")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Anxiety and Depression Among Dentists in the Kingdom of Saudi Arabia
Authors Mohamed Asif S, Ibrahim Assiri K, Mohammed Al Muburak H, Hamid Baig FA, Abdullah Arem S, Arora S, Mohammed Shamsudeen S, Shariff M, Shamsuddin S, Mohammed Lahiq AA
Received 28 November 2021
Accepted for publication 23 February 2022
Published 16 March 2022 Volume 2022:15 Pages 497—507
DOI https://doi.org/10.2147/RMHP.S350277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Shaik Mohamed Asif,1 Khalil Ibrahim Assiri,1 Hussain Mohammed Al Muburak,1 Fawaz Abdul Hamid Baig,2 Saeed Abdullah Arem,1 Suraj Arora,3 Shaik Mohammed Shamsudeen,1 Mansoor Shariff,4 Shaheen Shamsuddin,5 Anas Abdullah Mohammed Lahiq4
1Department of Diagnostic Science and Oral Biology, College of Dentistry, King Khalid University, Abha, Kingdom of Saudi Arabia; 2Department of Oral and Maxillofacial Surgery, College of Dentistry, King Khalid University, Abha, Kingdom of Saudi Arabia; 3Department of Restorative Dental Sciences, College of Dentistry, King Khalid University, Abha, Kingdom of Saudi Arabia; 4Department of Prosthetic Dentistry, College of Dentistry, King Khalid University, Abha, Kingdom of Saudi Arabia; 5Department of Orthodontics, College of Dentistry, King Khalid University, Abha, Kingdom of Saudi Arabia
Correspondence: Shaik Mohamed Asif, Department of Diagnostic Science and Oral Biology, College of Dentistry, King Khalid University, Abha, 61421, Kingdom of Saudi Arabia, Tel +966 557361821, Email [email protected]
Purpose: Dentists face a great deal of professional stress, in dental school and in practice. Their personal, as well as professional lives, get affected negatively by stress and poor mental health. This study aims to evaluate anxiety and depression among dentists of Abha in kingdom of Saudi Arabia.
Materials and Methods: A cross-sectional study was carried out among 246 registered dentists of Abha to assess anxiety and depression. Participants willing to participate, and completely filled questionnaire were included in study. Data regarding demography, work-related characters, lifestyle and self-reported physical and mental status were collected. Mental status was measured by using pre validated questionnaire Zung Self-Rating Anxiety Scale (SAS) and the Zung Self-Rating Depression Scale (SDS). Data were analyzed using Statistical Package for Social Sciences (SPSS 20) by IBM. Descriptive statistics, Pearson correlation, independent t test and one way ANOVA were used to analyze the data at the significant interval of p≤ 0.05.
Results: Different levels of anxiety and depression were noticed both in males and female dentist. There was no statistical difference in the mean scores between males and females. There was a statistical difference of anxiety and depression scores noticed among dentist working in government institution, with five to ten years of experience. Habits of smoking were shown to significantly affect the risk of anxiety and depression scores.
Conclusion: Dentist due to nature of the practice are prone for anxiety and clinical depression. Stress coping methods should be included in dental curriculum which would indirectly improve professional abilities and personal life.
Keywords: anxiety, dentists, depression
Introduction
Dentist, during initial stages of their practice experience difficulties for which they might not be aware off. It is because, their inference are not “down to earth” as they tend to expect more or less like a fairy tale which may end up in frustration leading to discomfort and emotional diversion.1 These kind of habits might cause burnout which might lead to never ending anxiety and depression.2 These stress related disorders are at ever increasing rate in today’s world with its impeding psychosocial toll on dentist’s health. Source of anxiety and depression might be from work place, due to financial issues or due to improper patient management.3 Their personal and professional life as well as their health might be negatively affected. These conditions are chronic, relentless and can worsen if not treated. It has been demonstrated that anxiety and depression can affect patient care and might lead to increase in treatment errors. According to World Health Organization, incidence rate of anxiety and depression has increased by more than 18% between 2005 and 2015.4 Hence, demand to curb on mental health condition globally is on rise. Most of them suffering from these diseases never discuss about their problem as there is shame and disgrace attached. Many studies have reported that anxiety and depression are encountered regularly among dentist.5 However, there is scarcity of data in Saudi Arabia and worst still in Abha the southern region of Saudi Arabia. Therefore, this study was conducted to evaluate the level of anxiety and depression among dentists of Abha, Saudi Arabia.
