Back to Journals » International Journal of General Medicine » Volume 19
Application Value of QRS Wave Potential in Predicting Left Ventricular Remodeling and Adverse Cardiovascular Events in Patients with Acute Myocardial Infarction After PCI
Authors Wu J, Lan H, Qian Y, Wang X
Received 29 August 2025
Accepted for publication 10 December 2025
Published 10 January 2026 Volume 2026:19 564055
DOI https://doi.org/10.2147/IJGM.S564055
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Jianmin Wu, Huaxian Lan, Yuanyuan Qian, Xiaoe Wang
Department of ECG, The Second Affiliated Hospital of Wenzhou Medical University, Wenzhou City, Zhejiang Province, 325000, People’s Republic of China
Correspondence: Xiaoe Wang, Department of ECG, The Second Affiliated Hospital of Wenzhou Medical University, No. 109, Academy West Road, Lucheng District, Wenzhou City, Zhejiang Province, 325000, People’s Republic of China, Email [email protected]
Objective: To investigate whether fragmented QRS (fQRS) on electrocardiogram (ECG) obtained 24– 48 hours after percutaneous coronary intervention (PCI) predicts left ventricular remodeling (LVRM) and major adverse cardiovascular events (MACE) in patients with acute myocardial infarction (AMI).
Methods: A total of 122 AMI patients who underwent PCI were prospectively enrolled and categorized into fQRS (n=48) and non-fQRS (n=74) groups based on post-PCI ECG findings. Clinical data, serum biomarkers, left ventricular function, and the incidence of MACE were compared between groups. Cox proportional hazards regression and logistic regression analyses were used to identify independent predictors of MACE and LVRM, respectively.
Results: Patients in the fQRS group exhibited significantly higher levels of cardiac biomarkers (cTnI, CPK, CK-MB), more adverse lipid profiles, and impaired renal function parameters (all P < 0.05). Echocardiographic assessment revealed significantly reduced left ventricular ejection fraction (51.5% vs 57.2%, P < 0.001) and increased wall thickness in the fQRS group. During one-year follow-up, the fQRS group had a substantially higher incidence of MACE (35.4% vs 10.8%, P < 0.001). Multivariate analysis confirmed post-PCI fQRS as an independent predictor for both LVRM (OR: 3.12, 95% CI: 1.48– 6.55, P = 0.003) and MACE (HR: 2.65, 95% CI: 1.52– 4.63, P = 0.001).
Conclusion: fQRS identified on ECG after PCI is a significant independent predictor of LVRM and MACE in AMI patients, providing valuable prognostic information for risk stratification.
Keywords: QRS fragmentation, myocardial infarction, percutaneous coronary intervention, left ventricular remodeling, adverse cardiovascular events
Introduction
Acute myocardial infarction (AMI) is a critical endpoint of coronary heart disease (CAD), characterized by plaque rupture and acute thrombosis due to coronary atherosclerosis, leading to severe myocardial ischemia and tissue necrosis.1 AMI remains a leading cause of mortality worldwide, with a rising incidence and younger onset age. Reperfusion therapy, including percutaneous coronary intervention (PCI), is the primary treatment for AMI, significantly improving short- and long-term outcomes by promptly reopening infarct-related arteries and reducing myocardial damage.2 Since Andreas Gruentzig accomplished the first human percutaneous balloon angioplasty in 1977 and Sigwart et al successfully implanted the first coronary stent in 1987, the field of interventional cardiology has seen rapid advancement. According to Weaver et al,3 PCI in the management of AMI has demonstrated the ability to promptly and completely open the infarction-related artery (IRA) and achieve myocardial reperfusion. This method has evolved into the preferred treatment for AMI, suitable for over 90% of patients.4
However, substantial variability in patient prognoses following PCI persists, with mortality rates remaining as high as 10%. This variability is partly due to left ventricular remodeling (LVRM), which significantly influences cardiac function and long-term prognosis.5 LVRM is a complex process involving molecular and cellular mechanisms that alter myocardial structure and function following AMI.6 Factors influencing LVRM include infarct location, with anterior descending branch occlusions often leading to larger infarcts and worse outcomes.7 Research, such as that by Łoboz-Grudzień et al,8 has highlighted the location of myocardial infarction as a significant determinant affecting LVRM post-AMI. Studies have shown that lesions in the LAD, especially proximal occlusions, exhibit slower ST-segment resolution on electrocardiography following PCI. These lesions often lead to more severe left ventricular dysfunction, larger infarct sizes, and poorer prognosis due to increased myocardial involvement. A Cox regression analysis involving 7311 patients with angina pectoris and myocardial infarction across Western Europe, Israel, Canada, Australia, and New Zealand, as reported by Clayton et al,9 further highlighted the correlation between coronary imaging characteristics and patient prognosis.
