Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Applying Target Trial Emulation to Evaluate Acupuncture Combined with Rehabilitation for Autism Spectrum Disorder in Children: A Retrospective Single-Center Real-World Protocol
Authors Wang X, Zhu RZ, Du XG, Song HJ
Received 26 August 2025
Accepted for publication 12 November 2025
Published 18 November 2025 Volume 2025:21 Pages 2513—2523
DOI https://doi.org/10.2147/NDT.S563199
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Roger Pinder
Xing Wang,1 Rui-Xuan Zhu,2 Xiao-Gang Du,1,* Hu-jie Song1,*
1Xi’an TCM Hospital of Encephalopathy, Shaanxi University of Chinese Medicine, Xi’an, Shaanxi, 710032, People’s Republic of China; 2First School of Clinical Medicine, Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, 712000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hu-jie Song, Xi’an TCM Hospital of Encephalopathy, Shaanxi University of Chinese Medicine, Xi’an, Shaanxi, 710032, People’s Republic of China, Email [email protected]
Background: Target trial emulation (TTE) has recently emerged as an innovative methodological framework for deriving causal inference from real-world data. Its use in complementary and integrative medicine, however, remains limited. This protocol applies TTE to evaluate the effectiveness of acupuncture combined with rehabilitation in children with ASD, aiming to generate rigorous real-world evidence and bridge the current evidence gap.
Methods: This retrospective TTE study will utilize anonymized data from the ASD registry of Xi’an TCM Hospital of Encephalopathy affiliated to Shaanxi University of Chinese Medicine. Children aged 2– 12 years diagnosed with ASD according to DSM-5 criteria will be included. The intervention group will receive rehabilitation therapy plus acupuncture, while the control group will receive standard rehabilitation therapy alone. A total of approximately 250– 300 participants will be included, ensuring at least 180 matched cases after propensity score matching. Statistical analyses will include paired t-tests, multivariable regression, and correlation analyses to estimate treatment effects and control for confounding. The TTE defines a clear time-zero (treatment initiation), prespecified censoring and crossover rules, and a causal estimand focusing on the average treatment effect among the treated (ATT). Balance diagnostics and sensitivity analyses will be performed to assess robustness.
Anticipated Results: This study is designed to evaluate whether acupuncture combined with rehabilitation leads to greater improvements in ATEC and ABC scores compared with rehabilitation alone. Exploratory neuroimaging analyses will be conducted to investigate potential mechanisms underlying treatment effects.
Conclusion: This protocol aims to evaluate the effectiveness of acupuncture combined with rehabilitation for children with ASD using a target trial emulation framework applied to real-world data. The study is designed to estimate the causal effect (ATT) while addressing confounding and missing-data issues, and its findings—whether positive or null—will inform future RCT design and the evidence-based integration of acupuncture in neurodevelopmental care.
Clinical Trial Number: Not applicable.
Keywords: autism spectrum disorder, acupuncture, target trial emulation, real-world evidence, RWE, rehabilitation
Introduction
Autism spectrum disorder (ASD) is a complex neurodevelopmental condition characterized by persistent deficits in social communication and interaction, alongside restricted and repetitive behaviors.1,2 Over the past decades, its prevalence has risen substantially worldwide. A systematic review reported that between 2012 and 2021, 71 studies from 34 countries provided 99 prevalence estimates, with a median prevalence of 100 per 10,000 children.3 Another study shows that the prevalence of ASD in Asia, America, Europe, Africa and Australia was between 0.4% to 1.7%.4 From 2017 to 2023, the prevalence of ASD in China was 7 per 1,000, showing an upward trend compared with the period before 2017.5 The increasing number of children with ASD poses significant challenges for healthcare systems, families, and society, as affected individuals often experience lifelong difficulties in education, social integration, and independent living.6,7 These challenges underscore the urgent need for effective and sustainable therapeutic strategies to improve clinical outcomes and quality of life.
Current standard treatments for ASD mainly consist of behavioral and developmental interventions, such as applied behavior analysis,8–10 speech and language therapy,11–13 and sensory integration training.14–16 While these approaches have demonstrated benefits, they typically require intensive and prolonged engagement, and therapeutic outcomes vary considerably between individuals.17 Pharmacological treatments are primarily targeted at comorbid behavioral symptoms such as irritability or hyperactivity, with limited efficacy for core deficits and potential risks of adverse effects with long-term use.18 These limitations highlight the need to explore complementary therapies that may augment standard care and address underlying pathophysiological mechanisms.
Acupuncture, a core modality of traditional Chinese medicine (TCM), has gained increasing attention as a complementary intervention for ASD.19,20 Preliminary clinical studies suggest that acupuncture may improve language, social interaction, and sensory behaviors in children with ASD.21 Potential mechanisms include modulation of brain functional connectivity,22 regulation of the gut–brain axis,23 and neuroimmune interactions.24 However, most existing studies, including randomized controlled trials (RCTs), are often limited by small sample sizes, difficulties in implementing credible sham acupuncture blinding, and high heterogeneity in acupoint selection and needling techniques. These methodological challenges have left the clinical effectiveness of acupuncture inconclusive and under debate. Therefore, robust evidence on its causal effectiveness remains lacking, and innovative analytical frameworks are required to bridge the gap between clinical practice and rigorous evidence generation.
