Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Antiretroviral Treatment Adherence Level and Associated Factors Among Adult HIV-Positive Patients on Both HIV/AIDS Care Models: Comparative Study in Selected Hospitals of Western Ethiopia, 2019
Authors Dibaba D ![]() , Kajela G
, Kajela G ![]() , Chego M
, Chego M ![]() , Ermeko T, Zenbaba D, Hailu S, Kasim J
, Ermeko T, Zenbaba D, Hailu S, Kasim J ![]() , Abdulkadir A
, Abdulkadir A ![]()
Received 4 July 2021
Accepted for publication 13 November 2021
Published 15 December 2021 Volume 2021:13 Pages 1067—1078
DOI https://doi.org/10.2147/HIV.S327784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Diriba Dibaba,1 Gemechu Kajela,2 Melese Chego,2 Tilahun Ermeko,1 Demisu Zenbaba,1 Sintayehu Hailu,1 Jeylan Kasim,1 Adem Abdulkadir1
1Public Health Department, MaddaWalabu University Goba Referral Hospital, Goba, Oromia, Ethiopia; 2Department of Public Health, Institute of Health Sciences, Wollega University, Nekemte, Oromia, Ethiopia
Correspondence: Adem Abdulkadir Email [email protected]
Background: Many studies investigating antiretroviral treatment (ART) adherence found the majority of patients had suboptimal adherence for a variety of different reasons. The study aimed to compare the ART adherence level and associated factors among adult human immune deficiency virus (HIV) positive patients on both care models in selected hospitals.
Methods: An institution-based comparative cross-sectional study was conducted among 463 HIV positive patients on ART. The study samples were selected using systematic random sampling, and pretested semi-structured interviewer administered questionnaire was used to collect data. Binary and multivariable logistic regression analyses were used to see the association between outcome and predictors using odds ratio with a 95% confidence interval to estimate the strength of the association.
Results: The study had a response rate of 445 (96.1%). Of the study participants, 325 (73%) and 120 (27%) were from the routine and appointment spacing models, respectively. Patients on the appointment spacing model had higher levels of optimum adherence (87.5% vs 74.27%, respectively; p = 0.006). Patients’ satisfaction with health service delivery (OR = 0.31, 95%: CI 0.11– 0.84), antiretroviral drug dosage taken per day (OR = 3, 95%: CI 1.16– 8.1), disclosure of HIV status (OR = 0.30, 95%: CI 0.09– 0.93), distance from patient residency to health facility (OR = 0.11, 95%: CI 0.03– 0.34), the memory aids used (OR = 0.02, 95%: CI 0.01– 0.05), and type of HIV/AIDS care model (OR= 0.24, 95%: CI 0.1– 0.6) were factors significantly associated with ART adherence level.
Conclusion: ART patients on the appointment spacing model had higher optimum ART adherence levels than those on the routine schedule due to factors like satisfaction status, disclosure status, type of memory aid used, type of ART care model used, and distance from the care facility. Therefore, promoting adherence enablers and alleviating barriers of ART adherence will improve ART adherence levels.
Keywords: ART adherence level, routine schedules, appointment spacing model
Introduction
Adherence to ART can be defined as the extent to which patients use their medications according to medical recommendations.1 The human immunodeficiency virus (HIV) is a major global health concern, including in Ethiopia. By the end of 2018, approximately 37.9 million people were living with HIV globally, with Sub-Saharan Africa accounting for nearly two-thirds of cases.2 In “World Health Statistics 2017,” the World Health Organization (WHO) reported that around 722,248 adult Ethiopians were living with HIV/AIDS, an increase of 3748 infections from the previous year.3 A high adherence level is a prerequisite for maintaining viral suppression and lowering the risk of drug resistance, which in turn prevents premature morbidity and mortality.4 Several studies worldwide indicated that ART adherence represented a major challenge in the treatment of HIV-positive patients.
According to a meta-analysis of studies conducted in Sub-Saharan Africa, 77% of people taking antiretroviral medications adhered to their ARV regimens,6 which is below the required optimum ART adherence level. Another systematic review and meta-analysis done in Latin America and the Caribbean in 2018 indicated that an overall adherence level of 70% among study participants.7 A study implemented in Botswana, Tanzania, and Uganda reported the average rates of non-adherence to ART ranged from 50% to 70%.8 A study presented at the 22nd International Conference on AIDS in Amsterdam, the Netherlands in 2018, of 59% of people on ART treatment, only 47% of patients had viral suppression.9 One study examining ART data from a variety of countries found that ART programs worldwide face substantial challenges in keeping patients on ART and achieving viral suppression.10 In Ethiopia, the majority of the studies reported that ART adherence levels were suboptimal. One study reported adherence rates of 83% for two hospitals in the Oromia Region,11 88.3% at Yirgalem Hospital in Addis Ababa, Ethiopia, and 81.2% at three hospitals in Addis Ababa.12 However, ART adherence levels less than 95% have been linked to poor suppression of HIV viral load and a decrease in cluster of differentiation of cell four (CD4) count, leading to disease progression and the development of drug resistance.13
According to comparative cross-sectional survey conducted in Yirgalem hospital in South Ethiopia and in eastern Ethiopia on adult HIV-positive ART patients, factors for non-adherence include age, monthly income, presence of opportunistic infections, forgetfulness, side effects of ART drugs, alcohol and drug abuse, poor social support, inadequate health provider-patient relationships, being away from home, fear of disclosure, educational level, and others.12,15,16 A cross-sectional study on adult HIV positives in Zimbabwe in 2016 showed that distance from the health institution, medication side effects, and adolescence were associated with non-adherence.14
Another strategy used globally and in our country to reduce suboptimal adherence to ART treatment is the implementation of differentiated HIV/AIDS care, such as the appointment spacing model (ASM).17 Even though ART adherence levels were known for both HIV/AIDS care models during patient’s enrollment, there was little evidence of ART adherence levels assessed after the ART patients enrolled in this model using the scientific research survey.17 Therefore, the study determined and compared adherence levels among ART patients on the routine and ASM models and relates them to associated factors to intervene as early as possible and scale up the ASM program effectively and efficiently.
Methods and Materials
Area of Study, Time Period, Design, and Study Population
An institutional-based comparative cross-sectional study was conducted from April 21 to May 21 at selected western hospitals in Ethiopia. The West Wollega zone is one of 18 zones of the Oromia regional state with an estimated total population of 1,872,601 according to the population projections of the 2007 census.18 Gimbi is its capital town, which lies 440 km west of Addis Ababa. These zones have 25 ART sites of which six are hospitals while the others are health centers. Around 3491 people were living with HIV positive on ART, of which 1057 were people living with HIV who were currently enrolled on the ASM model. These six hospitals hold approximately 65% of the total number of people living with HIV in the zone (West Wollega Zonal Health Office, Oromia, Western Ethiopia; HIV/AIDS control and prevention internal report; 2019 [unpublished report by email communication]).
