Back to Journals » Risk Management and Healthcare Policy » Volume 19
Application of Quality Control Circles in Remote ECG Network Management to Standardize ECG Operational Procedures
Authors Gong Z, Li Y, Liu Y, Luan S, Na X ![]()
Received 7 November 2025
Accepted for publication 14 February 2026
Published 19 February 2026 Volume 2026:19 575056
DOI https://doi.org/10.2147/RMHP.S575056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Zhihua Gong,1,* Yongxue Li,2,* Yumin Liu,1 Shaopeng Luan,3 Xiaodong Na1,4
1Department of Cardiac Function, Qingdao Central Hospital, University of Health and Rehabilitation Sciences, Qingdao, Shandong, People’s Republic of China; 2The First School of Clinical Medicine, Shandong University, Jinan, Shandong, People’s Republic of China; 3College of Computer Science and Engineering, University of New South Wales, Sydney, NSW, Australia; 4School of Rehabilitation Science and Engineering, University of Health and Rehabilitation Sciences, Qingdao, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaodong Na, School of Rehabilitation Science and Engineering, University of Health and Rehabilitation Sciences, No. 369, Qingdao National High-Tech Industrial Development Zone, Qingdao, Shandong, People’s Republic of China, Email [email protected]
Objective: To examine the effectiveness of Quality Control Circles (QCC)in remote Electrocardiography (ECG) network management, with a particular focus on evaluating their impact on improving operational standardization.
Methods: Electrocardiogram data from Qingdao Central Hospital was selected as the research subject. Among them, 402 cases collected from January to April 2024 were before the implementation of QCC activities, and 356 cases collected from January to April 2025 were after the implementation of QCC activities. The irregularity rates of the electrocardiogram data between the two groups were compared. By establishing QCC teams, issues related to non-standardized operations at the 12-lead ECG acquisition endpoints were analyzed, and targeted improvement measures were developed.
Results: Following QCC implementation, the non-compliant operation rate at 12-lead ECG collection endpoints within the network system significantly decreased, from 17.66% to 6.17% (P< 0.05), After QCC activities, members’ team spirit, QC techniques, mental development, communication and coordination, activity confidence, responsibility and honorall show positive improvement.
Conclusion: QCC activities can effectively standardize ECG network operational procedures, enhancing the level of operational standardization and reducing the risk of misdiagnosis and missed diagnoses caused by non-standardized operations, thereby demonstrating clinical application value.
Keywords: quality control circle, remote ECG network management, twelve-lead ECG, standardization development
Introduction
Electrocardiography (ECG) is a fundamental technique for clinical cardiovascular assessment, and its diagnostic value highly depends on the standardization of the operational procedure and the precision of signal acquisition. This non-invasive method captures the temporal and spatial variations of myocardial electrical activity, providing direct diagnostic evidence for common cardiac conditions such as arrhythmias and myocardial ischemia.1,2 Moreover, it plays a crucial role in perioperative risk assessment, monitoring drug efficacy, predicting cardiovascular diseases, and long-term health management.3 However, as the scenarios for ECG testing extend from traditional cardiology to multiple areas such as emergency departments, intensive care, and primary healthcare,4 there is significant heterogeneity in the professional backgrounds of the operators. A growing risk of disconnect in technical competence and quality awareness is emerging between highly concentrated ECG diagnostic specialists and an expanding pool of operators.
ECG is susceptible to interference from multiple factors in clinical applications, resulting in the formation of artifacts that substantially compromise the quality of ECG signals and diagnostic accuracy.5 Artifacts refer to abnormal waveforms caused by non-cardiac electrical activity, whose formation mechanisms are complex and primarily originate from four dimensions: technical factors include hardware issues such as device calibration deviations and poor electrode contact;6 operational factors involve human errors like inaccurate electrode placement and improper skin preparation; patient-related factors encompass individual variations such as body position changes and underlying medical conditions; environmental factors include external influences like electromagnetic interference and mechanical vibrations. These interferences not only obscure critical ECG features such as ST-segment changes and T-wave abnormalities but may also generate artifacts resembling arrhythmias, posing a significant risk of clinical misdiagnosis. Research indicates that ECG artifacts caused by non-standardized procedures are a major contributor to misdiagnosis and missed diagnosis.7 To systematically address this clinical challenge, the scientific management tool of quality circles has been integrated into ECG quality management systems. Through standardized process development and continuous quality improvement, this approach effectively enhances the standardization of ECG acquisition.