Target trial emulation (TTE) has emerged as a novel methodological approach to evaluate causal effects using real-world data.25–27 By explicitly defining eligibility criteria, treatment strategies, follow-up periods, and outcomes in alignment with randomized controlled trials, TTE mitigate confounding and selection bias inherent in observational studies. It enables researchers to estimate treatment effects as if a hypothetical randomized trial had been conducted. Importantly, TTE is particularly suited for interventions such as acupuncture, where blinding and placebo control are challenging, and where extensive real-world clinical data are available. Compared with traditional RCTs, this approach enhances feasibility, reduces ethical constraints, and improves external validity by reflecting real-world clinical conditions. Recent methodological developments have further standardized the use of TTE and real-world evidence (RWE) frameworks in clinical research, strengthening the causal interpretation of observational data.28
Given the limitations of current ASD treatments and the methodological challenges in acupuncture research, TTE offers a promising alternative to generate high-quality real-world evidence. However, to date, no study has applied a formal TTE framework to evaluate acupuncture for ASD. The present study aims to address this research gap by applying TTE to assess the effectiveness of acupuncture combined with rehabilitation therapy in improving the core symptoms of children with ASD. Using data from a comprehensive ASD registry, this study seeks to generate high-quality real-world evidence that may complement traditional RCTs, elucidate potential neural mechanisms, and inform the development of evidence-based acupuncture protocols for neurodevelopmental disorders.
Study Objectives
Primary objective: To evaluate the effectiveness of acupuncture combined with rehabilitation therapy in improving core symptoms of children with ASD, measured by changes in ATEC scores.
Secondary objective: To assess changes in ABC scores and exploratory multimodal neuroimaging indicators, examining potential alterations in brain connectivity associated with acupuncture intervention and their relationships with clinical improvements.
Hypotheses
Acupuncture combined with rehabilitation will lead to greater improvement in ATEC scores compared to rehabilitation alone.
Changes in ABC scores and neuroimaging metrics will be consistent with improvements in ATEC scores and correlate with clinical outcomes.
TTE Study Design and Data Source
This study employs the TTE approach to simulate a randomized controlled trial, thereby minimizing the confounding and selection biases commonly encountered in traditional observational studies and enhancing the reliability of causal inference regarding the efficacy of acupuncture. The data for this study are derived from the ASD specialty database of Xi’an TCM Hospital of Encephalopathy affiliated to Shaanxi University of Chinese Medicine, which contains retrospective clinical records of pediatric patients diagnosed with ASD according to DSM-5 criteria. The registry includes 5,648 cases admitted between January 2013 and April 2025. Data encompass demographic characteristics, diagnostic information, treatment histories (including rehabilitation and acupuncture), behavioral scale assessments (ATEC, ABC), and available neuroimaging findings. The workflow of the study is shown in Figure 1.
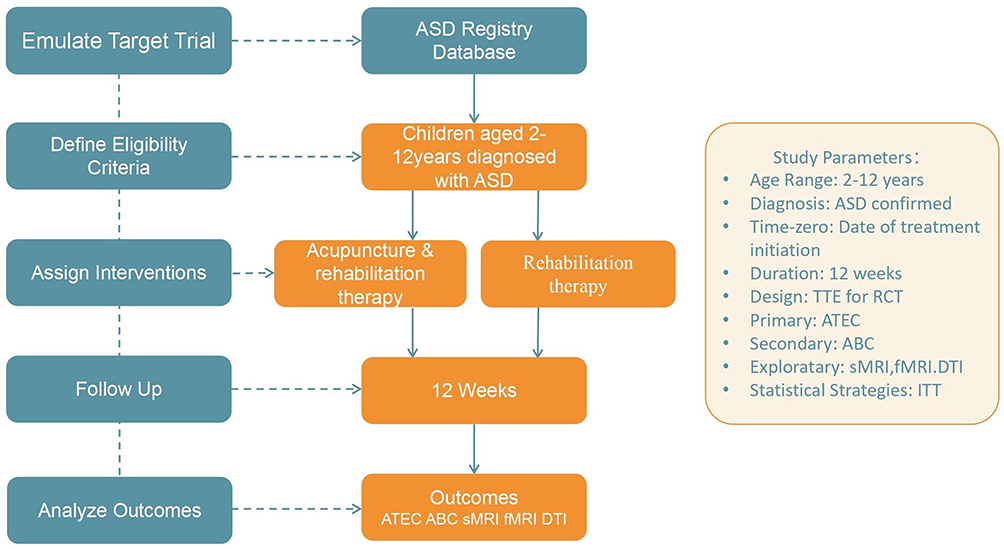 |
Figure 1 Target trial emulation framework for evaluating acupuncture combined with rehabilitation in children with ASD. Abbreviations: ASD, autism spectrum disorder; ATEC, Autism Treatment Evaluation Checklist; ABC, Aberrant Behavior Checklist; sMRI, structural magnetic resonance imaging; fMRI, functional magnetic resonance imaging; DTI, diffusion tensor imaging; TTE, target trial emulation; ITT, intention-to-treat. |
Time-zero was defined as the date of treatment initiation. Follow-up continued for 12 weeks, with censoring applied at treatment discontinuation, loss to follow-up, or completion of the observation window. Exposure was defined as receiving ≥2 acupuncture sessions per week for ≥12 weeks in the treatment group, or the same duration of rehabilitation in the control group.
The ASD database of Xi’an TCM Hospital of Encephalopathy is under the supervision of the hospital’s Ethics Committee. It is a closed database, accessible only to authorized investigators within the institution. The database has undergone internal validation and quality control procedures consistent with national data governance standards but is not publicly available to external researchers due to patient privacy protection.
