Back to Journals » Advances in Medical Education and Practice » Volume 17
Application of Artificial Intelligence in Medical Education: A Systematic and Narrative Review of Pedagogical Potential and Ethical Implications
Authors Ren Y ![]() , Wang Y, Dong S, Su W, Wu Y, Liang S, Yang X
, Wang Y, Dong S, Su W, Wu Y, Liang S, Yang X
Received 12 September 2025
Accepted for publication 2 January 2026
Published 15 January 2026 Volume 2026:17 567190
DOI https://doi.org/10.2147/AMEP.S567190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Yuan Ren,1 Ying Wang,2 Sheng Dong,1 Wei Su,1 Youtu Wu,1 Shikai Liang,1 Xuejun Yang1
1Department of Neurosurgery, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing, People’s Republic of China; 2Department of Neural Reconstruction, Beijing Neurosurgical Institute, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Xuejun Yang, Department of Neurosurgery, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, 168 Litang Road, Changping District, Beijing, 10084, People’s Republic of China, Email [email protected]
Abstract: Artificial intelligence (AI) is rapidly transforming medical education through large language models (LLMs), virtual reality (VR), intelligent tutoring systems, and decision-support platforms. These tools enable adaptive instruction, immersive simulation, and real-time feedback, showing strong potential to improve outcomes across health professions training. To explore both opportunities and risks, we conducted a systematic review of PubMed, EMBASE, Web of Science, and Scopus for English-language studies published between January 2015 and May 2025, following the PRISMA framework. Nineteen studies met eligibility criteria. AI modalities identified included LLMs such as ChatGPT, VR-based simulation systems, automated tutoring platforms, and clinical decision-support tools, spanning specialties including radiology, surgery, and psychiatry. Across contexts, AI enhanced examination performance, procedural competence, self-directed learning, engagement, and motivation relative to traditional methods. Students and faculty expressed strong interest and optimism but reported limited formal AI training, favoring interactive practice over didactic lectures. Despite these benefits, concerns consistently emerged regarding algorithmic bias, inaccuracy, data security, and the necessity of human oversight in educational and clinical settings. Ethical issues such as job displacement, the erosion of humanistic care, and the impact on the patient-physician relationship were also highlighted. Limited formal AI training, uneven institutional readiness, and gaps in faculty expertise were common challenges across regions.To harness its transformative potential responsibly, investment is required in faculty development, structured curricula addressing both technical and ethical competencies, and governance frameworks that ensure equitable, transparent, and accountable use. Properly integrated, AI can not only personalize learning and expand access but also support a more inclusive and ethically grounded vision for the future of medical education.
Keywords: artificial intelligence, medical education, simulation-based learning, student perceptions, curriculum integration
Introduction
The rapid integration of artificial intelligence (AI) into clinical practice is driving profound changes in medical education.1 AI technologies, particularly large language models (LLMs) such as ChatGPT2 and domain-specific platforms, are increasingly being explored for use in medical teaching, clinical simulation, and decision support.3 Current applications encompass automated generation of case vignettes, anatomy instruction, radiographic interpretation, and facilitation of ethical reasoning through natural language interaction.4 Immersive modalities such as virtual patient simulations, adaptive learning platforms, and AI-assisted decision systems offer scalable solutions to faculty shortages, infrastructural limitations, and resource disparities, thereby enhancing both educational quality and accessibility, especially in underserved regions.5,6
However, the adoption of AI in medical education extends far beyond technological innovation.3 It necessitates rethinking core paradigms, including student-teacher interaction, cultivation of critical thinking amid generative content, and ethical use of AI outputs. Concerns over data privacy, algorithmic bias, authorship, and accountability pose complex challenges for curriculum design and governance. Educators must not only teach about AI but also prepare students to collaborate with it ethically and clinically.
While many studies describe specific AI applications, such as simulation-based learning or diagnostic tutorials, most are fragmented by specialty, stage, or geography, and few link pedagogical benefits with ethical considerations. This review addresses this gap by synthesizing evidence on: (1) current AI use cases in preclinical and clinical education; (2) learners’ and educators’ perceptions, literacy, and readiness; (3) core ethical concerns, including fairness, accountability, privacy, and transparency; and (4) proposed curricular and governance strategies for responsible integration. The aim is to inform educators, leaders, and policymakers on leveraging AI’s potential while preserving professional values and clinical integrity.
Methods
Study Design
This systematic review was conducted by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The objective was to identify, synthesize, and critically appraise peer-reviewed literature addressing both the pedagogical applications of artificial intelligence (AI) in medical education and the ethical issues arising from its implementation.
Data Sources and Search Strategy
A comprehensive literature search was performed in PubMed, EMBASE, Web of Science, and Scopus for studies published between January 2015 and May 2025, a period selected to capture the rapid evolution of generative AI technologies such as ChatGPT. The search strategy combined population terms (eg, “medical education,” “health professional education,” “clinical training,” “medical students,” “residents”) with intervention terms (eg, “artificial intelligence,” “large language models,” “ChatGPT,” “generative AI,” “machine learning,” “educational technology”), application terms (eg, “AI-assisted learning”, “AI-based education”, “simulation-based learning”, “virtual reality training”, “problem-based learning”), and ethical terms (eg, “ethics”, “bias”, “privacy”, “accountability”, “trust”, “autonomy”, “AI governance”).
Inclusion and Exclusion Criteria
Eligible studies included peer-reviewed articles published in English that reported original research (quantitative, qualitative, or mixed-methods), systematic or narrative reviews, or theoretical discussions explicitly focusing on AI applications in medical or health professional education and incorporating an ethical dimension. Studies involving undergraduate medical students, postgraduate trainees, or medical educators were considered. Exclusion criteria comprised non-English publications, conference abstracts, editorials, letters, or opinion pieces without primary data; studies addressing AI solely in clinical practice without educational relevance; and papers on AI technical development lacking pedagogical or ethical focus.
