")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Application of Adjustable Skin Stretchers in Repairing Wound-Related Defects
Authors Shen Z, Chen S, Duan Y, Yu J, Pan D, Dong J, Wang S, Li Q, Xiao Y, Yuan X
Received 9 March 2023
Accepted for publication 18 July 2023
Published 5 September 2023 Volume 2023:16 Pages 2409—2417
DOI https://doi.org/10.2147/CCID.S411870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Zhimin Shen,1,* Shiping Chen,2,* Yiqiang Duan,1 Juan Yu,3 Dayang Pan,4 Jiaxin Dong,1 Shanglong Wang,1 Qizhe Li,1 Yinlong Xiao,1 Xun Yuan1
1Department of Orthopedics, The Affiliated Hospital of Guizhou Medical University, Guiyang City, People’s Republic of China; 2Department of Orthopedics, The No.1 People’s Hospital of Qingzhen, Qingzhen City, People’s Republic of China; 3The Affiliated Stomatological Hospital of Guizhou Medical University, Guiyang City, People’s Republic of China; 4The 4th People’s Hospital of Guiyang, Guiyang City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yiqiang Duan, Department of Orthopedics, The Affiliated Hospital of Guizhou Medical University, No. 28, Guiyijie Road, Guiyang City, Guizhou Province, 550004, People’s Republic of China, Email [email protected] Juan Yu, The Affiliated Stomatological Hospital of Guizhou Medical University, No. 9, Beijing Road, Guiyang City, Guizhou Province, 550004, People’s Republic of China, Email [email protected]
Objective: To explore the application value of adjustable skin stretchers for repairing skin wound defects.
Methods: Twenty patients with skin defects were included in this study. The largest defect was measured to be 45.4 cm × 13.3 cm (length × width) and the smallest one was 4.4 cm × 3.2 cm (length × width). All patients were subjected to adjustable skin stretchers and the short- and long-term clinical efficacy was evaluated.
Results: The wounds of all enrolled patients were healed completely except for one patient with a dorsal foot infection (the patient requested to return to the local county hospital for further treatment), with a total satisfaction of 100%. Postoperative 3-month follow-up showed scar formation, a little local hyperpigmentation, normal skin elasticity, and intact organs of involved cases, thus signifying the significant impact of adjacent joint activities.
Conclusion: Adjustable skin stretchers can accurately control the tension on wound margins, breaking the limitation of previous stretchers to provide objective quantitative indicators for clinical application. These stretchers are characterized by high use-value and are worth promoting.
Keywords: adjustable skin stretchers, wound-related defects, wound repair
Introduction
Background
Rapid development of modern transportation and social industry has witnessed a significant increase of high-energy damage, along with its resulting skin and soft tissue defects.1 Traditional methods for skin defects treatment typically involve skin grafts or transfer flaps to cover the wound surface.2–4 Thinner skin grafts help to afford higher survival rate of skin, while this procedure is largely dependent on wound status and fails to repair the complex wounds exposed in skeletons, joints and muscle tendons.5 The postoperative texture and elasticity remain to be improved. In this regard, the flaps with blood vessels and fat can address this issue, while the wound defect in the donor region needs extra treatment and dermatologic examination is of necessity. Taking together, the currently prevailing methods are largely accompanied by skin discomfort and damage in the beauty and function of the donor area. Meanwhile, the function and beauty of the recipient area are also far from satisfaction. Besides, the high blood loss amount, complex surgical procedures and high cost threaten to hamper their wider deployment in clinical applications.6
In this regard, skin stretching technique has been proposed to alleviate the concerns in traditional treatments.6 Specifically, the margins of wounds can be stretched towards the central region and triggers complete closure of the wounds within a short time. This technique also applies to the large-area wound using mechanical loading to afford gradual traction of the skin, which is inherently realized by creep response, ductility, viscoelasticity and stress relaxation.7,8 Adjustable skin stretchers with low operation cost, straightforward technique and absence of second surgery are therefore quite appealing for repairing wound-related defects, since they greatly shorten wound healing time, minimize scarring and alleviate patient’s pain.9,10
The main purpose of this study was to assess the application value of adjustable skin stretchers for repairing skin wound defects of 20 skin-defect patients with broad range of wound areas. The effectiveness of adjustable skin stretchers which controlled the tension on wound margins, was systematically evaluated to provide quantitative indicators for clinical application. These stretchers are characterized by high use-value and are worth promoting.