Prior to conducting the emulation using observational data, we explicitly defined the protocol of the hypothetical target trial. The eligibility criteria for study participants are as follows:
Inclusion Criteria
- Children aged 2–12 years.Diagnosis of ASD according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria.29
- Availability of complete intervention records, including acupuncture or conventional rehabilitation therapy, with a treatment frequency of ≥2 sessions per week and a treatment duration of ≥12 weeks.
- Completion of at least one pre-intervention and one post-intervention assessment of Autism Treatment Evaluation Checklist (ATEC).
- If (ABC) scores are also available, these cases will be included in the secondary outcome analysis.
- For participants included in the neuroimaging subgroup analysis, availability of structural MRI (sMRI), functional MRI (fMRI), and diffusion Tensor Imaging (DTI) data, with the interval between imaging and scale assessment ≤2 weeks.
Exclusion Criteria
- Absence of complete primary outcome data: failure to complete either the pre-intervention or post-intervention ATEC assessment.
- Severe missing data in clinical records or neuroimaging data, defined as >20% missingness.
- Coexisting severe intellectual disability or developmental delay, or comorbid genetic/metabolic disorders or neurodegenerative diseases that significantly affect neurodevelopment.
- Poorly controlled epileptic seizures or frequent adjustments to antiepileptic medications during the intervention period.
- Receipt of other concurrent interventions. Patients included in this study primarily received acupuncture combined with rehabilitation therapy, without concurrent use of pharmacological interventions beyond standard supportive care.
Intervention Methods
Control Group
Participants in the control group received standard rehabilitation therapy, comprising behavioral interventions (eg, applied behavior analysis and social skills training), speech and language therapy, and occupational/sensory integration training. These interventions were designed to ameliorate core symptoms and enhance daily living skills in children with autism spectrum disorder.
Treatment Group
In addition to the control group treatment, participants received acupuncture therapy.
Acupoint selection: Baihui (GV20), Naohu (GV17), Speech Area I, Speech Area II, Speech Area III, Neiguan (PC6), Shenmen (HT7), Yongquan (KI1), and Xuanzhong (GB39).
Needling technique: For scalp points, filiform needles were inserted subcutaneously into the aponeurosis at a depth of 1–1.5 cun using a transverse insertion technique. Baihui and Speech Areas II–III were inserted anterior-to-posterior, while Speech Area I was inserted inferior-to-superior, closely along the periosteum. Strong stimulation was applied using a “drawing-qi” technique with approximately 10 thrust–lift manipulations until a marked inward pulling sensation (deqi) was achieved. Needles at scalp points were retained for 2 hours. For body acupoints, conventional perpendicular insertion was applied with a retention time of 20 minutes.
The acupoint prescription follows the Guidelines for Clinical Diagnosis and Treatment of Pediatrics in Traditional Chinese Medicine: Autism Spectrum Disorders.30 After body needle removal, children were accompanied by nursing staff and parents in a quiet setting to ensure safety until the scalp needles were withdrawn. Acupuncture procedures followed standardized hospital protocols.
As this study is retrospective, individual therapist adherence could not be formally evaluated, but treatment consistency was indirectly ensured by the inclusion criteria (≥2 sessions per week for ≥12 weeks).
For the randomization process within this TTE, propensity score matching (PSM) will be applied to balance baseline characteristics between the two groups. The “time 0” is defined as the date of treatment initiation.
Consideration of Treatment Adherence in Retrospective Data
This study is based on children who have already completed the treatment as documented in their medical records. The inclusion criteria inherently select for a cohort with adequate adherence. Therefore, specific strategies employed in clinical practice to ensure child cooperation during acupuncture (eg, behavioral shaping, parental presence, desensitization techniques), while crucial for the initial delivery of care, are not variables analyzed within the scope of this TTE study.
Outcome Measures
The outcome measures of this study are divided into three categories: primary outcomes, secondary outcomes, and exploratory outcomes, aiming to comprehensively evaluate the clinical efficacy and neurobiological mechanisms of acupuncture intervention in children with ASD. ATEC and ABC scores were assessed at baseline and 12 weeks by trained pediatric rehabilitation specialists who were not involved in the acupuncture procedures to reduce observer bias.
Primary Outcome
ATEC score. This scale comprises four domains-speech/language/communication, sociability, sensory/cognitive awareness, and health/behavior—and provides a comprehensive assessment of symptom improvement in children with ASD.31 Chinese version of the ATEC has high reliability and validity, and its score can reflect the severity of autistic symptoms and developmental level of ASD children,32 thus ensuring its suitability for assessing therapeutic effectiveness in the local context.
Secondary Outcome
ABC score. The ABC is designed to assess multiple behavioral characteristics, including sensory responses, social relationships, motor skills, self-care, and language. Comparison of scores from baseline to post-intervention will further validate the behavioral improvements observed with acupuncture and complement the findings from the ATEC assessment.33 The Chinese version of the ABC has good reliability and validity in Chinese ASD patient populations,34 supporting its use as a reliable behavioral outcome measure in this study.
Exploratory Outcomes
To elucidate the neuroimaging mechanisms underlying acupuncture intervention, multimodal neuroimaging measures will be included as exploratory outcomes to evaluate structural, functional, and hemodynamic brain changes in relation to clinical efficacy. Specifically:
sMRI: Voxel-based morphometry (VBM) will be used to assess cortical thickness and gray matter volume, with a focus on social and emotion-related regions such as the prefrontal cortex, amygdala, and cingulate gyrus.
fMRI: Resting-state functional connectivity (including the default mode network and social brain networks), regional homogeneity (ReHo), and amplitude of low-frequency fluctuation (ALFF) will be analyzed to explore the impact of acupuncture on brain functional network reorganization.
