Back to Journals » Journal of Pain Research » Volume 18
Application of Intraoperative Awake Anesthesia and Three-Dimensional Reconstruction Technique in Percutaneous Microballoon Compression for Trigeminal Neuralgia
Authors Li X ![]() , Fan Y
, Fan Y ![]() , Chen Z
, Chen Z ![]() , Hui OY, Guo M
, Hui OY, Guo M ![]() , Feng G, Zhou J, Ling Y
, Feng G, Zhou J, Ling Y ![]() , Lin D
, Lin D ![]()
Received 24 April 2025
Accepted for publication 8 September 2025
Published 16 September 2025 Volume 2025:18 Pages 4833—4843
DOI https://doi.org/10.2147/JPR.S534449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jinlei Li
Video abstract of “Awake Anesthesia and 3D Technique in Trigeminal Neuralgia” [534449]
Views: 126
Xingke Li,1,2 Yanfeng Fan,1– 3 Ziyang Chen,1– 3 Ou-Yang Hui,1– 3 Min Guo,1– 3 Guili Feng,1– 3 Jianzhi Zhou,1– 3 Yuhui Ling,1– 3 Deliu Lin1– 3
1Department of Neurosurgery, Guangdong Sanjiu Brain Hospital, Guangzhou, People’s Republic of China; 2Institute of Clinical Teaching Center, Jinan University, Guangzhou, People’s Republic of China; 3Institute for Brain Research and Rehabilitation, South China Normal University, Guangzhou, People’s Republic of China
Correspondence: Deliu Lin, Email [email protected]
Objective: To examine the role of intraoperative awake anesthesia and the three-dimensional reconstruction technique in percutaneous microballoon compression (PBC) for the treatment of trigeminal neuralgia.
Methods: Seventy patients diagnosed with trigeminal neuralgia and admitted to Guangdong Sanjiu Brain Hospital from 2019 to 2022 were selected for the study.All patients were treated with PBC by three-dimensional (3D) reconstruction of preoperative and intraoperative images and intraoperative awake anesthesia. The duration of balloon compression during surgery was three minutes.After balloon compression during the procedure, the patient is awakened for effect assessment, allowing for real-time adjustments of the surgical strategy based on the evaluation.Postoperative pain relief was evaluated using the Brisman criteria.
Results: Pain completely disappeared immediately post-operation in 68 patients, and was significantly alleviated in two patients, with an efficacy rate of 100% and a cure rate of 97.1%. 60 patients experienced facial numbness on the affected side postoperatively, which showed different degrees of remission or disappearance within 6– 12 months after surgery. Eleven cases of herpes labialis (15.7%), one case of facial hematoma (1.4%), and three cases of postoperative psychiatric symptoms (4.3%) occurred, all of which recovered within 1– 2 weeks after surgery. Weakness in the masticatory muscles on the affected side was observed in four patients (5.7%), and all cases returned to normal within six months post-surgery.During follow-up 36– 60 months, there were five cases (7.1%) of pain recurrence on the affected side.
Conclusion: Awake anesthesia combined with 3D reconstruction technology for PBC surgery may provide a safer and more effective alternative for the treatment of trigeminal neuralgia.
Keywords: trigeminal neuralgia, awake anesthesia, three-dimensional reconstruction, microballoon compression
Introduction
Trigeminal neuralgia (TN) is primarily characterized by transient and episodic severe pain in the innervated area of the trigeminal nerve. The nature of the pain varies, presenting as electric shock-like, stabbing, cutting, or burning sensations, which seriously affect patients’ quality of life, as well as their ability to study and work.1 In the early stages of the disease, oral medications are typically prescribed for treatment.2 However, surgery is often required eventually due to drug resistance and side effects.3,4
Percutaneous microballoon compression (PBC) is currently a more commonly used minimally invasive surgical method for the treatment of TN. This technique was proposed by Mullan et al in 1983.5 PBC offers several advantages, including simplicity of operation, minimally invasive nature, low cost, painlessness under general anesthesia, and high reproducibility.6,7 For elderly and frail patients, individuals with refractory recurrent pain, individuals who are resistant or unable to tolerate craniotomy, or patients experiencing recurrence after microvascular decompression (MVD), PBC may be considered as the preferred surgical treatment option.8
After nearly four decades of clinical practice,various studies have reported PBC postoperative complications, such as hypoesthesia or paresthesia on the operated side, masticatory muscle weakness, corneal hyporeflexia, abducens nerve palsy, and intracerebral hemorrhage.6 The occurrence of these complications is closely related to the puncture site, direction, depth, specific position, size, compression time of the balloon.6 Therefore, the process of intraoperative puncture and the control of the balloon position, shape, size, and compression time are particularly important when conducting the PBC procedure. Moreover, TN is a condition characterized by subjective symptoms, and the degree of pain and relief cannot be quantified objectively. When the operation is performed under general anesthesia, the subjective feelings of the patient cannot be known to change, and the effect of the operation cannot be evaluated. Local anaesthesia does not completely resolve the severe pain generated when the puncture needle enters the trigeminal semilunar ganglion and balloon dilatation.Additionally, the patient’s anxiety, tension, and fear regarding the surgery can lead to discomfort during the procedure, hindering their cooperation and potentially causing fluctuations in blood pressure and heart rate, which negatively impacts the safety and effectiveness of the surgery.
