Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
ApoB Testing in Dyslipidemia Management: Knowledge and Practices of Healthcare Providers in Saudi Arabia
Authors Altuwalah AS, Alfehaid L ![]() , Alhmoud H, Alrasheedy AA
, Alhmoud H, Alrasheedy AA ![]() , Alhomoud IS
, Alhomoud IS ![]()
Received 13 August 2025
Accepted for publication 8 October 2025
Published 15 October 2025 Volume 2025:18 Pages 6667—6679
DOI https://doi.org/10.2147/JMDH.S560362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr David C. Mohr
Abdulaziz S Altuwalah,1,2 Lama Alfehaid,3– 5 Hussam Alhmoud,6 Alian A Alrasheedy,6 Ibrahim S Alhomoud6
1Pharmacy Services, Second Health Cluster, Ministry of Health, Riyadh, Saudi Arabia; 2Department of Pharmacy Practice, College of Pharmacy, AlMaarefa University, Riyadh, 13713, Saudi Arabia; 3Department of Pharmacy Practice, College of Pharmacy, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 4Pharmaceutical Care Department, King Abdulaziz Medical City, Riyadh, Saudi Arabia; 5King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 6Department of Pharmacy Practice, College of Pharmacy, Qassim University, Qassim, 51452, Saudi Arabia
Correspondence: Ibrahim S Alhomoud, Department of Pharmacy Practice, College of Pharmacy, Qassim University, Qassim, 51452, Saudi Arabia, Email [email protected]
Purpose: Apolipoprotein B (apoB), a direct measure of atherogenic lipoprotein particles, is recommended by clinical guidelines for cardiovascular risk assessment, particularly when low-density lipoprotein cholesterol (LDL-C) underestimates risk. Despite these endorsements, apoB testing remains significantly underutilized in clinical practice. This study evaluated the knowledge and practices of physicians and pharmacists in Saudi Arabia regarding apoB testing and its role in lipid management and cardiovascular risk stratification.
Methods: Cross-sectional survey-based study conducted with physicians and pharmacists across healthcare institutions using a validated questionnaire.
Results: A total of 158 participants completed the questionnaire, including 80 physicians (50.6%) and 78 pharmacists (49.4%). The overall mean knowledge score was 4.70 ± 3.13 (out of a maximum score of 10). Participants specializing in family medicine, cardiology, and ambulatory care had the highest mean knowledge scores among specialties. Physicians demonstrated a significantly higher knowledge score than pharmacists (6.00 ± 2.99 vs 3.36 ± 2.69; P < 0.001). While 69.6% recognized apoB as a direct measure of atherogenic lipoprotein particles, only 53.8% correctly identified it as the most reliable marker of residual atherosclerotic cardiovascular disease risk in patients with lipid profile discordance. A significantly higher proportion of participants with high knowledge reported measuring apoB levels or considering it whenever available in their practice than those with moderate and low levels of knowledge (88.2%, 53.1%, and 24.1%, respectively; P < 0.001).
Conclusion: ApoB testing remains underutilized among physicians and pharmacists in Saudi Arabia despite guideline recommendations. Targeted educational initiatives and national-level strategies are needed to enhance awareness and integration of apoB testing in risk assessment practices.
Keywords: apolipoprotein B, atherosclerosis, clinical guidelines, lipoproteins, cardiovascular risk
Introduction
Lipoproteins are complex macromolecular nanoparticles involved in the transport of lipids through systemic circulation.1,2 Lipoproteins are categorized into subclasses based on their size, density, and apolipoprotein composition.1 Two major apolipoproteins are apolipoprotein A (apoA) and apolipoprotein B (apoB).3 In particular, apoB defines atherogenic lipoproteins, including very low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), low-density lipoprotein (LDL), and lipoprotein(a).1,3–6 ApoB is a large structural protein, with only a single molecule accommodated within each atherogenic lipoprotein particle, making its plasma concentration a direct and quantitative measure of the total number of circulating atherogenic particles.3–5
Atherosclerotic cardiovascular disease (ASCVD) remains a leading cause of morbidity and mortality worldwide, driven largely by modifiable risk factors, including dyslipidemia.7,8 Traditionally, dyslipidemia management has focused on measuring low-density lipoprotein cholesterol (LDL-C).9,10 In most clinical settings, the close association between LDL-C, non-high-density lipoprotein cholesterol (non–HDL-C), and apoB results in similar cardiovascular risk classification.11–13 However, growing evidence demonstrates that the LDL-C marker alone may not provide a comprehensive assessment of atherogenic risk.4,14,15 LDL-C quantifies the cholesterol mass within LDL particles but does not reflect the number of circulating atherogenic particles.4,15 This limitation may lead to an underestimation of cardiovascular risk in individuals with elevated atherogenic particle numbers that are discordant with their LDL-C levels.4,15 In a Korean population-based analysis of over 9600 adults, 17.5% of individuals with normal traditional lipid profiles were newly identified as high-risk based on elevated apoB levels.16 These findings highlight the clinical utility of apoB in identifying individuals at elevated cardiovascular risk who may be misclassified as low-risk based solely on traditional lipid panels.