DTI: Integrity and microstructural changes of white matter tracts will be examined by quantifying fractional anisotropy (FA), axial diffusivity (AD), radial diffusivity (RD), and mean diffusivity (MD), with particular attention to tracts highly relevant to autism, such as the arcuate fasciculus, uncinate fasciculus, superior and inferior longitudinal fasciculi, inferior fronto-occipital fasciculus, cingulum bundle, and corpus callosum, and their associations with improvements in social function.
Neuroimaging analyses are exploratory in nature. Predefined regions of interest (ROIs) include the prefrontal cortex, amygdala, and cingulate gyrus, based on prior ASD neuroimaging literature. Multiple-comparison correction will be performed using false discovery rate (FDR) procedures to control for type I error.
Timing of Assessments
All outcome measures will be assessed at baseline (prior to intervention) and at 12 weeks after the intervention. The 12-week observation window represents the most consistent and complete follow-up period available in the clinical database. Although longer-term follow-up data exist for some patients, their timing is heterogeneous and will be explored in future prospective studies.
Sample Size Estimation
The sample size calculation is based on changes in the ATEC score as the primary outcome. According to previous studies and preliminary data, we expect an average improvement of approximately 3 points in the acupuncture group compared with the control group, with a standard deviation of about 6 points. Using a two-sided test with α = 0.05 and power = 80% (β = 0.2), the required sample size is at least 90 participants per group. Considering approximately 20% data loss in retrospective studies and additional loss due to propensity score matching, we plan to include 250–300 participants in total to ensure at least 180 matched participants (90 per group) for the primary analysis.
For neuroimaging analysis, which is a secondary outcome, approximately 20–30% of participants in the database are expected to have usable imaging data, yielding around 50–80 participants (25–40 per group) for exploratory analyses. No separate power calculation will be performed for this subgroup.
Participant Characteristics
Baseline demographic and clinical characteristics, including age, sex, duration of ASD, baseline ATEC and ABC scores, will be summarized for both the acupuncture plus rehabilitation group and the rehabilitation-only group. Continuous variables will be presented as means ± standard deviations, and categorical variables as frequencies and percentages. Between-group differences before and after propensity score matching will be assessed using independent-sample t-tests or chi-square tests, as appropriate. A summary table of participant characteristics will be provided to illustrate baseline comparability.
Statistical Analysis
The causal estimand corresponds to the average treatment effect among the treated (ATT). Effect estimates will be reported with 95% confidence intervals. PSM will be performed to emulate randomization using key baseline variables, including age, sex, duration of ASD, baseline ATEC and ABC scores. A 1:1 nearest-neighbor matching with a caliper width of 0.1--0.2 will be applied. Covariate balance between groups will be rigorously assessed using standardized mean differences (SMD), with successful matching defined as all covariates achieving SMD < 0.1.
The primary outcome, the change in ATEC scores, will be analyzed based on an emulated intention-to-treat (ITT) principle. A linear regression model will be used for the between-group comparison, adjusting for any residual imbalances in baseline characteristics to estimate the average treatment effect. Paired t-tests will be employed for within-group comparisons.
Secondary outcomes, including changes in ABC scores and multimodal neuroimaging measures, will be analyzed descriptively and using correlation analyses to explore relationships with clinical improvements. Missing data will be addressed using multiple imputation. All tests will be two-sided, with the significance level set at p < 0.05. All analyses will be conducted using R (version 4.3.3).
Anticipated Results
We anticipate that the acupuncture combined with rehabilitation group will demonstrate significantly greater improvements in ATEC scores compared to the rehabilitation-only group, supporting our primary hypothesis. For secondary outcomes, we expect corresponding improvements in ABC scores and observable changes in neuroimaging metrics, particularly in brain regions and networks associated with social communication and sensory processing. These findings would provide real-world evidence for the additive benefit of acupuncture in ASD management and offer preliminary insights into its potential neural mechanisms.
The results of this TTE study are expected to contribute meaningful evidence to the field of integrative medicine for ASD, potentially informing future randomized controlled trials and clinical practice guidelines.
Data Management
All analyses will be conducted using R (version 4.3.3) with scripted workflows to ensure reproducibility. Missing data patterns will be examined, and multiple imputation by chained equations will be used to address incomplete variables. All personal identifiers will be removed to ensure anonymity. The files will be password protected, and access will be restricted to authorized research team members only. Data entry and organization will involve double-checking by two team members to ensure accuracy. Regular data cleaning will be performed to identify and address missing values and anomalies. Multiple imputation methods will be applied to handle missing data where appropriate. Data will be regularly backed up and stored securely to prevent data loss and maintain data integrity. Quality control procedures include double data checking, validation of imputation results, and secure version-controlled data storage.
Discussion
The novelty of this study lies in evaluating acupuncture for ASD while demonstrating the feasibility of applying TTE in complementary medicine. By estimating causal effects from real-world data, this design offers a methodological advance over conventional observational studies and provides a practical template for future research where randomized trials are challenging.
