Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Appreciation of Increased Pulmonary Vascular Resistance from the Maximum Desaturation in 2-Chair Test: An Appraisal
Authors Bhattacharyya P ![]() , Sengupta S, Paul M, Saha D, De A
, Sengupta S, Paul M, Saha D, De A ![]() , Dey D, Ray S
, Dey D, Ray S
Received 20 March 2025
Accepted for publication 2 September 2025
Published 15 November 2025 Volume 2025:20 Pages 3725—3735
DOI https://doi.org/10.2147/COPD.S529320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Parthasarathi Bhattacharyya,1 Sayoni Sengupta,2,3 Mintu Paul,4 Dipanjan Saha,4 Aniruddha De,5 Debkanya Dey,6 Shuvanan Ray7
1Department of General Pulmonology Institute of Pulmocare and Research, Kolkata, West Bengal, India; 2Department of Pulmonary Circulation Institute of Pulmocare and Research, Kolkata, West Bengal, India; 3Department of Microbiology, Sister Nivedita University, Kolkata, West Bengal, India; 4Department of General Pulmonology,Institute of Pulmocare and Research, Kolkata, West Bengal, India; 5Department of Non-Interventional Cardiology, Suraksha Diagnostic, Kolkata, West Bengal, India; 6Department of Biotechnology and Dr. B. C. Guha Centre for Genetic Engineering and Biotechnology, University of Calcutta, Kolkata, West Bengal, India; 7Department of Interventional Cardiology, Fortis Hospital, Kolkata, West Bengal, India
Correspondence: Parthasarathi Bhattacharyya, Institute of Pulmocare and Research, DG-8, Action Area 1, New Town, Kolkata, West Bengal, 700156, Email [email protected]
Introduction: The desat max of 2-chair test, claimed to have identified the sildenafil responsiveness in COPD-PH (pulmonary hypertension), should represent high PVR (pulmonary vascular resistance).
Methods: Hemodynamically diagnosed PH in CLD (chronic lung disease)-patients were analyzed statistically and divided into two groups on high or low PVR (> 2 and ≤ 2 Wood units) to judge the power of the desat-max of 2-chair test differentiating them. Co-relationship of desat-max was sought with different spirometric, Doppler-echocardiographic, and RHC (right heart catheterization) derived parameters as TPG (trans-pulmonary gradient), PVR, mPAP (mean pulmonary pressure) and PCWP (pulmonary capillary wedge pressure). Further, the specificity and sensitivity of variable desat-max values were calculated and high PVR and a VIP plot was drawn with all available variables to see their impact on PVR compared to desat-max.
Results: We included 57 patients of CLD-PH consisting of COPD (n=26), chronic asthma (n=9), ILD (n=7), and miscellaneous diseases (n=15). When divided on high or low PVR, the two groups (n=39 and 18) stood similar in demographic, spirometric, and Doppler-echocardiography measurements. However, they differed in desat-max (− 8.76± 4.90 and − 3.61± 1.94; P< 0.0001) and in RHC derived mean-PVR (4.25± 2.97 vs 1.20± 0.53; P< 0.0001), mean-TPG (12.86± 4.84 vs 5.11± 2.78; P< 0.0001), cardiac output (3.77± 1.07 and 4.29± 1.15; P=0.02). The calculated best cut-off desat-max (> 4.5%) could identify high PVR with 72.22% sensitivity and 79.40% specificity with adjusted odds ratio of 19.55. The desat-max correlated best with RHC-measured PVR (r=0.56) but not with PCWP (r=0.09).
Conclusion: Desat-max of 2-chair test appears indicative of high PVR in CLD-PH. The revelation merits further research.