All HIV positive patients on the ART treatment program at West Wollega zone health facilities were source populations, and all HIV positive patients above 18 years old and on the first-line ART program at selected West Wollega zone hospitals and fulfilling inclusion criteria were the study population. But seriously ill patients who could not respond to our questions were excluded from the study.
Sample Size and Sampling Techniques
A double population proportion formula was used to calculate the required sample size manually; considering 50% of ART patients on the ASM model might have an optimum ART adherence level (by assumption) and 74% of ART patients on the routine schedule had optimal ART adherence,19 with a 95% confidence level, power of 80%, design effect of two, and with a ratio of one to three (1:3) ART patients on ASM to routine schedule respectively. A 10% non-response rate was added. Accordingly, a manually calculated total sample size yields 534 study participants from both models.
But since the total source populations were below ten thousand (3491 HIV/AIDS positive patients), a sample size correction formula was used, which brought a total sample size of 463 study participants.
Multistage sampling techniques were used to select the study population and setting. First hospitals providing ART service in the Wollega zone were stratified into governmental and non-governmental hospitals. Accordingly, there were four governmental and two non-governmental hospitals. Two hospitals from the government and one from the non-government were chosen using simple random sampling (SRS). After three hospitals were selected; the required total sample size was proportionally allocated to selected hospitals based on total ART patients found. At selected hospitals, the two strata sample frame list was prepared based on the types of ART treatment care model for eligible ART patients. Then, using patients’ unique ART numbers, the study unit was selected by systematic sampling method from a predetermined sample frame list.
Measurement
In this study, an ART patient on a routine HIV/AIDS care schedule is a patient who follows their appointment schedule according to previous (1–2 month) intervals for follow up. This type of appointment schedule was used for unstable ART patients, while the ART patient on the appointment spacing model is a patient who practices their appointment schedule every six months’ interval. These types of appointment schedules were practiced for stable category four ART patients according to the ASM classification tool.
Patients in the stable category four of ART: These are those ART patients receiving ART for at least 1 year with no adverse drug reactions requiring regular monitoring, no current illnesses or pregnancy, a good understanding of lifelong adherence and with evidence of treatment success.
Optimal ART adherence is defined as taking at least 95% of prescribed ARV drugs per specified period, whereas suboptimal ART adherence is defined as taking less than 95% of prescribed ARV drugs per specified period. A self-report recall period of one week and one month within data collection was used to measure adherence level in this study.
Data Collection Tools, Procedures, and Quality Control
Semi-structured interviewer-administered data collection tools were adapted and modified from literature written for a similar purpose.
Six diploma nurses’ data collectors and three public health officer supervisors were recruited purposively from health facilities providing ART services. They were trained for two days by the principal investigator on purpose and how to collect data. Before the interview began, the respondents had been informed about the objective of the study, and informed written consent was taken from the study participants.
The data collection tool was pre-tested on five per cent of the sample size to see the consistency of the tool outside of the study area. The questionnaire was prepared first in the English language, then translated into Afan Oromo, which is the local language, by another experienced person, and returned to the English language by another person to check for consistency between the two versions. The supervisors and principal investigator performed immediate supervision daily to ensure each completed questionnaire was completed.
Data Processing and Analysis Procedure
Descriptive analysis was used to describe the data using frequencies, distributions, proportions, and percentages. Tables were used for the presentation of data. Then, bivariate and multivariate logistic regression analysis was done to select candidate variables and factors independently associated with them, respectively. Accordingly, explanatory variables that had a p-value of less than 0.25 were included in the initial logistic models of multivariable analysis. Lastly, multivariable analysis was done to estimate crude and adjusted odds ratios together with their corresponding 95% confidence intervals. Accordingly, a P-value of less than 0.05 was declared as statistically significant in this study.
Results
Socio-Demographic and Economic Characteristics of Study Participants
Out of 463 study participants intended to be interviewed, 445 study participants were enrolled for the study, making a response rate of 96.1%. Respondents from the routine and appointment spacing model comprised 325 (73.1%) and 120 (26.9%) respectively, of which more than half of 254 (57.07%) of respondents were females. About two-thirds, 308 (69.2%) of study participants’ place of residency were urban dwellers, among whom a major proportion (70%) were enrolled from the ASM model rather than from the routine schedule (68.9%), but this difference was not statistically significant (P=0.91). In terms of marital status, more than half (327) (73.5%) of study participants were married, while 55 (12.5%) were never married, implying that more than half (240) (73.8%) of married study participants enrolled from the routine schedule than from the ASM model 87 (72.5%) (as show in Table 1).
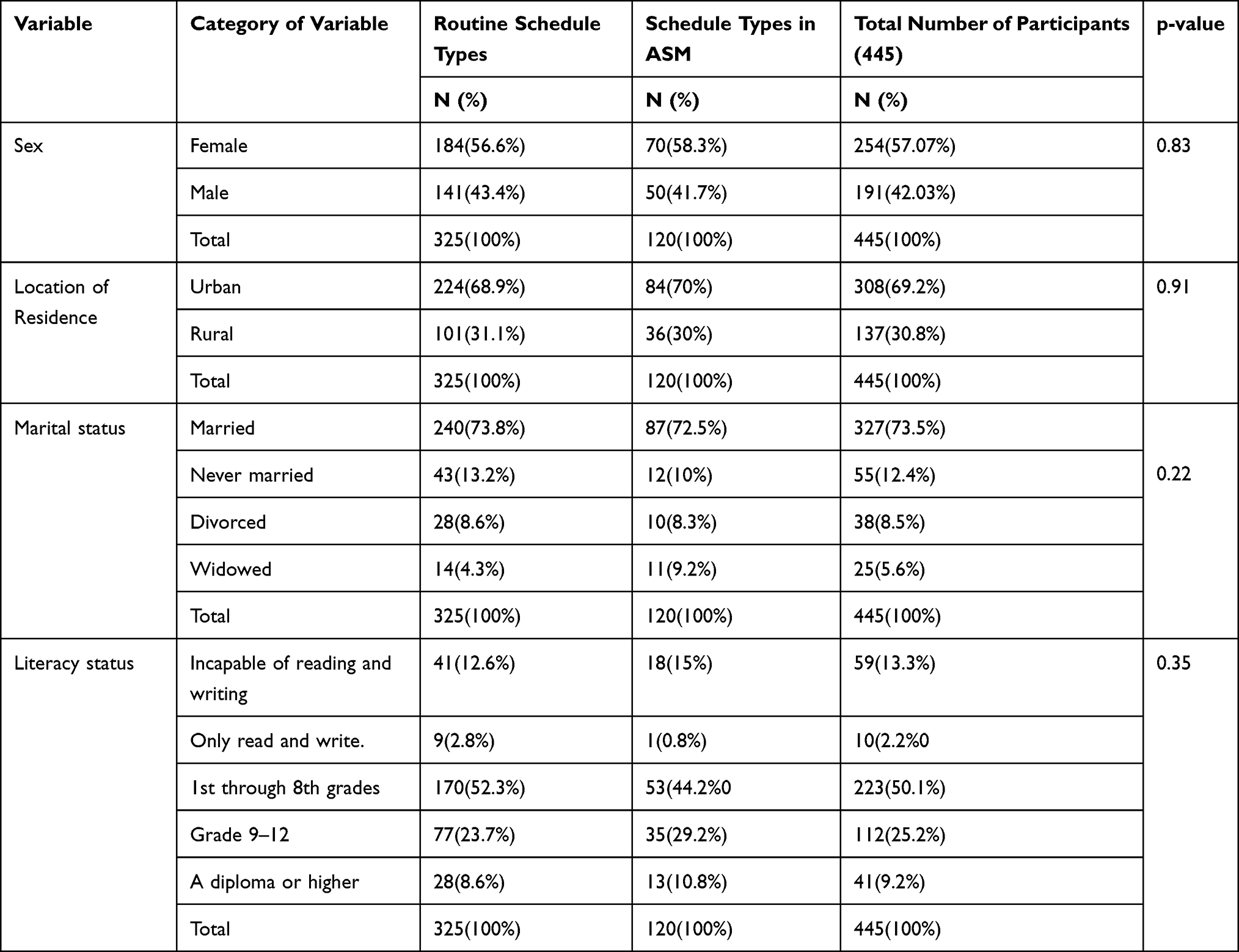 |
Table 1 Socioeconomic and Demographic Characteristics of ART Patients on Routine and Appointment Scheduling at West Wollega Zone Hospitals in 2019 (N=Total Number of Study Participants) |
Clinical Characteristics of Study Participants
More than third fourth (83%) of study participants’ viral load test results taken within one year of the data collection period were less than 1000 copies/mL, with a higher proportion (94%) being viral load test results of study participants from the ASM model compared to those of viral load study participants from the routine schedule 225 (79.2%), with no statistically significant difference (as shown in Table 2).
