Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Application of the Plan-Do-Check-Act Cycle in Reducing the Incidence of Dysphagia in Oral Cancer Patients After Radical Surgery
Authors Hu ZY, Xie LN, Liang GM, Qiu LY, Gao H, Hou JW ![]()
Received 12 November 2025
Accepted for publication 27 February 2026
Published 4 March 2026 Volume 2026:19 581089
DOI https://doi.org/10.2147/JMDH.S581089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Tilakavati Karupaiah
Ze-Ying Hu, Ling-Nv Xie, Guan-Mian Liang, Lan-Ying Qiu, Hang Gao, Jian-Wen Hou
Department of Head and Neck Surgery, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, 310022, People’s Republic of China
Correspondence: Jian-Wen Hou, Department of Head and Neck Surgery, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, 310022, People’s Republic of China, Tel +86 13567147265, Fax +86 0571-88128221, Email [email protected]
Objective: The incidence of postoperative dysphagia in oral cancer patients is high, significantly impacting their quality of life. This study aimed to investigate the efficacy of a PDCA cycle in reducing the incidence of postoperative dysphagia in oral cancer patients.
Methods: A non-synchronous pre-post control design was employed. From January to June 2024, 120 patients undergoing radical surgery for oral cancer were assigned to the control group, receiving routine care. While 120 patients admitted between July and December 2024 formed the observation group, receiving multidisciplinary swallowing rehabilitation management based on the Plan-Do-Check-Act (PDCA) cycle. Primary outcomes comprised the incidence of moderate-to-severe dysphagia at 1, 2, and 4 weeks post-surgery. Secondary outcomes included length of hospital stay, hospital costs, and nasogastric tube retention duration.
Results: There were no statistically significant differences between the two groups in terms of demographic and clinical characteristics. The proportions of patients with moderate to severe dysphagia 12.5% and 10%, preoperatively (P > 0.05). The observation group exhibited significantly lower rates of moderate-to-severe dysphagia at 2 weeks (50% vs.72.5%) and 4 weeks (27.5% vs 60%) postoperatively compared to the control group (p < 0.05). The observation group exhibited significantly reduced hospital stays (15.73 ± 6.217 vs 20.63 ± 2.713), lower hospital costs (4.30± 1.930 vs 5.16 ± 1.889), and shorter nasogastric tube retention times (13.07 ± 1.465 vs 15.08 ± 1.612) (p < 0.05).
Conclusion: The PDCA cycle management model, through systematic and standardized multidisciplinary collaboration, effectively reduces the incidence of moderate-to-severe dysphagia in oral cancer patients postoperatively. It promotes recovery of swallowing function, shortens hospital stays, and reduces medical costs, thereby serving as an effective method for improving the quality of dysphagia management following oral cancer surgery.
Keywords: oral cancer, dysphagia, PDCA, quality improvement, postoperative rehabilitation
Introduction
Oral cancer is the most common malignant tumor in the head and neck region, and includes cancers of the lip, tongue, gum, and floor of mouth, with over 90% of cases being classified as squamous cell carcinoma.1 According to global cancer statistics from 2020, approximately 378,000 new cases are diagnosed annually, ranking sixth globally in terms of incidence.2 The disease burden in China continues to rise. Currently, a comprehensive treatment model centered on surgical resection combined with radiotherapy and chemotherapy has increased the five-year overall survival rate to around 60%.3 Against this backdrop, the focus of treatment has expanded beyond merely improving survival rates to encompass long-term patient quality of life. One of the major long-term concerns is treatment-induced functional sequelae.
Dysphagia, which is highly prevalent and has severe clinical consequences, has emerged as a core issue affecting rehabilitation quality.4 Swallowing is a highly intricate neuromuscular coordination process that relies on the integrity of the anatomical structures of the mouth and throat and the integration of sensory and motor functions.5 While radical oral cancer surgery achieves complete tumor resection, it often inevitably damages critical structures and nerves, such as the tongue, mandible and soft palate, thereby impairing the physiological mechanisms of swallowing.6 Clinical studies report an extremely high incidence of postoperative dysphagia, ranging from 66% to 88%, with some studies indicating an initial incidence as high as 98% in the postoperative period.7–9 Data from October to December 2023 at our hospital indicate that the incidence of moderate to severe dysphagia within one week postoperatively reached 85.3%, with this proportion remaining at 63.3% at one month postoperatively. This complication directly causes physiological hazards such as aspiration, aspiration pneumonia, malnutrition and dehydration, and also exacerbates psychological distress such as anxiety and depression,2,10 creating a vicious cycle. Ultimately, these factors lead to adverse clinical outcomes, including prolonged hospital stays, increased medical costs and poor functional recovery.11
The occurrence and severity of postoperative dysphagia following oral cancer surgery result from the combined effects of multiple factors. Risk factors can be categorized into three groups: patient-related factors (such as advanced age, comorbidities, and smoking history), disease-related factors (such as tumor T-stage, primary site, and depth of invasion), and treatment-related factors (such as extent of surgical resection, neck lymph node dissection, tissue reconstruction method, and postoperative radiotherapy).7,12,13 Research confirms that the early initiation of swallowing rehabilitation training effectively reduces the incidence and severity of dysphagia.14 However, the current clinical management of swallowing disorders is fragmented and lacks standardized, multidisciplinary, collaborative processes covering preoperative assessment, intraoperative decision-making, postoperative rehabilitation, and long-term follow-up. This management model, characterized by poor multidisciplinary coordination, reactive interventions and discontinuity, significantly contributes to suboptimal outcomes in terms of swallowing function in patients.15
To address this challenge, clinical practice urgently requires a scientific, systematic theoretical framework that facilitates continuous quality improvement. The PDCA procedure offers an ideal, validated solution.16,17 The PDCA (Plan-Do-Check-Act) cycle management model, proposed by American management expert Dr. Deming, is a scientific procedure followed in comprehensive quality management. The four stages—Plan, Do, Check, and Act—are not a one-time process but a recurring cycle, where each cycle addresses and resolves specific issues, while unresolved problems enter the next cycle.18 Jin et al19 demonstrated that the PDCA cycle effectively enhanced the self-care capabilities of colorectal cancer stoma patients, improving their physical and mental health and reducing complication rates. Ultimately, this elevated their quality of life. Similarly, Zhou T et al20 research indicated that this model significantly alleviates postoperative pain and swelling in patients undergoing radial artery intervention, thereby enhancing patient comfort and specialized nursing standards. However, research into the application of the PDCA cycle in managing postoperative dysphagia rehabilitation for oral cancer patients is currently limited. Therefore, this study aims to systematically evaluate the efficacy of the PDCA cycle in reducing the incidence of moderate-to-severe postoperative dysphagia among oral cancer patients in our hospital, to explore its potential in this specific domain. The study seeks to provide novel management pathways and evidence-based support for clinical practice.
