Back to Journals » Infection and Drug Resistance » Volume 12
Application of the susceptible–infected–recovered deterministic model in a GII.P17 emergent norovirus strain outbreak in Romania in 2015
Authors Popovici ED ![]() , Negru DG
, Negru DG ![]() , Olariu T
, Olariu T ![]() , Nagy M
, Nagy M ![]() , Dinu S, Oprisan G, Zota L, Baditoiu LM
, Dinu S, Oprisan G, Zota L, Baditoiu LM ![]()
Received 5 February 2019
Accepted for publication 17 June 2019
Published 16 August 2019 Volume 2019:12 Pages 2543—2551
DOI https://doi.org/10.2147/IDR.S204175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Emilian Damian Popovici,1,2 Dana Gabriela Negru,3 Teodora Olariu,4 Mariana Nagy,5 Sorin Dinu,6 Gabriela Oprisan,6,7 Lavinia Zota,8 Luminita Mirela Baditoiu1
1Epidemiology Department, “Victor Babeş” University of Medicine and Pharmacy, Timişoara, Romania; 2National Institute of Public Health, Regional Public Health Centre, Timişoara, Romania; 3Private Medical Epidemiology Practice, Arad, Romania; 4Arad County Clinical Hospital, Arad, Romania; 5Department of Mathematics and Computer Science, "Aurel Vlaicu" University of Arad, Arad, Romania; 6Molecular Epidemiology Laboratory, Cantacuzino National Medical – Military Institute of Research and Development, Bucharest, Romania; 7Faculty of Pharmacy, "Titu Maiorescu" University, Bucharest, Romania; 8National Institute of Public Health, National Centre for Surveillance and Control of Communicable Diseases, Bucharest, Romania
Correspondence: Emilian Damian Popovici
Epidemiology Department, “Victor Babeş” University of Medicine and Pharmacy, No. 2, Piata Eftimie Murgu, Timişoara 300041, Romania
Tel +40 74 420 6030
Fax +40 25 649 2101
Email [email protected]
Purpose: This study shows the epidemiological profile of the first gastroenteritis outbreak of GII.P17 in the Romanian territory. An outbreak with such large amplitude in a European territory was previously undocumented.
Patients and methods: Using a cross-sectional design, with the susceptible-infected-recovered (SIR) deterministic compartmental model for a fixed population, and the cluster method for establishing the high-incidence zones, we carried out our investigation by means of questionnaires containing personal data, affected collectivities, disease onset and duration, symptoms displayed, medical assistance provided, previous antibiotic intake where applicable, food consumption and water sources, and sanitation conditions. The confirmation of cases was done based on the typical norovirus gastroenteritis symptomatology and using three laboratory confirmations (by molecular diagnosis) for GII.P17-GII.17 genotype noroviruses from three patients.
Results: A gastroenteritis outbreak occurred in October–November 2015, affecting 328 people in Arad, a county in Western Romania, covering 44 neighbouring localities with a total population of 35,440 people. The study detected an inter-human transmission of the infection, with an intrafamilial risk of disease of 2.26 (95% CI 1.76 to 2.90) compared with the community transmission (in school collectivity). The basic reproduction number Ro dropped from 1.26 to 0.18 during weeks 43:44, after controlling the transmission by decontamination and isolation.
Conclusion: SIR made it possible to highlight the expansion of the emerging norovirus strain infection from community to family collectivities. This study provides practical solutions to limit disease cases, even in the absence of etiology, and shows the importance of sometimes underestimated traditional control methods.
Keywords: norovirus, GII.17_Kawasaki, SIR, basic reproduction number
Introduction
Acute diarrheal disease (ADD) as a result of a norovirus infection is the most frequent gastrointestinal condition, accounting for one-fifth of all ADD cases worldwide, half of community-recorded ADD outbreaks, with a total of approximately 700 million cases and 200,000 deaths each year.1–4
The viruses, which are known by their high infectivity, can be transmitted through 3 main routes: contaminated water and food, interpersonal contact, and aerosols.1 There is autumn–winter–spring seasonality for norovirus-based gastroenteritis, characterized by an incubation period of 1–2 days, sudden onset through nausea, abdominal pain, vomiting, and often with sudden remission after another 1–3 days.5
Noroviruses, single-stranded positive-sense RNA viruses belonging to Caliciviridae Family, are currently classified in seven genogroups, from GI to GVII, based on amino acid differences present in the major structural protein (VP1).4 These genogroups are further divided in genotypes based on differences in the RNA polymerase region (polymerase genotype) and in the VP1 (capsid genotype). The strains infecting the human species belong to genogroups GI, GII, and GIV.2,6,7 There are 9 genotypes belonging to GI, 22 belonging to GII, and 2 genotypes to GIV.6,8
Of these, GII.4 viruses were prevalent since the mid-1990s, with an emergence of new variants typically every 2–3 years, as a consequence of point mutations and intragenotype recombination.6,9 Such pandemic GII.4 strains were US96, Farmington Hills 2002, Hunter 2004, Den Haag 2006b, New Orleans 2009, and Sydney 2012.10,11 Although the genotype GII.17 has been known to circulate among the human population since as early as 1978, it has sporadically been detected in Africa, Asia, Europe, North America, and South America, being associated with acute gastroenteritis in children and adults, including 4 outbreaks reported in the United States between 2000 and 2013.12 The emergence of new GII genotype 17 (known as Kawasaki 308) was signaled from November to December 2014 as an etiological agent in the gastroenteritis-based epidemic outbreaks in China (comprising at the same time at least 9 regions, from Beijing to Guangdong Province) and between December 2014 and March 2015 in Kawasaki, in Japan.11,13–15
