Back to Journals » Journal of Pain Research » Volume 16
Application of Continuous Sacral Block Guided by Ultrasound After Comprehensive Sacral Canal Scanning in Children Undergoing Laparoscopic Surgery: A Prospective, Randomized, Double-Blind Study
Authors Yan T, Yang X ![]() , Wang S, Chen J, Hu J
, Wang S, Chen J, Hu J ![]() , Zhou L
, Zhou L ![]() , Gao W
, Gao W
Received 29 September 2022
Accepted for publication 24 December 2022
Published 10 January 2023 Volume 2023:16 Pages 83—92
DOI https://doi.org/10.2147/JPR.S391501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Supplementary video of "Postoperative pain of children in PACU" [ID 391501].
Views: 130
Ting-ting Yan,* Xin-lu Yang,* Shan Wang, Jia-qi Chen, Ji-cheng Hu, Ling Zhou, Wei Gao
Department of Anesthesiology, First Affiliated Hospital of USTC (Anhui Provincial Hospital), University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Gao; Ling Zhou, Department of Anesthesiology, First Affiliated Hospital of USTC (Anhui Provincial Hospital), University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China, Tel +86-15605690073 ; +86-13866702756, Fax +86-551-62283912, Email [email protected]; [email protected]
Purpose: The present study aimed to explore the effects of continuous sacral block on the postoperative pain of children and the satisfaction of the nurses in post-anesthesia care unit (PACU). Also, the influence of the modified protocol of continuous sacral block was investigated.
Patients and Methods: A total of 60 children undergoing laparoscopic surgery were randomly divided into two groups: GI and GC groups. The general anesthesia was induced with midazolam, propofol, sufentanil and succinylcholine in both groups. In addition, the patients were subjected to continuous sacral block with levobupivacaine in group GC. The modified protocol of continuous sacral block was divided into three steps: comprehensive lumbar and sacral vertebral canal scanning by ultrasound, catheterization and administration. The EVENDOL pain scales and pediatric anesthesia emergence delirium scales of the children were evaluated at 5 min after extubation (T3), 90 min (T4), and 4 h (T5) after the operation. The nurses’ satisfaction scores at T3 -T4 and adverse events, such as nausea and vomiting, were also recorded, after the operation.
Results: After ultrasonic scanning, one patient in group GC was excluded due to the sacral hiatus atresia, which might lead to failure of catheterization. Data of 59 patients were collected for statistical analysis. Compared to the GI group, the EVENDOL scores and the pediatric anesthesia emergence delirium scales were reduced at T3, T4, and T5 (P < 0.05) in group GC. Furthermore, there was a higher rank of PACU nurses’ satisfaction in the GC group compared to the GI group (P < 0.05).
Conclusion: Based on the modified protocol, continuous sacral block provides reliable and safety analgesia for children undergoing laparoscopic surgery, thereby improving the satisfaction of PACU nurses.
Keywords: ultrasound-guided, lumbar and sacral vertebral canal scanning, postoperative pain, satisfaction of PACU nurses
Introduction
Effective postoperative pain management is one of key points in enhanced recovery after surgery for children. A previous study showed that 93% of children experienced pain after the operation, and 32% of children had behavioral changes at 4 weeks after discharge; the primary risk factor of behavioral changes was postoperative pain.1 Cornelius et al2 demonstrated that 17–32% of children who underwent surgery experienced moderate-to-severe pain, which was associated with physiological, psychological, and emotional health.3 Therefore, multimodal pain management techniques are necessary for children post-surgery. The sacral block anesthesia is a widely used technology in perioperative analgesia in children. Continuous sacral block has been used for urologic, lower abdominal, and lower limbs surgery.4,5 Due to the anatomical variation of sacral canal, the failure rate of sacral block without any visualization technology can reach 30%.6 The application of accurate imaging technology effectively improves the success rate of the puncture. Reportedly, the anatomical variation of the sacrococcygeal region can be found by ultrasound scanning before puncture to avoid the occurrence of severe complications.7 Another study reported two neonates with sacrococcygeal teratoma or sacral agenesis who were successfully placed with a sacral intervertebral catheter guided by ultrasound.8
In the post-anesthesia care unit (PACU), most of the children who experienced significant pain immediately after surgery, were taken care of by technical anesthesia nurses.9 In pediatric surgical patients, postoperative pain is a major risk factor for agitation,10 associated with the self-harm of the children and extra burden on and low satisfaction score of PACU nurses. The effect of postoperative pain management on children can be evaluated by PACU nurses through the EVENDOL pain scale (EPS)11 and Pediatric Anesthesia Emergence Delirium Scale (PAEDS).12 Therefore, the satisfaction scores of PACU nurses could evaluate based on the emergence from anesthesia and postoperative management in pediatric patients.