Methods
Study Design
This study employed a non-concurrent pre-post comparative design within a quasi-experimental framework.
Participants
Inclusion criteria: (1) confirmed diagnosis of oral cancer via postoperative pathological examination; (2) undergoing initial radical surgery for oral cancer; (3) aged 18 years or over; (4) conscious and capable of effective communication with researchers, and having voluntarily signed an informed consent form, and (5) family members or carers possess normal cognitive and comprehension abilities, are literate in Chinese, and can utilize the WeChat application for communication. Exclusion criteria: (1) The presence of psychiatric disorders or cognitive impairment that would prevent cooperation with the assessment and intervention; (2) irreversible dysphagia due to factors such as the transection of the recurrent laryngeal nerve during surgery; and (3) patients currently participating in other similar research studies.
Research Methods
Given the specific characteristics of the disease and ethical principles, subjects were selected using convenience sampling. The control group comprised 120 patients admitted between January and June 2024 who underwent radical surgery for oral cancer and received conventional nursing care. The observation group comprised 120 patients admitted between July and December 2024 who underwent radical surgery for oral cancer and received conventional nursing care supplemented by a multidisciplinary management model based on the PDCA cycle. Both groups underwent Food Intake Level Scale (FILS) assessments at preoperatively and at 1, 2, and 4 weeks postoperatively. Data collection interviews averaged 20 minutes in duration. All data were collected by two uniformly trained nurses during scheduled follow-up visits to ensure consistency and accuracy.
Due to significant differences in intervention methods, blinding of patients and researchers administering interventions was not feasible. To ensure impartiality in data analysis, an independent researcher coded the data using SPSS software, labeling the observation group as “A” and the control group as “B.” This maintained blinding of the data analyst regarding group assignments. After completing the study report, the researcher revealed the coding meanings: letter “A” corresponded to the observation group, and “B” corresponded to the control group.
Observation Group
Planning
(I) A retrospective analysis of clinical data from oral cancer patients at our hospital, conducted between October and December 2023, revealed that the incidence of moderate to severe dysphagia within one week post-surgery was 85.3%, with this figure remaining high at 63.3% one month post-surgery. This critical situation clearly indicates substantial room for improvement in the management of dysphagia following oral cancer surgery and establishes it as the core issue for this quality improvement project.
(II) A nine-member, multidisciplinary Continuous Quality Improvement (CQI) team was formed to address this issue. The team comprised one Head Nurse (Project Lead), one Oral and Maxillofacial Surgeon, one swallowing Rehabilitation Therapist (holding a master’s degree, with 8 years of experience), one Nutritionist and five Specialist Nurses. Roles were clearly defined: The surgeons and rehabilitation therapists were responsible for patient assessment, diagnosis and developing personalized rehabilitation programs and treatment plans, while the specialist nurses were responsible for implementing these plans, collecting data, conducting patient follow-ups, and delivering health education. The head nurse oversaw overall coordination, process supervision and resource support.
(III) Through a systematic review of existing workflows combined with brainstorming, the CQI team identified the following key issues in the current management process. Causes of formation are plotted as fishbone diagrams (Figure 1). The argumentation by Platonic analysis identified main causes, namely: lack of targeted rehabilitation measures, absence of systematic assessment and health education, inadequate professional skills, and poor training adherence (Figure 2).