Materials and Methods
A questionnaire based cross-sectional study was conducted among 246 registered dentists practicing in Abha city of Aseer Province Saudi Arabia, during academic year May 2019– January 2020. Ethical clearance was obtained from the Institutional Review Board of College of Dentistry, King Khalid University (duly approved by Institutional and Research committee SRC/EH/2019-20/46). All participants provided written informed consent prior to study after making them understand intention of the study and their confidentiality of data was maintained. Two co-authors approached and distributed questionnaire to each dentist at their clinics and explained the study design and purpose of the study. They were instructed to complete questionnaire within one week and were reminded once before the stipulated time. All registered dentists of Abha city were included in the study.
Inclusion Criteria
Participants willing to participate, and completely filled questionnaire were included in study.
Exclusion Criteria
Dentists who were not willing to participate and incompletely filled questionnaire were excluded from the study.
Validity and Reliability of Questionnaire
Reliability of questionnaire were assessed by using test re test. Cronbach’s-Alpha was used to ascertain internal consistency of the questionnaire. SAS had internal consistency with alpha coefficient of 0.82 and SDS with fair internal consistency with alpha coefficient of 0.68.
Distribution of SAS & SDS Questionnaire
Questionnaire were split into four sections, first being socio demographic data of the participant, second life style component, third being the work-related characters and self-reported health status was the fourth component. In self-reported health physical health was assessed by using Likert scale varying from “very bad” to “very good”. Mental health status was assessed by using norm-referenced Zung Self Anxiety Scale (SAS) and Self Rating Depression Scale (SDS) scales.6,7 SDS taps psychological and physiological symptoms, SAS taps affective and somatic symptoms selected from the Diagnostic criteria listed in the major American psychiatry literature.8,9 SDS & SAS have twenty item Likert scale with multiple choice answers. The raw score ranges from 20 to 80, where score of 20 is normal followed by 80 which are extremely anxiety and depressed levels. These scores are later converted to index score by dividing sum of raw score by 80 and multiplying by 100. Index score of 45 (raw score=36) was kept as a cut off point for clinically significant anxiety. 50 was the index cut off score for SDS that equated raw score of 40 as recommended by Zung. The acquired data were tabulated and cross checked by two co-authors.
Statistical Analysis
Data processing and analysis were carried out using the statistical package for social science (SPSS) software #20 by IBM. Descriptive statistics, Pearson correlation, independent t test and one-way ANOVA were used to analyze the data at the significant interval of p≤0.05.
Results
This exploratory cross-sectional questionnaire-based study was conducted among 246 dental practitioners, among which only one dentist did not complete the questionnaire generating response rate to 99.5%. Study group comprised of 138 (56.33%) males and 107 (43.67%) females of which 73.88% of them are married. 63.67% of dentists are specialist (Master’s/Saudi Board Certified). Among 245 dentist 161 (65.71%) are working in government hospitals. Most of them have 5 to 10 years of clinical experience (44.49%).58.37% of them reported of conflict and violence sometimes during their clinical practice. 48.16% of dentist reported their physical health status as fair and 42.45% of them reported as good. Among 138 male dentist 71.74% of them had marked to severe levels of anxiety and 69.5% of them were moderately depressed which was statistically significant. 84.11% of female dentist had marked to severe levels of anxiety and 67.29% of them were moderately depressed (Tables 1 and Tables 1).76.2% of specialist had marked to severe levels of anxiety and 68.59% of them were moderately depressed (p<0.01). 80.75% of dentist working in government hospitals showed marked to severe level of anxiety and 72.05% of them were moderately depressed. Dentist with five to ten years of clinical experience had marked to severe levels of anxiety (91.74%) and 67.89% were moderately depressed which was statistically significant. There was no significant relation between levels of anxiety and depression with working hours, sleeping time and exercise (Tables 1 and Tables 1). Table 3 shows prevalence of different levels of anxiety and depression among dentist where, 77.14% of them were having symptoms of marked to severe anxiety and 68.57% of them were moderately depressed. Pearson coefficient method was used to assess the correlation between anxiety and depression which was statistically significant. One way ANOVA & independent t test were used to compare socio demographic characters, life style, self-perceived physical health with respect to mean anxiety and depression scores (Tables 4 and Tables 5). The mean (SD) of anxiety in males was 49.93±12.91 which was not significant. However, the mean (SD) of depression was 58.43±9.20 which was statistically significant. The mean anxiety scores 49.68±12.37 in married dentist was not statistically significant. However, there was significant difference in mean depression 54.76±10.50 scores of married dentist There was a significant difference between mean anxiety and depression scores with relation to work related characters and self-perceived physical health status. There was no significant difference between mean anxiety and depression scores with relation to working hours and sleeping time (Tables 4 and Tables 5).