The GII.17 strain was also isolated in Hong Kong, in January–February 2015 in Taiwan, in South Korea, Nova Scotia/Canada, in USA, Brazil, Victoria/Australia, New Zealand, and South Africa.2,6,7,16–19 In Europe, the emerging strain GII.17_Kawasaki was identified in sporadic cases in 2015 in Italy, the Netherlands, Russia, but also in outbreaks between September and December 2016 in Germany.7,12,19,20
Mathematical models (the Kermack–McKendrick epidemic model or the Reed–Frost epidemic model) are used increasingly often to study the transmission of infectious diseases, to define the epidemic manifestation, and to assess the efficiency of control measures in reducing morbidity. In deterministic epidemic models, the people are assigned to one of the several different compartments. In Kermack-McKendrick’s SIR compartmental model, the entire population (considered to be constant in size, N = S + I + R) was divided into three compartments: Susceptible (S) – in which the people are susceptible if they have contact with a disease, people who were not actively or passively immunized; Infected (I) – this included all the people infected, capable of transmitting the disease to others; and Recovered/Resistant (R) – this included people that had already had the infection and were immunized. The model is used for describing the spread of viral diseases.
Aims
This article sets out to investigate the first GII.17_Kawasaki outbreak on the Romanian territory, which occurred between 16 October and 30 November 2015 (and was reported at European level in February 2016), using the SIR (Susceptible, Infected, Recovered) deterministic compartmental model for a fixed population.21
Materials and methods
Outbreak detection
The passive epidemiological surveillance system, regulated in Romania by Government Decision no 589/2007, based on clinical, laboratory, and epidemiological criteria, with outbreaks that reach 20 cases being reported to the public health authority, identified a higher ADD incidence in weeks 29–49 for the year 2015 in Arad County compared with the same period in 2014.22
Usually, the annual seasonality in Romania shows incidence peaks between the months of May and October, the etiology remains unmentioned for 98% of hospitalized cases, and clinical forms have a self-limited evolution in most cases. In 2015, the gastroenteritis onset occurred in October, with an evolution simultaneous to that of cold-season respiratory infections, characteristic of the northern hemisphere. The first cases were reported on 18 October 2015, in patients arriving at the Sebiș Hospital emergency ward, but the investigation later revealed cases with an onset as early as 16 October 2015. Cases were also reported in real time by the second hospital in this territory, by doctors involved in school health care services and by family doctors throughout the territory, with 44 villages and a total population of 35,440 inhabitants.
Establishing the case definition and methods for identifying/counting cases
The cases were classified into:
Probable cases – patients (regardless of gender, age, status – inpatients or outpatients), with at least two of the following 4 symptoms: diarrhea with at least 3 watery soft unformed stools in the past 24 hrs, vomiting, nausea and abdominal pain, present between 10 October and 1 December 2015, in the Sebiș area, with no other toxic, bacteriological, parasitic, or viral identified cause (n=325);
Confirmed cases were probable cases additionally testing positive for norovirus GII.17_Kawasaki by reverse transcription-polymerase chain reaction (RT-PCR) (n=3).
The samples submitted for molecular diagnosis came from the 4 most affected localities in the specified area, from probable cases that had ≥4 contacts who developed gastroenteritis during the specified time.
The definition of the ADD outbreak was: two or more cases with vomiting and diarrhea, with the GII.17_Kawasaki norovirus presence laboratory confirmed in at least two patients in a set period of time, with the epidemiological link established based on belonging to the same school or family collectivity (according to the CDC methodology).1
To calculate the susceptible population, it was considered that all patients had three types of contacts: family, work/school contacts, and other social contacts. For each pediatric patient, only family contacts and school colleagues were considered, and if there were multiple pediatric cases in the same class, these contacts were counted only once. For adult patients, family contacts and 13 social contacts per day per person were considered, and if there were multiple adult cases in the same family, those contacts were counted only once.
Study design
In this cross-sectional observational study, we used the SIR (Susceptible, Infected, Recovered) deterministic compartmental model, without demography (excluding births and deaths), for the population in the whole Sebiș territory, Romania, as well as the cluster method for establishing the high-incidence zones.23
The basic reproduction number R0 was calculated, defined as “the average number of secondary infections occurring when one infected person is introduced into a completely susceptible population”, with the formula Ro= C × P × D, where C stands for contacts, P is the infection probability among contacts, and D is the contagiousness duration.24,25 The attack rate was calculated as the total number of cases divided by the total population at risk.
