Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Application Value of STOP-Bang Questionnaire in Predicting Abnormal Metabolites
Authors Pang Q, Han L, Li J, Xu L, Wang Y
Received 23 October 2024
Accepted for publication 28 December 2024
Published 9 January 2025 Volume 2025:18 Pages 93—99
DOI https://doi.org/10.2147/DMSO.S499871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Qingyi Pang,1 Li Han,1 Jun Li,2 Lingling Xu,1 Yueheng Wang3
1Department of Endocrinology, Peking Union Medical College Hospital, Beijing, People’s Republic of China; 2Department of Endocrinology, Beijing Hepingli Hospital, Beijing, People’s Republic of China; 3Department of Ear, Nose and Throat, Beijing Hepingli Hospital, Beijing, People’s Republic of China
Correspondence: Lingling Xu; Yueheng Wang, Email [email protected]; [email protected]
Objective: To evaluate the application value of STOP-Bang questionnaire (SBQ) in predicting abnormal metabolites.
Methods: Totally 121 patients were included into the study and filled the questionnaires, and their clinical data were collected at the same time. These patients were grouped according to the questionnaire scores. The clinical data of patients in various groups were compared using R4.3.1 statistical software.
Results: Based on the SBQ score, the patients were divided into the following groups: low-risk group (0– 2 scores), mid-risk group (3– 4 scores), and high-risk group (5– 8 scores). SBQ score was related to several abnormal metabolites. A higher SBQ score indicated elevated uric acid (UA), waist circumference (WC), fasting blood glucose (FBG), hemoglobin A1c (HbA1c) and triacylglycerol (TG), but notably lower high density lipoprotein-cholesterol (HDL-C). In respect of liver function, alanine aminotransferase (ALT) and aspartate transaminase (AST) were both in low/mid-risk group than in high-risk group. With respect to renal function, there was a statistically significant difference in serum creatinine (SCr) (lowest in the low-risk group and highest in the high-risk group) but no such difference in estimated glomerular filtration rate (eGFR) among the three groups. The diagnosability analysis showed that the AUROC proved the good performance of SBQ in predicting metabolic syndrome (MetS) and hyperuricemia (HUA).
Conclusion: OSA frequently co-occurs with various metabolic disorders. SBQ, a widely used tool for assessing the risk of OSA, may also be a potential tool for predicting the presence of metabolic diseases. A higher SBQ score indicates a heightened susceptibility to more abnormal metabolites, but SBQ is poor in predicting liver and renal functions. The patients with SBQ score ≥ 3 are suggested to pay a visit to the Endocrine Department and Sleep Disorders Center for a comprehensive evaluation of comorbid Obstructive sleep apnea (OSA) and the management of systematic metabolism.
Keywords: STOP-Bang questionnaire, metabolic syndrome, hyperuricemia, obstructive sleep apnea, OSA, health management
Introduction
Obstructive sleep apnea (OSA) is a common systematic disease. Its most important characteristic is partial or complete recurrent upper airway obstruction during sleep, accompanied with or without snoring, inducing intermittent hypoxemia, hypercapnia and segmented sleep, as well as systemic oxidative stress, inflammatory reaction and sympathetic hyperactivity in a long time, which further aggravates hypertension, diabetes and dyslipidemia.1 OSA is closely associated with several metabolic disorders, such as obesity, glycolipid metabolism, purine metabolism, liver and renal metabolism, and a pathological state of such complex metabolic disorders is called metabolic syndrome (MetS).2 Compared with the ordinary population, OSA patients have a remarkably increased risk of MetS. A Chinese cross-sectional study showed that the morbidity rate of MetS was 18.6%, 30.4%, 43.8% and 57.1% in the patients with no, mild, moderate and severe OSA, respectively.3 Another prospective cohort study demonstrated that 17.2% of OSA patients developed MetS within 6 years.4 OSA is prone to aggregate with MetS components, and the latter are known risk factors for cardiovascular diseases (CVD), thus increasing the risk of cardiovascular events. Therefore, in clinical practice, an evaluation of abnormal metabolites shall be done in a timely manner for patients highly suspected of having OSA.