fQRS, a novel electrocardiographic (ECG) marker, is closely associated with abnormal myocardial scar conduction, myocardial necrosis, and conduction delays in the peri-infarction area.10,11 The presence of fQRS has been observed across a wide spectrum of cardiovascular diseases, including cardiomyopathy, coronary slow flow, left ventricular asynchrony, atrial fibrillation, and various arrhythmias.12–14 Several studies have evaluated the predictive value of fQRS in patients with myocardial infarction. A meta-analysis conducted by Güngör et al15 explored the association between fQRS and both in-hospital and long-term cardiovascular events in patients with AMI. Their findings revealed that fQRS is correlated with mortality, major adverse cardiovascular events (MACE), diminished left ventricular function, and the presence of multivessel disease in these patients. Tanriverdi et al16 investigated the relationship between single-lead fQRS and prognosis in patients with ST-segment elevation myocardial infarction (STEMI) following successful reperfusion therapy. Although conventional criteria require fQRS to appear in at least two leads, their study suggested that in STEMI patients, the presence of fQRS in one or more leads indicates an elevated cardiac risk.
Given the considerable variability in the prognosis of patients with coronary artery disease following direct PCI, accurately identifying patients with poorer prognoses from complex clinical data is crucial for frontline clinicians. Presently, there is limited research on the correlation between fQRS and LVRM and adverse cardiovascular events in AMI patients. Therefore, the aim of this study was to analyze LVRM in AMI patients post-PCI and the incidence of MACE within a specific timeframe.
Data and Methods
General Information
This retrospective study was conducted at a single center. Based on prior studies and preliminary data, the estimated prevalence of the fQRS pattern in patients with AMI undergoing PCI is approximately 30%. To detect a clinically significant difference in the primary outcome (eg, incidence of major adverse cardiac events MACE) with a power of 80% and a significance level of 0.005, a minimum of 110 patients is required. A total of 122 patients diagnosed with AMI underwent PCI at our hospital between January 2021 and December 2022 and were included as subjects for this study.
Selection Criteria
Inclusion Criteria
- Patients meeting the diagnostic criteria outlined in the European Society of Cardiology’s 2017 Guidelines for the Management of Acute Coronary Syndrome with unsustained ST Elevation.17 A 12-lead Static ECG was recorded at admission and again at 24–48 hours after PCI. In instances of lower wall myocardial infarction, assessment of the post-PCI ECG extended to include the examination of leads V3R to V5R and VT to V9 as needed.
- Confirmation of fragmented QRS (fQRS) presence through the post-PCI ECG observation.18 The fQRS pattern is characterized by at least two consecutive leads with an RSR’ pattern (≥1 R waves or s waves being fragmented) and the absence of interventricular heart block. fQRS often manifests in the infarct-related artery supply area across two or more leads. Independent evaluation of fQRS was conducted by two experienced attending physicians, and any discrepancies in their assessments were resolved through discussion to arrive at a final determination.
- Patients experiencing their first onset of AMI.
- Availability of complete medical history data.
- Prior informed consent from both patients and their families regarding their participation in the study.
Exclusion Criteria
- Primary valvular heart disease (including mild forms).
- Presence of cardiomyopathy.
- Pre-excitation syndrome.
- Patients with uncontrolled infections or severe electrolyte disturbances.
- Individuals with intraventricular heart block who have undergone permanent pacemaker implantation.
