Back to Journals » Risk Management and Healthcare Policy » Volume 16
Application of Public Health Precautionary Guidelines Before Contracting COVID-19: Lessons Learned from a Qualitative Descriptive Study
Authors Almulla H ![]() , Al-Ansari A
, Al-Ansari A
Received 4 November 2022
Accepted for publication 21 January 2023
Published 2 February 2023 Volume 2023:16 Pages 101—109
DOI https://doi.org/10.2147/RMHP.S396153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Hebah Almulla,1 Asim Al-Ansari2
1Department of Fundamentals of Nursing, College of Nursing, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Department of Preventive Dental Sciences, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Hebah Almulla, Tel +1 966 13 333-1648, Email [email protected]
Background: The COVID-19 pandemic has affected the Saudi population despite early efforts taken by officials. This study aimed to describe the precautionary measures taken by patients prior to their diagnosis with COVID-19.
Methods: A qualitative descriptive design was employed to collect data from a convenience sample of 26 participants who had COVID-19 and recovered. Data was collected through conducting telephone interviews and was then transcribed and analyzed using inductive content analysis methods adapted from grounded theory.
Results: Data analysis yielded six categories of precautionary measures participants reported using to minimize their risk of contracting COVID-19: (1) wearing a mask, (2) staying at home and avoiding crowds, (3) washing hands and wearing gloves, (4) following social distancing, (5) using sanitizers, and (6) not interacting with anyone.
Conclusion: The discrepancy found between the participants’ reported precautionary measures and their actual behavior, as well as the consistency and specificity with which they implemented some and not all measures raise concerns about existing public health messages. The study findings support the importance of well-structured and detailed communication when designing future public health campaigns and data-driven policies.
Keywords: precautionary measures, COVID-19, qualitative, content analysis, Saudi Arabia
Introduction
On March 11, 2020, The World Health Organization (WHO) declared COVID-19 a pandemic after assessing its concerning levels of spread and severity.1 Since then, the virus has led to over 536 million cases and 6.3 million deaths.2 Because of the highly infectious nature of the virus, the WHO emphasized the importance of implementing preventive and mitigation measures. During the early stages of the pandemic, people experiencing respiratory symptoms were explicitly advised to take preventive measures.3 However, as new evidence emerged, such as asymptomatic virus carriers, the WHO updated their precautionary guidance, generalizing it to everyone rather than only people with respiratory symptoms.4 The WHO provided the public with clear guidance on the necessary actions to reduce their risk of acquiring the virus, including handwashing, wearing a mask, coughing, sneezing into a tissue, having appropriate room ventilation, and following physical and social distancing.3 In addition, the WHO disseminated specific instructions for each preventive measure on its website and made these resources accessible by publishing them in various languages and forms like brochures, videos, printouts, and articles.4
In Saudi Arabia, in late January 2020, a royal decree established an emergency committee with membership drawing from 24 government bodies and headed by the Deputy Minister of Health; the committee included the ministries of finance, education, and interior and the Saudi Food and Drug Administration.5 In response to the first detected case of COVID-19 in Saudi Arabia, the committee made more than 28 critical decisions to contain the virus’s spread.5 Initially, they suspended travel to China, evacuated all Saudi citizens from China, and banned tourists from entering the kingdom. Later, the suspensions included international flights and visits to the holy mosques as well as education, social events, in-person work for government agencies, and public gatherings. In addition, mosques, shops, and malls were temporarily closed, and the government enforced a partial curfew during the pandemic’s early months.