At present, the recognized diagnostic gold standard for OSA is polysomnography (PSG);5 as PSG is time-consuming, laborious and expensive, and has high requirements for professional technologies and a long examination-waiting time, it is frequently used in the diagnostic examination of high-risk patients after OSA screening. STOP-Bang questionnaire (SBQ) is a simple, effective, and highly operable tool for OSA screening and has good sensitivity, thus it is currently recommended to screen high-risk OSA patients in the health check institutions, gross-root medical institutions and communities.6
According to the current literature search results, no studies have been found that involve the application of SBQ in evaluating the body’s risk of metabolic diseases. Based on the high correlation of OSA with several metabolic diseases, this study aimed to analyze the relationship between SBQ score and several metabolic disorders, which is expected to facilitate early consultation and early screening of patients with higher SBQ scores.
Materials and Methods
1. Study subjects: A total of 121 patients (71 males and 50 females, age: 21–79 (median: 59) years) signed written informed consent voluntarily and were selected who were admitted to Peking Union Medical College Hospital from July 2022 to January 2024. The exclusion criteria were below: patients diagnosed with OSA and who had received the relevant treatment; patients with severe heart, lung, liver and kidney diseases; patients with malignant tumors or a recent history of major physical or psychological trauma; patients with sleep-disordered breathing diseases except OSA; and patients with an age of <18 or >80 years. The clinical trial was approved by the ethics committee of Peking Union Medical College Hospital (I-22PJ477). The study complies with the Declaration of Helsinki. All subjects signed informed consent forms.
2. Methods: The uniformly trained doctors and nurses completed the questionnaire survey, physical examination, and blood sample collection. The general data of patients were collected by face-to-face SBQ survey. The questionnaire contained 8 binary items related to the clinical characteristics of sleep apnea (yes/no): snoring, fatigue, observable apnea, hypertension, body mass index (BMI) > 35kg/m2, age > 50 years, neck circumference (NC) > 40cm, and male. The answers to the above 8 questions were “yes” or “no”, “yes” was recorded as 1 score and “no” as 0 score; Items 1–4 and Items 5–8 in the questionnaire are filled by subjects and clinicians, respectively. The subjects were divided into 3 groups according to SBQ score: OSA low-risk group (0–2 scores), OSA mid-risk group (3–4 scores), and OSA high-risk group (5–8 scores).7 The physical examination included the measurement of subjects’ height, weight, NC and waist circumference (WC) as well as the calculation of BMI [BMI=weight(kg)/height2 (m2)]. The blood sample was collected via antecubital vein after overnight fasting by an experienced nurse. Hemoglobin A1c (HbA1c) level (intra-batch coefficient of variance (CV) < 3%, and inter-batch CV < 10%) was evaluated by high-performance liquid chromatography (HPLC). The following indicators were evaluated with an auto-analyzer: fasting blood-glucose (FBG), hemoglobin A1c (HbA1c), triacylglycerol (TG), high density lipoprotein-cholesterol (HDL-C), total cholesterol (TC), low density lipoprotein-cholesterol (LDL-C), uric acid (UA), alanine aminotransferase (ALT), aspartate transaminase (AST), direct bilirubin (DBil), total bilirubin (TBil), alkaline phosphatase (ALP), and serum creatinine (SCr). Estimated glomerular filtration rate (eGFR) was calculated using age, weight and SCr. [Male: eGFR=(140-age)*weight/(0.818*SCr); female: eGFR=(140-age)*weight/(0.818*SCr)*0.85].
3. Definition of metabolic syndrome: In the following 5 criteria, ≥3 were met: ① Abdominal obesity (ie, central obesity): WC ≥ 90cm for males and WC ≥ 85cm for females; ② FPG ≥ 6.1mmol/L and (or) 2hPG ≥ 7.8mmol/L, and (or) diagnosed diabetes under treatment; ③ blood pressure (BP) ≥130/85 mmHg, and (or) diagnosed hypertension under treatment; ④ fasting TG ≥ 1.7 mmol/L; and ⑤ fasting HDL-C < 1.04 mmol/L.8
4. Definition of hyperuricemia (HUA): It was defined as UA > 420umol/L twice in the non-same day for either men or women.9
5. Definition of liver injury: Liver injury was defined as ALT elevation or AST elevation. Furthermore, ALT elevation was defined as ALT > 40U/L for males and >31U/L for females, and AST elevation as AST > 37U/L for males and >31U/L for females.10
6. Statistical analysis: R4.6.1 software was used for statistical description and analysis. The quantitative data of normal distribution were presented as x ± s, and those with homogeneity of variance was tested by one-way analysis of variance (ANOVA); the quantitative data of skewed distribution were expressed as M(P25, P75), the categorical variables were presented as %, and in respect of inter-group comparison, the variables of skewed distribution were subjected to the non-parametric comparison by Kruskal–Wallis rank sum test. The qualitative data were expressed as n (%), and their inter-group comparison was performed with χ²-test. The significance level for two-sided test was α=0.05. Area under the receiver operating characteristic curve (AUROC) was used to make a cross-sectional evaluation on the value of SBQ score in predicting HUA and MetS. AUROC was plotted with sensitivity as y axis and false positive rate (1-specificity) as x axis. The optimal cut-off was used as the curve peak, with the biggest sum of sensitivity and specificity.
