Back to Journals » Cancer Management and Research » Volume 12
Application of 2011 International Federation for Cervical Pathology and Colposcopy Terminology on the Detection of Vaginal Intraepithelial Neoplasia
Authors Zhou Q, Zhang F, Sui L ![]() , Zhang H, Lin L, Li Y
, Zhang H, Lin L, Li Y
Received 11 April 2020
Accepted for publication 24 June 2020
Published 17 July 2020 Volume 2020:12 Pages 5987—5995
DOI https://doi.org/10.2147/CMAR.S257875
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Qi Zhou,* Feifei Zhang,* Long Sui, Hongwei Zhang, Lin Lin, Yanyun Li
Obstetrics and Gynecology Hospital of Fudan University, Shanghai 200011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanyun Li Tel +86 21 33189900
Fax +86 21 63450944
Email [email protected]
Purpose: To evaluate the colposcopic accuracy of the detection of vaginal intraepithelial neoplasia (VaIN) according to the colposcopic terminology for the vagina from the 2011 International Federation of Cervical Pathology and Colposcopy (IFCPC).
Methods: A total of 467 women who were suspected of having VaIN and underwent colposcopy at Obstetrics and Gynecology Hospital of Fudan University from January to December 2018 were included in this retrospective cohort study. The 2011 IFCPC revised terminology for the vagina was applied, and the agreement between colposcopic diagnosis and vaginal biopsy pathology was analysed.
Results: Agreement between colposcopy and pathology was 69.16% (kappa=0.437, p< 0.001), with 23.34% overestimated and 7.49% underestimated diagnosis for colposcopy. The agreement was the lowest (35.71%) in the high-grade VaIN group, which was significantly different from that of other lesion grade groups (p< 0.01). Among grade 1 findings, thin acetowhite epithelium was the most frequent (80.51%). Grade 2 findings and vascular patterns were rare. The positive predictive values of the micropapillary pattern were 55.98% for low-grade VaIN and 5.98% for high-grade VaIN. The specificity of iodine negativity was 10.92% for low-grade VaIN and 8.30% for high-grade VaIN. There were significant differences in the maximum size of single lesions and in the number of lesions among different grade lesion groups.
Conclusion: The agreement between colposcopy findings utilizing the 2011 IFCPC terminology and vaginal pathology is moderate, and more definite findings for high-grade VaIN may be needed. The micropapillary pattern can be considered an alternative low-grade finding, while iodine staining is nonspecific for all lesions. Scattered and spotty lesions suggest low-grade VaIN, while large single lesions suggest high-grade VaIN.
Keywords: colposcopy, vaginal intraepithelial neoplasia, VaIN, International Federation of Cervical Pathology and Colposcopy, IFCPC, terminology, cytology, human papillomavirus, HPV
Introduction
Vaginal intraepithelial neoplasia (VaIN) is considered to be a precursor of vaginal carcinoma, and the incidence has increased steadily over several decades, reaching approximately 0.2–0.6/100,000 in some reports.1–4 VaIN is commonly associated with human papillomavirus (HPV) infection, and HPV is found in approximately 90–98% of cases of VaIN.5,6 The American Society for Colposcopy and Cervical Pathology (ASCCP) and the College of American Pathologists (CAP) classified VaIN into low-grade VaIN and high-grade VaIN.7 Low-grade VaIN has a high rate of spontaneous regression and a low risk of progression to malignancy, while high-grade VaIN has a high risk of recurrence and progression to invasive vaginal cancer.8–11
For VaIN, different lesions require different therapeutic approaches; thus, a proper diagnosis is important. Since VaIN is often asymptomatic, its diagnosis is suspected in cases of abnormal cytology, followed by colposcopy and colposcopically guided biopsy of suspicious areas.1,12 There is general agreement that colposcopy plays a vital role in the detection of VaIN; however, it is more difficult for colposcopists to predict the histopathology of vaginal lesions than of cervical lesions. Studies have shown that the colposcopic characteristics of VaIN are extremely variable and nonspecific due to usually showing areas with varying degrees of acetowhite epithelium, abnormal vessel patterns and varying degrees of Lugol’s iodine staining. The histopathology can be more severe than that implied by the colposcopic impression in vaginal lesions. Boonlikit and Indraccolo analysed the consistency between colposcopic patterns of VaIN and histopathology and showed that vaginal colposcopy poorly predicted the severity of vaginal lesions.9,13,14
Worldwide, there was no uniform standard for colposcopic findings of VaIN until the International Federation for Cervical Pathology and Colposcopy (IFCPC) revised the colposcopic nomenclature in 2011, in which the colposcopic terminology for the vagina was included for the first time.15 The nomenclature provides standardized interpretations of the colposcopic findings of vaginal lesions and organizes a comprehensive classification system. However, due to limited reports and data on vaginal lesions, the vaginal colposcopic terminology is mostly based on cervical lesion patterns. Clinical evaluation studies on the applicability of the 2011 IFCPC terminology for the vagina are extremely scant.9,16
The aim of this study was to evaluate the application of the 2011 IFCPC terminology on the detection of VaIN. In this study, we analysed the colposcopic accuracy and significance of individual findings according to the 2011 IFCPC classification. Other findings, such as the micropapillary pattern and the maximum size of single lesions, were also analysed.