The use of data in this study was done observing the confidentiality and ethical principles for medical research involving human subjects, as imposed by the World Medical Association Declaration of Helsinki.26 As the study relies on data from the national communicable disease surveillance system, it was not necessary to request patients’ informed consent regarding this study. However, written informed consent was requested and obtained from patients from whom biological samples were taken, as well as from parents/legal guardians where the patients were minors. The study was approved by the Ethics Committee of the Arad Public Health Department (ref. no. 01/11.01.2017).
Microbiological analysis
The fecal samples for the bacteriological examination were taken in harvesters that had the Carry-Blair transport medium (Polymed Trade, Bucharest, Romania). In order to exclude the involvement of Salmonella spp. strains, the samples were initially seeded on the selenite broth, then on the SS medium (MLT, Arad, Romania). On the SS environment, the possible strains of Shigella spp. were also found, while for Yersinia spp., CIN-cefsulodin irgasan novobiocin medium was used (MLT, Arad, Romania). Seeding on the Mac Conkey medium with sorbitol (Sanimed, Bucharest, Romania) and using Escherichia coli O157- and Escherichia coli H7 (Denka Seiken, Tokyo, Japan)-specific agglutination serums enabled the exclusion of these strains. For children below 2 years of age, E. coli colonies were tested with polyvalent serums (Denka Seiken, Tokyo, Japan) for the purpose of excluding enteropathogen E. coli. The screening for protozoa and helminths was done both by direct microscopy (in lugol solution) and by the Willis-Hung hydrostatic method.
The presence of rotavirus and adenovirus strains was investigated by a commercial immunochromatographic rapid test: Adenovirus Test/Rotavirus Test (NADAL, Moers, Germany). By the same method, the noroviruses were initially investigated using Norovirus GI/GII Test (RIDA®QUICK Norovirus Test, Darmstadt, Germany).
Five fecal samples collected between 25 October and 17 November 2015 were sent to the Cantacuzino Institute reference laboratory in Bucharest.
Molecular analysis norovirus detection and typing
Here, viral RNA was extracted from 140 µL of PBS stool suspension (10% wt/vol) using QIAamp RNA Viral Mini Kit (Qiagen). A fragment of 1111 nt spanning the ORF1-ORF2 (RdRp-VP1) junction, a region recommended for norovirus typing, was amplified using primers JV12 and G2SKR.27 Three out of five samples yielded a PCR product suitable for sequencing (one sample from an adult and two samples from two young children). Sequencing was performed with BigDye Terminator v3.1 (Applied Biosystems) and Norovirus Genotyping Tool was employed for assigning genotype.28 The three sequences obtained were identical and the typing results indicated genotype GII.P17-GII.17. The sequences were deposited in GenBank under the accession numbers LT160589, LT160590, and LT160591. Phylogenetic analysis was conducted with Mega 6 software, neighbor-joining statistical method, Kimura 2-parameter, 1,000 bootstrap replications.28,29
Statistical analysis
The statistical analysis of the database was performed using the SPSS, version 20.0 (IBM, Chicago, IL). To determine the geospatial case distribution, ClusterSeer Demo version 2.5 (BioMedware, Ann Arbor) was used, with the application of statistical tests for cluster detection – the Cuzick-Edwards test and the Besag-Newell method.30 Frequencies, ratios, and proportions were used to summarize demographic data. To quantify the risk in the 2 types of collectivities, the contingency table was used, with a calculation of the chi2 and OR (Odd ratio) tests. The R2 goodness-of-fit coefficient was evidenced by linear regression.
Results
The active registration of all ADD cases related to the Sebiș territory by households, kindergartens, schools, or workplaces for the 10 October–1 December 2015 period reached a total number of 328 ADD cases, the gender ratio being 0.78:1; namely 145 male:183 female. The patients’ median age was 18 years, their mean age was 26.92 years (Standard Deviation: 22.01; Interquartile range: 10–40; age range: 1–95 years). Counting cases and finding their contacts, investigating absenteeism in schools and workplaces led to establishing 1186 kindergarten and school contacts at risk, 984 family contacts at risk, and 33,002 total population at risk (in the context of markets, fairs, collective activities, public transportation, etc.).
The daily case distribution was continuous at first and intermittent subsequently (Figure 1).
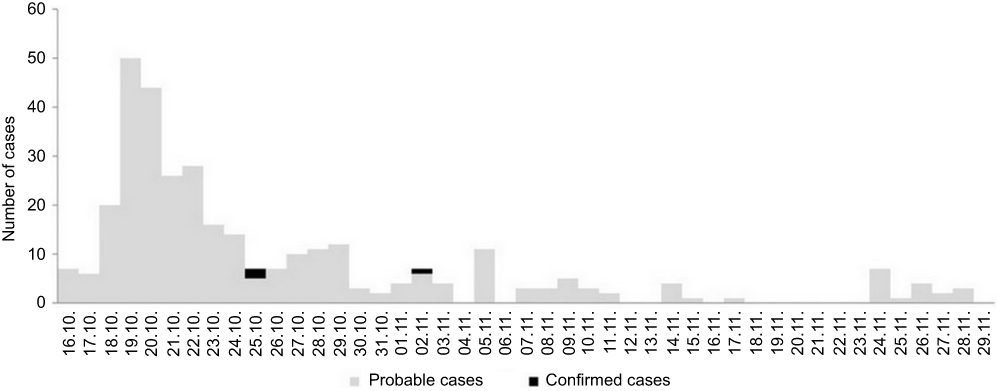 |
Figure 1 Outbreak of norovirus gastroenteritis – daily case distribution, Sebis area, Romania, 2015.Note: 16.10. to 29.11 represent dates from October 16 to November 29. |
The cases were either grouped in clusters (n = 302) or sporadic (n=26). A number of 114 cases were recorded in collectivities of children, kindergartens, schools. The Geospatial distribution of the cases has identified 28 ADD clusters, shown in Figure 2.