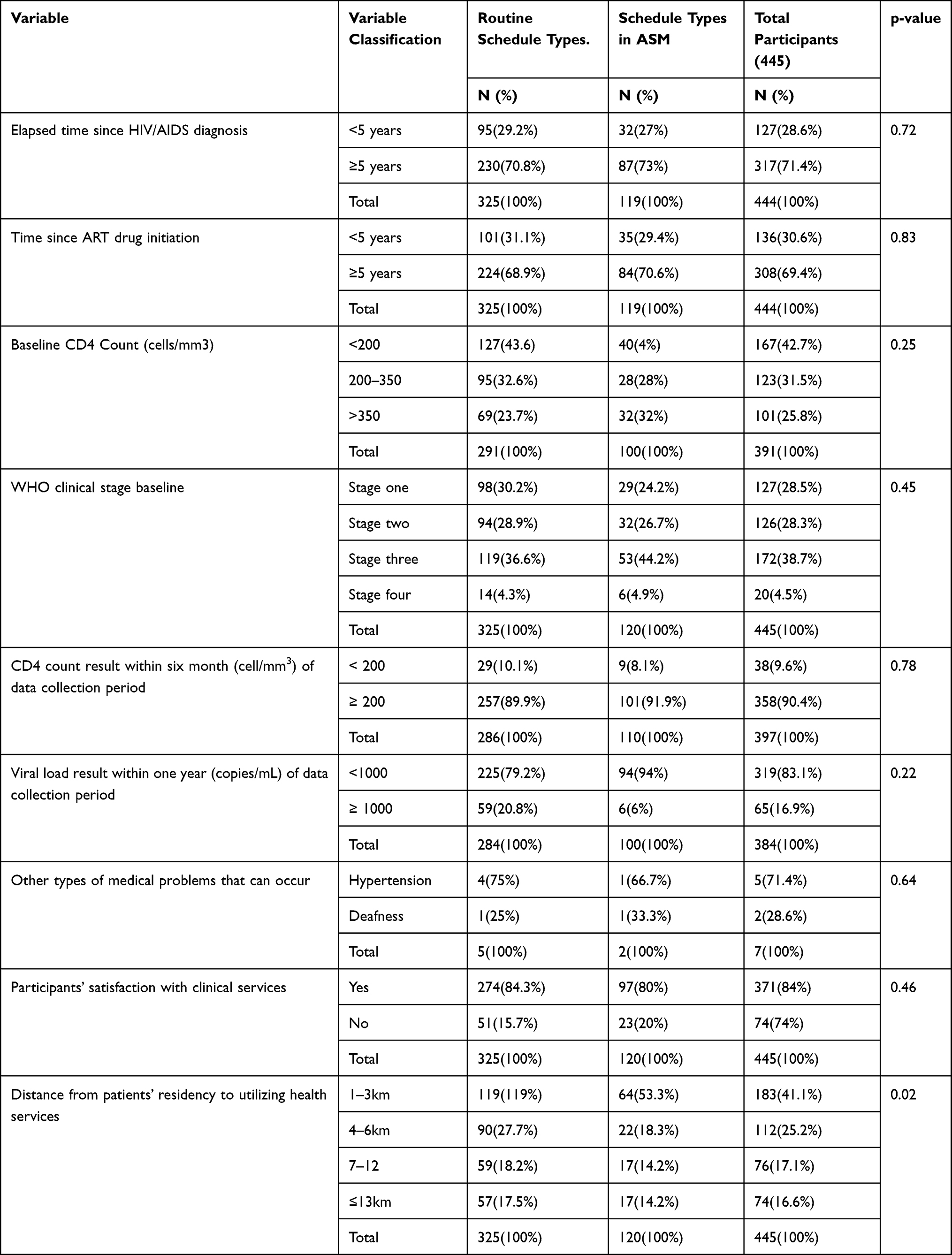 |
Table 2 Clinical Factors Characteristics of ART Patients on the Routine and Appointment Scheduling Models at Selected West Wollega Zone Hospitals in 2019 (N=Total Number of Study Participants) |
More than two-thirds (84%) of study participants reported satisfaction with their respective health professional service delivery given at their respective health facility, of which a higher proportion (84%) of study participants reported the routine schedule as compared to 97 (80.8%) of participants from the ASM model, which had no statistically significant difference (p=0.46) (as shown in Table 2).
ART Adherence Level and Appointment Following Status of Study Participants on Routine Schedule and ASM Model
In terms of appointment following status of study participants, ART patients who came strictly following their scheduled date were higher (59.2%) in the ASM model compared to (57.8%) of study participants on a routine schedule, though the difference was not statistically significant (p=0.88).
