")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Antiretroviral Therapy Service Quality and Associated Factors at Selected Public Hospitals, Addis Ababa, Ethiopia, 2021
Authors Tiruneh CT , Woldeyohannes FW
Received 7 November 2021
Accepted for publication 15 March 2022
Published 25 March 2022 Volume 2022:14 Pages 129—142
DOI https://doi.org/10.2147/HIV.S348254
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Chalachew Teshome Tiruneh,1 Fikirte Woldeselassie Woldeyohannes2
1Department of Antiretroviral Treatment Unit, Zewditu Memorial Hospital, Addis Ababa, Ethiopia; 2Department of Women, Children and Youth Director, Kotebe University of Education Menelik Ii Medical and Health Science College, Addis Ababa, Ethiopia
Correspondence: Fikirte Woldeselassie Woldeyohannes, Tel +0911417846, Email [email protected]
Background: It is important to offer high-quality HIV/AIDS treatment and antiretroviral medication to people living with the disease to improve health outcomes. The quality of health services has become a public health issue.
Objective: To assess ART service quality and associated factors at a selected public hospital, Addis Ababa, Ethiopia, in 2021.
Methods: A mixed study design was used from April to May 2021. Donabedian’s structure–process–outcome model of health care quality was employed as a framework. A total of 420 clients were interviewed to obtain quantitative data, and 08 key informant interviews and 357 program documents were reviewed. Quantitative data were checked, coded, and entered into Epi Info version 7.2 and exported into SPSS windows version 25.0. In the multivariable logistic regression analysis, variables with p-values < 0.05 and adjusted odds ratio (AOR) with 95% confidence interval (CI) were used to identify factors associated with client satisfaction. Qualitative data were transcribed and analysed using the ATLAS.ti version 8 software program and used to complement the quantitative findings.
Results: The overall quality of ART services was 73.3% for the availability of resources, 79.5% for healthcare providers’ compliance with the national guidelines, and 86.4% for client satisfaction with the quality of ART clinical services. Patients who disclosed their HIV status [AOR 10.7, 95% CI: 5.2– 22], months of ART [AOR 10.4, 95% CI: 3.89– 27.8], age group 34– 44, 45– 55, and 56– 76 years were found to be 5.1, 8.1, and 5 [AOR 5.1,95% CI:1.2– 22, AOR 8.1,95% CI:1.9– 35.5, AOR 5,95% CI:2.97– 9.44], respectively, and consultation time [AOR 3.5, 95% CI: 1.6– 7.35] were associated with client satisfaction on the quality of ART clinical services.
Conclusion: This study revealed that the overall quality of ART services in selected Addis Ababa public hospitals was good, although with the availability of resources and compliance health care providers need improvement.
Keywords: availability, compliance, satisfaction, ART, quality
Introduction
HIV/AIDS is the world’s most severe and critical public health pandemic today.1,2 Antiretroviral therapy is a therapeutic choice for HIV-positive individuals, allowing them to live longer, happier lives and increase their quality of life. People with HIV who do not have access to ARVs often die within one or two years of developing AIDS.3 Quality HIV/AIDS treatment is characterised by adherence to prescribed standards of care and includes treatments that have been proven to be healthy, inexpensive, and effective in reducing morbidity and mortality among HIV-positive individuals.4
One of the main strategic goals of the Ethiopian federal ministries is to improve and maintain high-quality HIV/AIDS diagnosis and treatment. Quality HIV/AIDS programs are critical for maintaining health, preventing disease, and reducing morbidity and mortality from illness, both of which are important for a stable country.5 The quality of services in terms of client satisfaction with ART services was associated with the availability of the services, patient-provider interaction, privacy during examination, confidentiality, educational status, and disclosure of HIV status to parents.6
Lack of professional skills and client-provider communication has been considered a priority component in determining the quality of care.