Results
1. General data: The subjects were aged 55 years on average, including 71 (58.7%) males. The differences in male percentage, NC, BMI, and hypertension rates among all three groups increase with the elevation of the SBQ scores, with the highest values observed in the high-risk group and the lowest in the low-risk group. (all P < 0.001); there were no statistically significant differences in age, hyperlipidemia, hypoglycemic drug treatment rate and urate-lowering drug treatment rate among three groups (P > 0.05) (see Table 1).
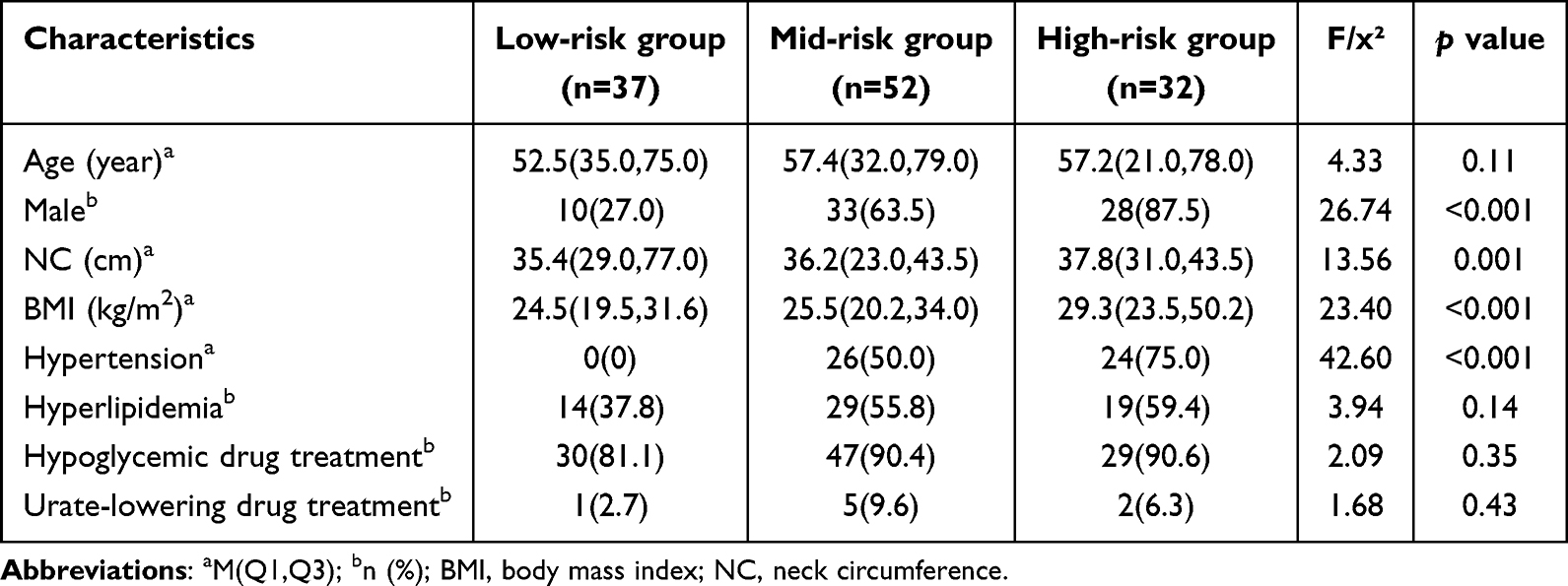 |
Table 1 General Data of Patients in 3 SBQ Groups |
2. Metabolic indicators: The incidence rate of metabolic syndrome in low-risk, mid-risk and high-risk groups was 18.9%, 44.2% and 75% (P < 0.001), respectively. The inter-group differences of WC, HbA1c, FBG, TG, HDL-C and UA were all statistically significant (P < 0.05) (see Table 2); as SBQ score increased, WC (87.6 vs 90.1 vs 97.9 cm), HbA1c (6.3% vs 6.73% vs 8.0%), FBG (6.2 vs 7.4 vs 9.1 mmol/L), TG (1.1 vs 1.6 vs 2.6 mmol/L) and UA (272.0 vs 335.6 vs 385.3 mmol/L) were elevated accordingly (all P < 0.001), but HDL-C (1.3 vs 1.2 vs 1.0 mmol/L, P = 0.001) was declined, ie, a higher SBQ score indicated more abnormal metabolic indicators (see Figure 1). The comparison of TC and LDL-C showed no statistically significant difference (P > 0.05) (see Table 2).
