Back to Journals » International Journal of General Medicine » Volume 17
Apolipoprotein E Gene ϵ4 Allele is Associated with Atherosclerosis in Multiple Vascular Beds
Authors Lin Y, Yang M, Liu Q, Cai Y, Zhang Z, Xu C, Luo M
Received 25 August 2024
Accepted for publication 26 October 2024
Published 3 November 2024 Volume 2024:17 Pages 5039—5048
DOI https://doi.org/10.2147/IJGM.S475771
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Youni Lin, Min Yang, Qifeng Liu, Yufu Cai, Zhouhua Zhang, Chongfei Xu, Ming Luo
Center for Cardiovascular Diseases, Meizhou People’s Hospital, Meizhou, People’s Republic of China
Correspondence: Youni Lin, Center for Cardiovascular Diseases, Meizhou People’s Hospital, Meizhou, People’s Republic of China, Email [email protected]
Background: Atherosclerosis is a systemic disease that can involve multiple vascular beds. The risk factors for atherosclerosis in multiple vascular beds remain unclear. Apolipoprotein E (APOE) is involved in inflammation and lipid deposition in the process of atherosclerosis. The objective of this study was to investigate whether APOE polymorphisms are associated with atherosclerosis in multiple vascular beds.
Methods: A total of 416 patients with atherosclerosis in single vascular bed and 658 patients with atherosclerosis in multiple vascular beds were included. APOE genotypes were detected and the differences of APOE genotypes between the groups were compared. Logistic regression analysis was performed to analyze the relationship between APOE genotypes and atherosclerosis in multiple vascular beds.
Results: APOE E3/E4 genotype frequency was lower in the patients with atherosclerosis in multiple vascular beds than that of patients with atherosclerosis in single vascular bed (11.4% vs 17.8%, P=0.004). There was no significant difference in age and gender distribution, proportion of history of smoking, alcohol consumption, hypertension, and diabetes mellitus between the two groups (all P> 0.05), and among patients with different APOE alleles (all P> 0.05). Logistic regression analysis indicated that APOE E3/E4 genotype (E3/E4 vs E3/E3: odds ratio (OR) 0.598, 95% confidence interval (CI): 0.419– 0.854, P=0.005), and APOE ϵ4 allele (ϵ4 vs ϵ3: OR 0.630, 95% CI: 0.444– 0.895, P=0.010) associated with atherosclerosis in multiple vascular beds.
Conclusion: APOE ϵ4 allele is associated with atherosclerosis in multiple vascular beds.
Keywords: APOE, polymorphism, atherosclerosis, multiple vascular beds
Introduction
Atherosclerosis refers to the occurrence of lipidosis in the intima of the artery, thickening of the intima, and gradually forming plaque, which reduces the elasticity of the artery, causes the formation of artery stenosis and thrombosis, and causes the obstruction of the artery blood supply,1 and ischemic changes.2,3 As a systemic disease, atherosclerosis can cause damage to multiple vascular beds throughout the body, mainly involving large and medium elastic arteries of systemic circulation, including carotid arteries, intracranial arteries, coronary arteries, aorta, renal arteries and peripheral arteries.4 Atherosclerosis lesions with two or more vascular beds throughout the body known as atherosclerosis in multiple vascular beds.5 About 20% of patients with atherosclerosis have lesions in multivessel beds.6 Major adverse cardiac events (MACE) outcomes are associated with the number and location of plaques, and studies of high-risk plaque characteristics can help assess the risk of MACE.7 Therefore, it is of great significance to predict the population at risk of atherosclerosis in multiple vascular beds for the prevention and treatment of cardiovascular diseases.8
It is believed that the formation process of atherosclerosis is related to inflammation, lipid deposition, and fibroplasia regulated by immune cells.9 And studies have shown that a functional deficiency or decrease in the overall level of apolipoprotein E (ApoE) can produce an imbalance in the number and function of immune cells.10,11 At the same time, lipid-enriched spleen macrophages release interleukin-23 (IL-23), inducing a large amount of hematopoietic stem and progenitor cells (HSPCs) to be released from the bone marrow niche.12 When HSPCs are located in the extramedullary position, they can encounter granulocyte-macrophage colony-stimulating factor (GM-CSF) and interleukin-3 (IL-3),13 and the net effect leads to the proliferation of HSPCs, the production of extramedullary leukocytes, and atherosclerosis is accelerated.14 As is an important plasma lipoprotein involved in lipid metabolism, ApoE deficiency in human may result in an abnormal ability to process cholesterol.15,16
The development of atherosclerosis is influenced by many factors, including eating habit, lifestyle, and environmental factors.17,18 Genetic predisposition is also an unavoidable factor in atherosclerosis.19 The APOE gene contains 4 exons and 3 introns.20 Three major alleles (ε2(rs429358 T-rs7412 T), ε3(rs429358 T-rs7412 C), and ε4(rs429358 C-rs7412 C)) were formed based on two non-synonymous SNPs: rs7412 (526 C>T) and rs429358 (388 C>T).21 Each allele can encode one protein isoform and form six different gene phenotypes: E2/E2, E2/E3, E2/E4, E3/E3, E3/E4, and E4/E4.22 Differences in ethnicity, and genetic background can affect the onset and progression of atherosclerosis.23–25 Several studies suggested that APOE gene polymorphisms have been widely recognized as a risk factor for atherosclerosis.26–28 However, the difference of APOE polymorphisms between atherosclerosis in multiple vascular beds and atherosclerosis in single vascular bed, and the relationship of APOE polymorphisms and atherosclerosis in multiple vascular beds remain unclear. In this study, we compared the differences between atherosclerosis in multiple vascular beds and atherosclerosis in single vascular bed, and analyzed risk factors for atherosclerosis in multiple vascular beds.