TTE explicitly defines eligibility, intervention, follow-up, and outcomes to approximate the causal inference of randomized trials within observational datasets.35,36 The TTE in this study was explicitly defined: the intervention group received acupuncture combined with rehabilitation training, while the control group underwent rehabilitation training alone; the study population was restricted to ASD children aged 2–12 years; the primary outcome was the ATEC score, and the secondary outcomes included the ABC score and multimodal neuroimaging measures. Confounding factors such as age, sex, and baseline disease severity were addressed using the PSM method, thereby reducing both selection bias and confounding bias. Although double-blinding typical of RCTs could not be implemented due to the retrospective nature of the data, potential evaluation bias was mitigated through standardized data extraction procedures and rigorous quality control measures during outcome assessment. Compared with conventional RCTs, this design has several practical advantages: no additional participant recruitment, reduced ethical risks and costs, and particular suitability for interventions with substantial clinical data. Nonetheless, its limitations must be acknowledged: PSM can only account for measured confounders, and unmeasured variables (eg, home environment, psychosocial support) may still introduce residual bias.
The mechanisms underlying the therapy of acupuncture in ASD constitute an important theoretical foundation for this study, integrating insights from modern neuroscience with the holistic principles of TCM. From a biomedical perspective, acupuncture may exert multi-target effects, including: (1) Neurotransmitter modulation: Acupuncture activates mesolimbic and mesocortical pathways, promoting balanced release and reuptake of monoamine neurotransmitters such as serotonin and dopamine.37–39 This mechanism may underpin improvements in emotional dysregulation and stereotyped behaviors in ASD. (2) Neuroplasticity enhancement: fMRI studies demonstrate that acupuncture increases connectivity within the default mode network (DMN) and prefrontal–temporal language networks in children with ASD, correlating with gains in communication abilities.40,41 (3) Neuroinflammation regulation: Stimulation of specific acupoints suppresses excessive microglial activation and reduces proinflammatory cytokines such as IL-6 and TNF-α, mitigating neuroinflammatory damage to synaptic development.42–44 These effects are consistent with the hypothesized pathophysiological sequence in ASD involving neurodevelopmental abnormalities, immune dysregulation, and neuroinflammation. In TCM theory, ASD is associated with patterns such as “five delays” and “five weaknesses”, reflecting disharmony among the heart, liver, spleen, and kidney.45,46 The acupuncture protocol integrates scalp and body points to harmonize the heart–brain–kidney axis This strategy aims to awaken the mind, open sensory orifices, and enhance speech and social functions: GV20 and GV17 are employed to activate cerebral functions and harmonize Yang, while Speech Areas I–III target the tongue meridians to promote language recovery.47–49 PC6 and HT7 calm the mind and regulate emotional disturbances, KI1 nourishes the kidney–brain axis and stabilizes neuroendocrine balance, and GB39, as the Convergent Point of Marrow, supports neurodevelopment.50–52 Collectively, these acupoints harmonize the Heart–Brain–Kidney functional network, open sensory orifices, and contribute to improvements in cognition and core autism symptoms. Emerging evidence from neuroimaging and physiological studies provides preliminary support for this TCM strategy, showing that stimulation of key acupoints like GV20 can modulate brain network connectivity, while body points such as HT7 and PC6 may regulate emotional and autonomic nervous system functions.53,54 Thus, the integrative approach of “head acupuncture to regulate the mind and body acupuncture to harmonize the viscera” reflects TCM’s holistic concept of “nourishing both form and spirit”, corroborated by modern findings on neurodevelopmental and immune modulation.
If future analyses confirm similar patterns, the findings could have several clinical implications. First, acupuncture may provide a safe alternative for children with poor response to pharmacological treatment or whose parents decline long-term psychotropic use; Second, as an adjunct to rehabilitation, acupuncture could shorten therapy duration—for example, modulation of oral sensory processing may accelerate speech training, and vestibular stimulation may enhance sensory integration training; Third, acupuncture may be particularly beneficial in early intervention when neuroplasticity is maximal, conferring stronger neuroprotective effects. However, several challenges must be addressed for broader clinical adoption: variability in acupuncture techniques (eg, acupoint selection, needling depth, and manipulation) across practitioners may affect outcomes;55 some children with ASD may exhibit heightened sensitivity or resistance to needling;56 and synergistic mechanisms between acupuncture and other interventions require further investigation through large-sample studies.
Beyond immediate clinical findings, this study holds broader methodological significance for the evidence-based evaluation of TCM interventions. On one hand, leveraging real-world data overcomes the limitations of traditional RCTs, such as small sample sizes and prolonged timelines, enabling validation of acupuncture’s therapeutic effects at the population level.57 On the other hand, integrating multimodal clinical indicators and behavioral outcomes may promote the transition of acupuncture research toward precision medicine.58 For example, future combination of machine learning with four-diagnostic data and behavioral scales could facilitate predictive modeling of individualized responses. Further research should expand to multicenter real-world studies to assess generalizability, incorporate multi-omics approaches (eg, microbiome, metabolomics) to elucidate the “acupuncture–brain–gut–immune” regulatory network, evaluate long-term outcomes and cost-effectiveness to inform health policy, and develop intelligent acupuncture devices to enhance standardization and accessibility of care. Overall, the present protocol focuses on methodological feasibility rather than clinical inference, providing a structured framework for subsequent real-world evaluations of acupuncture in ASD.