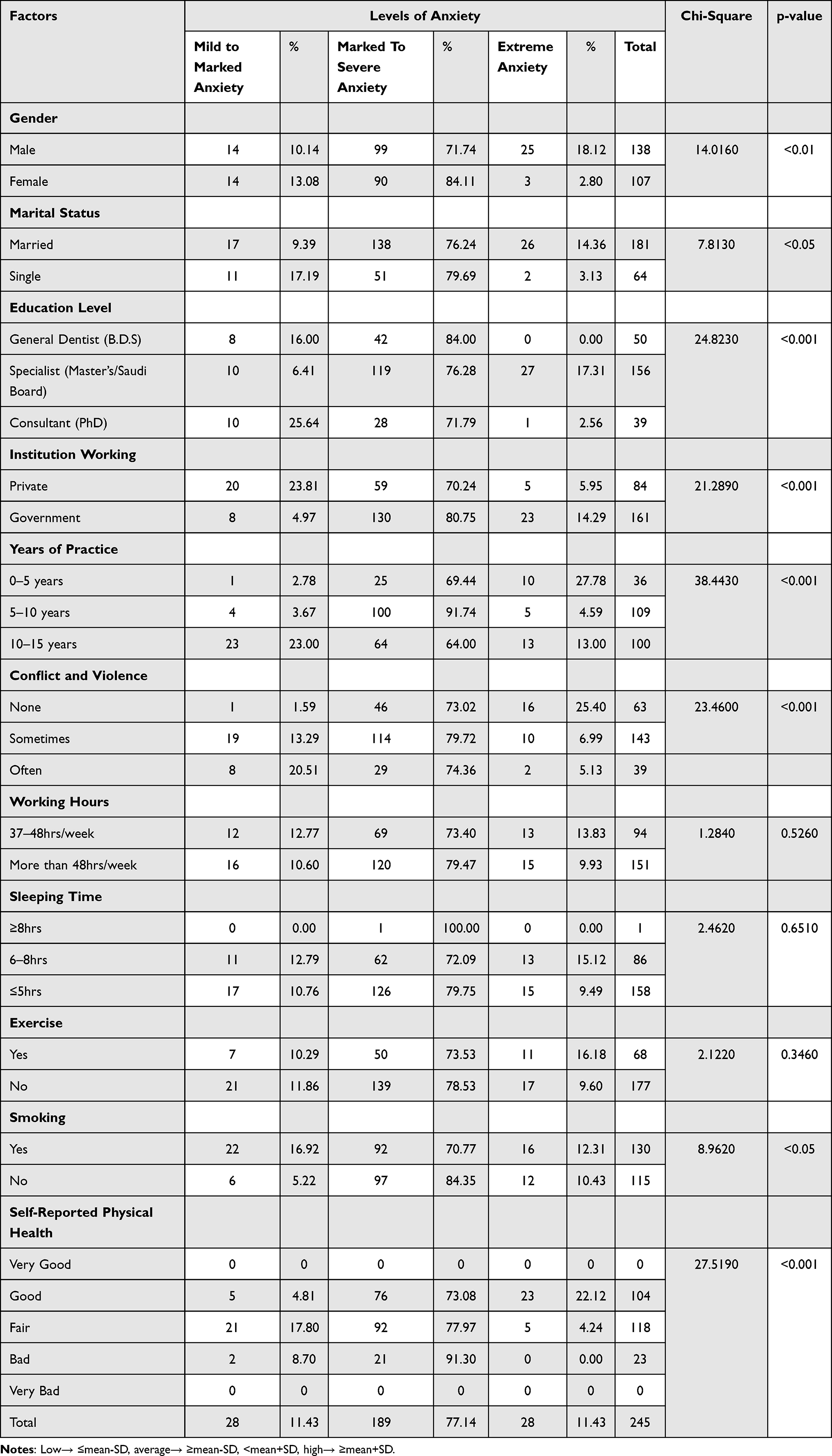 |
Table 1 Association Between Levels of Anxiety with Socio Demographic Characteristics, Work-Related Characteristics, Lifestyles and Self-Perceived Physical Health Status |
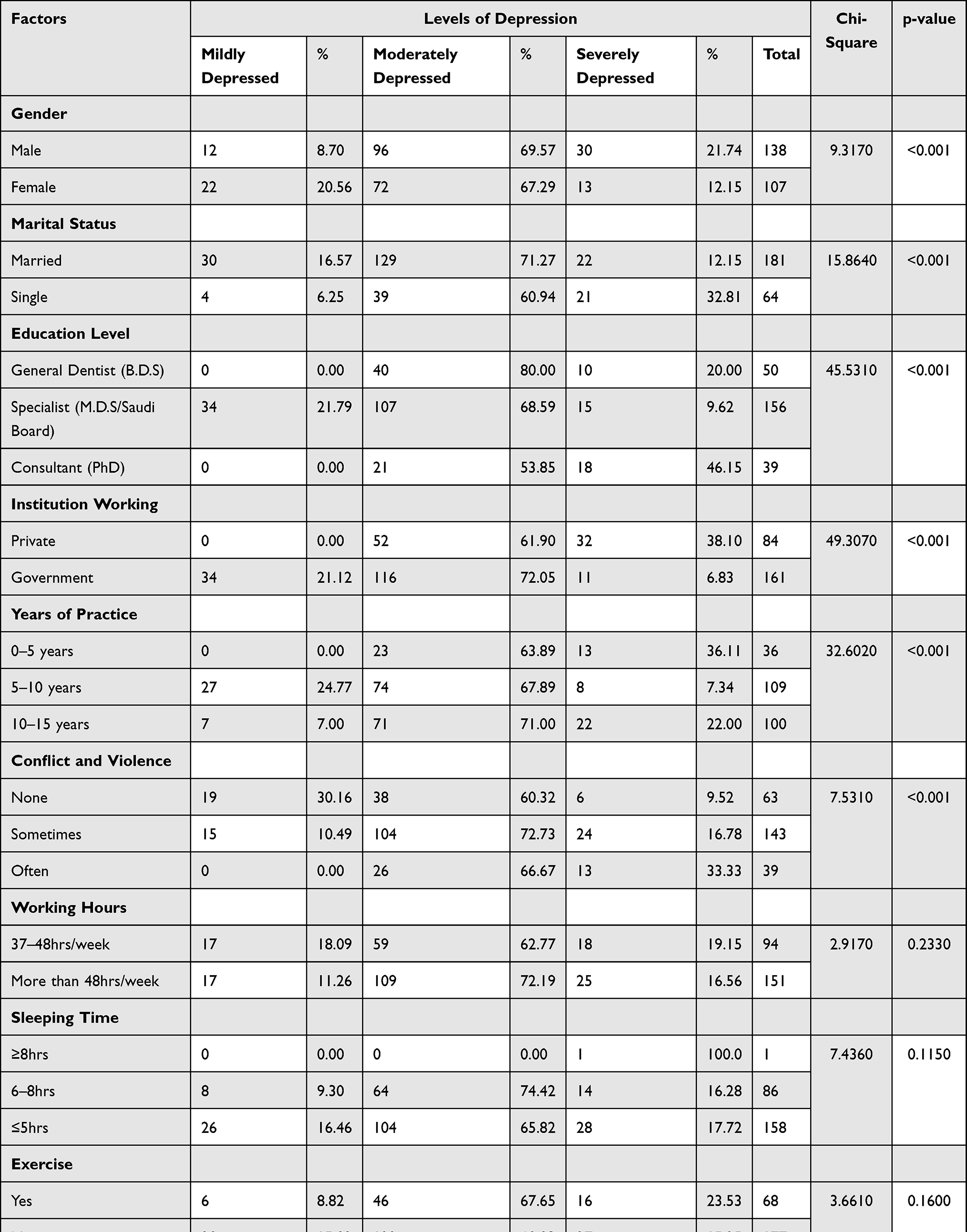 |
Table 2 Association Between Levels of Depression with Socio Demographic Characteristics, Work-Related Characteristics, Lifestyles and Self-Perceived Physical Health Status |
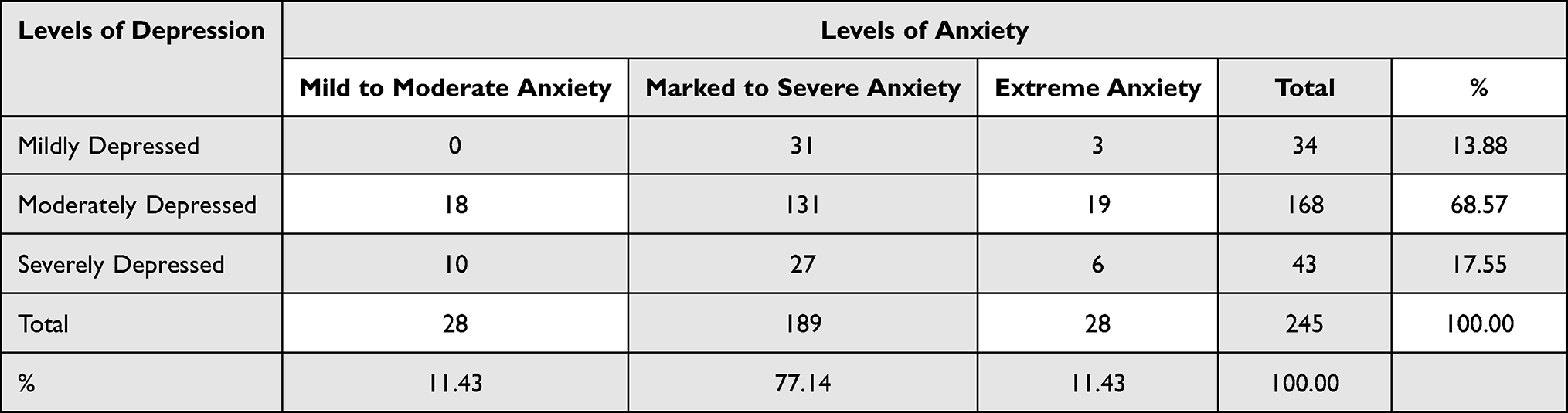 |
Table 3 Association Between Levels of Anxiety and Depression |
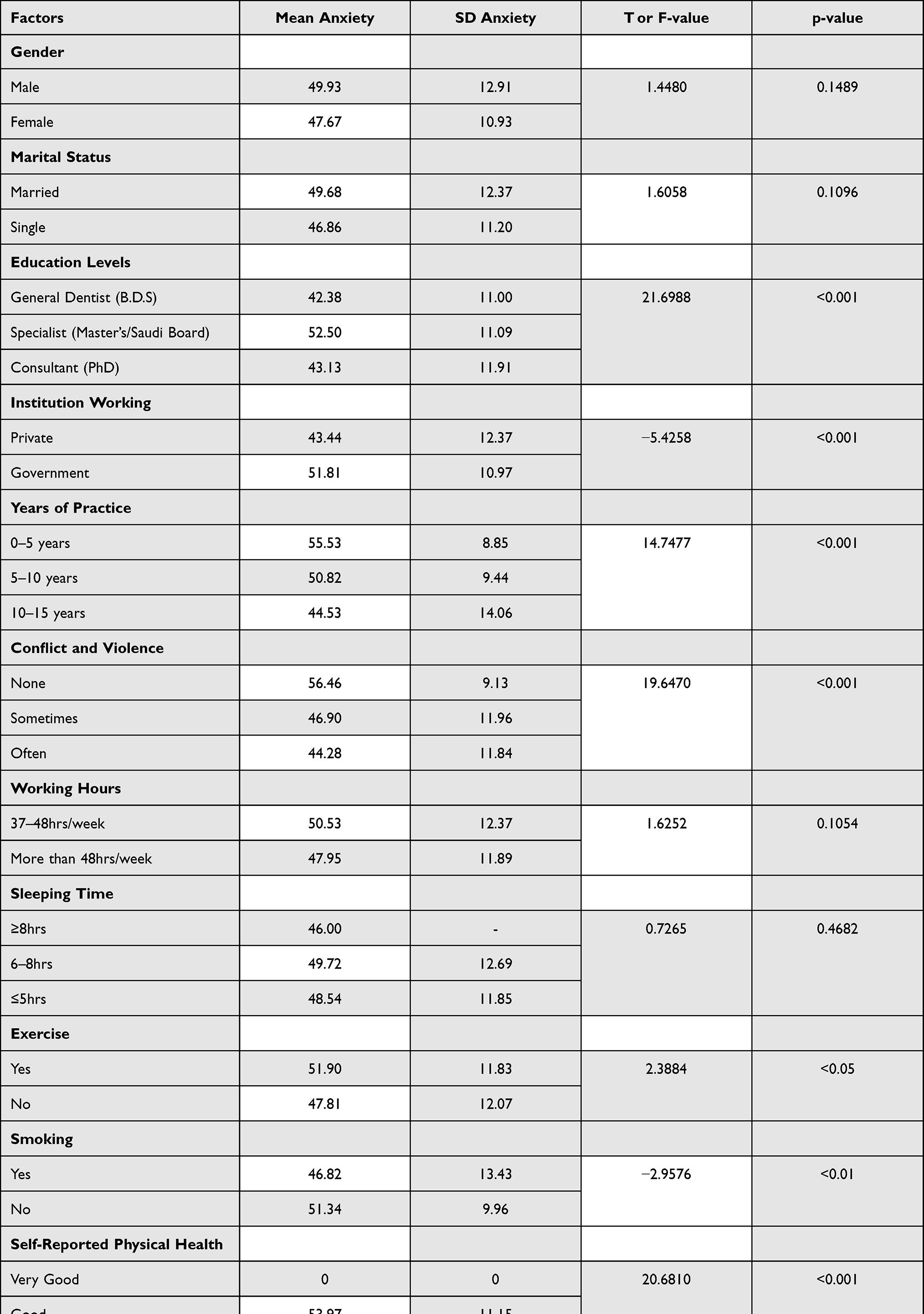 |
Table 4 Comparison of Socio Demographic Characteristics, Work-Related Characteristics, Lifestyles and Self-Perceived Physical Health Status with Respect to Mean Anxiety Scores by Independent t Test and One Way ANOVA Test |
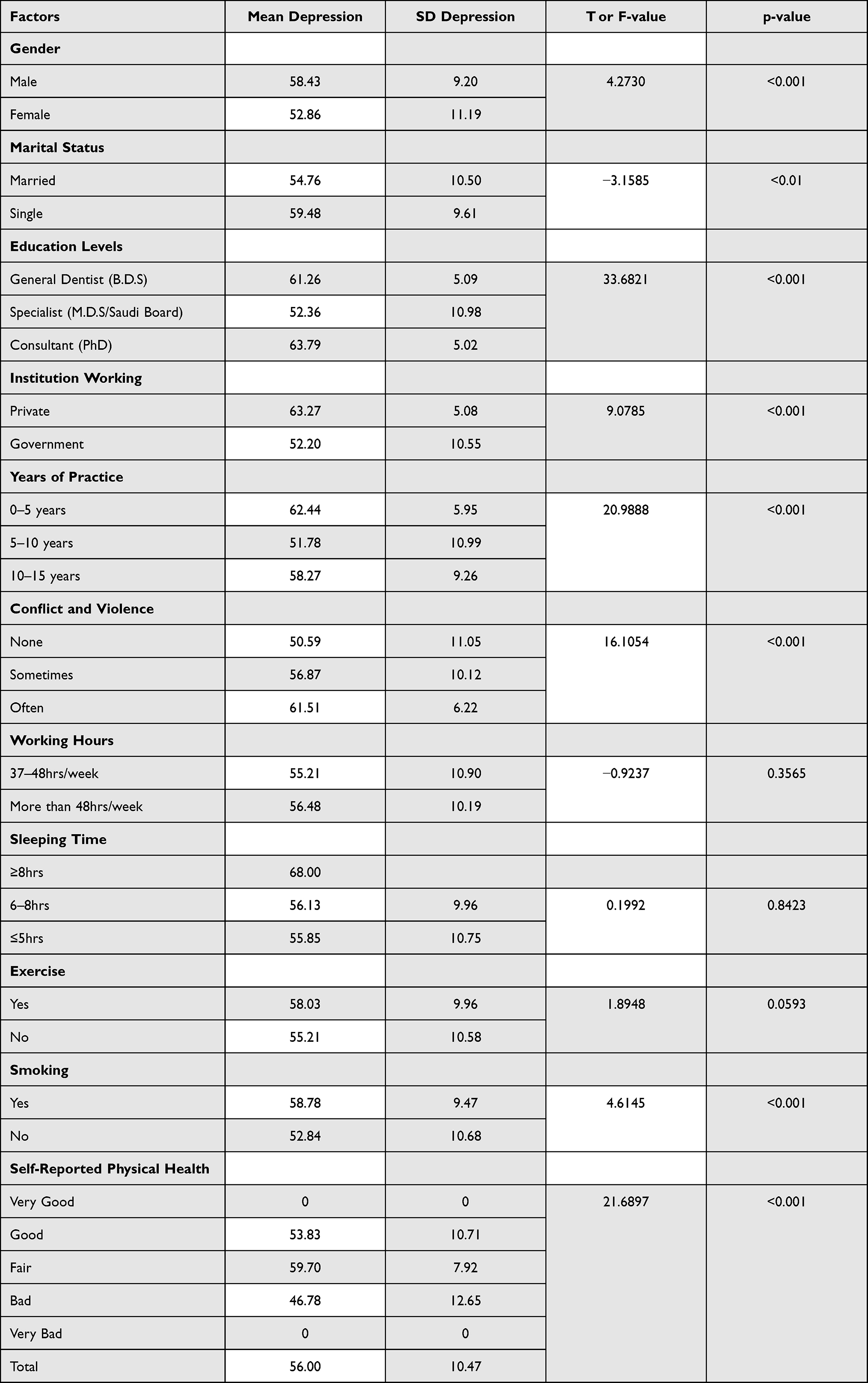 |
Table 5 Comparison of Socio Demographic Characteristics, Work-Related Characteristics, Lifestyles and Self-Perceived Physical Health Status with Respect to Mean Depression Scores by Independent t Test and One Way ANOVA Test |
Discussion