This study presents a modified PBC surgical technique that integrates intraoperative awake anesthesia with 3D reconstruction. Preoperative and intraoperative use of 3D reconstruction technology ensures successful puncture, precise balloon positioning, and satisfactory shaping. During surgery, assisted by awake anesthesia, communication with the patient is maintained to confirm the surgical outcome. This modified surgical approach was applied to treat 70 cases of TN. Clinical insights are summarized with the aim of exploring a safer and more effective adjunct method for PBC surgery, with the hope of further promoting its utilization.
Materials and Methods
Clinical Data
Basic Information
Seventy patients with trigeminal neuralgia (TN) were admitted to our center from January 2019 to March 2022, Inclusion criteria:classical TN and secondary TN, diagnosed according to the International Classification of Headache Disorders, 3rd edition (ICHD-3, 2018). Exclusion criteria: secondary TN (tumor and multiple sclerosis).Patients’ characteristics are presented in Table 1.
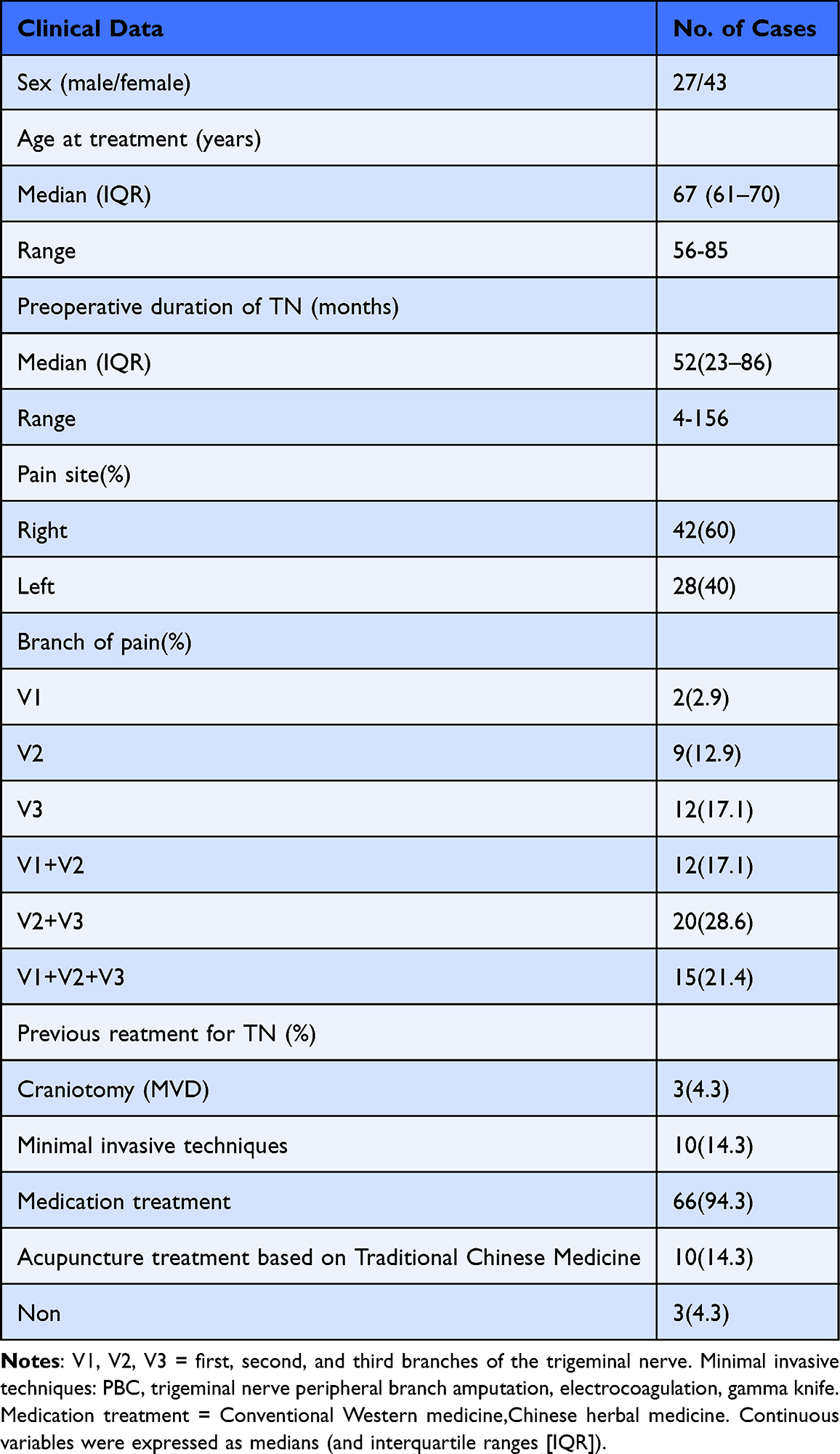 |
Table 1 Patient Characteristics of 70 Patients Undergoing PBCs |
Radiological Examination
Preoperative three-dimensional computed tomography (CT) was conducted for image reconstruction (Philips 64-layer CT, the scanning layer thickness is set at 0.75–1mm. The Extended BrillianceTM workstation software is used for three-dimensional reconstruction of skull, which can be completed within a few minutes with simple operation). Following skull reconstruction, the size of the foramen ovale was measured (Figure 1A and B), as well as the distance from the foramen ovale to the trigeminal foramen (Figure 1C), and the depth of the foramen ovale (Figure 1D). In 70 cases, the short diameter of the foramen ovale ranged from 2.1 mm to 6.5 mm, with an median of 3.8 mm (interquartile range [IQR] 3.1–4.8mm); the long diameter ranged from 4.2 mm to 11.8 mm, with an median of 5.6 mm (IQR 4.9–6.1mm). The largest foramen measured 6.5 mm × 11.8 mm, while the smallest was 2.1 mm × 4.2 mm.