Limitations
Several limitations should be acknowledged. First, the single-center design may limit generalizability due to potential regional and cultural differences. Second, standardization of the intervention remains challenging. Despite structured database annotations (eg, acupoint selection, frequency, treatment course), subtle variations in acupuncture techniques—such as needle angle and manipulation intensity—could influence therapeutic outcomes. Third, subjectivity in outcome assessment cannot be completely eliminated. Although standardized scales were used, subjective ratings could still introduce bias; incorporating objective biomarkers in future studies may address this issue. Fourth, long-term efficacy was not assessed; the study focused on a 12-week observation window and lacked extended follow-up data to determine the durability of treatment effects. Most importantly, as an observational study emulating a target trial, our findings are susceptible to residual confounding from unmeasured variables (eg, parenting style, psychosocial support, and home-based interventions). Furthermore, the exploratory neuroimaging analysis is constrained by the inherent challenges of retrospective data, including heterogeneity in scanning protocols and the lack of a prospectively standardized imaging pipeline. These limitations highlight the need for future studies to adopt multicenter collaboration, standardized operator training, incorporation of multimodal objective measures (eg, EEG, microbiome data), as well as long-term follow-up designs to enhance the reliability and translational value of the findings.
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Ethics Approval and Consent to Participate
This study strictly adheres to the ethical principles of medical research outlined in the Declaration of Helsinki, aiming to protect the rights and dignity of research subjects. The study protocol has been reviewed and approved by the Ethics Committee of Xi’an TCM Hospital of Encephalopathy affiliated to Shaanxi University of Chinese Medicine (Approval No.: XNLL-2025-018).
As this study uses only anonymized and de-identified existing clinical data and does not involve any additional intervention on patients, the Ethics Committee has waived the requirement for re consent. Patient privacy will be strictly protected throughout the study, and all applicable laws, regulations, and institutional data security policies will be followed. The study data access and analysis followed institutional data governance policies.
Acknowledgments
The authors would like to thank all the participants for their support and cooperation during this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Project of Shaanxi Administration of Traditional Chinese Medicine (2025-CXRC-28), the National Key R&D Program of China (2024YFC3507304) and Yong Talent Project of Xi’an Yingcai Program (2024).
Disclosure
The authors declare that they have no conflicts of interest related to this study.
References
1. Hirota T, King BH. Autism spectrum disorder: a review. J JAMA. 2023;329(2):157–168. doi:10.1001/jama.2022.23661
2. Qin L, Wang H, Ning W, Cui M, Wang Q. New advances in the diagnosis and treatment of autism spectrum disorders. Eur J Med Res. 2024;29(1):322. doi:10.1186/s40001-024-01916-2
3. Zeidan J, Fombonne E, Scorah J, et al. Global prevalence of autism: a systematic review update. Autism Res. 2022;15(5):778–790. doi:10.1002/aur.2696
4. Salari N, Rasoulpoor S, Rasoulpoor S, et al. The global prevalence of autism spectrum disorder: a comprehensive systematic review and meta-analysis. Italian J Pedia. 2022;48(1):112. doi:10.1186/s13052-022-01310-w
5. Jiang X, Chen X, Su J, Liu N. Prevalence of autism spectrum disorder in mainland China over the past 6 years: a systematic review and meta-analysis. BMC Psychiatry. 2024;24(1):404. doi:10.1186/s12888-024-05729-9
6. Hus Y, Segal O. Challenges surrounding the diagnosis of autism in children. Neuropsych Dis Treatment. 2021;Volume 17:3509–3529. doi:10.2147/NDT.S282569
7. Fombonne E, MacFarlane H, Salem AC. Epidemiological surveys of ASD: advances and remaining challenges. J Autism Develop Disord. 2021;51(12):4271–4290. doi:10.1007/s10803-021-05005-9
8. Gitimoghaddam M, Chichkine N, McArthur L, Sangha SS, Symington V. Applied behavior analysis in children and youth with autism spectrum disorders: a scoping review. Perspective Behav Sci. 2022;45(3):521–557. doi:10.1007/s40614-022-00338-x
9. Chung K-M, Chung E, Lee H. Behavioral interventions for autism spectrum disorder: a brief review and guidelines with a specific focus on applied behavior analysis. J Korean Acad Child Adoles Psychiatry. 2024;35(1):29. doi:10.5765/jkacap.230019
10. Esposito M, Fadda R, Ricciardi O, Mirizzi P, Mazza M, Valenti M. Ins and outs of applied behavior analysis (ABA) intervention in promoting social communicative abilities and theory of mind in children and adolescents with ASD: a systematic review. Behav Sci. 2025;15(6):814. doi:10.3390/bs15060814
11. Нryntsiv M, Zamishchak M, Bondarenko Y, Suprun H, Dushka A. Approaches to speech therapy for children with autism spectrum disorders (ASD). Int J. 2025;14(1):33.
12. Sourvinos S, Mavropoulos A, Kasselimis DS, et al. Brief report: speech and language therapy in children with ASD in an aquatic environment: the ASLT (aquatic speech and language therapy) program. J Autism Develop Disord. 2021;51(4):1406–1416. doi:10.1007/s10803-020-04629-7
13. Christopoulou M, Drosos K, Petinou K. Recent advances of telepractice for autism spectrum disorders in speech and language pathology. Neuropsych Dis Treatment. 2022;2379–2389. doi:10.2147/NDT.S384300
14. Camino-Alarcón J, Robles-Bello MA, Valencia-Naranjo N, Sarhani-Robles A. A systematic review of treatment for children with autism spectrum disorder: the sensory processing and sensory integration approach. Children. 2024;11(10):1222. doi:10.3390/children11101222
15. Shu D, Zhang G, Xue C, et al. Intervention effect of group sensory integration training on social responsiveness and N170 event-related potential of children with autism. Behav Sci. 2024;14(3):202. doi:10.3390/bs14030202
16. Randell E, Wright M, Milosevic S, et al. Sensory integration therapy for children with autism and sensory processing difficulties: the SenITA RCT. Health Technol Assess. 2022;26(29):1–140. doi:10.3310/TQGE0020
17. Ozsahin I, Mustapha MT, Albarwary S, Sanlidag B, Ozsahin DU, Butler TA. An investigation to choose the proper therapy technique in the management of autism spectrum disorder. J Comp Effect Res. 2021;10(5):423–437. doi:10.2217/cer-2020-0162
18. Davico C, Secci I, Vendrametto V, Vitiello B. Pharmacological treatments in autism spectrum disorder: a narrative review. J Psychopathol. 2023.