Materials and Methods
Study Population
Atherosclerosis in single vascular bed means that only one vascular bed has obvious atherosclerosis clinically. Atherosclerosis in multiple vascular beds refers to clinically significant atherosclerosis in two or more arterial vascular beds (≥2 arterial beds co-existing).5,29 Patients with atherosclerosis in single vascular bed and multiple vascular beds treated in Meizhou People’s Hospital were recruited from January 2016 to June 2020. The clinical data of these patients (age, gender, history of smoking, history of alcohol consumption, hypertension, and diabetes mellitus) were collected from the medical records system of our hospital. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital (Clearance No.: 2024-C-17). All participants were informed on the study procedures and goals and informed consent was obtained from all the participants.
Atherosclerotic plaque is the direct sign of atherosclerosis, and the clinical diagnosis of atherosclerosis is generally through imaging detection technology to identify plaque.30,31 Plaque was defined as a focal structure that invaded the lumen of the artery by at least 0.5 mm, or by 50% of the surrounding endo-media thickness, or by a thickness greater than 1.5 mm measured from the outer membrane to the endo-lumen interface.32 Atherosclerosis is determined by examining arterial plaque using techniques such as angiography, magnetic resonance imaging (MRI), computed tomography, or color Doppler ultrasonography, assessed by two senior radiologists in a double-blind evaluation. Potential subjects were included in any radiograph-based test showing arterial plaque. The diagnostic criteria for atherosclerosis were in accordance with the relevant diagnostic criteria formulated by the Cardiovascular Branch and the Neurology Branch of the Chinese Medical Association. Inclusion criteria are as follows: (1) Clinically diagnosed atherosclerosis, including coronary artery, carotid artery, cerebral artery, limb artery, and other vascular lesions; (2) The patient’s medical records are complete; (3) Age ≥18 years old. The exclusion criteria were: (1) Patients with incomplete clinical data; (2) Patients with severe infectious diseases, autoimmune diseases, organ dysfunction, and other diseases; (3) Age <18 years old. The diagnostic criteria for hypertension are systolic blood pressure of ≥140 mm Hg, diastolic blood pressure of ≥90 mm Hg.33 The diagnostic criteria for diabetes mellitus were fasting blood glucose ≥126.1 mg/dL, blood glucose ≥200 mg/dL 2 hours after loading.34
Determination of Serum Lipids and APOE Genotyping
Fasting blood was collected and serum was isolated. Triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), Apolipoprotein A1 (Apo-A1), and Apolipoprotein B (ApoB) levels in serum samples were assessed using automatic biochemical analysis system (Olympus AU5400 system, Tokyo, Japan) and corresponding kits. Whole blood samples were collected and genomic DNA was extracted. APOE polymorphisms (rs7412 and rs429358) were detected by APOE genotyping kit (Sinochips Bioscience Co., Ltd., Zhuhai, Guangdong, China) based on a gene chip method.35,36
Statistical Analysis
Categorical variables are expressed as percentages. The differences of genotype composition ratios and allele frequencies among patients with atherosclerosis in single vascular bed and atherosclerosis in multiple vascular beds were analyzed by the χ2 test. To measure the relative risk of APOE genotypes and alleles, logistic regression analysis was performed after adjusting for the factors of demographic characteristics, personal history, and disease history. P<0.05 was set as statistically significant.
Results
Characteristics of Subjects
A total number of 1074 patients with atherosclerosis were recruited. In this study, there were 736 males (68.5%) and 338 females (31.5%). There were 353 (32.9%) patients aged <65 years and 721 (67.1%) patients aged ≥65 years. There were 233 (21.7%) cases have a history of smoking, 37 (3.4%) cases have a history of alcoholism, 707 (65.8%) cases with hypertension history, 337 (31.4%) cases with diabetes mellitus history. This study included 416 patients with atherosclerosis in single vascular bed and 658 patients with atherosclerosis in multiple vascular beds. There was no significant difference in distributions of age and gender, proportion of smoking, alcohol consumption, hypertension, and diabetes between patients with single vascular bed and atherosclerosis in multiple vascular beds (all P>0.05). The difference of serum lipid-lipoprotein levels was not statistically significant (Table 1).
 |
Table 1 Clinical Characteristics of Patients with Atherosclerosis in Multiple Vascular Beds and Patients with Atherosclerosis in Single Vascular Bed |
Distribution Frequencies of APOE Genotypes and Alleles in Patients with Atherosclerosis in Multiple Vascular Beds and Patients with Atherosclerosis in Single Vascular Bed
The APOE genotypes in the patients with atherosclerosis in single vascular bed (χ2=4.782, P=0.310) and patients with atherosclerosis in multiple vascular beds (χ2=7.284, P=0.122) conformed to the Hardy-Weinberg equilibrium. Compared to the patients with atherosclerosis in single vascular bed, APOE E3/E4 genotype frequency was lower in the patients with atherosclerosis in multiple vascular beds (11.4% vs 17.8%, P=0.004) (Table 2).