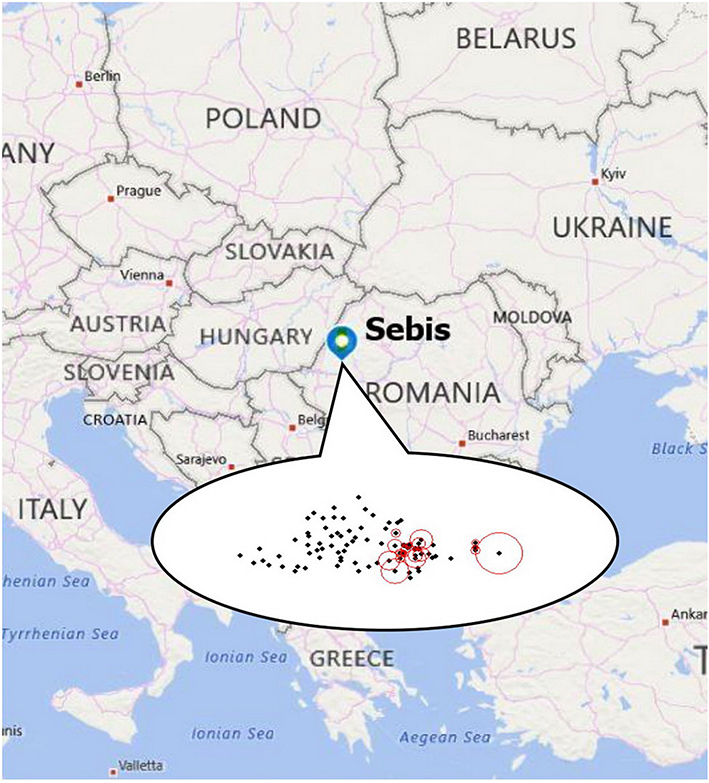 |
Figure 2 Outbreak of norovirus gastroenteritis, Sebis area, Romania, 2015 (cluster seer map, k10 cut-off).Note: The red-circled dots highlight the clusters identified after the software application (localities in which there are several cases). |
The attack rate for intrafamilial gastroenteritides was 21.75% versus 9.61% in kindergarten and school collectivities and 0.99% per total (Table 1). OR calculations revealed that the likelihood of people getting sick was higher in family collectivities versus preschool/school collectivity.
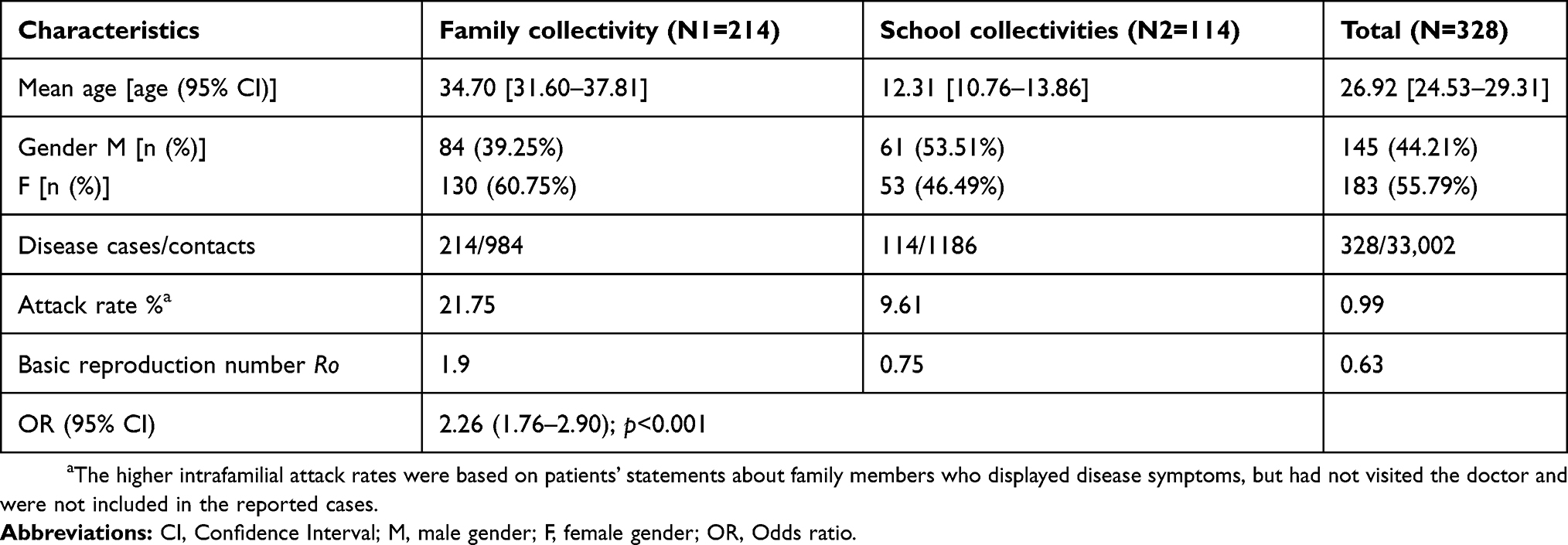 |
Table 1 Analytical statistics |
The disease onset was sudden, with no prodrome, through nausea (n=220, 67.07%), incoercible vomiting (n=214, 65.24%), abdominal pain (n=178, 54.27%), diarrhea (n=168, 51.22%), headache (n=100, 30.49%), dehydration (n=30, 9.15%), fever (n=20, 6.09%), and the disease remission was spectacular, just as sudden, through supportive treatment. The disease severity forms were mild and medium, with 8 (2.44%) cases hospitalized, 206 (62.80%) cases treated in the hospital outpatient ward, and 114 (34.76) cases by the family doctor. 3.35% of the patients had previous antibiotic treatment for other intercurrences. There were no complications or deaths; 2.44% were occupational & HCAIs (health care-associated infections), 10.36% were intrafamilial/household cases/retired people, and 33.23% of the cases occurred among kindergarten or school children, with a possible double source – school and family.