There are a few reports on the postoperative analgesic effect after ultrasound-guided sacral block in pediatric; and there are no report on the analgesic effect and the quality of recovery from anesthesia after ultrasound-guided continuous sacral block technique in pediatric patients. The purpose of this study, therefore, was to evaluate the anesthesia effect of ultrasound-guided continuous sacral block after comprehensive vertebral canal scanning, and meanwhile using the satisfaction of PACU nurses as feedback for the anesthesia strategy. Herein, we designed this prospective, randomized, and double-blind study to compare the effectiveness of perioperative general anesthesia vs ultrasound-guided continuous sacral block combined with general anesthesia. Thus, the present study aimed to evaluate the pain and the overall state of the children during the recovery from anesthesia based on the pain scores and PACU nurse’s satisfaction. The secondary purpose was to recommend the modified protocol of continuous sacral block, including a comprehensive lumbar and sacral vertebral canal scan.
Materials and Methods
Trial Design
This study was designed as a prospective, randomized, double-blind study, approved by the institutional ethics committee at the First Affiliated Hospital of University of Science and Technology of China, and registered on the China Clinical Trial Registration (chictr2000031390). Written informed consent was obtained from all eligible participants’ parents.
Participants
From April 2020 to March 2022, 60 pediatric patients scheduled for laparoscopic surgery were assessed before the study. The inclusion criteria were as follows: 1) age 0–6 years; 2) both genders; 3) American Society of Anesthesiologists Physical Status Classification I to II; 4) voluntary participation and cooperation of children and parents. The exclusion criteria were as follows: 1) allergy to the study drugs; 2) serious respiratory, cardiovascular, or nervous system diseases; 3) infection of puncture site; 4) coagulation disorder; 5) severe sacrococcygeal deformity (recognized by inspection, palpation, or imaging examinations).
Randomization
Eligible patients were randomly allocated to the GI or GC group. The continuous sacral block was performed after the induction of general anesthesia in the GC group, and no special treatment was administered after induction in the GI group. The allocation sequence was created by a computer-generated list. The allocation concealment was implemented using sequentially numbered, opaque, and sealed envelopes. Block randomization was performed with a 1:1 allocation ratio by a fixed block size.
Anesthesia
General Anesthesia
After entering the operating room, the electrocardiogram (ECG), mean blood pressure (MBP), heart rate (HR), pulse oxygen saturation (SpO2), end-tidal carbon dioxide partial pressure (ETCO2), and temperature were observed on the multifunctional monitor (Spacelabs Ultraview-2700, USA). All children were administered 0.05 mg/kg midazolam, 2–3 mg/kg propofol, 0.2–0.3 µg/kg sufentanil, and 2 mg/kg succinylcholine . Endotracheal intubation was performed after induction of anesthesia with an appropriate-sized endotracheal tube. The ventilation parameters were adjusted to maintain ETCO2 at 35–45 mmHg. In both groups, anesthesia was maintained with continuous inhalation of sevoflurane to achieve effective general anesthesia. Remifentanil 0.2 µg/kg/min was continuously injected in the GI group, and an equivalent volume of saline was administered in the GC group. Cisatracurium (0.05 mg/kg) was administered intermittently as needed during the operation. In group GC, a modified protocol of continuous sacral block was performed after the induction of general anesthesia, while no specific treatment was administered in the GI group after the induction of general anesthesia.
Modified Protocol of Continuous Sacral Block
The child was placed in the left lateral position with knees as close to the abdomen as possible. After sterilization of the injection site and the surrounding area, the ultrasonic diagnostic system (Wisonic, 20162230883) was used to scan the sacral canal by the probe (model LH15-6) with a sterile sheath on the sacrococcygeal of the children. The ultrasound transducer was placed perpendicularly to the posterior median line to obtain a transverse view. Then, we scanned the transverse plane from the coccyx toward the cephalad level. When the cross-sectional image of the sacral cornu was obtained, the ultrasound probe was rotated 90° to obtain longitudinal views of the sacral canal. Then, the probe was moved horizontally to the caudal side, and the caudal vertebra was observed; then, moving the probe horizontally to the cephalad level would allow viewing of the S5-S1 base of the sacrum vertebra. The terminal of the non-echo dural sac was observed through the spinous process. Subsequently, the probe was moved such as to view the sacrococcygeal ligament in the center of the screen (Figure 1A). Then, the needle was slowly advanced with in-plane technology, and the puncture needle body could be clearly seen moving in the tissue. The needle tip penetrating through the sacrococcygeal ligament and entering into the sacral canal was visualized on ultrasound imaging (Figure 1B). Then, the needle core was pulled out and the epidural catheter was placed at 1–1.5 cm depth. After confirming the absence of blood or cerebrospinal fluid, 1 mL saline was injected. Moreover, the sacrococcygeal ligament was lifted up and the liquid was spread into the hiatus cavity in the ultrasound images (Figure 1C and 1D). 0.25% levobupivacaine was slowly injected via the epidural catheter (<6-months-old 0.8 mL/kg and >6-months-old 1 mL/kg, up to 20 mL) at 10 min before surgery (Figure 2). Subsequently, levobupivacaine 0.3 mg/kg/h13,14 was pumped into the sacral canal through the catheter (Video 1). If hemodynamic changes caused by cutting or subsequent surgical procedure were observed, the block was deemed as failure, and remifentanil (0.2 µg/kg/min) should be used. Finally, the catheter was removed at the end of the operation.