Study Selection
All identified records were imported into a reference manager (eg, Rayyan), and duplicates were removed. Two independent reviewers screened titles and abstracts. Full texts were retrieved for all potentially eligible studies. Disagreements were resolved by discussion or consultation with a third reviewer.
A PRISMA flow diagram was used to depict the study selection process.
Data Extraction and Synthesis
A standardized extraction form was used to collect bibliographic details, study design, participant characteristics, AI application type and role (eg, simulation, diagnostics, assessment, chatbot-based learning), target educational level, reported outcomes (eg, learning effectiveness, attitudes, engagement, literacy), and ethical considerations (eg, privacy, bias, explainability, responsibility, emotional impact). A thematic synthesis approach was employed: descriptive coding was first applied to classify AI application contexts and ethical themes, followed by the generation of analytical themes grouped under four overarching domains, applications in medical education, AI literacy and student perception, ethical challenges, and curriculum and governance implications.
Results
Study Selection
The initial database search yielded 1488 records. After removing 688 duplicates, 800 titles and abstracts were screened. A total of 41 full-text articles were assessed for eligibility, and 19 studies met the inclusion criteria.
A PRISMA flow diagram summarizing the selection process is shown in Figure 1
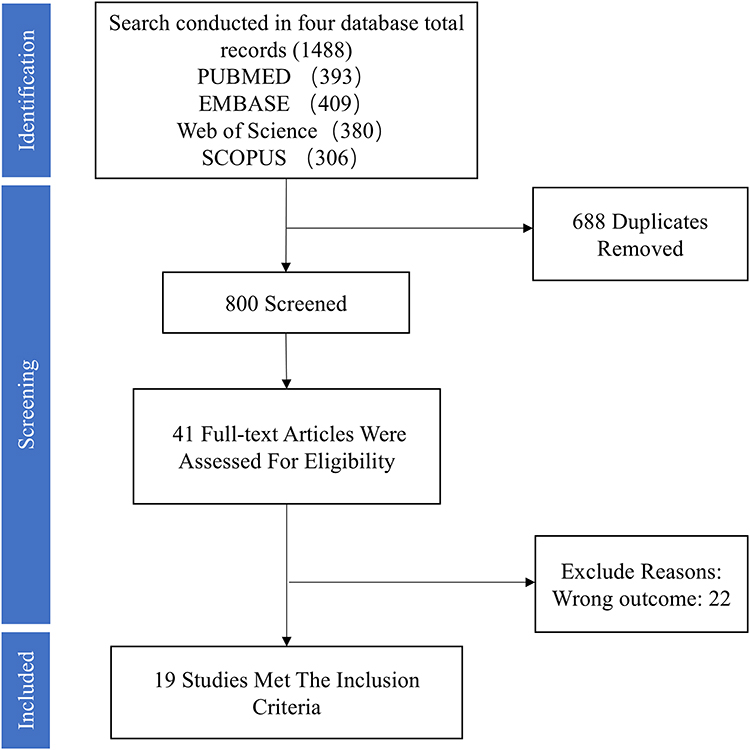 |
Figure 1 A PRISMA flow diagram. |
Study Characteristics
The target populations across the studies varied widely. A total of 12 studies involved undergraduate and postgraduate medical students. Three studies focused on interns, trainees, and residents, while one study included endoscopists with varying levels of experience. Additionally, two studies targeted healthcare professionals, including nurses and trainees. One study incorporated multi-stakeholder perspectives, involving both students and educators. Studies originated from 13 countries, predominantly USA, UK, China, Japan, Pakistan, Germany, Austria, Switzerland, Saudi Arabia, Jordan, Canada, Spain and India.
For the study on AI applications in medical education, the AI tools used varied across the research. Specifically, 3 studies utilized ChatGPT, 2 studies employed Virtual Reality (VR), 1 study applied AI-based teaching tools such as Watson for Oncology, and 2 studies incorporated Simulation-based Education (SBE).
Themes Identified
Effectiveness of AI-Based Tools
Eight studies evaluated the impact of AI-based tools on medical education outcomes, involving interventions such as ChatGPT (n = 3), Watson for Oncology (n = 1), simulation-based education (n = 1), and virtual reality (VR) systems (n = 2) with sample sizes ranging from 22 to 317 participants across undergraduate, intern, and resident cohorts. Outcomes clustered into three domains: academic performance, clinical/practical skills, and learning-related psychological measures (Table 1).
