")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Anxiety and Depression in Patients with Alopecia Areata in Eskisehir, Turkey
Received 4 June 2023
Accepted for publication 3 September 2023
Published 7 September 2023 Volume 2023:16 Pages 2443—2450
DOI https://doi.org/10.2147/CCID.S424374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Hamza Yildiz,1 Serkan Zincir2
1Department of Dermatology, Eskisehir Yunus Emre State Hospital, Eskisehir, Turkey; 2Department of Psychiatry, Eskisehir Yunus Emre State Hospital, Eskisehir, Turkey
Correspondence: Hamza Yildiz, Department of Dermatology, Eskisehir Yunus Emre State Hospital, Eskisehir, Turkey, Tel +90 222 220 45 30, Email [email protected]
Background: Conflicting results have emerged in studies conducted to reveal the relationship between alopecia areata (AA) and depression and anxiety. The comorbidity of depression and anxiety in patients with patchy AA who applied to a tertiary care center will be investigated and compared with a healthy control group.
Methods: This study included 86 patients with AA and 85 healthy volunteers. The patients and controls completed Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BDI).
Results: The average BDI of the patient group was 13.45± 8.59, while in the control group, it was 7.2± 5.7 (p = 0.002). The average BAI of the patient group was 12.56± 8.76, while in the control group, it was 6.01± 5.87 (p = 0.019). Depression was detected in 30.2% (n = 26) of the patients and anxiety was detected in 19.8% (n = 17) of the patients. In the control group, the rate of depression was 5.9% (n = 5) and the rate of anxiety was 7.1% (n = 6). There was a statistically significant difference between the patients and the control group in terms of depression (p < 0.001) and anxiety (p < 0.001).
Conclusion: Depression and anxiety were more prevalent in patients with AA than in healthy volunteers. Dermatologists should keep in mind psychiatric diseases such as depression and anxiety that may accompany patients diagnosed with AA.
Keywords: alopecia, alopecia areata, anxiety, Beck Depression Inventory, Beck Anxiety Inventory, depression
Background
Alopecia areata (AA) is a very common (2–3.5%), sudden onset, non-cicatricial, auto-immune disease.1 While it primarily affects the hair, it can also have emotional and psychological effects on individuals who suffer from it.2–4 Hair loss, especially in noticeable and sometimes unpredictable patterns, can lead to feelings of self-consciousness, embarrassment, and a decline in self-esteem. This can result in social withdrawal and avoidance of public situations. Insensitive comments or questions from others can contribute to feelings of isolation and sadness. The fear of being rejected or judged by others because of their appearance can lead to heightened anxiety and social anxiety.2–7
The sudden and unpredictable nature of hair loss in alopecia areata can lead to heightened levels of anxiety. People with alopecia areata often experience worries about their appearance, social interactions, and how others perceive them. They might feel self-conscious, fearing that others are staring or making judgments about their condition. This anxiety can be particularly strong during social events, public appearances, or when meeting new people. Chronic stress and anxiety associated with alopecia areata can contribute to the development of depression in some individuals.2–9
It has a negative effect on patients in terms of cosmetic appearance. Anxiety and depression are the most common psychopathology in adult patients.2–4 Some of the studies have found that anxiety and depression are more common in patients with alopecia areata.2–9 However, in some studies, these findings are not supported.10–12
In this cross-sectional study, the comorbidity of depression and anxiety in patients with patchy AA who applied to a tertiary care center will be investigated and compared with a healthy control group.
Methods
This study was designed as a cross-sectional study.
Study Population
Patients with patchy AA and healthy volunteers who applied to the dermatology outpatient clinic of our tertiary healthcare institution between November 2022 and December 2022 were included in our study.
The criteria for inclusion in this clinical trial for healthy volunteers are as follows; being over the age of 18, not having a current or previous diagnosis of alopecia areata, agreeing to participate in the study, and signing the informed consent form.
A physical examination of the patients was performed. Patients with AA are analyzed in 5 groups according to severity of alopecia tool (SALT) scores such as SALT 1, SALT 2, SALT 3, SALT 4, and SALT 5. The locations of the plaques of the patients with alopecia areata, the number of attacks, the duration of the lesion’s existence, and the treatments used were questioned and noted. The participants were asked about their age, gender, educational status, marital status, and employment status, and their answers were recorded. Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BDI) questionnaires were filled in by the patient and control groups.