The quality of health services has become a public health issue. Building quality into health systems is possible if several steps are followed and principles are applied. A lack of technical expertise in integrating and aligning quality management with normal procedures, as well as client-provider coordination about the mechanisms and results of services provided to them, has been identified as a critical factor in determining service quality.7
Provider-client interaction in counselling, testing, managing opportunistic infections, documentation, and related services improve client satisfaction with HIV services and enrolment and retention in the HIV services cascade. Patient satisfaction is an important indicator of the quality of health care provided. The quality of ART services in terms of client satisfaction remains a challenge.8,9
Although multiple studies have shown that ART is effective in reducing HIV-related deaths in Africa, there is little evidence on the quality of ART service delivery. Maintaining the quality of all services is a critical component of Ethiopia’s robust HIV/AIDS response.10
Improving quality and safety in health services at all levels of the healthcare system is currently the focus of the Ethiopian government because of the clear evidence that quality remains a serious concern. Studies on ART quality and client satisfaction have strengthened the success of public health policies in enhancing access to care. Quality of care helps identify the gap between clients’ expectations and what the institution has provided for them. Working through the process of quality and continuous quality improvement will create an environment for transforming the health sector and achieving the health outcome goals highlighted in the Ethiopian government growth and transformation plan and health sector transformation plan.
Therefore, this study aimed to assess the quality of ART services in terms of client satisfaction at public hospitals in Addis Ababa, Ethiopia by using Donabedian’s structure–process–outcome model of ART health care quality examining health services and evaluating the quality of health care. According to the model, information about the quality of care can be drawn from three categories: structure describes the context in which care is delivered, including hospital buildings, staff, financing, and equipment, process denotes the transactions between patients and providers throughout the delivery of healthcare; and outcomes refer to the effects of healthcare on the health status of patients and populations.11 The Donabedian model has potential limitations of sequential progression from structure to process to the outcome which has been described by some as too linear of a framework12 and consequently has a limited utility for recognising how the three domains influence and interact with each other.13
Methods
Study Area and Period
This study was conducted in Addis Ababa public hospitals from April to May 2021. Addis Ababa is Ethiopia’s capital city. During the study period, 13 government hospitals in Addis Ababa provided ART services, four of them were chosen using a simple random sample approach and four of the hospitals provided antiretroviral treatment to 19,367 HIV/AIDS patients.
Study Design and Population
A mixed study design with Donabedian’s structure–process–outcome model of health care quality was employed as a framework.14 The convergence mixed technique is probably the most familiar of the basic and advanced mixed methods strategies. The researcher gathered both quantitative and qualitative data simultaneously and then analysed the results to determine whether the findings validated or disproved each other.15 Quantitative and qualitative methods of data collection techniques such as client exit interviews, document reviews, and in-depth interviews were used. A cross-sectional study was used for quantitative analysis. All HIV-positive patients enrolled in ART clinical care and treatment, assigned program managers, and client charts in selected public hospitals of Addis Ababa were the study population.
Sample Size Determination and Sampling Procedure
The sample size for exit interviews was determined by considering a 95% confidence level, 5% marginal error, and the proportion of client level satisfaction was 54.6% which was obtained from a study conducted on the clinical care of people living with HIV/AIDS in the Dilchora referral hospital.16
n= (Za/2)2*p(1-p) Where n= Sample Size
D2
Za/2=95% confidence level (1.96)
P=Proportion of client satisfaction Level (0.546)
D= 5% marginal error (0.05)
N= (1.96)2*0.546(1–0.546) 3.8416*0.546*0.454 =381
(0.05)2 0.0025
By adding a 10%, non-response rate the total sample size was 420 clients.
The interviews were conducted with eight (08) key informants (program managers and health care providers) from four hospitals (Alert Hospital, St-Peters Specialised Hospitals, Zewditu Hospital, and Yekatit 12 Hospital).
The sample size for document review was calculated using the clinical quality audit formula to determine the delivery of ART clinical care according to the standards and compliance of health care providers in recording patient information.17 The charts of 357 patients were reviewed.
