Back to Journals » Risk Management and Healthcare Policy » Volume 18
Applying Quality Improvement Science to Patient Safety: Strategies, Frameworks, and Sustainable Solutions
Authors Madine M, Simsekler MCE ![]() , Salah K, Ellahham S
, Salah K, Ellahham S
Received 1 September 2025
Accepted for publication 22 November 2025
Published 4 December 2025 Volume 2025:18 Pages 3781—3791
DOI https://doi.org/10.2147/RMHP.S564459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Keon-Hyung Lee
Mohammad Madine,1 Mecit Can Emre Simsekler,2 Khaled Salah,1 Samer Ellahham3
1Department of Computer and Information Engineering, Khalifa University of Science & Technology, Abu Dhabi, United Arab Emirates; 2Department of Management Science & Engineering, Khalifa University of Science & Technology, Abu Dhabi, United Arab Emirates; 3Quality & Patient Safety Institute, Cleveland Clinic Abu Dhabi, Abu Dhabi, United Arab Emirates
Correspondence: Mecit Can Emre Simsekler, Department of Management Science & Engineering, Khalifa University of Science & Technology, Abu Dhabi, United Arab Emirates, Tel +97123124058, Email [email protected]
Abstract: Healthcare is a constantly evolving field enriched by new technologies, medications, and treatment methods. However, these continuous innovations also introduce new complexities that can pave the way for medical errors to arise. As a result, quality of care and patient safety are always at stake, highlighting the imperative to set up processes to avoid errors in healthcare at any cost. This need for systematic approaches has led to the adoption of Quality Improvement Science (QIS), which deals with the early identification of problems and suggests ways to prevent them in a proactive manner. This study explores the principles of QIS as applied to patient safety, examining various approaches and proposing strategies to implement effective solutions. It further investigates methods for constant quality improvement, emphasizing the roles of technology and human resources in enhancing healthcare quality and patient safety. In particular, it studies how artificial intelligence (AI) strengthens information gathering and organization to provide practical insights. Furthermore, this study discusses the enablers and barriers to successful implementation of these quality improvement processes. Crucially, this paper provides a comprehensive and actionable framework for selecting appropriate QIS tools and indicators, developed through a structured synthesis of QIS literature and represented as decision flows that enable systematic care delivery problem identification and analysis.
Keywords: patient safety, risk management, quality improvement science, quality of care, healthcare sustainability
Introduction
The core of any healthcare endeavor is to provide safe and efficient patient care. This requires continuous evaluation to enhance patient experience and outcomes.1 Additionally, high-quality care should be affordable and integrate the latest technology into its delivery model. Healthcare quality has, therefore, been a long-standing subject of discussion. For instance, in 2006, the World Health Organization (WHO) defined quality of care as “a process for making strategic choices in health systems”.2 Similarly, in 2013, the Institute of Medicine (IOM) defined healthcare quality as the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.3 However, despite several initiatives aimed at improving healthcare quality and safety, these goals remain largely unmet. Challenges persist in reducing medical errors,4 implementing evidence-based practice,5 reducing healthcare disparities,6 achieving care variation reductions (CVRs),7 and eliminating redundant and wasted resources.3
Consequently, quality-related challenges in healthcare stem from overuse, underuse, and misuse. Overuse is a situation where potential harm from a healthcare product or service outweighs its benefits. Underuse is when a product or service that would likely provide a benefit was not provided, and misuse occurs when a product or service results in a preventable complication.8 Hence, healthcare organizations need to adopt defined principles to address overuse, underuse, and misuse, thereby enhancing healthcare quality and patient safety. The management principles outlined by W. Edwards Deming offer a framework through which involved organizations can improve healthcare quality and safety without resource wastage.6 This highlights the increasing importance of the concept of Quality Improvement Science (QIS), also known as the Science of Improvement. QIS is a scientific endeavor driven by goals and outcomes, aiming to bring about sustained, affordable, and meaningful improvement in healthcare quality and safety. It aims to bridge the gap between best practices and actual care delivery, helping to identify and mend the lacunae in healthcare delivery.
According to the Institute for Healthcare Improvement (IHI), the science of improvement is an applied science that emphasizes innovation, rapid-cycle testing in the field, and spread in order to generate learning about what changes, in which contexts, produce improvements.9 This applied science combines multidisciplinary expert knowledge with improvement methods and tools. Multidisciplinary teams draw experts from clinical science, systems theory, psychology, statistics, and other disciplines.10 QIS applies across healthcare products, service providers, organizations, policymakers, and regulatory agencies. Thus, QIS plays a substantial and continuous role in improving quality and reducing cost throughout the entire spectrum of healthcare.11 Given that improvement depends on trustworthy measurement and interpretation in care delivery, technological approaches for sensing, automation, and analytics are most effective when combined with human expertise. Accordingly, combining digital tools with patient-facing connections leads to more durable gains than either approach alone.
