Back to Journals » International Medical Case Reports Journal » Volume 17
Application of the Fifth-Generation Cardiac Contractility Modulation Device in a Patient with Chronic Heart Failure: A Case Report
Authors Xie C, Xiang Y, Wu Y, Zhang Y
Received 6 August 2024
Accepted for publication 29 October 2024
Published 20 November 2024 Volume 2024:17 Pages 981—984
DOI https://doi.org/10.2147/IMCRJ.S490329
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Cui Xie,1 Yang Xiang,1 You Wu,1 Youen Zhang1,2
1Institute of Clinical Medicine and Department of Cardiology, Renmin Hospital, Hubei University of Medicine, Shiyan, Hubei, 442000, People’s Republic of China; 2Arteriosclerosis Cardiovascular Disease Clinical Medical Research Center of Hubei Province, Shiyan, Hubei, 442000, People’s Republic of China
Correspondence: Youen Zhang, Email [email protected]
Abstract: We present a patient of a 46-year-old female patient was admitted to our hospital due to chest tightness and shortness of breath that lasted for over a month. Echocardiography revealed left-ventricle diameter (anteroposterior) of 54 mm, electrocardiogram showed sinus bradycardia, and QRS duration of 90 ms. The patient experienced no chest tightness or shortness of breath, and there was a marked improvement in exercise tolerance and quality of life after cardiac contractility modulation implantation.
Keywords: heart failure, cardiac contractility modulation, dilated cardiomyopathy, ventricular remodeling
Introduction
Heart failure (HF) is a severe clinical syndrome primarily caused by cardiovascular disease. It is often accompanied by multiple comorbidities, and is a major public health concern. Pharmacological therapy for HF is effective for most patients, improving their quality of life and prolonging survival. However, over 10% of patients with HF respond poorly to drug therapy and progress to refractory HF.1 In recent years, it has been demonstrated that Cardiac Contractility Modulation (CCM), a new device-based therapy for treating HF, can enhance myocardial contractility, improve cardiac function, reverse ventricular remodeling in patients with HF,2 and in patients with refractory systolic heart failure following orthotopic heart transplant.3 This report details one case of CCM implantation performed at our hospital. The study followed the ethical principles of the Declaration of Helsinki.
Case Presentation
A 46-year-old female patient was admitted to our hospital due to chest tightness and shortness of breath that lasted for over a month. Her medical history included a partial thyroidectomy, and she had no history of smoking or alcohol consumption. She was treated with regular medications (Metoprolol succinate extended-release tablets, Sacubitril valsartan sodium tablets, Spironolactone, Dapagliflozin tablets) for HF, but the response was poor. During the physical examination, the patient was conscious and well-oriented. Her heart rate was 68 beats per minute, blood pressure was 150/98 mm Hg, respiratory rate was 20 beats per minute. There were no signs of bleeding or jaundice on the skin or mucous membranes, and no jugular venous distention was observed. The thyroid gland was not enlarged. Breath sounds were coarse in both lungs, with wet rales present at the lung bases. The heart rate was 68 bpm with a regular rhythm. The abdomen was soft, with no tenderness or rebound tenderness, and the liver and spleen were not palpable below the rib cage. The hepatojugular reflux sign was negative, but there was edema in both lower limbs.
She was hospitalized and underwent relevant examinations. Biochemical tests showed thyroid stimulating hormone (TSH) of 7.190 uIU/mL, triglycerides of 0.81 mmol/L, low-density lipoprotein cholesterol ((LDL-C)) of 2.61 mmol/L, serum lipoprotein (a) of 435 mg/L, and NT-proBNP of 6245 pg/mL. An electrocardiogram (ECG) examination showed sinus bradycardia, T-U wave abnormalities, and QRS duration of 90 ms. Further transthoracic echocardiography revealed left-atrium (LA) diameter (anteroposterior) of 41 mm, left-ventricle diameter (LVD, anteroposterior) of 54 mm; interventricular septum thickness in diastole (IVSD) of 9 mm, end-diastolic left-ventricular posterior wall thickness (LVPWd) of 9 mm, left-ventricular ejection fraction (LVEF) of 28% (M-mode), fraction shortening (FS) of 13%, and pulmonary artery pressure of 29 mm Hg. No significant coronary artery lesions were observed on coronary computed tomography angiography (CTA). The patient was diagnosed with dilated cardiomyopathy, class III heart failure with reduced LVEF according to the New York Heart Association (NYHA). Combined with the parameters, it can be observed that the volumes of the left atrium and left ventricle are gradually shrinking, indicating that the diastolic function of the left ventricle is improving. CCM treatment is reversing myocardial remodeling. In addition, E/e′ reflects the left ventricular filling pressure. The normal value should be less than 8. It can be observed that in this case, E/e′ returns to the normal value three months after CCM implantation. These two points both reflect the role of CCM in improving myocardial diastolic function in the treatment of heart failure. In summary, the patient had the following characteristics: (1) LVEF improved but remained as low as 30% after optimal drug therapy for heart failure; (2) Chest tightness and discomfort with slight activity, cardiac function grade III; (3) ECG shows narrow QRS. Considering the positive preoperative of levosimendan test, after general discussion and full communication with the patient and his family, it was decided to perform CCM implantation treatment.
