Back to Journals » International Journal of General Medicine » Volume 15
Application of Modified Triangular Perforator Flap in Repair of Small and Medium-Sized Facial Defect
Authors Gao MZ, Xiang XJ, Xiang M
Received 8 October 2022
Accepted for publication 5 December 2022
Published 16 December 2022 Volume 2022:15 Pages 8627—8635
DOI https://doi.org/10.2147/IJGM.S392659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Luca Testarelli
Ming-Zhu Gao,1,* Xin-Jian Xiang,2,* Mei Xiang3
1Department of Plastic Surgery, First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2Department of Plastic Surgery, the Second Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Department of Cardiac Surgery, Hainan General Hospital, Haikou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mei Xiang, Department of Cardiac Surgery, Hainan General Hospital, No. 19 Xiuhua Road, Xiuying District, Haikou, 570311, People’s Republic of China, Email [email protected]
Background: We investigated the application of local perforator flap or island flap with a modified triangular to repair small and medium facial defects.
Methods: (1) Before the operation, a Doppler flowmeter was used to investigate the superficial exit point of the perforator artery. The length to breadth ratio of the flap was more than 3– 4 times, and it contained 1– 2 perforator vessels. (2) The lesion was excised, and the skin was cut along the design line of the flap. The flap was separated and trimmed based on the defect degree. (3) The blood supply was confirmed, and the defect was then covered with the flap by “rotation and advancement” approach without causing tension. The incision was finally sutured in layers. (4) Postoperative routine care was performed according to the situation.
Results: The functional morphology and appearance of all 23 cases of skin flaps successfully recovered during follow-up. There was no major aesthetic and malformation recorded.
Conclusion: In summary, the modified triangular perforator flap can improve the functional appearance at the repaired small and medium facial defects.
Keywords: local flaps, modified triangular perforator flap, skin lesion, facial defect, postoperative care
Introduction
Excision of trauma scar, infection, superficial tumor, and giant pigmented nevus often leaves skin and soft tissue abnormalities. The primary method used for plastic and aesthetic repair is the use of a local pedicled skin flap. In contrast with skin grafting, remote skin flap and free skin flap have a simple operation with satisfactory postoperative results.1 Local pedicled flaps have been designed and applied in numerous scenarios,2 including V-Y flaps, Z-shaped flaps, Limberg flaps, and multilobed flaps. Perforator flaps have been extensively applied in clinical practice.3 Notably, triangular perforator flap is a modified design based on a V-Y flap, shaped like a buffalo horn with several benefits in the repair of defect wounds. O ‘Donnell et al4 proposed a triangular perforator in 1992 that was mainly applied to repair facial wound defects. Different sizes of triangular perforator flaps were designed as per the location and scope of soft tissue defect to repair the tissue defects of the calf, foot in our previous research.5–8 To achieve better therapeutic effect, we further modified the triangular flap. A huge modified triangular perforator valve (accounting for more than 1/2 of the middle and lower face), was prepared which successfully repaired large defects in several cases.9 Further, the modified triangular flap was applied to patients with small- and middle-size facial defects. In this paper, we aim to introduce a small and medium-sized modified triangular perforator flap or island flap with perforator pedicles which is used to repair facial deformities.
Materials and Methods
Clinical Data
A total of 23 patients with facial defects treated in the Plastic Surgery Department of the First Affiliated Hospital of Anhui Medical University between 2016 and 2021 were enrolled in this study. None of the patients had significant contraindications for surgery. The defects were caused by squamous cell carcinoma in 5 cases, basal cell carcinoma in 8 cases, pigmented nevus in 9 cases, and papilloma in 1 case. The defect area was 0.5 cm*1.5 cm ~ 3.0 cm*3.0 cm.
Surgical Methods
Modified Triangular Perforator Flap Design
Before surgery, a Doppler flow analyzer was used to assess the position and number of marked superficial outlet points of the perforating artery. The width of the defect was regarded as the top of the flap, and its length was 3–4 times higher than the defect length. The incision was designed along the skin Langer line or the existing skin fold line, and the flap contained 1–2 perforating vessels.6
Anatomy of Modified Triangular Perforator Flap
Based on the lesion nature, 2–3 mm of the tissue extending from the benign lesions was removed. Resection of the extended tissue ensured no residual cancer cells were left at the resection margin and base. The skin was cut along the design line of the flap, deep as the superficial layer of superficial muscular aponeurotic system (SMAS). The subcutaneous tissue was clearly separated from the periphery of the perforator vessels, and the subcutaneous fibrous tissue pedicled around the perforator vessels was used for blunt separation. Care was taken to prevent injury to the perforator vessels and facilitate venous and lymphatic reflux of the flap. The fat tissue under the flap was appropriately thinned with a small flap area. The flap was separated from both ends of the flap to the center to enable its pedicle could carry as little fibrous tissue as possible, and allow more freedom during rotation and advancement of the flap. First, the wound tissue edge was stitched, the wound surface was reduced, and damage to the blood supply was checked. Subsequently, the flap was directly separated under the fascia of SMAS to release the soft tissue if there was tension or limitation on the wound surface of the defect at a certain point. Care was taken to avoid injury to the facial nerve injury during surgery.