Simple random sampling was used to select four hospitals and a systematic random sampling technique was used to select 420 study subjects. The sample size for each hospital was determined using proportional allocation. To obtain the K value for each selected hospital the entire study population was divided by the study subjects (N/n) which was the interval of the study. For St-Peters Specialised Hospitals and Yekatit 12 Hospitals, the k value was seven. For the ALERT and Zewditu Hospitals, respectively, the K value was three. Client charts reviewed for quantitative data were selected until the sample size for chart review was fully collected. Study participants for key informants’ interviews were selected using purposive sampling. Participants who had worked for six months or more in that particular department were interviewed until data saturation was reached.
Data Collection Tools and Procedures
Data were collected from four hospitals (Alert Hospital, St-Peters Specialised Hospitals, Zewditu Hospital, and Yekatit 12 Hospital). Data collection instruments for quantitative data were prepared by reviewing different scientific works in the literature and national and international guidelines for HIV/AIDS care.
Qualitative data were collected through in-depth interviews with principal investigators from key informants (program managers and health care providers). The responses of key informants were recorded using a tape recorder and handwritten notes and analysed using Atlas software according to their theme.
Exit Interview Questionnaire
A structured questionnaire was used to assess client satisfaction, including respondents’ Socio-demographic characteristics (Age, Sex, Marital status, Educational status, Occupational status, Income level, Place of residence), waiting time(minutes) to receive service, consultation time in minutes, and travel distance in an hour.
Information related to the availability of program resources (human resources, infrastructure, material resources, logistics, and supplies) and information related to compliance (patient-provider interaction, and service appropriateness from the client’s point of view. The questionnaire contained 18 items with a 5-Likert scale and was adapted from similar literature conducted previously with little modification.4,18
Key Informant Interview Guide
An interview guide that assesses the experiences of program managers, health care providers, and adherence support in the provision of quality ART clinical care service, challenges in delivering quality service, and recommended solutions was used.
The Document Review
Three hundred and fifty-seven patient records were reviewed. Document review was conducted at a convenient time (on weekends) that did not compromise the daily activities of the clinic.
Data Collectors
Four BSc holder nurses who had basic ART training and previous work experience in the program and data collection were recruited as data collectors to conduct an exit interview. Two days of training were given before data collection on data collection tools and procedures, and ethical issues for data collectors. An in-depth interview was conducted with the principal investigator.
Study Variables
In this study client satisfaction was the outcome variable. Independent variables included were availability, compliance, socio-demographic characteristics (age, sex, marital status, educational status, occupational status, and income level), place of residence, waiting time (minutes) to receive service, consultation time in a minute, travel distance in an hour, availability of program resources, adherence to guidelines in diagnosis, treatment, counselling, client-provider interaction, waiting area and time, privacy, Comfortable and pleasant surroundings, and respective care.
Data Quality Control and Data Analysis
Two days of training and discussion were conducted on data collection tools and procedures, and ethical issues during data collection with research assistance.
Before the actual data collection, a pre-test was performed. The purpose of the pre-test was to ascertain patients ‘understanding of the items by asking about the appropriateness of responses and the time required to fill out the questionnaire. Finally, ambiguous and unclear questions were addressed. The supervisor and principal investigator conducted daily supervision during data collection fieldwork and the data were checked for completeness daily. Data were checked for proper collection and recording, coded separately, cleaned and entered into Epi Info version 7.2 and then exported to SPSS windows version 25 for analysis. Qualitative data were transcribed and analysed using the ATLAS.ti version 8 software program and used to complement the quantitative findings.
The negatively arranged questions were recorded in reverse before the scores were calculated to classify the cuts of the points. The median score was calculated and patients who had a score above the median score were considered satisfied while the median and below scores were considered not satisfied. Experts have argued that the median should be used as a measure of central tendency for Likert scale data.19
Descriptive statistics such as frequency, proportion, mean, and median of the variables were used to report the descriptive results. A reliability estimate was conducted and Cronbach’s alpha was 0.91 for the compliance factors and 0.7 for client satisfaction measurement tools. Bivariate logistic regression analysis was conducted and variables that satisfied the assumption of p≤0.25, which is the commonly used cutoff in our research community were considered as candidates for multivariate analysis and multivariate analysis was used to check statistical significance at p<0.05.