19. Wang L, Peng J-L, Qiao F-Q, et al. Clinical randomized controlled study of acupuncture treatment on children with autism spectrum disorder (ASD): a systematic review and meta‐analysis. Evid Based Complmen Alternat Med. 2021;2021(1):5549849. doi:10.1155/2021/5549849
20. Zhang Y, Zeng J, Wu D, et al. Effect and safety of acupuncture for autism spectrum disorders: a protocol for systematic review and meta-analysis. Medicine. 2021;100(11):e22269. doi:10.1097/MD.0000000000022269
21. Su T, Pei L. Acupuncture and oxytocinergic system: the promising treatment for autism. Transl Neurosci. 2021;12(1):96–102. doi:10.1515/tnsci-2021-0011
22. Chen J, Li H, Zhong D, et al. A bibliometric analysis of acupuncture for neurodevelopmental disorders: a Call for increased output and future research priorities. Heliyon. 2023;9(12):e22799. doi:10.1016/j.heliyon.2023.e22799
23. Wang J, Liu Y, Huang H-Y, Wu J-T, Wang W-J. Influence of acupuncture on the clinical manifestations and gastrointestinal symptoms of children with autism spectrum disorder. Chin Acupunct Moxibust. 2022;42(12):1373–1376. doi:10.13703/j.0255-2930.20220111-0004
24. Zhao P, Fu H, Cheng H, et al. Acupuncture at ST36 alleviates the behavioral disorder of autistic rats by inhibiting TXNIP-mediated activation of NLRP3. J Neuropathol Exp Neurol. 2022;81(2):127–134. doi:10.1093/jnen/nlab132
25. Habibdoust A, Zuo H, Koopman RJ, Gupta A, Mazzotti DR, Song X. Target trial emulation applications in hypertension research: a scoping review. medRxiv. 2025;
26. Kwee SA, Wong LL, Ludema C, et al. Target trial emulation: a design tool for cancer clinical trials. JCO Clin Cancer Inform. 2023;7(7):e2200140. doi:10.1200/CCI.22.00140
27. Zuo H, Yu L, Campbell SM, Yamamoto SS, Yuan Y. The implementation of target trial emulation for causal inference: a scoping review. J Clin Epidemiol. 2023;162:29–37. doi:10.1016/j.jclinepi.2023.08.003
28. Hernán MA, Robins JM. Using big data to emulate a target trial when a randomized trial is not available. Amer j epidemiol. 2016;183(8):758–764. doi:10.1093/aje/kwv254
29. Ma F. Diagnostic and statistical manual of mental disorders-5 (DSM-5). In: Encyclopedia of Gerontology and Population Aging. Springer; 2022:1414–1425.
30. Ningxia Z, Hujie S, Xiaogang D, et al. Guidelines for clinical diagnosis and treatment of pediatrics in traditional Chinese medicine: autism spectrum disorders. China J Trad Chin Med Pharm. 2023;38(07):3231–3236.
31. Martinez S. Autism treatment evaluation checklist (ATEC) norms: a “growth chart” for ATEC score changes as a function of age. Children. 2025.
32. Fang H, Yanling R, Li C, Xiaoyan K. Reliability and validity of the Chinese version of autism treatment evaluation checklist. Sichuan Mental Health. 2019;32(6):518.