The SIR (Susceptible, Infected, Recovered) deterministic compartmental models used the following ordinary differential equations (ODEs): estimated average period of infection: 2 days, infection rate: one new person every other day, β (transmission rate) =1/2, γ (recovery rate) =1/2. (Figure 3)
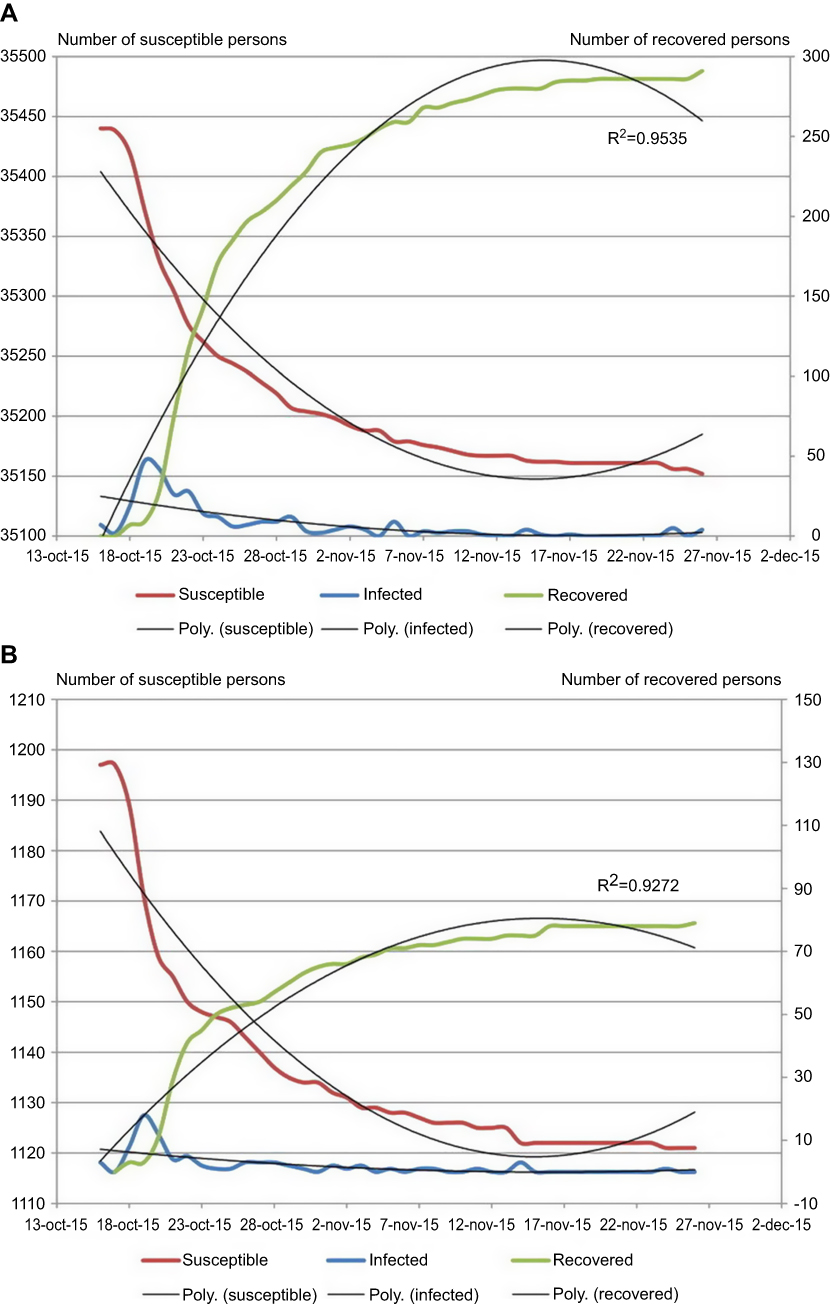 |
Figure 3 Outbreak of norovirus gastroenteritis – solution curves in the SIR without vital dynamics event, Romania, 2015. (A) in the Sebis area; (B) in the school collectivities.Abbreviations: SIR, susceptible-infected-recovered deterministic compartmental model; poly, polynomial approximations. |
The evolution was typical for inter-human transmission, with a peak in week 43 (between 18 and 24.10), when there was continuous transmission. In October, 264 cases were infected versus 64 cases in November, when the epidemic curve began to indicate intermittent transmission. Corroborating the SIR pattern for the population in the entire Sebiș territory with the one in the kindergartens and school children’s collectivities reveals that the peaks epidemics occur at the same time, with a quick lapse for week 44 (25 October to 1 November) in school and slower in the general population, which shows the contribution of kindergarteners and school children in accelerated the transmission of the infection.