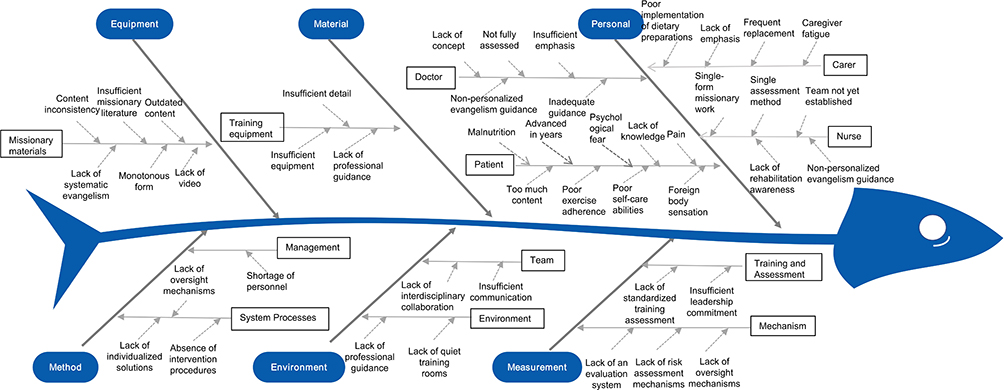 |
Figure 1 Reasons for the high incidence of dysphagia among oral cancer patients in the fishbone diagram. |
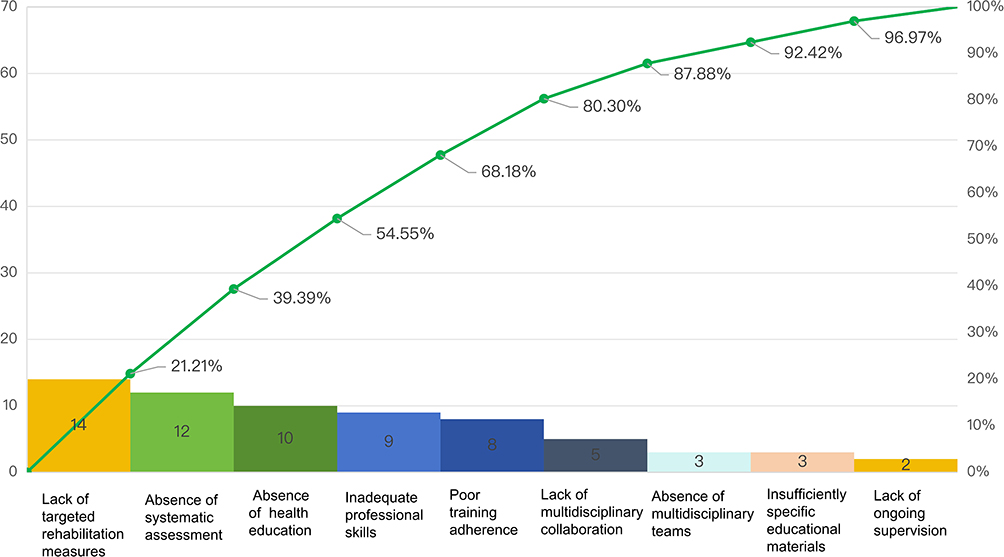 |
Figure 2 Pareto analysis of the primary factors contributing to dysphagia in oral cancer patients following surgery. |
Do
(I) All healthcare professionals in the CQI team undergo 10 hours of systematic training in swallowing rehabilitation theory and practice. This includes theoretical foundations, specific implementation methods for each stage, standardized communication techniques, and key points for swallowing function assessment and training. This ensures the team operates professionally and maintains consistent standards. Following the training, participants undergo both theoretical and skills assessments. The theoretical exam is scored out of 100 points, with a passing score of 90. The skills assessment is also scored out of 100 points, with a passing score of 95. Those who fail any assessment must retake the training until they pass.
(II) Through discussions with the CQI team, two systematic swallowing rehabilitation protocols were developed: one for patients undergoing oral cancer flap reconstruction and another for patients undergoing oral cancer non-flap reconstruction (Figures 3 and 4).
 |
Figure 3 Postoperative swallowing assessment and care protocol for oral cancer flap reconstruction patients. |
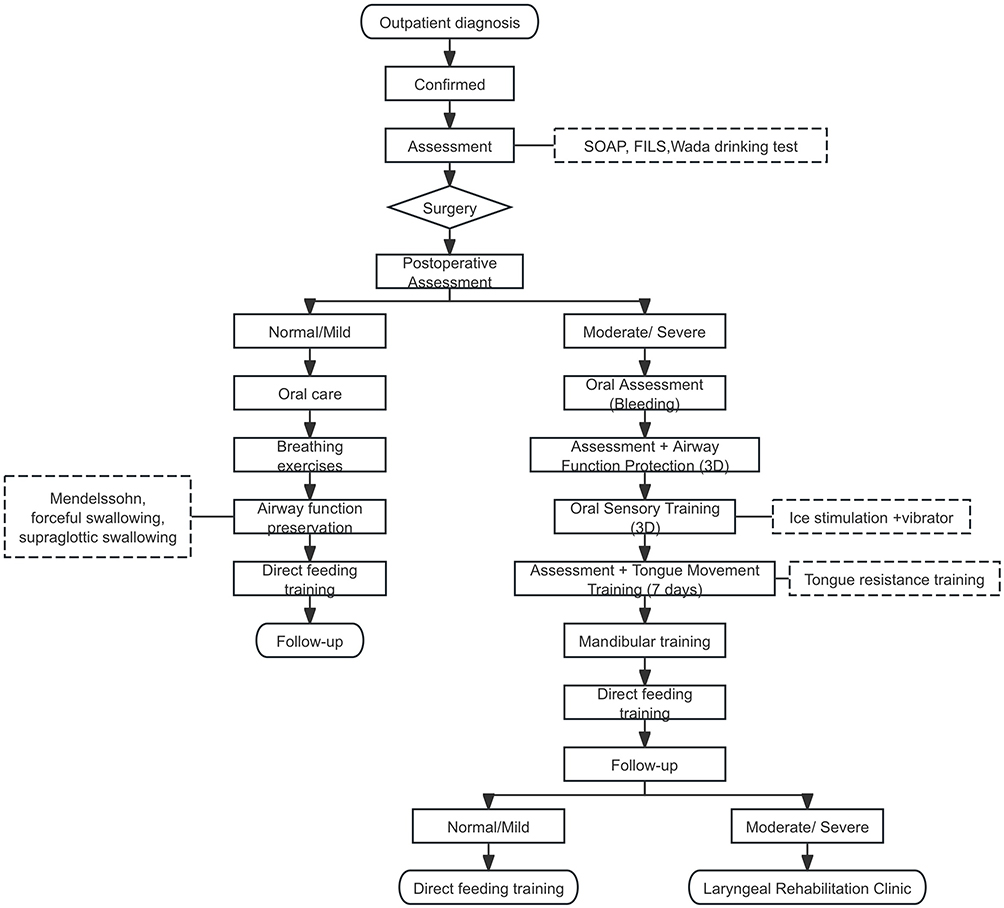 |
Figure 4 Postoperative swallowing assessment and care protocol for oral cancer patients without flap reconstruction. |
(III) Standardized content and enhanced patient education: Preoperatively disseminate disease knowledge and treatment plans; guide selection of mouthwashes and oral hygiene strategies; present successful surgical cases and share experiences; distribute health manuals and instructions for using the WeChat mini program. Inform patients about postoperative complication management, pain control, and airway management. Explain the importance of early, regular swallowing rehabilitation. Emphasize the necessity of consistent home-based exercises. Instruct on feeding environments, feeding positions, eating techniques, meal timing, portion control, and mouthful sizes.