Transfer of Modified Triangular Perforator Flap
After preparation of the flap, we confirmed that the blood supply to the flap cutting edge was intact; the defect wound surface was then covered by rotation and advancement of the flap without causing tension. The wound was then sutured in layers. When subcuticular suturing, atraumatic sharp needles were applied to minimize the injury of tissue. The epidermis was sutured with a 6–0 or 7–0 cosmetic suture, the donor site was slightly and subcutaneously separated, and the wound surface was appropriately pressurized. A subcutaneous drainage sheet was placed on the wound surface to prevent infections.
Postoperative Care
Postoperative care was conducted as follows. The drain was removed 24–72 hours after surgery, whereas the stitches were removed 7–10 days after surgery. Appropriate antibiotics were administered if the wound was infected after surgery. Generally, healthy young patients were treated during outpatient follow-up, whereas elderly patients or those with underlying diseases were hospitalized.
Results
Table 1 shows the basic information of enrolled patients. All the 23 cases of flaps survived after surgery, and the postoperative follow-up displayed satisfactory functional morphology and appearance recovery. There was no infection, cancer recurrence, displacement and deformity of facial organs. Likert 5-point scale was adopted to evaluate patient satisfaction, which contains 1–5 points. Blinded evaluation was conducted by an independent nurse, who asked the question: “How do you rate the outcome of your facial operation?” to the patients. Patients were required to give a number to indicate their satisfaction level 6 months postoperatively, as follows: 1 point (Poor), 2 point (Average), 3 point (Good), 4 point (Very good), 5 point (Beyond expectations). The proportion of patients who gave the same point was calculated. Postoperative follow-up showed high patient satisfaction. The statistical data of patient satisfaction levels are shown in Table 2 (6 months postoperatively).
 |
Table 1 Clinical and Demographics of Patients in This Study |
 |
Table 2 Patient Satisfaction Survey (6 Months Postoperatively) |
Case 1
A 62-year-old female patient had a tumor of more than 1 year in the right inner canthus region, which gradually increased in size in the last 2 months, presenting with surface ulceration and affecting vision. The patient was considered to have basal cell carcinoma (BCC). She was informed of the procedure, and enlarged lesions resection was performed in the outpatient department. During the operation, the upper and lower eyelid canthus were involved. The repair was performed through rotation and advancement of the modified triangular perforator flap. The flap successfully survived after surgery, and the postoperative pathological report was BCC. Besides, no residual cancer cells were found at the cutting edge. The functional morphology was satisfactory after 6 months of follow-up, there was no deformation of the inner canthus, and the visual acuity was normal (Figure 1).
 |
Figure 1 (A) Preoperative flap design for the 62-year-old female patient with a tumor in the inner canthus region slightly increased with irregular protrusions (2.0×2.4 cm). (B). Extended resection of the tumor with the defect wound, and the flap outline was incised. (C) The flap was lifted to visualize the pedicle of the perforator. (D) The wound was covered by the flap and sutured. (E) Postoperative follow-up at 7 days and complete survival of the flap. (F) Postoperative follow-up at 6 months and desired facial appearance. |
Case 2
A 23-year-old female patient presented with symptoms of pigmented nevus near the anterior nostril margin of the left alar that had recently grown in size and had an aesthetic impact, necessitating surgical resection. After outpatient examination, the patient was informed about the resection and agreed to the suggested repair plan by signing the informed consent form. The patient was operated in the outpatient operating room. A modified triangular perforator valve was designed along the nasolabial groove, and the perforator vessels of the alar base were used as the pedicle to repair the defect. After the operation, the flap was completely alive with a satisfactory appearance. Postoperative pathology displayed complex nevus (Figure 2).
 |
Figure 2 (A) Preoperative flap design for the 23-year-old female patient with a pigmented nevus near the anterior nostril margin (0.8×1.0 cm). (B) Postoperative follow-up at 7 days. (C) Postoperative follow-up at 1 month. |
Case 3
A 24-year-old male presented with an irregular lobulated skin lesion of 0.5cm * 1.5cm protruding at the right anterior nostril edge. Postoperative scar contracture would reduce the nostril, and both sides of the nostril would be asymmetric if laser cauterization was used to remove the mass. To avoid these outcomes, we proposed the modified triangular perforator flap. The patient signed informed consent preoperatively, the modified triangular flap was designed in the vestibular vault to repair the defect. Postoperative pathology suggested papilloma (Figure 3).