The CCM implantation procedure was similar to that of traditional pacemaker implantation. The patient was placed in a supine position, disinfected with a towel, and the left subclavian vein was punctured twice under local anesthesia, and the capsular bag was made after the guidewire was inserted. Under the guidance of the guidewire, two tear-off sheaths were fed, and two ventricular pacing leads (Medtronic 3830–69) were fed through the sheath, and the position of the wires was adjusted to the right ventricular septum surface with a distance of 3 cm. During the operation, the near-field electrode (RV) was tested, showing a pacing capture threshold of 0.5 V, a sensed R-wave amplitude greater than 10 mV, and a lead impedance of 1080 Ω; the far-field electrode (LS) showed a pacing threshold of 0.5 V, a sensed R-wave amplitude greater than 15 mV, and a lead impedance of 900 Ω. These measurements met the criteria for successful electrode implantation. Both leads were securely anchored into the right-ventricular septum. After ensuring the absence of palpable diaphragmatic stimulation with a 10 V pacing pulse at 0.4 ms pulse width, the leads were connected to the Optimizer Smart pulse generator. Subsequently, the output pulses were set, and parameters were programmed and optimized (Figure 1A and B).
 |
Figure 1 CCM electrode positions (A) RAO 30°; (B) Lao 45° and ECG during CCM pulse delivery (C). Abbreviations: RAO, right anterior oblique; LAO, left anterior oblique; ECG, electrocardiogram. |
Immediate postoperative ECG monitoring indicated normal CCM pulse delivery (Figure 1C). We observed the patients’ response to CCM by adhering to a standardized follow-up protocol. Utilizing a comprehensive array of assessment tools, including cardiac color Doppler ultrasonography, NT-ProBNP blood tests, six-minute walk tests (6MW), and the Minnesota Living with Heart Failure Questionnaire (MLHFQ), we systematically evaluated the clinical statuses of the patients. (Table 1 and Figure 2). The patient experienced no chest tightness or shortness of breath, and there was a marked improvement in exercise tolerance and quality of life.
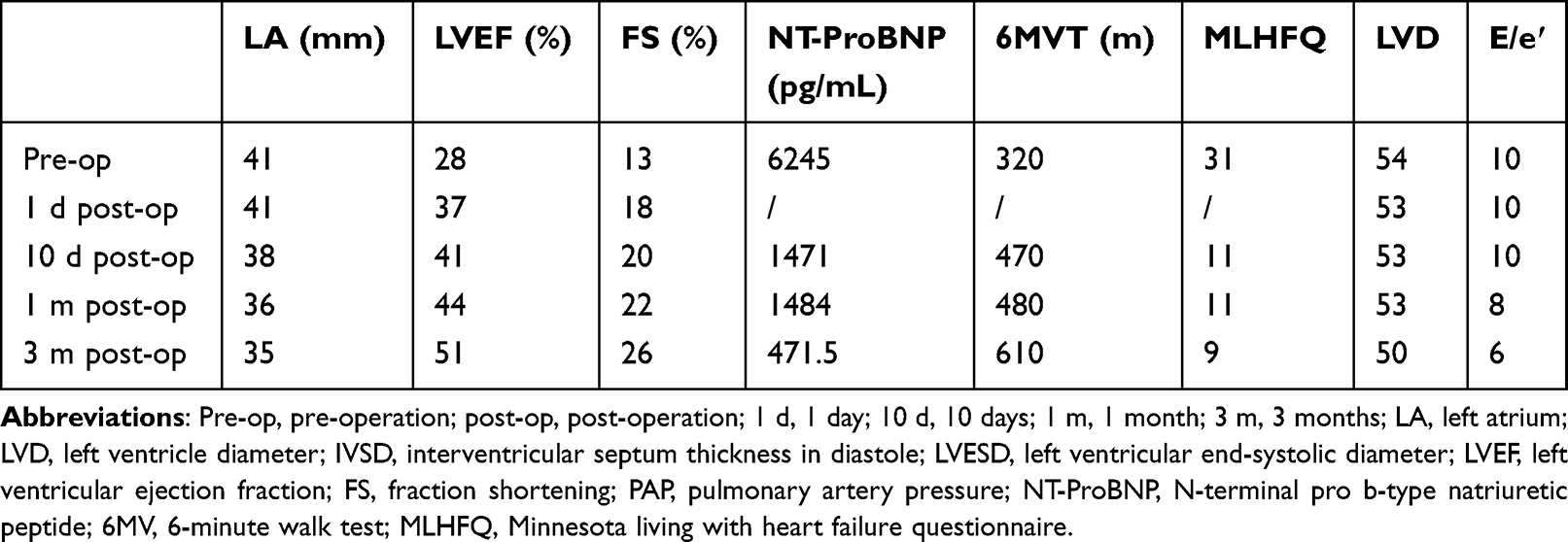 |