As the pandemic peaked, the committee enforced an around-the-clock curfew and activated mass field testing. Moreover, non-compliant private entities and individuals who violated the preventive measures faced penalties.5 The Saudi government and public authorities’ decisions were essential in shaping the curve of COVID-19 cases and deaths compared to other countries.6 Some measures, such as social distancing, wearing face masks, and avoiding public gatherings, remained imposed on the public and were backed by penalties even after the quarantine lifted and general and commercial activities resumed. Previous studies suggested that public adherence to the preventive measures was adequate during the severe acute respiratory system (SARS) outbreak due to imposing legal and financial consequences for non-compliance.7 In Saudi Arabia, around 40% of the participants revealed that they would not wear masks if there were no financial ramifications imposed by the government.8
The Saudi Ministry of Health (MOH) and other relevant authorities communicated preventive guidelines to the public through TV, radio, text messages, and media, including ongoing pandemic updates. The MOH also established a toll-free call center for any inquiries.9 Furthermore, the MOH boosted awareness through educational campaigns urging the public to stay home and follow precautionary measures.5 These measures included wearing a face mask, handwashing and sanitizing, social distancing, and avoiding public gatherings. Furthermore, the MOH designed various instructional materials to educate the public through their social media platforms, such as YouTube, Twitter, and Instagram. In addition, the MOH’s website included links and hyperlinks to educational information. For example, LiveWellMOH is a notable illustration that included posts and instructional materials—notably, it went beyond demonstrating the proper way to wear a mask, wash your hands, and use sanitizers.10
Although some measures contradicted Saudi social norms and values, such as being hospitable, citizens still believed in their importance and agreed with the Saudi authorities’ actions to contain the virus.11,12 Evidence suggests that 98% of Saudis were confident in the preventive measures the government initiated to fight the COVID-19 outbreak.11 In addition, a cross-sectional study investigating the knowledge, attitude, and practices of face mask-wearing reported that most Saudi citizens had sufficient knowledge and a positive attitude toward consistently using face masks.8 However, the study design refrained from extracting information regarding the degree of knowledge and demonstrated practices of the participants when using their face masks.8
In Saudi Arabia, the pandemic has affected around 800,000 despite early measures taken by officials.13 Various factors identified in the literature influence public compliance with preventive measures, including public knowledge and practice about the COVID-19 prevention protocols, public trust in the measures employed by the Saudi authorities, and the public’s risk perception.11,12,14–17 Although some research focused on the factors influencing Saudis’ compliance with the recommended preventive and precautionary measures, only three studies investigated the measures Saudis took to avoid contracting COVID-19.14–16 Two of the three studies used a quantitative design; only one used a qualitative design to understand the Saudis’ risk perceptions and precautionary behavior toward COVID-19.16 Additionally, none of these studies examined precautionary measures taken by COVID-19 patients before being confirmed positive for the virus. Instead, all prior studies conducted in Saudi Arabia were limited to information from unaffected individuals.
The current study thus aims to describe the precautionary measures COVID-19-positive patients carried out before they were diagnosed with COVID-19 and recovered. The implications of the results are essential for public health policymakers in Saudi Arabia and elsewhere to make effective, evidence-informed decisions during the current COVID-19 pandemic and for long-term preparations for future pandemics.
Methods
Study Design
This study used a qualitative descriptive design to collect data through semi-structured telephone interviews during the first wave of the pandemic between July 8, 2020, and September 6, 2020. Institutional Review Board (IRB) approval was obtained from Imam Abdulrahman bin Faisal University (IRB-2020-04-117), Saudi Arabia. This study was conducted following the Declaration of Helsinki’s ethical principles. A convenience sample of 26 participants who had contracted COVID-19 and recovered was recruited from two COVID-19–designated hospitals in the eastern region of Saudi Arabia. Participants were 21 to 60 years old, could communicate in Arabic, had a confirmed COVID-19 laboratory test, and were discharged home after being hospitalized with COVID-19.
The study used an IRB-approved script to contact eligible participants and obtain their consent to participate in the study. Before each interview, participants’ oral consent was obtained and audio recorded. ID code numbers were also assigned to participants to maintain their privacy throughout the study. In addition, the participant-informed consent emphasized that study results would be published while anonymizing the responses to ensure the participants’ privacy. The senior author then individually interviewed participants; the interviews were audio recorded.
This study aims to answer an open-ended question queried to each participant: “Before getting infected with COVID-19, what did you do, if anything, to minimize your risk of getting infected?” The authors then employed inductive content analysis to code data from participants’ words through a systematic and objective process.18–21
Analytic Strategy
Interview data audio files were transcribed verbatim in Arabic and then verified for accuracy; the transcriptions were translated into English before coding. For translation rigor and semantic and conceptual equivalence, a team of experts translated the data in phases.22–24 First, transcripts were translated into English by a qualified bilingual translator and then verified for accuracy by the bilingual authors. Then, 25% of the English-translated interviews were back-translated into Arabic and were checked against the original Arabic transcribed interviews to achieve translation validity.
The authors coded the translated data using inductive content analysis methods adapted from grounded theory.18,20,21,25,26 First, they read the transcripts to become familiar with the data and to identify the unit of analysis (complete idea), then unitized the data by breaking the verbatim text into specified units of analysis. Unitized data with common properties were organized into initial groups as part of open coding. Initial groups were then refined into defined categories. When possible, coders extracted category labels from participants’ words rather than from labels applied to them. A constant comparative analysis enabled ensuring the fit of each unit within its category and not with other categories. Results trustworthiness was obtained by peer debriefing and maintaining an audit trail.21,27 Whenever there was a disagreement about the categories, the authors strove to reach a consensus.