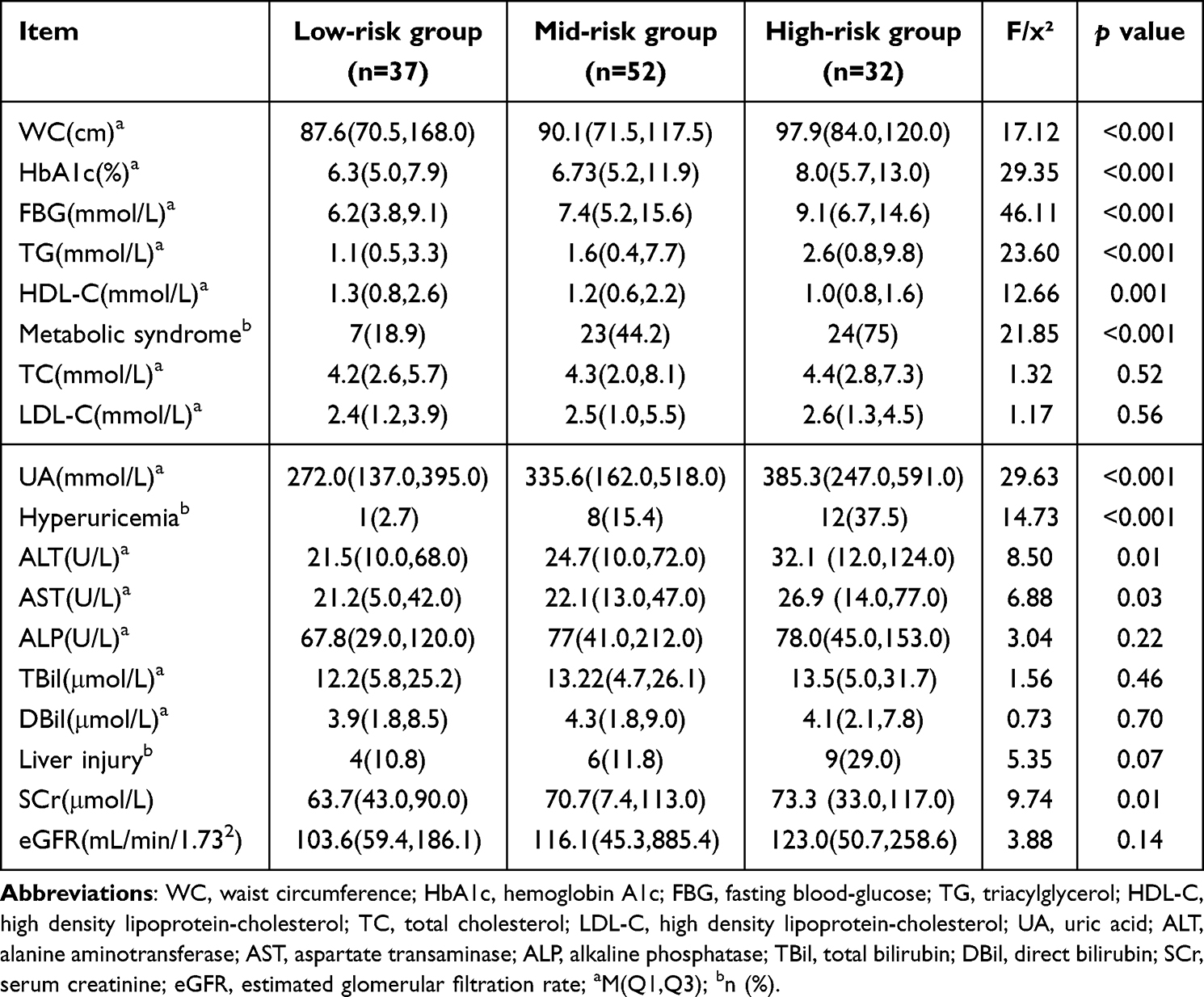 |
Table 2 Comparison of Metabolic Indicators and Liver & Renal Function Indicators Among 3 SBQ Groups |
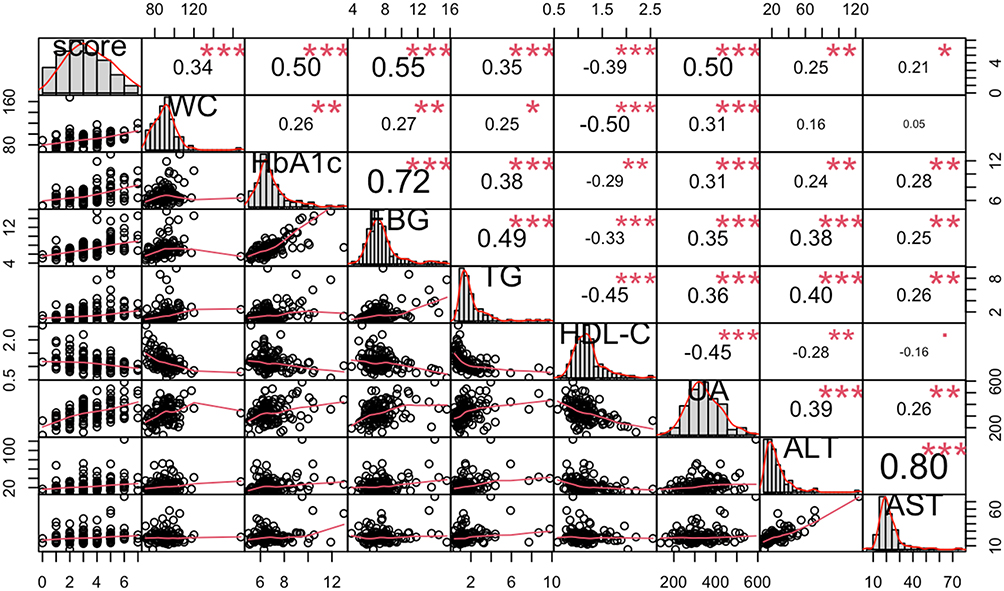 |
Figure 1 Correlations of SBQ score with metabolic indicators and liver function indicators. :0.1<P<0.05, P*: P<0.05; **: P<0.01; ***: P<0.001. Abbreviations: score, STOP-Bang questionnaire score; WC, waist circumference (cm); HbA1c, hemoglobin A1c (%); FBG, fasting blood-glucose (mmol/L); TG, triacylglycerol (mmol/L); HDL-C, high density lipoprotein-cholesterol (mmol/L); UA, uric acid (mmol/L); ALT, alanine aminotransferase (U/L); AST, aspartate transaminase (U/L). |
3. Liver & renal function indicators: The inter-group differences of ALT, AST and SCr were statistically significant (all P < 0.05), but no statistically significant difference was observed in ALP, TBil, DBil, liver injury percentage and eGFR (P > 0.05) (see Table 2 and Figure 2). ALT and AST in the high-risk group were higher than those in the low-risk and mid-risk groups (P < 0.01) (see Figure 2). ALT (21.5 vs 24.7 vs 32.1 U/L, P = 0.01) and AST (21.2 vs 22.1 vs 26.9 U/L, P = 0.03) were elevated with the increase of SBQ score (see Table 2 and Figure 1).