ApoB-containing lipoproteins smaller than 70 nm, such as LDL and its remnants, can traverse the endothelial barrier and enter the subendothelial space.17–19 The rate of this penetration is modulated by several pathological conditions, including uncontrolled hypertension, insulin resistance, inflammation, and smoking, all of which increase endothelial permeability and promote lipoprotein retention.17–19 Therefore, apoB measurements are recommended to enhance the assessment of atherogenic particle burden in certain patient populations, including those with metabolic dysfunction, elevated triglycerides, or persistent atherosclerotic risk, despite achieving guideline-recommended LDL-C levels.4,5,10,20,21
Major national and international guidelines recommend apoB as a superior marker of atherogenic risk in selected patient populations.4,5,10,20–22 Table 1 shows the groups most likely to benefit from apoB measurement, including individuals with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, or very low LDL-C levels. However, these guidelines do not endorse apoB testing for all patients or consider it the universal standard of care. Instead, its use is particularly recommended in populations where discordance between LDL-C and atherogenic particle burden is more likely. Despite this, apoB measurement has not been widely adopted in routine clinical practice. For example, a cross-sectional analysis of 2019 United States commercial and Medicare Advantage claims data, involving over 7 million adults, found that only 0.21% received an apoB measurement.23 This significant underutilization in evaluating cardiovascular risk assessment indicates a gap between guideline recommendations and clinical practice.24,25 In Saudi Arabia, studies on the knowledge and practices of healthcare professionals regarding apoB testing in clinical practice are lacking. To address this gap, we evaluated physicians’ and pharmacists’ knowledge of apoB and its role in lipid management and cardiovascular risk stratification. Additionally, we evaluated their practices in apoB testing. Consequently, this study would provide valuable data to health policymakers on the application of up-to-date lipid management guidelines and cardiovascular risk assessment.
 |
Table 1 Guideline-Recommended ApoB Targets and Indicated Patient Populations for Atherogenic Risk Assessment4,5,10,21,22 |
Material and Methods
Study Design, Setting, and Population
This descriptive cross-sectional design targeted licensed physicians and pharmacists from a variety of healthcare institutions across Saudi Arabia who were actively practicing at the time of data collection. Pharmacists were included in this study as integral members of interdisciplinary cardiovascular care teams, with evidence indicating that their involvement improves lipid-lowering therapy optimization.26 The target population was recruited from several healthcare institutions, including specialized cardiac centers, academic medical centers, outpatient clinics, and general hospitals. This range of settings was intended to ensure that the collected data captured the diverse clinical environments and practice patterns. Exclusion criteria were healthcare professionals who were not actively practicing and trainees without an independent license. The study was conducted between February and May 2025.
Study Instrument
The development of the study questionnaire was informed by the current literature and guidelines addressing the role of apoB in managing dyslipidemia and preventing ASCVD.4,21 For content validity, the draft questionnaire was subjected to expert review by two board-certified ambulatory care and cardiology pharmacists, followed by revisions by the study authors to further improve clarity, relevance, and alignment with the study objectives. For face validity, it was pilot tested on a small cohort of healthcare professionals from the target population to ensure a clear understanding, applicability, and feasibility before data collection. The internal consistency of the knowledge domain of the questionnaire was assessed. The Cronbach’s alpha (α) was 0.887, which demonstrated a good level of reliability.27 The questionnaire comprised four parts. The first part included the demographic information and professional characteristics of the participants. The second part included 10 items to evaluate participants’ knowledge regarding the role of apoB in guiding the management of dyslipidemia and the prevention of ASCVD. The response options for the eight items were “yes”, “no”, and “not sure.” Correct answers were given one point, whereas incorrect or unsure answers were given zero points. Item 9 concerned choosing among clinical scenarios with only one correct option. Similarly, item 10 has four options, with only one being the correct answer. Correct answers for items 9 and 10 were also given one point, while incorrect or uncertain responses were given zero points, as they indicated a lack of knowledge. Consequently, the knowledge domain scores ranged from 0 to 10. The third part had two questions to explore the current practice regarding how often a risk calculator was used to estimate the 10-year risk of ASCVD in the participants’ practice for primary prevention, and the other was to assess the current apoB testing practices among the participants. The fourth part sought to evaluate the participants’ interest in attending a continuing educational activity focused on the role of apoB in cardiovascular risk assessment. The complete questionnaire is provided as Supplementary Material 1.