Cognizance of stress is under control of an individual attitude, belief and cultural background. One of the predisposing factor for stress in an individual is due to discrepancy between different types of demands and capacity of an individual to accomplish. Stress may motivate a person to attain exceptionally high performance or can lead to anxiety, depression, unprofessional conduct and burn out. Anxiety and depression are the most prevalent of mental illness contributing to the global disability burden.10 Clinicians and research often screen anxiety and depression by using self-reported psycho motor tools which are of criterion-referenced and norm- referenced measures. Criterion-referenced measures are diagnosed based on the endorsement of published diagnostic classification system. In contrast norm-referenced measures compares individuals test results to those of normative group.11 These scales typically suggest score ranges linked to symptom severity descriptors, and have a “clinically significant” total score cut off point beyond which scores are considered indicative of presence of disorder. Zung’s SAS & SDS are two such norm-referenced scales with sensitivity of 89% and 93% and specificity of 69% respectively.12 In recent year’s dentists physical and mental health has been a focus of interest worldwide. They are under stress due to multiple factors like work overload, job dissatisfaction, security issues and financial problems.13 To the best of our knowledge this is the first study which assessed the level of anxiety and depression among dentists of Abha. Among 138 Male dentist in our study 71.74% of them had marked to sever anxiety symptoms and 69.5% of them were moderately depressed. 84.11% of female dentist had marked to sever anxiety symptoms and 67.29% of them were moderately depressed. 76.24% of married dentist had marked to severe anxiety symptoms and 71.27% of them were moderately depressed. These findings are not in accordance with study conducted by Mathias et al where married dental professionals exhibit less anxiety and depression.14 Dentist working in government hospitals had marked to sever anxiety levels and were moderately depressed when compared to dentist working in private sector. When enquired regarding the reason, it was noticed that most of the dentist working in government sector are expatriates (non-Saudi’s), who work on yearly contract basis. They were not sure about their next contract renewal which was influencing on their future social and financial wellbeing. However, dentist working in private sector their contract renewal was either for three years or five years which was not hampering on their social and financial