The adherence level to ART drugs of study participants was assessed using the patient self-report method in this study, with a recall period of a week and a month within a data collection period. Therefore, based on the quantity of ART drug dose taken per day, the total actual ART drugs taken per week and month were used to calculate the overall adherence level to ART drugs. Accordingly, the adherence level of the study of study participants tends to vary with the types of appointment schedule method and the recall period used. The optimum adherence level to ART drugs found among study participants on the ASM model was higher (109.8%) than the optimum adherence level found among participants on routine schedule 292 (89.8%) from the recall period within one week of data collection, but there was no statistically significant difference observed between these two models (P=0.5). However, the optimal ART adherence level to ART drugs among study participants on the routine schedule was lower (74.27%) than the optimal ART adherence level to ART drugs among study participants on the ASM model, indicating a statistically significant difference between the two models (p=0.006).
Factors Those are Independently Associated with the ART Adherence Level in ART Patients on a Routine Schedule
The multivariable analysis table revealed that factors such as the number of ART drug doses taken per day, client satisfaction with health professional service delivery at their respective health facility, and the distance of ART patients from their residence to their health facility were independently associated with ART adherence level for patients enrolled in this model.
Thus, ART patients who took two doses of ART drugs per day had three times more likely to adhere (OR=3, 95% CI 1.16–8.1) than those ART patients who took one dose of ART drug per day (as shown in Table 3).
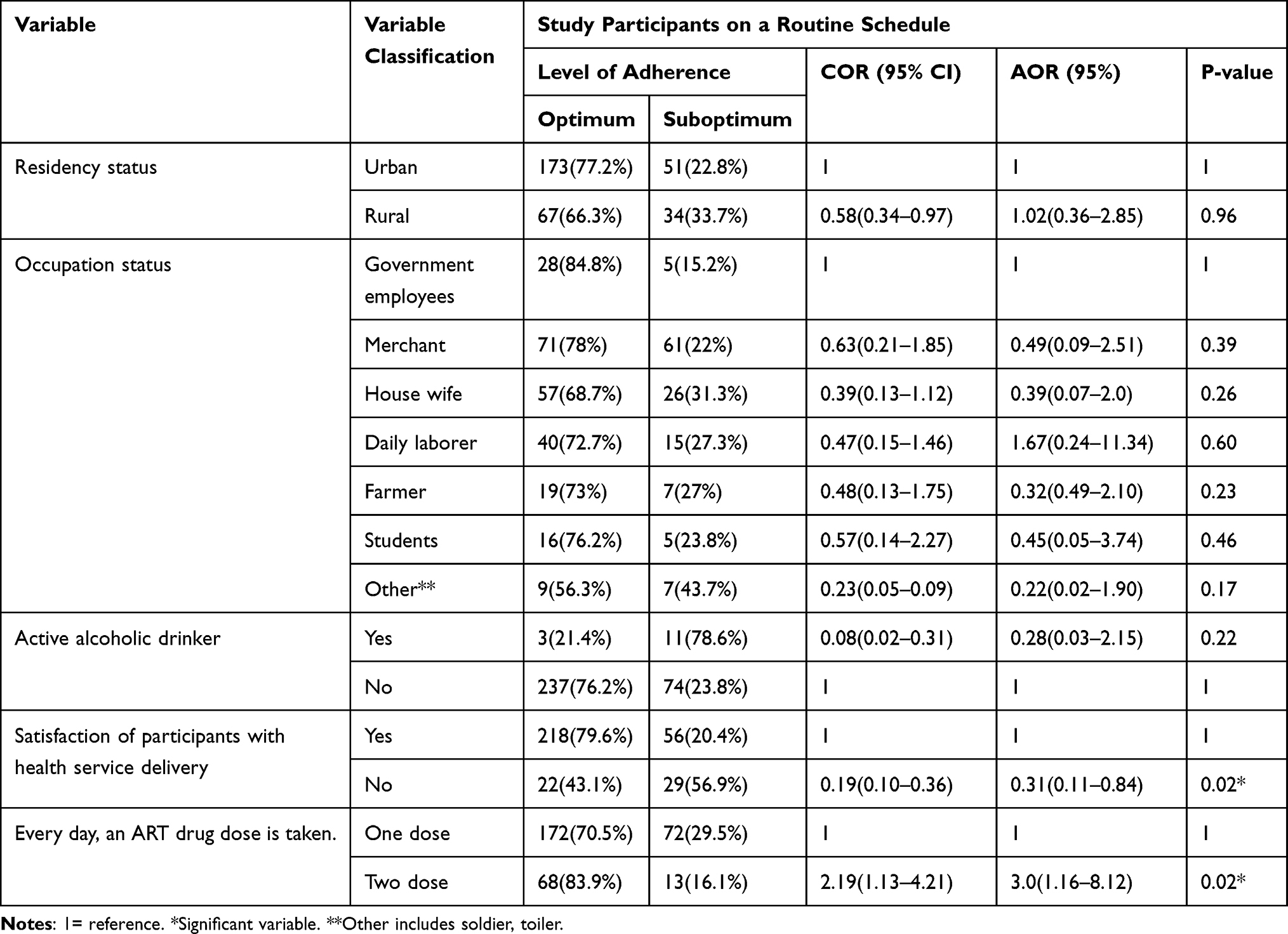 |
Table 3 Socio-Demographic, Health-Care Delivery-Related and Behavioral Factors That Were Independently Associated with ART Adherence Level to ARV Drugs Among ART Patients on a Routine Schedule at Selected West Wollega Zone Hospitals in 2019 |
ART patients on the routine schedule indicated that ART patients who were dissatisfied with the health service given at their respective health facility had 69% lower odds of adhering to their ART drug (OR=0.31, 95% CI 0.11–0.84) than those ART patients who were satisfied with the health service given at their respective health facilities (as shown in Table 3).
ART patients who came from a distance of at least thirteen kilometers (13KM) had 89% lower odds of adherence to their ART drug (OR=0.11, 95% CI 0.03–0.34) than those who came from a distance of at most three kilometers (1–3km) to follow their appointment schedule (as shown in Table 4).