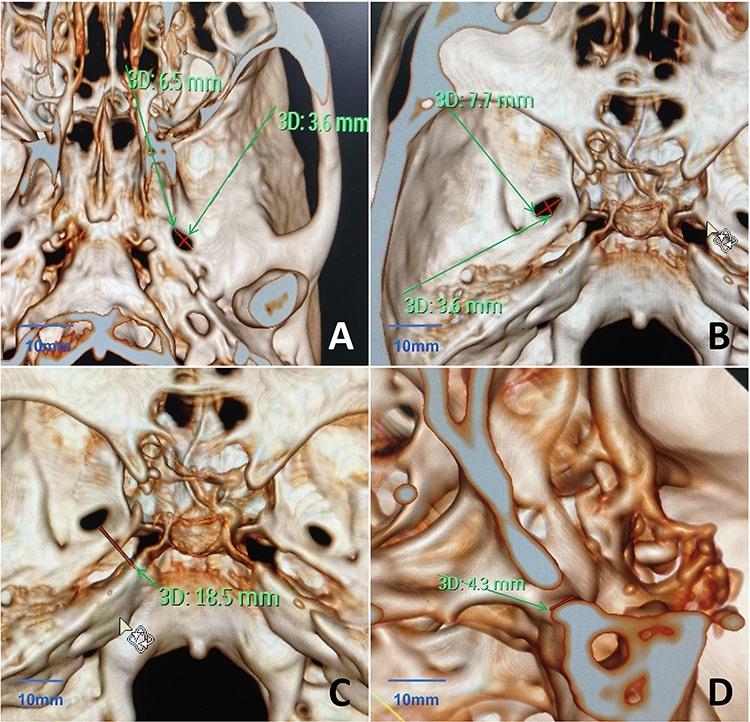 |
Figure 1 Preoperative CT 3D reconstruction to understand the skull base and foramen ovale. (A) Long and short diameters of the extracranial foramen ovale(redline). (B) Long and short diameters of the intracranial foramen ovale(redline). (C) Distance from the foramen ovale to the trigeminal nerve foramen(redline). (D) Depth of the foramen ovale(redline).The red line indicated by the green arrow represents the measured length.Scale bar,10mm. |
Surgical Methods-The Same Surgical Approach Was Applied to All Patients
Preoperative Preparation
Patients were instructed to fast for six hours prior to the procedure. After the induction of general anesthesia, the patient was positioned supine with the head slightly tilted back, approximately 10–15 degrees.
Anesthesia Implementation Details
Remifentanil was administered intravenously at a dose of 0.8–1.2μg/kg. Muscle relaxant: Rocuronium was injected intravenously at a dose of 0.6–1.0mg/kg. Anesthetic: Cyclopropylphenol was administered intravenously at a dose of 0.4–0.6mg/kg. For elderly, frail patients, or those classified as ASA III–IV, the dosage should be reduced to 0.2–0.4mg/kg, with slow administration (over approximately 10 seconds). Following rapid sequence induction, tracheal intubation, and mechanical ventilation, intraoperative maintenance involved continuous infusion of Remifentanil at a rate of [1.2–12μg/(kg·h)] and Cyclopropylphenol at a rate of [0.4–0.6 mg/(kg·h)], without the use of muscle relaxants. The dosage of maintenance anesthetics was adjusted based on changes in vital sign monitoring. All maintenance anesthetics were discontinued three minutes after successful puncture, balloon formation, and compression of the trigeminal ganglion. Awakening generally occurs within 10–15minutes.The duration of anesthesia required throughout the surgical procedure is approximately 25 to 30 minutes.
Puncture Site
The Hartel anterior approach was utilized for the puncture. The puncture site was situated approximately 2.5cm lateral to the corner of the mouth on the affected side. Two additional reference points were identified: approximately 0.5cm below the ipsilateral pupil and approximately 3cm anterior to the external auditory canal at the level of the zygomatic arch.
Puncture Procedure
A CTZ-14 gauge puncture needle from Qinyuan Company, Shenzhen, was utilized for the puncture. Under fluoroscopic guidance from a dual C-arm digital subtraction angiography (DSA) X-ray machine by GE, USA, the puncture needle was directed into the foramen ovale. 3D reconstruction of the skull base was performed using the DSA X-ray machine to confirm the positioning of the puncture needle at the foramen ovale when necessary (Using the integrated InSpace 3D software,The voxel size is in the range of 0.1–1 mm).