QCC is a scientific quality management methodology first proposed in 1962 by Japanese quality management expert Kaoru Ishikawa.8 Its core concept involves establishing cross-departmental, cross-level collaborative teams that systematically address quality issues in the workplace through the application of scientific tools such as Plan-Do-Check-Act (PDCA) cycles.9 In the healthcare sector, QCC is widely applied to improve the quality of services, optimize diagnosis and treatment processes, and improve patient outcomes. A study by Chen et al10 in an oral hospital in Shandong showed that combining QCC with PDCA cycles increased healthcare workers’ hand hygiene compliance from 60.1% to 97.2%, establishing a “monitor-evaluate-feedback” model for infection control. In a study by Wang at Sichuan Friendship Hospital,11 QCC activities reduced the failure rate of Surgical Instrument Preprocessing from 2.9% to 1.1%, while simultaneously enhancing team members’ professional knowledge and collaborative capabilities. The Xiamen Zhongshan Hospital study12 provided the first evidence demonstrating the effectiveness of QCC in increasing the rate of early rehabilitation intervention in stroke patients from 45.23% to 59.55%. Standardized procedures have been established to institutionalize these interventions over time. These studies not only confirm QCC’s effectiveness in addressing healthcare quality issues but also provide replicable quality management models for medical institutions, demonstrating the method’s broad application potential in enhancing healthcare quality.
In provincial hospital evaluations, QCC activities have become a strict standard for assessing hospital management performance. Reducing internal errors, cutting costs, improving satisfaction, enhancing work quality, and boosting economic performance are the main focus areas of QCC initiatives. These measures have greatly promoted the hospital’s proactive role in quality management and control.13
However, the complexity of medicine requires quality control circle members to engage in cross-professional collaboration, which leads to high demands for both personalization and standardization of the quality control circles.11 Therefore, the selection criteria for members are stringent, and members need specialized training to be competent in quality control circle work. Setting target values for the quality control circles is also a major challenge. If the target values are too low, it means the goals can be easily achieved, resulting in a low confidence level; if the target values are too high, it indicates an inaccurate assessment of the team’s capabilities, making it difficult to achieve the desired improvement. These factors have caused quality control circle activities to be primarily limited to tertiary hospitals, making them difficult to implement and popularize in medium- and small-sized hospitals.
The personalized and standardized characteristics of the quality control circle provide significant advantages for standardized electrocardiogram (ECG) practice. By bringing together cardiologists, nurses, network engineers, instrument engineers, and other professionals, it creatively combines individual working memory with tools to achieve process optimization.14 At the same time, the quality control circle can encompass the entire ECG workflow, standardize processes, and develop detailed and clear standard guidelines for reference. To enhance compliance with ECG network operational standards and deliver improved patient care, this study implemented a QCC initiative within ECG network management from January to April 2025. Through the integration of Internet data management, the ECG diagnosis is analyzed in all aspects and dimensions. There was no previous precedent for implementing QCC in the field of electrocardiography, so this is a pioneering study. Through multidimensional attribution analysis, the study identified the root causes of nonconforming practices and established a replicable and practical approach to improve the quality of ECG performance.
Materials and Methods
This study utilized a pre-post comparative design based on the hospital’s ECG network database, analyzing ECG examination data from two periods: January to April 2024 (pre-intervention) and January to April 2025 (post-intervention). A total of 758 ECG examination records were included, and statistical analysis of procedural compliance was conducted through a standardized evaluation process. We used all the data from ECG network database of our hospital during this time period as a sample, classified the samples into standardized and non-standardized categories based on the established criteria, and used the chi-square test to verify the effectiveness of QCC implementation in improving operational compliance. The study approved by the Ethical Committee of Qingdao Central Hospital grant number KY202209902. The study complied with the Declaration of Helsinki. All participants had signed informed consent forms.