 |
Table 2 Distribution Frequencies of APOE Genotypes and Alleles in Patients with Atherosclerosis in Multiple Vascular Beds and Patients with Atherosclerosis in Single Vascular Bed |
Comparison of Characteristics and Lipid Levels Among Patients Stratified by APOE Alleles
Patients with the E2/E4 genotype (n=17) were excluded from this analysis because of the ε2 and ε4 alleles have opposite effects on lipid metabolism.35,36 The patients carried ɛ4 allele had higher level in TG (1.99±1.66 mmol/L vs 1.64±1.34 mmol/L), TC (5.33±1.34 mmol/L vs 4.86±1.38 mmol/L), LDL-C (3.18±1.02 mmol/L vs 2.80±1.00 mmol/L), Apo-B (1.03±0.33 g/L vs 0.90±0.31 g/L) than those with ɛ3 allele; patients with ɛ4 allele had higher TC (5.33±1.34 mmol/L vs 4.75±1.44 mmol/L), LDL-C (3.18±1.02 mmol/L vs 2.58±1.05 mmol/L), Apo-B (1.03±0.33 g/L vs 0.85±0.31 g/L) than those with ɛ2 allele (all P<0.05) (Table 3).
 |
Table 3 Clinical Characteristics of Subjects Stratified by APOE Alleles |
Association of the Risk Factors with Atherosclerosis in Multiple Vascular Beds
APOE E3/E4 genotype (E3/E4 vs E3/E3: odds ratio (OR) 0.599, 95% confidence interval (CI): 0.421–0.852, P=0.004) and ε4 allele (ε4 vs ε3: OR 0.630, 95% CI: 0.445–0.892, P=0.009) were associated with atherosclerosis in multiple vascular beds in univariate logistic regression analysis. In multivariate logistic regression analysis, APOE E3/E4 genotype (E3/E4 vs E3/E3: OR 0.598, 95% CI: 0.419–0.854, P=0.005), and ε4 allele (ε4 vs ε3: OR 0.630, 95% CI: 0.444–0.895, P=0.010) were associated with atherosclerosis in multiple vascular beds after adjusting for gender, age, smoking, drinking, hypertension, and diabetes mellitus (Table 4).
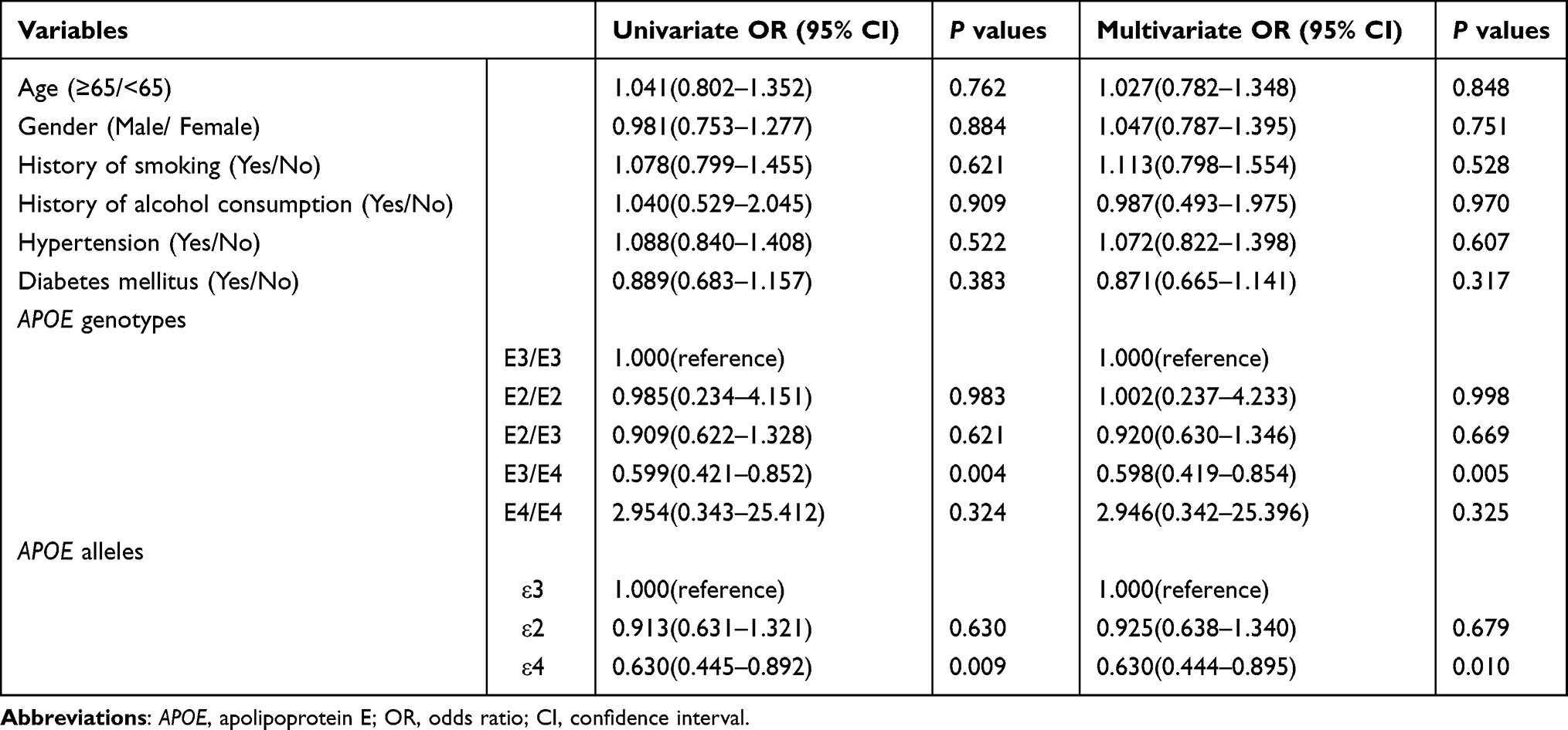 |
Table 4 Multivariate Logistic Regression of Variables Related to Atherosclerosis in Multiple Vascular Beds |
Discussion
Atherosclerosis is a systemic disease that can involve multiple vascular beds.37,38 Atherosclerotic patients with multi-vessel beds have significantly higher morbidity and mortality than patients with single-vessel bed.39 Currently, most scholars believe that atherosclerosis is caused by the joint action of many risk factors. However, there are different degrees of arterial lesions in different parts of the same patient, which indicates that the risk factors for atherosclerosis may have different degrees of effect on arteries in different parts. A study in mouse models has found that the location specificity of the formation of atherosclerosis in different vascular beds is genetically controlled.40
In the current study, the relationship between APOE gene rs7412 and rs429358 polymorphisms and atherosclerosis in multiple vascular beds was analyzed. The results showed that the frequency of the APOE E3/E4 genotype was lower in the patients with atherosclerosis in multiple vascular beds than that in the patients with atherosclerosis in single vascular bed (11.4% vs 17.8%, P=0.004). Multivariate logistic regression indicated that APOE E3/E4 genotype and APOE ε4 allele were associated with atherosclerosis in multiple vascular beds. At present, there have been some reports on the relationship between APOE genotypes and cardiovascular and cerebrovascular diseases. APOE subtypes, especially