Materials and Methods
This was a retrospective cohort study. From January 2018 to December 2018, a total of 467 women with clinically suspected VaIN who underwent colposcopy at the Obstetrics and Gynecology Hospital of Fudan University were included. The inclusion criteria were as follows: abnormal cytological results, positive high-risk HPV testing (Hybrid Capture II or Cobas HPV test) or suspicious clinical manifestations. Abnormal cytological results included atypical squamous cells of undetermined significance (ASC-US), low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion (ASC-H), squamous cell carcinoma (SCC) and atypical glandular cells (AGC). Suspicious clinical manifestations included abnormal vaginal discharge/bleeding, recurrent erosion, polyp, cyst, condylomas and gross neoplasm. The exclusion criteria were as follows: vaginal pathology results obtained within the previous year; pelvic radiotherapy; pervious ablation therapy of the vagina such as by laser, cryotherapy and focused ultrasound; inadequate colposcopy examination; or incomplete data without histopathologic diagnosis. All the women signed informed consent forms before the colposcopy, and institutional review board approval was obtained properly.
Colposcopic examinations and diagnoses were performed by 3 experienced colposcopists who had at least 5 years of experience in colposcopic diagnosis with 2011 IFCPC nomenclature. A Leisegang BG/LED Y/C optoelectronic integrated digital colposcopy system (Leisegang Feinmechanik Optik GmbH, Berlin, Germany) was used to observe colposcopic patterns and measure the size of the lesions; images were obtained by an optical camera (Canon EOS600D). All colposcopic examinations were performed following a standard colposcopy protocol, including the application of 5% acetic solution, Lugol’s iodine solution for the Schiller test and a colposcopy-directed biopsy, which was taken at the site most suspected of VaIN.17
Based on the 2011 IFCPC terminology of the vagina,15 a detailed description of the colposcopic findings and initial diagnosis were recorded. (1) General assessment: adequate or inadequate for the reason; whether the patient had undergone hysterectomy. (2) Normal colposcopic findings: squamous epithelium: mature or atrophic. (3) Abnormal colposcopic findings: location and total size of the lesion; the maximum size of single lesions and the number of lesions; minor changes including thin acetowhite epithelium, fine punctuation and fine mosaic; major changes including dense acetowhite epithelium, coarse punctuation and coarse mosaic; suspicious for invasion including atypical vessels, fragile vessels, irregular surface, etc.; nonspecific findings including iodine negativity, leukoplakia and columnar epithelium (adenosis). (4) Miscellaneous findings: erosion, condyloma, polyp, cyst, endometriosis, etc. (5) Finally, an initial diagnosis, which was classified as normal or benign lesion, LSIL, HSIL or invasive carcinoma, was proposed by the same colposcopist based on the documents above. Although the micropapillary pattern, which was defined as an area of acetowhite with irregular micropapillary surface, was not included in the 2011 IFCPC terminology, it was indicated to be associated with VaIN in some studies.9,18 Thus, we also considered and analysed the micropapillary pattern separately.
Vaginal biopsy was performed at the most suspicious areas under colposcopy. Histopathological diagnoses, classified as normal or benign lesion, LSIL, HSIL, or carcinoma (including microinvasive carcinoma and invasive carcinoma) according to the 2012 Lower Anogenital Squamous Terminology (LAST),7 were made by two consultant pathologists in our hospital and taken as the gold standard for diagnosis.
Statistical analysis was performed using the Statistical Package for Social Sciences Version 19.0 Software (SPSS 19.0). Consistency analysis between colposcopic diagnosis and vaginal histopathology involved determining the frequency of perfect agreement, agreement within one grade (which were assessed with the weighted kappa statistic), overestimated diagnosis and underestimated diagnosis. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), false positive rate (FPR), false negative rate (FNR) and Youden Index (YI, sensitivity + specificity − 1) were used to assess accuracy and predictability. The chi-squared test or Wilcoxon rank-sum test was used to compare the coincidence rates among different categorical variables. Analysis of variance (F-test) or the Kruskal–Wallis test was used for comparison of quantitative variables among groups. The Spearman rank correlation coefficient was used to assess the correlations among different characteristic variables. Confidence intervals (95% CI) were calculated where appropriate. Any P value less than 0.05 was considered statistically significant.
Results
Agreement Between Colposcopic Diagnosis and Vaginal Histopathology
Perfect agreement between the IFCPC classification-based colposcopic diagnosis and vaginal histopathology was achieved for 69.16% (323/467) of cases, with a consistency of kappa=0.437 (p<0.001). Agreement within one grade occurred for 98.72% (461/467) of cases, with a consistency of kappa=0.977 (p<0.001). For the histopathologically diagnosed normal/benign, LSIL, HSIL and carcinoma groups, perfect agreement between colposcopic diagnosis and vaginal histopathology was achieved for 66.89% (196/293), 75.16% (115/153), 35.71% (5/14) and 100% (7/7) of cases, respectively. The difference in perfect agreement among the four groups was statistically significant (χ2=13.756, p<0.01). Among the colposcopic diagnoses, 109 were overestimated (23.34%, 109/467), and 35 were underestimated (7.49%, 35/467). Within two or more grades, five diagnoses were overestimated, while one was underestimated (Table 1).