Materials and Methods
Materials
Adjustable skin stretchers were provided by Henan Keke Biological Technology Co., Ltd. It mainly consisted of stretch rods, propulsion tubes, limit screws, spring coils, nuts, measuring rulers, L-shaped connectors, and Kirschner wires, which can be used in conjunction with bone needles to stretch the skin and adjust the pressure according to the skin blood flow (Figure 1).
 |
Figure 1 Schematic diagram of an adjustable skin distractor (A: drawbar, B: front nut, C: fastening screw, D: L-shaped connecting rod, E: measurement scale, F: elastic ring, G: propelling tube, H: rear nut). |
Participants
Twenty patients (male: 13, female: 7; mean age, 47 years old) with skin defects who came to our hospital from September 2016 to September 2018 were enrolled in this study. Among these, 6 had open fractures with soft tissue defects, 7 had avulsion injuries, 4 had postoperative surgical incision nonunion, 1 had bedsore, 1 had infection and expansion, and 1 had inflammatory necrosis. The largest area of skin defect was measured to be 45.4 cm × 13.3 cm (length × width) and the smallest was 4.4 cm × 3.2 cm (length × width). This study was approved by the Ethics Committee of The Affiliated Hospital of Guizhou Medical University, NO. 2018 (134). All the patients provided informed consent for the case details to be published. The patients were also well aware of the fact that these consent forms were for publication of the case details and images. The research was complying with the guidelines for human studies and conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Exclusion Criteria
The main exclusion criteria in this study were listed as follows: (1) Patients with severe malnutrition, coagulopathy, and/or skin blood flow disorders around the wound. (2) Patients with infectious skin diseases who had to receive postoperative management in separate rooms. (3) Patients with insufficient normal skin around the wound.
Surgical Procedures
The boundary of the skin defect was subjected to complete clearing and digitally photographed. Preoperative preparation, such as intravenous antibiotics and anesthesia, were then administered. Subsequently, routine disinfection, draping, thorough debridement around the wound edges, trimming of the wound edges, and removal of the dead skin were carried out in sequence. At the edge of approximately 0.5–1.5 cm was an ideal distance of inflammatory skin or abnormal brittle skin. A Kirschner wire (diameter: 1.5–2.0 nm) was used to penetrate through the skin at approximately 1–1.5 cm along the margin of wound (based on clinical judgment). The exposed part of the wire was approximately 2–3 cm, which was then used to connect the two sides of the Kirschner wire to the skin stretcher, adjust the pressure, and close the skin on both sides of the wound (Figure 2). The pressure was adjusted every day until the skin was closed. Direct wound closure can be realized without extra pressure or suture or local skin shrinking. Antibiotics was administered 24–48 hours after surgery and the skin color around the stretch was monitored. The amount of stretch tension was adjusted, the dressing was changed, and symptomatic support treatment was provided.
 |
Figure 2 Schematic illustration of the surgical procedures. |
Postoperative Care
The tension of the skin stretcher was adjusted on the first day after surgery. Tension was further adjusted 2–3 times per day according to the wound status and maintained at 3–5 kg. The skin was closed 7–10 days after surgery using an indwelling suture, which was removed upon complete wound healing. The skin closure was preserved for 2–3 days to ensure that the skin was completely sutured before removal.