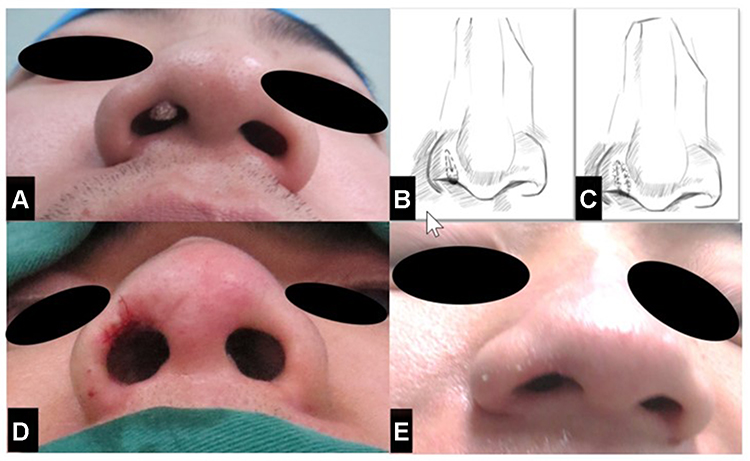 |
Figure 3 (A) The 24-year-old male patient with an irregular lobulated skin lesion (0.5×1.5 cm). (B). Surgical design Diagram 1. (C) Surgical design Diagram 2. (D) Postoperative follow-up at 7 days. (E). Postoperative follow-up at 6 months and complete survival of the flap. |
Case 4
A 56-year-old female patient had a lesion in the upper eyelid under the right eyebrow for 3 months. The lesion surface was ulcerated and did not heal. The patient was considered to have BCC and was in good health. We designed a modified triangular flap with the supratrochlear artery as the perforator vessel. Postoperative pathological findings suggested BCC, and there were no residual cancer cells at the cutting edge. The patient reported satisfactory postoperative recovery during follow-up (Figure 4).
 |
Figure 4 (A). Preoperative flap design for the 56-year-old female patient had a mass in the upper eyelid under the right eyebrow (2.0×2.0 cm). (B) Extended resection for the lesion and the flap outline was incised. (C) The immediate postoperative. (D) Postoperative follow-up at 7 days and complete survival of the flap. |
Case 5
A 36-year-old female patient presented with a pigmented lesion and a sulcus of the left cheek. The patient was informed about the modified triangular pedicled flap procedure and signed informed consent. Enlarged lesion resection was performed in the outpatient operating room. The nasal and labial sulcus perforator modified triangular pedicled flap was designed to be repaired by rotation and advancement with the facial artery as the source vessel. The flap completely survived after the operation, and functional appearance was satisfactory. The postoperative pathological report showed pigmented BCC (Figure 5).
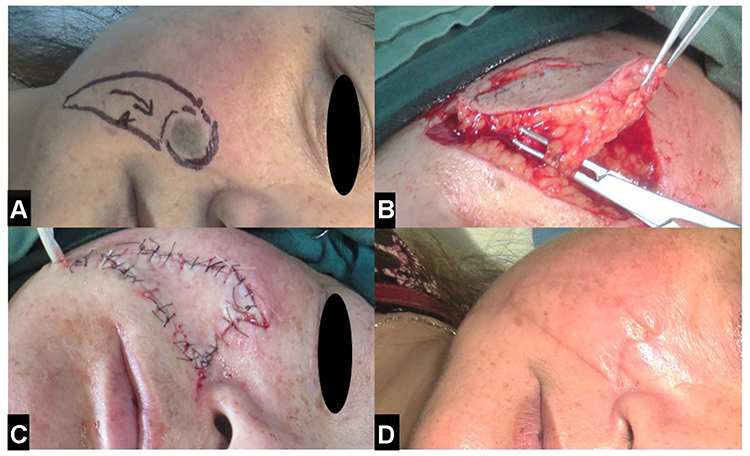 |
Figure 5 (A) Preoperative flap design for the 36-year-old female patient presented with a pigmented lesion beside the sulcus of the left cheek (2.0×2.5 cm). (B) Extended resection for the lesion and the flap outline was incised. The flap was lifted to observe the pedicle of the perforator. (C) The immediate postoperative. (D) Postoperative follow-up at 6 months and complete survival of the flap. |
Case 6
A 42-year-old man had a pigmented mass on the left alar of the nose, that had greatly enlarged and ulcerated with bleeding fluid outflow. The patient was considered to have BCC. The patient was informed about the modified triangular pedicled flap procedure and signed informed consent. The nasal alar base of the nasolabial groove was used as the perforating pedicle, which appeared like an ox horn island flap. The defect was transferred to the alar defect area through a loose subcutaneous tunnel (the defect base was alar cartilage surface). The flap completely survived after the operation, and the pathological report suggested BCC. There was no cancer recurrence and the functional function was satisfactory after the 6 months of follow-up (Figure 6).