The decrease or increase of the ratio for the highest and lowest frequency of cases between two full weeks is a prognosis indicator to assess the infection strength and is always followed by a change in the basic reproduction number Ro, so the 14:198 for weeks 42:43 becomes 198:52 for weeks 43:44, accompanied by a change of the Ro from 1.26 to 0.18.31 This downward trend was concurrent with the application of decontamination measures, of personal/collective hygiene and health education initiated from week 44, in kindergartens and school collectivities.
To exclude the possible etiologies, 151 stool tests were performed, of which 72 were associated with a coproparasitological test (especially to children), 50 samples were tested for the exclusion of adenoviruses and rotaviruses, 5 samples were tested for the exclusion of the Coxsackie enteroviruses, including 4 samples submitted for rapid norovirus tests. The microbiological analyses were performed both before and after diagnosis confirmation by molecular analysis. Biological samples were negative for adenoviruses, rotaviruses, and noroviruses, through rapid screening diagnostic tests. They were also negative for bacterial and parasitic etiology, while other causes, such as mushroom poisoning, were ruled out by case history. The Cantacuzino Institute in Bucharest identified the presence of norovirus GII.P17-GII.17 in the biological samples of three of the patients (one sample from an adult and two samples from two young children), and the presence of norovirus GII was confirmed in the fourth, without genotyping.21 Positive samples were taken on October 25 (2), November 2, and November 17 (each 1 sample). The phylogenetic analysis, previously published in a quick communication in Eurosurveillance, placed the norovirus strains in the same sub-cluster with the Kawasaki 308 strain, identified in Japan in 2015.21
Discussion
This outbreak in West Romania, which lasted 46 days during October–November 2015 and was caused by the strain GII.P17-GII.17 (Kawasaki-308 lineage), was the first European documentation of an extensive epidemiological event involving this emerging strain, just one year after its identification in Asia.21
After the detection and confirmation of this outbreak, a broad investigation was carried out by distributing questionnaires that included personal data, collectivity membership, disease onset and duration, symptoms, medical assistance provided, previous antibiotic intake where relevant, food consumption and water sources, sanitation conditions. To identify new links between disease cases, adult contacts also filled in a questionnaire about their living and sanitation conditions and community contacts.
Although waterborne transmission was not excluded, the involvement of the fecal-oral mechanism in the amplification of the outbreak was obvious in both school and family collectivities. For that reason, the population was informed about the need to intensify hygiene measures, education facilities were disinfected repeatedly, and patients with alarming disease manifestations were isolated at home or in the hospital. School absenteeism, which led to an exclusion of the sick persons from the collectivity, along with rigorous hand hygiene measures and surface decontamination, contributed to breaking the disease transmission from students to members of their families.
Maintaining personal and collective hygiene as well as isolating sick people has proved to be effective both in children’s collectivities and in the family environment.31 A recent study by Marsh ZA et al shows that the secondary attack rate was significantly higher among those living in a household with two or more primary cases (adjusted Incidence Rate Ratio =2.0; Confidence interval 1.17–3.47) and at least one primary case with diarrhea (adjusted Incidence Rate Ratio =2.8; Confidence interval 1.35–5.93).32 Another study on the transmission of noroviruses in school collectivities shows that in addition to water and food transmission, a large number of cases may also involve vomiting (adjusted Odd Ratio 4.7 in 24.8% of cases).33 All these require intensification of decontamination and personal hygiene measures, with emphasis on hand hygiene, in accordance with the Basic Concepts of Infection Control methodology.34 The importance of school collectivities in increasing the epidemiological manifestation of the noroviruses was also discussed by Roni Kraut et al, who investigated the potential role of the start of a new school year in the seasonality of infections with this etiology.35
The study proved that, even though the disease OR was double in families with students, intensive interventions in schools were beneficial. Adopting good hygiene practices in children’s collectivities and in their households made it possible to obtain intermittent transmission, and then interrupt the outbreak, after informing and alerting the entire population. The difficulties encountered came from the fact that only 76% of the restrooms in the affected school units benefited from running water, a situation commonly found in Romanian rural areas, which constituted a significant favorable factor to this epidemic.