securities. Dentist with more than five years of clinical experience had marked to sever anxiety levels and were moderately depressed. It could be due to the rules implemented by Saudi government to replace the old existing non-Saudi staff with their national citizens, as number of non-Saudi’s working in health sector are more compared to Saudi’s. Specialist were more depressed and had marked to severe anxiety levels when compared to general practitioners and consultant. This could be due to the fact that, most patients and complicated cases in the dental hospitals are referred to specialist rather than to a general dentist which caused an overload of patients and compromise in time management for specialist. Consultants in Abha are very few and due to exuberant consultant charges and patient affordability, patients prefer to go to a specialist rather than going to a consultant. Our study revealed that there was no significant correlation between levels of anxiety and depression in relation to number of working hours, sleeping time and physical exercise. However, there was significant correlation between levels of anxiety and depression in relation to that of smoking and self-reported physical health. These findings are in accordance with the study conducted by Prasad,15 from India and Gong,16 from china where their study revealed significant association between, smoking habits, self-reported physical health to that of anxiety and depression. It is a well-known fact that physical exercise keeps a person more energetic and efficient. It also develops a self-esteem, self-control and self-discipline in a person. Different levels of anxiety and depression were not mong dentist of our study. However, majority of them were having marked to severe anxiety symptoms, and they were moderately depressed. Similar findings have been previously reported by Madhan et al among post graduate students.17 High expectations from the ground reality are the real stress inducing situations which causes anxiety and depression.18,19 Hence, there is a requirement of reassessment of one’s own perspective and belief in light that can be achieved in reality or not.
Limitation
Results of our present study cannot be generalized as it was conducted in Abha the capital city of Aseer. Moreover, there are chances of respondent’s bias as it was a questionnaire-based study which is easy to manipulate if the respondents are not willing to give an authenticated response or may have difficulty in recollecting required information.