(IV) Provide one-on-one guidance: For patients who underwent non-flap transplantation: Day 1: Instruct patients on effective coughing techniques and conduct an oral assessment. DAY 3: Conduct airway function protection training and oral sensory training. Day 7: Perform tongue movement exercises, jaw exercises, and direct feeding training. For patients who underwent flap transplantation: Day 1: Instruct patients on effective coughing techniques, conduct an oral and flap assessment. Day 2: Perform oral rinsing. Day 7: Conduct airway function protection training. Day 10: Conduct oral sensory training and breath-holding vocalization exercises. Day 11–14: Conduct tongue movement exercises and intermittent tube feeding training. Day 15: Perform direct feeding training. Each session lasts 5–10 minutes, performed 2–5 times daily. The smart screen displays a WeChat Mini Program QR code for easy patient access, with swallowing rehabilitation videos available through the WeChat mini program. Patient exchange sessions are held every Wednesday afternoon to facilitate group training for patients.
(V) Standardized assessment protocols: Rehabilitation therapists or specialist rehabilitation nurses conduct preoperative evaluations using Subjective Objective Assessment Plan (SOAP), FILS, and the Wada drinking test. Postoperative assessments employ FILS and Volume Viscosity Swallowing Test - Chinese Version (vvst-cv), with individual health records established for each patient to ensure continuity and timeliness of rehabilitation.
Check
The head nurse ensures comprehensive implementation of quality checks and nursing interventions for each patient. Compare the incidence of moderate-to-severe dysphagia at 1 week, 2 weeks, and 4 weeks post-surgery before and after implementing the PDCA cycle. Daily reminders are sent via the WeChat mini program at 8 PM to prompt patients to complete their rehabilitation check-ins, thereby enhancing rehabilitation compliance. By comparing data before and after the improvement, determine whether the quality improvement objectives have been achieved. If the objectives are not met, conduct an in-depth analysis of the causes to guide subsequent adjustments.
Act
(1) Convert clinically validated swallowing rehabilitation protocols and related training procedures into the institution’s standard operating procedures and implement them throughout the entire department.
(2) The CQI team convenes monthly meetings to review inspection findings, analyze root causes, and incorporate unresolved issues from the current cycle or newly identified problems into subsequent PDCA cycles as new improvement priorities. This spiral-driven continuous quality improvement approach ultimately achieves the long-term goal of optimizing patients’ swallowing function and quality of life.
Control Group
Implement standard care protocols, including oral care, psychological support, pain management, wound care dietary and rehabilitation guidance. Rehabilitation guidance includes dry swallowing exercises, supraglottic elevation training, oral motor exercises, and coughing training, conducted for 30 minutes daily.
Observation Indicators
Demographic Data Collection
At enrollment, demographic and baseline clinical characteristics were collected for all participants, including age, gender, tumor subtype, tumor staging, smoking history, alcohol consumption history, underlying medical conditions, and dysphagia grading.
Food Intake LEVEL Scale
The Food Intake LEVEL Scale (FILS) prototype was developed in Japan in 1993 by Fujishima et al for dysphagia assessment. This scale measures the severity of swallowing difficulties by evaluating patients’ ability to ingest oral food in daily life. Severe dysphagia: (levels 1–3) correspond to varying degrees of non-oral feeding. Moderate dysphagia: (levels 4–6) correspond to varying degrees of oral intake and alternative nutrition. Mild dysphagia: (levels 7–9) correspond to varying degrees of exclusive oral intake. Normal: (level 10) corresponds to normal oral intake capacity. Weighted kappa coefficients for interrater reliability ranged from 0.70 to 0.90 and those for intrarater reliability ranged from 0.83 to 0.90.21
Medical-Related Information
Hospitalization days, nasogastric tube retention time, hospitalization costs were retrieved from the medical record system. Hospitalization days and nasogastric tube retention time are expressed in “days,” while hospitalization costs are expressed in “ten thousand yuan.”
Statistical Methods
The required sample size was determined using G*Power 3.1 software. Calculations indicated that at an α level of 0.05 and an effect size (w) of 0.4, a minimum sample size of 200 cases was required to achieve 80.0% test power. Accounting for a 10% attrition rate, the study initially planned to enroll 220 participants. The final total number of participants enrolled was 240.
SPSS for Windows (version 26; IBM) was used for data analysis. Continuous variables were presented as mean ± standard deviation ( ), and between-group comparisons were conducted using t tests. Categorical variables were reported as counts and percentages (%), and between group comparisons were performed using chi-square tests. A p-value of < 0.05 was considered as indicating a statistically significant difference.
), and between-group comparisons were conducted using t tests. Categorical variables were reported as counts and percentages (%), and between group comparisons were performed using chi-square tests. A p-value of < 0.05 was considered as indicating a statistically significant difference.
Ethical Considerations
This study was reviewed and approved by the Ethics Committee at Zhejiang Cancer Hospital (approval no. 2023–1251), and all procedures were conducted in accordance with the principles of the Declaration of Helsinki. As part of a routine quality improvement initiative, written informed consent was obtained from all enrolled patients.