Questionnaires
Beck Depression Scale
The BDI is a 21-item self-report inventory that measures the somatic, emotional, cognitive, and motivational symptoms of depression. The purpose of the scale is not to diagnose depression. It is to objectively determine the degree of depression. The 21 category signs have 4 options. The subject marks one of the 4 options, which are determined as 0, 1, 2, and 3 according to the previous week’s experience. The overall score is the sum of the points awarded to the 21 items. It shows that the depression level increases as the score increases. It was developed by Beck et al.13 It was modified by Hisli et al for Turkish society.14 It has been reported that a score of 17 and above indicates clinical depression in the Turkish population.
Beck Anxiety Scale
BAI is proposed as an instrument to assess clinical anxiety. The BAI is a 21-item survey. Individuals fill out this form themselves. The questions include anxiety symptoms. Physical (tremor, etc.), cognitive (fear of losing control, fear that something terrible will happen, etc.), and emotional state (anger, tension, etc.) collects information. Participants are asked to score each symptom according to a Likert-type scale of 0, 1, 2, and 3 points over the past week. Higher scores represent higher levels of anxiety. This questionnaire was developed by Beck et al. It was adapted to the Turkish population by Ulusoy et al.15
Statistical Analysis
Statistical analysis of the obtained data was done with SPSS version 22.0. Pearson chi-square test was used to analyze whether there was a difference between the discrete variables between the groups. Student’s t-test was used to determine whether there was a difference between the variables. Continuous variables were given as mean ± standard deviation and discrete variables as numbers and percentages. A p-value below 0.05 was considered statistically significant.
The numerical figures obtained from the measurements were expressed as mean±standard deviation, and the data obtained by counting were expressed as frequency (%). The prevalence of the above was evaluated using the Fischer exact test.
Results
Patient’s Demographics
A total of 171 participants (patients with AA and healthy individuals), 86 of whom had AA and 85 of whom were healthy volunteers, were included in this study. The mean age of participants was 32.94±10.73 (range, 20–65) years. Of these patients, the mean age of female participants was 34.15±11.56 (range, 20–60) years. The mean age of male patients was 31.92±9.92 years, ranging from 20 years to 65 years.
The study reviewed a total of 86 patients with AA, including 29 (33.7%) female and 57 (66.3%) male patients. The mean age of patients was 33.41±11.09 (range, 20–65) years. Of these patients, the mean age of female patients was 35.55±12.83 (range, 20–60) years. The mean age of male patients was 32.33±10.05 years, ranging from 20 years to 65 years.
The study reviewed a total of 85 healthy volunteers, including 49 (57.6%) female and 36 (42.4%) male healthy volunteers. The mean age of healthy volunteers was 32.45±10.39 (range, 20–56) years. Of these healthy volunteers, the mean age of female patients was 33.32±10.79 (range, 20–56) years. The mean age of male healthy volunteers was 31.27±9.84 years, ranging from 20 years to 54 years.
There was no statistically significant difference between the mean age of the patients with AA and healthy individuals (p = 0.71). Similarly, when the age groups were compared, there was no significant difference between the groups (p= 0.58).
42 (48.8%) were married and 44 (51.2%) were single in the patients with AA, whereas 35 (41.2%) were married and 36 (42.4%) were single in the healthy individuals. The difference was not significant (p = 0.19).
In the patients with AA, 46 (53.5%) patients were employed, 35 (40.7) patients were unemployed and 5 (5.8%) patients were retired. In the control group, 34 (40%) patients had a job, 50 (28.8) patients were unemployed, and 1 (1.2%) patient were retired. When the groups were compared in terms of unemployment, it was found to be statistically significant between the groups (p= 0.02).
When their educational status was examined, there were 8 (9.3%) patients at the elementary level, 27 (31.4%) patients at the secondary level, and 51 (59.3) patients who graduated from the university in the patient group. This was 6 (7.1%), 34 (40%), and 45 (52.9%) respectively, in the control group. When the groups were compared in terms of educational status, it was not found statistically significant between the groups (p= 0.48).
The mean disease duration of 86 AA patients was found to be 4.89±10.27 months.
The socio-demographic characteristics of the case and control groups are presented in Table 1.