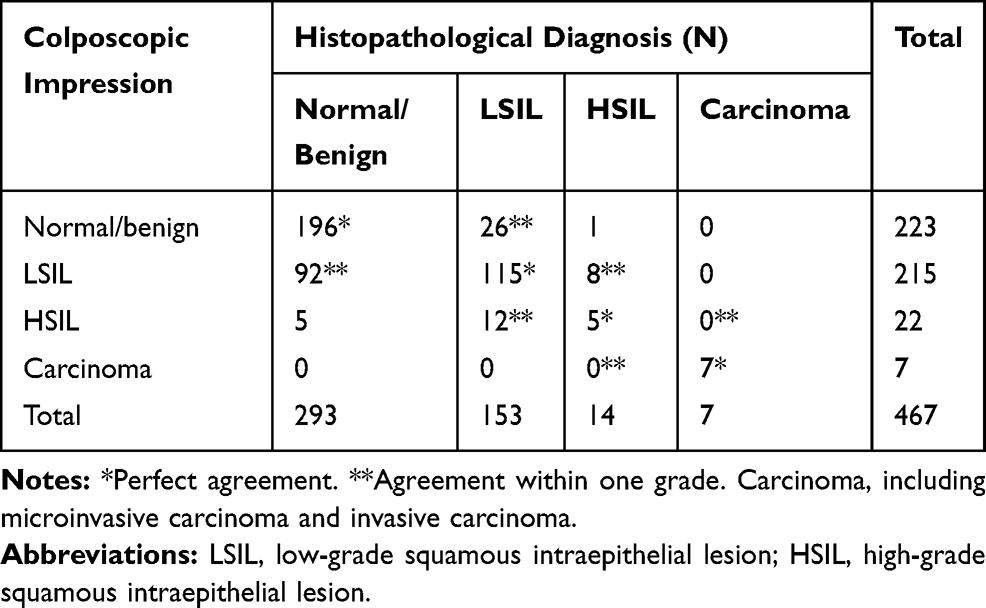 |
Table 1 Agreement Between Colposcopic Diagnosis and Vaginal Histopathology |
When taking HSIL as the cutoff, the sensitivity, specificity, FPR, FNR, PPV and NPV of colposcopic diagnosis were 57.14% (12/21), 96.19% (429/446), 3.81%, 42.86%, 41.38% (12/29) and 97.95% (429/438), respectively. When taking LSIL instead of HSIL as the cutoff, the sensitivity, specificity, FPR, FNR, PPV and NPV of colposcopic diagnosis were 84.48% (147/174), 66.89% (196/293), 33.11%, 15.52%, 60.25% (147/244) and 87.89% (196/223), respectively.
Evaluation of the 2011 IFCPC Colposcopic Findings for VaIN
The correlation between colposcopic findings and vaginal histopathology is shown in Table 2. Thin acetowhite epithelium (80.51%, 316/467), dense acetowhite epithelium (6.00%, 28/467), iodine negativity (91.86%, 429/467) and erosion (8.99%, 42/467) were the most common findings in Grade 1 patterns, Grade 2 patterns, nonspecific patterns and miscellaneous findings, respectively. Among the 429 women who had iodine negativity, 310 were associated to thin acetowhite and 31 were associated to dense acetowhite. Eighty-nine patients had iodine negativity as only abnormal finding (not associated to other grade I or II abnormality), 1 in which was associated with LSIL lesions, 14 in which were associated with HSIL lesions and 74 were benign or normal.
 |
Table 2 Correlation of Colposcopic Findings in the 2011 IFCPC Nomenclature and Vaginal Histopathology |
The diagnostic value of individual colposcopic findings in the 2011 IFCPC terminology in predicting vaginal pathology at different cutoffs (LSIL+ and HSIL+ lesions) was calculated, including the common findings, such as thin acetowhite epithelium, dense acetowhite epithelium, iodine negativity and erosion (Table 3). In addition, atypical vessels and masses could be seen in all cancer patients.