Results
Sample Characteristics
Of the 26 participants who participated, 18 (69%) were males, and 8 (31%) were females, averaging 43 (SD 9.2) years of age and ranging from 21 to 60 years. See Table 1 for a detailed demographic description of the study sample.
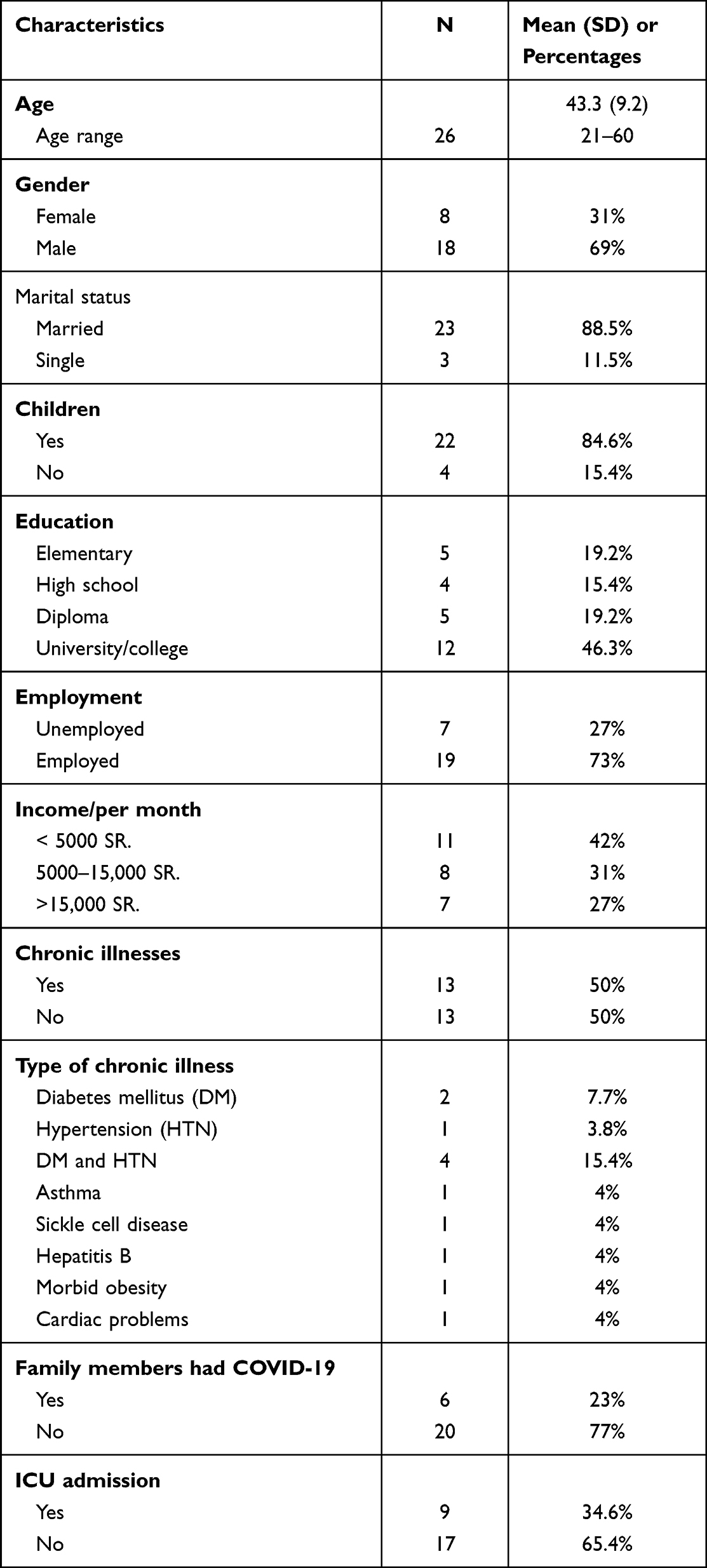 |
Table 1 Participants’ Demographic Characteristics (N = 26) |
Data analysis resulted in six categories of precautionary measures that participants reported they used to minimize their risk of contracting COVID-19 before testing positive: (1) wearing a mask, (2) staying at home and avoiding crowds, (3) washing hands and wearing gloves, (4) following social distancing, (5) using sanitizers, and (6) not interacting with anyone, including refraining from visits. Table 2 summarizes each category.