Ethical Considerations
The Kotebe Metropolitan University Menelik II Medical and Health Science College, Alert Hospital, St-Peters Specialised Hospital, and the Institutional Review Board of Addis Ababa regional health bureau gave ethical clearance letters. A letter of permission to conduct the study was secured from the Addis Ababa Regional Health Office, and four hospitals. Informed consent was obtained from the respondents and institutions for data collection. Covid 19 protocol and safety were maintained. The questionnaires were anonymous which kept the privacy and confidentiality of the participants.
Result
Socio-Demographic Characteristics of Study Subject
A total of 420 HIV/AIDS-positive clients were interviewed. In this study 167 (39.8%) were from Zewditu Memorial Hospital, 140 (33.3%) were from ALERT Hospital, 65 (15.5%) were from Yekatit 12 Hospitals and 48 (11.4%) were from St Peter Hospital. In this study, the number of female patients (67.1%) was higher than that of men. The mean age of the respondents was 43.8 (±9.8 years) and the majority 176 (41.9%) and 153 (36.4%) of clients lied in the age range of 34–44 and 45–55 years old respectively. Regarding marital status, 184 (43.8%) of the respondents were married 84 (20%) were single, 80 (19%) were widowed and 72 (17.2%) were divorced. The majority of respondents (74.5%) were orthodox religious followers. Unemployment accounted for 124 (29.5%) followed by others (Driver, housewife, and student) 102 (24%), while 30.2% of clients were elementary (1–8) educational level and secondary (9–12) level (31.9%) education, with the majority of clients receiving ART clinical services for more than 5 years (more than 60 months) (Table 1).
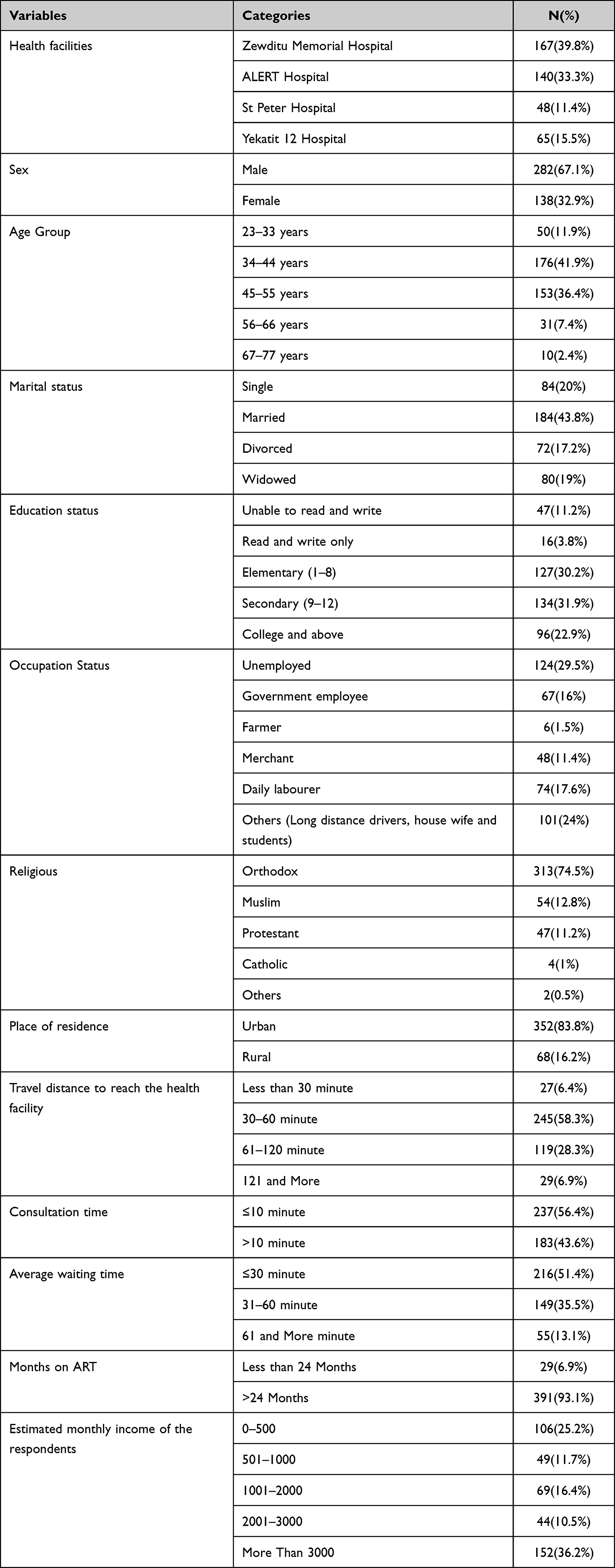 |
Table 1 Sociodemographic Characteristics of Respondents in Client Satisfaction with the Quality of ART Clinical Service in Selected Addis Ababa Public Hospitals, 2021 (n=420) |
Availability Dimension (Structural Quality Indicators)
This study was conducted in four government hospitals in Addis Ababa that provide ART services. The availability of the resources required to provide the service was assessed based on the three minimum packages of the ART program. These are clinical, pharmacy, and laboratory criteria for facility accreditation to provide ART services at different levels of facilities.
Regarding infrastructure, there were separate ART clinics in all hospitals for the program with on-site pharmacy and laboratory services, except in one hospital without on-site ART laboratories. There were separate rooms for examination, counselling services, and data clerks in all hospitals but there was a space problem in two hospitals; one room was used for two clients at the same time for ART refill and drug adherence counselling.