This study provides a detailed discussion on QIS, its role, and effective integration into the healthcare system for safety, timeliness, affordability, and continuous improvement. Building upon these foundations, this paper proposes a practical framework to guide healthcare professionals through the systematic application of QIS for patient safety. This proposed framework emerges from a structured analysis of quality improvement, as outlined in Figure 1. Furthermore, Figure 2 presents a high-level knowledge map visually interconnecting these concepts and highlighting the study’s depth.
 |
Figure 1 Roadmap outlining the progression of analysis on quality improvement science for patient safety. |
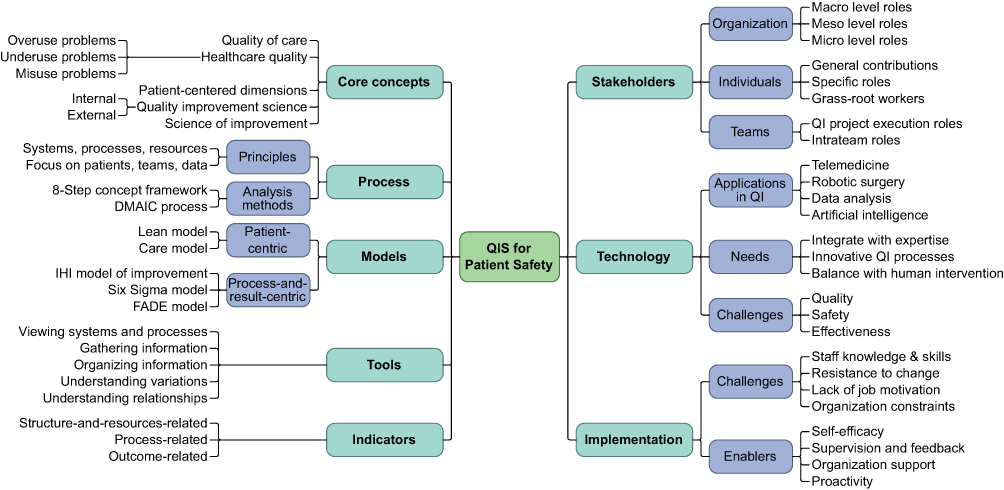 |
Figure 2 Comprehensive knowledge map illustrating the key concepts of quality improvement science in patient safety. |
The remainder of this paper is organized as follows: Section 2 discusses foundational concepts, processes, and models of quality improvement. Section 3 identifies the roles of stakeholders and technology. Section 4 explores available tools and indicators. Section 5 addresses implementation challenges and enablers. Section 6 presents a detailed discussion of the framework’s implications and challenges, and Section 7 concludes the study with key takeaways and future directions.
Background: Healthcare Quality Improvement
Effective quality provision requires clear and categorical definitions. Starting in 2001, the Institute of Medicine (IOM) emphasized patient-centered care as a key driver toward quality, highlighting its respect for patient values, preferences, and expressed needs; involvement of family and friends; assurance of physical comfort; provision of emotional support; coordination and integration; and informative, communicative, and educative aspects.3 While patients are the direct recipients of healthcare, and thus a primary focus, healthcare quality encompasses many other attributes not directly patient-centric, as its definition has evolved over time. The Agency for Healthcare Research and Quality (AHRQ) defines QI as “doing the right things and doing them right”, often associated with improved patient outcomes. This view of QI represents a more comprehensive indicator of quality compared to focusing solely on guideline-based therapies or safety.12 Earlier research identified four attributes defining healthcare quality: effectiveness, safety, having a culture of excellence, and achievement of desired outcomes. Based on these attributes, researchers defined healthcare quality as “the assessment and provision of effective and safe care, reflected in a culture of excellence, resulting in the attainment of optimal or desired health”.13
QI can be internal or external. Internal QI focuses on the clinician-patient relationship, aiming to increase patient and provider satisfaction by simplifying procedures, reducing costs, and enhancing medical care, care delivery, workplace morale, and productivity. External QI, conversely, emphasizes clinician education, health policies, accreditation, and certifications for benchmarking quality care.8 Healthcare organizations and practices utilize both forms of QI through quality control and quality assurance measures, to implement, measure, and improvise, forming the integral basis of QIS.
Quality Improvement Process
Though the QI process varies by need, it should align with available systems, processes, and resources, prioritizing patients, team involvement, and generated data.14 Healthcare delivery relies on specific clinical guidelines, comprising multiple steps. Accordingly, healthcare organizations are effectively clinical microsystems that involve providers and patients.15 Choosing and implementing QI projects in healthcare can be challenging, particularly when a QI process is initiated in response to an adverse event or patient complaint. Such incidents trigger urgent stakeholder meetings to identify rapid improvement measures and prevent recurrence. However, whenever possible, QI projects should be prioritized based on urgency and impact, or feasibility and need criteria.
Most healthcare organizations now incorporate some quality checks into their systems. However, evidence shows that despite these measures, some aspects of patient care improve while others worsen. This highlights the importance of identifying specific quality attributes that require prioritized focus,13 and analyzing the success or failure of various quality improvement efforts. Earlier research provided an eight-step concept analysis framework for examining healthcare quality: concept selection; aim and purpose of analysis; uses; quality attributes; constructing a model case; expanding the concept to similar and related cases; identification of antecedents and consequences; and defining the empirical referents.16
Another method for analyzing the quality is the five-phase Define, Measure, Analyze, Improve, Control (DMAIC) process.17 In the first step, the QI activity is defined, including its purpose, goals, and patient requirements. Next, performance of the QI activity is measured using various processes and analysis methods. Subsequently, a root cause analysis identifies failures and defects, after which the QI process is improved through different approaches. The final step establishes a quality control plan.18
AI applications are increasingly supporting patient care and quality improvement by enabling automated process monitoring and large-scale analysis of unstructured clinical information, thereby facilitating timely, patient-centered decisions.19
Models of Quality Improvement
The next challenge is to select the suitable QI model according to the need. All have several common characteristics such as setting the right goals; charting a structured path to achieve them cost-effectively, efficiently, and in a timely manner; ensuring accountability for roles in healthcare delivery; applying scrutiny and analysis; maintaining a constant improvement cycle; and upholding transparency.12 There are five primary types of improvement models: two are patient-centric in their approach, and three are process-and-result-centric. A summary of these models, including their primary focus, methodology, and guiding principles, is presented in Table 1.