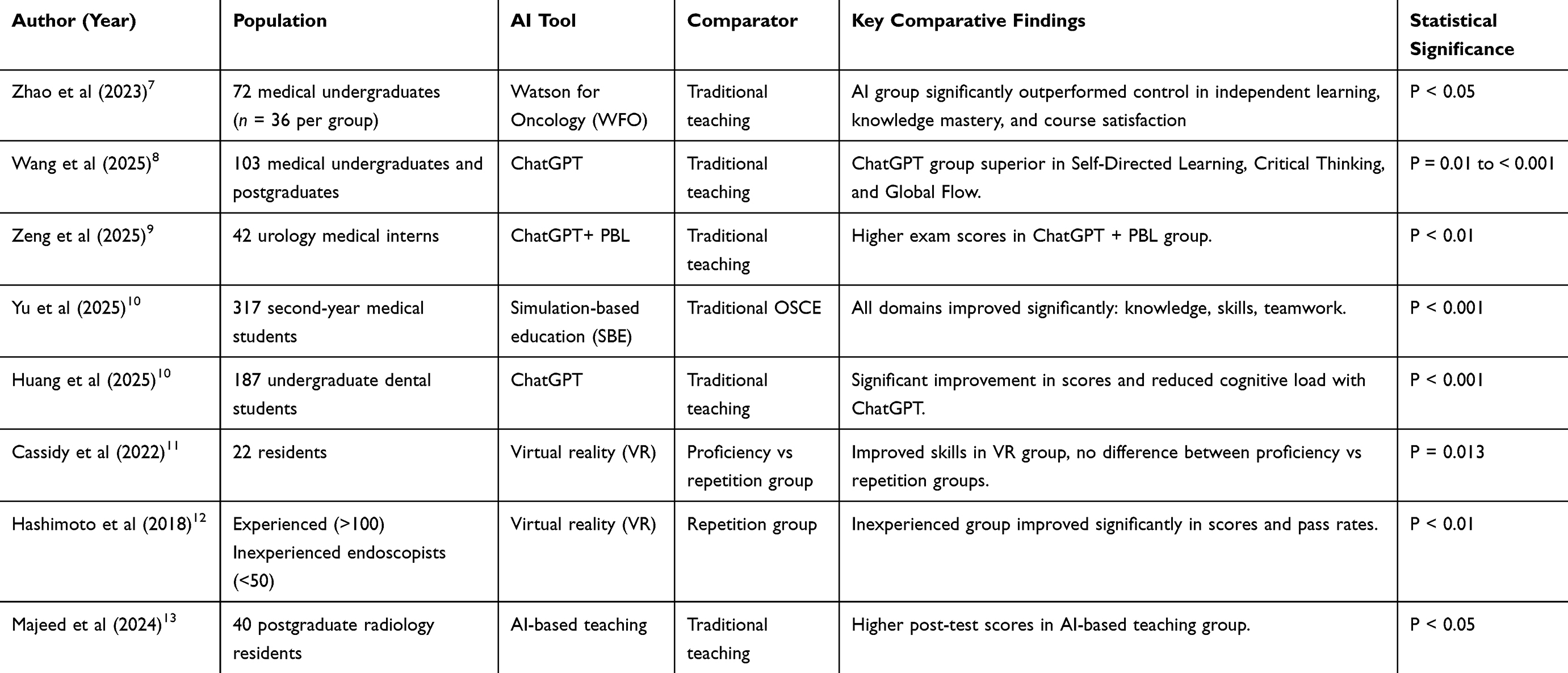 |
Table 1 AI Tools in Medical Education: Comparison of Study Findings and Outcomes |
Six studies assessed academic performance through standardized or course-specific examinations. Compared to traditional teaching, AI-based interventions were associated with significantly higher academic scores.
Three studies evaluated clinical and procedural skills in contexts such as OSCEs, communication training, and surgical/endoscopic instruction. AI-enhanced simulation-based education provided personalized, real-time feedback and adaptive pathways, yielding marked improvements in practical skills, communication, imaging interpretation, and teamwork. In VR-based endoscopy training, AI integration significantly increased GAGES and FES scores, improved practice efficiency, and elevated post-training pass rates. Similarly, AI models have demonstrated substantial potential in diagnostic and prognostic applications. The RAINMAN deep learning-based semiautomated workflow improved diagnostic performance for nasopharyngeal carcinoma, enhancing both sensitivity and specificity, while reducing radiologist workload.14 AI-based models for nasopharyngeal imaging in NKTCL also outperformed resident radiologists, with AUCs ranging from 0.905 to 0.960, and improved prognostic accuracy for survival prediction.15 Moreover, the MODERN deep learning model for detecting recurrent nasopharyngeal carcinoma achieved accuracy comparable to expert radiologists, and when combined with radiologists, further boosted diagnostic accuracy (P < 0.001).16 These examples highlight AI’s potential to optimize clinical skills, diagnostic accuracy, and therapeutic decisions.
Four studies evaluated engagement,7–10 motivation, or cognitive outcomes of AI-assisted education. Across these studies, AI interventions consistently led to significantly higher levels of independent learning, self-directed learning, learning motivation, participation, and satisfaction compared with traditional approaches. Notably, AI-supported groups also demonstrated enhanced self-efficacy, critical thinking skills, and reduced cognitive load. These findings suggest that AI-based tools such as ChatGPT and Watson for Oncology may promote deeper learning and more positive learner experiences. Students reported high satisfaction with ChatGPT-based learning, citing its interactive and personalized features as key motivators. However, some noted limitations, including occasional misunderstanding of prompts and difficulty handling surgical terminology. An observed AI error rate of approximately 15% highlighted the need for instructor oversight to ensure accuracy.9
Medical Students’ AI Literacy and Attitudes
Most students held positive views about digital health, especially technologies like big data, telemedicine, and wearables, though fewer recognized the value of decision support systems (Table 2). Practical, hands-on training was preferred over traditional lectures, and interest in the ethical and legal aspects of digital health remained relatively limited.17
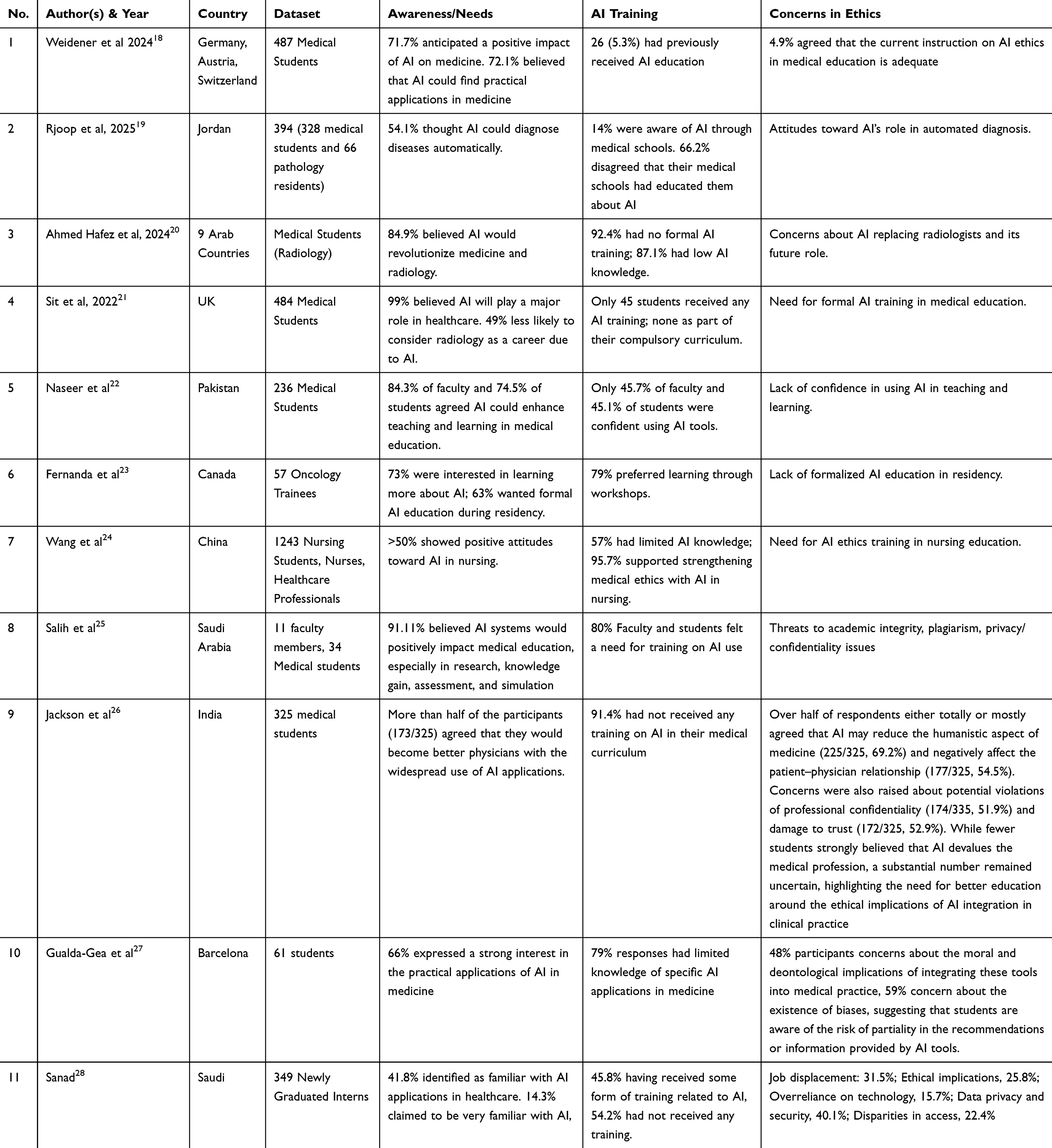 |
Table 2 Summary of Studies on Awareness, AI Training, and Ethical Concerns |
Review studies reveal that medical students and trainees generally hold a positive attitude toward the application of artificial intelligence (AI) in healthcare. Across studies from Europe, the Middle East, South Asia, East Asia, and North America, students widely recognized AI’s potential in radiology, diagnostics, and education but reported minimal exposure and limited formal training—often electives, workshops, or online modules rather than core curriculum. Over 80% in several studies had no structured AI education, and confidence in AI tool use was generally low among both students and faculty.
However, a significant gap exists between general interest and actual competence. Many students and educators expressed a lack of confidence in effectively using AI tools. For example, in Pakistan, fewer than half of both students and educators felt comfortable applying AI in teaching or learning. In Jordan and other Arab countries, while students had high expectations of AI’s diagnostic potential, they lacked hands-on experience and structured training.