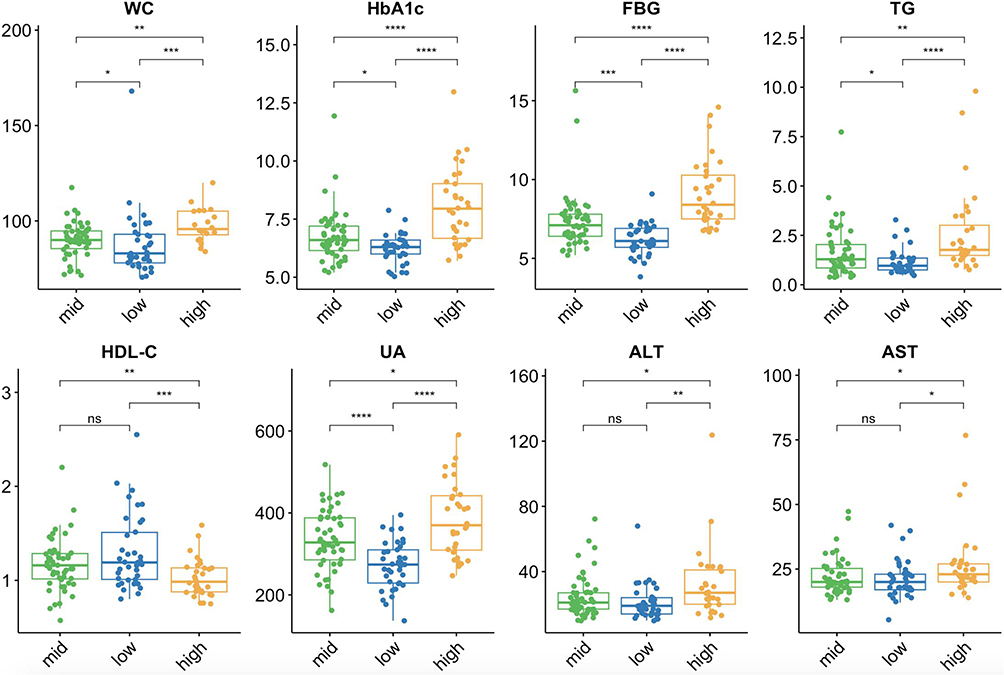 |
Figure 2 Comparison of metabolic indicators and liver and renal function indicators among 3 SBQ groups. Abbreviations: WC, waist circumference (cm); HbA1c, hemoglobin A1c (%); FBG, fasting blood-glucose (mmol/L); TG, triacylglycerol (mmol/L); HDL-C, high density lipoprotein-cholesterol (mmol/L); UA, uric acid (mmol/L); ALT, alanine aminotransferase (U/L); AST, aspartate transaminase (U/L). low: low-risk group (0–2 scores); mid: mid-risk group (3–4 scores); high: high-risk group (5–8 scores). ns: P > 0.05; *: P < 0.05;**: P < 0.01; ***: P < 0.001; ****: P < 0.0001. |
4. Diagnosability analysis: In predicting MetS, the AUROC, optimal cut-off, sensitivity and specificity of SBQ score were 0.743 (95% CI: 0.657–0.829), ≥ 3.5, 63.0% and 70.1%; in predicting HUA, they were 0.735 (95% CI: 0.626–0.843), ≥ 4.5, 57.1% and 80.6% (see Figure 3).
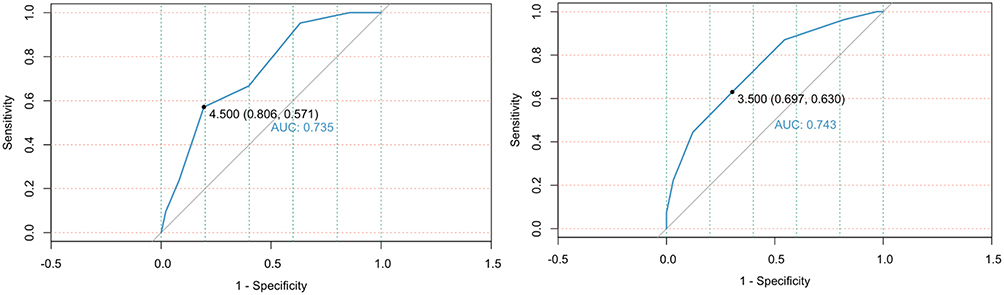 |
Figure 3 ROC curves of hyperuricemia (left) and metabolic syndrome (right). |
Discussion
OSA is closely related to MetS and its multi-disease component and is more correlated with obesity and lipid metabolism disorders.11 A meta-analysis showed that SBQ had a combined sensitivity of 85%, 88% and 90% for all OSAs, moderate to severe OSA, and severe OSA, with a combined specificity of 47%, 29% and 27%, respectively, and an AUROC of 0.84, 0.67, and 0.63, respectively.12 Currently, most screening questionnaires are designed for a specific population of OSA, MetS or HUA. In this study, we firstly analyzed the risk of several abnormal metabolic indicators (eg, MetS and HUA) by combining SBQ score. Our study demonstrated that compared with the low-risk group (SBQ score < 3), the mid/high-risk group (SBQ score ≥ 3) (ie, OSA high-risk population) suffered from a higher risk of several abnormal metabolic indicators and then an evidently increased risk of MetS and HUA. Further statistical analysis proved the good performance of SBQ in predicting MetS and HUA. This provides a new basis for the simultaneous prediction on the risks of OSA and several abnormal body metabolites in the clinical work by using SBQ, and expands the application value of SBQ in the evaluation of the risk of metabolic diseases.