Keywords: 2-chair test, maximum desaturation, pulmonary arterial pressure
Introduction
Pulmonary hypertension (PH) is defined by mean PAP (pulmonary artery pressure) of 20 mmHg, or PVR of >2.0 Wood unit.1 Group-3 PH are those derived from chronic lung diseases (CLD).2 Several lung diseases are incriminated to cause variable degree of PH as COPD, ILD, sarcoidosis and others.2 COPD is the most frequent diagnosis in group-3 PH.3,4 Physiologically, there is either chronic hypoxemia from hypoventilation (OSA) or a jeopardy of lung function through chronic airflow obstruction (COPD), or parenchymal restriction (ILD) or both combined pulmonary fibrosis and emphysema (CPFE). PH can evolve in COPD/CLD either from a primary pulmonary circulatory impairment as it happens in pulmonary artery hypertension (PAH), or secondary to structural and functional perturbation from a chronic lung disease. The former (rare in frequency), keeps the lung-functions relatively preserved while in the later (commonly encountered), there is a gross reduction in lung function. The presence of PH in COPD or any chronic lung disease implies a compromise in functional capacity, quality of life, and survival prospects.5,6
The PH in CLD is essentially a precapillary but its complexities are far from clear and despite several pulmonary vasodilators available, there is no recommendation favouring their use in CLD-PH. The impression applies to PH from both airway and parenchymal lung diseases except the recent revelation of the positive role of inhaled treprostinil in ILD-PH.7
CLD-PH may coexist with group-II and group-IV pulmonary hypertension. The pathogenesis of CLD-PH results from both general and individual disease specific characteristics where the lung disease induced hypoxemia8 and the pulmonary vascular endothelial dysfunction appears important.9 Other mechanisms as constriction or loss of pulmonary vascular bed, compression of alveolar vessels, and occasional polycythaemia can play in genesis of PH. While the knowledge of CLD-PH is evolving, there is unanimity of opinion regarding the deleterious effects of PH on functionality, quality of life, life expectancy, and the indication of oxygen therapy.3 The right heart catheterization (RHC) remains the gold standard test to confirm PH although clinical, radiological, and echocardiographic exercises can help to offer a screening diagnosis. The pulmonary vascular resistance (PVR) acts as the important marker in PH to understand the presence of precapillary PH/pulmonary vascular remodeling and it displays crucial diagnostic and prognostic value with therapeutic implications.10 The appreciation of PVR (trans-pulmonary gradient; TPG/cardiac output) is only possible through right heart catheterization. Until date, there is an unmet need for a good but simple and objective noninvasive or clinical marker of high PVR.11,12
Due to the incapability to perform RHC, the authors observed that the patients with CLD-PH show postexercise desaturation that led them to evolve the 2-Chair Test (2CT), an assessment tool of measuring postexercise cardiopulmonary recovery response.13 They further observed and subsequently hypothesized that desat-max or maximum desaturation in 2CT is useful to appreciate responders to vasodilators in COPD-PH with poor WHO functional status.14 The concept was endorsed hemodynamically in a small number of patients.15 However, further hemodynamic validation of the endorsement was essential to justify the role of this desat-max, a PERR (postexercise recovery response) parameter to demonstrate its ability to identify precapillary pulmonary hypertension or PVR. The present manuscript depicts the efforts in the direction of identifying the relationship of desat-max (derived from 2CT) with PVR derived from RHC to address the unmet need of a noninvasive biomarker of increased PVR.
Methods
The protocol was approved by the independent Ethics Committee of the Institute of Pulmocare and Research (DCGI registration no. ECR/159/Inst/WB/2013/RR-20). The study was conducted complying to ethical principles for medical research involving human subjects of the Declaration of Helsinki. The subjects were recruited from the outpatient department of the institute on written informed consents. We selected willing patients with chronic lung disease(CLD) as defined by the National Cancer Institute.16 The confirmation of their lung disease was performed through spirometry, HRCT chest and other necessary evaluations as per our institutional algorithm and the final diagnosis with inclusions were independently decided by the investigating pulmonologist on a defined protocol.14,17
The screening diagnosis of PH was done according to the clinico-radio-echocardiographic protocol of the institute17 followed by confirmation through RHC. We integrated the 2CT in the evaluation because it evolved as an effort to denote our observation of an overt postexercise desaturation uniformly in patients with CLD-PH. In our observation, CLD-PH patients with high (>3%) desaturation (desat-max) in the postexercise period had responded to pulmonary vasodilators.14 The phenomenon appeared hemodynamically endorsed on RHC in a small number of patients where we found higher desat-max associated with higher PVR.15 Since RHC was part of another project, we included the 2CT in the exercise to demonstrate further an association of desat-max of 2CT to RHC derived PVR. The exclusion included sick patients, age less than<45 and >75 years, active smoking, suspicion of any malignancy or pulmonary thromboembolism, history of recent exacerbations (with 6 weeks), active or recent lung infection, any active systemic disease, contraindications or unwillingness for evaluation with spirometry or echocardiography or RHC, and 2-chair test. A desat-max of <3%, and the revelation of disproportionately high PA pressure or no PH on RHC were included in exclusion criteria.