Results
Tension Profiles, Stretch Time and Suture Time
Among the 20 patients, the maximum skin and soft tissue defects were 45.4 cm ×13.3 cm and the minimum were 4.4 cm × 3.2 cm. As shown in Table 1, the maximum intraoperative tension of the wound was 5 kg and the minimum was 3 kg, with an average value of 3.85 kg. The maximum postoperative tension of the wound was 5 kg and the minimum was 2 kg, with an average value of 3.70 kg. The maximum operation time of the skin stretching was 42 minutes and the minimum was 14 minutes, with an average of 20.6 minutes. The wound was sutured when the distance between the two wounds was less than 0.5 cm, and the average stretching time was 6.95 days. The experimental data were subjected to independent sample t-test in this study. The maximum reduction rate of the intraoperative wound width was 100% and the minimum was 18.6%, with an average rate of 45.0%. Of the 20 patients, all had completely healed wounds (Table 2, Figures 3 and 4), except for one patient with a dorsal foot infection (Kirschner wire was cut and discarded), who was subjected to drainage-assisted irrigation under negative pressure but unfortunately characterized by incomplete wound healing. The patient was discharged and transferred to the local county hospital for further treatment. The patient satisfaction survey was conducted by telephone follow-up, occasionally accompanied by outpatient follow-up. The results show that 13 cases were very satisfied, 6 cases were satisfied, and 1 case was basically satisfied. The total satisfaction was 100%.
 |
Table 1 Descriptive Statistics of Preoperative Tension, Postoperative Tension, Operative Distraction Time, Postoperative Distraction Time in 20 Wounds |
 |
Table 2 Ratio of Shortening During and After Surgery in 20 Wounds |
 |
Figure 3 Histogram of wound width changes in 20 patients. Notes: Horizontal axis represents the patient number; vertical axis represents the wound width. |
 |
Figure 4 Ratio of shortening during and after surgery in 20 wounds. Notes: The postoperative descent ratio of the wound width was significantly lower than the intraoperative descent ratio. |
Typical Case 1
A 53-year-old female patient who had a car accident with open fracture in the left calf and a skin defect with an exposed bone covering 15.5 cm ×7.8 cm ×1.5 cm (length × width × depth) is shown in Figure 5a. A 3-kg traction force during and after surgery was used (Figure 5b and c).
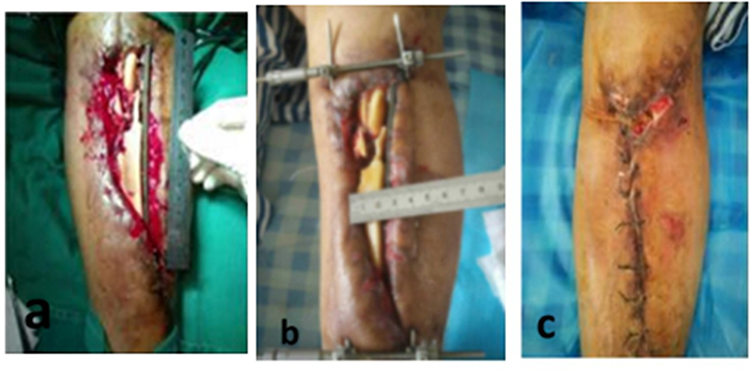 |
Figure 5 The wound image of typical case 1. (a) preoperation, (b) postoperative day 4, (c) postoperative day 15. The length, width and depth of the wound are 15.5 cm, 7.8 cm and 1.5 cm, respectively. The area is 120.9 cm2. |
Typical Case 2
A 37-year-old male patient with buttock skin necrosis 5 days after a car accident injury. The buttock skin defect size was measured to be 45.4 cm ×13.3 cm × 2 cm (length × width × depth), as shown in Figure 6a. A 5-kg traction force during and after surgery was used (Figure 6b–d).
 |
Figure 6 The wound image of typical case 2. (a) preoperation, (b) VSD was placed a week later, (c) intraoperation, (d) postoperative day 17. The length, width and depth of the wound are 45.4 cm, 13.3 cm and 2 cm, respectively. The area is 603.82 cm2. |
Typical Case 3
A 28-year-old male developed a skin defect in the left ankle caused by a car accident (Figure 7a). This was repaired with a flap of sural nerve nutritional vessels, and the flap area was 19.1 cm ×3.3 cm ×0.7 cm (length × width × depth), as shown in Figure 7b. A 5-kg traction force was stretched for 25 minutes and the wound at the donor site was sutured immediately after surgery (Figure 7b and c).