 |
Figure 1 Procedure of ultrasound-guided continuous sacral block. (A) The ultrasound image of the sacral canal between the S3 and S5 in median sagittal plane. (B) The needle (indicated by the triangular arrow) entered the sacral canal. (C and D) The local anaesthetic spread in the sacral canal (the light blue area). Abbreviations: S3, base of third sacrum; S4, base of fourth sacrum; S5, base of fifth sacrum; SL, sacrococcygeal ligament. |
 |
Figure 2 The back of one patient containing the catheter after continuous sacral block. |
Postoperation
Postoperatively, the children in both groups were transferred to PACU, and the anesthesia nurse was mainly responsible for the supervision and nursing during this period. After extubation, one of the family members was allowed into PACU to accompany the child. The children were transferred to the ward 90 min after the operation. EVENDOL pain scale was comprehensively scored from five aspects for the final grade: Vocal or verbal expression, Facial expression, Movements, Postures, and Interaction with the environment.11 Pediatric anesthesia emergence delirium scale (Supplementary Table 1) was comprehensively scored from five questions for the final grade: The child makes eye contact with the caregiver (not at all/just a little/quite a bit/very much/extremely), The child’s actions are purposeful (not at all/just a little/quite a bit/very much/extremely), The child is aware of his/her surroundings (not at all /just a little/quite a bit/very much/extremely), The child is restless (not at all/just a little/quite a bit/very much/extremely), and The child is inconsolable (not at all/just a little/quite a bit/very much/extremely).12 When the EPS score was >4, additional analgesia of intravenous tramadol (1 mg/kg) was provided.
Blinding
An attending, with experienced ultrasonic technology, was responsible for sacral block and management of anesthesia. Only the investigator who performed randomization and the attending who implemented the anesthesia were aware of the group assignments. Other investigators, who were unaware of group allocation, performed perioperative assessments and did the records. The data analysis was performed by an independent research staff who was not informed the group assignment. All catheter placements were performed when the children were unconscious before the operation. A medical patch was covered after pulling out the epidural catheters in the GC group, and the same medical patch at the same position was affixed in the GI group. Only the investigator responsible for randomization and the anesthesiologist who administered anesthesia were aware of the assignments.
Outcomes
The primary outcomes of the current study were the scores of EPS at 5 min after extubation (T3). The secondary outcomes included the scores of EPS at 90 min (T4), and 4 h after the operation (T5), the area under the curve of EPS-time (AUCEPS-time) which was calculated to represent a cumulative pain intensity, the scores of PAEDS at T3-T5, the nurses’ satisfaction score (Supplementary Table 2) at T3 and T4, and the rate of rescue analgesia. The MBP and HR were recorded at 5 min after induction (T0), the time of skin incision (T1), end of the operation (T2), and T3. The consumption of remifentanil, levobupivacaine and cisatracurium during the operation were also recorded. In addition, adverse events, such as nausea and vomiting, were also recorded postoperatively.
Statistical Analysis
According to our preliminary results, the mean ± standard deviation (SD) EPS scores at 5 min after extubation were 2.21 ± 1.21 and 3.40 ± 1.39 in the GC and GI groups, respectively. A minimum sample size of 27 patients was estimated for each group, with a two-sided type I error of 0.05 and a power of 0.9. Considering a 10% dropout, 30 children were recruited in each group. All the data were analyzed statistically using the SPSS 20.0 software. QQ-plots were used to assess the normality of the data. The parametric data were presented as mean ± SD, while the nonparametric data were displayed as the median (interquartile range, IQR), and the categorical data were expressed as percentages. Numerical data were compared using the independent t-test or the Mann–Whitney test depending on their distribution, and the categorical data were compared by chi-square or Fisher’s exact test. P < 0.05 was considered statistically significant.
Results
A total of 60 pediatric patients were assessed for eligibility and randomly assigned to the GC and GI groups in this study. One patient in group GC was excluded due to technical difficulty of catheter placement after ultrasonic scanning (Figure 3). Therefore, 59 patients were included in the final analyses (Figure 4). No significant differences were observed in terms of age, weight, gender composition, ASA classification, or perioperative hemodynamics between the two groups (Table 1).