33. Cassidy A. Autism behavior checklist. In: Encyclopedia of Autism Spectrum Disorders. Springer; 2021:462–463.
34. Kat S, Xu L, Guo Y, et al. Reliability and validity of the simplified Chinese version of the aberrant behavior checklist in Chinese autism population. Front Psychiatry. 2020;11:545445. doi:10.3389/fpsyt.2020.545445
35. Yang J, Wang L, Chen L, et al. A comprehensive step-by-step approach for the implementation of target trial emulation: evaluating fluid resuscitation strategies in post-laparoscopic septic shock as an example. Laparoscopic Endoscopic Robotic Surg. 2025;8(1):28–44. doi:10.1016/j.lers.2025.01.001
36. Li H, Zang C, Xu Z, et al. Federated target trial emulation using distributed observational data for treatment effect estimation. Npj Digital Med. 2025;8(1):387. doi:10.1038/s41746-025-01803-y
37. Ma J, Yin X, Cui K, Wang J, Li W, Xu S. Mechanisms of acupuncture in treating depression: a review. ChinMed. 2025;20(1):29. doi:10.1186/s13020-025-01080-7
38. Wang X, Wang J, Han R, Yu C, Shen F. Neural circuit mechanisms of acupuncture effect: where are we now? Front Neurol. 2024;15:1399925. doi:10.3389/fneur.2024.1399925
39. Li H, Xiang Q, Ren R, Wang G. Acupuncture as a complementary therapy for Alzheimer’s disease. J Alzheimers Dis. 2024;101(s1):S503–S520. doi:10.3233/JAD-231250
40. Wang Q, Li H-Y, Li Y-D, et al. Resting-state abnormalities in functional connectivity of the default mode network in autism spectrum disorder: a meta-analysis. Brain Imaging Behav Sci. 2021;15(5):2583–2592. doi:10.1007/s11682-021-00460-5
41. Cong J, Zhuang W, Liu Y, et al. Altered default mode network causal connectivity patterns in autism spectrum disorder revealed by Liang information flow analysis. Human Brain Mapp. 2023;44(6):2279–2293. doi:10.1002/hbm.26209
42. Li N, Guo Y, Gong Y, et al. The anti-inflammatory actions and mechanisms of acupuncture from acupoint to target organs via neuro-immune regulation. J Inflamm Res. 2021;Volume 14:7191–7224. doi:10.2147/JIR.S341581
43. Liu J, Zhou J, You C, et al. Research progress in the mechanism of acupuncture regulating microglia in the treatment of Alzheimer’s disease. Front Neurosci. 2024;18:1435082. doi:10.3389/fnins.2024.1435082
44. Yu W-L, Park J-Y, Park H-J, Kim S-N. Changes of local microenvironment and systemic immunity after acupuncture stimulation during inflammation: a literature review of animal studies. Front Neurol. 2023;13:1086195. doi:10.3389/fneur.2022.1086195
45. Hao N, Song Q. Advances in Chinese and Western medicine research on autism spectrum disorders. Soc Med Health Manag. 2023;4(2):21–28.
46. Sun P. Application of shen regulation with acupuncture in the treatment of children with autism. Inter J Clin Acupunct. 2022;31(3).
47. Liu D-N, Zhou J, Huang X-R, et al. Effect of electroacupuncture at “Shuigou”(GV26) and “Baihui”(GV20) on autophagy of hippo-campal neurons in rats with cerebral ischemia-reperfusion injury. Acupuncture Res. 2022;47(6):491–496. doi:10.13702/j.1000-0607.20210561
48. Ye M, Fan AY, Wang H, Hu ZD. Xuelong Huang, the earliest founder of “scalp acupuncture-zones therapy”. Med Acupuncture. 2025.
49. Richards LG, Cramer SC. Therapies targeting stroke recovery. Stroke. 2023;54(1):265–269. doi:10.1161/STROKEAHA.122.041729
50. Cong L, Yu X, Huang M, et al. Enhancing emotion regulation: investigating the efficacy of transcutaneous electrical acupoint stimulation at PC6 in reducing fear of heights. Front Psychol. 2024;15:1371014. doi:10.3389/fpsyg.2024.1371014
51. Du L, Song X-J, Li Z-W, Liao L-X, Zhu Y-H. Combined use of Shenmen (HT 7) and Sanyinjiao (SP 6) to improve the anxiety and depression in patients with insomnia: a randomized controlled trial. Chin Acupunct Moxibust. 2022;42(1):13–17. doi:10.13703/j.0255-2930.20210113-k0002
52. Ziyue Y, Weihua Z. Professor Zhang Weihua’s clinical experience in the application of Yongquan acupoint. Modern Health Sci. 2025;8(1):131–p131. doi:10.30560/mhs.v8n1p131
53. Duan G, He Q, Pang Y, et al. Altered amygdala resting-state functional connectivity following acupuncture stimulation at BaiHui (GV20) in first-episode drug-Naïve major depressive disorder. Brain Imaging Behav Sci. 2020;14(6):2269–2280. doi:10.1007/s11682-019-00178-5
54. Li Y-W, Li W, Wang S-T, et al. The autonomic nervous system: a potential link to the efficacy of acupuncture. Front Neurosci. 2022;16:1038945. doi:10.3389/fnins.2022.1038945
55. Vickers AJ, Vertosick EA, Lewith G, et al. Do the effects of acupuncture vary between acupuncturists? analysis of the acupuncture trialists’ collaboration individual patient data meta-analysis. Acupuncture Med. 2021;39(4):309–317. doi:10.1177/0964528420959089
56. Dobson O, Symons FJ, McMurtry CM. Making needle procedures comfortable for autistic children: caregiver perspectives. Res Autism Spectrum Disord. 2023;107:102208. doi:10.1016/j.rasd.2023.102208
57. Borkar DS, Parke DW, Lee AY. Leveraging real-world evidence to enhance clinical trials. Ophthalmology. 2024;131(7):756–758. doi:10.1016/j.ophtha.2024.04.014
58. Bao Y, Ding H, Zhang Z, et al. Intelligent acupuncture: data-driven revolution of traditional Chinese medicine. Acupunct Herbal Med. 2023;3(4):271–284. doi:10.1097/HM9.0000000000000077
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture Ameliorated Behavioral Abnormalities in the Autism Rat Model via Pathways for Hippocampal Serotonin

Chen S, Huang L, Liu G, Kang J, Qian Q, Wang J, Wang R, Zheng L, Wang H, Ou P
Neuropsychiatric Disease and Treatment 2023, 19:951-972
Published Date: 18 April 2023
Study on the Therapeutic Effect of Yu-Mu-Tiao-Shen Acupuncture on Rats with Autism Spectrum Disorder
Jia Q, Wang X, Li Z, Li W, Jia R, Yue Z, Zhu Z, Ma B
Neuropsychiatric Disease and Treatment 2025, 21:2195-2210
Published Date: 25 September 2025