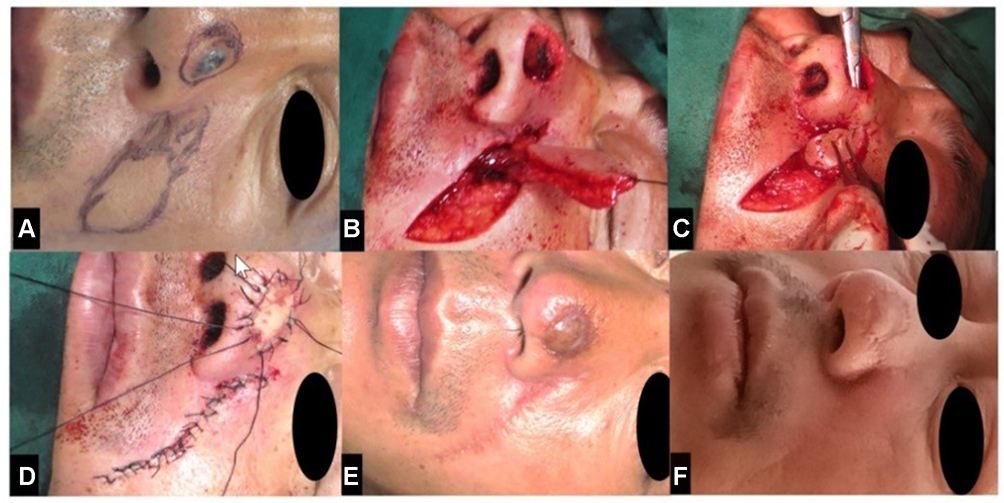 |
Figure 6 (A) Preoperative flap design for the 42-year-old man presented with a pigmented mass on the left alar of the nose, that had markedly enlarged and ulcerated (1.0×1.5 cm). (B). The flap was lifted to observe the pedicle of perforator vessels. (C) The flap was trailed through a subcutaneous tunnel. (D). The immediate postoperative. (E) Postoperative follow-up at 7 days and complete survival of the flap. (F) Postoperative follow-up at 6 months and good facial appearance. |
Discussion
For facial defects caused by trauma facial mass, tumor resection, or other reasons, a small area can extend the wound and directly stitch it, or free skin grafting can be used to cover it. However, the formation of postoperative scar influences the functional appearance.10 The modified triangular flap has a flexible design, and branches and perforators of blood vessels provide blood supply to the flap. In the present study, we used the modified triangular flaps to repair various tissue defects in different parts of the body and achieved good clinical results.6–8 After a long-term follow-up, we observed that all the modified triangular perforator flaps survived, and the morphology, as well as appearance of the face, were satisfactorily restored. Moreover, local cosmetic subunits were efficiently retained or reconstructed. Moreover, postoperative recovery was quick with good satisfaction. As shown in case 3, the lesion was located in the cosmetic subunit of the nose alar and involved the edge of the anterior nostril. A small modified triangular flap was designed on the inner and outer sides to rotate and push forward to ensure that the alar nose and the anterior nostril were symmetrical. This was aimed at complementing the deficiency of nose alar and achieving satisfactory cosmetic results, which cannot be achieved by other reconstructive surgery methods.