Balloon Formation and Compression Process
The stylet of the puncture needle was removed, and a No.5 balloon catheter was inserted into the Meckel’s cave. Subsequently, 0.2–0.4 mL of contrast agent was injected into the balloon cavity. 3D reconstruction using the DSA X-ray machine was performed to confirm the positioning of the balloon within Meckel’s cave when necessary. Then, additional contrast agent was injected into the balloon until it achieved an ideal pear shape (Figure 2A). A comprehensive 3D reconstruction was performed to confirm the shape of the balloon (Figure 2B). The volume of contrast agent injected into the balloon ranged from approximately 0.45 mL to 1.0 mL, and the compression time of the balloon was approximately three minutes.
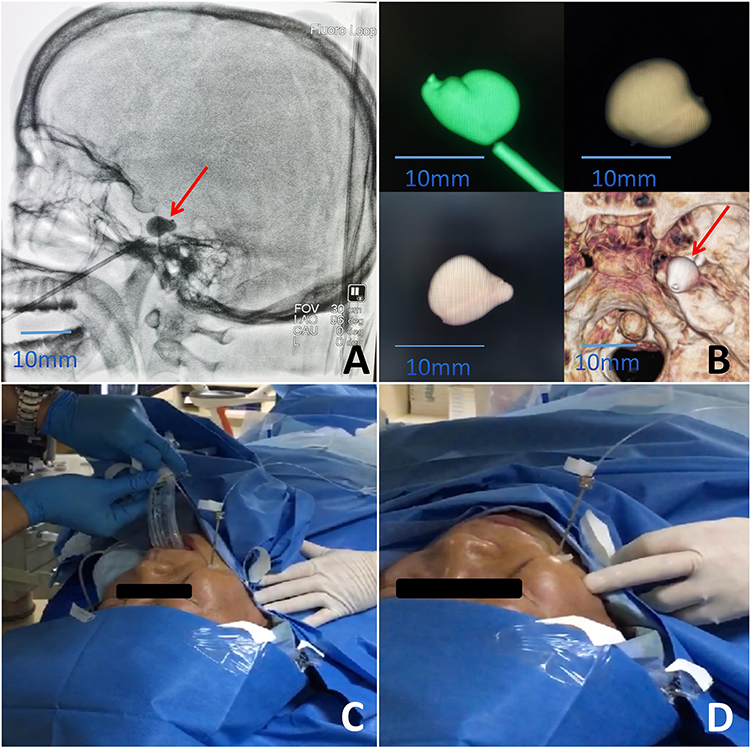 |
Figure 2 Intraoperative 3D reconstruction of the balloon and awake anesthesia process. (A) Balloon shape under lateral fluoroscopy. (B) Balloon shape after 3D reconstruction. (C) Removal of the laryngeal mask, awakening the patient during surgery. (D) Communication with the patient, touching the trigger points, inquiring about any occurrence of pain, hypoesthesia, and numbness on the affected side.Scale bar,10mm. |
The intraoperative anesthesia awakening process
Under the supervision of an anesthesiologist, the patient was awakened during the procedure. Meanwhile, the laryngeal mask was removed, while the puncture needle remained in place (Figure 2C), and communication with the patient was initiated. For patients exhibiting obvious trigger points preoperatively, stimulation of these trigger points and touching the area of preoperative pain onset (Figure 2D) were performed. Patients were asked whether they experienced numbness or pain on the affected side. For patients without obvious trigger points preoperatively, both the affected and unaffected sides were touched, and the patient was asked to compare the sensation between the two sides, particularly noting any reduction in sensation or numbness on the affected side. If pain was not triggered or if numbness was evident on the affected side, the surgery could be concluded. If the patient still experienced pain or lacked numbness, the balloon catheter could be readjusted in terms of size and shape, followed by an additional compression period of 30 seconds to 3 minutes. Communication with the patient was resumed after achieving the desired effect. Upon achieving the desired outcome, the puncture needle was withdrawn, pressure was applied to the puncture site for a few minutes, and sterile dressings were applied. The patient was observed for any complications, such as impaired eye movement or conjunctival congestion on the affected side.
Postoperative Outcome Assessment
Postoperatively, the degree of pain relief was assessed using the Brisman standard.9 (Complete cure: no pain and no medicine; Significant efficacy: pain relief rate >90%, occasional medication still required).The pain relief rate was calculated using the Visual Analogue Scale (VAS) scores: the preoperative VAS score minus the postoperative VAS score, divided by the preoperative score. The resulting value represents the relief rate.
Results
Intraoperative Observation
With the assistance of 3D reconstruction, successful puncture of the foramen ovale was achieved in all patients, with the balloon catheter fully entering Meckel’s cave. Awake anesthesia was successfully administered to all patients intraoperatively. Among the patients, 69 cases exhibited a pear-shaped or pear-like morphology of the balloon (Figure 3A and B), while one case presented with a peanut-like morphology (Figure 3C).Upon awakening from anesthesia, six patients reported that they were still experiencing pain symptoms. Consequently, the balloon was reinflated to maintain compression on the trigeminal ganglion. The compression was sustained for 60 seconds in four patients and 90 seconds in two patients,following which the pain symptoms subsided. Intraoperatively,the median balloon volume was 0.59mL (IQR 4.6–7.1mL).