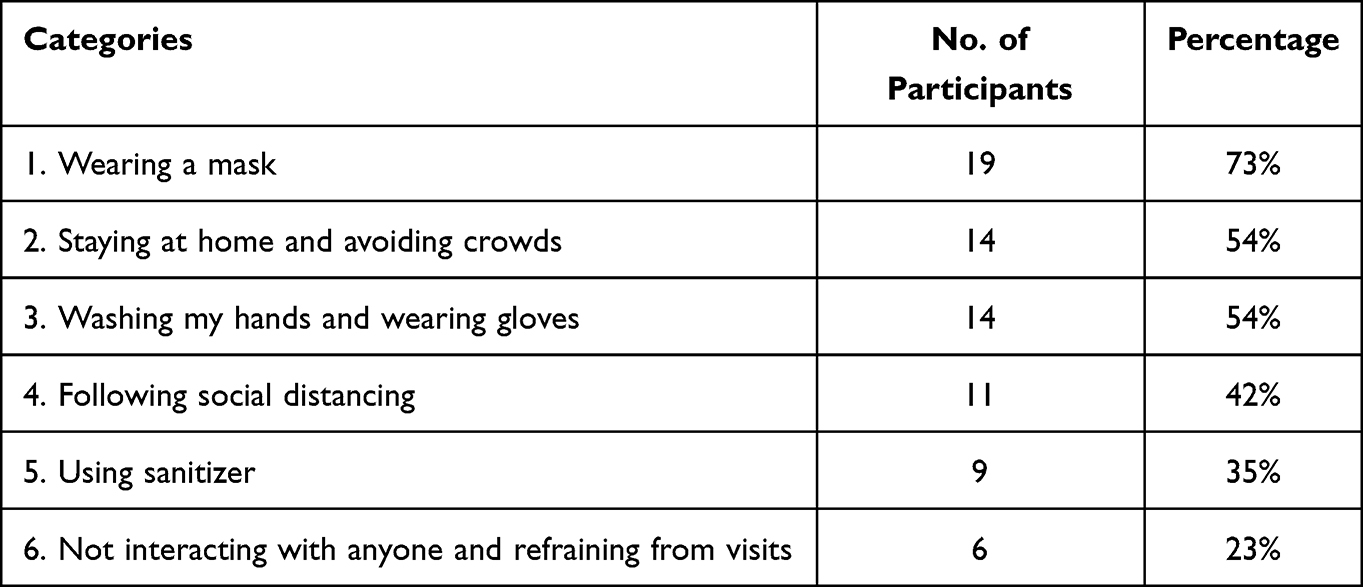 |
Table 2 Categories of the Reported Self-Precautionary Measures (N = 26) |
Some participants reported taking precautions but did not specifically describe what they did: “I apply all instructed precautions by the MOH (1006); I used to take normal precautions (1015); I used to take every precaution (1004)”. However, two of the 26 patients who recovered from COVID-19 reported not taking any precautionary measures before becoming infected. When asked, they stated, “No, I didn’t do anything (1004); we were neglecting the precautions at work, to be honest (1045).”
Category One: Wearing a Mask
Most study participants (73%) reported using masks before contracting COVID-19: “I was using the mask (1026); I was wearing the mask (1024).” Indeed, it was the only precaution one participant took: “I did nothing, just the mask (1018).” Others explained they wore their masks when they left home or were at work: “When I leave the house, I wear a mask” (1008); “I wear a mask when I go out” (1040); “I wear a mask when I go to the supermarket only” (1045). One participant stated that he had to remove his mask during prayer: “I stay with the mask till the end of my working hours; I remove my mask only when I pray” (1035). Another participant explained why he may have contracted COVID-19 despite mask-wearing: “I was wearing the mask, but I think the problem is that I was using it the wrong way. I used to change my mask every week, not every day” (1018).
Category Two: Staying at Home and Avoiding Crowds
Over half of the study sample (54%) described isolating themselves at home and avoiding crowds when asked what measures they took to avoid contracting COVID-19 before their illness. Most participants stated they did not leave home at all: “I stayed at home for 3 months” (1024); “I didn’t go out at all. I didn’t even see the street” (1002); “I isolated myself; I was away” (1046). Others mentioned they would leave the house for work or grocery shopping: “I wasn’t leaving home except for work” (1031); “I don’t go anywhere other than the nearest supermarkets to my home” (1023). One participant emphasized, “I was working remotely for 3 months before I got infected” (1046). Others discussed staying away from crowds: “I avoid crowded areas. I don’t go to malls or markets if there is nothing necessary” (1006).
Category Three: Washing My Hands and Using Gloves
In our study sample, 54% reported washing their hands and using gloves as a precautionary measure to reduce their risk of catching the virus: “I wash my hands” (1008); “I wear gloves” (1023); “I was wearing gloves all the time” (1044).