Sampling Method and Data Collection Procedure
The survey was administered online via a restricted-access Google Forms platform, accessible only to the study investigators, and the link was distributed directly to the target participants by the data collection team. Personal identifying information was not collected, which ensured both data security and participant confidentiality. Participation in the study was voluntary, and no incentives were offered to participants for completing the survey. Using the Raosoft® sample size calculator (http://www.raosoft.com/samplesize.html, accessed on 10 November 2024),28 with a margin of error of 5%, a confidence level of 95%, and a 50% level of variance, the sample size was estimated to be 384. A convenience sampling procedure was adopted due to considerations of feasibility and logistical constraints. This sampling approach may limit the generalizability of the findings and thus should be considered when interpreting the results. Given the available resources, the time constraints, and the need to distribute the survey link to healthcare professionals across various practice settings and hospitals, the research team was able to recruit a sample of 158 participants during the study period.
Statistical Analysis
Descriptive statistics, including frequencies, percentages, means, and standard deviations (SD), were used to summarize the data. Inferential statistics, including an independent samples t-test and one-way analysis of variance (ANOVA), were used to explore the associations between the participants’ level of knowledge and their demographics and practice characteristics. When one-way ANOVA indicated a statistically significant difference between groups, post-hoc Tukey’s Honestly Significant Difference (HSD) test was used to determine which specific pairs of groups had statistically significant differences. To examine the association between the knowledge and practice of the participants, the chi-square test for independence and the alternative Fisher’s exact test were used. For this purpose, the level of knowledge was categorized into three levels: low (< 50%), moderate (50 to < 70%), and high (≥ 70%). Data analyses were performed using IBM SPSS Statistics version 30 for Windows (Armonk, NY, USA: IBM Corp). Statistical significance was set at P < 0.05.
Results
Participants’ Demographic Data and Characteristics
Complete responses were received from 158 healthcare professionals from several healthcare institutions in Saudi Arabia. Of these, 58.9% (n = 93) were male, and 41.1% (n = 65) were female. Of the participants, 39.9% (n = 63) were < 35 years old, 38.0% (n = 60) were 35–40 years of age, and 22.1% (n = 35) were aged > 40 years. Regarding the participants’ professions, 50.6% (n = 80) were physicians, and 49.4% (n = 78) were pharmacists. The participants were from different specialties, including cardiology (n = 32; 20.3%), internal medicine (n = 17; 10.8%), family medicine (n = 14; 8.9%), ambulatory care (n = 11; 7.0%), general practitioners (n = 30; 19.0%), and other specialties (n = 54; 34.2%). The primary workplaces of participants were government hospitals and clinics (n = 122; 77.2%). The experience of the participants ranges from ≤ 5 years as a practicing physician or pharmacist (n = 46; 29.1%) to > 15 years (n = 19; 12.0%). The average number of patients per week ranged from < 25 (n = 28; 17.7%) to > 100 patients per week (n = 25; 15.8%). The demographic data and participant characteristics are summarized in Table 2.
 |
Table 2 Demographic and Professional Characteristics of Participants (n = 158) |
Participants’ Knowledge of the Role of ApoB in Guiding the Management of Dyslipidemia and Prevention of ASCVD
The total knowledge score (mean ± SD) was 4.70 ± 3.13 out of a maximum attainable score of 10. Consequently, the overall rate of correct answers to knowledge statements or questions was 47%. Most participants (n = 110; 69.6%) correctly stated that apoB measurement provides additional essential information beyond that provided by a standard lipoprotein lipid panel. Similarly, most participants (n = 110; 69.6%) recognized the role of apoB in quantifying circulating atherogenic particles. However, only 31.0% (n = 49) of participants correctly responded and answered with “No” to the statement “LDL-C is superior to apoB in ASCVD risk assessment.” Only 41.1% (n = 65) of the participants were aware that there were suggested prevention or treatment thresholds for apoB. Less than half of the participants (n = 68; 43.0%) were aware that clinical guidelines had been published in Saudi Arabia, which guide apoB analysis. Of the participants, 45.6% (n = 72) were able to identify that the statement “apoB measurement is only beneficial for assessing the impact of genetic risk factors of dyslipidemia” was incorrect. Similarly, only 37.3% (n = 59) of participants were able to identify that the statement “apoB is only measured in patients who have already experienced a cardiovascular event” is incorrect. Only 26.6% (n=42) of the participants were aware that apoB measurement does not require specialized laboratories. Approximately half of the participants (n = 82; 51.9%) correctly identified the discordance between LDL-C and non–HDL-C levels as a clinical scenario in which apoB testing is most beneficial for ASCVD risk assessment. Similarly, 53.8% (n = 85) of the participants were aware that apoB is the most reliable marker for assessing ASCVD residual risk in patients with lipid profile discordance. The participants’ responses to the statements and questions regarding their knowledge of the roles of apoB are presented in Table 3.