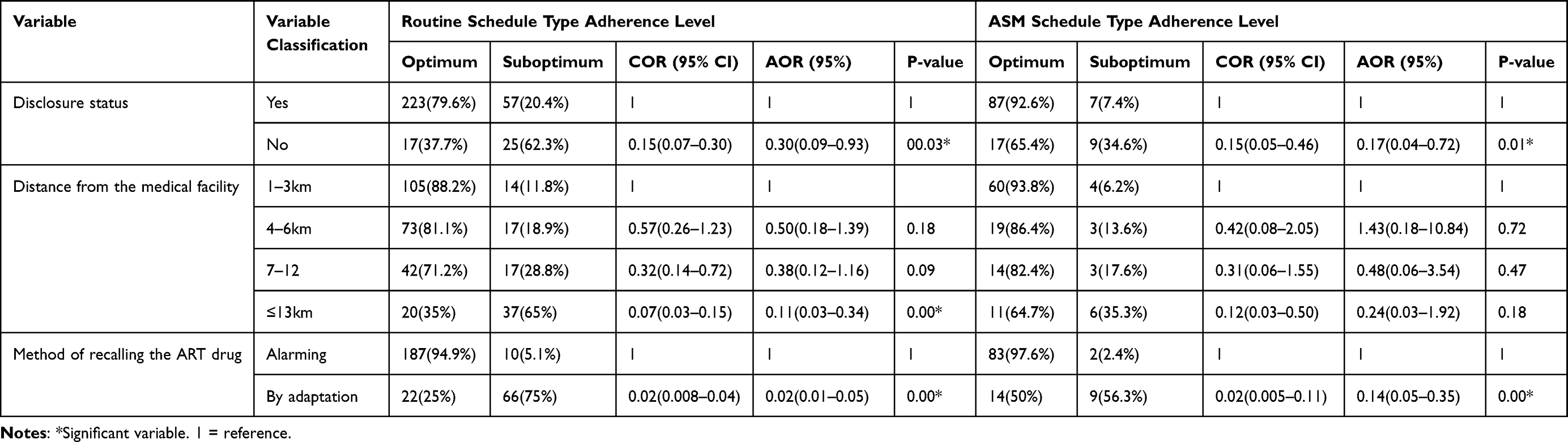 |
Table 4 Independently Associated Social-Clinical and Geographical Factors with ART Adherence Levels to ARV Drugs Among ART Patients on Routine and ASM Schedules at Selected West Wollega Zone Hospitals in 2019 |
Factors Independently Associated with ART Adherence Level in Both Routine and ASM Schedule Models
The ART patients who failed to disclose their HIV/AIDS status to others had 70% lower odds of adhering to their ART drug (OR=0.30, 95% CI 0.09–0.93) than those ART patients who disclosed their HIV/AIDS to others (as shown in Table 4).
ART patients who took their ART drug simply by adaption had 98% lower odds of adherence (OR=0.02, 95%: CI 0.01–0.05) than those who used alarms as memory aids, but ART patients who used another person to remind time of their ART drugs had 83% lower odds of adherence (OR=0.17, 95%: CI 0.05–0.5) than those ART patients who used alarms as a reminder of ART time (as shown in Table 4).
Factors Independently Associated with ART Adherence Levels to ARV Drugs Among Total ART Patients from Combined ART Care Models
Concerning ART patients’ satisfaction with health services provided by their respective health facilities, the results of multivariate binary logistic regression performed on general study participants from both models revealed that ART patients who were dissatisfied with health services had 80% lower odds of adhering to their ART drug (OR=0.2, 95% CI 0.14–0.7) than those ART patients who were satisfied with health services. In addition to the above factors, HIV/AIDS serostatus disclosure to others also influences ART patients’ adherence level. Therefore, ART patients who failed to disclose their HIV/AIDS status to others had 74% lower odds of adhering to their ART drug (OR=0.26, 95% CI 0.01–0.6) than those ART patients who disclosed their HIV/AIDS to others (as shown in Table 5).
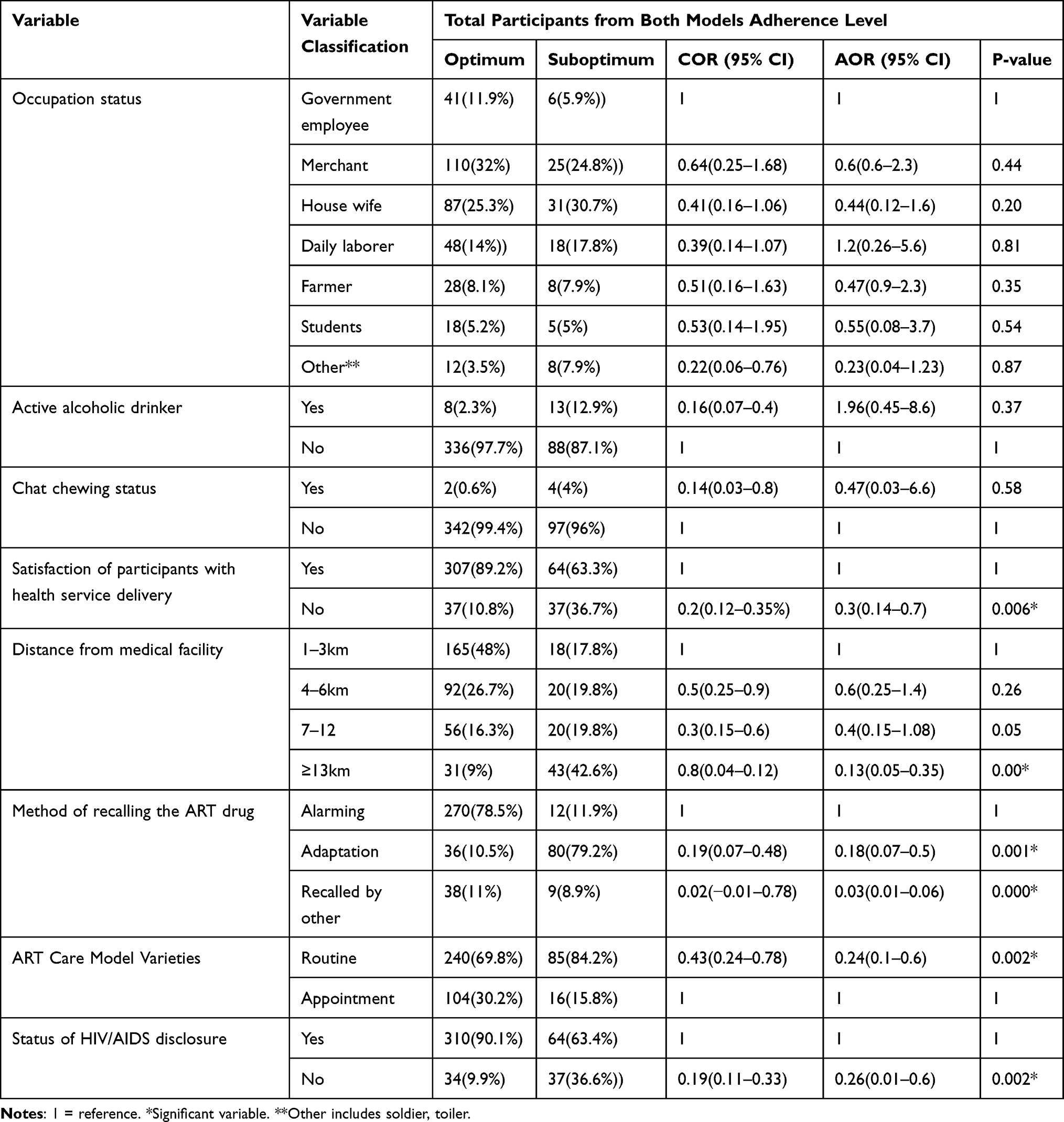 |
Table 5 Factors That are Independently Associated with ART Adherence Level to ARV Drugs in Total ART Patients from Both Models at Selected West Wollega Zone Hospitals in 2019 |
ART patients who came from a distance of at least thirteen kilometers (≥13KM) had 87% lower odds of adherence to their ART drug (OR=0.13, 95%: CI 0.05–0.35) than those who came from a distance of at most three kilometers (1–3km) to follow their appointment schedule (as shown in Table 5).