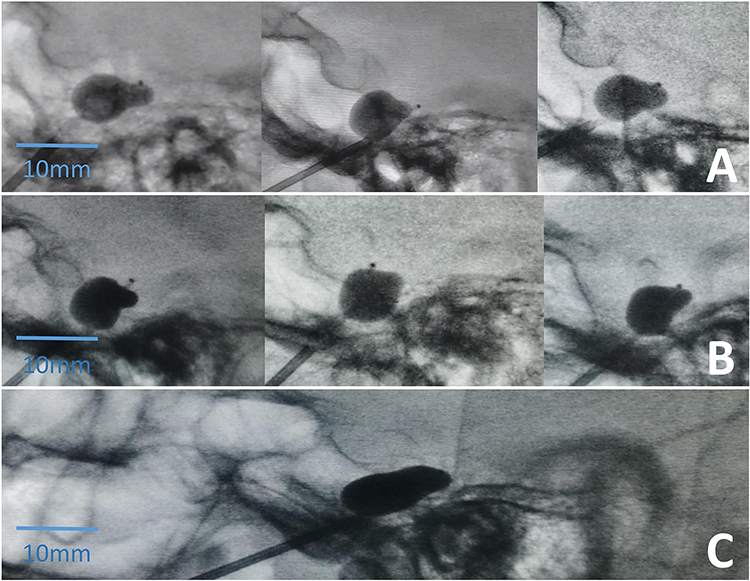 |
Figure 3 Types of balloon formation during the surgery. (A) Pear-shaped balloon. (B) Pear-like balloon. (C) Peanut-shaped balloon.Scale bar,10mm. |
Postoperative Conditions
After surgery, 68 patients experienced a complete disappearance of pain symptoms (including patients in whom the balloon exhibited a peanut shape), with two patients showing significant efficacy. The efficacy rate was 100%, and the cure rate was 97.1% (Postoperative pain resolved completely and immediately, and did not recur within three months). No serious complications were observed. The most common complication was ipsilateral facial numbness (60 out of 70 cases), which alleviated or resolved within 6–12 months. Other complications are detailed in Table 2.
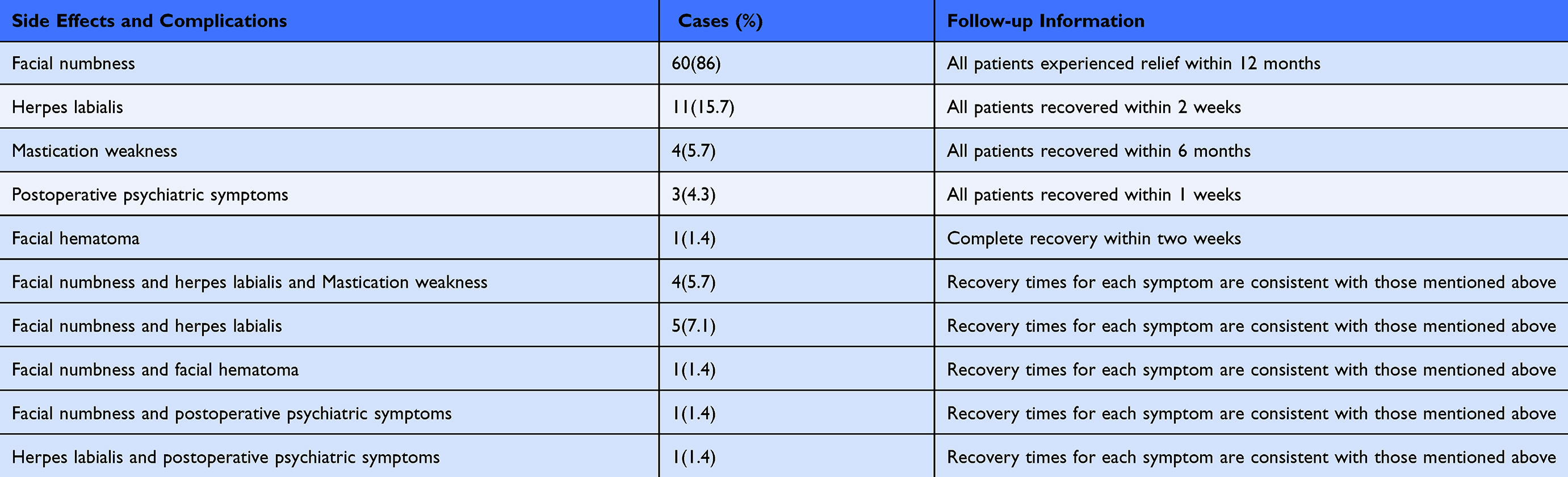 |
Table 2 Side Effects and Complications in 70 Patients After PBC (Complications Immediately Following Surgery) |
Follow-up
In this study, the postoperative hospital stays ranged from two to three days.During follow-up 36–60 months. Among the cases, there were five instances of pain recurrence (7.1%). Both cases with significant efficacy experienced pain resolution within 1 month without intervention. Among the 60 patients who experienced facial numbness postoperatively, all patients had varying degrees of relief or disappearance of facial numbness were observed within 6–12 months (At the six-month postoperative follow-up, 11.5% of patients reported complete resolution of numbness. By the 12-month mark, 28.6% of patients had experienced complete resolution of numbness), After 60 months of follow-up, facial numbness disappeared in 82% (49/60). It was observed that patients with postoperative numbness had a lower recurrence rate of pain (Table 3).