Three participants spoke about wearing gloves at work and when shopping: “I shop wearing gloves” (1034). Only one participant provided further details:
I wear gloves before I carry the groceries to the house. I have my own gloves in the car; I don’t use the ones from the shops or supermarkets or whatever they provide. After I am done shopping, I go back to my car, and I remove the gloves and throw them in the trash. When I go home, I wear new gloves when carrying the groceries inside. (1035)
Category Four: Following Social Distancing
Around half (42%) of the interviewed participants explained that they followed social distancing and avoided contact with others before being infected: “I keep a distance” (1008); “I apply social distancing” (1006). Three participants mentioned following social distancing at work: “I keep distance from workers and customers” (1023); “There is a distance between me and my coworkers” (1032). Two participants explained that they avoided shaking hands; instead, they greeted others from a distance: “I didn’t shake anyone’s hand” (1003); “I wasn’t touching anyone” (1024). Three participants cautiously avoided contact with others. One stated, “I didn’t come in contact with anyone” (1043). One participant went so far as to avoid contact with his immediate family: “I don’t come close to my wife or daughter at home” (1035). Although several participants claimed they maintained social distance, only one specified the distance he kept, stating, “We kept distance like more than a meter” (1023).
Category Five: Using Sanitizers
Several participants (35%) reported they purchased and used sanitizers: “We brought the sanitizers and placed them at the entrance of the house” (1023); “We always carry a sanitizer, antibacterial sanitizer” (1029). In addition, a few participants indicated they sanitized their hands and shopping bags: “I protect myself by keeping my hands sanitized” (1031); “I sanitize the shopping bags” (1008). However, no participants mentioned sanitizing surfaces or explained the method or amount of time they sanitized their hands.
Category Six: Not Interacting with Anyone and Refraining from Visits
During the pandemic, several study participants (23%) abstained from interacting with people. They refrained from visiting others or inviting them to their homes to protect themselves and the people around them: “I never interacted with anyone” (1024); “I don’t interact with people” (1021); “I don’t invite people, and I don’t visit anybody” (1006). One participant provided additional details about the changes he made:
In my home, I used to have a lot of people coming to visit on a daily basis. My house was the meeting place for the neighborhood where I live. Neighbors come to my home, and as I have a say on the people in my area, I managed to put these visits on hold until the pandemic problem is over. (1023)
Discussion
This study is the first in the Kingdom of Saudi Arabia to interview patients recovering from COVID-19 after hospitalization to understand, in the participants’ own words, their self-protective behaviors before getting the virus. This information could better facilitate public health authorities to prepare future public health educational programs and precautionary instructions.
Among the 26 participants, only two reported not taking any precautions, yet all contracted the virus. Nevertheless, most reported wearing face masks, staying home, avoiding crowded areas, washing their hands, using gloves and sanitizers, following social distancing, and refraining from interacting with and visiting others. The findings are consistent with the knowledge and practices reported by participants in other studies conducted in Saudi Arabia.14–16 Although most participants reported carrying out the self-precautions, all were hospitalized due to COVID-19. Assuming their reported responses were not affected by a self-enhancement or social desirability bias, the question becomes: What was missing? What was insufficient in their application of those precautions? This study’s results provide partial answers. Ultimately, the present study illustrates the importance of understanding how participants applied the precautions and highlights the disparity between participants’ reported knowledge of the measures and their actual precautionary behavior.
Interviews revealed several possible explanations for why individuals contracted COVID-19 despite taking precautions. First, not all participants reported carrying out all the recommended precautions; it is a dosage problem. For example, one person claimed that the mask was the only precaution he applied: “I did nothing, just the mask” (1018). Second, although 73% reported using a face mask, we are unaware of the mask participants used and whether it was worn correctly. Third, in the early stages of the first wave of the COVID-19 pandemic, some people used paper masks and reused them multiple times. For instance, one participant reported: “I was wearing the mask, but I think the problem is that I was using it the wrong way. I used to change my mask every week, not every day” (1018). Finally, we are unaware of how participants removed and discarded their masks. For example, one participant reported removing his mask at work to pray, and we do not know how long it took him to put his mask on after prayer. During the interview, the participant disclosed why he might have contracted COVID-19, saying: “I think I got COVID after I forgot to put back my mask after taking it off at work to pray” (1035).