2-Chair Test
All the included patients underwent the 2CT.13 Similar to the 6-minutes’ walk test (6MWT), the 2-chair test also includes a sub-optimal exercise. The novelty of the test lies in its nature of assessment of the cardiopulmonary specific postexercise recovery response measured through change in pulse rate and arterial oxygen saturation unlike the 6MWT that counts the distance walked or the exercise capacity. The maximum desaturation (indicated as “desat-max”) derived of the 2-chair test correlates to the sickness of a patient18 and a high desat-max (>3%) appeared useful in CLD-PH to guide vasodilator therapy.14,15 This encouraged us to further explore its quality to identify raised PVR in CLD-PH.
We collected the 2CT result for each patient on a software. However, we included those with desat-max of >3% based on our previous experience.14,15 The sample size was calculated form our previous experience15 that necessitates inclusion of 22 patients for a power of 99% using the Cohen’s formula. Incidentally, we could include a much higher number (n=57) of patients in our observation.19
Echocardiography
A single expert performed the Doppler-echocardiography on a protocol for all the patients with clinico-radiological suspicion of PH remaining blind about the purpose of the research. The tests included understanding of left ventricular (LV) function (LV ejection fraction, regional wall motion abnormality, presence of systolic and diastolic LV dysfunction) and right ventricular (tricuspid annular plane systolic excursion; TAPSE) functions, and the measurement systolic pulmonary arterial pressure (sPAP). The mean PAP (mPAP) was derived by using the regression formula (mPAP= 0.61*sPAP+ 2 mmHg)20 and the early mitral flow velocity/early mitral annular velocity (E/e’) was considered to represent the left ventricular filling pressure (LVFP) an important marker of left ventricular diastolic dysfunction (LVDD).21,22 The candidates with heart failure with reduced ejection fraction (HFrEF) or any regional wall motion abnormality and valvular heart disease were excluded from the study.
Right Heart Catheterization (RHC)
The RHC was conducted within 48 hours of echocardiography through a venous cannulation depending upon the operator’s preference. It helped to directly measure the mean pressure (systolic, diastolic and end-diastolic) at right atrium, right ventricle, and the pulmonary artery. The wedge pressure was noted using an inflated Swan–Ganz balloon tipped catheter following standard procedural protocols.23 The oxygen saturation was computed from pulmonary artery (PA), right ventricle (RV), right atrium (RA), superior vena cava (SVC), inferior vena cava (IVC). The oxygen consumption was calculated by the Dehmer formula where the estimated VO2 (oxygen consumption) equals to 125 × body surface area (BSA).24 The measurement of BSA was done by including body weight (kg) and height (cm) in the calculation.25 The cardiac output was measured using Fick’s principle.24 The TPG was calculated by subtracting the PCWP from the mean pulmonary artery pressure (mPAP) values and the PVR was calculated by dividing the TPG with cardiac output.26
Statistical Analysis
The Graphpad Prism-7 software was used for statistical comparison between the groups (ie PVR>2 and PVR<2 Wood unit) using unpaired t-test. The normality and lognormality were checked using the D’Agostino–Pearson test using the software. The t-test was then computed using Wilcoxon test, for the data failing to pass the normality testing. The desat-max on qualifying with significant difference (P≤0.0001) was decided to be used to calculate the sensitivity and specificity of its variable cut-off levels to identify the high PVR through computing a receiver operating characteristic (ROC) curve. Further, to appreciate the relative contribution of all the different but related (demographic, spirometric, echocardiographic, and hemodynamic) parameters for high PVR, the co-relationship of these parameters with desat-max was looked for using the Pearson coefficient and a VIP plot was drawn using the free version of Metaboanalyst (version-6) software. Finally, a forest plot was drawn with the adjusted odds ratios (ORs) with the parameters that proved significant to differentiate the high vs low PVR.