ART patients who simply adapted to their ARV drug had an 82% lower chance of adhering to their ART drug (OR=0.0.18, 95% CI 0.07–0.5) than ART patients who used alarm as a memory aid during drug taking (as shown in Table 5).
Finally, controlling other variables types of ART care model affects ART adherence level independently. Thus, ART patients who enrolled in the routine schedule had 76% lower odds of adherence to their ART drug (OR=0.24, 95% CI 0.0.1–0.6) than ART patients enrolled in the appointment spacing model (as shown in Table 5).
Discussion
Patients on the appointment spacing model had higher levels of optimum adherence than those on the routine schedule. Patients’ satisfaction with health service delivery, antiretroviral drug (ARV) dosage taken per day, disclosure of HIV sero-status, distance from patient residency to health facility, memory aids ART patients used and the type of HIV/AIDS care model were factors significantly associated with ART adherence level.
The optimal ART adherence level found from this study result for study participants on a routine schedule (74.3%) is consistent with the results of a study done in Yirgalem hospital in 2009, which was 74.2%,12 in Cape Coast metropolis, Ghana in 2018 which was 79.5%20 and in behavioral disease counseling center, Iran in 2019 which was 75.4%.46 However, it is lower than the study findings in Bale Robe Hospital of 2014, which was 83.1%,21 DebreBerhan Keble Health Centre and DebreBerhan Referral Hospital of 2018 which was 87.2%,22 Kathmandu District in Nepal of 2014, which was 86.7%,23 and University of Gondar Referral Hospital of 2014, which was 88.2%24 and higher than the study findings in Embu teaching and referral hospital comprehensive care clinic of 2016 which was 48.2%25 and Embe Hospital of 2016 which was 48.2%.26
This variation observed in different locations may have different reasons. For example, it could be related to the heterogeneity in ART adherence measurement methods since there is no consensus exists about the gold standard measurement of adherence of ART drugs, and it could also be due to different sample sizes taken by different authors.
The multivariate binary logistic regression of this study indicated that ART adherence level was affected by different factors, including the satisfaction of ART patients with the service delivered at their respective health facility. So, ART patients who were dissatisfied with health service delivery at their respective health facility had 69% lower odds of adhering to their ART drug (OR=0.31, 95%: CI 0.11–0.84) than those ART patients who were satisfied with the health service delivered at their respective health facility. This finding is consistent with the findings of a cross-sectional analytical study conducted in South Africa in 2017,27 Nigeria in 2013,28 a systematic review in Sub-Saharan Africa in 2016,29 Gondar University Referral Hospital in 2016,30 and Hossana Town in Southern Ethiopia in 2018.31
ART patients who received two doses of ART drugs per day were three times more likely to adhere (OR=3, 95% CI 1.16–8.1) than ART patients who received one dose of ART drug per day, but this finding contradicts one RCT study conducted in the United States in 2017.32 This variation could be due to the presence of other factors like age of participants, stage of HIV/AIDS, the status of ART side effects, and magnitude of viral load found in ART patients, which distort the direct relationship between ART adherence level and dose as well as the types of ART regimen patients use.32 scenario is true in this study, which found.
Another social factor affecting ART drug adherence among HIV positive patients was the disclosure of HIV/AIDS serostatus to an influential person. ART patients who did not disclose their HIV/AIDS status to others had a 70% lower chance of adhering to their ART drug (OR=0.30, 95% CI 0.09–0.93) than those who did. This finding is consistent with the studies done in Ghana in 2018,20 in Tanzania in 2015,33 in Goma, Democratic Republic of Congo (DRC) (a retrospective cohort study from Goma, Democratic Republic of Congo (DRC)34 (a systematic review and meta-analysis study done in Ethiopia in 2019,19,35 in Harar and Dire Dawa towns of Eastern Ethiopia in 2015,16 and in Hara town of North-Eastern Ethiopia in 2018.36
The distance of patients from health facilities also affects ART adherence levels among HIV/AIDS patients. Thus, ART patients who came from a distance of at least thirteen kilometres (13KM) had 89% lower odds of adherence to their ART drug (OR=0.11, 95% CI 0.03–0.34) than those who came from a distance of at most three kilometres (1–3km) to follow their appointment schedule. Even though the cut points and scale of measurement used by different authors were different, this study’s findings were similar to those of studies done in Zimbabwe in 201614 and in Nigeria in 2016.37 However, the result of a study done in Coastal South India in 2016 showed that distance did not affect ART adherence level.38 This could be due to the different sample size taken by the authors.
ART patients who took their ART drug simply by adaption had 98% lower odds of adherence to the ART drug (OR=0.02, 95%: CI 0.01–0.05) than those who used alarms as ART drug timers, but ART patients whose other person reminded them of the time of ART taking had 83% lower odds of adherence to the ART drug (OR=0.17, 95%: CI 0.05–0.5) than those who used alarms as a reminder of ART patients whose other person's alert. This finding is consistent with the study done in Nigeria in 2012,39 Results from a Cohort in South India in 2012,40 a rapid systematic review in South Africa in 2014,41 and Northwest Ethiopia in 2014.42 Even though different studies support the use of memory aid to increase ART adherence level, using memory aid all the time could not promote ART adherence level.43 This variation could be due to the fact that ART adherence level was not a unilateral cause, rather it was multi-causal and needed under control and following other factors. Finally, controlling for other exploratory variables, ART care model types, and ART patients enrolled all have an independent effect on ART adherence level. Thus, ART patients who enrolled on the routine schedule had 76% lower odds of adherence to their ART drug (OR=0.24, 95% CI 0.0.1–0.6) than ART patients enrolled on the appointment spacing model.
Even though comparative quantitative study research done on this topic is scarce, this finding is consistent with the comparative qualitative research studies done in Zambia in 2018,44 in South Sudan, the Central African Republic, and the DRC.45 However, in a 2017 study conducted in South Africa’s Western Cape, there was no significant difference in adherence levels between these two models.27 This might be due to the variation of the ART adherence measuring method undertaken, which was the self-report technique in this study and a mixed type for the later one.
The chance of recall bias and social desirability bias occurs due to the ART adherence assessment, which was based on self-report. Chart review resulted in missing some data like the current and baseline patient’s viral load and CD4 count.
Conclusions and Recommendations
ART patients on the appointment spacing model had a higher proportion of optimum ART Adherence levels than ART patients on the routine schedule. The level of ARV drug adherence among ART patients from both HIV/AIDS care models was determined by ART patients’ satisfaction with their health service delivery at their respective health facilities, their disclosure status about their HIV/AIDS serostatus to others, and the type of memory aids used. ART patients used to remember the time of ARV drug-taking, the distance between their residency and their respective health facility, and the type of HIV/AIDS care model ART patients enrolled in. ART care provider health professionals should encourage the appointment spacing model of the HIV/AIDS care program for all stable ART patients found at their ART clinics. Furthermore, health professionals providing ART services and Adherence counselors should provide intensive counseling about the risks of missing their ARV drug, advice patients on using memory aids to remember the time of ARV drug uptake, advice patients to disclose their HIV/AIDS status, and advice patients to follow drug uptake in the nearest health facility. Other researchers should evaluate ART retention outcome in addition to measuring mixed types of ART adherence.