Perceptions of institutional readiness varied by region. In Saudi Arabia, most educators believed their institutions had the resources to integrate AI, yet students cited issues such as outdated software, poor infrastructure, and insufficient expert support. Educators often indicated that they required more training and support, while students were seen as more adaptable to emerging technologies.25 Despite these gaps, both faculty and students generally agreed that AI could be integrated into current curricula with moderate adjustments and appropriate oversight.
In terms of AI usage in medical education, more than half of the students (54.1%) recognize AI’s potential for automating disease diagnosis, with 80.7% agreeing that AI could assist in recommending appropriate investigations. However, training on AI applications, particularly in fields such as radiology and diagnostics, remains insufficient. For example, 92.4% of students in an Arab countries study had not received formal AI training, and 87.1% had low levels of AI knowledge. This lack of training is echoed by the findings in Pakistan, where 45.7% of faculty and 45.1% of students expressed a lack of confidence in using AI-based tools for teaching and learning.
Ethical Challenges in the Use of AI for Teaching
Ethical concerns were prominent across all regions, especially regarding job displacement, data privacy, algorithmic bias, and the erosion of humanistic care (Table 2). In the UK, 49% of medical students said AI made them hesitant to pursue radiology as a career. In India and Canada, over half of the participants worried that AI might damage the patient-physician relationship. Many students also expressed uncertainty about AI’s legal and moral accountability, and in some studies, fewer than 5% felt their current ethics training was adequate. To address these concerns, some educators have begun integrating ethical training into AI-related teaching, including using tools like ChatGPT to simulate clinical dilemmas and promote critical reflection.29 Further, viewpoints from educational literature advocate for an embedded ethics approach, systematically integrating AI ethics content into existing bioethics or medical ethics curricula. Such frameworks help students grasp not only ethical principles but also practical implications of AI in healthcare.30 Complementing this, case-based and scenario-driven teaching strategies are commonly used to enhance students’ ethical sensitivity and humanistic awareness.31
Discussion
Summary of Key Findings
This review highlights the expanding applications of AI across various levels of medical education, including undergraduate, postgraduate, and continuing education. Participants reported AI being used in diverse instructional formats, such as virtual and augmented reality, intelligent tutoring systems, and machine learning–driven simulations. These tools have been adopted across multiple clinical disciplines, such as radiology, cardiology, psychiatry, surgery, as well as related fields like nursing, anesthesia, and public health.32 Some institutions were reported to have introduced AI-focused curricula covering topics such as programming, algorithms, and computer science. Learners described VR-based instruction as engaging and helpful in building confidence, providing a safe environment for problem-solving and experiential learning. AI and telemedicine were generally viewed as key enablers for improving healthcare access, particularly in underserved settings.33
Compared with lecture-based, standardized, and uniform curricula, AI enables adaptive, interactive, and data-driven instruction, offering personalized feedback, complex clinical simulations, and continuous performance analytics. When combined with traditional teaching, AI has been shown to improve examination performance, procedural competence, and decision-making. However, mentorship, empathy, and ethical reasoning, core strengths of conventional education remain irreplaceable, positioning AI as a complement rather than a substitute. Although students generally view AI positively, most lack formal training on its responsible use. Despite strong enthusiasm, current medical curricula often do not include structured AI education. Therefore, institutions must prioritize the development of policy frameworks, pedagogical strategies, and oversight mechanisms to ensure that AI is integrated responsibly into traditional medical education models.