In a cohort study of 1853 OSA patients without MetS, the 5.9-year follow-up showed that 17.2% OSA patients developed MetS, and further subgroup analysis revealed that moderate and severe OSA patients were closely associated with the occurrence of MetS (OR = 2.58 after correcting the confounding factors).1,2 As shown by the results of another meta-analysis of 18 studies involving 157,607 patients (including 32,395 patients with OSA), UA in OSA patients was higher than that in non-OSAS patients (WMD = 52.25, 95% CI: 36.16–64.33).13 Based on the results of a study to investigate the change of UA excretion via urine in OSA patients before and after continuous positive airway pressure (CPAP) treatment (20 OSA patients vs 10 healthy controls), the mean UA excretion was (0.55 ± 0.10) mg/dl before treatment, and remarkably decreased to (0.30 ± 0.01) mg/dl after treatment, similar to that in the control group ((0.32 ± 0.03) mg/dl).14 This may be related to the improvement of renal hemodynamics in OSA patients by CPAP.15 These findings are highly consistent with our study conclusion.
OSA and MetS both can damage the body’s multiple systems, of which the cardiovascular system is damaged most frequently and seriously. The morbidity rate of cardiovascular diseases (CVD) and the risk of CVD-related death are significantly higher in the populations of OSA and MetS than in the ordinary population, thus increasing the medical burden of individuals, families, and society.16,17 The studies have shown that the risk of CVD-related death in severe OSA patients is increased by 2.7 folds as compared with non-OSA patients.18,19 Similarly, the risk of CVD in MetS patients is increased by 2.35 folds, specifically, the risk of myocardial infarction is increased by 1.99 folds and that of stroke by 2.27 folds;20 MetS and relevant diseases bring an increase of 60% to the total healthcare costs.21 Therefore, in order to improve the prognosis and quality of life of patients and reduce the social and economic burdens, it is of great significance to early identify OSA and MetS high-risk populations, regularly monitor the relevant indicators of metabolic syndrome and actively take the proper clinical interventions. Our study has confirmed that SBQ can not only screen OSA high-risk patients but also help the early identification of individuals with possible abnormal metabolites. Meanwhile, considering good performance of SBQ in predicting MetS and (or) HUA, we advocate SBQ screening of OSA patients by professionally trained doctors or nurses in the grass-root hospitals and recommend transferring patients with SBQ score ≥3 to the Sleep Disorders Department and Endocrine Department for the comprehensive evaluation of OSA and systematic metabolism, respectively.
This study has the following limitations: (1) it is a cross-sectional study with a poor causality testing capability; (2) no further subgroup analysis was performed on the ethnicity, education, exercise and food habit of patients; (3) there was a small sample size, and more large-sample-size longitudinal studies and (or) interventional studies are needed to detect the improvement effects of various metabolic indicators before and after the standard treatment of OSA and thus validate our study conclusion.
Conclusion
This study has proven that SBQ, as a convenient and promising screening tool, can identify individuals possibly with several abnormal metabolites (especially MetS and HUA) in Chinese population from a cross-sectional view.
Funding
This study was funded by CAMS Innovation Fund for Medical Sciences (CIFMS, 2021-I2M-C&T-B-003), CAMS Innovation Fund for Medical Sciences (CIFMS, 2021-I2M-1-002) and National High Level Hospital Clinical Research Funding (2022-PUMCH-B-015).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Heffernan A, Duplancic D, Kumric M, et al. Metabolic Crossroads: unveiling the Complex Interactions between Obstructive Sleep Apnoea and Metabolic Syndrome[J/OL]. Int J Mol Sci. 2024;25(6):3243. doi:10.3390/ijms25063243
2. Patel SR. Obstructive Sleep Apnea[J/OL]. Ann Internal Med. 2019;171(11):ITC81–ITC96. doi:10.7326/AITC201912030
3. B GW, P LY, H XH, et al. Obstructive sleep apnea and metabolic syndrome: an association study based on a large sample clinical database][J/OL. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021;56(12):1263–1269. doi:10.3760/cma.j.cn115330-20210531-00314