 |
Table 1 Comparative Characterization of QI Models in Healthcare |
Patient-Centric Quality Improvement Models
Lean Model
This model is based on the patient’s perspective, mapping the value stream from patient needs. It emphasizes how value flows to the patient cost-effectively and in a timely manner.12
Care Model
This model promotes high-quality disease management and prevention by focusing on fundamental aspects of care. It engages patients in their own care and facilitates active interactions between patients and healthcare providers.
Process-and-Result-Centric Quality Improvement Models
The IHI’s Model for Improvement
Developed by Associates of Process Improvement (API) and based on W. Edwards Deming’s work,9 this model facilitates QIS application by defining the improvement aim, designing a specific idea and plan, and outlining measurement strategies. Small tests are then planned and executed, with lessons applied to larger test cycles, leading to effective and safely implementable solutions.20 Plan-Do-Study-Act (PDSA) cycles are the backbone of QI in healthcare. QI teams analyze extensive data to design these cycles, which involve repeated validity tests to adapt and implement the QI model effectively. Each cycle assesses the success of the intervention, continuing until a successful intervention is ready for implementation. Rapid cycle improvement (RCI) offers a more practical, real-time approach to testing QI changes. This method involves conducting several small, interlinked PDSA cycles concurrently within a physician practice to assess various care aspects, such as scheduling, diagnostics, and medication, allowing for improved quality and easy progress tracking. In larger hospitals, these cycles can be implemented physician-wise or department-wise.21
Six Sigma Model
The DMAIC approach is integral to the Six Sigma model.17 This model also uses the DMADV (Define, Measure, Analyze, Design, Verify) methodology for developing new processes.22
FADE Model
The FADE QI model involves four broad steps:23 Focus on the process to be improved; Analyze the data collected; Develop action steps for improvement; and Execute the action plans and evaluate and monitor the QI measure to ensure success.
Stakeholders and Technology
Organization
Micro, meso, and macro healthcare systems, and all individuals involved in healthcare delivery, bear responsibility for providing quality care safely, efficiently, and timely.24 At the macro level, national health systems contribute toward QI through regulatory systems, national policies and priorities, financing, and accreditation. At the meso level, hospitals advance QI by improving structures, cultures, practices, systems, processes, and strategies. They achieve this by recruiting, supporting, and retaining an efficient workforce; building quality- and safety-centric work processes; optimally utilizing generated data; and ensuring readily available technical resources to support improvement. At the micro-levels, organizational teams and departments focus on communication, competence, clinical and care models, professional work, and relational issues to contribute to QI.11 QI teams can brainstorm and analyze root causes of problems, assess their impact, plan successful QI initiatives, analyze results, and implement them. Various techniques like graphs, affinity diagrams, Pareto charts, storyboards, and voting can be employed. Practice Facilitators (PFs) and QI coaches can facilitate these brainstorming sessions. Initiatives starting at the micro-level can significantly impact meso and macro levels.8
Individuals
Individuals contribute to QI by focusing on patient orientation, building competency, improving work quality, sharing responsibility with managers, and fostering a cooperative work environment.25 Patients and the broader community also contribute by providing valuable feedback, which healthcare organizations and providers can use to enhance care delivery and experience.26 Frontline personnel doing grass-root work often possess the best solutions for further improvement. Effective communication among team members and easy connectivity with project leaders are vital for engaging the team, facilitating better solutions, and effectively achieving QI goals.27
Teams
For effective execution of a QI project, a team requires Specific, Measurable, Attainable, Relevant, and Time-bound (SMART) goals. Consequently, every QI project typically includes an expert lead and a project manager. The Expert provides subject matter guidance. The team leader, usually the project manager, plays a significant role in building a strong, purposeful team. A good team leader empowers everyone to work towards the goal and holds them accountable for their contributions.8 While there is no absolute rule regarding team size, a group of 5 to 15 members usually works effectively. Very small teams often face resource crunch, whereas overly large teams complicate execution and coordination. Nevertheless, no team can be effectively managed and channeled toward a QI goal without dedicated, committed leadership and fully accountable members.8
Technology
Technology is revolutionizing healthcare delivery and has resulted in new healthcare delivery microsystems. Telemedicine, for instance, connects clinicians and patients, proving valuable in diagnosis and decision-making. Technology also plays a vital role in enabling robotic surgery, facilitating extensive data analysis for modeling diagnosis, treatment, and prevention approaches, and utilizing AI to identify patients at risk and improve their diagnosis and management.19 However, a pressing need exists to integrate engineering and technology knowledge with healthcare expertise. This integration brings new challenges for delivering quality healthcare safely and effectively. Given the constant innovation in this area, there is an urgent need for innovative QI processes that balance technology and human intervention. Therefore, QI processes that integrate both are essential, giving QIS a pivotal role in the evolving telemedicine and technology-driven healthcare sector.