APOE2 and APOE4, have been confirmed as markers of arteriosclerotic cardiovascular disease.41 APOE ε4 allele is closely associated with dyslipidemia and coronary heart disease.42 APOE ε4 and ε2 alleles are risk factors for peripheral artery disease (PAD).43 APOE gene variant is associated with intracranial atherosclerosis (ICAS).26 APOE ε4 allele was an risk factor for carotid atherosclerosis (CAS).44 APOE ε2/ε2 genotype was significantly associated with a higher risk of PAD, but not with other vascular diseases.45 Of course, there are some opposite results. APOE ε4 allele was not associated with carotid atherosclerosis.46 There was no relationship between APOE polymorphism and PAD.47 APOE genotype is not associated with cerebral atherosclerosis.48
APOE is an important component of plasma lipoprotein, a major ligand of lipid transporter and low-density lipoprotein receptor, through which it clears triglyceride-rich lipoproteins from circulation.27,49 Therefore, the main function of APOE is to resist arteriosclerosis and maintain the balance of plasma lipid metabolism.50,51 The mechanism of APOE involved in atherosclerosis may be related to the role of APOE in lipid accumulation and the regulation of inflammation in vascular endothelium.52,53 Atherosclerosis is the result of lipid infiltration, oxidative stress and inflammation in the intima cells. APOE is a glycoprotein that helps stabilize and dissolve lipoproteins in the blood circulation.20 Although ε3 is the dominant allele, the APOE alleles frequency varies widely across populations.35,54 In human evolution, the ε4 allele is considered an ancestral APOE allele.55,56 The activity of APOE4 is poor, and its function is not enough to maintain the balance of lipid metabolism and inflammatory response in blood vessels, so APOE ε4 allele carriers are more prone to multiple atherosclerosis. Atherosclerosis is a systemic disease process, most commonly coronary and cerebral atherosclerosis, and recent attention has focused on the combination of atherosclerosis in other vascular beds and their risk factors.5 It is the first report of the relationship of APOE genotypes and atherosclerosis in multiple vascular beds.
In addition, there is a relationship between APOE genotypes and lipid levels differences. APOE is the ligand for the LDL-C receptor family of proteins and itself assimilates and transfers lipids, and the binding ability of APOE2 to LDL-C was significantly reduced.20 The APOE ε4 allele was associated with elevated levels of LDL-C.21,57–60 Some studies suggested that APOE ε4 allele was related to elevated TG,61–63 TC,59,64 and Apo-B.60 However, another study has found no statistically significant difference in lipid levels in patients with different APOE alleles.65 In present study, the patients with ɛ4 allele had higher levels in TC, LDL-C, and Apo-B than those with ɛ3 allele and ɛ2 allele, respectively. To sum up, more studies are needed to reveal the effects of different APOE alleles on lipid levels. In addition, the influence of APOE alleles on the regulation of different lipid profiles may be caused by the combined action of many factors.66–68 The effects of these factors add complexity to the regulation of lipid levels.