The advantages of the modified triangular perforator flap include: (1) The flap was designed as a modified triangular flap with anterior and concave sides, which was advanced and easily rotated. Unlike the simple V-Y flap, the modified triangular flap had cambered side edges, allowing long-distance and greater freedom. The proximal horn-type flap was wider, with two arc-shaped sides divided into concave and convex lateral sides. The convex side was longer, and the position of perforators was selected as the pivot. With propulsion, the concave side was given prominence, covering the wound. A Y-shaped suture was used to seal the donor site, reducing the tension of the flap. As a result, the repair range correspondingly increased, and the linear scar contracture deformity was reduced. (2) Because the modified triangular flap’s donor site forms a narrow and long horn shape, it can be directly closed without skin transplantation or additional donor site injury. (3) For facial defects and other exposed parts, postoperative flaps were close to the local normal skin color. Therefore, although the flap operation causes auxiliary incision, compared with other reconstructive surgery methods, including the dermatoplasty and composite graft, its general postoperative evaluation is good. (4) Small and medium-sized defects can be surgically treated in the outpatient department. Postoperative care is relatively simple and acceptable, making it widely applied even in partially underdeveloped areas.
The facial artery and its branches primarily supply most regions of the face.11–16 Additionally, other blood vessels communicate with each other in the head and face forming a network. Many perforator flaps can be freely designed as the anatomic basis of blood supply to the perforator flaps based on the assumption of multi-source blood supply to the face.17–19 Anatomical analysis demonstrated that, although the pedicle flap eliminated the well-known blood vessels, the aspect ratio was higher than that produced by conventional random flap in design.20 The mechanism of its survival may include: (1) The anatomical basis for its life is may be the highly rich vascular nets and pedicle vascular in each layer of the face. (2) The pedicle blood perfusion pressure was high. Studies have shown that the survival of skin flap is closely related to pedicle vascular perfusion pressure. The face and head are close to the heart, hence have a high pedicle blood vessel perfusion pressure.
The major points to be noted during surgical application include: (1) Before surgery, a Doppler ultrasonography blood flow detector should be utilized to detect the perforating arteries of the surrounding skin, and the flap should have at least 1–2 perforating vessels. To prevent injury to the perforator vessel, a blunt separation should be adopted while separating the flap near it. (2) The design head width of the perforator flap should be slightly larger than the width of the defect, and the length should be about 3–4 times that of the defect. The end of the flap should be designed to be narrow to allow direct suturing without trimming; (3) When cutting the skin, the concave side of the modified triangular fascial flap should only be applied for skin and subcutaneous tissues, whereas the convex side should be used for the superficial layer of SMAS. The convex side is longer, and the position of perforators is selected as the pivot. Therefore, the skin should be cut to near the superficial layer of SMAS to reduce risk of vascular injury. The thinner tissue in the concave side allows better propulsion when covering the wound. Thus, the concave side of the flap should only be cut up to the skin and subcutaneous tissue level. If the flap develops tension limit during rotation, it can extend to underneath the SMAS causing soft tissue release. This will prevent damage to the facial nerve branches. Local excess skin is common when the flap head has a cup-shaped defect. Due to a lack of blood flow, it is frequently removed in traditional surgical methods. The excess skin inserted to the defect side can be used to maximize the amount of tissue available and relieve local tension in the modified triangular perforator flap. (4) The end of the flap in the canthus should be tightly fixed with the deep ligament and periosteum during the eyelid procedure to prevent flap relaxation and eyelid ectropion. (5) Intraoperative hemostasis should be conducted thoroughly, however, the frequent use of intraoperative electrocoagulation should be reduced to prevent fat liquefaction in subcutaneous wounds, which can potentially affect the wound-healing process. Drainage tablets can be placed after the surgery, and the incision should be properly pressurized and bandaged. (6) Postoperative head height rest position was used to minimize postoperative flap swelling and promote venous reflux; the drainage strip was removed based on the circumstances. Limitations: All skin flap grafting operations may cause donor site scar, which may lead to discontent. Less stress may reduce but not avoid the possibility of scar hypertrophy. Moreover, the delicate operation on the vessels requires vast experience, and this may limit the application of this technique.
Conclusion
In conclusion, the cases presented in this study demonstrate that the modified triangular perforator flap repairs small- and medium-sized face defects, resulting in a more natural and beautiful appearance. The flap has the advantage of maintaining facial subunits.
Abbreviations
SMAS, Superficial Muscular Aponeurotic System; BCC, basal cell carcinoma.
Ethics Approval and Consent to Participate
Informed consent was obtained from all individual participants included in the study. The study protocol was approved by the ethics committee of First Affiliated Hospital of Anhui Medical University. Reference number: Quick-PJ 2022-4-41.