Comparison with Existing Literature
It is our view that AI functions best as a complement to, rather than a substitute for, traditional medical education, a stance supported by prior studies. Systematic reviews in anatomy confirm that AI-powered tools, such as virtual dissection simulations and machine learning–enhanced feedback systems, can improve knowledge retention and application-level reasoning while preserving human judgment.34–36 Similarly, radiology education literature suggests that AI enables “precision education”, allowing customized feedback and adaptive learning tailored to trainee progress.37 Although these domain-specific studies highlight AI’s value, few reviews integrate educational applications and ethical dimensions cohesively. Our review addresses this gap by mapping AI tools to both pedagogical benefits and ethical considerations across undergraduate and postgraduate education.
Although these domain-specific studies highlight AI’s value, few reviews integrate educational applications and ethical dimensions cohesively. Our review addresses this gap by mapping AI tools to both pedagogical benefits and ethical considerations across undergraduate and postgraduate education.38 Broader analyses identify domains such as fairness, consent, data privacy, and patient-centered care, emphasizing the need for multidisciplinary oversight.39 Narrative reviews also note risks of bias, academic integrity issues, and content misuse, calling for curricula that foster critical evaluation alongside technical competence.40
Furthermore, effective implementation of generative AI tools like ChatGPT requires mindful consideration of usability, credibility, fairness, cost, and ethical transparency, elements that must be embedded into faculty training and curriculum design.41 A recent transparency index framework underscores the essential role of embedding accountability, interpretability, and stakeholder-informed design into AI systems for education.42
Educational Implications
To effectively integrate artificial intelligence (AI) into medical education, a tiered curriculum aligned with the competency-based medical education (CBME) framework has been widely recommended. At the foundational level, students should be introduced to core concepts such as algorithmic logic, data science fundamentals, and digital ethics, to build basic literacy and foster awareness of issues like bias, privacy, and accountability.43 At the intermediate level, case-based learning approaches can facilitate critical appraisal of AI-assisted clinical tools, enabling students to contextualize and apply these technologies in real-world decision-making.44 The advanced level may include electives or research projects focused on algorithm development, AI fairness, or human-machine collaboration, which promote deeper technical insight and reflective professionalism.1,45 Empirical examples further support this structure: Ngiam and Khor46 emphasized the integration of AI literacy and ethical reasoning to enhance students’ preparedness for AI-enabled healthcare, while institutions have begun embedding AI content within interdisciplinary modules across medicine, engineering, and data science.47 Such multi-level designs not only improve students’ conceptual understanding but also foster a sense of professional responsibility and critical engagement with emerging technologies in healthcare.
Ethical and Regulatory Considerations
Incorporating ethical principles into AI education is essential to ensure responsible use in clinical practice. Badal et al48 identified eight guiding principles, such as promoting equity, ensuring clinical relevance, and integrating social determinants, that highlight the need for fairness, transparency, and patient-centered care. Embedding these values into curricula can foster students’ ethical reasoning and contextual awareness. As AI reshapes healthcare and education, robust governance frameworks and faculty training are critical to balance innovation with accountability and ensure responsible implementation.49
AI systems should be consciously designed to mitigate rather than exacerbate health disparities, especially by ensuring access, inclusivity, and adaptability in low-resource settings. This includes designing tools that can operate with locally available data, favoring transparency and cost-effectiveness over black-box sophistication.38,50 Second, clinical relevance must be defined from the outset, ensuring that AI outcomes correspond with meaningful patient benefit and align with real-world clinical goals.3,51 Third, the reduction of overdiagnosis and overtreatment must be a target in AI development, especially in areas like cancer care, where AI tools may risk amplifying detection without improving survival.52,53
Furthermore, AI tools must demonstrate medical value; that is, they should improve health outcomes or reduce costs compared to existing standards.54 To achieve this, the early involvement of key stakeholders, such as clinicians and health economists, is essential.55,56 In addition, AI models must integrate the social and biological determinants of health, including socioeconomic status, environmental exposures, and chronic stress, to more accurately reflect the complex drivers of disease.57,58 These tools should be adaptable to local populations, prioritizing transferability and modular design over one-size-fits-all solutions.59
Beyond technical and clinical considerations, ethical AI education should also address academic integrity, privacy, and humanistic practice. Students’ use of AI in learning or assessments raises concerns about plagiarism and over-reliance, emphasizing the need for clear guidelines on responsible use and proper attribution. Data security and privacy must be highlighted, particularly when AI interacts with patient or student data, ensuring anonymization, informed consent, and secure handling. AI should augment rather than replace human judgment, maintaining patient-centered care and professional empathy, which can be reinforced through ethics discussions and communication training. Transparency and explainability of AI outputs are essential for fostering critical thinking and understanding system limitations. Moreover, AI applications must comply with legal and regulatory frameworks to clarify accountability and liability. Finally, ethical education should be adapted to diverse global contexts, promoting equitable access, culturally sensitive instruction, and scalable, low-cost training resources to bridge disparities in AI readiness.