 |
Table 3 Participants’ Knowledge of the Role of ApoB in Guiding the Management of Dyslipidemia and Prevention of ASCVD |
Assessment of Participants’ Practice Regarding Risk Assessment and ApoB Testing
Participants were asked how often they used a risk calculator to estimate the 10-year risk of ASCVD in their primary prevention practice. Of these, 13.3% (n = 21) mentioned that they never used a risk calculator to estimate the 10-year risk of ASCVD, 31.6% (n = 50) mentioned that they rarely used one, and 41.1% (n = 65) mentioned that they occasionally used it. Only 13.9% (n = 22) of the participants frequently used risk calculators to estimate the 10-year risk of ASCVD in their primary prevention practice.
Regarding the routine assessment of apoB levels in patients considered to be at high risk for ASCVD, practices varied among the participants, with only 26.6% routinely assessing apoB levels in these patients. Specifically, 1.9% (n = 3) of the participants indicated that they measured apoB levels for all patients identified as high-risk, and 24.7% (n = 39) reserved apoB testing for specific high-risk cases based on individual assessments. The remaining three-quarters of the participants did not assess apoB levels in their routine practice. However, 27.2% (n = 43) reported considering testing for apoB whenever available in their practice settings. However, 15.2% (n = 24) reported not measuring apoB levels because they did not perceive a need for its use, and 31.0% (n = 49) did not measure it because they were not familiar with its clinical use. The results are summarized in Table 4.
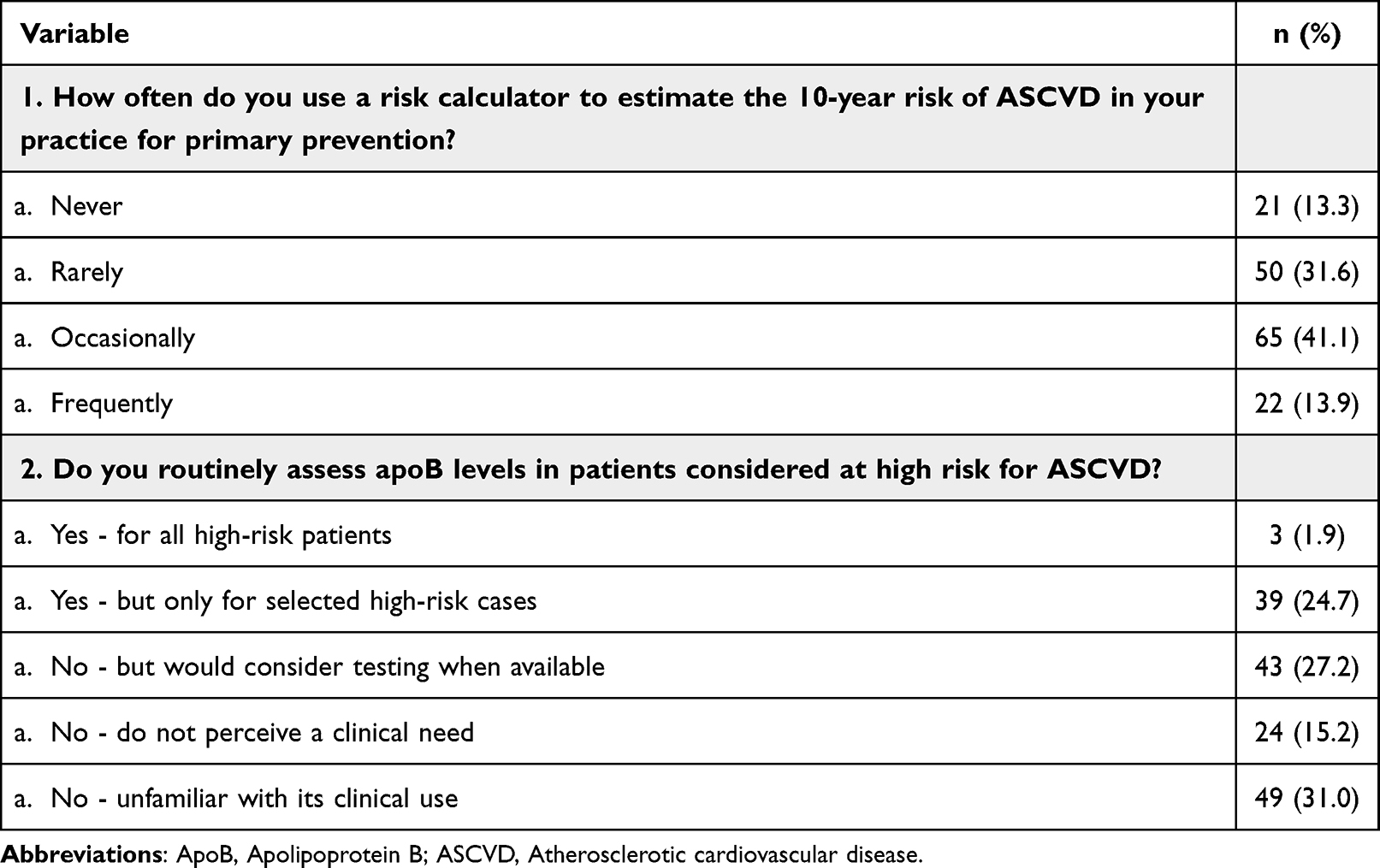 |
Table 4 Questions Regarding Current Apo B Testing Practice |
Perceived Need for Continuing Education on ApoB in Cardiovascular Risk Management
Participants were asked about their interest in attending a continuing education activity focused on the role of apoB in cardiovascular risk assessment. In total, 26.6% (n = 42) reported being very interested, 41.1% (n = 65) were interested, and 25.3% (n = 40) were neutral. Only 3.2% (n = 5) and 3.8% (n = 6) of the participants reported being not interested or very not interested, respectively. The results are shown in Figure 1.