It is important to emphasize that participants in this study are considered “early acquirers” of the virus, having acquired it when the nature of the spread was unclear, even in the health community. Furthermore, a Cochrane systematic review was also indicated that there was insufficient evidence to show the effectiveness of masks in reducing the spread of respiratory viral infection during seasonal influenza.28 These and other factors have inevitably contributed to many individuals’ less-than-optimal application of precautionary measures.28 Again, as this paper’s introduction notes, Saudis had sufficient knowledge and practice using face masks to prevent infection.8 However, in the same study, 43% of participants reported reusing the masks, and 30% reported not washing their hands after touching their face masks. Moreover, 50% did not always wash their hands after removing their masks.8
A group of participants discussed hand washing and using gloves. However, we are unaware if they were carrying out this precaution correctly. For example, the duration of their handwashing was unclear except for one interviewee who said: “We wash our hands for 20 seconds with soap” (1034). Additionally, no participant mentioned scrubbing their fingers while washing. In addition, although participants reported wearing gloves, the frequency of changing them was not reported. A few participants spoke about staying home, working remotely, and avoiding going to malls and markets. However, the majority did not strictly avoid crowds as one said “I do as much as I can” (1015). Others said, “I tried not to go out” (1040), and “if I have something important [to get], I will get it and go back home” (1046).
The findings describe that some participants followed social distancing. However, their consistency level in following social distancing and what they considered a sufficient distance to prevent contracting the virus is unknown. Only one interviewee explicitly said, “We kept [a] distance of like more than a meter” (1023). A third of the study sample spoke about using sanitizers and placing them everywhere. One participant stated, “I have a sanitizer in the office and another sanitizer in the car, and I have one in the house” (1006). They mentioned sanitizing their hands and shopping bags, but whether they sanitized surfaces, counters, and door handles remained unclear. Further, it was uncertain if they were applying hand sanitizers to fingers, fingertips, or in-between fingers.
As the introduction detailed above, the Saudi governmental health authorities and the MOH made efforts to educate the public and deliver reliable information about precautionary measures through various sources and platforms. However, reported results showed that participants were selective and inconsistent in following precautionary measures, for which a possible explanation is a lack of initiative among the public to access those guidelines. A potential reason for this is the public becoming overwhelmed by a deluge of media information, including constant updates about COVID-19 cases and deaths and ongoing changes in regulations and guidelines during the pandemic’s early stages. As a result, they were not actively seeking information about the precautions and, instead, tracking cases in their communities and neighborhoods.
Moreover, this inconsistency may be influenced by how the general Saudi population is more accustomed to using WhatsApp as their primary form of media, and the information exchanged on that platform is not always credible. Complicating this further is that while most of the public uses social media, a portion is not acquainted with technology and accessing links and videos, especially the elderly and uneducated. These explanations are supported by a study assessing the public engagement with the MOH Twitter account during the pandemic, which found that public engagement was negatively associated with including hyperlinks and multimedia files. In addition, warnings and reassurance messages received higher public engagement than educational materials.29
Finally, several study limitations need to be considered. For example, social desirability or self-enhancement bias may have confounded the study findings. Also, telephone instead of face-to-face interviews precluded our ability to capture nonverbal cues or build rapport with participants. Finally, the nature of qualitative reported experiences may not generalize to other settings or all individuals impacted by COVID-19.
Conclusion
Understanding individuals’ precautionary behavior from qualitative data gathered during the COVID-19 pandemic is critical for enhanced policymaking. The study findings can serve as evidence to consider when planning and developing effective public health communication models for behavior change, potentially reducing the transmission of COVID-19. In light of these findings, future policies must detail the implementation of the recommended public health precautionary measures to prevent as much miscommunication as possible and ensure proper execution of the measures. Although the MOH and WHO can be lauded for their early and attentive response to the emerging evidence of the precautionary measures, study participants’ reports of carrying out these measures revealed they were inconsistent and selective. For example, participants were not always using masks and were not replacing them as often as needed. It is a dosage and fidelity problem in public health. Information or knowledge is necessary, but future public health campaigns could be strengthened by modeling how the precautionary measures should be implemented.
Furthermore, public health authorities must consider strategies to disseminate the MOH’s reliable resources and enhance their accessibility by promoting them in ways tailored to the public’s media consumption habits. For example, as social media feeds constantly change, it is easy to miss informative tweets or posts if one does not actively seek official accounts of the MOH or other institutions. Finally, public health authorities should prioritize posting reliable resources in areas where they can attract ample attention, such as billboards, waiting areas, restaurant tables, and gas stations: these are locations where people actively seek something to pass the time and are thus more likely to access such information.
Data Sharing Statement
Deidentified limited dataset supporting the study findings is available upon reasonable request from the corresponding author.
