development and validation of a predictive model. Alazawi W, ed. PLoS One. 2014;9(6):e99167. doi:10.1371/journal.pone.0099167
107. Poon RT, Fan ST, Ng IO, Lo CM, Liu CL, Wong J. Different risk factors and prognosis for early and late intrahepatic recurrence after resection of hepatocellular carcinoma. Cancer. 2000;89(3):500–507. doi:10.1002/1097-0142(20000801)89:3<500::AID-CNCR4>3.0.CO;2-O
108. Marasco G, Colecchia A, Colli A, et al. Role of liver and spleen stiffness in predicting the recurrence of hepatocellular carcinoma after resection. J Hepatol. 2019;70(3):440–448. doi:10.1016/j.jhep.2018.10.022
109. Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
110. Citterio D, Facciorusso A, Sposito C, Rota R, Bhoori S, Mazzaferro V. Hierarchic interaction of factors associated with liver decompensation after resection for hepatocellular carcinoma. JAMA Surg. 2016;151(9):846–853. doi:10.1001/jamasurg.2016.1121
111. Cucchetti A, Cescon M, Golfieri R, et al. Hepatic venous pressure gradient in the preoperative assessment of patients with resectable hepatocellular carcinoma. J Hepatol. 2016;64(1):79–86. doi:10.1016/j.jhep.2015.08.025
112. Cescon M, Colecchia A, Cucchetti A, et al. Value of transient elastography measured with fibroscan in predicting the outcome of hepatic resection for Hepatocellular Carcinoma. Ann Surg. 2012;256(5):706–713. doi:10.1097/SLA.0b013e3182724ce8
113. Hu H, Han H, Han XK, Wang WP, Ding H. Nomogram for individualised prediction of liver failure risk after hepatectomy in patients with resectable hepatocellular carcinoma: the evidence from ultrasound data. Eur Radiol. 2018;28(2):877–885. doi:10.1007/s00330-017-4900-2
114. Kim SU, Ahn SH, Park JY, et al. Prediction of postoperative hepatic insufficiency by liver stiffness measurement (FibroScan®) before curative resection of hepatocellular carcinoma: a pilot study. Hepatol Int. 2008;2(4):471–477. doi:10.1007/s12072-008-9091-0
115. Serenari M, Han KH, Ravaioli F, et al. A nomogram based on liver stiffness predicts postoperative complications in patients with hepatocellular carcinoma. J Hepatol. 2020. doi:10.1016/j.jhep.2020.04.032
116. Rajakannu M, Cherqui D, Ciacio O, et al. Liver stiffness measurement by transient elastography predicts late posthepatectomy outcomes in patients undergoing resection for hepatocellular carcinoma. Surgery. 2017;162(4):766–774. doi:10.1016/j.surg.2017.06.006
117. Marasco G, Colecchia A, Dajti E, et al. Prediction of posthepatectomy liver failure: role of SSM and LSPS. J Surg Oncol. 2019;119:3. doi:10.1002/jso.25345
118. Peng W, Zhang X-Y, Li C, Wen T-F, Yan L-N, Yang J-Y. Spleen stiffness and volume help to predict posthepatectomy liver failure in patients with hepatocellular carcinoma. Medicine (Baltimore). 2019;98(18):e15458. doi:10.1097/MD.0000000000015458
119. Kim HY, So YH, Kim W, et al. Non-invasive response prediction in prophylactic carvedilol therapy for cirrhotic patients with esophageal varices. J Hepatol. 2019;70(3):412–422. doi:10.1016/j.jhep.2018.10.018
120. Jansen C, Möller P, Meyer C, et al. Increase in liver stiffness after transjugular intrahepatic portosystemic shunt is associated with inflammation and predicts mortality. Hepatology. 2018;67(4):1472–1484. doi:10.1002/hep.29612
121. De Santis A, Nardelli S, Bassanelli C, et al. Modification of splenic stiffness on acoustic radiation force impulse parallels the variation of portal pressure induced by transjugular intrahepatic portosystemic shunt. J Gastroenterol Hepatol. 2018;33(3):704–709. doi:10.1111/jgh.13907
122. Han H, Yang J, Zhuge Y, Zhang M, Wu M. Point Shear Wave Elastography to Evaluate and Monitor Changing Portal Venous Pressure in Patients with Decompensated Cirrhosis. Ultrasound Med Biol. 2017;43(6):1134–1140. doi:10.1016/j.ultrasmedbio.2017.01.019
123. Novelli PM, Cho K, Rubin JM. Sonographic assessment of spleen stiffness before and after transjugular intrahepatic portosystemic shunt placement with or without concurrent embolization of portal systemic collateral veins in patients with cirrhosis and portal hypertension: a feasibility study. J Ultrasound Med. 2015;34(3):443–449. doi:10.7863/ultra.34.3.443
124. Giunta M, La Mura V, Conti CB, et al. The role of spleen and liver elastography and color-doppler ultrasound in the assessment of transjugular intrahepatic portosystemic shunt function. Ultrasound Med Biol. 2020;46(7):1641–1650. doi:10.1016/j.ultrasmedbio.2020.04.007
125. Gao J, Zheng X, Zheng -Y-Y, et al. Shear wave elastography of the spleen for monitoring transjugular intrahepatic portosystemic shunt function: a pilot study. J Ultrasound Med. 2016;35(5):951–958. doi:10.7863/ultra.15.07009
126. Buechter M, Manka P, Theysohn JM, Reinboldt M, Canbay A, Kahraman A. Spleen stiffness is positively correlated with HVPG and decreases significantly after TIPS implantation. Dig Liver Dis. 2018;50(1):54–60. doi:10.1016/j.dld.2017.09.138
127. Han H, Yang J, Jin WK, et al. Diagnostic value of conventional ultrasound and shear wave elastography in detecting transjugular intrahepatic portosystemic shunt dysfunction. Acta Radiol. 2020:028418512097518. doi:10.1177/0284185120975183.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.