 |
Figure 7 The wound image of typical case 3. (a) preoperation, (b) intraoperation, (c) postoperative day 15. The length, width and depth of the wound are 19.1 cm, 3.3 cm and 0.7 cm, respectively. The area is 63.03 cm2. |
Discussion
Traumatic, skin, and soft tissue defects of the limbs caused by various reasons are common cases in orthopedic clinical practice.11 High-tension wounds are prone to result in skin necrosis after direct suture. Specifically, wounds cannot be closed immediately and the subcutaneous musculoskeletal tissues are directly exposed, thereby leading to highly susceptible situation. The adjustable skin retractor takes advantage of the elasticity that is inherent in skin, which is stretched by the force. The healthy skin on both sides of the wound is pulled toward the central region by an external force. Skin elasticity and mechanical stretchability are used to disperse marginal tension into the surrounding skin, and dynamic stretching of the tissue is maximized through the stretching effect to assure wound closing.12 Medina used skin stretchers to treat the incision after forearm bone fascia compartment reduction, thus avoiding skin grafting.13 Santiago et al used self-made continuous external tissue expanders to treat 14 patients with large soft tissue defects of the limbs due to blast injuries, including 12 patients (85.7%) who received second suturing on the wound surface, and 2 patients who underwent reoperation for surgical flap transplantation.14 Fletcheret et al designed a skin stretcher based on the Ilizarov frame,15 the skin and soft tissue defects were reconstructed while treating the open fractures. Verhaegen, Bashir, and Senchenkovet et al also used self-modified skin stretchers to treat skin and soft tissue defects.16–18 Their research further confirmed the significant effect of skin stretchers on repairing skin and soft tissue defects. Application of closure skin stretching can replace skin grafting or skin transplantation, reduce surgical risks and traumas for patients with chronic diseases, and accelerate wound healing.19
Adjustable skin stretchers are characterized by the combined merits: (1) it is an accurate tension measurement device which provides quantitative indicators for clinical application research, (2) it can monitor the changes in the wound surface and surrounding tissues, (3) small surgical trauma can be treated under local anesthesia, which has little effect on the skin itself, without interfering with normal healing, (4) the lightweight stretcher with simple structure has favorable biocompatibility and exerts little impact on patient’s activities, (5) it is suitable for irregular skin defects and can be used in combination, and (6) it is affordable.18
Here we also clarify the contraindications are as follows for clinical treatment: (1) patients with severe malnutrition and/or coagulopathy, (2) patients with skin blood flow disorders around the wound, (3) patients with infectious skin diseases, (4) patients who cannot comply with postoperative treatment (4) patients share less-than-expected healthy skin around the wound. We would also suggest that if a control group with similar defect size is involved in future study, the comparison can reinforce the effectiveness of outcome parameters.
Although skin stretchers have been used for more than 40 years, previous endeavors focus mostly on the adjustment of stretch tension completely based on experience. Accurate tension measurement device that can provide quantitative indicators for clinical application research remains largely unavailable for a quite long period, adjustable skin stretchers provide a perfect solution. Note that flap transplantation, skin expansion, skin stretching, and tissue engineering of skin have their own advantages and disadvantages, optimum treatment plans for involved patients differ from each other. If an adjustable skin stretcher is required for treating skin and soft tissue defects, then its use coupled with a quantitative system is more conducive for clinical operations. Due to the small number of cases, objective indicators might be lacking when assessing skin inflammation and determining the distance between the needle entry point and the skin defect area. Based on clinical experience, objective indicators might also be lacking when adjusting the traction force according to the blood supply and patient’s tolerance levels. The combined issues pose additional difficulties in clinical operation, the detailed information of traction force and wound surface area await further statistical exploration and improvement.
Data Sharing Statement
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Written Consent Statement
All the patients provided informed consent for the case details to be published. The patients were also well aware of the fact that these consent forms were for publication of the case details and images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declared that they have no competing interest.