 |
Figure 1 Level of Interest in Attending Continuing Education on ApoB for Cardiovascular Risk Management. |
Association Between Participants’ Demographics and Characteristics and Their Level of Knowledge of the Role of ApoB
As shown in Table 5, statistically significant differences were observed in the level of knowledge among study participants in terms of their demographic and practice characteristics. The female participants exhibited a higher level of knowledge (mean ± SD = 5.29 ± 3.14) than the male participants (4.28 ± 3.07; P = 0.045).
 |
Table 5 Association Between Participants’ Demographic and Professional Characteristics and Their Knowledge of the Role of ApoB |
In terms of age, younger participants (aged < 35 years) had a lower level of knowledge (3.06 ± 2.63) than participants aged 35–40 years (5.78 ±2.77) and those aged 41–45 years (6.05 ± 3.36; P < 0.001).
In terms of specialty, participants specializing in cardiology (6.53 ± 3.03) had a statistically significantly higher level of knowledge than GPs (3.67 ± 2.59; P = 0.002) and other medical specialties (3.41 ± 2.88; P < 0.001). Similarly, participants in family medicine demonstrated a higher level of knowledge (6.79 ± 2.69) than GPs (P = 0.012) and other medical specialties (P < 0.002).
In terms of years of experience, participants with 11–15 years of experience demonstrated a higher level of knowledge (6.34 ± 3.10) than those with 1–5 years (3.26 ± 2.74; P < 0.001) and those with 6–10 years (4.69 ± 2.79; P = 0.037).
In terms of the number of patients seen per week, participants who reported managing 51–75 patients per week demonstrated a statistically significantly higher level of knowledge (5.96 ± 2.60) than those managing < 25 patients (2.82 ± 2.51; P < 0.001), 25–50 patients (4.06 ± 2.81; P = 0.027), and > 100 patients (3.48 ± 3.33; P = 0.005). Similarly, participants who reported managing 76–100 patients per week recorded a significantly higher level of knowledge (6.58 ± 3.08) than those managing < 25 (P < 0.001), 25–50 (P = 0.009), and > 100 patients (3.48 ± 3.33; P = 0.002).
Association Between the Level of Knowledge and Practice of Risk Assessment and ApoB Testing
As shown in Table 6, statistically significant associations were found between the level of knowledge and practice of risk assessment and apoB testing.
 |
Table 6 Association Between the Level of Knowledge and Practice of Risk Assessment and ApoB Testing |
A higher proportion of participants with high knowledge occasionally or frequently used the risk calculator to estimate the 10-year risk of ASCVD than participants with moderate and low levels of knowledge (74.5%, 53.1%, and 39.6%, respectively; P = 0.001).
Similarly, a higher proportion of participants with high knowledge reported measuring apoB levels or considering it whenever available in their practice than those with moderate and low levels of knowledge (88.2%, 53.1%, and 24.1%, respectively; P < 0.001).
Discussion
The findings of the study revealed gaps in knowledge and practices among many participants. The overall rate of correct responses to knowledge questions about apoB was 47%, and only 13.9% of the participants reported the routine use of a 10-year ASCVD risk calculator. Although guideline-directed prevention strategies for ASCVD are well established, their uptake in clinical practice remains limited.29 A survey conducted at a single center in Saudi Arabia found that approximately 40% of family physicians did not incorporate ASCVD risk estimators into their clinical practice.30 These findings highlight the need for improvement in this area of practice. This could be addressed through initiatives and strategies to ensure the translation of clinical guidelines into daily practice.