- Patients diagnosed with known mental or intellectual developmental disorders or those unwilling to cooperate.
- Severe pulmonary, liver, or renal insufficiency.
- Recent use of anti-arrhythmic drugs such as bretylium and amiodarone.
- Presence of bundle branch blocks (RBBB or LBBB), as these conditions can interfere with the accurate identification of fQRS patterns.
Risk Stratification for NSTEMI Patients
For patients diagnosed with NSTEMI, cardiovascular risk stratification was performed at admission in accordance with the 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation.19 Patients were categorized into very high-, high-, and intermediate-risk groups based on established criteria. The very high-risk category includes patients with hemodynamic instability, cardiogenic shock, recurrent or ongoing chest pain refractory to medical treatment, life-threatening arrhythmias, mechanical complications of myocardial infarction, acute heart failure, or dynamic ST- or T-wave changes, particularly with intermittent ST-segment elevation. The high-risk category is defined by an established diagnosis of NSTEMI, dynamic or presumably new contiguous ST/T-wave changes, or a GRACE risk score >140. Finally, the intermediate-risk group includes patients with diabetes mellitus, renal insufficiency (eGFR <60 mL/min/1.73 m2), left ventricular ejection fraction (LVEF) <40%, or a GRACE risk score of 109–140 [1].
Data Collection and Biochemical Index Detection
General data were gathered, encompassing gender, age, body mass index, smoking history, and past medical records. The levels of creatine phosphokinase and creatine kinase isoenzyme were assessed through spectrophotometry using the Beckman Coulter AU680 automatic biochemical analyzer after centrifugation. Fasting venous blood samples were collected from patients on the morning following admission. Subsequently, after centrifugation, the supernatant was utilized for spectrophotometric analysis of total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), serum creatinine, blood urea nitrogen, and blood uric acid using an automatic biochemical analyzer.
Follow-up Process
Patients were followed for 1 year after the index procedure. The primary focus of follow-up was the occurrence of MACE. Clinical follow-up, including the assessment for MACE, was conducted through bi-monthly telephone interviews and by reviewing the hospital’s electronic medical records. Non-cardiac deaths, ie, those due to malignancy, were excluded from the MACE composite endpoint as per the defined study outcome In addition to clinical follow-up, echocardiographic examinations were systematically scheduled and performed at specified intervals (at 3, 6, and 12 months post-PCI) during outpatient visits to actively monitor changes in left ventricular structure and function. All follow-up data, both clinical and echocardiographic, were centrally recorded and managed. MACE was defined as a composite endpoint including recurrent myocardial infarction, heart failure requiring hospitalization, sudden cardiac death, stroke or transient ischemic attack.
Echocardiography
Following admission, patients underwent echocardiography examinations using the Philips HD3 color Doppler ultrasound equipped with a probe frequency of 2~4 MHz. The assessment routinely recorded the size of each ventricle and the thickness of the ventricular walls. Parameters such as left ventricular ejection fraction (LVEF), interventricular septal thickness (IVST), and left ventricular posterior wall thickness (LVPW) were specifically extracted and documented.
LVRM was defined based on changes in echocardiographic parameters. Specifically, LVRM was diagnosed if any of the following criteria were met: a decrease in LVEF to ≤45%, an increase in left ventricular end-diastolic dimension (LVEDd) by ≥20% compared to baseline, or an increase in left ventricular mass index (LVMI) by ≥20% compared to baseline. These indices were derived from measurements of LVEDd, interventricular septal depth (IVSd), and left ventricular posterior wall depth (PWd) taken from the left ventricular long-axis view. Additionally, the left ventricular mass index (LVMI) was calculated using the Devereux correction formula, where left ventricular mass (LVM) = 0.8 × {1.04 × [(LVEDd + IVSd + PWd)3 - (LVEDd)3]} + 0.6. LVMI was determined by dividing LVM by the body surface area (BSA), calculated as BSA (m2) = 0.0061 × body height (cm) + 0.0128 × body mass (kg) - 0.1529.20
Electrocardiogram (ECG) Monitoring
The fQRS diagnosis was based on a standard 12-lead ECG obtained 24–48 hours after the successful PCI procedure. This timing was chosen to allow for stabilization of the initial ischemic injury and to ensure that the identified fQRS complex represents the established infarct-related scar tissue after reperfusion. The same filter settings (0.05--100 Hz) and assessment criteria by two experienced physicians were applied. Patients were then categorized into fQRS and non-fQRS groups.