Governance and Curriculum Frameworks for Responsible AI Integration
International consensus increasingly underscores the need for ethical guidelines and regulatory structures for AI integration in medical education. The FUTURE AI guideline, developed via a modified Delphi process with global experts, outlines six principles for trustworthy AI: fairness, universality, traceability, usability, robustness, and explainability, spanning technical, legal, clinical, and ethical dimensions across the AI lifecycle.60,61 Similarly, Delphi-based consensus in surgical training has produced frameworks addressing data protection, transparency, bias, and accountability in AI-driven tools.62
To operationalize these principles, educators propose curriculum strategies such as modular AI courses integrating AI literacy and ethics into existing bioethics programs. The Embedded AI Ethics Education Framework builds on established ethics curricula to target risks like misuse or bias, offering a practical roadmap for medical schools.30
Model frameworks aligned with governance principles include Trustworthy AI, Human-in-the-loop designs, and AI-augmented feedback systems. For instance, AI-based formative feedback in clinical skills training, such as MedSimAI simulations has improved performance assessment while maintaining educator oversight.63 Augmented feedback models, validated through expert consensus, further validate the pedagogical value of real-time data-driven guidance balanced with human judgement.64
Limitations and Future Directions
This review is limited by its English-only scope, potential bias from self-reported data, and the absence of longitudinal or interventional studies, which restricts our understanding of AI’s long-term impact on learners. A key limitation is the lack of more comparative studies, which reflects the early stage of research in this field. The heterogeneity in study designs and populations prevented the use of quantitative meta-analysis, and thus, a narrative synthesis approach was employed to summarize the findings across studies. Rapid advances in generative AI may also render some findings outdated. Future priorities include developing standardized AI-literacy frameworks, conducting long-term evaluations, and fostering interdisciplinary co-creation to ensure relevance and ethical soundness.65 Recognizing the significant regional disparities in healthcare resources and infrastructure, future efforts should tailor AI implementation strategies to local contexts. For example, resource-rich settings could focus on advanced AI models and multi-centre validation studies, while resource-limited regions may benefit from lightweight, scalable AI solutions and shared data platforms.54 Achieving global consensus on core AI competencies will be critical; however, these competencies should remain adaptable to diverse local capabilities to ensure both feasibility and practical impact. Moreover, the recent FUTURE-AI international consensus guideline emphasizes fairness, universality, traceability, usability, robustness, and explainability as key guiding principles for trustworthy healthcare AI systems.61 Incorporating such internationally endorsed guidelines into region-sensitive adoption pathways can help bridge the gap between high-resource and low-resource settings, enhancing both scalability and equity of AI deployment.
Conclusion
AI offers unprecedented opportunities to enhance medical education, but its value lies in complementing, not replacing human teaching. Embedding AI literacy, ethical reasoning, and critical appraisal into curricula is essential to address fairness, accountability, privacy, and transparency. With collaborative governance, institutions can harness AI’s potential while safeguarding professional values and patient-centered care.
Funding
BTCH 1st Young Talent Enlightenment Program (2024-2026) to Yuan Ren; The National Natural Science Foundation of China (8217053406).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Masters K. Artificial intelligence in medical education. Med Teach. 2019;41(9):976–13. doi:10.1080/0142159x.2019.1595557
2. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. doi:10.1371/journal.pdig.0000198
3. Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56. doi:10.1038/s41591-018-0300-7
4. Chatha WA. From Scalpel to Simulation: reviewing the Future of Cadaveric Dissection in the Upcoming Era of Virtual and Augmented Reality and Artificial Intelligence. Cureus. 2024;16(10):e71578. doi:10.7759/cureus.71578
5. Hui M, Sacoransky E, Chung A, Kwan BYM. Exploring the integration of artificial intelligence in radiology education: a scoping review. Current Problems in Diagnostic Radiology. 2025;54(3):332–338. doi:10.1067/j.cpradiol.2024.10.012
6. Bray NN, Wheeler D, Zumwalt J. AI-Enhanced Rural Medical Education: bridging Gaps and Building Trust. Acad Med. 2025;100(9S Suppl 1):S39–s42. doi:10.1097/acm.0000000000006105
7. Zhao C, Xu T, Yao Y, Song Q, Xu B. Comparison of case-based learning using Watson for oncology and traditional method in teaching undergraduate medical students. Int J Med Inform. 2023;177:105117. doi:10.1016/j.ijmedinf.2023.105117
8. Shalong W, Yi Z, Bin Z, et al. Enhancing self-directed learning with custom GPT AI facilitation among medical students: a randomized controlled trial. Med Teach. 2025;47(7):1126–1133. doi:10.1080/0142159x.2024.2413023
9. Hui Z, Zewu Z, Jiao H, Yu C. Application of ChatGPT-assisted problem-based learning teaching method in clinical medical education. BMC Med Educ. 2025;25(1):50. doi:10.1186/s12909-024-06321-1
10. Yu H, Zhao J, Su L, Zhang J. Application of simulation-based education in the instruction of medical students from non-radiology specialties. BMC Med Educ. 2025;25(1):966. doi:10.1186/s12909-025-07572-2
11. Cassidy DJ, Coe TM, Jogerst KM, et al. Transfer of virtual reality endoscopy training to live animal colonoscopy: a randomized control trial of proficiency vs. repetition-based training. Surg Endosc. 2022;36(9):6767–6776. doi:10.1007/s00464-021-08958-1