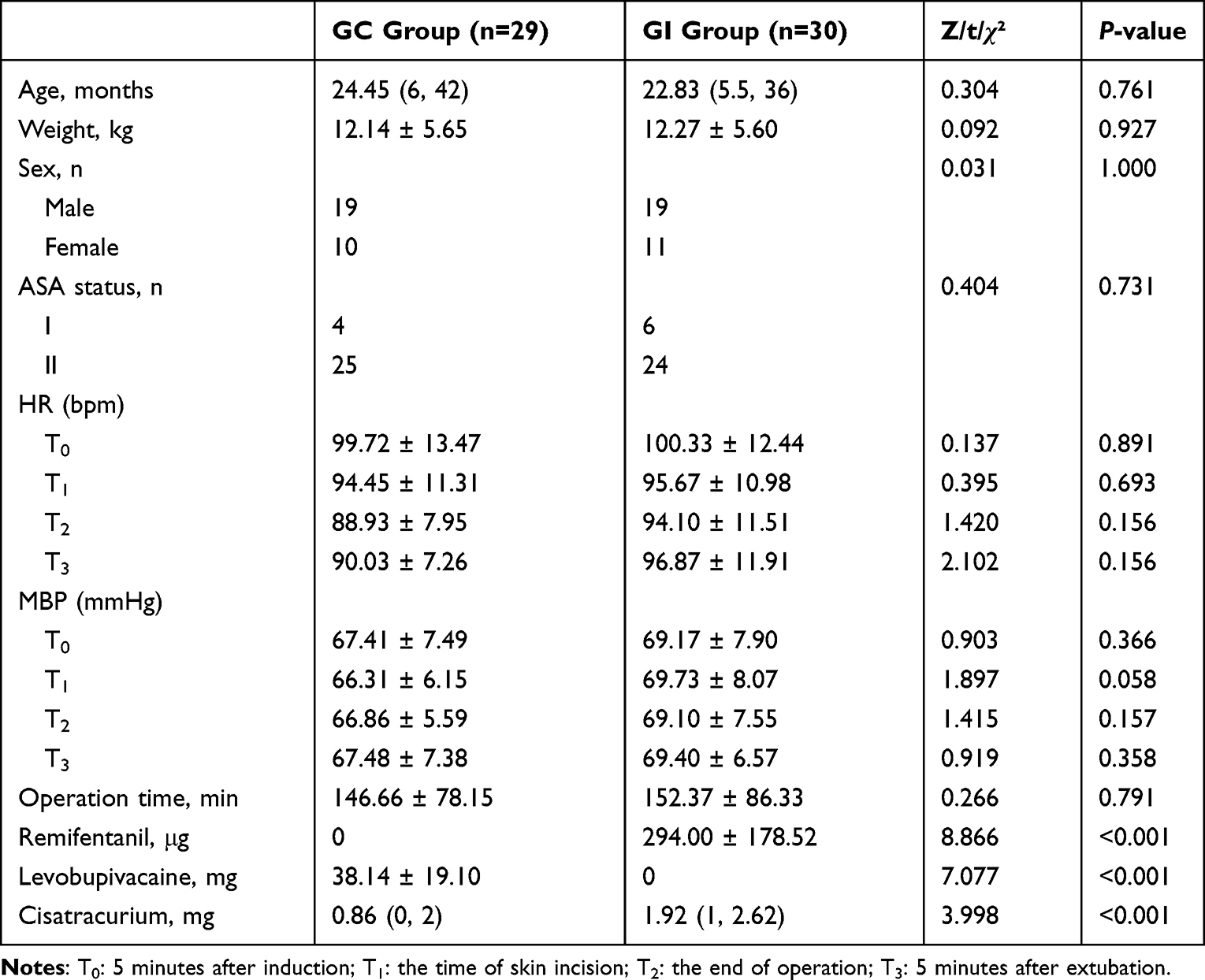 |
Table 1 General Characteristics of Participating Patients (n = 59) |
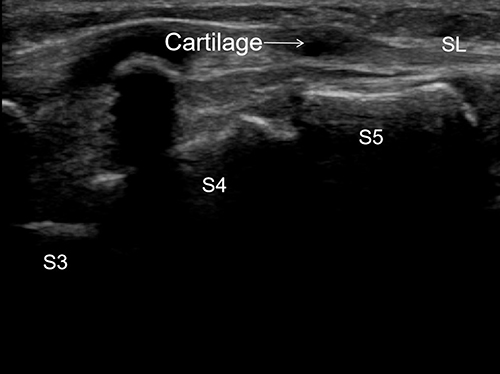 |
Figure 3 The sacral hiatus was covered by cartilage. Abbreviations: S3, base of third sacrum; S4, base of fourth sacrum; S5, base of fifth sacrum; SL, sacrococcygeal ligament. |
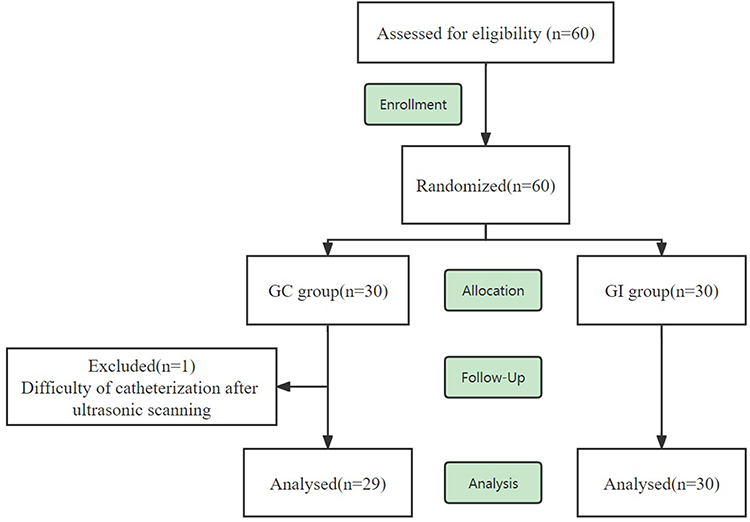 |
Figure 4 Flow chart of study showing the flow of patients in the trial. |
As shown in Table 2, the GC group provided better analgesic effects, as indicated by lower EPS scores than the GI group at T3–T5. From 5 min after extubation to 4 h after surgery, the GC group had a smaller AUCEPS-time than the GI group (3.55 ± 0.85 vs 5.85 ± 0.98, P < 0.001). The secondary outcomes are shown in Table 3. The GC group had lower PAEDS scores than the GI group at T3 (2.79 ± 1.15 vs 4.50 ± 1.50, P < 0.001), T4 (2.21 ± 0.98 vs 3.83 ± 1.23, P < 0.001), and T5 (1.83 ± 0.71 vs 3.03 ± 0.89, P < 0.001), while the nurses’ satisfaction scores were higher in the GC group compared to the GI group at T3 (16.24 ± 1.66 vs 14.47±1.94, P = 0.001) and T4 (16.14 ± 1.30 vs 14.87 ± 1.28, P < 0.001) in the PACU. According to this finding, 7 patients in the GI group and 1 patient in the GC group needed tramadol in the PACU. The rate of rescue analgesia was significantly higher in the GI group compared to the GC group (P < 0.001).