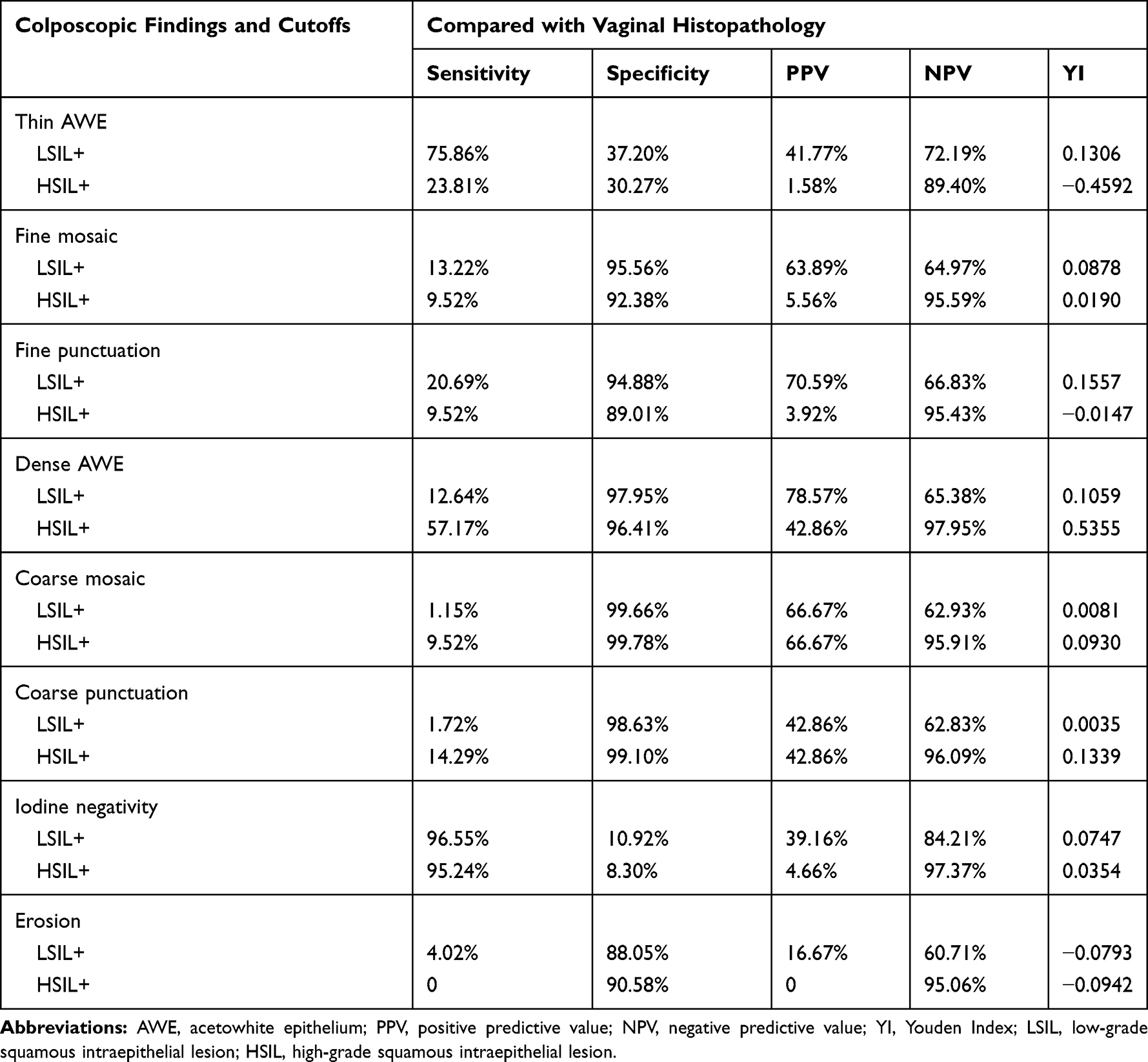 |
Table 3 Diagnostic Value of Individual Colposcopic Findings in Predicting Vaginal Pathology at Different Cutoffs |
Other Colposcopic Findings and Clinical Characteristics
The micropapillary pattern was observed in 184 women (39.40%, 184/467). Specifically, it was observed in 92 (60.13%, 92/153) of the 153 women with a histopathologic diagnosis of LSIL and in 9 (64.29%, 9/14) of the 14 women with HSIL, and there was no significant difference in the frequency between the two groups (F=0.093, p=0.761). When taking LSIL as the cutoff, the sensitivity, specificity, PPV, NPV and YI of micropapillary patterns were 59.20% (103/174), 72.35% (212/293), 55.98% (103/184), 74.91% (212/283) and 0.3155, respectively. When taking HSIL as the cutoff, the sensitivity, specificity, PPV, NPV and YI of micropapillary patterns were 52.38% (11/21), 61.21% (273/446), 5.98% (11/184), 96.47% (273/283), and 0.1359, respectively.
The correlation between hysterectomy and vaginal lesions is shown in Table 4. In detail, 23 (33.82%, 23/68) of the 68 women who underwent hysterectomy and 151 (37.84%, 151/399) of the 399 who did not undergo hysterectomy were diagnosed with vaginal lesions by histopathology. Forty-five (15.36%, 45/293) of the 293 women who were histopathologically diagnosed with normal or benign lesions, 15 (9.8%, 15/153) of the 153 with LSIL, 4 (28.57%, 4/14) of the 14 with HSIL and 4 (57.14%, 4/7) of the 7 with carcinoma had undergone hysterectomy. There was a statistically significant difference between the number of patients that did and did not undergo hysterectomy among the different lesion grade groups (p<0.01).