Consent Statement
All the patients in the case had been informed via written consent, which approved the publishment of the personal details and images.
Acknowledgments
The authors would like to sincerely thank Jin-loqng Ning for valuable guidance in our study. Major contribution of this paper is from the Department of Cardiac Surgery, Hainan General Hospital. Ming-Zhu Gao and Xin-Jian Xiang are co-first authors for this study.
Funding
This study received no external funding.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Ganry L, Ettinger KS, Rougier G, et al. Revisiting the temporal artery posterior auricular skin flap with an anatomical basis stepwise pedicle dissection for use in targeted facial subunit reconstruction. Head Neck. 2020;42(11):3153–3160. doi:10.1002/hed.26362
2. Larrabee WF. Design of local skin flaps. Otolaryngol Clin North Am. 1990;23(5):899–923. doi:10.1016/S0030-6665(20)31217-2
3. Stepanov IUI. Perforator dlia kozhnykh transplantatov [Perforator for skin transplants]. Khirurgiia. 1980;(7):87. Russian.
4. Georgeu GA, EL-MUTTARDI N. The horn shaped fascio-cutaneous flap usage in cutaneous malignancy of the leg. Br J Plast Surg. 2004;57(1):66–76. doi:10.1016/j.bjps.2003.10.013
5. Li XY, Li XJ, Ning JL, et al. Application of foot Angle perforator flap to repair the defect of heel and anterior plantar base. J Plast Surg. 2013;5:29. Chinese.
6. Ma DM, LI XJ, Ning JL, et al. Anatomical basis and clinical application of angular perforator flap pedicled with inner canthus artery. J Plast Surg. 2015;4:31. Chinese.
7. Ma LI, Xiaojing LI, Jinlong Ning, et al. Clinical application of leg angular perforator fascial flap. J Plast Surg. 2011;5:27. Chinese.
8. Yao WD, Li XJ, Ning JL, et al. Clinical application of adjacent angular perforator fascial flap in the trunk. Chin J Plast Surg. 2014;4:30. Chinese.
9. Weng XJ, Li XJ. Reconstruction of large facial malignant tumor defects using local angular perforator flap. J Craniofac Surg. 2019;30(4):1268–1269. doi:10.1097/SCS.0000000000005276
10. Kohlhauser M, Luze H, Nischwitz SP, et al. Historical evolution of skin grafting-A journey through time. Medicina. 2021;57(4):348. doi:10.3390/medicina57040348
11. Nakajima H, Imanishi N, Aiso S. Facial artery in the upper lip and nose: anatomy and a clinical application. Plast Reconstr Surg. 2002;109(3):855–61; discussion 62–3. doi:10.1097/00006534-200203000-00003
12. Loukas M, Hullett J, Louis RG, et al. A detailed observation of variations of the facial artery, with emphasis on the superior labial artery. Surg Radiol Anat. 2006;28(3):316–324. doi:10.1007/s00276-006-0093-0
13. Larrabee WF, Makielski KH, Henderson JL. Surgical Anatomy of the Face. Philadelphia: Lippincott Williams and Wilkins; 2004:58–105.
14. Erian A, Shiffman MA. Facial anatomy. In: Advanced Surgical Facial Rejuvenation: Art and Clinical PracticeBerlin. Springer; 2012:3–14.
15. Wobig JL, Dailey JWFacial anatomy. In: Oculofacial Plastic Surgery: Face, Lacrimal System. New York: Thieme. 2004:3–10.
16. Janfaza P. Surgical Anatomy of the Head and Neck. Philadelphia: Saunders Elsevier; 2009.
17. Drake R, Vogl AW, Mitchell AW. Gray’s Anatomy.
18. Gileva KS, Gazimagomedova AR, Topografo-anatomicheskoe i klinicheskoe obosnovanie primeneniya perforantnogo krovosnabzhaemogo loskuta s periaurikulyarnoi oblasti iz basseina poverkhnostnoi visochnoi arterii [Anatomical and clinical rationale for the use of a perforant flap from the periauricular region the blood-supplied from pool of the superficial temporal artery]. Khirurgiia. 2021;5:78–88. Russian. doi:10.17116/hirurgia202105178
19. Marur T, Tuna Y, Demirci S. Facial anatomy. Clin Dermatol. 2014;32(1):14–23. doi:10.1016/j.clindermatol.2013.05.022
20. Lucas JB. The physiology and biomechanics of skin flaps. Facial Plast Surg Clin North Am. 2017;25(3):303–311. doi:10.1016/j.fsc.2017.03.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.