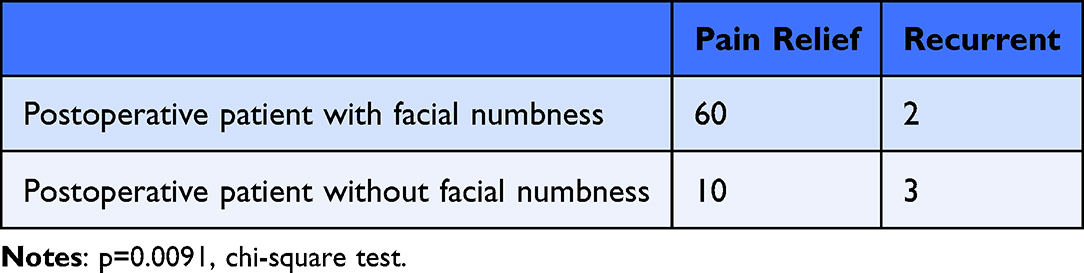 |
Table 3 Results of 70 Patients After PBC |
Discussion
This study is the first to explore the 3D reconstruction of images combined with awake anesthesia for PBC surgery. Preoperative and intraoperative image reconstruction techniques were used to ensure successful puncture, satisfactory balloon shape, and surgery was performed with the aid of awake anesthesia, and the surgical results could be confirmed during surgery. Among the 70 cases of TN patients in this study who underwent this modified PBC, according to the Brisman standard,The immediate postoperative effectiveness rate was 100%, and the complete cure rate was 97.1%.According to the relevant literature6,10,11 the pain relief rate after PBC surgery is approximately 82% to 97.1%, while the recurrence rate within 3 to 5 years postoperatively is often greater than 20%. In contrast, our group demonstrated higher effectiveness and cure rates, along with a lower recurrence rate (7.1%).No severe complications, such as rupture of the internal carotid artery or intracerebral hemorrhage, occurred during or after the operation6.
In this study, a 3D reconstruction technique was used to ensure successful puncture of the foramen ovale during PBC surgery. The first step in PBC surgery is the successful puncture of the foramen ovale and Meckel’s cave. Studies12,13 have revealed significant individual variations in the foramen ovale among adults. There are instances of small foramen ovale or nearby bony spurs,14–17 as well as other conditions, which may result in puncture failure.Shallow puncture effects surgical outcomes, while deep puncture can lead to various surgical complications such as intracranial hemorrhage, damage to the oculomotor nerve, or abducens nerve injury.18 In this study, CT 3D reconstruction technique was performed preoperatively to visually observe the bone condition near the foramen ovale, measure the size and depth of the foramen ovale, and identify the approximate depth from the foramen ovale to the trigeminal foramen with adequate preparation before puncture. During puncture, 3D reconstruction is performed using DSA X-ray machine, and measurement tools can be used to measure the depth of needle insertion and ensure that the puncture needle smoothly reaches the foramen ovale, so as to reduce the risk of puncture and avoid puncture failure.
3D reconstruction also ensures satisfactory balloon shape and correct positioning during PBC surgery. Intraoperative acquisition of a pear-shaped balloon is critical to surgical success.19,20 In traditional PBC surgery, balloon visualization is positioned with the aid of a traditional C-arm machine, and whether the balloon is inflated in a “pear-shaped” shape can only be judged on standard lateral images, which may be completed by repeated head position adjustment during surgery. In this study, 3D reconstruction using the DSA machine allowed for the precise determination of the specific position of the balloon, the relationship between the 3D shape of the balloon and the surrounding tissues. Additionally, it enabled direct observation of the balloon morphology from multiple perspectives, ensuring the balloon appeared pear-shaped. Compared to traditional guidance using a C-arm machine for puncture and balloon formation, the use of three-dimensional reconstruction improves the efficiency of puncture and balloon formation, ensures the balloon is in the correct position, and thereby reduces the risk of surgical complications. This is particularly beneficial for cases with abnormal skull base anatomy that may pose difficulties during puncture.Furthermore, the preoperative and intraoperative 3D reconstructions require only routine CT 3D scanning, utilizing the built-in 3D reconstruction software of the CT and DSA systems.it is simple to operate, has a short learning curve, does not increase surgical costs, and is an easily mastered and readily promotable technique.
Awake anesthesia not only enhances patient comfort but also allows for real-time assessment of surgical outcomes, thereby improving the success rate of the surgery. Communication with the patient was conducted to determine whether the compression time was appropriate and to evaluate the surgical outcome. This allowed for decisions regarding the termination of the procedure or adjustments to the surgical strategy, as well as the timely detection of related complications. In this group of patients, pain assessment was performed under awake anesthesia after 3 minutes of balloon compression, revealing that 6 patients still experienced significant pain on the affected side. Subsequent compression of the trigeminal ganglion was continued under awake anesthesia, resulting in the resolution of pain symptoms. If conventional anesthesia had been used, these 6 patients might have experienced persistent trigeminal neuralgia postoperatively, which could have reduced the cure rate by approximately 8.6% (6/70). It can be inferred that these outcomes are not only related to the precision of the balloon’s shape and positioning, as guided by intraoperative three-dimensional image reconstruction, but are also closely associated with the re-compression of the trigeminal ganglion following adjustments to the balloon during awake anesthesia.