Several recognized cardiovascular risk factors were associated with the development of multi-site atherosclerotic disease.69 However, there was no significant relationship between gender, age, smoking, alcohol consumption, hypertension, and diabetes mellitus and the risk of atherosclerosis in multiple vascular beds in this study. Smoking, heavy drinking, and a history of hypertension, and diabetes mellitus are all recognized factors that increase the risk of cardiovascular disease.70 Study has found that the incidence of arterial disease may vary by gender.71 A study found that smoking was associated with subclinical atherosclerosis in multi-vessel beds in a Japanese male population.72 Old age, smoking, and hypertension were associated with atherosclerosis in multiple vascular beds.73 The prevalence of hypertension and type 2 diabetes mellitus in patients with multi-vessel atherosclerotic disease is significantly higher than that in patients with single-vessel disease.74 To sum up, the occurrence of atherosclerosis is the result of a variety of factors.
This study found that APOE ε4 allele is associated with atherosclerosis in multiple vascular beds. However, there are some shortcomings. First, no imaging data was collected during the data collection process owing to a retrospective study, the relationship between APOE polymorphisms and the degree of embolization of sclerotic vessels was not investigated. Second, the subjects of this study come from a single medical institution, and selection bias is inevitable because the population is not completely representative. Third, this study only studied the relationship between APOE genotypes and the risk of atherosclerosis in multiple vascular beds, and did not analyze the expression of APOE. Future researches need to conduct targeted research on the above deficiencies.
Conclusion
An association between APOE genotypes and atherosclerosis in multiple vascular beds was found in this cohort study. APOE ε4 allele is associated with atherosclerosis in multiple vascular beds. It can provide reference for the identification and management of patients with atherosclerosis in multiple vascular beds.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
All participants were informed on the study procedures and goals and informed consent was obtained from all the participants. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital.
Acknowledgments
The authors thank their colleagues, who were not listed in the authorship of the Meizhou People’s Hospital, for their helpful comments on the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program for Social Development of Meizhou (Grant No.: 2023B09).
Disclosure
The authors declare that they have no competing interests.
References
1. Liu H, Zhu L, Chen L, Li L. Therapeutic potential of traditional Chinese medicine in atherosclerosis: a review. Phytother Res. 2022;36(11):4080–4100. doi:10.1002/ptr.7590
2. Xu J, Kitada M, Ogura Y, Koya D. Relationship between autophagy and metabolic syndrome characteristics in the pathogenesis of atherosclerosis. Front Cell Dev Biol. 2021;9:641852. doi:10.3389/fcell.2021.641852
3. Xiang Q, Tian F, Xu J, Du X, Zhang S, Liu L. New insight into dyslipidemia-induced cellular senescence in atherosclerosis. Biol Rev Camb Philos Soc. 2022;97(5):1844–1867. doi:10.1111/brv.12866
4. Hisamatsu T, Miura K, Ohkubo T, et al. Home blood pressure variability and subclinical atherosclerosis in multiple vascular beds: a population-based study. J Hypertens. 2018;36(11):2193–2203. doi:10.1097/HJH.0000000000001810
5. Aday AW, Matsushita K. Epidemiology of peripheral artery disease and polyvascular disease. Circ Res. 2021;128(12):1818–1832. doi:10.1161/CIRCRESAHA.121.318535
6. Weissler EH, Jones WS, Desormais I, et al. Polyvascular disease: a narrative review of current evidence and a consideration of the role of antithrombotic therapy. Atherosclerosis. 2020;315:10–17. doi:10.1016/j.atherosclerosis.2020.11.001
7. Stone PH, Libby P, Boden WE. Fundamental pathobiology of coronary atherosclerosis and clinical implications for chronic ischemic heart disease management-the plaque hypothesis: a narrative review. JAMA Cardiol. 2023;8(2):192–201. doi:10.1001/jamacardio.2022.3926
8. Martelli E, Enea I. Focus on the most common paucisymptomatic vasculopathic population, from diagnosis to secondary prevention of complications. Diagnostics. 2023;13(14):2356. doi:10.3390/diagnostics13142356
9. Vallejo J, Cochain C. Heterogeneity of immune cells in human atherosclerosis revealed by scRNA-Seq. Cardiovasc Res. 2021;117(13):2537–2543. doi:10.1093/cvr/cvab260