Establishment of the QCC Team
A QCC team was established on December 1, 2015, under the name “Lianxin Circle.” Its mission is to foster unity and collaboration across hospital departments, centered around the ECG network. Aligning with the broader Internet Plus environment, the team aims to fully explore and actively develop the Internet of Things (IoT), applying big data information management models to promote the development of hospital informatization. The team consists of nine members: two associate chief physicians, two attending physicians, three physicians, one nurse practitioner, and one senior engineer. QCC activities follow the PDCA cycle monthly: Plan (set monthly goals at the beginning of each month) → Do (implement countermeasures) → Check (analyze data at month-end) → Act (optimize deficiencies; eg, in February 2025, upon identifying “poor cooperation from elderly patients,” the countermeasure “involve multiple family members in procedures” was added).15 The QCC activities ran from January to April 2025. The circle leader strictly followed the 3:4:2:1 principle to create a Gantt chart for activity planning. Weekly meetings were held to discuss progress, assign responsibilities, and set deadlines for each task, ensuring activities advanced according to schedule.
Topic Selection
Team members employed brainstorming techniques and utilized the 531 scoring method15 to evaluate potential topics based on their impact on 12-lead ECG diagnostic accuracy, importance, urgency, and team capability. The topic “Reducing Non-Compliance Rates in 12-Lead ECG Procedures” was ultimately selected as the activity focus.
Current Status Assessment
After thoroughly understanding the service process of the ECG network,16 a workflow diagram was drawn. An investigation was conducted on the ECG network database from January to April 2024 and January to April 2025. Using the 5W2H method, a checklist was created to investigate the number of non-standard ECG operation cases and their causes,17 totaling 758 cases. According to the hospital’s monthly quality control statistics, the non-compliant operation rate = number of non-compliant operations / total number of operations = 17.66%. As shown in Figure 1 (Pareto chart), the primary causes of non-compliant procedures included: data collection artifacts, insufficient acquisition time, data transmission failures, data analysis software malfunctions, patient skin allergies, patient refusal due to dissatisfaction, computer malfunctions, data reception failures, data information asymmetry, and network failures. Based on the Pareto principle18 (80/20 principle), addressing the two issues of “data collection artifacts” and “insufficient acquisition time” is the primary focus of this activity. Data collection artifacts refer to waveform abnormalities caused by non-cardiac factors such as environmental or electrode interference. Insufficient acquisition time refers to situations where the ordinary electrocardiogram is recorded for less than 10 seconds, or a 24-hour ambulatory electrocardiogram is recorded for less than 24 hours.
 |
Figure 1 ECG Network Data in Medical Consortium. Data collection artifacts and Insufficient acquisition time are the two most significant reasons. Data collection artifacts is closely related to various factors such as the environment, equipment, and patients, while Insufficient acquisition time depends more on the operator. |
Goal Setting
Based on the current value, improvement priorities, and circle capability, the target value is calculated as: Target Value = Current Value - Improvement Value = Current Value - (Current Value × Improvement Focus × Circle Capability) = 17.66% - (17.66% × 81.69% × 80.51%) = 6.05%. Considering comprehensive factors, the activity group ultimately set the target value for the non-standard operation rate at 7.05%.
Analysis of Non-Compliant Operation Causes
All QCC members first employed brainstorming techniques to conduct a comprehensive analysis across five dimensions: personnel, machinery, materials, methods, and environment. They visualized findings using a fishbone diagram (Figure 2), 18 identifying 20 potential influencing factors. Subsequently, the 531 scoring method was applied to quantitatively evaluate each terminal factor, and six key factors were selected based on the Pareto principle. The research team developed a detailed factor verification plan, employing a combination of on-site observation, in-depth interviews, and literature review for empirical validation. This process ultimately identified four core factors affecting operational standardization: insufficient professional skills of operators, poor patient cooperation, unstable equipment performance, and non-compliant examination environments. These factors interact synergistically, collectively forming key barriers to ECG acquisition quality.