Future Implications
In future longitudinal studies in different regions of Aseer should be conducted to gain substantial results. Research should also be done to identify the sources and reasons of anxiety and test its impact longitudinally among dental practitioners.
Conclusion
Dentists are prone for anxiety disorders and clinical depression owing to the nature of clinical practice and due to high expectations from the same. In future, stress coping methods should be included in the dental curriculum to manage this kind of disorders which indirectly improves the professional abilities and personal life.
Data Sharing Statement
Supporting data are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Our study complies with declaration of Helsinki. Ethical clearance was obtained from the Institutional Review Board of College of Dentistry, King Khalid University (duly approved by Institutional and Research committee SRC/EH/2019-20/46). All participants provided written informed consent prior to study after making them understand intention of the study and their confidentiality of data was maintained.
Acknowledgment
The research was funded by the Deanship of Scientific Research at King Khalid university through the small Research Group project under grant number (RGP.1/336/42).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Gorter RC, Eijkman MA. Career expectations and the type of dentist in the light of burnout. Ned Tijdschr Tandheelkd. 2002;109:212–216.
2. Kumar S, Dagli RJ, Mathur A. Perceived sources of stress amongst Indian dental students. Eur J Dent Educ. 2009;13(1):39–45. doi:10.1111/j.1600-0579.2008.00535.x
3. Alzahem AM, van der Molen HT, Alaujan AH. Stress amongst dental students: a systematic review. Eur J Dent Educ. 2011;15(1):8–18. doi:10.1111/j.1600-0579.2010.00640.x
4. World Health Organization. Mental health [Internet]. WHO. [Cited March 23, 2017]. Available from: http://www.who.int/mental_health/en/.
5. Badran DH, Al-Ali MH, Duaibis RB, et al. Burnout among clinical dental students at Jordanian universities. East Mediterr Health J. 2010;16(4):434–437. doi:10.26719/2010.16.4.434
6. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
7. Zung WW. A rating instrument for anxiety disorders. Psychosom. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
8. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
9. Tanaka-Matsumi J, Kameoka VA. Reliabilities and concurrent validities of popular self-report measures of depression, anxiety, and social desirability. Consult Clin Psychol. 1986;54:328. doi:10.1037/0022-006X.54.3.328
10. Andrews G, Henderson S, Hall W. Prevalence, comorbidity, disability and service utilisation overview of the Australian National Mental Health Survey. Br J Psychiatry. 2001;178:145–153. doi:10.1192/bjp.178.2.145
11. Kupfer DJ. Dimensional models for research and diagnosis: a current dilemma. J Abnorm Psychol. 2005;114:557–559. doi:10.1037/0021-843X.114.4.557
12. Dunstain DA, Scott N, Todd A. Screening for anxiety and depression: reassessing the utility of Zung Scales. BMC Psychiatry. 2017;17(329):1–8. doi:10.1186/s12888-016-1163-4
13. Wallace JE. Mental health and stigma in the medical profession. Health. 2012;16(1):03–18. doi:10.1177/1363459310371080
14. Mathias S, Koerber A, Fadavi S, et al. Specialty and sex as predictors for depression in dentists. J Am Dent Assoc. 2005;136(10):1388–11395. doi:10.14219/jada.archive.2005.0052
15. Prasad M, Rajpatthi B, Singla A, et al. Assessment of anxiety and depression among dental practitioners- an exploratory cross-sectional study. J Clin Diagn Res. 2017;11(10):ZC01–ZC04.
16. Gong Y, Han T, Chen W, et al. Prevalence of anxiety and depressive symptoms and related risk factors among physicians in China: a cross-sectional study. PLoS One. 2014;9(7):e103242. doi:10.1371/journal.pone.0103242
17. Madhan B, Rajpurohit A, Gayathri H. Mental health of post graduate orthodontic students in India: a multi institution survey. J Dent Educ. 2012;76(2):200–209. doi:10.1002/j.0022-0337.2012.76.2.tb05247.x
18. Kulkarni S, Dagli N, Duraiswamy P, et al. Stress and professional burnout among newly graduated dentists. J Int Soc Prev Community Dent. 2016;6:535–541. doi:10.4103/2231-0762.195509
19. Alharbi R, Alsuhaibani K, Almarshad A, et al. Depression and anxiety among high school students at Qassim Region. J Fam Med Prim Care. 2019;8:504–510. doi:10.4103/jfmpc.jfmpc_383_18
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.