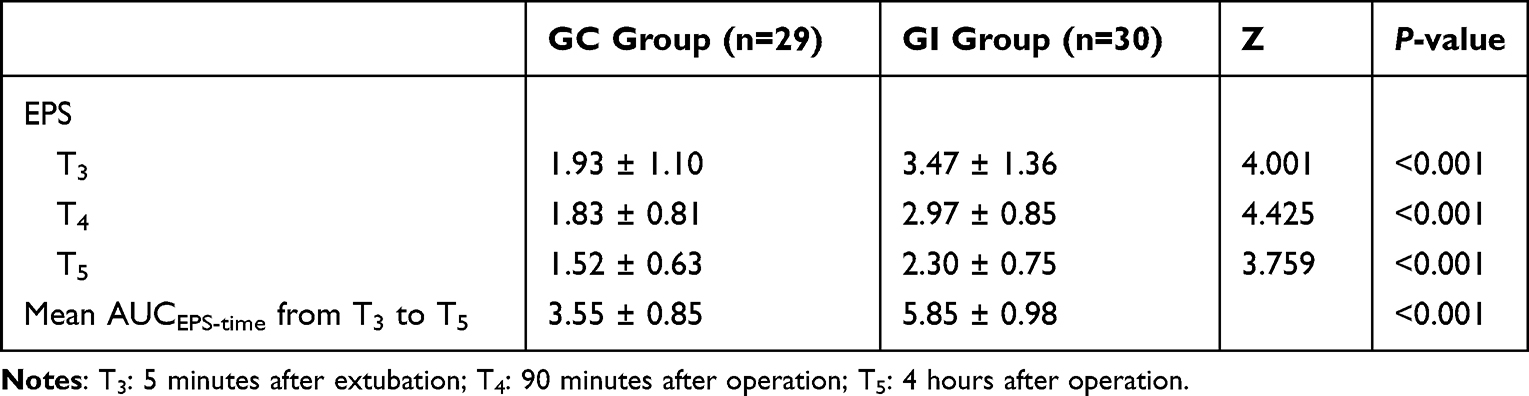 |
Table 2 Comparison of the Analgesic Effects Between the Two Groups (n = 59) |
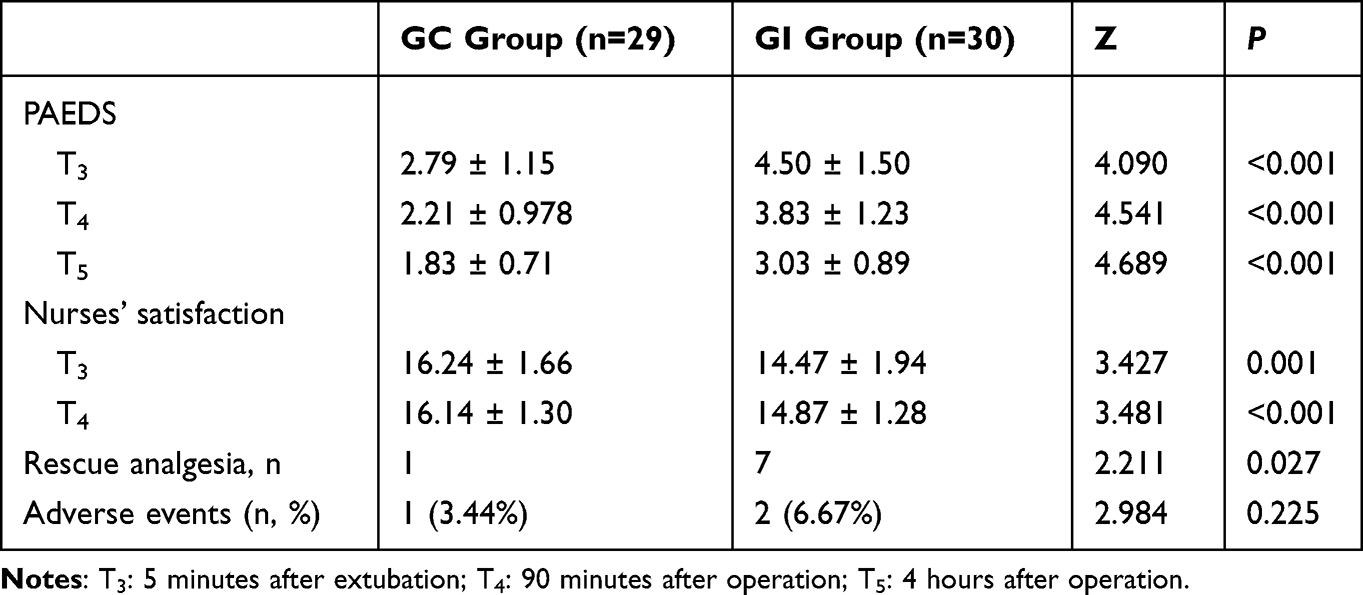 |
Table 3 Other Outcomes of Patients (n = 59) |
The GC group provided better analgesic effects after surgery and reduced the usage of cisatracurium [0.86 (0–2) vs 1.92 (1–2.62), P < 0.001] during the surgery. The consumption of remifentanil in group GI was 294.00 ± 178.52 µg. At same time, levobupivacaine in group GC was 38.14 ± 19.10 mg. No significant differences were observed in the adverse events between the two groups.
Discussion
In the current study, we aimed to explore the effects of the continuous sacral block on postoperative pain of children and on the satisfaction of PACU nurses. In addition, the improvement of the procedure and its influence on the safety of continuous sacral block were explored. The results revealed that continuous sacral block in children undergoing laparoscopic surgery reduced the use of opioids during the operation and improved the satisfaction of PACU nurses. Furthermore, the modified protocol of continuous sacral block detected the anatomical abnormalities of the lumbar and sacral vertebral canal in advance, observed the puncture needle path in real-time, and determined the depth of catheter placement to ensure the safety of process.
The connective tissue in the children’s epidural space was loose, and the diffusion range of drugs was large. Thus, by using a reasonable drug, the anesthesia plane of the sacral block could reach T4, which can safely and effectively meet the analgesic needs of children’s intracardiac, abdominal, pelvic, and perineal surgery.15–17 The current study used laparoscopic enteric and urological surgeries. No statistically significant difference was observed in the changes in blood pressure and heart rate between the two groups during T0–T2. Thus, we speculated that the sacral block could provide an analgesic effect similar to that caused by opioids and alleviate intraoperative pain. Previous studies have shown that epidural analgesia was an acceptable method for postoperative analgesia for newborns, infants, and children while reducing the use of systemic opioids and avoiding opioid-related