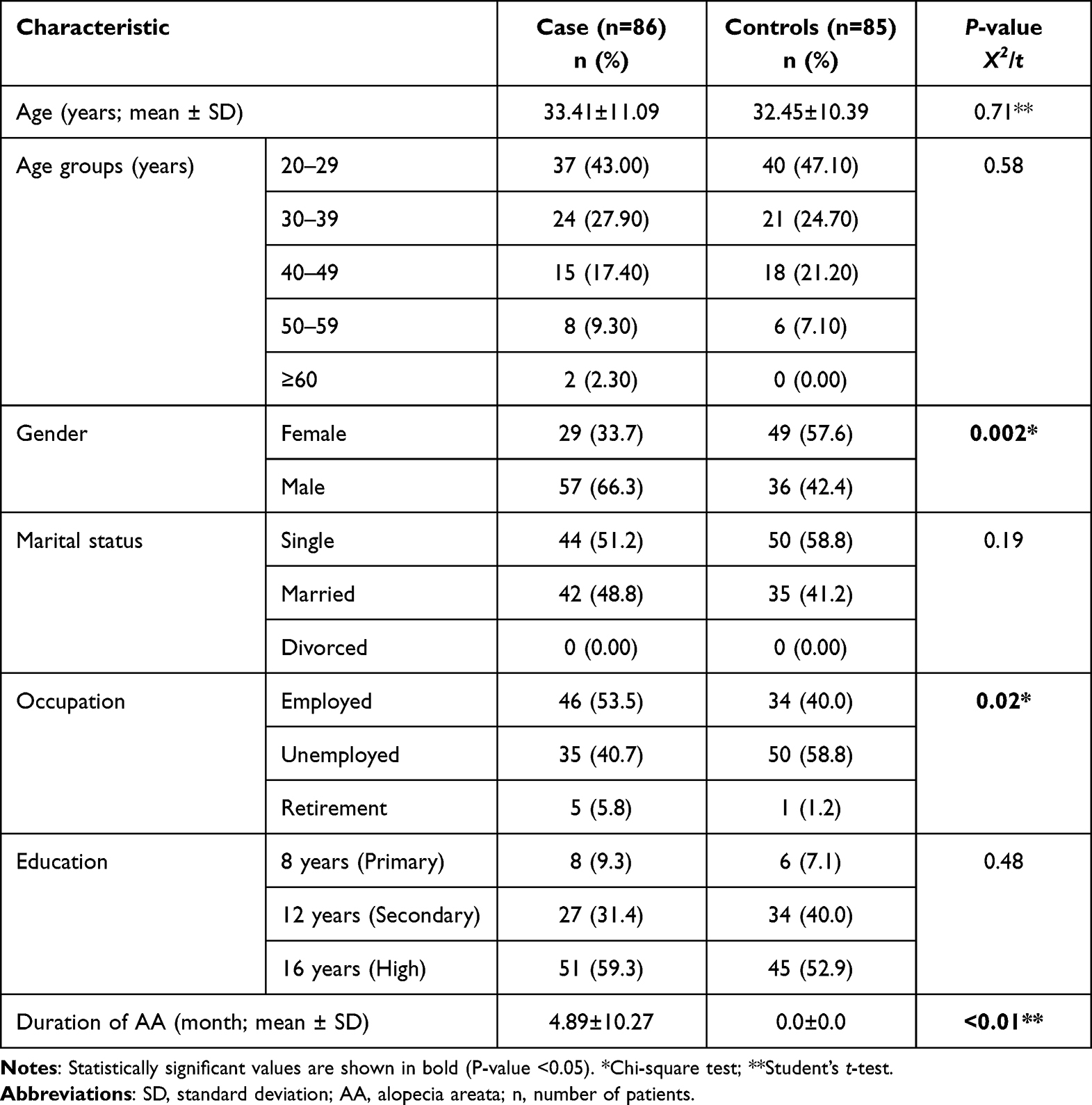 |
Table 1 Sociodemographic Characteristics of the Case and Control Groups |
The average BDI of the patient group was 13.45±8.59, while in the control group, it was 7.2±5.7, and there was a statistically significant difference (p = 0.002). When the presence and absence of depression were compared in the patient and control group for men (p = 0.01) and women (p < 0.01), there was a statistically significant difference between the two groups.
The average BAI of the patient group was 12.56±8.76, while in the control group, it was 6.01±5.87, and there was a statistically significant difference (p= 0.019). The presence and absence of anxiety for men (p = 0.86) and women (p < 0.001). Decisively compared in the patient and control group, there was no statistically significant difference in men but there was in women between the two groups.
In the patients with AA, depression was detected in 26 (30.2%) patients, and anxiety was found in 17 (19.7%) patients. In healthy individuals, depression was detected in 5 (11.6%) patients, and anxiety was found in 6 (15.19%) patients. The frequency of depression and anxiety based on sex is presented in Table 2.