In this study, only 26.6% of participants routinely assessed apoB in high-risk ASCVD patients, suggesting missed opportunities for more accurate risk stratification and lipid management. In addition, despite guideline recommendations favoring apoB for detecting residual atherogenic risk, 69% of the participants either perceived LDL-C as a superior marker for ASCVD risk assessment or were unsure. Limited awareness of the national dyslipidemia guidelines, which include recommendations on apoB measurement and treatment thresholds, may further contribute to its underutilization in clinical practice. From an economic perspective, broader adoption of apoB testing would not result in a substantial financial burden. In the United States, adding apoB testing to routine lipid panels at each visit marginally raises costs by approximately 1%.31 Moreover, repeated measurements at every follow-up visit are unnecessary, further mitigating any incremental economic impact.15 This is particularly important, as it was evident in our study that participants with high knowledge were more likely to measure the apoB level or consider it whenever available in their practice than those with lower levels of knowledge.
Most participants in this study thought that apoB testing required specialized laboratories or were unsure about this aspect. ApoB testing does not require specialized laboratory infrastructure; clinical laboratories routinely perform apoB testing using standardized automated immunoassays.32 National and international guidelines have emphasized that apoB measurement is technically feasible and readily implementable within existing laboratory systems.4,5,10,21,22 Therefore, the underutilization of apoB testing is more likely attributable to clinician awareness, ordering practices, uncertainty about appropriate apoB target levels or how to interpret and act on the results, and familiarity with guidelines, rather than logistical or technical barriers.15
Upon further evaluation of the participants’ demographics, the study identified significant associations between some demographic and practice characteristics and knowledge levels regarding the role of apoB in managing dyslipidemia and preventing ASCVD. Participants specializing in family medicine and cardiology demonstrated significantly higher apoB-related knowledge scores than general practitioners and other specialties. Physicians demonstrated significantly higher apoB-related knowledge scores than pharmacists. These findings suggest that a higher level of engagement in cardiovascular risk stratification is associated with a better understanding of the clinical role of apoB testing. Furthermore, knowledge scores were modestly but significantly higher among female participants. Participants under 35 years of age had significantly lower knowledge scores than their older peers, with the highest scores found in the 41–45 age group. The rapid expansion of medical knowledge may disproportionately challenge early-career healthcare providers, who are still developing the experience and strategies needed to stay current.33
This study is, to our knowledge, the first to specifically assess apoB-related knowledge and practice among both physicians and pharmacists in Saudi Arabia. The interdisciplinary focus represents a novel contribution and has revealed important insights. For example, we found that pharmacists had significantly lower apoB knowledge scores compared to physicians. Such a disparity between professions has not been highlighted in previous literature and suggests a need for targeted educational outreach to pharmacy professionals. The study included a diverse cohort of participants from various professional backgrounds and medical specialties, offering a broad perspective on the current practice patterns.
This study has several important implications and provides valuable data to inform health policy decisions and provide future guidance. The study indicated that apoB testing is infrequently utilized in routine clinical practice as a marker for cardiovascular risk assessment despite the well-established utility of apoB in identifying residual ASCVD risk. Consequently, the findings of this study could be a foundation for developing targeted educational initiatives, such as continuing medical education (CME) programs, to enhance the integration of evidence-based recommendations and the interdisciplinary management of cardiovascular risk. It also highlights the importance of establishing institutional protocols that incorporate apoB testing in appropriately selected high-risk populations to ensure a thorough evaluation of residual ASCVD risk.
Strengths and Limitations
This study provides new insights into the knowledge and practices of physicians and pharmacists regarding apoB testing. It sheds light on the status of applying evolving lipid management guidelines in real-world settings, providing implications for the Saudi healthcare system and beyond. However, the study had some limitations. Most participants were recruited from government hospitals and clinics. However, government institutions are the major providers of healthcare services in Saudi Arabia. The study employed a convenience sampling strategy and had a relatively small sample size. These limitations could limit the generalizability of the results to the whole country. However, as mentioned earlier, these limitations were unavoidable due to logistical barriers and available resources. Overall, we believe the study provides valuable data and guidance to help health policymakers design strategies related to applying up-to-date lipid management guidelines and best practices of cardiovascular risk assessment. This is particularly important given the scarcity of existing literature on this topic, especially the knowledge and practices of healthcare providers regarding ApoB testing in real practice settings. Future studies should investigate whether enhanced apoB adoption enhances dyslipidemia management outcomes, particularly in populations in which inaccurate risk stratification may increase preventable ASCVD events.
Conclusion
Despite the endorsement of apoB testing by several international guidelines as a superior marker for cardiovascular risk assessment, its clinical adoption by physicians and pharmacists in Saudi Arabia remains limited. This study demonstrates that apoB testing is infrequently incorporated into routine practice. These findings underscore the need for targeted educational initiatives to enhance awareness and understanding of the clinical utility of apoB in lipid management and cardiovascular risk stratification. Additionally, more national guidance and institutional protocols are essential to support the integration of apoB testing into clinical workflows, ensuring comprehensive risk assessment and management of dyslipidemia. Future research should explore the impact of improved apoB adoption on clinical outcomes, particularly in populations at risk of misclassification using traditional lipid panels. Addressing these gaps could lead to more effective prevention strategies and better management of the ASCVD risk.