Results
This study included a total of 240 patients, all of whom completed all follow-up visits. There were no statistically significant differences between the two groups in terms of demographic and clinical characteristics (P > 0.05) (Table 1). Overall, 56.3% of participants had a history of smoking, 51.7% had a history of alcohol consumption, and 95.0% of participants had one or more underlying medical conditions.
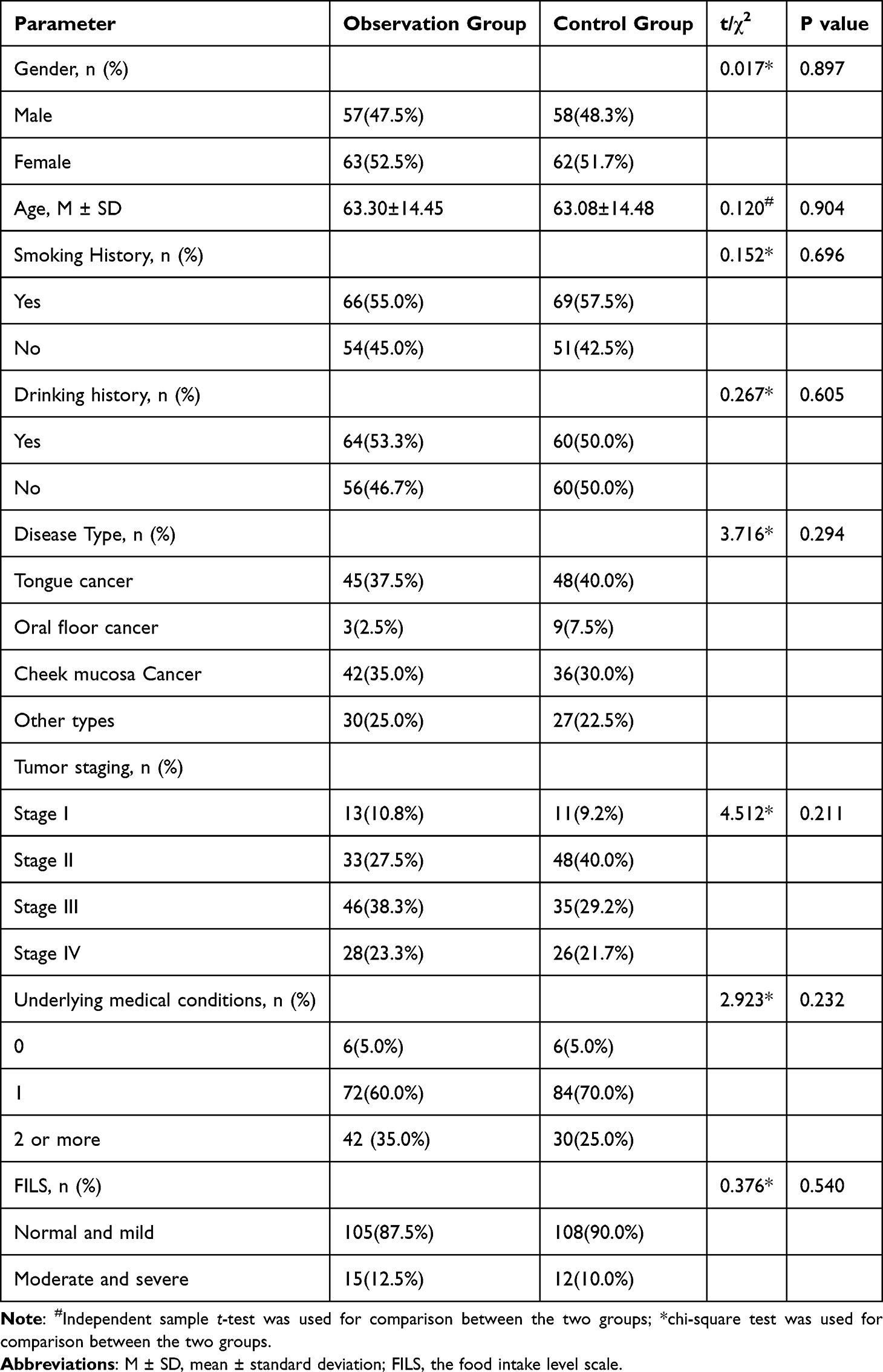 |
Table 1 Baseline Demographic and Clinical Characteristics of Study Participants (n = 240) |
The observation group’s nursing care is a structured, systematic, and dynamic cyclical process of proactive quality management; the control group’s nursing care is a static, fragmented, and execution-focused routine protocol. The proportions of patients with moderate to severe dysphagia in the observation group and control group were 12.5% and 10% preoperatively, respectively, and 80% and 85% 1 week postoperatively. There was no statistically significant difference between the two groups (P > 0.05). At 2 weeks postoperatively, the proportions of patients with moderate to severe dysphagia in the observation group and control group were 50% and 72.5%, respectively. At 4 weeks postoperatively, the proportions were 27.5% and 60%, respectively. The differences between groups were statistically significant (P < 0.05) (Table 2).