10. Yvan-Charvet L, Pagler T, Gautier EL, et al. ATP-binding cassette transporters and HDL suppress hematopoietic stem cell proliferation. Science. 2010;328(5986):1689–1693. doi:10.1126/science.1189731
11. Murphy AJ, Akhtari M, Tolani S, et al. ApoE regulates hematopoietic stem cell proliferation, monocytosis, and monocyte accumulation in atherosclerotic lesions in mice. J Clin Invest. 2011;121(10):4138–4149. doi:10.1172/JCI57559
12. Sarrazy V, Viaud M, Westerterp M, et al. Disruption of Glut1 in hematopoietic stem cells prevents myelopoiesis and enhanced glucose flux in atheromatous plaques of ApoE(-/-) mice. Circ Res. 2016;118(7):1062–1077. doi:10.1161/CIRCRESAHA.115.307599
13. Robbins CS, Chudnovskiy A, Rauch PJ, et al. Extramedullary hematopoiesis generates Ly-6C(high) monocytes that infiltrate atherosclerotic lesions. Circulation. 2012;125(2):364–374. doi:10.1161/CIRCULATIONAHA.111.061986
14. Swirski FK, Nahrendorf M. Leukocyte behavior in atherosclerosis, myocardial infarction, and heart failure. Science. 2013;339(6116):161–166. doi:10.1126/science.1230719
15. Paquette M, Bernard S, Paré G. Dysbetalipoproteinemia: differentiating multifactorial remnant cholesterol disease from genetic ApoE deficiency. J Clin Endocrinol Metab. 2022;107(2):538–548. doi:10.1210/clinem/dgab648
16. Fujiwara Y, Okada S, Uryu K, Maru I, Komohara Y. The extract of Ilex kudingcha inhibits atherosclerosis in apoE-deficient mice by suppressing cholesterol accumulation in macrophages. Biosci Biotechnol Biochem. 2021;85(10):2177–2184. doi:10.1093/bbb/zbab140
17. Zhou F, Tang J, Li P, Liao B, Qin C. Distribution of cerebral artery stenosis and risk factors in ethnic Zhuang and Han patients with ischemic stroke in Guangxi province. Ann Palliat Med. 2020;9(2):256–263. doi:10.21037/apm.2020.02.32
18. Lechner K, von Schacky C, McKenzie AL, et al. Lifestyle factors and high-risk atherosclerosis: pathways and mechanisms beyond traditional risk factors. Eur J Prev Cardiol. 2020;27(4):394–406. doi:10.1177/2047487319869400
19. Abraham G, Rutten-Jacobs L, Inouye M. Risk prediction using polygenic risk scores for prevention of stroke and other cardiovascular diseases. Stroke. 2021;52(9):2983–2991. doi:10.1161/STROKEAHA.120.032619
20. Marais AD. Apolipoprotein E in lipoprotein metabolism, health and cardiovascular disease. Pathology. 2019;51(2):165–176. doi:10.1016/j.pathol.2018.11.002
21. Khalil YA, Rabès JP, Boileau C, Varret M. APOE gene variants in primary dyslipidemia. Atherosclerosis. 2021;328:11–22. doi:10.1016/j.atherosclerosis.2021.05.007
22. Seripa D, D’Onofrio G, Panza F, Cascavilla L, Masullo C, Pilotto A. The genetics of the human APOE polymorphism. Rejuvenation Res. 2011;14(5):491–500. doi:10.1089/rej.2011.1169
23. Kubota M, Yoneda M, Watanabe H, Egusa G. Progression of carotid atherosclerosis in Two Japanese populations with different lifestyles. J Atheroscler Thromb. 2017;24(10):1069–1074. doi:10.5551/jat.39578
24. Elfaki I, Mir R, Almutairi FM, Duhier FMA. Cytochrome P450: polymorphisms and roles in cancer, diabetes and atherosclerosis. Asian Pac J Cancer Prev. 2018;19(8):2057–2070. doi:10.22034/APJCP.2018.19.8.2057
25. Liu Y, Wang X, Zhang Q, et al. Relationship between dietary patterns and carotid atherosclerosis among people aged 50 years or older: a population-based study in China. Front Nutr. 2021;8:723726. doi:10.3389/fnut.2021.723726
26. Liu M, Gutierrez J. Genetic risk factors of intracranial atherosclerosis. Curr Atheroscler Rep. 2020;22(4):13. doi:10.1007/s11883-020-0831-5
27. Marais AD. Apolipoprotein E and atherosclerosis. Curr Atheroscler Rep. 2021;23(7):34. doi:10.1007/s11883-021-00933-4
28. Wei G, Li B, Wang H, et al. Apolipoprotein E E3/E4 genotype is associated with an increased risk of coronary atherosclerosis in patients with hypertension. BMC Cardiovasc Disord. 2024;24(1):486. doi:10.1186/s12872-024-04169-3
29. Gutierrez JA, Aday AW, Patel MR, Jones WS. Polyvascular disease: reappraisal of the current clinical landscape. Circ Cardiovasc Interv. 2019;12(12):e007385. doi:10.1161/CIRCINTERVENTIONS.119.007385
30. Benson JC, Saba L. MR imaging of carotid artery atherosclerosis: updated evidence on high-risk plaque features and emerging trends. Am J Neuroradiol. 2023;44(8):880–888. doi:10.3174/ajnr.A7921
31. Mushenkova NV, Summerhill VI, Zhang D, Romanenko EB, Grechko AV, Orekhov AN. Current advances in the diagnostic imaging of atherosclerosis: insights into the pathophysiology of vulnerable plaque. Int J Mol Sci. 2020;21(8):2992. doi:10.3390/ijms21082992