Statistical Analysis
The collected data were analyzed using SPSS 21.0 software. Categorical data were presented as percentages (%), while continuous variables were expressed as mean ± standard deviation (x ± s). Group comparisons were conducted using the X^2 test for categorical data and the t-test for continuous variables.
Survival analysis for MACE was performed using Kaplan-Meier survival curves with the Log rank test, with time zero defined as the date of the post-PCI ECG. Cox proportional hazards regression analysis was employed to identify independent predictors of MACE. Logistic regression analysis was used to identify independent predictors of LVRM.
The criteria for inclusion and exclusion in the analysis were set at P<0.10 and P<0.15, respectively. These criteria were used to select variables for inclusion in the multivariate analysis based on their univariate associations with the outcome. Selection of dependent and independent variables was based on specific circumstances. All statistical tests were two-sided, and a P-value <0.05 was considered statistically significant.
Results
Comparison of Two Groups of Basic Data
Based on the presence or absence of fQRS on the post-PCI ECG, the 122 patients were categorized into two groups. The fQRS group consisted of 48 patients (39.3%), while the non-fQRS group comprised 74 patients (60.7%). The baseline clinical characteristics of the two groups are summarized in Table 1. There were no significant differences in gender, age, BMI, smoking history, and past medical history between the groups (P > 0.05). Consistent with the more severe initial injury often associated with subsequent scar formation, the fQRS group had a significantly higher proportion of STEMI patients compared to the non-fQRS group (77.1% vs 48.6%, P = 0.002). Similarly, among the 56 NSTEMI patients, the distribution across risk categories (very high, high, intermediate) was comparable between the two groups (P = 0.554).
 |
Table 1 Baseline Clinical Characteristics |
Comparison of Serum and Heart-Related Indexes
Comparative analysis of serum and cardiac biomarkers demonstrated significant differences between the groups (Table 2). Patients in the fQRS group exhibited a more adverse lipid profile, characterized by significantly higher levels of TC and LDL-C, and lower levels of HDL-C (all P < 0.01). Furthermore, markers of myocardial necrosis (cTnI, CPK, CK-MB) were substantially elevated in the fQRS group (all P < 0.001), consistent with a greater extent of myocardial injury. Parameters indicative of renal function and metabolic status (Scr, BUN, Blood UA) were also less favorable in the fQRS group (all P < 0.05).
 |
Table 2 Comparison of Serum and Heart-Related Indexes Between Two Groups |
Comparison of LV Function Between Two Groups
Echocardiographic assessment of left ventricular function and structure revealed significant impairments in the fQRS group (Table 3, Figure 1). Compared to the non-fQRS group, patients with fQRS had a significantly lower left ventricular ejection fraction (LVEF) and greater wall thickness, as evidenced by increased interventricular septal thickness (IVST) and left ventricular posterior wall (LVPW) thickness (all P < 0.001). These findings are consistent with more pronounced left ventricular dysfunction and early remodeling in patients with post-infarct fQRS.