Ethics Approval and Informed Consent
The ethical approval was obtained from Imam Abdulrahman bin Faisal University (IAU) Institutional Review Board (IRB), (IRB-2020-04-117), Saudi Arabia. Oral consents were obtained and audio-recorded from all study participants prior to contacting the interviews. Participants were informed about the study objectives, benefits and risk, and their voluntary participation. ID code numbers were assigned to participants to maintain their confidentiality throughout the study.
Acknowledgments
We acknowledge the contributions of Prof. Frances Marcus Lewis for her guidance throughout the study. We would also like to thank Bushra Bawazier for her assistance during the recruitment process and Noor Qaw for verifying the transcribed interviews. Finally, we would like to thank the 26 participants who were interviewed for this study.
Author Contributions
Both authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. Have written, revised, and critically reviewed the article. They also, have agreed on the chosen journal to which the article will be submitted. Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. Agree to take responsibility and be accountable for the contents of the article.
Funding
This study was funded by the Grants Program for COVID-19 of Imam Abdulrahman Bin Faisal University, projectID # (COVID19-2020-014-Nurs).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO director-general’s opening remarks at the media briefing on COVID-19 [World Health Organization]. Geneva: WHO Director-General’s Speeches; 2020. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020.
2. World Health Organization. Weekly epidemiological update on COVID-19 [World Health Organization]. Geneva: Emergency Situational Updates; 2022. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---22-june-2022.
3. World Health Organization. Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19) [World Health Organization]. Geneva: COVID-19 Infection Prevention and Control; 2020. Available from: https://www.who.int/publications/i/item/rational-use-of-personal-protective-equipment-(ppe)-for-coronavirus-disease-(covid-19).
4. World Health Organization. Advice for the public: coronavirus disease (COVID-19) [World Health Organization]. Geneva: Coronavirus disease (COVID-19); 2021. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public.
5. Ministry of Health. Saudi Arabia’s experience in health preparedness and response to COVID-19 pandemic [Ministry of Health]. Saudi Arabia: Ministry of Health (MOH) Publications; 2020. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Pages/Publications-2020-10-27-001.aspx.
6. Alshammari TM, Altebainawi AF, Alenzi KA. Importance of early precautionary actions in avoiding the spread of COVID-19: Saudi Arabia as an Example. Saudi Pharm Jl. 2020;28(7):898–9027. doi:10.1016/j.jsps.2020.05.005
7. Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis. 2020;20(5):102–107. doi:10.1016/S1473-3099(20)30129-8
8. Meo SA, Alqahtani SA, Aljedaie GM, Binmeather FS, AlRasheed RA, Albarrak RM. Face masks use and its role in restraining the spread of COVID-19 pandemic in Saudi Arabia: knowledge, attitude, and practices based cross-sectional study. Front Public Health. 2022;9:1–9.
9. Ministry of Health. MOH: call (973) Service Center for inquiries about Novel Coronavirus. Saudi Arabia: Media Centre, MOH News [Ministry of Health]; 2020. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-02-29-002.aspx.
10. Ministry of Health. MOH clarifies precautionary measures for COVID-19 home quarantine [Ministry of Health]. Saudi Arabia: Media Centre, MOH News [Ministry of Health]; 2020. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-06-19-006.aspx.
11. Almutairi AF, BaniMustafa AA, Alessa YM, Almutairi SB, Almaleh Y. Public trust and compliance with the precautionary measures against COVID-19 employed by authorities in Saudi Arabia. Risk Manag Healthc Policy. 2020;13:753–760.
12. Al-Shammary AA, Hassan SU-N, Zahra A, Algahtani FBZ, Suleiman S. Role of community-based measures in adherence to self-protective behaviors during first wave of COVID-19 pandemic in Saudi Arabia. Health Promot Perspect. 2021;11(1):69. doi:10.34172/hpp.2021.10
13. Ministry of Health. Cumulative total confirmed cases [Ministry of Health]. Saudi Arabia: COVID 19 Dashboard; 2020. Available from: https://covid19.moh.gov.sa/.
14. Abolfotouh MA, Almutairi AF, Banimustafa AA, Hagras SA, Al Jeraisy M. Behavior responses and attitude of the public to COVID-19 pandemic during movement restrictions in Saudi Arabia. Int J Gen Med. 2021;14:741–753.