32. Touboul PJ, Hennerici MG, Meairs S, et al. Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd,4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc Dis. 2012;34(4):290–296. doi:10.1159/000343145
33. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China: results from the China hypertension survey, 2012-2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
34. Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317(24):2515–2523. doi:10.1001/jama.2017.7596
35. Liu Q, Wu H. APOE gene ɛ4 allele (388C-526C) effects on serum lipids and risk of coronary artery disease in southern Chinese Hakka population. J Clin Lab Anal. 2021;35(9):e23925. doi:10.1002/jcla.23925
36. Rao H, Wu H. APOE genetic polymorphism rs7412 T/T genotype may be a risk factor for essential hypertension among Hakka people in Southern China. Int J Hypertens. 2022;2022:8145896. doi:10.1155/2022/8145896
37. Xie J, Pan T, Luo W, Zhang S, Fang Y, Xu Z. CYP2C19 *2/*2 genotype is a risk factor for multi-site arteriosclerosis: a hospital-based cohort study. Int J Gen Med. 2023;16:5139–5146. doi:10.2147/IJGM.S437251
38. Cai N, Li C, Gu X, et al. ALDH2 rs671 and MTHFR rs1801133 polymorphisms are risk factors for arteriosclerosis in multiple arteries. BMC Cardiovasc Disord. 2023;23(1):319. doi:10.1186/s12872-023-03354-0
39. Poredos P, Blinc A, Novo S, Antignani PL. How to manage patients with polyvascular atherosclerotic disease. Position paper of the International Union of Angiology. Int Angiol. 2021;40(1):29–41. doi:10.23736/S0392-9590.20.04518-6
40. Kayashima Y, Maeda-Smithies N. Atherosclerosis in different vascular locations unbiasedly approached with mouse genetics. Genes. 2020;11(12):1427. doi:10.3390/genes11121427
41. Dittrich J, Beutner F, Teren A, et al. Plasma levels of apolipoproteins C-III, A-IV, and E are independently associated with stable atherosclerotic cardiovascular disease. Atherosclerosis. 2019;281:17–24. doi:10.1016/j.atherosclerosis.2018.11.006
42. Ji H, Zhou C, Pan R, et al. APOE hypermethylation is significantly associated with coronary heart disease in males. Gene. 2019;689:84–89. doi:10.1016/j.gene.2018.11.088
43. Rasmussen KL, Luo J, Nordestgaard BG, Tybjærg-Hansen A, Frikke-Schmidt R. APOE and vascular disease: sequencing and genotyping in general population cohorts. Atherosclerosis. 2023;385:117218. doi:10.1016/j.atherosclerosis.2023.117218
44. Ma W, Zhang L, Luo L, et al. Effect of apolipoprotein E ε4 allele on the progression of carotid atherosclerosis through apolipoprotein levels. Pharmgenomics Pers Med. 2022;15:653–661. doi:10.2147/PGPM.S367471
45. Koopal C, Geerlings MI, Muller M, et al. The relation between apolipoprotein E (APOE) genotype and peripheral artery disease in patients at high risk for cardiovascular disease. Atherosclerosis. 2016;246:187–192. doi:10.1016/j.atherosclerosis.2016.01.009
46. Paradela RS, Farias-Itao DS, Leite REP, et al. Apolipoprotein E ε2 allele is associated with lower risk of carotid artery obstruction in a population-based autopsy study. J Stroke Cerebrovasc Dis. 2023;32(9):107229. doi:10.1016/j.jstrokecerebrovasdis.2023.107229
47. Hu Y, Ling T, Yu M, et al. Apolipoprotein E gene polymorphism, glycated hemoglobin, and peripheral arterial disease risk in Chinese type 2 diabetic patients. Dis Markers. 2020;2020:6040525. doi:10.1155/2020/6040525
48. Paradela RS, Farias-Itao DS, Leite REP, et al. Apolipoprotein E genotypes were not associated with intracranial atherosclerosis: a population-based autopsy study. Cardiovasc Pathol. 2023;62:107479. doi:10.1016/j.carpath.2022.107479
49. Jiang CL, Lin FJ. Insights into the roles of apolipoprotein E in adipocyte biology and obesity. Int J Obes. 2024;48(9):1205–1215. doi:10.1038/s41366-024-01549-9
50. Papachristou NI, Blair HC, Kalyvioti ES, et al. Western-type diet differentially modulates osteoblast, osteoclast, and lipoblast differentiation and activation in a background of APOE deficiency. Lab Invest. 2018;98(12):1516–1526. doi:10.1038/s41374-018-0107-7
51. Veronese N, Stubbs B, Crepaldi G, et al. Relationship between low bone mineral density and fractures with incident cardiovascular disease: a systematic review and meta-analysis. J Bone Miner Res. 2017;32(5):1126–1135. doi:10.1002/jbmr.3089
52. Bai XQ, Peng J, Wang MM, et al. PCSK9: a potential regulator of apoE/apoER2 against inflammation in atherosclerosis? Clin Chim Acta. 2018;483:192–196. doi:10.1016/j.cca.2018.04.040
53. Linton MF, Yancey PG, Davies SS, et al. The role of lipids and lipoproteins in atherosclerosis. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext. South Dartmouth (MA): MDText.com, Inc.Copyright © 2000-2023, MDText.com, Inc.; 2000. PMID: 26844337.