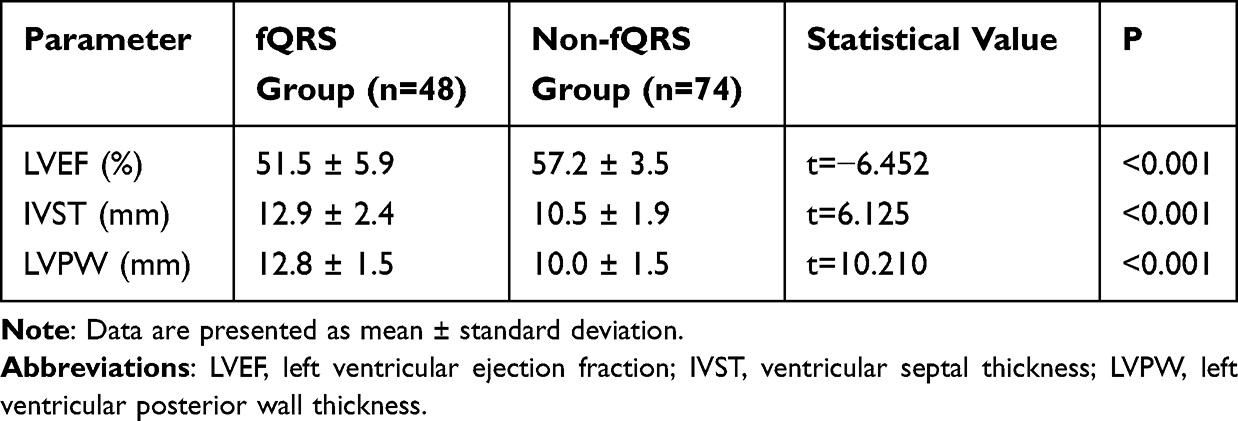 |
Table 3 Comparison of LV Function Between Two Groups |
 |
Figure 1 Comparison of left ventricular (LV) function and structure parameters between patients with fragmented QRS complex (fQRS) and those without (Non-fQRS). Violin plots with overlaid boxplots show distributions of left ventricular ejection fraction (LVEF), interventricular septal thickness (IVST), and left ventricular posterior wall thickness (LVPW) across two groups. ****P < 0.001, independent t-test. Horizontal lines with asterisks indicate the level of statistical significance. |
The Occurrence of MACE During Follow-up
Over the one-year follow-up, the cumulative incidence of MACE was significantly higher in the fQRS group compared to the non-fQRS group (35.4% vs 10.8%, P < 0.001) (Table 4 and Figure 2). Kaplan-Meier survival analysis confirmed a significantly higher event-free survival rate in the non-fQRS group (Log-rank P < 0.001). The distribution of individual MACE components is detailed in Table 4.
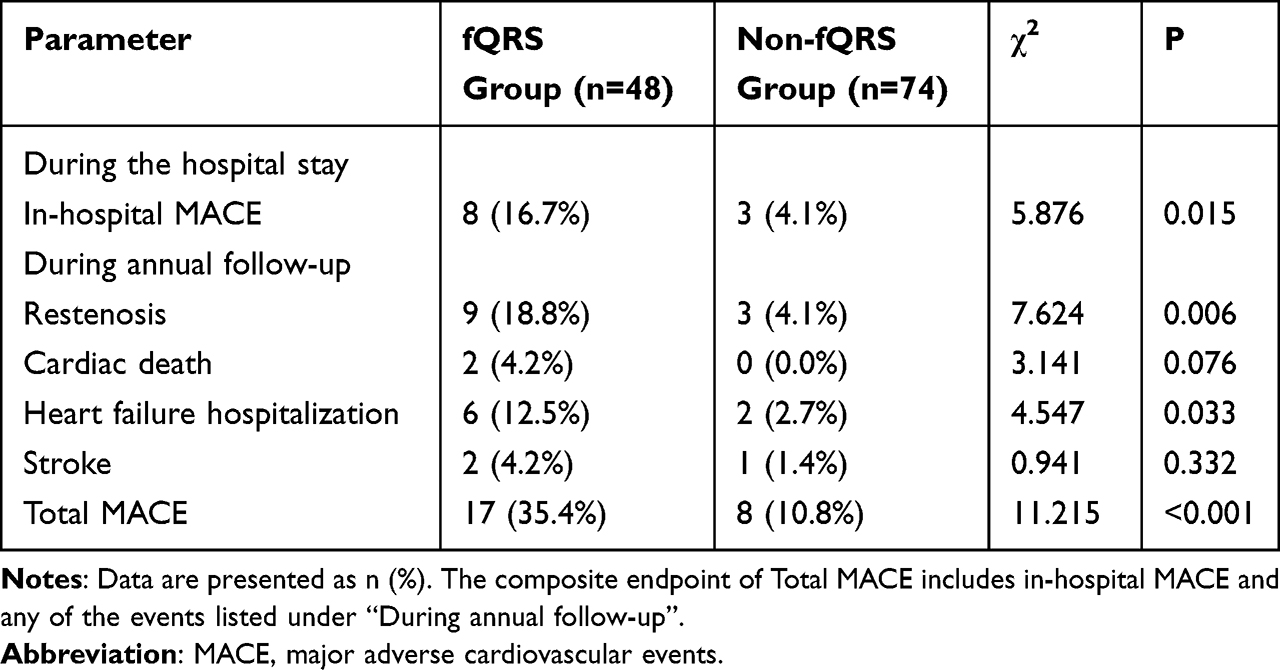 |
Table 4 The Occurrence of MACE |
 |
Figure 2 Incidence of major adverse cardiovascular events (MACE) components during one-year follow-up between fQRS and Non-fQRS groups. Bar plots display the number of cases of restenosis, cardiac death, heart failure hospitalization, and total MACE in each group. |
Logistic Regression Analysis
Multivariable regression analyses were performed to identify independent predictors of the primary outcomes. In the Cox proportional hazards model for MACE, which included gender, hypertension, diabetes, hyperlipidemia, ST-segment resolution, infarct location, and post-PCI fQRS, the presence of post-PCI fQRS remained a strong independent predictor (HR: 2.65, 95% CI: 1.52–4.63, P = 0.001). Anterior myocardial infarction (HR: 2.55, 95% CI: 1.50–4.35, P = 0.001) and diabetes mellitus (HR: 2.20, 95% CI: 1.10–4.39, P = 0.026) were also identified as significant independent risk factors for MACE.
Furthermore, in a logistic regression model adjusted for potential confounders, post-PCI fQRS was confirmed to be an independent risk factor for the development of LVRM (OR: 3.12, 95% CI: 1.48–6.55, P = 0.003).
Discussion
The principal finding of our study is that the fragmented QRS complex, identified on ECG 24 to 48 hours after primary PCI, serves as a significant and independent predictor of both left ventricular remodeling and major adverse cardiovascular events in patients with acute myocardial infarction. This specific timing for fQRS assessment was deliberately chosen to capture the established infarct-related scar tissue after reperfusion, thereby providing a more robust evaluation of its prognostic utility.