Abbreviations
AIDS, acquired immune deficiency syndrome; ART, antiretroviral therapy; ARV, Antiretroviral drug; AOR, adjusted odd ratio; CD4, the cluster of differentiation 4; DRC, Democratic Republic of Congo; HIV, human immune deficiency virus; OR, odds ratio; PLWH, people living with human immune deficiency; SMA, the six-monthly appointment; SRS, simple random sampling; SPSS, Statistical Product and Service Solution; UNAIDS, United Nations Programme on acquired immune deficiency syndrome; VL, viral load; WHO, World Health Organization.
Data Sharing Statement
All data and materials are available and will be submitted by MrAdem Abdulkadir if needed.
Ethical Clearance
Ethical clearance was obtained from the ethical review committee of WollegaUniversity (number 233/WU/2019) in compliance with the Declaration of Helsinki. And official permission letter was secured from the hospital’s administrative office. The study subjects were informed about the objective and purpose of the study and written consent was obtained. Confidentiality of the information was assured and information was collected secretly.
Acknowledgments
The authors would like to thank Wollega University, the Institute of Health Science, and the Department of Public Health for their permission and support to undertake this study. Then my deepest gratitude and sincere appreciation go to all the data collectors, supervisors, study participants, and hospitals in the West Wollega zone health office and selected hospitals whose contributions were vital for the data collection activity.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The data collection process of this study was funded mainly by the principal investigator.
Disclosure
The authors declare that they have no conflicts of interest for this work nor regarding the publication of the paper.
References
1. Wood E, Hogg RS, Yip B, Harrigan PR, O’Shaughnessy MV, Montaner JS. Effect of medication adherence on survival of HIV-infected adults who start highly active antiretroviral therapy when the CD4+ cell count is 0.200 to 0.350× 109 cells/L. Ann Intern Med. 2003;139(10):810–816. doi:10.7326/0003-4819-139-10-200311180-00008
2. UNAIDS. Fact sheet - world AIDS day 2021; 2021. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf. Accessed December 5, 2021.
3. World Health Organization. World health statistics 2019: monitoring health for the SDGs, sustainable development goals; 2019. Available from: https://apps.who.int/iris/handle/10665/324835. Accessed December 5, 2021.
4. UNAIDS. 2006 Report on the global AIDS epidemic; 2006. Available from: https://data.unaids.org/pub/report/2006/2006_gr_en.pdf. Accessed December 5, 2021.
5. UNAIDS. Ambitious treatment targets: writing the final chapter of the AIDS epidemic; 2014. Available from: https://www.unaids.org/sites/default/files/media_asset/JC2670_UNAIDS_Treatment_Targets_en.pdf. Accessed December 5, 2021.
6. Mills EJ, Nachega JB, Buchan I, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: a meta-analysis. JAMA. 2006;296(6):679–690. doi:10.1001/jama.296.6.679
7. Costa JD, Torres TS, Coelho LE, Luz PM. Adherence to antiretroviral therapy for HIV/AIDS in Latin America and the Caribbean: systematic review and meta‐analysis. J Int AIDS Soc. 2018;21(1):e25066. doi:10.1002/jia2.25066
8. UNAIDS. Global AIDS Update 2016; 2016. Available from: https://www.unaids.org/sites/default/files/media_asset/global-AIDS-update-2016_en.pdf. Accessed December 5, 2021.
9. Psomas CK, Fidler S, Macartney M, et al. Highlights from the 22nd International AIDS Conference (AIDS 2018), 22–27 July 2018, Amsterdam, the Netherlands. J Virus Eradication. 2018;4(4):238–247. doi:10.1016/S2055-6640(20)30310-1
10. Fox MP, Rosen S. Retention of adult patients on antiretroviral therapy in low-and middle-income countries: systematic review and meta-analysis 2008–2013. J Acquir Immune Defic Syndr. 2015;69(1):98. doi:10.1097/QAI.0000000000000553
11. Federal HIV/AIDS Prevention and Control Office. HIV prevention in Ethiopia national road map 2018-2020; 2018. Available from: https://ethiopia.unfpa.org/sites/default/files/pub-pdf/HIV%20Prevention%20in%20Ethiopia%20National%20Road%20Map%202018%20-%202020%20FINAL_FINAL.pdf. Accessed December 5, 2021.
12. Markos E, Worku A, Davey G. Adherence to ART in PLWHA and Yirgalem hospital, South Ethiopia. Ethiop J Health Dev. 2009;22(2):174–179.
13. Mabunda K, Ngamasana EL, Babalola JO, Zunza M, Nyasulu P. Determinants of poor adherence to antiretroviral treatment using a combined effect of age and education among human immunodeficiency virus infected young adults attending care at Letaba Hospital HIV Clinic, Limpopo Province, South Africa. Pan Afr Med J. 2019;32:37.
14. Gonah L, Mukwirimba A. Determinants of optimal adherence to antiretroviral therapy among people living with HIV/AIDS registered for antiretroviral therapy in Zimbabwe. Med J Zambia. 2016;43(4):174–183.
15. Mitiku H, Abdosh T, Teklemariam Z. Factors affecting adherence to antiretroviral treatment in Harari national regional state, Eastern Ethiopia. Int Sch Res Notices. 2013;5:960954.
16. Letta S, Demissie A, Oljira L, Dessie Y. Factors associated with adherence to Antiretroviral Therapy (ART) among adult people living with HIV and attending their clinical care, Eastern Ethiopia. BMC Int Health Hum Rights. 2015;15(1):1–7. doi:10.1186/s12914-015-0071-x
17. Assefa T, Melaku Z, Amdino W, et al. Implementation of the appointment spacing model of differentiated service delivery in Ethiopia: successes and challenges; 2018. PEPFAR; ICAP. Available from: https://cquin.icap.columbia.edu/wp-content/uploads/2020/03/Assefa-et-al_AIDS2018.pdf. Accessed December 5, 2021.
18. Central Statistical Agency, Ethiopia; ICF International, USA. Ethiopia Demographic and Health Survey 2011; 2011. Available from: https://dhsprogram.com/pubs/pdf/fr255/fr255.pdf. Accessed December 5, 2021.
19. Amberbir A, Woldemichael K, Getachew S, Girma B, Deribe K. Predictors of adherence to antiretroviral therapy among HIV-infected persons: a prospective study in Southwest Ethiopia. BMC Public Health. 2008;8(1):1–9. doi:10.1186/1471-2458-8-265
20. Prah J, Hayfron-Benjamin A, Abdulai M, Lasim O, Nartey Y. Factors affecting adherence to antiretroviral therapy among HIV/AIDS patients in cape coast metropolis. Ghana J HIV AIDS. 2018;4(1). doi:10.16966/2380-5536.149
21. Mohammed AY, Ahmed MB, Tefera TB. Assessment of factors affecting art adherence among people living with human immune virus in bale robe hospital, south EastEthiopia. Am J Public Health. 2015;3(2):60–67.