Framework for Tools and Indicators
Once a QI model is selected, specific tools are deployed for its implementation. These tools are required as healthcare professionals, who are often tasked with implementation, may not have adequate specialized training and expertise. Thus, these tools serve to train professionals in various QIS aspects.9 Table 2 summarizes essential QI tools, their categories, descriptions, and uses. The selection prioritizes tools that are well documented in the QI literature, applicable in healthcare delivery, and span all QI phases and data modalities.
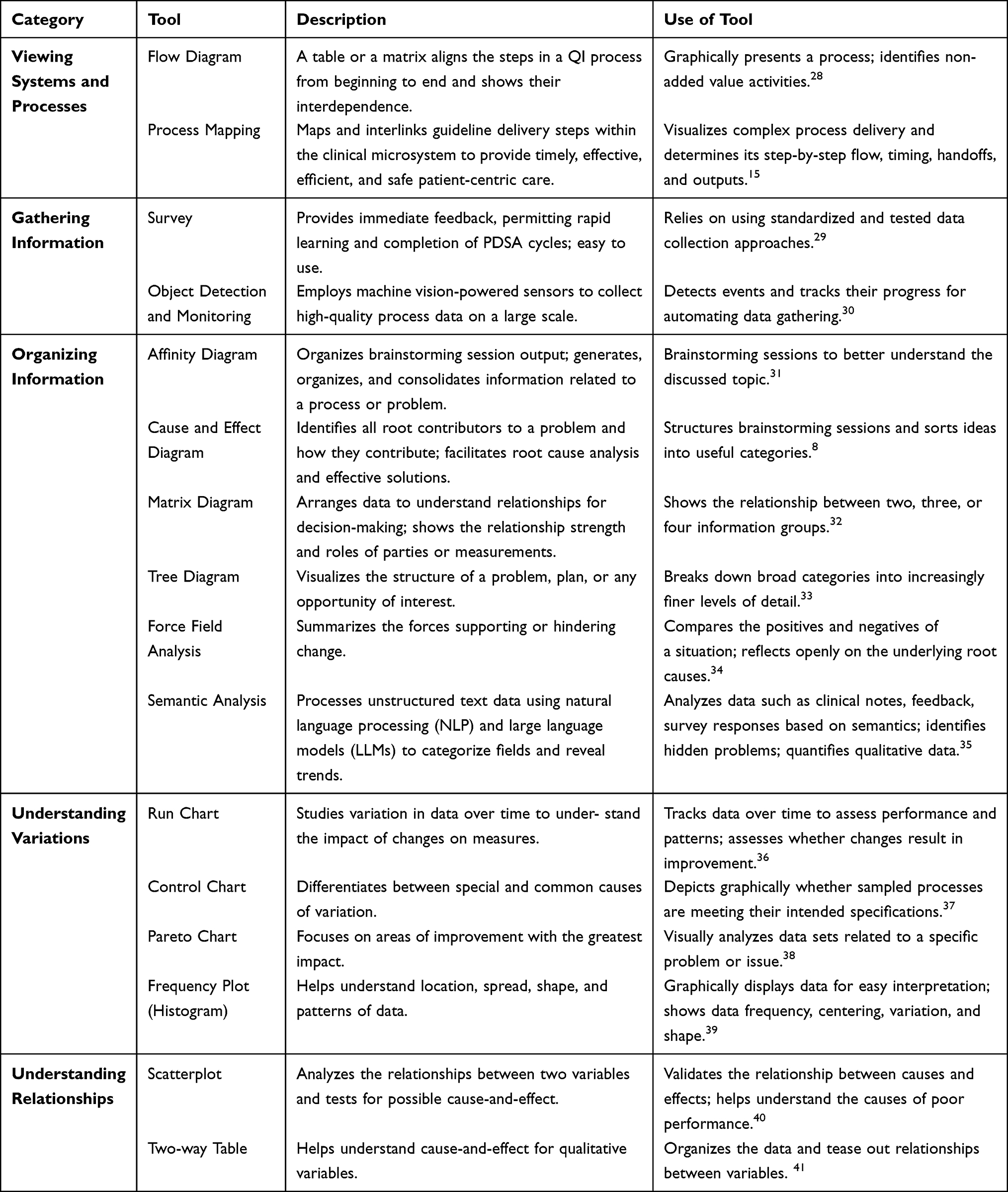 |
Table 2 Summary of Some QI Tools, Their Category, Description and Uses |
Given that the QI process is based on systems, processes, activities, and outcomes, quality improvement indicators are similarly categorized by structure, resources, processes, and outcomes.42 These indicators are summarized in Table 3, although more tools and methods may also be incorporated based on the needs and requirements of a specific healthcare setting.