adverse reactions.18,19 In this study, the use of opioids in group GC was less than that in group GI but provided an effective postoperative analgesia. The decrease in rescue analgesia reduced the occurrence of postoperative nausea and vomiting caused by opioids in children. Patient, surgery, and anesthesia factors contribute to risk and degree of postoperative nausea and vomiting experienced.20 There was no significant differences in the adverse events between the two groups. We have speculated it might be two reasons. Firstly, the operations were not last as long which cannot gave rise to opioids retention. Secondly, nausea, defined as a feeling of sickness with an inclination to vomit, is difficult to diagnose in an infant or nonverbal child.20 Some potential nausea may be underestimated. However, although there was no statistical significance in adverse events, the group GC provided better analgesic effects which was more beneficial for children. Nonetheless, the use of muscle relaxants in group GC was less than that in group GI; the muscle relaxation effect was caused by continuous sacral block.
Since the sacrum of children has not been completely ossified, the sacrum and sacral canal structure could be imaged by ultrasound compared to that of adults. Thus, in the current trial, the lumbar and sacral vertebral canals were scanned comprehensively before the continuous sacral block. One child in our study did not undergo continuous sacral block due to the identification of abnormal dissection in advance. In a previous study,21 the out-of-plane technique did not take complete advantage of ultrasound in children. Herein, we used the technique of in-plane needle insertion. Beyond that, some children had the sacral anatomical abnormality resulting in difficulty or failure of puncture in previous studies,22,23 and the dural sac can be terminated on the S3 or lower level.24,25 Therefore, according to the modified protocol of continuous sacral block, the terminal position of the dural sac, the sacral fissure structure, and the injected drug spread could be observed in real-time by ultrasound; together, these features reduced the incidence of puncture failure, dural sac injury, or total spinal anesthesia.