Table 1 Follow-Up Results After CCM Implantation |
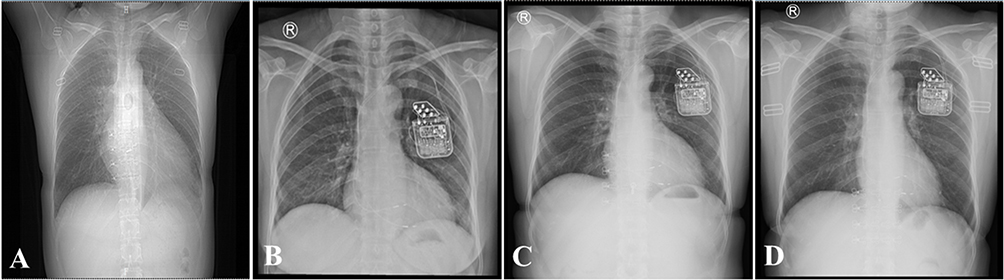 |
Figure 2 Chest fluoroscopic views of the leads at different time points: before CCM implantation (A), 10 days after CMM implantation (B), 1 month after CCM implantation (C), and 3 months after CCM implantation (D). |
Discussion
HF is a severe manifestation or late stage of various heart diseases, with high mortality and readmission rates. The prevalence of HF among adults in developed countries is 1.0%–2.0%.4 Despite significant advances in treating HF with reduced LVEF through etiological treatment, optimal medications, device implantation, ventricular assist devices, and heart transplantation, many patients with HF still experience frequent hospitalizations, significantly decreased quality of life, and poor overall prognosis.5
CCM is a device-based therapy option that delivers nonexcitatory electrical pulses to the ventricles during the absolute refractory period, enhancing myocardial contractility during systole, who do not benefit from CRT and are still symptomatic despite optimal medical therapy. The mechanism of CCM is different than that of traditional optimal medical therapy. CCM appears to normalize the phosphorylation levels of phospholamban and to enhance calcium handling through upregulation of sarco/endoplasmic reticulum calcium ATPase (SERCA2a) and restoration of the sodium/calcium exchanger.6 Multiple randomized controlled trials have demonstrated that CCM can safely improve exercise tolerance and quality of life in HF patients with LVEF of 25%–45% and a narrow QRS complex. Therefore, guidelines recommend considering CCM for chronic NYHA class III HF patients with LVEF between 25% and 45%, and QRS <130 ms (without cardiac resynchronization therapy indication), who respond poorly to optimal medications.7 Previous research has indicated that CCM delivers potent bidirectional stimuli during the myocardial absolute refractory period, transiently increasing transmembrane calcium (Ca2+) influx and enhancing myocardial contractility.8 CCM also alters gene expression, reduces myocardial fibrosis, and improves ventricular remodeling.