12. Hashimoto DA, Petrusa E, Phitayakorn R, Valle C, Casey B, Gee D. A proficiency-based virtual reality endoscopy curriculum improves performance on the fundamentals of endoscopic surgery examination. Surg Endosc. 2018;32(3):1397–1404. doi:10.1007/s00464-017-5821-5
13. Majeed AI. Comparison of Artificial Intelligence-based learning with the traditional method in the diagnosis of COVID-19 chest radiographs among postgraduate radiology residents. Khyber Med Univ J. 2024;16(2):140–144. doi:10.35845/kmuj.2024.23503
14. Huang YY, Deng YS, Liu Y, et al. A deep learning-based semiautomated workflow for triaging follow-up MR scans in treated nasopharyngeal carcinoma. iScience. 2023;26(12):108347. doi:10.1016/j.isci.2023.108347
15. Zhang Y, Deng Y, Zou Q, et al. Artificial intelligence for diagnosis and prognosis prediction of natural killer/T cell lymphoma using magnetic resonance imaging. Cell Rep Med. 2024;5(5):101551. doi:10.1016/j.xcrm.2024.101551
16. Deng Y, Huang Y, Jing B, et al. Deep learning-based recurrence detector on magnetic resonance scans in nasopharyngeal carcinoma: a multicenter study. Eur J Radiol. 2023;168:111084. doi:10.1016/j.ejrad.2023.111084
17. Ma M, Li Y, Gao L, et al. The need for digital health education among next-generation health workers in China: a cross-sectional survey on digital health education. BMC Medical Educ. 2023;23(1):541. doi:10.1186/s12909-023-04407-w
18. Weidener L, Fischer M. Artificial Intelligence in Medicine: cross-Sectional Study Among Medical Students on Application, Education, and Ethical Aspects. JMIR Med Educ. 2024;10:e51247. doi:10.2196/51247
19. Rjoop A, Al-Qudah M, Alkhasawneh R, et al. Awareness and Attitude Toward Artificial Intelligence Among Medical Students and Pathology Trainees: survey Study. JMIR Med Educ. 2025;11:e62669. doi:10.2196/62669
20. Allam AH, Eltewacy NK, Alabdallat YJ, Owais TA, Salman S, Ebada MA. Knowledge, attitude, and perception of Arab medical students towards artificial intelligence in medicine and radiology: a multi-national cross-sectional study. Eur Radiol. 2024;34(7):1–14. doi:10.1007/s00330-023-10509-2
21. Sit C, Srinivasan R, Amlani A, et al. Attitudes and perceptions of UK medical students towards artificial intelligence and radiology: a multicentre survey. Insights Imaging. 2020;11(1):14. doi:10.1186/s13244-019-0830-7
22. Naseer MA, Saeed S, Afzal A, Ali S, Malik MGR. Navigating the integration of artificial intelligence in the medical education curriculum: a mixed-methods study exploring the perspectives of medical students and faculty in Pakistan. BMC Med Educ. 2025;25(1):273. doi:10.1186/s12909-024-06552-2
23. Favorito FM, Collie L, Kennedy T, et al. A Survey of Perspectives and Educational Needs of Canadian Oncology Residents on Artificial Intelligence. J Cancer Educ. 2025;40(2):273–279. doi:10.1007/s13187-024-02509-7
24. Wang X, Fei F, Wei J, et al. Knowledge and attitudes toward artificial intelligence in nursing among various categories of professionals in China: a cross-sectional study. Front Public Health. 2024;12:1433252. doi:10.3389/fpubh.2024.1433252
25. Salih SM. Perceptions of Faculty and Students About Use of Artificial Intelligence in Medical Education: a Qualitative Study. Cureus. 2024;16(4):e57605. doi:10.7759/cureus.57605
26. Jackson P, Ponath Sukumaran G, Babu C, et al. Artificial intelligence in medical education - perception among medical students. BMC Medical Educ. 2024;24(1):804. doi:10.1186/s12909-024-05760-0
27. Gualda-Gea JJ, Barón-Miras LE, Bertran MJ, Vilella A, Torá-Rocamora I, Prat A. Perceptions and future perspectives of medical students on the use of artificial intelligence based chatbots: an exploratory analysis. Front Med Lausanne. 2025;12:1529305. doi:10.3389/fmed.2025.1529305
28. Sanad AH, Alsaegh AS, Abdulla HM, et al. Perceptions of Artificial Intelligence in Medicine Among Newly Graduated Interns: a Cross-Sectional Study. Cureus. 2024;16(10):e71216. doi:10.7759/cureus.71216
29. Roy AD, Das D, Mondal H. Efficacy of ChatGPT in solving attitude, ethics, and communication case scenario used for competency-based medical education in India: a case study. J Educ Health Promot. 2024;13:22. doi:10.4103/jehp.jehp_625_23
30. Quinn TP, Coghlan S. Readying medical students for medical AI: the need to embed AI ethics education. arXiv preprint arXiv:210902866. 2021.
31. Weidener L, Fischer M. Teaching AI Ethics in Medical Education: a Scoping Review of Current Literature and Practices. Perspect Med Educ. 2023;12(1):399–410. doi:10.5334/pme.954
32. Poalelungi DG, Musat CL, Fulga A, et al. Advancing Patient Care: how Artificial Intelligence Is Transforming Healthcare. J Pers Med. 2023;13(8):1214. doi:10.3390/jpm13081214
33. Alrashed FA, Ahmad T, Almurdi MM, et al. Incorporating Technology Adoption in Medical Education: a Qualitative Study of Medical Students’ Perspectives. Adv Med Educ Pract. 2024;15:615–625. doi:10.2147/amep.S464555
34. Joseph TS, Gowrie S, Montalbano MJ, et al. The Roles of Artificial Intelligence in Teaching Anatomy: a Systematic Review. Clin Anat. 2025;38(5):552–567. doi:10.1002/ca.24272
35. Duan S, Liu C, Rong T, Zhao Y, Liu B. Integrating AI in medical education: a comprehensive study of medical students’ attitudes, concerns, and behavioral intentions. BMC Medical Educ. 2025;25(1):599. doi:10.1186/s12909-025-07177-9
36. Abdellatif H, Al Mushaiqri M, Albalushi H, Al-Zaabi AA, Roychoudhury S, Teaching DS. Learning and Assessing Anatomy with Artificial Intelligence: the Road to a Better Future. Int J Environ Res Public Health. 2022;19(21):14209. doi:10.3390/ijerph192114209
37. Tejani AS, Elhalawani H, Moy L, Kohli M, Kahn CE. Artificial Intelligence and Radiology Education. Radiol. 2023;5(1):e220084. doi:10.1148/ryai.220084
38. Zhang J, Zhang ZM. Ethics and governance of trustworthy medical artificial intelligence. BMC Medical Informatics and Decision. Making. 2023;23(1):7. doi:10.1186/s12911-023-02103-9
39. Weiner EB, Dankwa-Mullan I, Nelson WA, Hassanpour S. Ethical challenges and evolving strategies in the integration of artificial intelligence into clinical practice. PLOS Digital Health. 2025;4(4):e0000810.