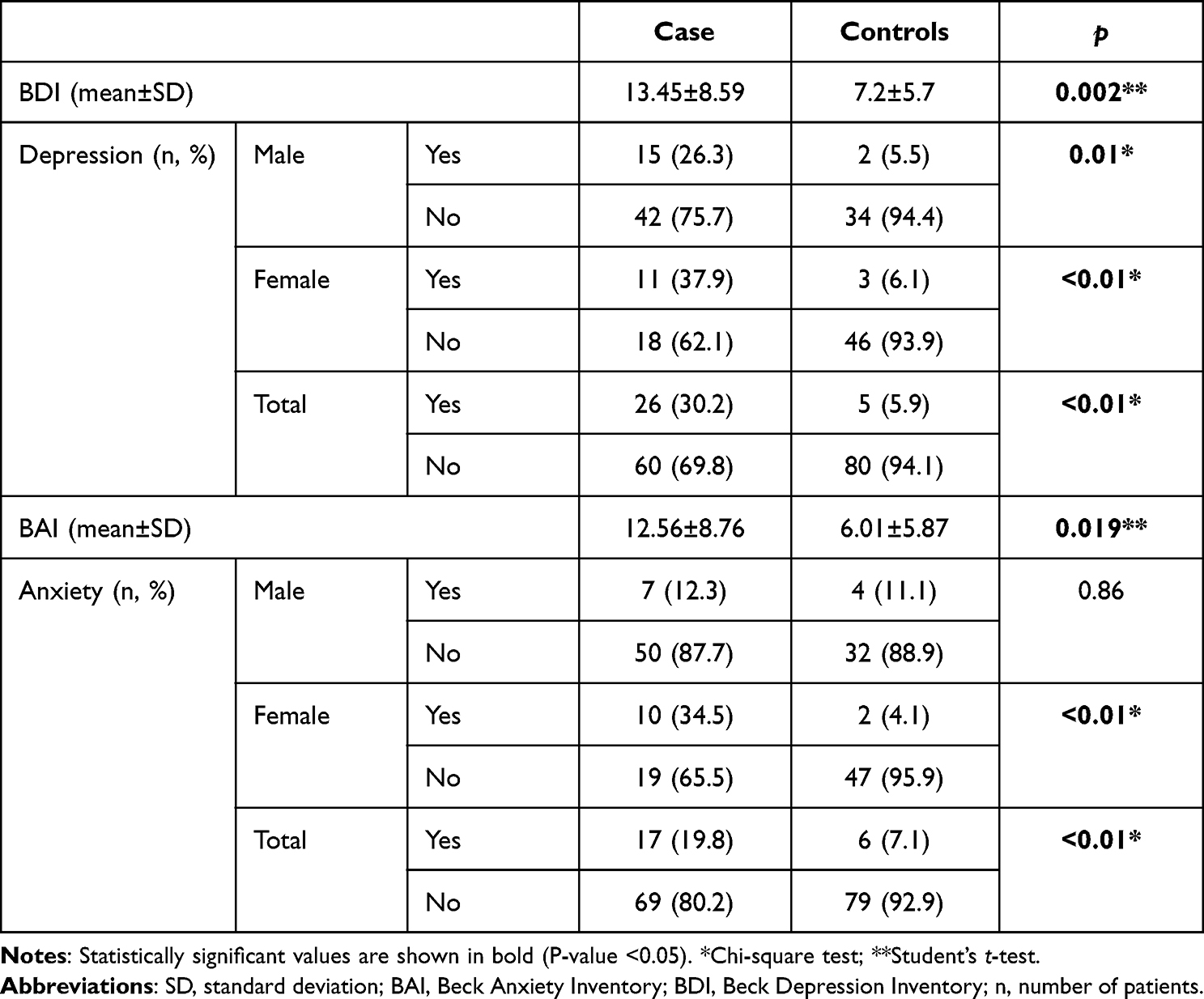 |
Table 2 Frequency of Depression and Anxiety Based on Sex |
Table 3 demonstrates the prevalence of anxiety and depression in the groups based on occupation, education, and marital status.