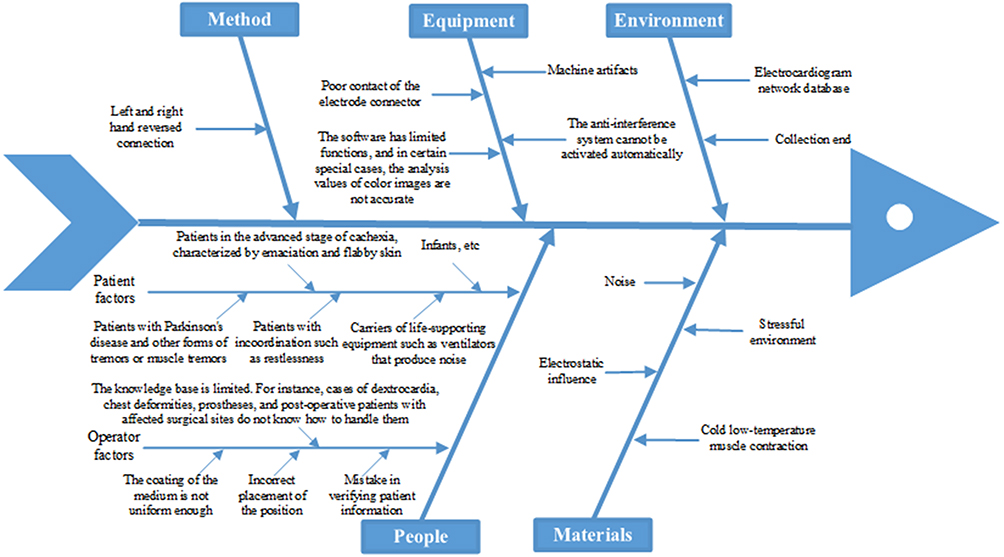 |
Figure 2 Fishbone Diagram of Factors Affecting Operations. Personnel, Equipment, Materials, Methods, and Environment. The factors of improper operation were analyzed from the human perspective, where human-related reasons include both the patient and the operator. |
Strategy Formulation and Implementation
Based on the four key factors identified through fishbone diagram analysis, a systematic improvement plan comprising four components was developed by establishing an integrated quality improvement system encompassing personnel, equipment, patients, and environment:
(1) Standardized ECG Operator Training: The research team collaborated with the Nursing Department and Medical Technology Department to establish a multi-tiered training system. By engaging ECG specialists to conduct standardized operational training, emphasis was placed on enhancing operators’ technical proficiency and quality control awareness. Concurrently, a rigorous training management system was implemented, requiring all new hires to complete a one-month rotation training in the ECG lab. A quarterly assessment mechanism was introduced to ensure training effectiveness. Statistical data revealed a 95% training participation rate, average assessment scores exceeding 95 points, and knowledge retention rates rising to 96%, significantly elevating operators’ professional competence.
(2) Improving ECG Acquisition Methods for Special Patient Groups: The research team developed differentiated solutions. For anxious or tense patients, psychological interventions such as playing soothing music and guiding deep breathing were implemented. For elderly and cachectic patients, Electrode patch-assisted fixation and multi-person coordination techniques were developed. Standardized sedation protocols were applied for infant and pediatric patients. For patients with limb impairments, innovative adjustments were made to electrode placement, including elevating upper limb electrodes and combining lower limb leads. By establishing a supervision and inspection mechanism, the standardized implementation of all specialized acquisition protocols was ensured, effectively improving the examination success rate for special patient groups.
(3) Ensuring High-Quality Equipment Operation: The study implemented a systematic upgrade and maintenance plan. Priority was given to procuring new electrocardiograph machines with sampling rates exceeding 1000Hz, equipped with high-resolution displays and low-noise amplifiers. These were complemented by professional-grade hypoallergenic electrode pads, ensuring signal acquisition quality at the hardware level. The Medical Technology Department established a comprehensive equipment maintenance system, including daily functional inspections, quarterly performance calibrations, and a 30-minute rapid response mechanism. This ensures equipment remains in optimal working condition, significantly reducing operational non-compliance issues caused by equipment failures.
(4) Improving the ECG recording environment: Systematic improvements were implemented across both physical and human dimensions. The physical environment can affect the accuracy of equipment, while stress and other emotional factors can cause temporary abnormalities in cardiac electrical activity.19 Physically, examination beds are preheated with electric blankets or an Infrared heating lamp during autumn and winter to maintain comfortable temperatures, while strictly eliminating electromagnetic interference sources like smartwatches. Culturally, standardized communication protocols were implemented, including assisting patients with clothing adjustments, removing metal accessories, and providing psychological reassurance. This comprehensive optimization of environmental conditions creates favorable circumstances for ECG examinations, effectively reducing data collection artifacts caused by environmental factors.
Experimental Results
Following QCC implementation, the non-compliant operation rate at 12-lead ECG collection endpoints within the network system significantly decreased, from 17.66% to 6.17% (P<0.05), After QCC activities, members’ team spirit, QC techniques, mental development, communication and coordination, activity confidence, responsibility and honorall show positive improvement.
This study employed the PDCA cycle and quality circles to reduce non-standardized medical data collection rates and complaint rates, demonstrating the effectiveness of quality circles in standardizing medical processes. Statistical analysis was conducted using SPSS30.0 software, with comparisons made via chi-square tests. P < 0.05 was considered statistically significant.