Results
Out of the 57 cases evaluated with RHC, 39 patients had PVR≥2 Wood units. The demographic, clinical, spirometric, 2-chair test, echocardiographic and hemodynamic parameters are observed in them (Table 1).
 |
Table 1 Comparison of Demography, Spirometry and Hemodynamic Characteristics |
The desat-max can discriminate the two groups significantly (P<0.0001) along with other parameters including the PVR. Thus, the PVR was chosen to compute ROC curves to find the best and the variable cut-off values of desat max for discrimination high from normal PVR (Table 2).
 |
Table 2 Demonstration of Effective Cut-offs for Desat Max Derived from ROC |
Further, VIP and score plots (Figure 1A and B) elaborate the relative importance of the different parameters in contributing to high PVR (Figure 1A) and the overlap between the two groups (Figure 1B).
 |
Figure 1 (A) The variance importance in projection (VIP) plot shows the relative position of the desat-max to appreciate the detection capacity of high pulmonary vascular resistance (PVR) from low along with other parameters. (B) The score plots show two distinct clusters made of high and low PVR incorporating the variables with some overlaps. |
Furthermore, when calculated, it was found that the univariate OR for PVR is 10.08 (95%CI: 2.636–35.66) with desat-max of >4 and <=4 (Figure 2). The two significant RHC-derived hemodynamic parameters (mean-PAP and cardiac output) and the desat max with a cut-off of 4% differentiating the high or low PVR were computed for their univariate (Figure 2A) and adjusted (Figure 2B) ORs and displayed as forest plots in (Figure 2A and B).
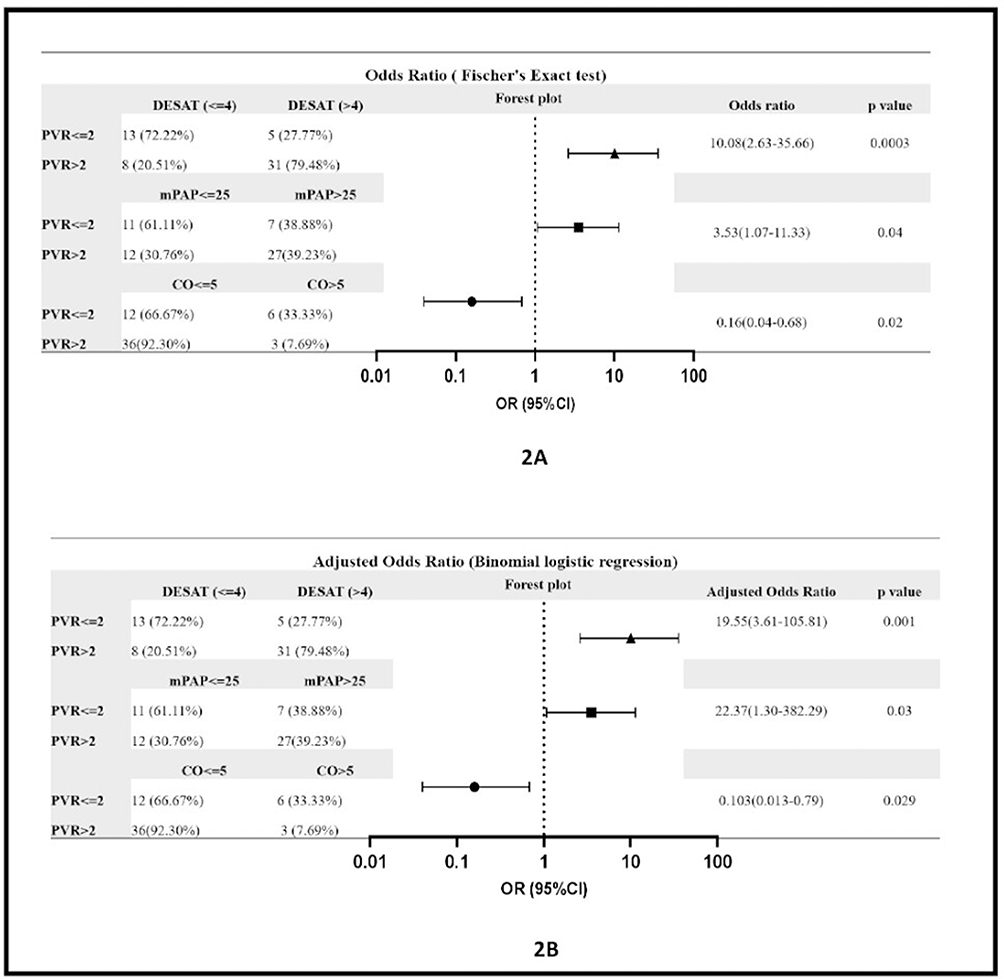 |
Figure 2 Shows the univariate and adjusted odds ratios of the important hemodynamic parameters and desat max for the presence or absence or high PVR. Abbreviations: mpap, mean pulmonary artery pressure; CO, cardiac output; PVR, pulmonary vascular resistance. |
The correlation between desat max with different spirometry and hemodynamic parameters are given Figure 3.