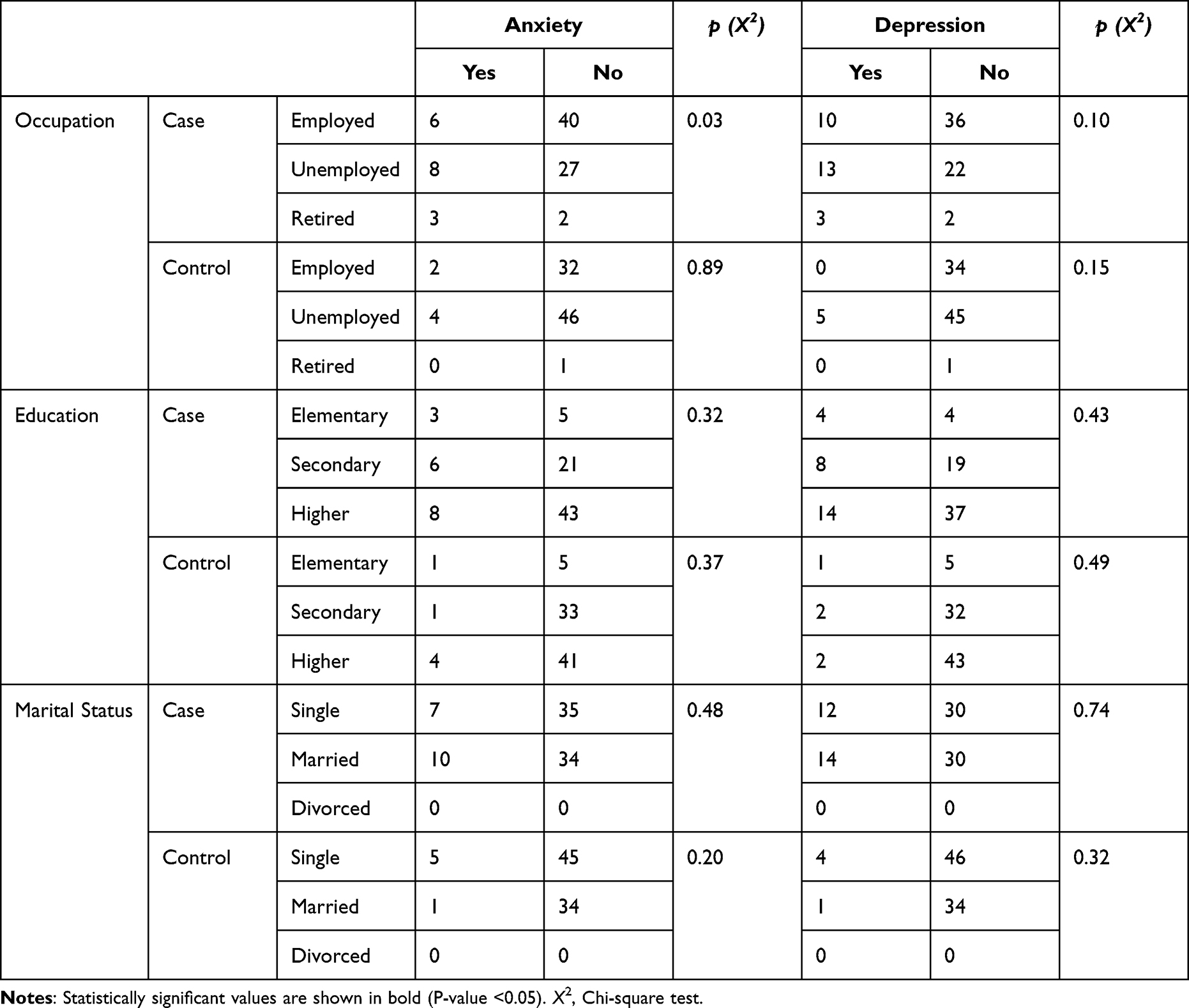 |
Table 3 Prevalence of Anxiety and Depression in the Groups Based on Occupation, Education, and Marital Status |
The presence of depression and anxiety in patients was investigated in these groups. Depression was found in 22 of the cases in SALT 1 (n=81, 94.2%) and anxiety was found in 15 patients. Depression was found in 3 of the patients in SALT 2 (n = 4, 4.7%) and anxiety in one. There was only one patient in SALT 3 and this patient was found to have depression and anxiety. There were no patients in the SALT 4 and 5 groups. Table 4 shows the frequency and mean of the depression and anxiety scores of the patients with AA based on the severity of the AA.