Although achieving a pear-shaped balloon during PBC surgery is considered a key factor for surgical success, there are instances where the balloon fails to assume a pear-shaped configuration. Such conditions may result from balloon displacement, causing it to be positioned outside of Meckel’s cave, which could lead to a lower pain relief rate postoperatively and difficulties in confirming surgical effectiveness during the procedure. With three-dimensional reconstruction during surgery, the correct position of the balloon can be clearly identified; moreover, patient awakening following balloon compression allows for immediate assessment of surgical outcomes. In one case in our series, the intraoperative balloon exhibited a peanut shape (Figure 3C). Using intraoperative three-dimensional reconstruction, we confirmed the balloon position within Meckel’s cave. Complemented by awake anesthesia, the patient’s postoperative pain symptoms completely disappeared., and no recurrence was observed during the 60-month follow-up period. It is suggested that in special cases, a balloon may not necessarily present as pear-shaped; however, confirming that the balloon is located within Meckel’s cave and conducting evaluations under awake anesthesia can enhance the surgeon’s confidence in successfully completing the procedure.
Regarding complications, PBC is believed to produce analgesic effects by disrupting the structure of nerve fibers, with its efficacy depending on the extent of nerve fiber destruction. The primary mechanism involves the mechanical compression of large myelinated nerve fibers by the balloon, leading to damage of sensory nerve fibers.6,21 In this group of cases, 60 patients (86%) experienced postoperative facial numbness on the affected side, indicating a relatively high incidence. This phenomenon may be related to the repeated adjustments of the balloon morphology, position, and compression time during the surgical procedure in pursuit of an ideal balloon shape. Furthermore, if the patient is awakened intraoperatively and pain has not yet resolved, additional procedures such as extending compression time or adjusting the balloon position may be conducted, potentially resulting in more severe damage to sensory nerve fibers. Statistical analysis in this group also revealed that patients experiencing facial numbness had a lower recurrence rate of pain (Table 3). Recent reports have highlighted a modified percutaneous balloon compression (PBC) technique. Compared with conventional methods, this technique inflicts greater damage to sensory nerve fibers, resulting in improved long-term efficacy.22 It can be hypothesized that the more severe the damage to sensory nerve fibers, the better the pain relief may be, although this is associated with a higher probability of facial numbness.The mechanical compression in PBC primarily affects sensory nerve fibers, with minimal injury to motor nerve fibers. Consequently, there are few cases of masticatory muscle weakness in this group of cases, reported in only 4 instances, all of which recovered to normal within 6 months. Herpes simplex is closely associated with the compression and reactivation of the herpes virus latent in the trigeminal ganglion.11 During PBC, the trigeminocardiac reflex (TCR) may occur, manifesting as a significant decrease in heart rate and a reduction in blood pressure. This physiological response results in the adjustment of systemic and cerebral blood circulation, leading to blood being redirected to the brain and an increase in cerebral blood flow.6 In patients who developed transient psychiatric symptoms postoperatively in this group, a significant TCR was observed during the procedure. It is hypothesized that the increase in cerebral blood flow within a short period may lead to associated adverse symptoms, such as transient psychiatric symptoms. Notably, there were no major complications, including oculomotor disturbances, carotid artery rupture, or cerebral hemorrhage in this group, which may be attributed to the assistance of the three-dimensional reconstruction technique.
Conclusion
This study is the first to utilize modified PBC surgery with 3D reconstruction, combined with awake anesthesia, for the treatment of TN. The overall cure rate and efficacy rate are at a high level, with no occurrence of serious complications. This study aims to provide an easy-to-implement alternative to the modified PBC technique. However, this study also has several limitations.First, because the number of studies was limited, errors associated with the chance were unavoidable and may have introduced bias in the results.Second, this study tended to be a retrospective analysis and lacked a necessary control group, resulting in significant limitations. It is imperative to objectively evaluate heterogeneity and publication bias; therefore, future studies should be large-scale, well-designed randomized controlled trials, and multicenter studies are warranted to validate our findings.
Abbreviations
3D, Three-dimensional; CT, Computed tomography; DSA, Digital subtraction angiography; MVD, Microvascular decompression; PBC, Percutaneous microballoon compression; TN, Trigeminal neuralgia.
Ethics Statement
This study was approved by the Medical Ethics Committee of Guangdong Sanjiu Brain Hospital (Approval Number: 2021-01-021). Written informed consent was obtained from all participants before their inclusion in the study,Including the psychological stress responses that may occur after awakening during surgery, as well as the psychological counseling that should be provided when necessary. All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Funding
This research was supported by grants from the National Natural Science Foundation of China- Young Scientist Fund (Grant No. 82301928 to Chen) and the Science and Technology Program of Guangzhou Municipality (Grant No. 202201011720 to Fan). The funding agencies had no role in the study design, data collection and analysis, decision to publish, or preparation of the paper. The authors gratefully acknowledge the financial support that made this research possible.
Disclosure
The authors declare no conflicts of interest.