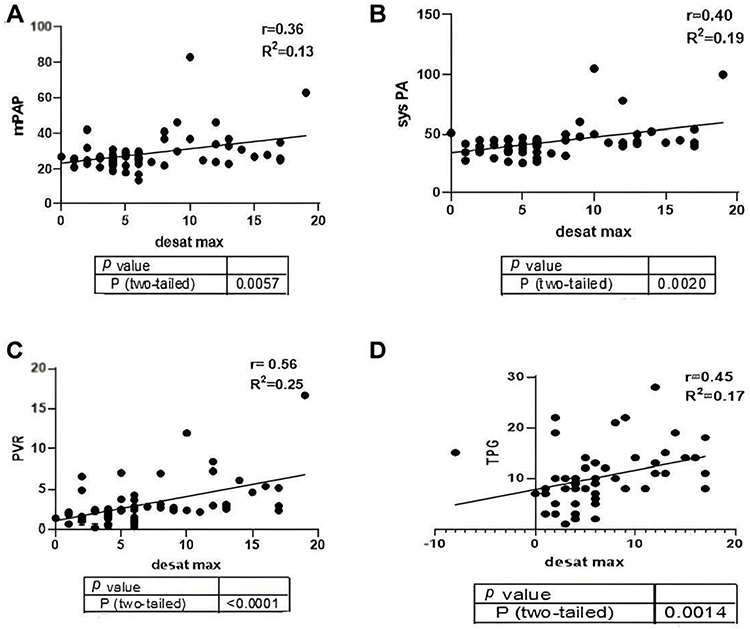 |
Figure 3 The correlation of desat max with right heart catheterization (RHC) derived hemodynamic parameters with Pearson coefficients. (A) Desat max vs mPAP (RHC). (B) Desat max with sys PA. (C) Desat max with PVR. (D) TPG withdesat max. Abbreviations: mPAP, mean pulmonary artery pressure; PVR, pulmonary vascular resistance; sys PAP, systolic pulmonary artery pressure; TPG, transpulmonary gradient. |
Discussion
The two groups of CLD-PH with or without high PVR had similar baseline demographic, clinical, and spirometry characteristics (Table 1). Interestingly, the desat-max was found to differ significantly (−8.76±4.90 vs −3.61 ±1.94; P-value <0.0001) between the groups.
On right heart catheterization, the difference was significant in systolic-PAP (47.05±15.46 vs 37.22±7.27, P=0.004), mean PAP (31.71±11.94 vs 23.83±4.60, P=0.002), TPG (12.86±4.86 vs 5.11±2.78, P=<0.0001) and PVR (4.25±2.97 vs 1.20±0.53, P=<0.0001) (Table 1). However, on echocardiography, the systolic-PAP, m-PAP (calculated) but not the TPG show difference as significant.
Out of the hemodynamic parameters, the desat-max correlates best to the PVR (r=0.56; P=0.0001) (Figure 3). The calculated specificity and sensitivity of different cut-offs for desat-max (Table 2) displays the best acceptable value to be around 4%. With desat-max of >4 and <=4, the adjusted odds ratio of 19.55 appears impressive and a novel marker for the presence of raised PVR (Figure 2).
The PVR represents the resistance in the precapillary pulmonary circuit that imparts the majority of PH in CLD in our present series. Precapillary pulmonary hypertension is amenable to the action of the vasodilators.10 Our revelation stands novel with prospect of enormous applicability. It explains and justifies the role of desat-max in deciding the use of pulmonary vasodilators for COPD-PH patients with poor functional WHO class earlier.14,15 Other parameters associated with understanding precapillary PH as mean-PAP, TPG, do demonstrate similar but less strong association with desat-max.
In our observation, the patients of CLD had a co-presence of high pulmonary venous pressure evident from universally high PCWP (>15 mmHg) (Table 1). Incidentally, such postcapillary PH can exist commonly concomitant to precapillary PH in COPD15,26 and the comorbidities often contribute to that.27 The raised PCWP is universal in our (non-COPD) CLDs. Thus, the desat-max seems effective to indicate high PVR in mixed pre- and postcapillary PH.