Problem Improvement
The study findings indicate that the implementation of quality circles has yielded significant quality improvement outcomes. Data sourced from the ECG Network Database, as shown in Table 1, through systematic interventions and team collaboration, the rate of non-standard ECG procedures decreased significantly from 17.66% pre-intervention to 6.17%, exceeding the predetermined target of 7.05%. A paired chi-square test was used to compare the pre- and post-intervention non-compliance rates between the two groups. Since both samples originated from the same ECG network system, there were no statistically significant differences in baseline patient characteristics (eg, age, underlying diseases) between the groups (P>0.05). The sample size discrepancy (402 vs 356 cases) resulted from natural fluctuations in patient volume and was adjusted for through “monthly patient volume normalization.” This adjustment was validated as statistically significant via χ2 testing (χ2=23.12, P<0.01). Further analysis (Figure 3) revealed marked improvement trends across all non-compliant categories. The two most critical issues—“data collection artifacts” and “insufficient acquisition time”—showed the most pronounced reduction, with their incidence rates dropping from 13.43% to 3.93%, representing a 71% decrease. Particularly noteworthy is the substantial reduction in “ data collection artifacts,” which dropped from 9.2% to 2.25%, demonstrating especially significant improvement. During the three-month consolidation period follow-up, the rate of non-standardized procedures decreased further by 1.82% compared to the active phase, while the rate of standardized procedures increased by 4.11%. This sustained improvement trend fully validates the effectiveness and sustainability of the implemented countermeasures.
 |
Table 1 Statistical Data Comparison Before and After Improvement (Three-Line Chart). The Non-Compliance Rate Before QCC Was 17.66%, and the Non-Compliance Rate After QCC Was 6.17%. Its Effectiveness Was Confirmed Through a Chi-Square Test (χ2=23.12,P<0.01) |
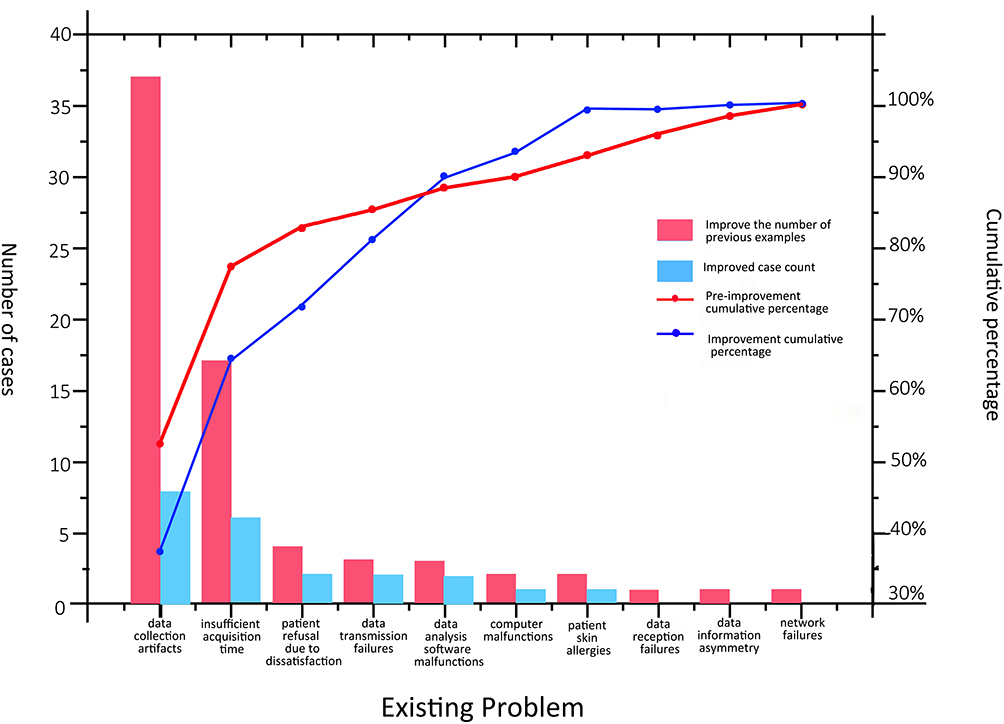 |
Figure 3 Pre- and Post-Activity Electrocardiogram Network Data. |
Economic Impact
This study achieved remarkable results in enhancing healthcare service quality through the implementation of quality circles. Statistical analysis of complaint records from the Patient-Physician Communication Office revealed a marked downward trend in patient complaints post-intervention. The monthly average decreased from 32 to 23 cases, representing a 28.13% reduction. This change reflects a substantial improvement in clinical service quality. At the same time, patient commendations increased from an average of 46 per month to 51 per month, representing a 10.87% rise. These data shifts not only demonstrate heightened patient satisfaction but also indirectly indicate improved efficiency in healthcare resource utilization, reducing wasteful practices such as redundant tests caused by non-standard procedures.