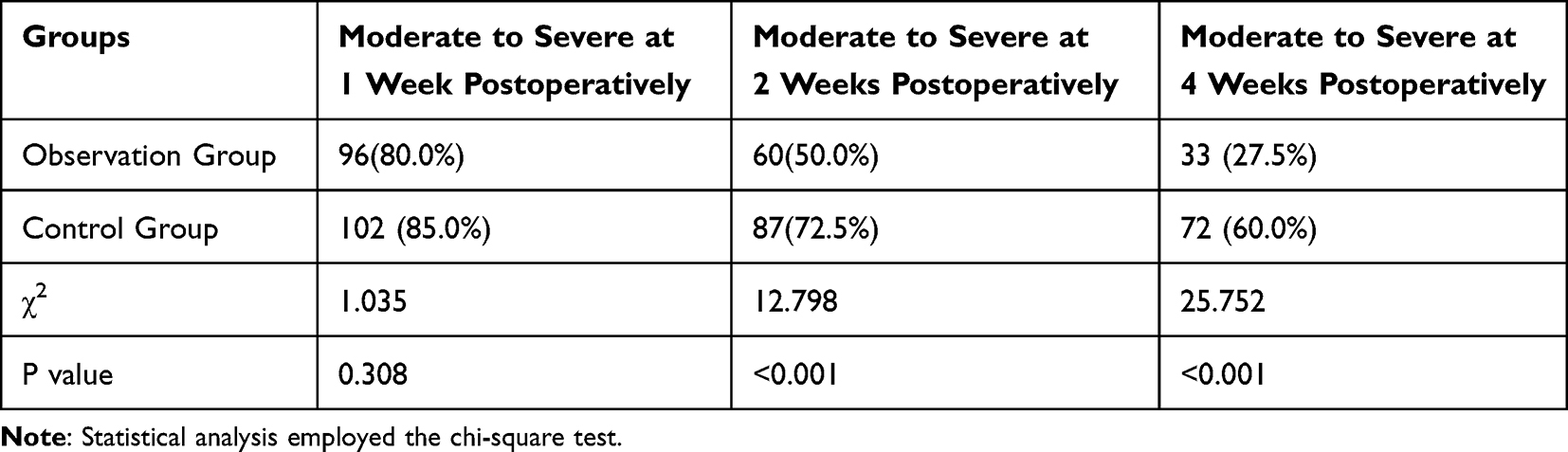 |
Table 2 Comparison of Moderate to Severe Dysphagia Among Oral Cancer Patients Before and After Implementation (n = 240) |
Additionally, the observation group demonstrated shorter hospitalization days (15.73 ± 6.217 vs 20.63 ± 2.713), nasogastric tube retention time (13.07 ± 1.465 vs 15.08 ± 1.612), and hospitalization costs (4.30 ± 1.930 vs 5.16 ± 1.889) were significantly lower than those in the control group, with all differences being statistically significant (P < 0.05) (Table 3).
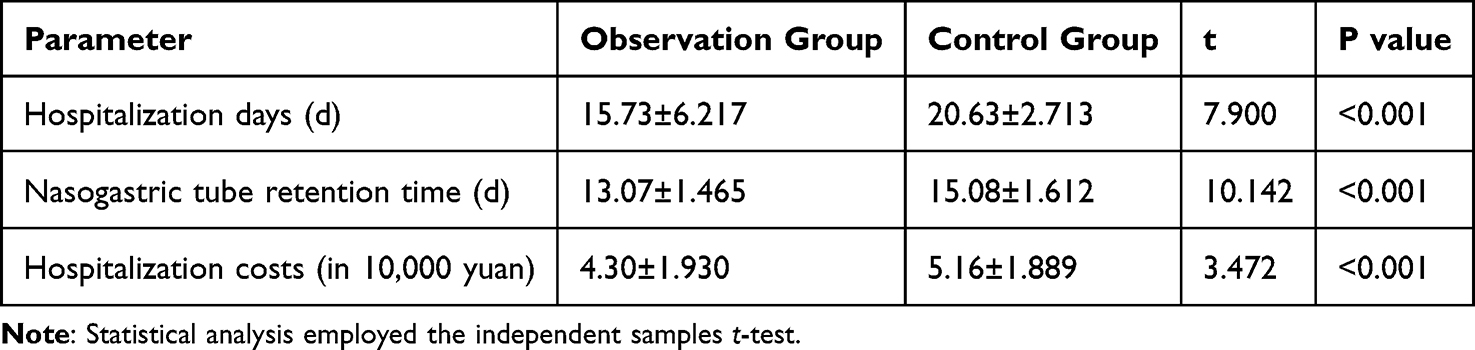 |
Table 3 Comparison of Hospitalization days, Costs, and Nasogastric Tube Retention Time Among Oral Cancer Patients Before and After Implementation (n = 240) |
Pareto analysis indicates that the lack of targeted rehabilitation measures, absence of systematic assessment, absence of health education, insufficient professional skills, and poor training adherence are the primary factors affecting swallowing rehabilitation for oral cancer patients (Figure 2).
Discussion
This study systematically investigated the application of the PDCA cycle in managing postoperative dysphagia among oral cancer patients. Results demonstrated that a standardized multidisciplinary dysphagia rehabilitation management model based on the PDCA cycle significantly reduced the incidence of moderate-to-severe dysphagia at 2 and 4 weeks postoperatively. Concurrently, it shortened hospitalization days, lowered hospitalization costs, and facilitated nasogastric tube removal. This aligns with Lu X’s research findings on applying the PDCA cycle to swallowing rehabilitation following cerebral infarction.22 These findings demonstrate that this model provides an effective structured pathway to address fragmented management of postoperative dysphagia in oral cancer patients. It establishes a comprehensive, precision-oriented rehabilitation pathway encompassing inpatient management, outpatient continuation, and multidisciplinary collaboration, offering a replicable and sustainable new management paradigm for functional recovery in this patient population.