To date, the number of CCM implantation cases and the extent of follow-up data in China remain limited. As shown in previous clinical studies, in this case, echocardiographic assessments conducted preoperatively, immediately postoperatively, and during follow-up demonstrated significant improvements in the left atrium, left-ventricular end-diastolic diameter, and overall left-ventricular function. 6MWT has some predictive value in patients with chronic heart failure, which can be used to quantify the severity of cardiopulmonary disease. Minnesota living with heart failure questionnaire (MLHFQ) is a specific scale for evaluating the quality of life of patients with heart failure, and is often used in clinical trials and community project management to evaluate the typical symptoms and signs, physical activities, social relationships, sexual activities, work, and mood of patients with heart failure. The scale includes 3 dimensions and 21 items of symptoms, physical activity and emotion, and each item adopts a 6-level Likert score of 0–5, and the higher the score, the worse the quality of life. The patient’s symptoms had improved significantly, as shown by an increase in walked distance at the 6MWT and MLHFQ. Currently, CCM is being extensively evaluated for the treatment of HF. Ongoing clinical trials aim to assess the efficacy of CCM in patients who are nonresponders to cardiac resynchronization therapy with low LVEF (≤35%) and wide QRS complex (≥130 ms), and in those with HF with preserved LVEF (HFpEF). Should these studies confirm its effectiveness, the indications for CCM implantation could be broadened to include these patient populations, potentially offering a promising treatment strategy.
Ethics and Consent
Institutional approval is not required for publication, so informed written consent for using patient information and case report publication was obtained from the patient as long as identifying data are anonymous.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Truby LK, Rogers JG. Advanced Heart Failure: epidemiology, Diagnosis, and Therapeutic Approaches. JACC Heart Fail. 2020;8(7):523–536.
2. Abraham WT, Kuck KH, Goldsmith RL, et al. A Randomized Controlled Trial to Evaluate the Safety and Efficacy of Cardiac Contractility Modulation. JACC Heart Fail. 2018;6(10):874–883. doi:10.1016/j.jchf.2018.04.010
3. Pierucci N, Mirco La Fazia V, Gianni C, et al. Cardiac contractility modulation in a patient with refractory systolic heart failure following orthotopic heart transplant. Case Reports Heart Rhythm Case Rep. 2023;10(1):33–37.
4. Virani SS, Alonso A, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2020 Update: a Report From the American Heart Association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
5. Bozkurt B, Tariq Ahmad C, Alexander KM, et al. Heart Failure Epidemiology and Outcomes Statistics: a Report of the Heart Failure Society of America. J Card Fail. 2023;29(10):1412–1451. doi:10.1016/j.cardfail.2023.07.006
6. Marks AR. Calcium cycling proteins and heart failure: mechanisms and therapeutics. J Clin Invest. 2013;123(1):46–52. doi:10.1172/JCI62834
7. Witte K, Hasenfuss G, Kloppe A, et al. Cost-effectiveness of a cardiac contractility modulation device in heart failure with normal QRS duration. ESC Heart Fail. 2019;6(6):1178–1187. doi:10.1002/ehf2.12526
8. Winter J, Brack KE, Ng GA. Cardiac contractility modulation in the treatment of heart failure: initial results and unanswered questions. Eur J Heart Fail. 2011;13(7):700–710. doi:10.1093/eurjhf/hfr042
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Kuoxin Formula in the Treatment of Dilated Cardiomyopathy-Related Heart Failure: Study Protocol of a Randomized, Double-Blind, Placebo-Controlled, Multi-Center Clinical Trial
Wu Q, An S, Lee R, Gao D, Zhou Y, Peng L, Hu C, Yao L, Zhou C, Zhou L, Gao J, Cao M, Mao M, Li G, Deng B, Xu Y, Wang Y
International Journal of General Medicine 2024, 17:1909-1921
Published Date: 6 May 2024
Cardiac Myosin Activators in Heart Failure: Experimental Advances Amid Clinical Uncertainty
Hou L, Lin B, Ji X, Huang A
Drug Design, Development and Therapy 2026, 20:568587
Published Date: 12 January 2026
Value of Color Doppler Echocardiography for Predicting Heart Failure After Percutaneous Coronary Intervention in Patients with Acute Myocardial Infarction
Ren L, Hu Z, Huang Z, Xu L
International Journal of General Medicine 2026, 19:608632
Published Date: 11 June 2026