Intangible Outcomes
These QCC activities yielded multifaceted gains in enhancing the team’s overall capabilities. Through sustained quality improvement practices, members achieved significant proficiency in applying quality management tools, including proficient use of quality control techniques such as Pareto charts and fishbone diagrams. More importantly, team members demonstrated substantial growth in problem-solving skills, innovative thinking, and quality awareness. The cross-departmental collaboration mechanism established during the activity not only improved work efficiency but also fostered a spirit of cooperation and a sense of responsibility among team members.20 These intangible gains have laid a solid foundation for building a culture of continuous quality improvement within the hospital and provided valuable experience for future quality improvement projects. Through regular experience sharing and the establishment of standardized operating procedures, these achievements will generate a lasting impact on a broader scale (Figure 4).
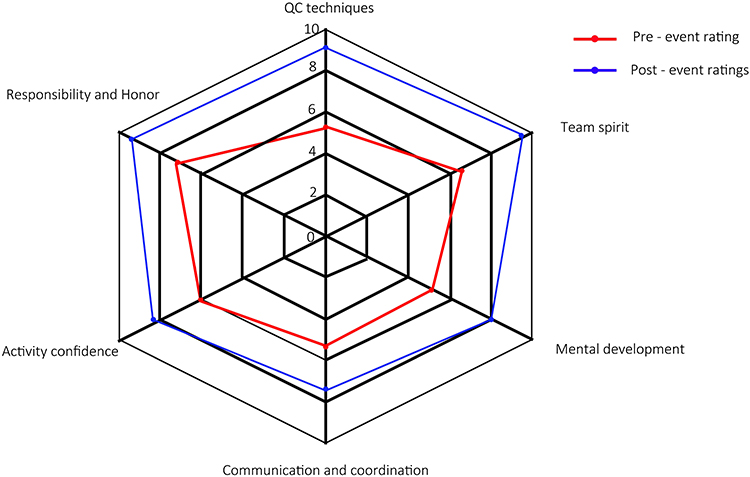 |
Figure 4 Group Scores Before and After the Activity. QCC members rated each other within the group according to a standard scoring sheet before and after the activity, and all scores showed significant improvement after the activity. |
Discussion
ECG operation is a common and significant problem in clinical ECG collection, as it reduces both collection efficiency and accuracy. Through a QCC activity, we analyzed the reasons for irregular operations and developed solutions, successfully reducing the occurrence of non-compliant operations the main reasons for improper operation. The reasons include collection data artifacts, insufficient collection time, data transmission failures, data analysis software malfunctions, patient skin allergies, patient dissatisfaction and refusal of examination, computer malfunctions, data reception failures, information asymmetry, and network failures, among which “data collection artifacts” and “insufficient collection time” are the two primary causes.
The collection time for a routine ECG should be at least 10 seconds, while a 24-hour Holter monitor ECG requires a duration of more than 24 hours. Insufficient collection time can easily lead to missed abnormal cardiac activities, resulting in misdiagnosis. Clinicians must ensure the required collection duration when performing ECG collection, and patients wearing a 24-hour Holter monitor should be instructed to wear it for at least 24 hours.
Data collection artifacts occur due to various reasons, resulting in ECG artifacts that do not reflect the heart’s true electrical activity, which can easily lead to misdiagnosis. The generation of ECG artifacts involves complex interactions among multiple factors, including equipment, operator, patient, and environment. These artifacts not only compromise signal acquisition quality but may also lead to clinical misinterpretation.21 Through systematic analysis, this study identified key factors affecting ECG quality and proposed targeted improvement strategies. The findings are explored in depth across three dimensions below:
Equipment and Operational Level
At the equipment and operational level, electrode issues represent a primary cause of artifacts. Poor contact or displacement of electrodes can directly lead to signal interruption or distortion, closely related to factors such as inadequate skin cleansing, excessive body hair not shaved, poor electrode quality, or dried conductive gel.22 Equipment problems such as aging, broken, or tangled lead wires, along with poor battery contact or low battery power, can also cause intermittent signal interference. Non-standardized operational procedures significantly impact quality, particularly the common practice of improper electrode placement that fails to avoid areas with dense muscle or fat. The study found that operators’ familiarity with equipment performance directly affects procedural quality, with most operational errors stemming from insufficient understanding of device characteristics.