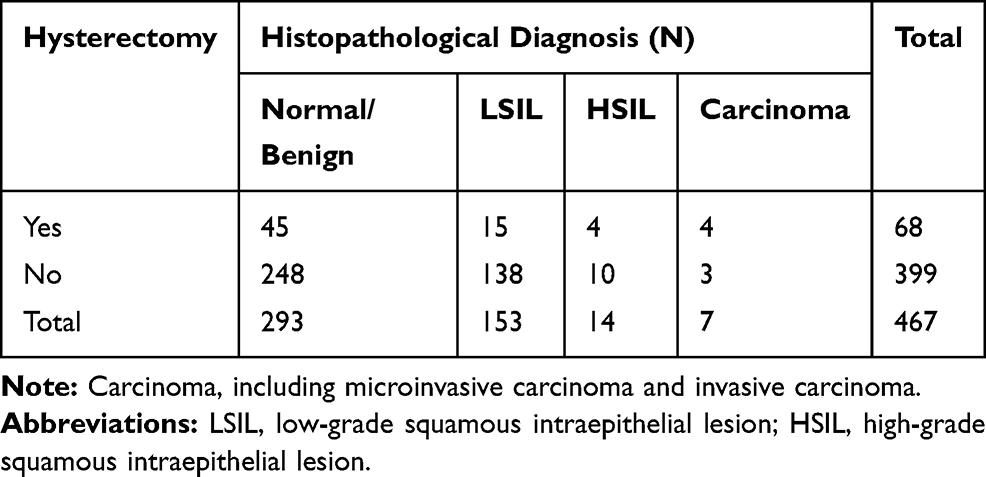 |
Table 4 Hysterectomy and Vaginal Histopathological Diagnosis |
The averages of the total lesion size for women with histopathologic diagnoses of normal or benign lesions, LSIL, HSIL and carcinoma were 4.12±6.57 cm2, 3.01±3.48 cm2, 3.79±2.38 cm2 and 4.71±3.07 cm2, respectively. There was a poor correlation between the total size and grade of the vaginal lesions (F=1.383, p=0.247). The averages of the maximum size of single lesions in women with histopathologic diagnoses of normal or benign LSIL, HSIL and carcinoma were 2.18±4.80 cm2, 1.92±2.52 cm2, 2.29±2.01 cm2, and 4.71±3.07 cm2, respectively. There was a significant linear trend between the maximum size of single lesions and the vaginal lesion grade (p<0.001). The mean numbers of lesions in women with histopathologic diagnoses of normal or benign lesions, LSIL, HSIL and carcinoma were 8.00±13.82, 4.12±6.84, 4.07±4.99 and 1, respectively. The differences in the numbers of lesions among different grade lesion groups were statistically significant (F=4.423, p<0.01).
The correlation between location and vaginal lesion grade is shown in Table 5. There were significant differences in the frequencies of VaIN among the four sides of the vaginal wall (anterior, left, right and posterior) (p<0.001). For high-grade VaIN or above, the posterior wall was the most common site (8/28), and the anterior wall was the least common (7/28). The frequency of VaIN (45.18%, 211/467) in the upper third of the vagina was much higher than that in the lower two-thirds (3.21%, 15/467). This was the same for any side of the vaginal wall.
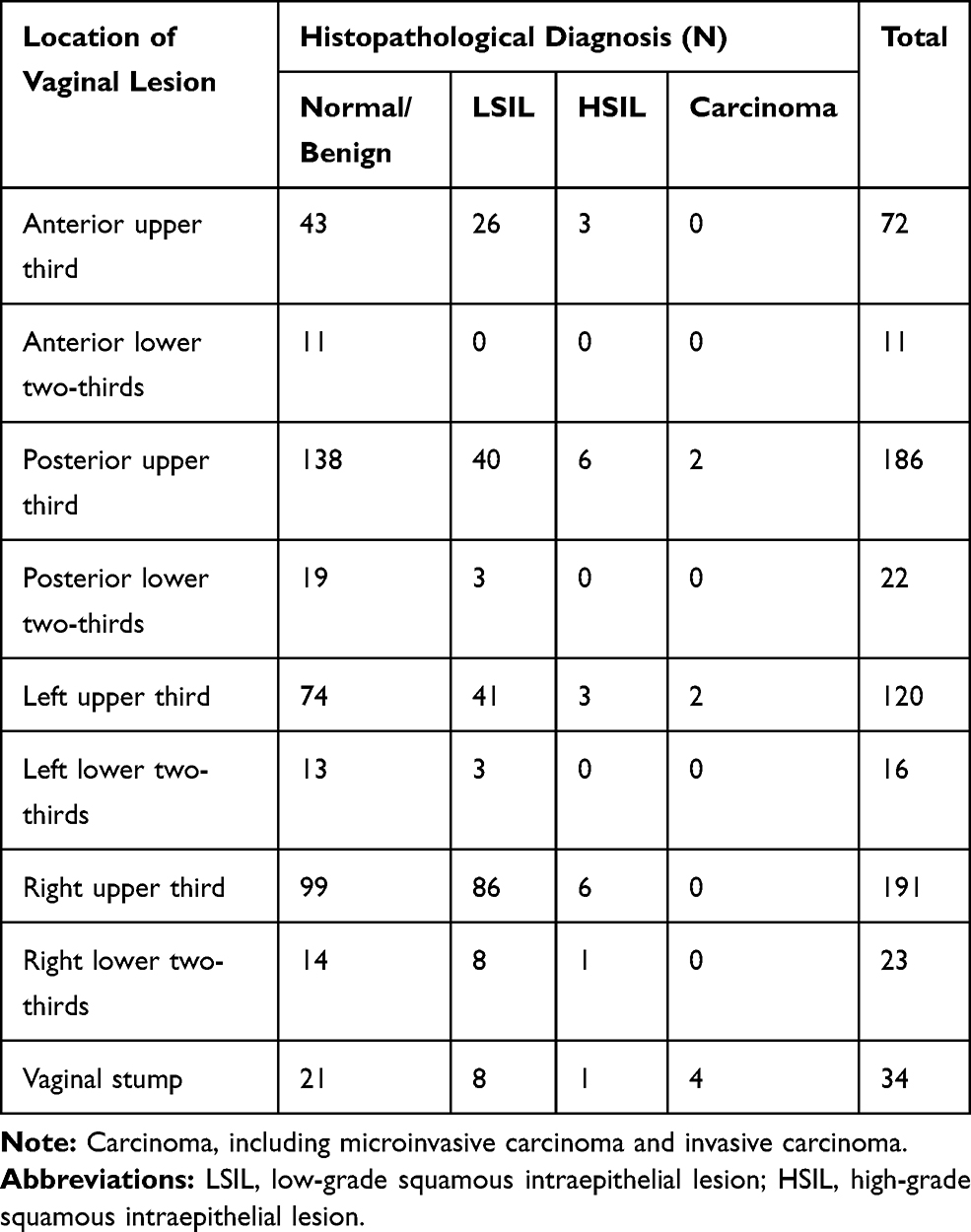 |
Table 5 Location of Vaginal Lesions and Vaginal Histopathological Diagnosis |
The mean ± SD age of all women was 46.26±12.40 years (range: 20–72 years), while the mean age of patients with VaIN was 44.82 years (range: 20–71 years). For women with histopathologic diagnoses of normal or benign lesions, LSIL, HSIL and carcinoma, the ages were 46.92±11.91 years, 44.01±13.21 years, 54.57±8.44 years and 51.14±9.03 years, respectively. The distribution of age among the different lesion grade groups was significantly different (p<0.01, F=4.511). However, we found that the Spearman (rs) coefficient, which was used to evaluate the potential rank correlation between age and grade of vaginal lesion, indicated a poor correlation (rs= −0.055, p=0.239).