References
1. Canton G, Santolini F, Stella M, Moretti A, Murena L, Murena L. Strategies to minimize soft tissues and septic complications in staged management of high-energy proximal tibia fractures. Eur J Orthop Surg Traumatol. 2020;30:1–10. doi:10.1007/s00590-019-02619-9
2. Cheng LF, Lee JT, Hsu H, Wu MS. Simple skin-stretching device in assisted tension-free wound closure. Ann Plast Surg. 2017;78:S52. doi:10.1097/SAP.0000000000001006
3. Dong Q, Gu G, Wang L, et al. Application of modified adjustable skin stretching and secure wound-closure system in repairing of skin and soft tissue defect. Chin J Repar Recons Surg. 2017;31:1481–1484.
4. Wolfe SW, Hotchkiss RN. Green’s Operative Hand Surgery.
5. Wang G, Zhang X, Zhang Z, Wei Z. Clinical study on a skin stretching technique with adjustable external fixators to treat skin defects. Medicine. 2020;99:37.
6. Xu J, Chang R, Zhang W, et al. Skin stretch suturing with Nice knots in the treatment of small- or medium-sized wounds. J Orthop Surg Res. 2020;15:488. doi:10.1186/s13018-020-02007-8
7. Hussain SH, Limthongkul B, Humphreys TR. The biomechanical properties of the skin. Dermatol Surg. 2013;39:193–203. doi:10.1111/dsu.12095
8. Song M, Zhang Z, Liu T, et al. EASApprox® skin‑stretching system: a secure and effective method to achieve wound closure. Exp Ther Med. 2017;14:531–538. doi:10.3892/etm.2017.4539
9. Zhou J, Zhao Y, Yang W, et al. Use of mechanical stretching to treat skin graft contracture. J Burn Care Res. 2020;41:892–899. doi:10.1093/jbcr/iraa033
10. Alam M, Roongpisuthipong W, Kim NA, et al. Utility of recorded guided imagery and relaxing music in reducing patient pain and anxiety, and surgeon anxiety, during cutaneous surgical procedures: a single-blinded randomized controlled trial. J Am Acad Derma. 2016;75:585–589. doi:10.1016/j.jaad.2016.02.1143
11. Azoury SC, Stranix JT, Othman S, Kimia R, Kovach SJ. Outcomes following soft-tissue reconstruction for traumatic lower extremity defects at an orthoplastic limb salvage center: the need for lower extremity guidelines for salvage (L.E.G.S.). Orthop Surg. 2021;3:1–7. doi:10.1016/j.orthop.2020.12.003
12. Flynn C, Taberner A, Nielsen P. Modeling the mechanical response of in vivo human skin under a rich set of deformations. Anns Biomed Eng. 2011;39:1935. doi:10.1007/s10439-011-0292-7
13. Medina C, Spears J, Mitra A. The use of an innovative device for wound closure after upper extremity fasciotomy. Hand. 2008;3:146–151. doi:10.1007/s11552-007-9082-y
14. Santiago GF, Bograd B, Basile PL, Howard RT, Fleming M, Valerio IL. Soft tissue injury management with a continuous external tissue expander. Ann Plast Surg. 2012;69:418–421. doi:10.1097/SAP.0b013e31824a4584
15. Fletcher MDA, Solomin LN. Definitive management of significant soft tissue loss associated with open diaphyseal fractures utilising circular external fixation without free tissue transfer, a comprehensive review of the literature and illustrative case. Euro J Orthop Surg Trauma. 2015;25:65–75. doi:10.1007/s00590-014-1441-0
16. Verhaegen PDHM, van der Wal MBA, Bloemen MCT, et al. Sustainable effect of skin stretching for burn scar excision: long-term results of a multicenter randomized controlled trial. Burns. 2011;37:1222–1228. doi:10.1016/j.burns.2011.04.018
17. Bashir AH. Wound closure by skin traction: an application of tissue expansion. Br J Plast Surg. 1987;40:582–587. doi:10.1016/0007-1226(87)90151-2
18. Senchenkov A, Manders EK. Tissue expansion. Res Gate. 2010; 2010:21–27.
19. Sharma M, Balasubramanian D, Thankappan K, et al. Propeller flaps in the closure of free fibula flap donor site skin defects. Ann Plast Surg. 2013;71:76–79. doi:10.1097/SAP.0b013e318248b813
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.