54. Wu H, Huang Q, Yu Z, Wu H, Zhong Z. The SNPs rs429358 and rs7412 of APOE gene are association with cerebral infarction but not SNPs rs2306283 and rs4149056 of SLCO1B1 gene in southern Chinese Hakka population. Lipids Health Dis. 2020;19(1):202. doi:10.1186/s12944-020-01379-4
55. Oriá RB, Patrick PD, Blackman JA, Lima AA, Guerrant RL. Role of apolipoprotein E4 in protecting children against early childhood diarrhea outcomes and implications for later development. Med Hypotheses. 2007;68(5):1099–1107. doi:10.1016/j.mehy.2006.09.036
56. Trumble BC, Stieglitz J, Blackwell AD, et al. Apolipoprotein E4 is associated with improved cognitive function in Amazonian forager-horticulturalists with a high parasite burden. FASEB J. 2017;31(4):1508–1515. doi:10.1096/fj.201601084R
57. Larifla L, Armand C, Bangou J, et al. Association of APOE gene polymorphism with lipid profile and coronary artery disease in Afro-Caribbeans. PLoS One. 2017;12(7):e0181620. doi:10.1371/journal.pone.0181620
58. Martínez-Magaña JJ, Genis-Mendoza AD. Association between APOE polymorphisms and lipid profile in Mexican Amerindian population. Mol Genet Genomic Med. 2019;7(11):e958. doi:10.1002/mgg3.958
59. Petrovic D, Zorc M, Peterlin B. Effect of apolipoprotein E polymorphism and apolipoprotein A-1 gene promoter polymorphism on lipid parameters and premature coronary artery disease. Folia Biol. 2000;46(5):181–185. PMID: 11055796.
60. Tascilar N, Dursun A, Ankarali H, et al. Relationship of apoE polymorphism with lipoprotein(a), apoA, apoB and lipid levels in atherosclerotic infarct. J Neurol Sci. 2009;277(1–2):17–21. doi:10.1016/j.jns.2008.09.034
61. Wang C, Yan W, Wang H, Zhu J, Chen H. APOE polymorphism is associated with blood lipid and serum uric acid metabolism in hypertension or coronary heart disease in a Chinese population. Pharmacogenomics. 2019;20(14):1021–1031. doi:10.2217/pgs-2019-0048
62. Gan C, Zhang Y, Liang F, Guo X, Zhong Z. Effects of APOE gene ε4 allele on serum lipid profiles and risk of cardiovascular disease and tumorigenesis in southern Chinese population. World J Surg Oncol. 2022;20(1):280. doi:10.1186/s12957-022-02748-2
63. Liu X, Lin Q, Fan K, et al. The effects of genetic polymorphisms of APOE on circulating lipid levels in middle-aged and elderly Chinese Fujian Han population: toward age- and sex-personalized management. Lipids Health Dis. 2021;20(1):158. doi:10.1186/s12944-021-01587-6
64. Long L, Sun Q. Analysis of APOE and SLCO1B1 gene polymorphism and correlation with dyslipidemia in China. Clin Lab. 2022;68(11). doi:10.7754/Clin.Lab.2022.220143
65. Shafagoj YA, Naffa RG, El-Khateeb MS, et al. APOE gene polymorphism among Jordanian Alzheimer`s patients with relation to lipid profile. Neurosciences. 2018;23(1):29–34. doi:10.17712/nsj.2018.1.20170169
66. Zhang QH, Yin RX, Gao H, et al. Association of the SPTLC3 rs364585 polymorphism and serum lipid profiles in two Chinese ethnic groups. Lipids Health Dis. 2017;16(1):1. doi:10.1186/s12944-016-0392-3
67. Abuzhalihan J, Adi D, Wang YT, et al. APLP2 gene polymorphisms are associated with high TC and LDL-C levels in Chinese population in Xinjiang, China. Biosci Rep. 2020;40(8):BSR20200357. doi:10.1042/BSR20200357
68. Agongo G, Amenga-Etego L, Nonterah EA, et al. Candidate gene analysis reveals strong association of CETP variants with high density lipoprotein cholesterol and PCSK9 variants with low density lipoprotein cholesterol in Ghanaian adults: an AWI-gen sub-study. Front Genet. 2020;11:456661. doi:10.3389/fgene.2020.456661
69. Paraskevas KI, Bessias N, Papas TT, Gekas CD, Andrikopoulos V, Mikhailidis DP. Do different vascular risk factors affect all arteries equally? Angiology. 2008;59(4):397–401. doi:10.1177/0003319708318383
70. Pastore I, Bolla AM, Montefusco L, et al. The impact of diabetes mellitus on cardiovascular risk onset in children and adolescents. Int J Mol Sci. 2020;21(14):4928. doi:10.3390/ijms21144928
71. Pabon M, Cheng S. Sex differences in peripheral artery disease. Circ Res. 2022;130(4):496–511. doi:10.1161/CIRCRESAHA.121.320702
72. Hisamatsu T, Miura K, Arima H, et al. Smoking, smoking cessation, and measures of subclinical atherosclerosis in multiple vascular beds in Japanese men. J Am Heart Assoc. 2016;5(9):e003738. doi:10.1161/JAHA.116.003738
73. van der Meer IM, Iglesias Del Sol A, Hak AE, Bots ML, Hofman A, Witteman JC. Risk factors for progression of atherosclerosis measured at multiple sites in the arterial tree: the Rotterdam study. Stroke. 2003;34(10):2374–2379. doi:10.1161/01.STR.0000088643.07108.19
74. Dilic M, Dzubur A, Kusljugic Z, Balic S, Pepic E. Correlation of arterial hypertension and type 2 diabetes mellitus with type of polyvascular atherosclerotic disease. Med Arh. 2010;64(5):264–268. PMID: 21287949.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.