Patient-Related Factors and Environmental Interference
Patient-related factors and environmental interference are equally critical. During dynamic ECG monitoring, vigorous activities like chest expansions, lifting heavy objects, or frequent upper limb movements can generate electromyographic interference. Additionally, the patient did not stay away from electromagnetic fields such as cell phones and microwave ovens as instructed, and wearing static-prone synthetic fabrics may introduce external electromagnetic interference. Some chronic disease patients may experience electrode detachment or contact dermatitis due to excessive sweating or skin sensitivity, further compromising signal quality. Environmental factors account for a significant proportion of total artifacts, with electromagnetic interference being the most prevalent.23
Operator Proficiency
Operator proficiency is another critical factor affecting examination quality. Trainees and new operators in primary care settings are prone to errors, such as mixing up left and right electrode leads or performing procedures in the incorrect order. This primarily stems from inadequate training before deployment, particularly insufficient patient education. Patients often lack understanding of the examination’s purpose and precautions, leading to poor compliance. Establishing a robust quality management system and training mechanism is crucial, including standardizing operational procedures, enhancing pre-service training and assessment, and improving health education.
Conclusion
As a vital tool in clinical diagnosis, the standardization of ECG procedures directly impacts the accuracy and reliability of diagnostic outcomes. This study systematically applied the QCC management method to conduct an in-depth analysis of key factors contributing to non-standard ECG practices across five dimensions: personnel, equipment, materials, methodology, and environment. Targeted improvement measures were subsequently developed. Results demonstrated that through interventions including establishing a standardized training system, optimizing management protocols for special patient groups, improving equipment maintenance procedures, and enhancing examination environment conditions, the non-compliance rate in ECG operations significantly decreased from 17.66% pre-intervention to 6.17%, exceeding the predetermined target. This improvement not only standardized the ECG network operation procedures for medical staff but also comprehensively elevated the service quality of ECG examinations.
More importantly, this study yielded multiple positive effects: clinically, It effectively reduces the occurrence of irregular ECG operations.; administratively, it established a sustainable quality improvement mechanism; and at the personnel level, it enhanced the team’s professional skills and collaborative capabilities. Looking ahead, the integration of emerging technologies like artificial intelligence with quality management approaches such as quality circles holds promise for continuously elevating ECG examination quality. This advancement will provide more reliable diagnostic foundations for clinical practice, ultimately benefiting a broader patient population. Future research will further explore the application of intelligent technologies in quality improvement and the feasibility of extending this model to other medical examination procedures.
Funding
This work was supported by the Shandong Provincial Natural Science Foundation under Grant ZR2025QC1581.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ceasovschih A, Șorodoc V, Covantsev S, et al. Electrocardiogram features in non-cardiac diseases: from mechanisms to practical aspects. J Multidiscipl Healthc. 2024;17:1695–10. doi:10.2147/JMDH.S445549
2. Balta A, Ceasovschih A, Șorodoc V, et al. Broad electrocardiogram syndromes spectrum: from common emergencies to particular electrical heart disorders. J Personal Med. 2022;12(11):1754. doi:10.3390/jpm12111754
3. Anbalagan T, Nath MK, Vijayalakshmi D, et al. Analysis of various techniques for ECG signal in healthcare, past, present, and future. Biomed Engineer Advanc. 2023;6:100089. doi:10.1016/j.bea.2023.100089