Multiple factors might dynamically influence the development and progression of PH in a CLD leading to a spectrum of severity of PH with its physiological consequences. They could modify or add to the usual natural history of CLD-PH with individual-specific characteristics. The right ventricular (RV) function appears as one such component. In this context, our patients displayed a relatively preserved TAPSE (tricuspid annular plane systolic excursion; 22.40±3.88 mm; the (normal value is 15–25mm), a marker of RV systolic function.28 Such preservation of RV systolic function does not exclude RV affection but indicates a possible successful adaptation of RV to cope with the slow increment of afterload imposed by the raised PAP.
It appears intriguing to explain the decline in the immediate postexercise resting saturation in 2CT. Thus, the desat-max seems to represent the impact of the loss of ability and/or agility of the precapillary pulmonary circuit to re-adjust to the altered circulatory demand in postexercise recovery period. The very fact that PH is more frequently observed in advanced CLD (as in COPD) with the loss of lung function,29 supports the presence of a possible and parallel event of vascular remodeling in COPD/CLD.30 It appears that there is an increase in ventilation/perfusion (V/Q) mismatch during the recovery period. This increased postexercise V/Q mismatch is likely to have originated from a compromised circulatory reserve. Immediate postexercise in 2CT, the metabolic demand drops but the return of deoxygenated blood from the tissue is increased. Such deoxygenated venous blood may act as a modulator of the pulmonary vascular tone (vasoconstrictor) to add-on to the incapability of the already compromised pulmonary vascular reserve to maintain an optimal V/Q relationship. This could explain the desaturation to happen in the postexercise recovery response in 2-chair test. Further in depth understating of the issue demands intricate research.
There is a significant reduction of cardiac output (3.77±1.01 vs 4.29±1.15 L/min; P=0.02) in the patients with high PVR where the right ventricular dysfunction likely predominates. The right ventricle (RV) demonstrates a variable degree of hypertrophy to accommodate the increased afterload until a point of time when it starts dilatation.30,31 Maladaptation of the RV in the face of PH is one of the major events that influences the functional capacity and prognosis.32 Incidentally, we cannot evolve an efficient understanding of the RV functional recovery dynamics from our data; one needs intricate evaluations of RV functions in such patients with raised afterload but normal TAPSE.
The frequent presence of left ventricular diastolic dysfunction (LVDD) in our patients is also intriguing as evident from raised E/e’ as (13.32±4.13). LVDD in COPD is found to the tune of 30 to 70%.33 Since we excluded the sick and unstable patients at the outset, this suggests that desat max does not correlate to left ventricular end diastolic pressure (LVEDP) in stable CLD patients. However, the relationship is intriguing and may change in overt heart failure with or without preserved ejection fraction (HFpEF) making this area of association of HFpEF with desat-max an interesting domain of research.
The VIP plot that depicts and allows a comparison of the strength of association of different parameters with PVR clearly helps us appreciate the efficiency of desat-max in this regard (Figure 1A). According to the score-plot (Figure 1B), though distinct, there is an overlap of low and high PVR groups; the factors responsible for such overlap need to be explored.
There are several lacunae in the research. The number of recruits is small; the echocardiography should have been more exhaustive, especially to determine the left and right ventricular functions. The possible overt diastolic heart failure that, although unlikely, was not confirmed. All the raised PCWP cases should have been rechecked with left heart catheterization and measurement of the left ventricular end diastolic pressure to have a much more objective and robust evidence for postcapillary component of pulmonary hypertension. MRI studies of the ventricular structural and functional status may add to our understanding of ventricular dysfunctions in these patients.
In our observation, the universally high postcapillary PH was interesting; the issue itself demands separate research for epidemiological confirmation, possible etiological clues, and understanding the mechanistic pathways. Such postcapillary PH can evolve from left ventricular diastolic dysfunction or the postcapillary vascular problem in the pulmonary venous circuit.34 Although we have some idea about the presence of left ventricular relaxation abnormality (diastolic dysfunction), we cannot comment on the possibility of obvious remodeling in the pulmonary venous system in COPD as reported.35 For COPD (the majority in our cohort), there is loss of venous capacitance from the destruction of alveolar walls or possible compression from dynamic hyperinflation; the mechanism could be different for restrictive or mixed obstructive and restrictive diseases. More research is warranted in this front.