Discussion
Considering the importance of colposcopy in the detection of VaIN, the IFCPC revised the colposcopic terminology for the vagina for the first time in 2011. However, the clinical applicability of the IFCPC vaginal terminology still needs to be evaluated.9,16 In this study, we assessed the agreement between colposcopic diagnosis and histopathology according to the 2011 IFCPC classification in VaIN through a retrospective cohort study of 467 women. We analysed the significance of individual findings according to the 2011 IFCPC classification and some other findings, such as the micropapillary pattern.
Our results showed that the agreement between the colposcopic diagnosis and histologic diagnosis was 69.16% with a kappa statistic of 0.437, and the sensitivity and specificity of colposcopy for detecting VaIN were 66.89% and 84.48%, respectively. In this study, with the colposcopic terminology for the vagina of the 2011 IFCPC, the agreement between colposcopy and histopathology was moderate, and both the sensitivity and specificity were above 60%. These values were better than those in previous studies, which showed a poor correlation between the grade of colposcopic abnormalities and the histopathologic grading of VaIN.9,13,14,16 Therefore, as the IFCPC nomenclature for the vagina becomes better understood and applied—providing standardized interpretations of and an organized, comprehensive classification system for colposcopic findings of vaginal lesions—the accuracy of the colposcopic diagnosis on VaIN is being improved and approaching that for the cervix.19–22 However, it should be noted that, in our study, the agreement rate was the lowest (35.71%) in the HSIL group, which was significantly different from that of the other lesion grade groups (LSIL and carcinoma). Although the accuracy of colposcopy for detecting VaIN was improved due to the implementation of the IFCPC nomenclature, more definite and practical findings for high-grade VaIN colposcopic patterns may be needed in further studies.
In our cohort, when the IFCPC classification terminology was applied, the rate of overestimated diagnosis (23.34%) was much higher than that of underestimated diagnosis (7.49%) for VaIN. This was similar to Stuebs’ report16 but different from previous studies on the cervix, which showed that the IFCPC classification was relatively balanced in overestimated and underestimated diagnoses in the cervix.16,19 Moreover, the negative predictive values were much higher than the positive predictive values for both high-grade and low-grade VaIN. This supported the idea that colposcopic patterns are more likely to be overestimated than underestimated by observers. It is therefore recommend the colposcopy to be performed by experienced colposcopists. It is noted that, among 14 patients with HSIL histology, 9 of them is underestimated by colposcopy (64%), which suggest the importance of a biopsy in the case of suspected VaIN, even when the colposcopic impression is not so “bad”.
A highlight of the 2011 IFCPC terminology is the standardized interpretation and comprehensive classification of abnormal colposcopic findings for vaginal lesions. In this study, we individually analysed these abnormal colposcopic findings in detail. Similar to previous studies,13,14 thin acetowhite epithelium was the most frequent (80.51%) grade 1 finding. However, its value in diagnosing low-grade VaIN needs to be further explored because of the low sensitivity (75.86%) and specificity (37.20%) obtained in this study. Fine mosaic and fine punctuation were all uncommon, but their specificity (95.56% and 94.88%) was promising. All grade 2 findings and vascular patterns that are common in the cervix were rather rare in the vagina. However, they have high value in excluding lesions with high negative predictive value and specificity.19,21 Lugol’s non-staining was quite common, but its specificity was very low for both LSIL (10.92%) and HSIL (8.30%). Therefore, we considered it a nonspecific finding for screening vaginal lesions. These results may provide a basis for the implementation of the IFCPC colposcopic terminology of the vagina but are different from Sopracordevole’s opinion, in which Lugol’s non-staining was considered a grade 1 abnormal colposcopy.9
The micropapillary pattern, not included in the 2011 IFCPC terminology, seems to be associated with VaIN in some studies.9,18 This colposcopic pattern is quite rare in the cervix but seems to be relatively common on the vaginal epithelium.9,18 In our cohort, the frequency of the micropapillary pattern was 39.40%, and its positive predictive values for LSIL and HSIL were 55.98% and 5.98%, respectively. Therefore, in our opinion, the micropapillary pattern can be considered an alternative finding for LSIL due to its high incident frequency and positive predictive value. This pattern was associated with less severe disease, and it could probably be an expression of a persistent HPV infection, which is consistent with Sopracordevole’s opinion.9 However, further studies clarifying this assessment are needed.