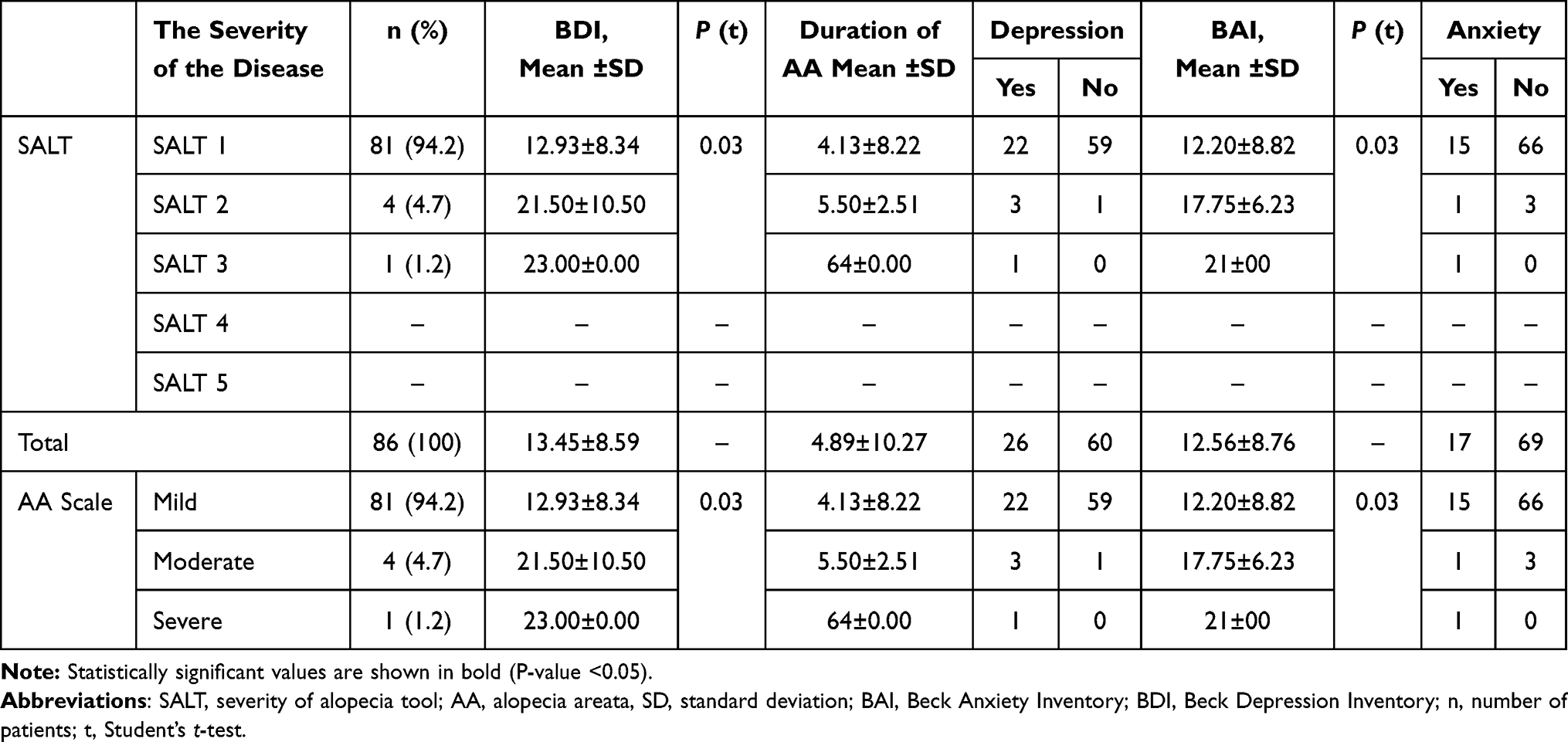 |
Table 4 Frequency and Mean of the Depression and Anxiety Score of the Case Group Based on the Severity of the Alopecia Areata |
Discussion
Although AA can occur at any age, the first onset is often in the third and fourth decades of life. The mean age of onset for AA was reported between 25.2 and 36.3 years in the review by Frinke et al.16 Consistent with this in our study, 43% of the patients who applied to our clinic with the complaint of AA were between the ages of 20–29.