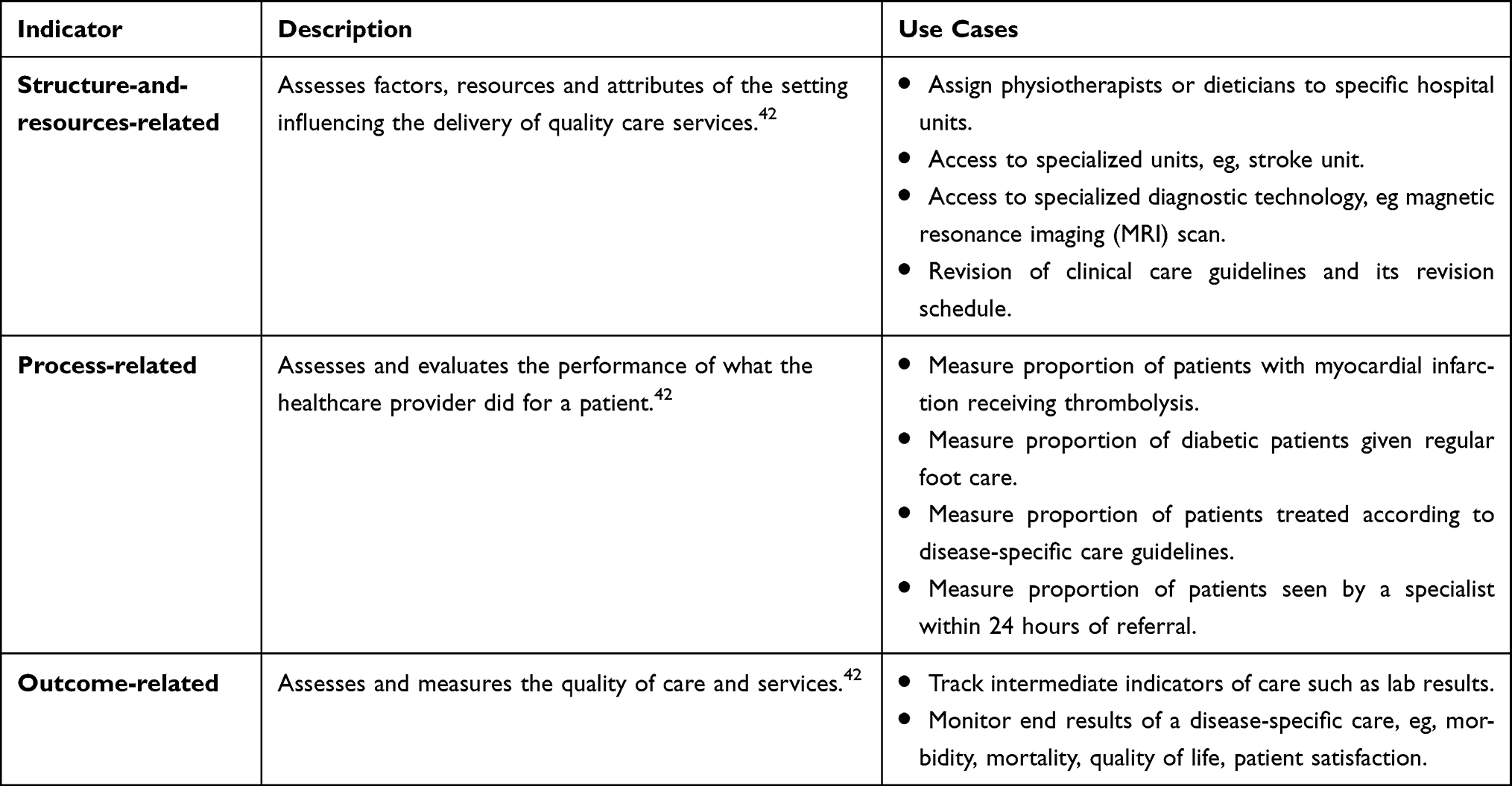 |
Table 3 Examples of Indicators Related to Structure, Process, and Outcome |
The proposed framework in Figure 3 employs a decision flow diagram that guides the selection of QI tools and indicators. It mirrors the typical stages of a QI cycle by separating problem understanding, data collection, and data analysis. The first phase emphasizes problem framing and process visualization. The second phase commits to what is measured and why, while remaining agnostic about specific analytic methods. The third phase aligns analytic choices with data character and monitoring intent, and it differentiates trend tracking from stability assessment and diagnosis from prioritization.