The PACU nurses, as medical personnel with professional knowledge and skills, were an integral part of perioperative medical care. As a link between anesthesiologists and patients’ families, they could provide continuous care to patients in PACU and evaluate the changes in the condition of patients from a professional point of view. The PACU nurses’ satisfaction criteria were based on the number of additional interventions that needed to be implemented. The more appropriate anesthesia strategy had been taken, the less additional intervention was needed in the PACU for children. Previous studies had a simple scoring,26,27 which was not ascribed to specific items. In the current study, the satisfaction of PACU nurses was comprehensively scored from five aspects for the final grade: length of the stage of analepsia time, pacification, alertness, airway intervention, and pain. The scores included almost every aspect of PACU nurses’ monitoring and intervention of the children, which reflected the appropriateness of preoperative and intraoperative anesthesia strategies from another perspective. The scores could be used as feedback for the anesthesiologists and had significance in the evaluation of the anesthesia strategy. A multifaceted evaluation was conducive to the improvement of anesthesia strategy by anesthesiologists. Moreover, crying and delirium caused by pain in children could increase the noise level in PACU; the noise level might reduce nurses’ mood swings of nurses.28 Patients in hospitals with better nurse work environments were less likely to be admitted to an intensive care unit and less likely to die.27 In this study, the satisfaction score of PACU nurses in group GC was higher than that in group GI. This finding indicated that general anesthesia combined with continuous sacral block provided effective intraoperative and postoperative analgesia and appeased the children, reduced the intervention measures in PACU, and improved the satisfaction of PACU nurses.
Nevertheless, the present study has several limitations. First, it was a single-center study. The results and conclusions of our trial need to be confirmed by multi-center trials. Second, we did not observe and record the duration of the continuous sacral block. This observation has been incorporated into our next continuous sacral block research project. Third, we did not follow up in the long term to assess the behavioral and psychological changes in children.
Conclusion
In conclusion, the continuous sacral block in children undergoing laparoscopic surgery could provide postoperative analgesia, reduce intraoperative and postoperative opioid medication and improve PACU nurses’ satisfaction. Also, our modified protocol of continuous sacral canal block guided by ultrasound ensured the safety of the procedure.
Abbreviations
PACU, post-anesthesia care unit; ASA, American Society of anesthesiologists; ECG, electrocardiogram; MBP, mean blood pressure; HR, heart rate; SpO2, pulse oxygen saturation; ETCO2, end-expiratory carbon dioxide; EPS, EVENDOL pain scale; PAEDS, pediatric anesthesia emergence delirium scale; AUC, area under the curve; SL, sacrococcygeal ligaments.
Data Sharing Statement
The authors state that all data in the manuscript are accessible if requested (contact e-mail address [email protected]). The authors verify that all data intended for sharing are deidentified.
Ethics Approval and Informed Consent
The Ethics Committee at the First Affiliated Hospital of USTC approved this trial. Written informed consent was obtained from all patients recruited to the study, in accordance with the code of the Declaration of Helsinki. The trial was registered at the Chinese Clinical Trial Registry (ChiCTR2000031390).
Acknowledgments
Ting-ting Yan and Xin-lu Yang are co-first authors for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nina Mary P, Howard Richard F, Wade Angie M, et al. Pain and behaviour changes in children following surgery. Arch Dis Child. 2012;97:879–884. doi:10.1136/archdischild-2011-301378
2. Groenewald Cornelius B, Rabbitts Jennifer A, Schroeder Darrell R, et al. Prevalence of moderate-severe pain in hospitalized children. Paediatr Anaesth. 2012;22(7):661–668. doi:10.1111/j.1460-9592.2012.03807.x
3. American Academy of Pediatrics. Committee on psychosocial aspects of child and family health, task force on pain in infants, children, and adolescents, the assessment and management of acute pain in infants, children, and adolescents. Pediatrics. 2001;108:793–797. doi:10.1542/peds.108.3.793
4. Adilović AŠ, Rizvanović N, Adilović H, et al. Caudal block with analgosedation - a superior anaesthesia technique for lower abdominal surgery in paediatric population. Med Glas. 2019;16. doi:10.17392/1017-19
5. Bosenberg A. Benefits of regional anesthesia in children. Paediatr Anaesth. 2012;22:10–18. doi:10.1111/j.1460-9592.2011.03691.x