References
1. Ashina S, Robertson CE, Srikiatkhachorn A, et al. Trigeminal neuralgia. Nat Rev Dis Primers. 2024;10(1):39. doi:10.1038/s41572-024-00523-z
2. Zakrzewska JM, Linskey ME. Trigeminal neuralgia. BMJ Clin Evid. 2014;2014:1207.
3. Chen F, Xu H, Liu J, et al. Efficacy and safety of nucleoside antiviral drugs for treatment of recurrent herpes labialis: a systematic review and meta-analysis. J Oral Pathol Med. 2017;46(8):561–568. doi:10.1111/jop.12534
4. Wiffen P, Collins S, McQuay H, Carroll D, Jadad A, Moore A. Anticonvulsant drugs for acute and chronic pain. Cochrane Database Syst Rev. 2005;3:CD001133. doi:10.1002/14651858.CD001133.pub2
5. Mullan S, Duda EE, Patronas NJ. Some examples of balloon technology in neurosurgery. J Neurosurg. 1980;52(3):321–329. doi:10.3171/jns.1980.52.3.0321
6. Xia Y, Yu G, Min F, Xiang H, Huang J, Leng J. The focus and new progress of percutaneous balloon compression for the treatment of trigeminal neuralgia. J Pain Res. 2022;15:3059–3068. doi:10.2147/JPR.S374433
7. Ying X, Wang H, Deng S, Chen Y, Zhang J, Yu W. Long-term outcome of percutaneous balloon compression for trigeminal neuralgia patients elder than 80 years: a STROBE-compliant article. Medicine. 2017;96(39):e8199. doi:10.1097/MD.0000000000008199
8. Noorani I, Lodge A, Durnford A, Vajramani G, Sparrow O. Comparison of first-time microvascular decompression with percutaneous surgery for trigeminal neuralgia: long-term outcomes and prognostic factors. Acta Neurochir. 2021;163(6):1623–1634. doi:10.1007/s00701-021-04793-4
9. Brisman R. Gamma knife radiosurgery for primary management for trigeminal neuralgia. J Neurosurg. 2000;93(supplement_3):159–161. doi:10.3171/jns.2000.93.supplement
10. Baabor MG, Perez-Limonte L. Percutaneous balloon compression of the gasserian ganglion for the treatment of trigeminal neuralgia: personal experience of 206 patients. Acta Neurochir Suppl. 2011;108:251–254. doi:10.1007/978-3-211-99370-5_39
11. Wu Z, Zhao Y, Liu J, Fan Y, Yang Y. Comparison of the safety and efficacy of radiofrequency thermocoagulation with percutaneous balloon compression for treating trigeminal neuralgia: a systematic review and meta-analysis. Front Neurol. 2023;14:1178335. doi:10.3389/fneur.2023.1178335
12. Raguž M, Dumić-čule I, Almahariq F, et al. Foramen ovale and foramen rotundum: characterization of postnatal development. Acta Clin Croat. 2022;60(3):415–422. doi:10.20471/acc.2021.60.03.11
13. Prakash KG, Saniya K, Honnegowda TM, Ramkishore HS, Nautiyal A. Morphometric and anatomic variations of foramen ovale in human skull and its clinical importance. Asian J Neurosurg. 2019;14(4):1134–1137. doi:10.4103/ajns.AJNS_243_19
14. Iwanaga J, Patra A, Ravi KS, Dumont AS, Tubbs RS. Anatomical relationship between the foramen ovale and the lateral plate of the pterygoid process: application to percutaneous treatments of trigeminal neuralgia. Neurosurg Rev. 2022;45(3):2193–2199. doi:10.1007/s10143-021-01715-x
15. Somesh MS, Sridevi HB, Prabhu LV, et al. A morphometric study of foramen ovale. Turk Neurosurg. 2011;21(3):378–383. doi:10.5137/1019-5149.JTN.3927-10.2
16. Tubbs RS, WR M, Apaydin N, et al. Ossification of ligaments near the foramen ovale: an anatomic study with potential clinical significance regarding transcutaneous approaches to the skull base. Neurosurgery. 2009;65(6 Suppl):60–64. doi:10.1227/01.NEU.0000345952.64041.9C
17. Zhu B, Wang H, Liu M, Cheng K, Li Z, Li Y. Morphologic study of foramen oval region on surgery approach for trigeminal neuralgia. J Craniofac Surg. 2015;26(2):541–543. doi:10.1097/SCS.0000000000001217
18. Kouzounias K, Schechtmann G, Lind G, et al. Factors that influence outcome of percutaneous balloon compression in the treatment of trigeminal neuralgia. Neurosurgery. 2010;67(4):925–934. doi:10.1227/NEU.0b013e3181eb5230
19. Asplund P, Linderoth B, Bergenheim AT. The predictive power of balloon shape and change of sensory functions on outcome of percutaneous balloon compression for trigeminal neuralgia. J Neurosurg. 2010;113(3):498–507. doi:10.3171/2010.2.JNS091466
20. Sun C, Zheng W, Zhu Q, Du Q, Yu W. The transformation of the balloon shape in percutaneous balloon compression for trigeminal neuralgia. J Pain Res. 2021;14:3805–3814. PMID: 34934354; PMCID: PMC8684418. doi:10.2147/JPR.S343783
21. Messlinger K, Russo AF. Current understanding of trigeminal ganglion structure and function in headache. Cephalalgia. 2019;39(13):1661–1674. doi:10.1177/0333102418786261
22. Wang H, Hu S, Huang ZN, et al. Riveting technique in percutaneous balloon compression for trigeminal neuralgia remedy. Clin Neurol Neurosurg. 2024;240:108245. doi:10.1016/j.clineuro.2024.108245
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.