4. Wang R, Veera SCM, Asan O, et al. A systematic review on the use of consumer-based ECG wearables on cardiac health monitoring. IEEE J Biomed Health Inform. 2024;28(11):6525–6537. doi:10.1109/JBHI.2024.3456028
5. Saini SK, Gupta R. Artificial intelligence methods for analysis of electrocardiogram signals for cardiac abnormalities: state-of-the-art and future challenges. Artif Intell Rev. 2022;55(2):1519–1565. doi:10.1007/s10462-021-09999-7
6. Raut K, Ghosh A, Kapoor A. The unusual case of a Topsy-Turvy ECG with a pseudo-infarct pattern. J Electrocardiol. 2021;69:93–95. doi:10.1016/j.jelectrocard.2021.09.008
7. Kraik K, Dykiert IA, Niewiadomska J, et al. The most common errors in automatic ECG interpretation. Front Physiol. 2025;16:1590170. doi:10.3389/fphys.2025.1590170
8. Zhang D, Liao M, Liu T. Implementation and promotion of quality control circle: a starter for quality improvement in Chinese hospitals. Risk Manage Healthc Policy. 2020;Volume 13:1215–1224. doi:10.2147/RMHP.S261998
9. Zhao H, Hu M, Cao Y, et al. Study on the application of quality control circle activity in postoperative nursing of elderly dental implants. Medicine. 2024;103(2):e36894. doi:10.1097/MD.0000000000036894
10. Chen P, Yuan T, Sun Q, et al. Role of quality control circle in sustained improvement of hand hygiene compliance: an observational study in a stomatology hospital in Shandong, China. Antimicrob Resist Infect Control. 2016;5(1):54. doi:10.1186/s13756-016-0160-1
11. Wang Y, Zhou X, Zhu Y, et al. Effect of quality control circle activities on reducing the failure rate of surgical instrument pre-treatment. Risk Manage Healthc Policy. 2025;Volume 18:1837–1845. doi:10.2147/RMHP.S520770
12. Wang J, Xia L, Zheng N, et al. Application of quality control circle in improving early rehabilitation intervention rate of stroke patients. Risk Manage Healthc Policy. 2025;Volume 18:1209–1216. doi:10.2147/RMHP.S502704
13. Wang LR, Wang Y, Lou Y, et al. The Role of Quality Control Circles in Sustained Improvement of Medical Quality. Springer Plus; 2013:1141.
14. Garofalo S, Battaglia S, Di Pellegrino G. Individual differences in working memory capacity and cue-guided behavior in humans. Sci Rep. 2019;9(1):7327. doi:10.1038/s41598-019-43860-w
15. Yao S, Yi L, Hu R, et al. Using the task-oriented quality control circle to build the central sterile supply department quality control system for foreign objects remaining in sterile packages. Risk Manage Healthc Policy. 2025;Volume 18:1441–1454. doi:10.2147/RMHP.S514458
16. Hsieh J, Hsu M W. A cloud computing based 12-lead ECG telemedicine service. BMC Med Inf Decis Making. 2012;12(1):77. doi:10.1186/1472-6947-12-77
17. Monteiro DE, Fialho ICTS, Passos PM, et al. Management of coping with the risks of COVID-19 in an onco-hematological outpatient clinic: an experience report. Revista Brasileira de Enfermagem. 2021;74(suppl 1):e20201080. doi:10.1590/0034-7167-2020-1080
18. Kumah A, Nwogu CN, Issah AR, et al. Cause-and-effect (fishbone) diagram: a tool for generating and organizing quality improvement ideas. Global J Quality Safety Healthc. 2024;7(2):85–87. doi:10.36401/JQSH-23-42
19. Battaglia S, Nazzi C, Thayer JF. Heart’s tale of trauma: fear-conditioned heart rate changes in post-traumatic stress disorder. Acta Psychiatrica Scandinavica. 2023;148(5):463–466. doi:10.1111/acps.13602
20. Lingling L, Fei P, Chunyi G, et al. Effect of quality control circle activity on shortening postoperative urinary catheter indwelling time of obstetrics and gynecology department patients undergoing abdominal surgery. Zhonghua Yiyuan Ganranxue Zazhi. 2024;34(2):288–293.
21. Wasimuddin M, Elleithy K, Abuzneid AS, et al. Stages-based ECG signal analysis from traditional signal processing to machine learning approaches: a survey. IEEE Access. 2020;8:177782–177803. doi:10.1109/ACCESS.2020.3026968
22. Lezhnina IA, Boyakhchyan AA, Ivanov MA, et al. The influence of skin-electrode contact on the quality of ECG recording for personal telemedicine systems[C]//IOP. Conference Series. 2019;516(1):012048.
23. Aliyev F, Türkoğlu C, Çeliker C, et al. Electromagnetic interference with electrocardiogram recording of exercise test equipment. Turk Kardiyol Dern Ars. 2010;38(5):352–354.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.