Subsequently, we found that both LSIL and HSIL were found in the upper third of the vagina much more commonly than in the lower two-thirds of the vagina. These results are in agreement with the IFCPC terminology and with the results of many previous studies.15,23–25 Interestingly, significant differences were found in the frequencies of VaIN among the four sides of the vaginal wall, and for high-grade VaIN or above, the most common location was the posterior wall, followed by the right lateral and left lateral walls, with the rarest location being the anterior wall. However, the exact explanation for this difference is currently unknown and should be evaluated by further large series of studies.
Multifocal lesions are quite common among vaginal lesions.24 In our cohort, there was no significant difference in the total size of the lesions among the different lesion grade groups, but there were significant differences in the maximum size of single lesions and number of lesions. Notably, there was a significant linear trend between the maximum size of single lesions and the severity of the lesion. In addition, the higher the grade of the lesion in a group, the smaller the average number of lesions was. Based on the results above, we speculated that scattered and spotty lesions suggest low-grade VaIN, while large single lesions suggest high-grade VaIN. Thus, the authors suggest to perform biopsy at the maximum lesion in case of multiple lesions.
The relationship between hysterectomy and vaginal lesions has been previously studied, but different results have been obtained.24,26,27 In the present study, there were significant differences in the proportion of patients who underwent hysterectomy among different grade lesion groups, and the carcinoma group had the highest proportion, followed by the HSIL group. Hence, close follow-up and careful screening may still be needed for post-hysterectomy patients because of the high proportion of high-grade lesions or above in our results.
In our cohort, the mean age of all patients was 46.26 years, while the mean age of patients with VaIN was 44.82 years, which was nearly equal to that reported in some previous studies9,26 and indicates the age of the population susceptible to VaIN. We found that the distribution of age among different lesion grade groups (normal/benign, LSIL, HSIL and carcinoma) was significantly different, but the correlation between age and vaginal lesion grade was poor. These results were not identical to Zeligs’ and Bradbury’s reports,26,28 possibly because of differences in sample selection and sample size.
In conclusion, our study supports the importance of the clinical application of the 2011 IFCPC terminology for the detection of VaIN. Although the agreement between colposcopic diagnosis and vaginal histopathology was moderate, the nomenclature, in which most findings for the vagina are organized systemically, represents the latest global understanding of precancerous lesions of the vagina and has great significance for guiding biopsy. However, our study suggests that more appropriate and definite findings for high-grade VaIN are needed, and the significance of the micropapillary pattern and iodine staining remains to be discussed in future studies. Moreover, some lesion characteristics, such as the number of lesions and the maximum size of single lesions, should be recorded to aid in VaIN classification.
Data Sharing Statement
The data used in this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki. All women gave a written informed consent to participate in the study, which was approved by the Ethical Committee of the Obstetrics and Gynecology Hospital of Fudan University (Shanghai, China).
Patient Consent for Publication
Written consent for publication was obtained from patients and/or their legal guardians.
Disclosure
The authors declare that they have no competing interests.
References
1. Tranoulis A, Laios A, Mitsopoulos V, Lutchman-Singh K, Thomakos N. Efficacy of 5% imiquimod for the treatment of Vaginal intraepithelial neoplasia-a systematic review of the literature and a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2017;218:129–136. doi:10.1016/j.ejogrb.2017.09.020
2. Barcellini A, Lecchi M, Tenconi C, et al. High-dose-rate brachytherapy for high-grade vaginal intraepithelial neoplasia: a dosimetric analysis. J Contemp Brachytherapy. 2019;11(2):146–151. doi:10.5114/jcb.2019.84696
3. Cong Q, Song Y, Wang Q, Zhang H, Gao S, Sui L. A retrospective study of cytology, high-risk HPV, and colposcopy results of vaginal intraepithelial neoplasia patients. Biomed Res Int. 2018;2018:5894801. doi:10.1155/2018/5894801
4. Kim MK, Lee IH, Lee KH. Clinical outcomes and risk of recurrence among patients with vaginal intraepithelial neoplasia: a comprehensive analysis of 576 cases. J Gynecol Oncol. 2018;29(1):e6. doi:10.3802/jgo.2018.29.e6
5. Bryan S, Barbara C, Thomas J, Olaitan A. HPV vaccine in the treatment of usual type vulval and vaginal intraepithelial neoplasia: a systematic review. BMC Women’s Health. 2019;19(1):3. doi:10.1186/s12905-018-0707-9
6. Frega A, Sopracordevole F, Assorgi C, et al. Vaginal intraepithelial neoplasia: a therapeutical dilemma. Anticancer Res. 2013;33(1):29–38.