40. Sirasanagandla SR, Rajendran SS, Mogali SR, Bouchareb Y, Shaffi N, Al-Rahbi A. From Cadavers to Neural Networks: a Narrative Review on Artificial Intelligence Tools in Anatomy Teaching. Education Sciences. 2025;15(3):283.
41. Quttainah M, Mishra V, Madakam S, Lurie Y. Cost, Usability, Credibility, Fairness, Accountability, Transparency, and Explainability Framework for Safe and Effective Large Language Models in Medical Education: narrative Review and Qualitative Study. Original Paper JMIR AI. 2024;3:e51834. doi:10.2196/51834
42. Chaudhry MA, Cukurova M, Luckin R. A transparency index framework for AI in education. Springer. 2022;195–198.
43. Chan KS, Zary N. Applications and Challenges of Implementing Artificial Intelligence in Medical Education: integrative Review. JMIR Med Educ. 2019;5(1):e13930. doi:10.2196/13930
44. Ejaz H, McGrath H, Wong BL, Guise A, Vercauteren T, Shapey J. Artificial intelligence and medical education: a global mixed-methods study of medical students’ perspectives. Digit Health. 2022;8:20552076221089099. doi:10.1177/20552076221089099
45. Kolachalama VB, Garg PS. Machine learning and medical education. Npj Digital Med. 2018;1(1):54. doi:10.1038/s41746-018-0061-1
46. Ngiam KY, Khor IW. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019;20(5):e262–e273. doi:10.1016/s1470-2045(19)30149-4
47. Succi MD, Chang BS, Rao AS. Building the AI-Enabled Medical School of the Future. JAMA. 2025;333(19):1665–1666. doi:10.1001/jama.2025.2789
48. Badal K, Lee CM, Esserman LJ. Guiding principles for the responsible development of artificial intelligence tools for healthcare. Communicat Med. 2023;3(1):47. doi:10.1038/s43856-023-00279-9
49. Knopp MI, Warm EJ, Weber D, et al. AI-Enabled Medical Education: threads of Change, Promising Futures, and Risky Realities Across Four Potential Future Worlds. JMIR Med Educ. 2023;9:e50373. doi:10.2196/50373
50. Yu L, Zhai X. Use of artificial intelligence to address health disparities in low- and middle-income countries: a thematic analysis of ethical issues. Public Health. 2024;234:77–83. doi:10.1016/j.puhe.2024.05.029
51. Ahmed MI, Spooner B, Isherwood J, Lane M, Orrock E, Dennison A. A Systematic Review of the Barriers to the Implementation of Artificial Intelligence in Healthcare. Cureus. 2023;15(10):e46454. doi:10.7759/cureus.46454
52. Welch HG, Black WC. Overdiagnosis in Cancer. JNCI J National Cancer Inst. 2010;102(9):605–613. doi:10.1093/jnci/djq099
53. He J, Baxter SL, Xu J, Xu J, Zhou X, Zhang K. The practical implementation of artificial intelligence technologies in medicine. Nature Med. 2019;25(1):30–36. doi:10.1038/s41591-018-0307-0
54. Ciecierski-Holmes T, Singh R, Axt M, Brenner S, Barteit S. Artificial intelligence for strengthening healthcare systems in low- and middle-income countries: a systematic scoping review. NPJ Digit Med. 2022;5(1):162. doi:10.1038/s41746-022-00700-y
55. Abràmoff MD, Roehrenbeck C, Trujillo S, et al. A reimbursement framework for artificial intelligence in healthcare. NPJ Digit Med. 2022;5(1):72. doi:10.1038/s41746-022-00621-w
56. Nasarian E, Alizadehsani R, Acharya UR, Tsui K-L. Designing interpretable ML system to enhance trust in healthcare: a systematic review to proposed responsible clinician-AI-collaboration framework. Information Fusion. 2024;108:102412. doi:10.1016/j.inffus.2024.102412
57. Segar MW, Hall JL, Jhund PS, et al. Machine Learning-Based Models Incorporating Social Determinants of Health vs Traditional Models for Predicting In-Hospital Mortality in Patients With Heart Failure. JAMA Cardiol. 2022;7(8):844–854. doi:10.1001/jamacardio.2022.1900
58. Zhao Y, Wood EP, Mirin N, Cook SH, Chunara R. Social Determinants in Machine Learning Cardiovascular Disease Prediction Models: a Systematic Review. Am J Prev Med. 2021;61(4):596–605. doi:10.1016/j.amepre.2021.04.016
59. Yang J, Dung NT, Thach PN, et al. Generalizability assessment of AI models across hospitals in a low-middle and high income country. Nat Commun. 2024;15(1):8270. doi:10.1038/s41467-024-52618-6
60. Lee YM, Kim S, Lee YH, et al. Defining Medical AI Competencies for Medical School Graduates: outcomes of a Delphi Survey and Medical Student/Educator Questionnaire of South Korean Medical Schools. Acad Med. 2024;99(5):524–533. doi:10.1097/acm.0000000000005618
61. Lekadir K, Frangi AF, Porras AR, et al. FUTURE-AI: international consensus guideline for trustworthy and deployable artificial intelligence in healthcare. BMJ. 2025;388.
62. Collins JW, Marcus HJ, Ghazi A, et al. Ethical implications of AI in robotic surgical training: a Delphi consensus statement. Eur Urol Focus. 2022;8(2):613–622. doi:10.1016/j.euf.2021.04.006
63. Hicke Y, Geathers J, Rajashekar N, et al. MedSimAI: simulation and formative feedback generation to enhance deliberate practice in medical education. arXiv preprint. 2025;
64. Micallef J, Button D, Uribe Quevedo A, McClatchey C, King L, Dubrowski A. Defining the Nature of Augmented Feedback for Learning Intraosseous Access Skills in Simulation-Based Health Professions Education. Cureus. 2023;15(7):e41869. doi:10.7759/cureus.41869
65. Ang C-S. Developing AI literacy in healthcare education: bridging the gap in competency assessment. Discover Educ. 2025;4(1):372. doi:10.1007/s44217-025-00812-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.