15. Alahdal H, Basingab F, Alotaibi R. An analytical study on the awareness, attitude, and practice during the COVID-19 pandemic in Riyadh, Saudi Arabia. J Infect Public Health. 2020;13(10):1446–1452. doi:10.1016/j.jiph.2020.06.015
16. Alqahtani MM, Arnout BA, Fadhel FH, Sufyan NS. Risk perceptions of COVID-19 and its impact on precautionary behavior: a qualitative study. Patient Educ Couns. 2021;104(8):1860–1867. doi:10.1016/j.pec.2021.02.025
17. Siddiqui AA, Alshammary F, Amin J, et al. Knowledge and practice regarding prevention of COVID-19 among the Saudi Arabian population. Work. 2020;66(4):767–775. doi:10.3233/WOR-203223
18. Corbin JM, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory.
19. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
20. Lewis FM, Deal LW. Balancing our lives: a study of the married couple’s experience with breast cancer recurrence. Oncol Nurs Forum. 1995;22(6):943–953.
21. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J of Eval. 2006;27(2):237–246. doi:10.1177/1098214005283748
22. Al-Amer R, Ramjan L, Glew P, Darwish M, Salamonson Y. Translation of interviews from a source language to a target language: examining issues in cross-cultural health care research. J Clin Nurs. 2015;24(9–10):1151–1162. doi:10.1111/jocn.12681
23. Chen HY, Boore JR. Translation and back-translation in qualitative nursing research: methodological review. J Clin Nurs. 2010;19(1–2):234–239. doi:10.1111/j.1365-2702.2009.02896.x
24. Clark L, Birkhead AS, Fernandez C, Egger MJ. A transcription and translation protocol for sensitive cross-cultural team research. Qual Health Res. 2017;27(12):1751–1764. doi:10.1177/1049732317726761
25. Almulla HA, Lewis FM. Losing her: children’s reported concerns in the first 6 months of their mother’s breast cancer diagnosis. Cancer Nurs. 2020;43(6):514–520. doi:10.1097/NCC.0000000000000763
26. Zahlis EH, Shands ME, Lewis FM. Upping my game as a parent: attributed gains in participating in a cancer parenting program for child-rearing parents with advanced cancer. Palliat Support Care. 2020;18(3):339–345. doi:10.1017/S1478951520000103
27. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
28. Jefferson T, Del Mar C, Dooley L, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ. 2009;339:b3675. doi:10.1136/bmj.b3675
29. Alhassan FM, AlDossary SA. The Saudi Ministry of Health’s twitter communication strategies and public engagement during the COVID-19 pandemic: content analysis study. JMIR Public Health Surveill. 2021;7(7):
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics, Outcomes and Prognostic Factors for Critical Illness in Hospitalized COVID-19 Patients in Saudi Arabia: A Retrospective Cohort Study
El-Kady AM, Aldakheel FM, Allemailem KS, Almatroudi A, Dbas Alharbi R, Al Hamed H, Alsulami M, Alshehri WA, El-Ashram S, Kreys E, Mohamed K, Al-Megrin WAI, Elshabrawy HA
International Journal of General Medicine 2022, 15:6945-6963
Published Date: 31 August 2022
Epidemiological Characteristics and Outcomes Predictors for Intensive Care Unit COVID-19 Patients in Al-Madinah, Saudi Arabia. Retrospective Cohort Study
Alhoufie ST, Mumena WA, Alsharif N, Makhdoom HM, Almutawif YA, Alfarouk KO, Alharbi MZ, Aljabri K, Aljifri A
Infection and Drug Resistance 2023, 16:5573-5586
Published Date: 24 August 2023
Assessment of the Mental, Social, and Educational Impact of the COVID-19 Quarantine and Predictors: A Survey-Based- Study from Saudi Parents
Bashatah L, Aseri S, Al-Rawi MBA
Psychology Research and Behavior Management 2024, 17:317-328
Published Date: 1 February 2024
Knowledge, Attitude and Practice Toward Artificial Intelligence Among Healthcare Workers in Private Polyclinics in Jeddah, Saudi Arabia
Serbaya SH, Khan AA, Surbaya SH, Alzahrani SM
Advances in Medical Education and Practice 2024, 15:269-280
Published Date: 5 April 2024
New-Onset Hypertension Following COVID-19 Among Aseer Residents, Kingdom of Saudi Arabia; Community-Based Screening
Ali Alshaikh A, M Alyazidi HA, Mohammad Al Nuwayhidh AM, Mohammed Madkhali AM, Saleh S Alshehri A, Ali Alshahrani S, Alqarni MA, Alslatin HSMR, Hassan Alshehri M, Alsultan OHA, Aladhadhi HMS, Al-Ayedh AA, Alhumayed RS, Ghazy RM
International Journal of General Medicine 2025, 18:6469-6481
Published Date: 25 October 2025