Data Sharing Statement
The technical appendix, statistical code, and de-identified dataset are available from the corresponding author upon reasonable request. The data have not been deposited in a public repository.
Ethics Approval and Informed Consent
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of King Fahad Medical City, Riyadh, Saudi Arabia (IRB Log Number: 24-685E). This study was conducted following the principles of the Declaration of Helsinki. The first item in the questionnaire served as an informed consent statement requiring participants to confirm their voluntary agreement to participate in the study.
Acknowledgments
The Researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2025).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors. Only the open-access fee was covered by financial support from Qassim University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sniderman AD, Thanassoulis G, Glavinovic T, et al. Apolipoprotein B Particles and Cardiovascular Disease: a Narrative Review. JAMA Cardiol. 2019;4(12):1287. doi:10.1001/jamacardio.2019.3780
2. Berndsen ZT, Cassidy CK. The structure of apolipoprotein B100 from human low-density lipoprotein. Nature. 2025;638(8051):836–843. doi:10.1038/s41586-024-08467-w
3. Glavinovic T, Thanassoulis G, de Graaf J, Couture P, Hegele RA, Sniderman AD. Physiological Bases for the Superiority of Apolipoprotein B Over Low-Density Lipoprotein Cholesterol and Non-High-Density Lipoprotein Cholesterol as a Marker of Cardiovascular Risk. J Am Heart Assoc. 2022;11(20):e025858. doi:10.1161/JAHA.122.025858
4. Soffer DE, Marston NA, Maki KC, et al. Role of apolipoprotein B in the clinical management of cardiovascular risk in adults: an Expert Clinical Consensus from the National Lipid Association. J Clin Lipidol. 2024;18(5):e647–e663. doi:10.1016/j.jacl.2024.08.013
5. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188. doi:10.1093/eurheartj/ehz455
6. Alhomoud IS, Talasaz A, Mehta A, et al. Role of lipoprotein(a) in atherosclerotic cardiovascular disease: a review of current and emerging therapies. Pharmacother J Hum Pharmacol Drug Ther. 2023;43(10):1051–1063. doi:10.1002/phar.2851
7. Global Cardiovascular Risk Consortium, Magnussen C, Ojeda FM, et al. Global Effect of Modifiable Risk Factors on Cardiovascular Disease and Mortality. N Engl J Med. 2023;389(14):1273–1285. doi:10.1056/NEJMoa2206916.
8. Mensah GA, Fuster V, Murray CJL, Roth GA. Global Burden of Cardiovascular Diseases and Risks Collaborators. Global Burden of Cardiovascular Diseases and Risks, 1990-2022. J Am Coll Cardiol. 2023;82(25):2350–2473. doi:10.1016/j.jacc.2023.11.007
9. Wilkinson MJ, Lepor NE, Michos ED. Evolving Management of Low-Density Lipoprotein Cholesterol: a Personalized Approach to Preventing Atherosclerotic Cardiovascular Disease Across the Risk Continuum. J Am Heart Assoc. 2023;12(11):e028892. doi:10.1161/JAHA.122.028892
10. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25). doi:10.1161/CIR.0000000000000625
11. Collaboration ERF, Di Angelantonio E, Gao P, et al. Lipid-related markers and cardiovascular disease prediction. JAMA. 2012;307(23):2499–2506. doi:10.1001/jama.2012.6571
12. van den Berg MJ, van der Graaf Y, de Borst GJ, et al. Low-Density Lipoprotein Cholesterol, Non-High-Density Lipoprotein Cholesterol, Triglycerides, and Apolipoprotein B and Cardiovascular Risk in Patients With Manifest Arterial Disease. Am J Cardiol. 2016;118(6):804–810. doi:10.1016/j.amjcard.2016.06.048
13. van Deventer HE, Miller WG, Myers GL, et al. Non-HDL cholesterol shows improved accuracy for cardiovascular risk score classification compared to direct or calculated LDL cholesterol in a dyslipidemic population. Clin Chem. 2011;57(3):490–501. doi:10.1373/clinchem.2010.154773
14. Sniderman AD, Navar AM, Thanassoulis G. Apolipoprotein B vs Low-Density Lipoprotein Cholesterol and Non–High-Density Lipoprotein Cholesterol as the Primary Measure of Apolipoprotein B Lipoprotein-Related Risk: the Debate Is Over. JAMA Cardiol. 2022;7(3):257. doi:10.1001/jamacardio.2021.5080