22. Mengistie A, Birhane A, Tesfahun E, City DB. Assessment of adherence to antiretroviral therapy among adult people living with HIV/AIDS in North East, Ethiopia. bioRxiv. 2018:492330. doi:10.1101/492330
23. Shigdel R, Klouman E, Bhandari A, Ahmed LA. Factors associated with adherence to antiretroviral therapy in HIV-infected patients in Kathmandu District, Nepal. HIV/AIDS. 2014;6:109.
24. Molla AA, Gelagay AA, Mekonnen HS, Teshome DF. Adherence to antiretroviral therapy and associated factors among HIV positive adults attending care and treatment in University of Gondar Referral Hospital, Northwest Ethiopia. BMC Infect Dis. 2018;18(1):1–8.
25. Mugoh EK, Kabiru E, Mwaniki J. Patient factors influencing adherence to ART treatment among HIV/AIDS patients in embu teaching and referral hospital comprehensive care clinic. J Public Health. 2016;18(4):375–380.
26. Abera A, Fenti B, Tesfaye T, Balcha F. Factors influencing adherence to antiretroviral therapy among people living with HIV/AIDS at ART Clinic in Jimma University teaching hospital, Southwest Ethiopia. J Pharma Rep. 2015;1(101):2.
27. DeJager GA, Crowley T, Esterhuizen TM. Patient satisfaction and treatment adherence of stable human immunodeficiency virus-positive patients in antiretroviral adherence clubs and clinics. Afr J Prim Health Care Fam Med. 2018;10(1):1–8.
28. Oche MO, Raji MO, Kaoje AU, et al. Clients satisfaction with antiretroviral therapy services in a tertiary hospital in Sokoto, Nigeria. J AIDS HIV Res. 2013;5(9):328–333.
29. Heestermans T, Browne JL, Aitken SC, Vervoort SC, Klipstein-Grobusch K. Determinants of adherence to antiretroviral therapy among HIV-positive adults in sub-Saharan Africa: a systematic review. BMJ Glob Heal. 2016;1(4):1–13.
30. Abebe TB, Erku DA, Gebresillassie BM, Haile KT, Mekuria AB. expectation and satisfaction of hiV/AiDs patients toward the pharmaceutical care provided at Gondar University referral hospital, northwestern Ethiopia: a cross-sectional study. Patient Prefer Adherence. 2016;10:2073. doi:10.2147/PPA.S114720
31. Doyore F, Moges B. Client satisfaction to antiretroviral treatment services and associated factors among clients attending ART clinics in Hossana town, southern Ethiopia. Clin Res. 2016;2(6):6.
32. Chen Y, Chen K, Kalichman SC. Barriers to HIV medication adherence as a function of regimen simplification. Ann Behav Med. 2017;51(1):67–78. doi:10.1007/s12160-016-9827-3
33. Buma D, Bakari M, Fawzi W, Mugusi F. The influence of HIV-status disclosure on adherence, immunological and virological outcomes among HIV-infected patients started on antiretroviral therapy in Dar-es-Salaam, Tanzania.
34. Akilimali PZ, Musumari PM, Kashala-Abotnes E, et al. Disclosure of HIV status and its impact on the loss in the follow-up of HIV-infected patients on potent anti-retroviral therapy programs in a (post-) conflict setting: a retrospective cohort study from Goma, Democratic Republic of Congo. PLoS One. 2017;12(2):e0171407. doi:10.1371/journal.pone.0171407
35. Dessie G, Wagnew F, Mulugeta H, et al. The effect of disclosure on adherence to antiretroviral therapy among adults living with HIV in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2019;19(1):1–8. doi:10.1186/s12879-019-4148-3
36. Legesse TA, Reta MA. Adherence to antiretroviral therapy and associated factors among people living with HIV/AIDS in Hara town and its surroundings, North-Eastern Ethiopia: a cross-sectional study. Ethiop J Health Sci. 2019;29(3):299–308.
37. Augustina O, Omotayo OE, Geoffrey E. Factors associated with non-adherence of HIV/AIDS patients to HAART regimen in a healthcare facility in IkotEkpene, AkwaIbom State, Nigeria. J AIDS HIV Res. 2019;11(3):16–24. doi:10.5897/JAHR2018.0481
38. Achappa B, Madi D, Bhaskaran U, Ramapuram JT, Rao S, Mahalingam S. Adherence to antiretroviral therapy among people living with HIV. N Am J Med Sci. 2013;5(3):220. doi:10.4103/1947-2714.109196
39. Maduka O, Tobin-West CI. Adherence counseling and reminder text messages improve uptake of antiretroviral therapy in a tertiary hospital in Nigeria. Niger J Clin Pract. 2013;16(3):302–308. doi:10.4103/1119-3077.113451
40. Rodrigues R, Shet A, Antony J, et al. Supporting adherence to antiretroviral therapy with mobile phone reminders: results from a cohort in South India. PLoS One. 2012;7(8):e40723. doi:10.1371/journal.pone.0040723
41. Chaiyachati KH, Ogbuoji O, Price M, Suthar AB, Negussie EK, Bärnighausen T. Interventions to improve adherence to antiretroviral therapy: a rapid systematic review. AIDS. 2014;1(28):S187–204. doi:10.1097/QAD.0000000000000252
42. Arage G, Tessema GA, Kassa H. Adherence to antiretroviral therapy and its associated factors among children at South Wollo Zone Hospitals, Northeast Ethiopia: a cross-sectional study. BMC Public Health. 2014;14(1):1–7. doi:10.1186/1471-2458-14-365
43. Ontario HIV Treatment Network. Reminder systems for people living with HIV; 2015. Available from: https://www.ohtn.on.ca/rapid-response-95-reminder-systems-for-people-living-with-hiv-2/. Accessed December 6, 2021.
44. Mody A, Roy M, Sikombe K, et al. Improved retention with 6-month clinic return intervals for stable human immunodeficiency virus-infected patients in Zambia. Clin Infect Dis. 2018;66(2):237–243. doi:10.1093/cid/cix756
45. Ssonko C, Gonzalez L, Mesic A, et al. Delivering HIV care in challenging operating environments: the MSF experience towards differentiated models of care for settings with multiple basic health care needs. J Int AIDS Soc. 2017;20:21654. doi:10.7448/IAS.20.5.21654
46. Morowatisharifabad MA, Movahed E, Farokhzadian J, Nikooie R. Antiretroviral therapy adherence and its determinant factors among people living with HIV/AIDS: a case study in Iran. BMC Res Notes. 2019;1–5. doi:10.1186/s13104-019-4204-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.