Disease and pathogen surveillance was intensified and the population was subsequently monitored for 10 days after closing the focus. The effectiveness of control measures consisted in the fact that no new cases occurred after the focus was closed. The SIR deterministic compartmental models have made it possible to highlight the role of school collectivities in increasing the transmission of the emerging strain in the population, as well as the effectiveness of control measures. The use of R0 and mathematical models in determining the effectiveness of hygiene measures was also mentioned by Gaythorpe et al in a recent review of the modeling and dynamics of norovirus transmission.25
The occurrence of HCAIs in hospital staff that assisted the patients was not followed by disease cases in other patients. Throughout the investigation, up-to-date information was communicated to public health authorities, as well as the local and central administration.
The study limitations
The study describes the situation in an epidemic that affected a limited area in western Romania and where the index source was not identified, although the epidemiological investigation led to hypotheses confirmed by the effectiveness of the implemented control measures. Initially, the Kaplan criteria were not applied, due to the absence of information on the etiology of gastroenteritis. The most significant limitation of the study is the small number of samples subjected to molecular analysis, for the strict confirmation of the etiology and genotype.
Conclusion
The SIR model made it possible to highlight the spread of the infection with the emerging norovirus strain from school collectivities in the territory. Public health interventions in kindergarten and school collectivities were effective by neutralizing the network nodes represented by these collectivities in the inter-human disease transmission mechanism. Consequently, the transmission chain was successfully broken. This study offers practical solutions to limit disease cases, even in the absence of etiology, and shows the importance of sometimes underestimated traditional control measures, such as decontamination and isolation. It can serve to review public health practices in order to prevent and control other epidemic outbreaks.
Ethics approval and informed consent
As the study relies on data from the national communicable disease surveillance system, it was not necessary to request patients’ informed consent. However, written informed consent was requested and obtained from outpatients from whom biological samples were taken, as well as from parents/legal guardians where the patients were minors. The study was approved by the Ethics Committee of the Arad Public Health Department (reference numb 01/11.01.2017). Our study did not involve the use of any animals.
Acknowledgments
We gratefully acknowledge the generous contribution and assistance of Mr. Cristian Chis in preparing the manuscript. Our study did not benefit from any other funds other than those allocated for public system of surveillance and control of communicable diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. Updated norovirus outbreak management and disease prevention guidelines. MMWR Recomm Rep. 2011;60(RR03):1–15. Available from:: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6003a1.htm. Accessed July 11, 2019.
2. Bruggink LD, Moselen JM, Marshall JA. The molecular epidemiology of norovirus outbreaks in Victoria, 2014 to 2015. Commun Dis Intell Q Rep. 2017;41(1):E21–E32.
3. Ahmed SM, Hall AJ, Robinson AE, et al. Global prevalence of norovirus in cases of gastroenteritis: a systematic review and meta-analysis. Lancet Infect Dis. 2014;14(8):725–730. doi:10.1016/S1473-3099(14)70767-4
4. Kazama S, Miura T, Masago Y, et al. Environmental surveillance of norovirus genogroups I and II for sensitive detection of epidemic variants. Appl Environ Microbiol. 2017;83(9):e03406–e03416. doi:10.1128/AEM.03406-16
5. Siebenga JJ, Vennema H, Zheng DP, et al. Norovirus illness is a global problem: emergence and spread of norovirus GII.4 variants, 2001–2007. J Infect Dis. 2009;200(5):802–812. doi:10.1086/605127
6. LeBlanc JJ, Pettipas J, Gaston D, et al. Outbreak of norovirus GII.P17-GII.17 in the Canadian Province of Nova Scotia. Canad J Infect Dis Med Microb. 2016. doi:10.1155/2016/1280247
7. Medici MC, Tummolo F, Calderaro A, et al. Identification of the novel Kawasaki 2014 GII.17 human norovirus strain in Italy, 2015. Euro Surveill. 2015;20(35):30010. doi:10.2807/1560-7917.ES.2015.20.35.30010
8. Ushijima H, Thongprachum A, Okitsu S, Khamrin P. Immunochromatographic tests for rapid diagnosis of noroviruses. In: Chan PKS, Kwan HS, Chan MCW, editors. The Norovirus: Features, Detection, and Prevention of Foodborne Disease. Academic Press. London: Elsevier; 2017:155–161.
9. Lu J, Fang L, Zheng H, et al. The evolution and transmission of epidemic GII.17 noroviruses. JID. 2016;214:556–564. doi:10.1093/infdis/jiw389
10. Koo ES, Kim MS, Choi YS, Park KS, Jeong YS. Occurrence of novel GII.17 and GII.21 norovirus variants in the coastal environment of South Korea in 2015. PLoS One. 2017;12(2):e0172237. doi:10.1371/journal.pone.0172237
11. Verhoef L, Boxman IL, Duizer E, et al. Multiple exposures during a norovirus outbreak on a river-cruise sailing through Europe, 2006. Euro Surveill. 2008;13(24):18899.