15. Sniderman AD, Dufresne L, Pencina KM, Bilgic S, Thanassoulis G, Pencina MJ. Discordance among apoB, non–high-density lipoprotein cholesterol, and triglycerides: implications for cardiovascular prevention. Eur Heart J. 2024;45(27):2410–2418. doi:10.1093/eurheartj/ehae258
16. Choi R, Sg L, Eh L. Effect of Adding Apolipoprotein B Testing on the Prevalence of Dyslipidemia and Risk of Cardiovascular Disease in the Korean Adult Population. Metabolites. 2024;14(3):169. doi:10.3390/metabo14030169
17. Miller M, Stone NJ, Ballantyne C, et al. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123(20):2292–2333. doi:10.1161/CIR.0b013e3182160726
18. Takahashi M, Yagyu H, Tazoe F, et al. Macrophage lipoprotein lipase modulates the development of atherosclerosis but not adiposity. J Lipid Res. 2013;54(4):1124–1134. doi:10.1194/jlr.M035568
19. Wang L, Gill R, Pedersen TL, Higgins LJ, Newman JW, Rutledge JC. Triglyceride-rich lipoprotein lipolysis releases neutral and oxidized FFAs that induce endothelial cell inflammation. J Lipid Res. 2009;50(2):204–213. doi:10.1194/jlr.M700505-JLR200
20. Wilson PWF, Jacobson TA, Martin SS, et al. Lipid measurements in the management of cardiovascular diseases: practical recommendations a scientific statement from the national lipid association writing group. J Clin Lipidol. 2021;15(5):629–648. doi:10.1016/j.jacl.2021.09.046
21. AlRahimi J, AlSaif S, Alasnag M, et al. 2022 Saudi Guidelines for the Management of Dyslipidemia. Heart Views off J Gulf Heart Assoc. 2023;24(2):67–92. doi:10.4103/heartviews.heartviews_102_22
22. Pearson GJ, Thanassoulis G, Anderson TJ, et al. 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults. Can J Cardiol. 2021;37(8):1129–1150. doi:10.1016/j.cjca.2021.03.016
23. Murdock DJ, Moll K, Sanchez RJ, et al. Low prevalence of testing for apolipoprotein B and lipoprotein (a) in the real world. Am J Prev Cardiol. 2024;19:100721. doi:10.1016/j.ajpc.2024.100721
24. Alhomoud IS, Aldakhil SA, Alhosan RF, et al. Knowledge, Counseling Practice, Perceived Barriers, and Clinical Decision-Making of Community Pharmacists in Saudi Arabia Regarding Glucagon-Like Peptide-1 Receptor Agonists and Sodium-Glucose Cotransporter 2 Inhibitors. Diabet Metab Syndr Obes Targets Ther. 2025;18:3093–3107. doi:10.2147/DMSO.S552287
25. Martelli E, Enea I, Zamboni M, et al. Focus on the Most Common Paucisymptomatic Vasculopathic Population, from Diagnosis to Secondary Prevention of Complications. Diagn Basel Switz. 2023;13(14):2356. doi:10.3390/diagnostics13142356
26. Charrois TL, Zolezzi M, Koshman SL, et al. A systematic review of the evidence for pharmacist care of patients with dyslipidemia. Pharmacotherapy. 2012;32(3):222–233. doi:10.1002/j.1875-9114.2012.01022.x
27. Bland JM, Dg A. Cronbach’s alpha. BMJ. 1997;314(7080):572. doi:10.1136/bmj.314.7080.572
28. Raosoft. Raosoft Sample Size Calculator.
29. Virani SS. Statins and Primary Atherosclerotic Cardiovascular Disease Prevention—What We Know, Where We Need to Go, and Why Are We Not There Already? JAMA Netw Open. 2022;5(8):e2228538. doi:10.1001/jamanetworkopen.2022.28538
30. Almigbal TH, Almunif DS, Ali Deshisha E, et al. Physicians’ perceptions and beliefs on the current dyslipidemia management practices within Saudi Arabia. Saudi Pharm J. 2023;31(10):101759. doi:10.1016/j.jsps.2023.101759
31. Kohli-Lynch CN, Thanassoulis G, Moran AE, Sniderman AD. The clinical utility of apoB versus LDL-C/non-HDL-C. Clin Chim Acta Int J Clin Chem. 2020;508:103–108. doi:10.1016/j.cca.2020.05.001
32. Contois JH, Langlois MR, Cobbaert C, Sniderman AD. Standardization of Apolipoprotein B, LDL-Cholesterol, and Non-HDL-Cholesterol. J Am Heart Assoc. 2023;12(15):e030405. doi:10.1161/JAHA.123.030405
33. Densen P. Challenges and opportunities facing medical education. Trans Am Clin Climatol Assoc. 2011;122:48–58.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.