4. Hirotsu C, Haba-Rubio J, M TS, et al. Obstructive sleep apnoea as a risk factor for incident metabolic syndrome: a joined Episono and HypnoLaus prospective cohorts study[J/OL]. Europ resp J. 2018;52(5):1801150. doi:10.1183/13993003.01150-2018
5. Jafari B, Mohsenin V. Polysomnography[J/OL]. Clinics Chest Med. 2010;31(2):287–297. doi:10.1016/j.ccm.2010.02.005
6. Sleep Disordered Breathing Group of Chinese Thoracic Society of CMA, Sleep-Disordered Breathing Equipment Group of Technical Committee for Breathing Equipment of CAME. Expert consensus on screening and management of high-risk population with obstructive sleep apnea in adults [J/OL]. Chinese J Health Manag. 2022;16(08):520–528. doi:10.3760/cma.j.cn115624-20220615-00460
7. Seguin L, Tamisier R, Deletombe B, et al. Preoperative Screening for Obstructive Sleep Apnea Using Alternative Scoring Models of the Sleep Tiredness Observed Pressure-Body Mass Index Age Neck Circumference Gender Questionnaire: an External Validation[J/OL]. Anesthesia Analg. 2020;131(4):1025–1031. doi:10.1213/ANE.0000000000004909
8. Chinese Society of Health Management of CMA, editorial board of Chinese Journal of Health Management, National Clinical Research Center for Geriatric Disorders (Xiangya Hospital). Expert consensus on prevention & control health education of metabolic syndrome in adults [J/OL]. Chinese J Health Manag. 2024;18(02):81–92. doi:10.3760/cma.j.cn115624-20231201-00314
9. Yefei H, Kehu Y, Shuhong C, et al. Practice guideline for patients with hyperuricemia and gout [J/OL]. Chinese J Int Med. 2020;59(07):519–527. doi:10.3760/cma.j.cn112138-20200505-00449
10. K CL, Liu LK, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia[J/OL]. J Am Med Directors Assoc. 2014;15(2):95–101. doi:10.1016/j.jamda.2013.11.025
11. Wang F, Xiong X, Xu H, et al. The association between obstructive sleep apnea syndrome and metabolic syndrome: a confirmatory factor analysis[J/OL]. Sleep Breath. 2019;23(3):1011–1019. doi:10.1007/s11325-019-01804-8
12. Hwang M, Nagappa M, Guluzade N, et al. Validation of the STOP-Bang questionnaire as a preoperative screening tool for obstructive sleep apnea: a systematic review and meta-analysis[J/OL]. BMC Anesthes. 2022;22(1):366. doi:10.1186/s12871-022-01912-1
13. Shi T, Min M, Sun C, et al. A meta-analysis of the association between gout, serum uric acid level, and obstructive sleep apnea[J/OL]. Sleep Breath. 2019;23(4):1047–1057. doi:10.1007/s11325-019-01827-1
14. Sahebjani H. Changes in urinary uric acid excretion in obstructive sleep apnea before and after therapy with nasal continuous positive airway pressure[J/OL]. Chest. 1998;113(6):1604–1608. doi:10.1378/chest.113.6.1604
15. Zamarrón E, Jaureguizar A, García-Sánchez A, et al. Continuous Positive Airway Pressure Effect on Albuminuria Progression in Patients with Obstructive Sleep Apnea and Diabetic Kidney Disease: a Randomized Clinical Trial[J/OL]. Am J Respir Crit Care Med. 2023;207(6):757–767. doi:10.1164/rccm.202206-1091OC
16. Polecka A, Olszewska N, Danielski Ł, et al. Association between Obstructive Sleep Apnea and Heart Failure in Adults-A Systematic Review[J/OL]. J Clin Med. 2023;12(19):6139. doi:10.3390/jcm12196139
17. Højager A, M SM, K TP, et al. Estimates of 10-year risk of cardiovascular death and adherence to cardiovascular risk factor management in Danish patients investigated for obstructive sleep apnea[J/OL]. Sleep Med. 2023;104:22–28. doi:10.1016/j.sleep.2023.02.009
18. Young T, Finn L, E PP, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort[J]. Sleep. 2008;31(8):1071–1078. doi:10.1002/14651858.CD001106.pub3
19. M PN, S CB, L GJ, et al. Sleep-disordered breathing and mortality: a prospective cohort study[J/OL]. PLoS Med. 2009;6(8):e1000132. doi:10.1371/journal.pmed.1000132
20. Mottillo S, B FK, Genest J, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis[J/OL]. J Amer Coll Card. 2010;56(14):1113–1132. doi:10.1016/j.jacc.2010.05.034
21. Álvarez-Bustos A, Rodríguez-Sánchez B, A C-CJ, et al. Healthcare cost expenditures associated to frailty and sarcopenia[J/OL]. BMC Geriatrics. 2022;22(1):747. doi:10.1186/s12877-022-03439-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.