Postoperative dysphagia, due to its high incidence and severe clinical consequences, has become a core issue affecting the long-term quality of life of oral cancer patients.23 Historical data from our center indicate that the incidence of moderate to severe dysphagia within 1 week postoperatively reaches 85.3%, closely aligning with literature reports and underscoring the widespread severity of this clinical challenge.7–9 Although the efficacy of early rehabilitation interventions has been established, traditional management models—lacking systematic protocols and multidisciplinary collaboration—often result in passive, disjointed interventions with suboptimal outcomes.14 No significant difference in swallowing function was observed between the observation and control groups at 1 week post-surgery. This was primarily attributed to the universal, transient impact of acute surgical trauma, tissue edema, and pain on swallowing physiology.24 However, the significant differences observed at subsequent time points (2 and 4 weeks post-surgery) powerfully demonstrate that the value of the PDCA cycle lies not in preventing acute-phase damage, but in proactively and specifically promoting functional recovery through an optimized management system, thereby shortening the duration of severe functional impairment. This proactive management approach represents a significant advancement over traditional reactive models.
The effectiveness of this study is primarily attributed to the multidimensional strategies implemented during both the “planning” and “do” phases. First, establishing a multidisciplinary team was crucial, ensuring that the developed protocols were scientifically grounded and professionally executed. Previous research has confirmed that multidisciplinary collaboration is essential for managing complex conditions such as dysphagia in head and neck cancer patients.25 Second, developing two distinct systematic rehabilitation pathways—one for patients undergoing flap grafting and another for those without—significantly accelerated swallowing function recovery. Third, a standardized 10-hour training program for healthcare providers ensured all team members acquired essential theoretical knowledge and practical skills, effectively addressing the root issue of “inadequate professional expertise.” This enhanced assessment accuracy and intervention effectiveness.
Crucially, this study established a structured health education and follow-up monitoring system via the WeChat platform, overcoming the temporal and spatial constraints of traditional hospital-based management. This approach directly addresses the long-standing challenges of absence of health education and poor training adherence during the home rehabilitation phase.26 Weekly patient exchange meetings foster a supportive community atmosphere, significantly enhancing patient engagement and adherence. The results of the “check” phase confirmed that the incidence of moderate to severe dysphagia significantly decreased following project implementation. This success reveals a critical insight: for multidimensional clinical issues like postoperative dysphagia—involving physiological, behavioral, and systemic factors—a model focused on system optimization and process reengineering often yields more profound and lasting impacts than introducing isolated new technologies or medications. These findings resonate with the positive outcomes achieved by Jin et al19 and Zhou Tao et al20 when applying the PDCA cycle in other disease domains, extending the model’s efficacy to the complex field of head and neck cancer rehabilitation. Finally, the “act” phase ensured the sustainability of the improvements. By formally incorporating validated protocols into institutional standard operating procedures, we have integrated new practices into routine care. More importantly, consciously incorporating unresolved or newly identified challenges into subsequent PDCA cycles embodies the core principle of continuous quality improvement, laying the foundation for ongoing optimization of patients’ swallowing function and quality of life.
Limitations
First, this study is a single-center investigation with a limited sample size and employs a non-synchronous pre-post design. Although baseline characteristics are comparable, temporal bias that cannot be fully controlled may still exist. Second, the assessment of intervention efficacy primarily relied on the FILS scale. While this scale demonstrates good clinical applicability, it lacks support from objective imaging assessments such as VFSS or FEES as gold standards. Future studies may seek collaboration with centers equipped with relevant devices to incorporate more objective physiological indicators.
Conclusion
In summary, the findings of this study indicate that the postoperative swallowing rehabilitation management model for oral cancer patients, developed based on the PDCA cycle, effectively reduces the incidence of moderate-to-severe dysphagia, and accelerates the recovery of swallowing function. Through systematic problem analysis, multidisciplinary team collaboration, and continuous quality improvement cycles, this model successfully translates evidence-based practice into a standardized clinical pathway that is implementable and monitorable. Therefore, the PDCA cycle represents a highly promising and effective strategy for enhancing the quality of post-operative dysphagia management in oral cancer patients and improving patient outcomes. It warrants broader implementation in clinical practice and further in-depth research.
Abbreviations
PDCA, Plan, do, check, act; CQI, Continuous Quality Improvement; FILS, Food Intake LEVEL Scale; VVST, Volume-Viscosity Swallowing Test; VFSS, video fluoroscopic swallowing studies; sEMG, surface electromyography.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Zhejiang Cancer Hospital (Approval no. 2023-1251). Written informed consent was obtained from all participants.