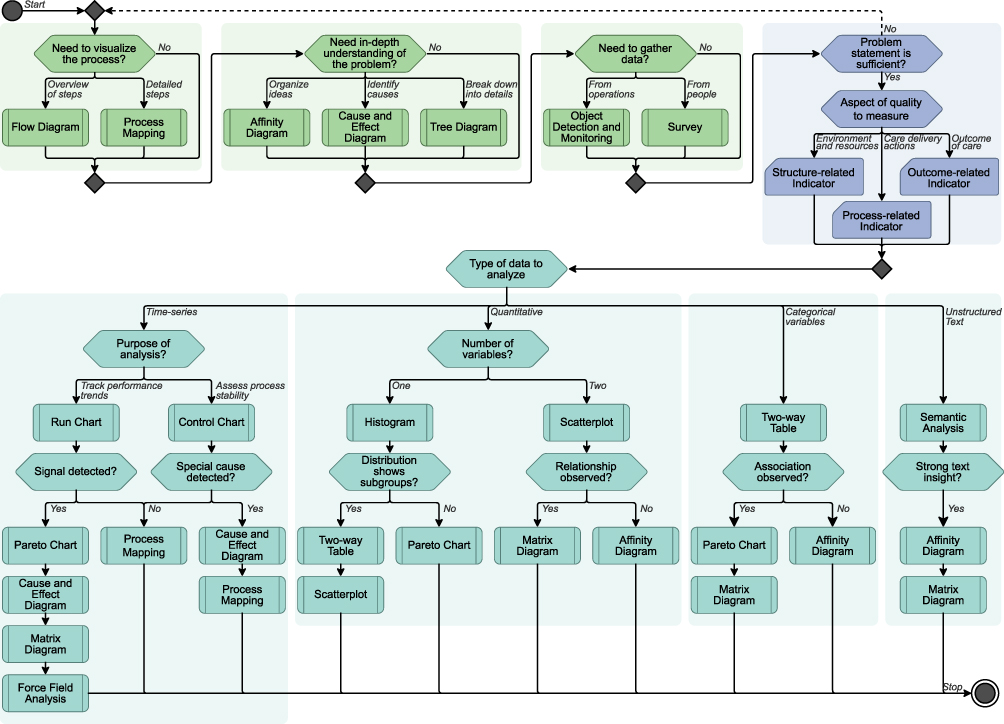 |
Figure 3 Decision flow diagram for selecting quality improvement tools and indicators. The flow comprises green, blue, turquoise stages for problem understanding, data collection, and data analysis, respectively. |
The structure of the decision flows in forward and return paths that protect against uninformed decisions. For example, the flow ensures that the understanding of the problem is sufficient before moving to the data collection stage. Additionally, depending on the type and shape of the collected measurements, the flow suggests utilizing a sequence of specific analysis tools for time-series, quantitative, categorical, and text-based data. Individuals such as nurses and service leads apply scoping tools and structuring diagrams to converge on a problem statement. At later stages, a multidisciplinary team performs data collection by selecting the indicators, sensing plan, and assigning a measure lead who ensures data collection feasibility and screening. The teams also perform data analysis using prioritization tools to rank contributors, in addition to small-scale PDSA cycles that let the team leader ensure decisions advance only when the problem is understood and measurements are trustworthy. Throughout the stages, practice facilitators and QI coaches assist individuals and teams toward successful execution of the QI process.
Implementation Challenges and Enablers
Despite the tremendous potential of various QI tools to improve healthcare, their implementation faces numerous challenges. Key challenges include:
- Limited staff knowledge and skills. A study43 found that QI implementation assistants reported limited educational backgrounds among some healthcare staff, which impeded skill and knowledge acquisition. They also noted that increased workload and implementation difficulties stemmed from challenges with staff receptiveness and skill development.
- Resistance to change. Resistance to change can significantly hinder effective QI tool implementation, particularly during preliminary stages.43 The staff in the study were unenthusiastic about attending professional training, citing a lack of interest and rigid thinking patterns. Furthermore, several nurses perceived no practical difference between current practices and QI offerings, which limited their interest to follow new instructions.
- Lack of job motivation. Some of the study participants43 viewed their roles merely as jobs, thus placing little importance on learning new QI tools. They also reported that a lack of team cohesion diminished their motivation to excel in new quality methods.
- Organizational constraints. Participants in the study consistently identified constraints such as resource scarcity, limited funding, poor team management, inadequate facilities, and time scarcity as major organizational barriers.43 Some reported that limited time made it difficult to perform duties and adhere to care protocols. Additionally, a lack of human resources, or staff shortages, was cited as another significant barrier to supporting QI tool implementation.
In contrast to these challenges, several enablers support the successful implementation of QI tools in healthcare settings:
- Self-efficacy. Clinical nurses in the study43 stated that when a challenge or doubt was encountered, they sought out evidence-based methods, such as consulting literature or online resources. This greatly stimulated their motivation to overcome difficulties and improved their capabilities and confidence.
- Supervision and feedback. Many participants highlighted the importance of administrative supervision and feedback. Some nurses proposed assigning experienced and skilled staff as site champions within each care unit to mentor and provide encouraging feedback to other staff, often referred to as mentees.43
- Organizational support. Organizational support is an additional enabler for QI tool implementation, especially for achieving sustainable development. Most study participants believed that a supportive learning environment and adequate resources were essential for successful implementation. Online training was also considered an effective and flexible method to alleviate barriers to specialized training, such as cost, scheduling, and training site availability.43
- Proactivity. Several studies confirm the importance of proactivity and motivation for behavior change, highlighting proactivity as fundamental for establishing a positive QI implementation process.44 Healthcare organizations can further enhance participant proactivity by establishing incentive mechanisms.43
Discussion
Although organizational QI processes are integral to improving quality, they vary significantly across departments and between organizations with similar objectives. Moreover, there is often no clarity within organizations regarding which processes to prioritize. The involvement of different stakeholders at various stages of a QI process results in differing opinions, conflicting needs, and inconsistent evaluation expertise. For instance, PFs are not always available to coach healthcare professionals, while doctors and nurses are often too busy and lack incentives to learn QIS principles. Additionally, resource availability influences implementation for QI enablers, low-resource healthcare systems often rely on affordable training and site champions, whereas high-resource systems draw on formal programs and dedicated funding for staff training. Consequently, QI applicability also varies by national context, as differences in governance, regulation, and accreditation influence healthcare delivery priorities, tool adoption, indicator selection, and the pace and sustainability of implementation across countries.
QIS is experiencing rapid technological and functional growth to meet the ever-increasing demand for high-quality and safe healthcare. There is an urgent need to educate and train organizations and healthcare providers about the various aspects of QIS. QI must be a continuous and sustained process, requiring constant monitoring and adaptation to achieve optimal outcomes. Integrating various healthcare stakeholders under a single QI platform is essential to facilitate the exchange of expertise, ideas, and technology. QI facilitators represent an upcoming field that needs to be integrated into organizational structures to provide QI training and oversee the identification and implementation of QI processes. QIS is positioned to play a pivotal role in improving healthcare delivery and patient safety in the future.