7. Darragh TM, Colgan TJ, Thomas Cox J, et al. The lower anogenital squamous terminology standardization project for HPV-associated lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Int J Gynecol Pathol. 2013;32(1):76–115. doi:10.1097/PGP.0b013e31826916c7
8. Gunderson CC, Nugent EK, Elfrink SH, Gold MA, Moore KN. A contemporary analysis of epidemiology and management of vaginal intraepithelial neoplasia. Am J Obstet Gynecol. 2013;208(5):
9. Sopracordevole F, Barbero M, Clemente N, et al. Colposcopic patterns of vaginal intraepithelial neoplasia: a study from the Italian Society of Colposcopy and Cervico-Vaginal Pathology. Eur J Cancer Prev. 2018;27(2):152–157. doi:10.1097/CEJ.0000000000000287
10. Bogani G, Ditto A, Martinelli F, et al. LASER treatment for women with high-grade vaginal intraepithelial neoplasia: a propensity-matched analysis on the efficacy of ablative versus excisional procedures. Lasers Surg Med. 2018;50(9):933–939. doi:10.1002/lsm.22941
11. Hodeib M, Cohen JG, Mehta S, et al. Recurrence and risk of progression to lower genital tract malignancy in women with high grade VAIN. Gynecol Oncol. 2016;141(3):507–510. doi:10.1016/j.ygyno.2016.03.033
12. Bertoli HK, Rasmussen CL, Sand FL, et al. Human papillomavirus and p16 in squamous cell carcinoma and intraepithelial neoplasia of the vagina. Int J Cancer. 2019;145(1):78–86. doi:10.1002/ijc.32078
13. Boonlikit S, Noinual N. Vaginal intraepithelial neoplasia: a retrospective analysis of clinical features and colpohistology. J Obstet Gynaecol Res. 2010;36(1):94–100. doi:10.1111/j.1447-0756.2009.01108.x
14. Indraccolo U, Baldoni A. A simplified classification for describing colposcopic vaginal patterns. J Low Genit Tract Dis. 2012;16(2):75–79. doi:10.1097/LGT.0b013e318237ec82
15. Bornstein J, Bentley J, Bosze P, et al. 2011 colposcopic terminology of the International Federation for Cervical Pathology and Colposcopy. Obstet Gynecol. 2012;120(1):166–172. doi:10.1097/AOG.0b013e318254f90c
16. Stuebs FA, Koch MC, Mehlhorn G, et al. Accuracy of colposcopic findings in detecting vaginal intraepithelial neoplasia: a retrospective study. Arch Gynecol Obstet. 2020;301(3):769–777. doi:10.1007/s00404-020-05441-5
17. Wee WW, Chia YN, Yam PK. Diagnosis and treatment of vaginal intraepithelial neoplasia. Int J Gynaecol Obstet. 2012;117(1):15–17. doi:10.1016/j.ijgo.2011.10.033
18. Sopracordevole F, Clemente N, Barbero M, et al. Colposcopic patterns of vaginal intraepithelial neoplasia: a focus on low-grade lesions. Eur Rev Med Pharmacol Sci. 2017;21(12):2823–2828.
19. Li Y, Duan X, Sui L, et al. Closer to a uniform language in colposcopy: study on the potential application of 2011 International Federation for Cervical Pathology and Colposcopy Terminology in clinical practice. Biomed Res Int. 2017;2017:8984516.
20. Rema PN, Mathew A, Thomas S. Performance of colposcopic scoring by modified International Federation of Cervical Pathology and Colposcopy terminology for diagnosing cervical intraepithelial neoplasia in a low-resource setting. South Asian J Cancer. 2019;8(4):218–220. doi:10.4103/sajc.sajc_302_18
21. Fan A, Wang C, Zhang L, Yan Y, Han C, Xue F. Diagnostic value of the 2011 International Federation for Cervical Pathology and Colposcopy Terminology in predicting cervical lesions. Oncotarget. 2018;9(10):9166–9176. doi:10.18632/oncotarget.24074
22. Stuebs FA, Schulmeyer CE, Mehlhorn G, et al. Accuracy of colposcopy-directed biopsy in detecting early cervical neoplasia: a retrospective study. Arch Gynecol Obstet. 2019;299(2):525–532. doi:10.1007/s00404-018-4953-8
23. Gurumurthy M, Cruickshank ME. Management of vaginal intraepithelial neoplasia. J Low Genit Tract Dis. 2012;16(3):306–312. doi:10.1097/LGT.0b013e31823da7fb
24. Jentschke M, Hoffmeister V, Soergel P, Hillemanns P. Clinical presentation, treatment and outcome of vaginal intraepithelial neoplasia. Arch Gynecol Obstet. 2016;293(2):415–419. doi:10.1007/s00404-015-3835-6
25. Lamos C, Mihaljevic C, Aulmann S, et al. Detection of human papillomavirus infection in patients with vaginal intraepithelial neoplasia. PLoS One. 2016;11(12):e0167386. doi:10.1371/journal.pone.0167386
26. Zeligs KP, Byrd K, Tarney CM, et al. A clinicopathologic study of vaginal intraepithelial neoplasia. Obstet Gynecol. 2013;122(6):1223–1230. doi:10.1097/01.AOG.0000435450.08980.de
27. Field A, Bhagat N, Clark S, Speed T, Razvi K. Vaginal intraepithelial neoplasia: a retrospective study of treatment and outcomes among a cohort of UK women. J Low Genit Tract Dis. 2020;24(1):43–47. doi:10.1097/LGT.0000000000000502
28. Bradbury M, Xercavins N, Garcia-Jimenez A, et al. Vaginal intraepithelial neoplasia: clinical presentation, management, and outcomes in relation to HIV infection status. J Low Genit Tract Dis. 2019;23(1):7–12. doi:10.1097/LGT.0000000000000431
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.