In our study, the patient and case group were compared in terms of educational status, and no statistically significant difference was found (p = 0.48). Contrary to our study, Aghaei et al found that the patient group had a lower level of education when compared with the control group. They explained the reason for the lower educational level being more common in the case group as follows. The low level of education, as a result, leads to personal and social problems, and vice versa. Problems that prevent a person from continuing their education can have undesirable effects on a person psychologically and mentally.17
In various studies, the prevalence of lifetime psychiatric disorders in AA patients has been reported as 66–74%. The prevalence of generalized anxiety disorder was found to be 39%-62%, while the lifetime prevalence of depression was found to be 38–39%.6,11,18,19
When the studies investigating the prevalence of depression in AA patients are reviewed, there are 3 patient groups: pediatric patients, children and adults, and adults only. Our study is to compare the prevalence of depression and anxiety in adult AA patients with the control group. For this reason, studies in which adult patients with AA were examined were reviewed. Colon et al reported that the lifetime depression rate was 39% in their study. The point prevalence rates found in various cross-sectional studies are as follows; 7.4%,6 18%,3 21.74%,7 and 55.29%.8 In the study conducted by Senna et al in 2021, the prevalence was found to be 9.5%.20 Also, adults with AA have a higher chance of being diagnosed with depressive disorder than healthy controls.2–4,9 In our study, the prevalence of depression was 30.2% (n = 26) in the case group, while it was 5.9% (n = 5) in the control group (p < 0.001).
Some studies do not support these studies. Conic et al found 14.7% depression in patients with AA and 11% in the control group and did not detect a significant difference between them (p = 0.19).12 31 AA patients, 29 vitiligo patients, and 30 control patients volunteered to participate in the study of Erdogan et al. There was no statistically significant difference between the patients with AA and the control group according to the BDI (p = 0.110) inventory.21
In studies investigating the prevalence of anxiety in adult AA patients, point prevalence rates were reported as 3.24%,4 4%,3 8.4%,20 and 13.70%.12 In addition, some case-control studies reported that people with AA had a higher chance of being diagnosed with an anxiety disorder compared to healthy controls.2–4,9,22,23
Aghaei et al included 40 patients with AA and 40 control patients in their study using the BDI and BAI. They found that there were more depression (p=0.008) and anxiety (p=0.003) in the patient group than in the control group.17 They applied the BDI and BAI inventory to the participants. It varies between 22.2–39% for generalized anxiety disorders in people with AA.6,11 The findings in our study were similar to these publications. The prevalence of anxiety was 19.8% (n = 17) in the case group, while it was 7.1% (n = 6) in the control group (p < 0.001).
Some studies do not support these studies. Conic et al found 13.7% anxiety in patients with AA and 9.9% in the control group and did not detect a significant difference between them (p = 0.19).12 Cordan et al included 43 patients with AA and 53 healthy volunteers, and it was not found statistically significant in terms of anxiety between the groups (p > 0.05).24 There was no statistically significant difference between the patients with AA and the control group according to the BDI (p = 0.110) and BAI (p = 0.169) inventory.10
Limitations
The main limitation of this study is that the number of participants is low. Apart from this, in addition to being cross-sectional and single-centered, the absence of structured interviews and psychiatric evaluations can be considered another limitation.
Conclusion
Depression and anxiety were more prevalent in patients with AA than in healthy volunteers. Dermatologists should keep in mind psychiatric diseases such as depression and anxiety that may accompany patients diagnosed with AA.
Ethical Consideration
The required ethical approval was obtained from the Ethics Committee of Osmangazi University (E-80558721-050.99-2300043495, 2022-62). This study is done in accordance with the Helsinki Declaration.
Informed Consent
Participants and volunteers were informed about the purpose of the study and informed consent was obtained.
Funding
The authors received no specific funding for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sayar K, Köse O, Ebrinç S, Çetin M. Hopelessness, depression and alexithymia in young Turkish soldiers suffering from alopecia areata. Dermatol Psychosom. 2001;2(1):12–15. doi:10.1159/000049631