Our data demonstrate that patients with post-PCI fQRS sustained more severe myocardial injury, as evidenced by significantly elevated levels of cardiac troponin I and creatine kinase-MB, consistent with a larger infarct size.21 This group also exhibited a more adverse metabolic profile and signs of early structural remodeling, characterized by lower LVEF and greater ventricular wall thickness. These findings align with the pathophysiological concept that fQRS signifies a substrate of myocardial scar and conduction heterogeneity, which arises from mechanisms such as local scarring and peri-infarct block, leading to disrupted depolarization.22,23 This electrical disorganization is increasingly recognized as a marker of the underlying substrate that promotes mechanical dyssynchrony and adverse remodeling,24,25 a process intimately linked to heart failure progression and poor long-term outcomes.26
The prognostic significance of fQRS was further underscored by a markedly higher incidence of MACE during follow-up, a finding that persisted after comprehensive adjustment for potential confounders. The strong association we observed aligns with and extends previous research. A meta-analysis by Güngör et al15 and others have previously linked fQRS to mortality, diminished left ventricular function, and multivessel disease in AMI patients.27 Our study strengthens this evidence by specifically linking the fQRS complex observed after successful revascularization to subsequent risks, thereby providing a more refined temporal link between the established scar and future events. Our results are also in concordance with studies that have associated fQRS with the severity of coronary artery lesions and cardiac events.28,29
Several limitations of our study warrant consideration. First, the single-center, retrospective observational design inherently limits causal inference. Second, although our sample size was adequate for the primary analyses, a larger cohort would provide greater statistical power for analyzing individual MACE components. Third, we did not systematically collect data on arrhythmic events, which represent important outcomes related to the electrically unstable substrate that fQRS may represent. Future prospective, multicenter studies are needed to validate our findings and explore the underlying mechanisms in greater depth.