AI can strengthen these efforts by expanding the applicability of data collection and analysis. To ensure trustworthy adoption, technologies must be introduced through small PDSA cycles to continuously assess its impact and the stability of processes. While integrating evolving technologies into traditional processes can enable patient-centered improvements, they require active attention to preserve measurement validity and process continuity. AI in particular has inherent drawbacks such as bias in unscreened data, nondeterministic performance, and limited explainability.
Conclusion
This paper addressed the crucial need for effective application of QIS in enhancing patient safety within the healthcare landscape. The study proposed a comprehensive framework designed to guide healthcare professionals through the systematic implementation of QIS. Beyond developing the framework, the study thoroughly investigated the established concepts, processes, and models in QI. Furthermore, it explored the critical roles of various stakeholders and the significant influence of technology, particularly AI, in driving quality initiatives. The paper also detailed a practical guide for effectively selecting tools and indicators throughout the QI cycle, in addition to identifying key challenges and enablers impacting the successful QI implementation efforts. The structured analysis demonstrates that the systematic application of QIS can empower healthcare professionals in improving patient safety, especially when it is integrated into the stakeholder QI platforms and adopted by dedicated QI facilitators. Such successful application enables sustainable identification, analysis, and resolution of quality issues, leading to a culture of continuous improvement in healthcare quality. Future research may extend the framework with pilot implementations that evaluate the effectiveness of the decision-flow paths and develop practical toolkits and role-specific training curricula.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Berry LL. Service innovation is urgent in healthcare. AMS Rev. 2019;9(1–2):78–92. doi:10.1007/s13162-019-00135-x
2. World Health Organization. Quality of care: a process for making strategic choices in health systems. 2006. Available from: https://iris.who.int/bitstream/handle/10665/43470/9241563249_eng.pdf.
3. Institute of Medicine, Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press; 2001.
4. Sheikh A, Rudan I, Cresswell K, et al. Agreeing on global research priorities for medication safety: an international prioritisation exercise. J Global Health. 2019;9(1). doi:10.7189/jogh.09.010422
5. Powell BJ, Fernandez ME, Williams NJ, et al. Enhancing the impact of implementation strategies in healthcare: a research agenda. Front Public Health. 2019;7:7. doi:10.3389/fpubh.2019.00003
6. The Deming Institute. The W. Edwards deming institute. 2019. Available from: https://web.archive.org/web/20250308091652/https://deming.org/the-deming-philosophy.
7. Bresnick J. Cutting variation in hospital care brings high quality, lower costs. 2018. Available from: https://web.archive.org/web/20190902202553/https://healthitanalytics.com/news/cutting-variation-in-hospital-care-brings-high-quality-lower-costs.
8. Varkey P, ed.. Medical Quality Management: Theory and Practice.
9. Institute for Healthcare Improvement. Institute for healthcare improvement: science of improvement. 2019. Available from: https://web.archive.org/web/20231101235450/https://www.ihi.org/about/Pages/ScienceofImprovement.aspx.
10. Coughlin K, Posencheg MA. Common quality improvement methodologies including the model for improvement, lean, and six sigma. Clin Perinatol. 2023;50(2):285–306. doi:10.1016/j.clp.2023.02.002
11. Fulop NJ, Ramsay AIG. How organisations contribute to improving the quality of healthcare. Group BMJP, ed. BMJ. 2019;366. doi:10.1136/bmj.l4496
12. Agency for Healthcare Research and Quality. Section 4: ways to approach the quality improvement process. 2019. Available from: https://web.archive.org/web/20250309082304/https://www.ahrq.gov/cahps/quality-improvement/improvement-guide/4-approach-qi-process/index.html.
13. Allen-Duck A, Robinson JC, Stewart MW. Healthcare quality: a concept analysis. Nurs Forum. 2017;52(4):377–386. doi:10.1111/nuf.12207
14. D’Eramo AL. Quality improvement tools. Quality and safety education for nurses: core competencies for nursing leadership and care management. Springer Publishing Company; 2022;403–406.
15. Wasson JH, Godfrey MM, Nelson EC, Mohr JJ, Batalden PB. Microsystems in health care: part 4. planning patient-centered care. Joint Commission J Quality Safety. 2003;29(5):227–237. doi:10.1016/s1549-3741(03)29027-4
16. Walker LO, Avant KC. Strategies for Theory Construction in Nursing.
17. American Society for Quality. DMAIC process: define, measure, analyze, improve, control. 2019. Available from: https://web.archive.org/web/20250317204532/https://asq.org/quality-resources/dmaic.