Conclusion
The 2-chair test derived desat-max appears as a novel noninvasive marker of precapillary PH/PVR in combined pre- and postcapillary pulmonary hypertension with CLD. Further research with detailed hemodynamic assessment, advanced imaging, and other modalities is essential to validate the observation in different groups of PH. One needs to elaborate the physiological foundation of the observation categorically. Such efforts may prove worthwhile in clinical applications as early diagnosis, patient stratification, and treatment decisions involving pulmonary vasodilators.
Ethical Approval
The study was approved by independent Institutional Ethics Committee (IEC).
Acknowledgments
The authors acknowledge all the staffs of Institute of Pulmocare and Research, Kolkata and all the patients who willingly participated in this study. We also thank West Bengal Department of Science and Technology (WB-DST) who partially supported our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
It was partially supported by West Bengal Department of Science and Technology (WB-DST) through a research grant for a project related to pulmonary hypertension.
Disclosure
The authors report no competing interests in this work.
References
1. Humbert M, Kovacs G, Hoeper MM, et al. ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European society of cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the international society for heart and lung transplantation (ISHLT) and the European reference network on rare respiratory diseases (ERN-LUNG). Eur Heart J. 2022;43(38):3618–3731. doi:10.1093/eurheartj/ehac237
2. Seeger W, Adir Y, Barberà JA, et al. Pulmonary hypertension in chronic lung diseases. Journal of the American College of Cardiology. 2013;63(1):62. doi:10.1016/j.jacc.2013.10.036
3. Nathan SD, Barbera JA, Gaine SP, et al. Pulmonary hypertension in chronic lung disease and hypoxia. Eur Respir J. 2019;53(1):1801914. doi:10.1183/13993003.01914-2018
4. Minai OA, Chaouat A, Adnot S. Pulmonary hypertension in COPD: epidemiology, significance, and management. Chest. 2010;137(6):39S–51S. doi:10.1378/chest.10-0087
5. Boutou AK, Pitsiou GG, Trigonis I, et al. Exercise capacity in idiopathic pulmonary fibrosis: the effect of pulmonary hypertension. Respirology. 2011;16(3):451–458. doi:10.1111/j.1440-1843.2010.01909.x
6. Klinger JR. Group III pulmonary hypertension. Cardiology Clinics. 2016;34(3):413–433. doi:10.1016/j.ccl.2016.04.003
7. Weatherald J, Nathan SD, El-Kersh K, et al. Inhaled treprostinil in patients with pulmonary hypertension associated with interstitial lung disease with less severe haemodynamics: a post hoc analysis of the increase study. BMJ Open Respiratory Research. 2024:11. doi:10.1136/bmjresp-2023-002116
8. Pak O, Aldashev A, Welsh D, et al. The effects of hypoxia on the cells of the pulmonary vasculature. Eur Respir J. 2007;30(2):364–372. doi:10.1183/09031936.00128706
9. Szucs B, Szucs C, Petrekanits M, et al. Molecular characteristics and treatment of endothelial dysfunction in patients with COPD: a review article. Int J Mol Sci. 2019;20(18):4329. doi:10.3390/ijms20184329
10. Deng J. Clinical application of pulmonary vascular resistance in patients with pulmonary arterial hypertension. Journal of Cardiothoracic Surgery. 2021;16(1) doi:10.1186/s13019-021-01696-4
11. Rumiz E, Cubillos A, Vilar JV, et al. Inaccuracy of a non-invasive estimation of pulmonary vascular resistance assessed by cardiovascular magnetic resonance in heart failure patients. Sci Rep. 2021;11(16597). doi:10.1038/s41598-021958975
12. Abbas AE, Franey LM, Marwick T, et al. Noninvasive assessment of pulmonary vascular resistance by Doppler echocardiography. J Am Soc Echocardiogr. 2013;26(10):1170–1177. doi:10.1016/j.echo.2013.06.003
13. Bhattacharyya P, Saha D, Paul M, et al. Two chair tests: a substitute of 6 min walk test appear cardiopulmonary reserve specific. BMJ Open Respiratory Research. 2020;7(1):e000447.
14. Bhattacharyya P, Sengupta S, Bhattacharjee, et al. Post exercise desaturation can help identifying treatment responders of COPD pulmonary hypertension in real world: an appraisal. J Pulm Respir Med. 2018;08(04). doi:10.4172/2161-105x.1000469
15. Bhattacharyya P, Sengupta S, Ray S, et al. Hemodynamic endorsement of post-exercise desaturation-based decision of treating COPD-PH: a pilot observation. J Pulm Respir Med. 2020;10(2): 1–5.