Conclusion
The fQRS complex on a standard ECG performed after PCI is a readily available, non-invasive marker that identifies AMI patients at high risk for left ventricular remodeling and major adverse cardiovascular events. Its integration into routine risk stratification protocols could help in tailoring more intensive follow-up and management strategies for this vulnerable patient subgroup.
Data Sharing Statement
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of The Second Affiliated Hospital of Wenzhou Medical University (2021-K-199-01). Informed consent was obtained from all the participants. All methods were carried out in accordance with Declaration of Helsinki.
Consent for Publication
All the authors confirming that written informed consent was obtained from all subjects and/or their legal guardian(s).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Khan S, Al Miraj AK. Clinical profile of right ventricular infarction in patients with acute inferior wall myocardial infarction. Sch Int J Tradit Complement Med. 2021;4(10):203–10.
2. Maznyczka AM, Oldroyd KG, McCartney P, McEntegart M, Berry C. The potential use of the index of microcirculatory resistance to guide stratification of patients for adjunctive therapy in acute myocardial infarction. JACC. 2019;12(10):951–966. doi:10.1016/j.jcin.2019.01.246
3. Weaver WD, Simes RJ, Betriu A, et al. Comparison of primary coronary angioplasty and intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review. JAMA. 1997;278(23):2093–2098. doi:10.1001/jama.1997.03550230069040
4. Kandaswamy E, Zuo L. Recent advances in treatment of coronary artery disease: role of science and technology. Int J Mol Sci. 2018;19(2):424. doi:10.3390/ijms19020424
5. Shohel SR, Rahaman AFMA, Ahmed IU. Outcome of primary angioplasty as compared with thrombolytic therapy for acute myocardial infarction. Cardiovasc J. 2023;15(2):142–149.
6. Frantz S, Hundertmark MJ, Schulz-Menger J, Bengel FM, Bauersachs J. Left ventricular remodelling post-myocardial infarction: pathophysiology, imaging, and novel therapies. Eur Heart J. 2022;43(27):2549–2561. doi:10.1093/eurheartj/ehac223
7. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–e639. doi:10.1161/CIR.0000000000001052
8. Łoboz-grudzień K, Kowalska A, Brzezińska B, Sokalski L, Jaroch J. Early predictors of adverse left ventricular remodelling after myocardial infarction treated by primary angioplasty. Cardiol J. 2007;14(3):238–245.
9. Clayton TC, Lubsen J, Pocock SJ, et al. Risk score for predicting death, myocardial infarction, and stroke in patients with stable angina, based on a large randomised trial cohort of patients. BMJ. 2005;331(7521):869. doi:10.1136/bmj.38603.656076.63
10. Cho HJ, Yoon JY, Kim N, et al. Predictive value of a fragmented QRS complex in diagnosing patients with myocardial ischemia. Clin Cardiol. 2019;42(3):379–384. doi:10.1002/clc.23148
11. Hagiwara H, Watanabe M, Kadosaka T, et al. Fragmented QRS on 12-lead electrocardiogram predicts long-term prognosis in patients with cardiac sarcoidosis. Heart Vessels. 2023;38(6):803–816. doi:10.1007/s00380-022-02229-2
12. Kamal D, Hashem M. Role of QRS fragmentation in 12-lead surface ECG in prediction of isolated epicardial coronary artery ectasia and its anatomical distribution in patients without acute coronary syndromes. Egypt Heart J. 2020;72(1):28. doi:10.1186/s43044-020-00054-4
13. Vandenberk B, Robyns T, Goovaerts G, et al. Inter- and intra-observer variability of visual fragmented QRS scoring in ischemic and non-ischemic cardiomyopathy. J Electrocardiol. 2018;51(3):549–554. doi:10.1016/j.jelectrocard.2017.12.002
14. Yılmaz AS, Şatıroğlu Ö, Çetin M. Fragmented QRS predicted major adverse cardiovascular events in patients with coronary artery disease and percutaneous coronary intervention, 10-years of follow-up. Kardiologiia. 2022;62(1):72–79. doi:10.18087/cardio.2022.1.n1679
15. Güngör B, Özcan KS, Karataş MB, Şahin İ, Öztürk R, Bolca O. Prognostic value of QRS fragmentation in patients with acute myocardial infarction: a meta-analysis. Ann Noninvasive Electrocardiol. 2016;21(6):604–612. doi:10.1111/anec.12357
16. Tanriverdi Z, Dursun H, Colluoglu T, Kaya D. Single derivation fragmented QRS can predict poor prognosis in successfully revascularized acute STEMI patients. Arq Bras Cardiol. 2017;109(3):213–221. doi:10.5935/abc.20170099
17. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
18. Fedulaev YN, Makarova IV, Pinchuk TV, Chuvarayan GA. QRS-fragmentation: perspectives for use in clinical practice. Ann Russ Acad Med Sci. 2021;76(3):279–286.
19. Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Rev Esp Cardiol. 2021;74(6):544. doi:10.1016/j.rec.2021.05.002
20. Devereux RB, Alonso DR, Lutas EM, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986;57(6):450–458. doi:10.1016/0002-9149(86)90771-X
21. Chetran A, Costache AD, Ciongradi CI, et al. ECG and biomarker profile in patients with acute heart failure: a pilot study. Diagnostics. 2022;12(12):3037. doi:10.3390/diagnostics12123037
22. Das MK, Khan B, Jacob S, Kumar A, Mahenthiran J. Significance of a fragmented QRS complex versus a Q wave in patients with coronary artery disease. Circulation. 2006;113(21):2495–2501. doi:10.1161/CIRCULATIONAHA.105.595892
23. Gasowska-Bajger B, Gasowska-Bodnar A, Knapp P, Bodnar L. Prognostic significance of survivin expression in patients with ovarian carcinoma: a meta-analysis. J Clin Med. 2021;10(4):879. doi:10.3390/jcm10040879
24. Aimo A, Gaggin HK, Barison A, Emdin M, Jl J Jr. Imaging, biomarker, and clinical predictors of cardiac remodeling in heart failure with reduced ejection fraction. JACC Heart Fail. 2019;7(9):782–794. doi:10.1016/j.jchf.2019.06.004
25. Leancă SA, Crișu D, Petriș AO, et al. Left ventricular remodeling after myocardial infarction: from physiopathology to treatment. Life. 2022;12(8):1111. doi:10.3390/life12081111
26. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur J Heart Fail. 2022;24(1):4–131. doi:10.1002/ejhf.2333
27. Luo G, Li Q, Duan J, Peng Y, Zhang Z. The predictive value of fragmented QRS for cardiovascular events in acute myocardial infarction: a systematic review and meta-analysis. Front Physiol. 2020;11:1027. doi:10.3389/fphys.2020.01027
28. Attachaipanich T, Krittayaphong R. Fragmented QRS as a predictor of in-hospital life-threatening arrhythmic complications in ST-elevation myocardial infarction patients. Ann Noninvasive Electrocardiol. 2019;24(1):e12593. doi:10.1111/anec.12593
29. Fedulaev Y, Makarova I, Pinchuk T. Fragmented QRS as a marker of coronary atherosclerosis severity evaluated by the Gensini score. Ann Cardiol Angeiol. 2021;70(3):143–147. doi:10.1016/j.ancard.2021.03.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pan-Immune-Inflammatory Value Predicts the Risk of Myocardial Infarction Among Patients with Unstable Angina Pectoris and the Outcomes After Percutaneous Coronary Intervention
Chen C, Zhao B, Fan Y, Peng J
International Journal of General Medicine 2025, 18:7433-7445
Published Date: 10 December 2025
Universal Early Discharge Protocol for Acute Myocardial Infarction: A Single-Center Prospective Validation
Bauer D, Berka V, Neuberg M, Odvodyová D, Maliničová I, Lašmanská S, Smitalová S, Mašek P, Kočka V, Moťovská Z, Kozel M, Bartošková K, Toušek P
Vascular Health and Risk Management 2026, 22:581820
Published Date: 9 April 2026