18. Thakur V, Anthony Akerele O, Brake N, et al. Use of a lean six sigma approach to investigate excessive quality control (QC) material use and resulting costs. Clin Biochem. 2023;112:53–60. doi:10.1016/j.clinbiochem.2022.12.001
19. Habran E, Saulpic O, Zarlowski P. Digitalisation in healthcare: an analysis of projects proposed by practitioners. British J Healthcare Manage. 2018;24(3):150–155. doi:10.12968/bjhc.2018.24.3.150
20. Reed JE, Antonacci G, Armstrong N, et al. What is improvement science, and what makes it different? An outline of the field and its frontiers. Front Health Serv. 2025:4. doi:10.3389/frhs.2024.1454658
21. Underhill H, LeBlanc M, Macfarlane R, Hutton L. Using quality improvement frameworks to develop, implement, and evaluate a novel ambulatory oncology pharmacy practice model: a descriptive example. Am J Health Syst Pharm. 2024;81(24):1297–1304. doi:10.1093/ajhp/zxae184
22. Tsung F, Wang K. Six Sigma. In: Pham H., editor. Springer Handbook of Engineering Statistics. London: Springer;2023:239–259. doi:10.1007/978-1-4471-7503-2_13
23. U.S. Department of Health and Human Services. Health resources and services administration. Quality Improvement. 2011. Available from: https://web.archive.org/web/20220808145121/https://www.hrsa.gov/sites/default/files/quality/toolbox/508pdfs/qualityimprovement.pdf.
24. Bethune RM, Ball S, Doran N, et al. How safety culture surveys influence the quality and safety of healthcare organisations. Cureus. 2023. doi:10.7759/cureus.44603
25. Huotari P, Havrdová Z. Stakeholders’ roles and responsibilities regarding quality of care. Int J Health Care Qual Assur. 2016;29(8):864–876. doi:10.1108/ijhcqa-06-2015-0070
26. Silver SA, Harel Z, McQuillan R, et al. How to begin a quality improvement project. Clin J Am Soc Nephrol. 2016;11(5):893–900. doi:10.2215/cjn.11491015
27. Sull D, Sull C. With goals, fast beats smart. MIT Sloan Manage Rev. 2018;59(4):1–11.
28. Prasad B, Strand N. A flow-chart-based methodology for process improvement. In: Quality Concepts ‘93 World Class Manufacturing. Engineering Society of Detroit (ESD) and American Society for Quality Control (ASQC); 1993:53–74. doi:10.13140/rg.2.1.2559.4327
29. Ponto J. Understanding and evaluating survey research. J Adv Practit Oncol. 2015;6(2):168–171.
30. Sritart H, Tosranon P, Taertulakarn S. An artificial intelligence-enabled consumables tracking system for medical laboratories. J Intell Syst. 2024;33(1):20230208. doi:10.1515/jisys-2023-0208
31. Lucero A. Using affinity diagrams to evaluate interactive prototypes. In: Abascal J, Barbosa S, Fetter M, Gross T, Palanque P, Winckler M, editors. Human-Computer Interaction – INTERACT 2015. Springer International Publishing; 2015:231–248. doi:10.1007/978-3-319-22668-2_19
32. van der Meij J, van Amelsvoort M, Anjewierden A. How design guides learning from matrix diagrams. Instructional Sci. 2017;45(6):751–767. doi:10.1007/s11251-017-9425-1
33. Yin Y. Using tree diagrams as an assessment tool in statistics education. Educ Assess. 2012;17(1):22–49. doi:10.1080/10627197.2012.697850
34. Shrivastava S, Shrivastava P, Ramasamy J. Force field analysis: an effective tool in qualitative research. J Curr Res Sci Med. 2017;3(2):139. doi:10.4103/jcrsm.jcrsm_55_17
35. Zheng NS, Keloth VK, You K, et al. Detection of gastrointestinal bleeding with large language models to aid quality improvement and appropriate reimbursement. Gastroenterology. 2025;168(1):111–120.e4. doi:10.1053/j.gastro.2024.09.014
36. Anhøj J, Olesen AV. Run charts revisited: a simulation study of run chart rules for detection of non-random variation in health care processes. Hills RK, ed. PLoS One. 2014;9(11):e113825. doi:10.1371/journal.pone.0113825
37. Colosimo BM, Pacella M. A comparison study of control charts for statistical monitoring of functional data. Int J P Res. 2009;48(6):1575–1601. doi:10.1080/00207540802662888
38. Hossen J, Ahmad N, Ali SM. An application of Pareto analysis and cause-and-effect diagram (CED) to examine stoppage losses: a textile case from Bangladesh. J Textile Instit. 2017;108(11):2013–2020. doi:10.1080/00405000.2017.1308786
39. M S. Frequency distribution. J pharmacol Pharmacotherap. 2011;2(1):54–56. doi:10.4103/0976-500x.77120
40. Rensink RA. The nature of correlation perception in scatterplots. Psychonomic Bull Rev. 2016;24(3):776–797. doi:10.3758/s13423-016-1174-7
41. Vives-Mestres M, Casanova A. Modeling and visualizing two-way contingency tables using compositional data analysis: a case-study on individual self-prediction of migraine days. Stat Med. 2021;40(2):213–225. doi:10.1002/sim.8769
42. Mainz J. Defining and classifying clinical indicators for quality improvement. Int J Qual Health Care. 2003;15(6):523–530. doi:10.1093/intqhc/mzg081
43. Zhao Y, Liao L, Feng H, Chen H, Ning H. Enablers and barriers to implementing care quality improvement program in nursing homes in China. BMC Geriatr. 2021;21(1). doi:10.1186/s12877-021-02488-0
44. Leary JC, Schainker EG, Leyenaar JK. The unwritten rules of mentorship: facilitators of and barriers to effective mentorship in pediatric hospital medicine. Hospital Pediatrics. 2016;6(4):219–225. doi:10.1542/hpeds.2015-0108
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.