6. Barham G, Hilton A. Caudal epidurals: the accuracy of blind needle placement and the value of a confirmatory epidurogram. Eur Spine J. 2010;19:1479–1483. doi:10.1007/s00586-010-1469-8
7. Schwartz D, Al-Najjar H, Connelly NR. Caudal block in a child with a sacral dimple utilizing ultrasonography. Paediatr Anaesth. 2011;21:1073–1074. doi:10.1111/j.1460-9592.2011.03621.x
8. Visoiu M, Nubani LA, Nicolay MD, Polaner D. Nicolay Michael Dustin, continuous ultrasound-guided sacral intervertebral block for postoperative analgesia in neonates. Paediatr Anaesth. 2022;32(1):82–84. doi:10.1111/pan.14305
9. Fortier Michelle A, Chou J, Maurer Eva L, et al. Acute to chronic postoperative pain in children: preliminary findings. J Pediatr Surg. 2011;46(9):1700–1705. doi:10.1016/j.jpedsurg.2011.03.074
10. Kanaya A. Emergence agitation in children: risk factors, prevention, and treatment. J Anesth. 2016;30:261–267. doi:10.1007/s00540-015-2098-5
11. Fournier-Charrière E, Tourniaire B, Carbajal R, et al. EVENDOL, a new behavioral pain scale for children ages 0 to 7 years in the emergency department: design and validation. Pain. 2012;153:1573–1582. doi:10.1016/j.pain.2012.02.024
12. Russell PS, Mammen PM, Shankar SR, et al. Pediatric anesthesia emergence delirium scale: a diagnostic meta-analysis. World J Clin Pediatr. 2022;11:196–205. doi:10.5409/wjcp.v11.i2.196
13. Okonkwo I, Bendon AA, Cervellione RM, et al. Continuous caudal epidural analgesia and early feeding in delayed bladder exstrophy repair: a nine-year experience. J Pediatr Urol. 2019;15(1):76.e1–76.e8. doi:10.1016/j.jpurol.2018.10.022
14. Mevorach DL, Perkins FM, Isaacson SA. Bupivacaine toxicity secondary to continuous caudal epidural infusion in children. Anesth Analg. 1993;77:1305–1306. doi:10.1213/00000539-199312000-00042
15. Rosen KR, Rosen DA. Caudal epidural morphine for control of pain following open heart surgery in children. Anesthesiology. 1989;70:418–421. doi:10.1097/00000542-198903000-00009
16. Nguyen Khoa N, Byrd Heather S, Tan Jonathan M, Ramamoorthy C. Caudal analgesia and cardiothoracic surgery: a look at postoperative pain scores in a pediatric population. Paediatr Anaesth. 2016;26(11):1060–1063. doi:10.1111/pan.12990
17. Relland Lance M, Tobias Joseph D, Martin D, et al. Ultrasound-guided rectus sheath block, caudal analgesia, or surgical site infiltration for pediatric umbilical herniorrhaphy: a prospective, double-blinded, randomized comparison of three regional anesthetic techniques. J Pain Res. 2017;10:2629–2634. doi:10.2147/JPR.S144259
18. Payne KA, Hendrix MR, Wade WJ. Caudal bupivacaine for postoperative analgesia in pediatric lower limb surgery. J Pediatr Surg. 1993;28(2):155–157. doi:10.1016/S0022-3468(05)80262-3
19. Wolf Andrew R. Effects of regional analgesia on stress responses to pediatric surgery. Paediatr Anaesth. 2012;22(1):19–24. doi:10.1111/j.1460-9592.2011.03714.x
20. Stoops S, Kovac A. New insights into the pathophysiology and risk factors for PONV. Best Pract Res Clin Anaesthesiol. 2020;34(4):667–679. doi:10.1016/j.bpa.2020.06.001
21. Karaca O, Pinar Huseyin U, Gokmen Z, et al. Ultrasound-guided versus conventional caudal block in children: a prospective randomized study. Eur J Pediatr Surg. 2019;29(06):533–538. doi:10.1055/s-0038-1676980
22. Abera Z, Amanuel G, Bekele A, et al. Assessment of morphological and morphometrical variations of sacral hiatus in dry human sacrum in Ethiopia. Local Reg Anesth. 2021;14:25–32. doi:10.2147/LRA.S277556
23. Nakahashi M, Uei H, Hoshino M, et al. Anatomical evaluation of the sacral hiatus using ultrasound imaging: factors that inhibit needle insertion during caudal epidural block procedures. Pain Pract. 2020;20(1):55–61. doi:10.1111/papr.12826
24. Joo J, Kim J, Lee J. The prevalence of anatomical variations that can cause inadvertent dural puncture when performing caudal block in Koreans: a study using magnetic resonance imaging. Anaesthesia. 2010;65:23–26. doi:10.1111/j.1365-2044.2009.06168.x
25. Senoglu N, Senoglu M, Ozkan F, et al. The level of termination of the dural sac by MRI and its clinical relevance in caudal epidural block in adults. Surg Radiol Anat. 2013;35(7):579–584. doi:10.1007/s00276-013-1108-2
26. Uysal HY, Takmaz SA, Yaman F, et al. The efficacy of intravenous paracetamol versus tramadol for postoperative analgesia after adenotonsillectomy in children. J Clin Anesth. 2011;23(1):53–57. doi:10.1016/j.jclinane.2010.07.001
27. Visoiu M, Joy Lendi N, Grudziak Jan S, et al. The effectiveness of ambulatory continuous peripheral nerve blocks for postoperative pain management in children and adolescents. Paediatr Anaesth. 2014;24(11):1141–1148. doi:10.1111/pan.12518
28. Cvach M, Doyle P, Wong SY, et al. Decreasing pediatric PACU noise level and alarm fatigue: a quality improvement initiative to improve safety and satisfaction. J Perianesth Nurs. 2020;35(4):357–364. doi:10.1016/j.jopan.2020.01.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.