Acknowledgments
We thank all patients who participated in the study and clinical staff for their help in conducting this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Health Commission of Zhejiang Province (2025KY718) and the Zhejiang Cancer Hospital Nursing Scientific Research Special Cultivation Fund (NSR2025A1).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rodríguez-Molinero J, Migueláñez-Medrán BDC, Puente-Gutiérrez C, et al. Association between oral cancer and diet: an update. Nutrients. 2021;13(4):1299. doi:10.3390/nu13041299
2. Wang RN, Gao J, Zheng XY, Dong Y. Illness uncertainty and dysphagia in Chinese oral cancer patients: the mediation effect of catastrophic cognition. Support Care Cancer. 2024;32(8):535. doi:10.1007/s00520-024-08728-4
3. Epstein JB, Miaskowski C. Oral pain in the cancer patient. J Natl Cancer Inst Monogr. 2019;2019(53):lgz003. doi:10.1093/jncimonographs/lgz003
4. Krisciunas GP, Castellano K, McCulloch TM, et al. Impact of compliance on dysphagia rehabilitation in head and neck cancer patients: results from a multi-center clinical trial. Dysphagia. 2017;32(2):327–12. doi:10.1007/s00455-016-9760-4
5. Ambrocio KR, Miles A, Bhutada AM, Choi D, Garand KL. Defining normal sequential swallowing biomechanics. Dysphagia. 2023;38(6):1497–1510. doi:10.1007/s00455-023-10576-z
6. Hasegawa Y, Sugahara K, Fukuoka T, et al. Change in tongue pressure in patients with head and neck cancer after surgical resection. Odontology. 2017;105(4):494–503. doi:10.1007/s10266-016-0291-0
7. Kao SST, Peters MDJ, Krishnan SG, Ooi EH. Swallowing outcomes following primary surgical resection and primary free flap reconstruction for oral and oropharyngeal squamous cell carcinomas: a systematic review. Laryngoscope. 2016;126(7):1572–1580. doi:10.1002/lary.25894
8. Cocks H, Ah-See K, Capel M, Taylor P. Palliative and supportive care in head and neck cancer: united Kingdom national multidisciplinary guidelines. J Laryngol Otol. 2016;130(S2):S198–S207. doi:10.1017/S0022215116000633
9. Pezdirec M, Strojan P, Boltezar IH. Swallowing disorders after treatment for head and neck cancer. Radiol Oncol. 2019;53(2):225–230. doi:10.2478/raon-2019-0028
10. A. c KS, van der Molen L, van den Brekel MWM, Hilgers FJM. Current assessment and treatment strategies of dysphagia in head and neck cancer patients: a systematic review of the 2012/13 literature. Curr Opin Support Palliat Care. 2014;8(2):152–163. doi:10.1097/SPC.0000000000000050
11. Yamaguchi K, Okumura T, Oikawa Y, et al. Effect of oral intake initiation-establishment interval on hospital stay after oral cancer surgery. Oral Dis. 2024;30(8):4948–4955. doi:10.1111/odi.14985
12. Huang ZS, Chen WL, Huang ZQ, Yang ZH. Dysphagia in tongue cancer patients before and after surgery. J Oral Maxillofac Surg. 2016;74(10):2067–2072. doi:10.1016/j.joms.2016.03.031
13. Hasegawa T, Yatagai N, Furukawa T, et al. The prospective evaluation and risk factors of dysphagia after surgery in patients with oral cancer. J Otolaryngol Head Neck Surg. 2021;50(1):4. doi:10.1186/s40463-020-00479-6
14. Hajdú SF, Wessel I, Dalton SO, Eskildsen SJ, Johansen C. Swallowing exercise during head and neck cancer treatment: results of a randomized trial. Dysphagia. 2022;37(4):749–762. doi:10.1007/s00455-021-10320-5
15. Y S, Jw P, M K, et al. Clinical practice guidelines for oropharyngeal dysphagia. Ann Rehabil Med. 2023;47(Suppl 1). doi:10.5535/arm.23069
16. Moyce S, Claudio D, Velazquez M. Using the PDCA cycle to uncover sources of mental health disparities for hispanics. Int J Ment Health Nurs. 2023;32(2):556–566. doi:10.1111/inm.13100
17. Zeng X, Huang X, Wang P, et al. The application of the PDCA cycle in the nutritional management of patients with nasopharyngeal carcinoma. Support Care Cancer. 2023;31(5):251. doi:10.1007/s00520-023-07724-4
18. Rai VK, Sharma A, Thakur A. Quality control of nanoemulsion: by PDCA cycle and 7QC tools. Curr Drug Deliv. 2021;18(9):1244–1255. doi:10.2174/1567201818666210203180516
19. Jin Y, Li C, Zhang X, Jin Y, Yi L, Cui J. Effect of FOCUS-PDCA procedure on improving self-care ability of patients undergoing colostomy for rectal câncer. Rev Esc Enferm USP. 2021;55:e03729. doi:10.1590/S1980-220X2020012503729
20. Zhou T, Liu J, Wang S, Zhang Q. Impact of FOCUS-PDCA on reducing the incidence of complications after transradial intervention. Minerva Cardiol Angiol. 2025;73(2):154–162. doi:10.23736/S2724-5683.24.06544-X
21. Kunieda K, Ohno T, Fujishima I, Hojo K, Morita T. Reliability and validity of a tool to measure the severity of dysphagia: the food intake LEVEL scale. J Pain Symptom Manage. 2013;46(2):201–206. doi:10.1016/j.jpainsymman.2012.07.020
22. Lu X, Zhang J, Wang R, Liu X. Application value of the FOCUS-PDCA cycle in nursing care for dysphagia in patients with cerebral infarction: a meta-analysis. Arq Neuropsiquiatr. 2025;83(6):1–8. doi:10.1055/s-0045-1809417
23. Mathew A, Lockwood MB, Steffen A, et al. Symptom cluster experiences of patients operated for oral cancer: a mixed methods study. Semin Oncol Nurs. 2023;39(3):151407. doi:10.1016/j.soncn.2023.151407
24. Hey C, Goeze A, Sader R, Zaretsky E. FraMaDySc: dysphagia screening for patients after surgery for head and neck cancer. Eur Arch Oto-Rhino-Laryngol. 2023;280(5):2585–2592. doi:10.1007/s00405-023-07865-6
25. Kristensen MB, Isenring E, Brown B. Nutrition and swallowing therapy strategies for patients with head and neck cancer. Nutr. 2020;69:110548. doi:10.1016/j.nut.2019.06.028
26. Robison RD, Butz N, Gustafson S, et al. Ready for discharge, but are they ready to go home? Examining neighborhood-level disadvantage as a marker of the social exposome and the swallowing care process in a retrospective cohort of inpatients with dementia. Am J Speech-Lang Pathol. 2024;33(3):1536–1547. doi:10.1044/2024_AJSLP-23-00332
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Nurse-Led Swallowing Rehabilitation on Swallowing Function, Quality of Life, and Adherence in Patients with Oral Cancer: A Single Center Randomized Controlled Trial
Hu ZY, Xie LN, Liang GM, Liu YW, Wen XX, Hou JW
Patient Preference and Adherence 2026, 20:577315
Published Date: 17 January 2026