2. Tzur Bitan D, Berzin D, Kridin K, Cohen A. The association between alopecia areata and anxiety, depression, schizophrenia, and bipolar disorder: a population-based study. Arch Dermatol Res. 2022;314(5):463–468. doi:10.1007/s00403-021-02247-6
3. Karia SB, De Sousa A, Shah N, Sonavane S, Bharati A. Psychiatric morbidity and quality of life in skin diseases: a comparison of alopecia areata and psoriasis. Ind Psychiatry J. 2015;24(2):125–128. doi:10.4103/0972-6748.181724
4. Macbeth AE, Holmes S, Harries M, et al. The associated burden of mental health conditions in alopecia areata: a population-based study in UK primary care. Br J Dermatol. 2022;187(1):73–81. doi:10.1111/bjd.21055
5. van Dalen M, Muller Kirsten S, Kasperkovitz-Oosterloo Johanna M, Okkerse Jolanda ME, Pasmans Suzanne GMA. Anxiety, depression, and quality of life in children and adults with alopecia areata: a systematic review and meta-analysis. Front Med. 2022;9:1–24. doi:10.3389/fmed.2022.1054898
6. Ruiz-Doblado S, Carrizosa A, García-Hernández MJ. Alopecia areata: psychiatric comorbidity and adjustment to illness. Int J Dermatol. 2003;42(6):434–437. doi:10.1046/j.1365-4362.2003.01340.x
7. Mirza MA, Jung SJ, Sun W, Qureshi AA, Cho E. Association of depression and alopecia areata in women: a prospective study. J Dermatol. 2021;48(8):1296–1298. doi:10.1111/1346-8138.15931
8. Sorour F, Abdelmoaty A, Bahary MH, El Birqdar B. Psychiatric disorders associated with some chronic dermatologic diseases among a group of Egyptian dermatology outpatient clinic attendants. J Egypt Women Dermatol Soc. 2017;14(1):31–36. doi:10.1097/01.EWX.0000503397.22746.bd
9. Kim JC, Lee ES, Choi JW. Impact of alopecia areata on psychiatric disorders: a retrospective cohort study. J Am Acad Dermatol. 2020;82(2):484–486. doi:10.1016/j.jaad.2019.06.1304
10. Erdoğan SS, Gür TF, Doğan B. Anxiety and depression in pediatric patients with vitiligo and alopecia areata and their parents: a cross-sectional controlled study. J Cosmet Dermatol. 2021;20(7):2232–2239. doi:10.1111/jocd.13807
11. Colón EA, Popkin MK, Callies AL, Dessert NJ, Hordinsky MK. Lifetime prevalence of psychiatric disorders in patients with alopecia areata. Compr Psychiatry. 1991;32(3):245–251. doi:10.1016/0010-440X(91)90045-E
12. Conic RZ, Miller R, Piliang M, Bergfeld W, AtanaskovaMesinkovska N. Comorbidities in patients with alopecia areata. J Am Acad Dermatol. 2017;76(4):755–757. doi:10.1016/j.jaad.2016.12.007
13. Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive Therapy for Depression. New York: Guilford; 1979.
14. Hisli N. Validity and reliability of Beck depression inventory in university students. J Psychol. 1989;7:3–13.
15. Ulusoy M, Sahin NH, Erkmen H. Turkish version of the Beck Anxiety Inventory: psychometric properties. J Cog Psychother. 1998;12(2):163.
16. Fricke A, Miteva M. Epidemiology and burden of alopecia areata: a systematic review. Clin Cosmet Investig Dermatol. 2015;8:397–403. doi:10.2147/CCID.S53985
17. Aghaei S, Saki N, Daneshmand KB. Prevalence of psychological disorders in patients with alopecia areata in comparison with normal subjects. Int Schol Res Not. 2014;2014:1–4.
18. Sellami R, Masmoudi J, Ouali U, et al. The relationship between alopecia areata and alexithymia, anxiety and depression: a case-control study. Indian J Dermatol. 2014;59(4):421. doi:10.4103/0019-5154.135525
19. Chu SY, Chen YJ, Tseng WC, et al. Psychiatric comorbidities in patients with alopecia areata in Taiwan: a case-control study. Br J Dermatol. 2012;166(3):525–531. doi:10.1111/j.1365-2133.2011.10714.x
20. Senna M, Ko J, Tosti A, et al. Alopecia areata treatment patterns, healthcare resource utilization, and comorbidities in the Us population using insurance claims. Adv Ther. 2021;38(9):4646–4658. doi:10.1007/s12325-021-01845-0
21. Tekindal M, Tekindal MA. Validity and reliability of basic depression scale for Turkey. Med J West Black Sea. 2021;5(3):452–463.
22. Sánchez-Díaz M, Montero-Vílchez T, Cuenca-Barrales C, Molina-Leyva A, Arias-Santiago S. Prevalence and implications of type D personality in patients with alopecia areata: a marker of quality-of-life impairment and mood status disturbances, a comparative study. J Eur Acad Dermatol Venereol. 2023;37(5):1064–1070. doi:10.1111/jdv.18733
23. Okhovat JP, Marks DH, Manatis-Lornell A, Hagigeorges D, Locascio JJ, Senna MM. Association between alopecia areata, anxiety, and depression: a systematic review and meta-analysis. J Am Acad Dermatol. 2023;88(5):1040–1050. doi:10.1016/j.jaad.2019.05.086
24. CordanYazici A, Basterzi A, Tot Acar S, et al. Alopecia areata and alexithymia. Turk Psikiyatri Derg. 2006;17(2):101–106.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.