12. de Graaf M, van Beek J, Vennema H, et al. Emergence of a novel GII.17 norovirus – end of the GII.4 era? Euro Surveill. 2015;20(26):21178. doi:10.2807/1560-7917.ES2015.20.26.21178
13. Lu J, Sun L, Fang L, et al. Gastroenteritis outbreaks caused by norovirus GII.17, Guangdong Province, China, 2014±2015. Emerg Infect Dis. 2015;21(7):1240–1242. doi:10.3201/eid2107.150226
14. Matsushima Y, Ishikawa M, Shimizu T, et al. Genetic analyses of GII.17 norovirus strains in diarrheal disease outbreaks from December 2014 to March 2015 in Japan reveal a novel polymerase sequence and amino acid substitutions in the capsid region. Euro Surveill. 2015;20(26):21173. doi:10.2807/1560-7917.ES2015.20.26.21173
15. Pan L, Xue C, Fu H, et al. The novel norovirus genotype GII.17 is the predominant strain in diarrheal patients in Shanghai. China Gut Pathog. 2016;8:49. doi:10.1186/s13099-016-0131-3
16. Lee CC, Feng Y, Chen SY, Tsai CN, Lai MW, Chiu CH. Emerging Norovirus GII.17 in Taiwan. Clin Infect Dis. 2015;61(11):1762–1764.
17. Cannon JL, Barclay L, Collins NR, et al. Genetic and epidemiologic trends of norovirus outbreaks in the United States from 2013 to 2016 demonstrated emergence of novel GII.4 recombinant viruses. J Clin Microbiol. 2017;55:2208–22021. doi:10.1128/JCM.00962-17
18. Andrade JSR, Fumian TM, Leite JPG, et al. Detection and molecular characterization of emergent GII.P17/GII.17 Norovirus in Brazil, 2015. Infect Genet Evol. 2017;51:28–32. doi:10.1016/j.meegid.2017.03.011
19. Chan M, Hu Y, Chen H, et al. Global Spread of Norovirus GII.17 Kawasaki 308, 2014–2016. Emerg Infect Dis. 2017;23(8):1354–1359. doi:10.3201/eid2308.161138
20. Niendorf S, Jacobsen S, Faber M, et al. Steep rise in norovirus cases and emergence of a new recombinant strain GII.P16-GII.2, Germany, winter 2016. Euro Surveill. 2017;22(4):30447. doi:10.2807/1560-7917.ES.2017.22.4.30447
21. Dinu S, Nagy M, Negru D, Popovici E, Zota L, Oprișan G. Molecular identification of emergent GII.P17-GII.17 norovirus genotype, Romania, 2015. Euro Surveill. 2016;21(7):30141. doi:10.2807/1560-7917.ES.2016.21.7.30141
22. National Institute of Public Health. ADD and cholera surveillance methodology; 2015. (in Romanian). Available from: https://www.cnscbt.ro/index.php/metodologii/bda/226-metodologia-supraveghere-bda-si-holera-2015.
23. Rodrigues HS. Application of SIR epidemiological model: new trends. Int J Appl Math Inf. 2016;10:92–97.
24. Jones JH Notes on R0; Available from: http://web.stanford.edu/~jhj1/teachingdocs/Jones-on-R0.pdf.
25. Gaythorpe KAM, Trotter C, Lopman B, Steele M, Conlan AJK. Norovirus transmission dynamics: a modelling review. Epidemiol Infect. 2018;146:147–158. doi:10.1017/S095026881800122X
26. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
27. Kojima S, Kageyama T, Fukushi S, et al. Genogroup-specific PCR primers for detection of Norwalk-like viruses. J Virol Methods. 2002;100(1–2):107–114.
28. Kroneman A, Vennema H, Deforche K, et al. An automated genotyping tool for enteroviruses and noroviruses. J Clin Virol. 2011;51(2):121–125. doi:10.1016/j.jcv.2011.03.006
29. Tamura K, Stecher G, Peterson D, Filipski A, Kumar S. MEGA6: molecular evolutionary genetics analysis version 6.0. Mol Biol Evol. 2013;30(12):2725–2729. doi:10.1093/molbev/mst197
30. BioMedware. ClusterSeer; Available from: https://www.biomedware.com/?module=Page&sID=clusterseer.
31. Sandora TJ, Shih MC, Goldmann DA. Reducing absenteeism from gastrointestinal and respiratory illness in elementary school students: a randomized, controlled trial of an infection-control intervention. Pediatrics. 2008;121(6):e1555–e1562. doi:10.1542/peds.2007-2597
32. Marsh ZA, Grytdal SP, Beggs JC, Leshem E. The unwelcome houseguest: secondary household transmission of norovirus. Epidemiol Infect. 2018;146(2):159–167. doi:10.1017/S0950268817002783
33. Godoy P, Alseda M, Bartolome R, Claveria D. Norovirus gastroenteritis outbreak transmitted by food and vomit in a high school. Epidemiol Infect. 2016;144(9):1951–1958. doi:10.1017/S0950268815003283
34. International Federation of Infection Control. Basic Concepts.
35. Kraut RY, Snedeker KG, Babenko O, Honish L. Influence of school year on seasonality of norovirus outbreaks in developed countries. Can J Infect Dis Med Microbiol. 2017;9258140. doi:10.1155/2017/9258140
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.