16. NCI dictionary of cancer terms. Cancer.gov. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/chronic-lung-disease.
17. Bhattacharyya P, Sengupta S, Saha D, et al. Group III pulmonary hypertension: relative frequency of different etiologies in a referral pulmonary OPD. The Journal of Association of Chest Physicians. 2020;8(2):69–75. doi:10.4103/jacp.jacp_3_20
18. Bhattacharyya P, Chakraborty W, Paul M, Sengupta S, Saha D. The desat-max in 2-chair test appears to be a worthwhile parameter to identify sickness: an appraisal. Indian J Med Res. 2025;161(2):174. doi:10.25259/IJMR_952_2024
19. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Routledge; 2013.
20. Chemla D, Castelain V, Humbert M, et al. New formula for predicting mean pulmonary artery pressure using systolic pulmonary artery pressure. Chest J. 2004;126(4):1313–1317. doi:10.1378/chest.126.4.1313
21. Previtali M, Chieffo E, Ferrario M, et al. Is mitral E/E’ ratio a reliable predictor of left ventricular diastolic pressures in patients without heart failure? Eur Heart J Cardiovasc Imaging. 2011;13(7):588–595. doi:10.1093/ejechocard/jer286
22. Zhang F, Liang Y, Chen X, et al. Echocardiographic evaluation of left ventricular end diastolic pressure in patients with diastolic heart failure. Medicine. 2020;99(49):e22683. doi:10.1097/md.0000000000022683
23. Nair R, Lamaa N. Pulmonary capillary wedge pressure. StatPearls - NCBI Bookshelf. 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557748/.
24. Dehmer GJ, Firth BG, Hillis LD. Oxygen consumption in adult patients during cardiac catheterization. Clinical Cardiology. 1982;5(8):436–440. doi:10.1002/clc.4960050803
25. Lee JY, Choi JW, Kim H. Determination of body surface area and formulas to estimate body surface area using the alginate method. Journal of Physiological Anthropology. 2008;27(2):71–82. doi:10.2114/jpa2.27.71
26. Scharf SM, Iqbal M, Keller C, et al. Hemodynamic characterization of patients with severe emphysema. Am J Respir Crit Care Med. 2002;166(3):314–322. doi:10.1164/rccm.2107027
27. Butler J, Schrijen F, Henriquez A, et al. Cause of the raised wedge pressure on exercise in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1988;138(2):350–354. doi:10.1164/ajrccm/138.2.350
28. Modin D, Møgelvang R, Andersen DM, et al. Right ventricular function evaluated by tricuspid annular plane systolic excursion predicts cardiovascular death in the general population. Journal of the American Heart Association. 2019;8(10). doi:10.1161/jaha.119.012197
29. Chaouat A, Naeije R, Weitzenblum E. Pulmonary hypertension in COPD. Eur Respir J. 2008;32(5):1371–1385. doi:10.1183/09031936.00015608
30. Vonk Noordegraaf A, Westerhof BE, Westerhof N. The relationship between the right ventricle and its load in pulmonary hypertension. Journal of the American College of Cardiology. 2017;69(2):236–243. doi:10.1016/j.jacc.2016.10.047
31. Noordegraaf AV, Chin KM, Haddad F, et al. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: an update. Eur Respir J. 2019;53(1).
32. Ryan JJ, Huston J, Kutty S, et al. Right ventricular adaptation and failure in pulmonary arterial hypertension. Cana J Cardiol. 2015;31(4):391–406. doi:10.1016/j.cjca.2015.01.023
33. Boussuges A, Pinet C, Molenat F, et al. Left atrial and ventricular filling in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;162(2):670–675. doi:10.1164/ajrccm.162.2.9908056
34. De Jesus Perez VA, Haddad F, Zamanian RT. Diagnosis and management of pulmonary hypertension associated with left ventricular diastolic dysfunction. Pulmonary Circulation. 2012;2(2):163–169. doi:10.4103/2045-8932.97598
35. Andersen KH, Andersen CB, Gustafsson F, et al. Pulmonary venous remodeling in COPD‐pulmonary hypertension and idiopathic pulmonary arterial hypertension. Pulmonary Circulation. 2017;7(2):514–521. doi:10.1177/2045893217709762
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.