Regarding other infrastructures, all the facilities had functional computers, electric supply; water supply, internet access, waiting area, and latrines with adequate sittings were available in all hospitals while functional telephones were available in two hospitals.
Regarding medical equipment and supplies, there were no functional blood pressure cuffs, reflex hammers, otoscopes, tongue blades, and thermometers available in each health facility. Adult and child scales, height scales, and examination beds were available in all facilities during the data collection period.
There were 30 nurse professionals, 16 medical doctors, 08 laboratory professionals (lab sample collectors), 10 pharmacists and 21 data clerks working in clinics in the study areas. Regarding training, health care providers received basic ART training in the last twelve months except for three nurses and all laboratory professionals working in the ART laboratory did not receive any training in the last twelve months. One daily internist was assigned for a consultation to provide HIV/AIDS clinical care.
Laboratory services are provided in the facilities for clients. Laboratory equipment such as a Microscope, Refrigerator, Centrifuge, and IP supplies are available in all facilities. Equipment such as sterilising equipment, CD4 Count Machines, Clinical chemistry auto analysis, CBC Machines, and X-rays are available in all facilities. A Viral load machine is available at the Addis Ababa city administration regional laboratory, Ethiopian public health institute and ALERT Hospital which do viral load count for all lab samples sent from public health facilities.
There was a separate drug-dispensing unit for ART clients in all hospitals. Regarding the availability of ARV drugs, all first-line regimens were available during the data collection period. There is a shortage of second-line regimens in all hospitals while lamivudine (3TC) was stocked out for three weeks before the data collection period in one hospital. Family planning drugs were not available in all hospitals at HIV/AIDS clinics except condoms but there is internal referral and linkage for family planning to the family planning unit if the client wants any family planning.
Service aiding resource availability such as recording and reporting materials are important resources for program implementation. Service recording and reporting tools such as registration logbook (ART, Pre-ART, ART follow up, and intake form), internal and external referral formats and appointment calendars are available in all facilities. Other services aiding tools such as standard operating procedures, ART guidelines, and adherence counselling protocols were available in all facilities providing the service. Only one facility had ART implementation guidelines.
The quality of ART clinical service in terms of program resource availability was measured to be 73.3%, which is good but needs improvement (Table 2).
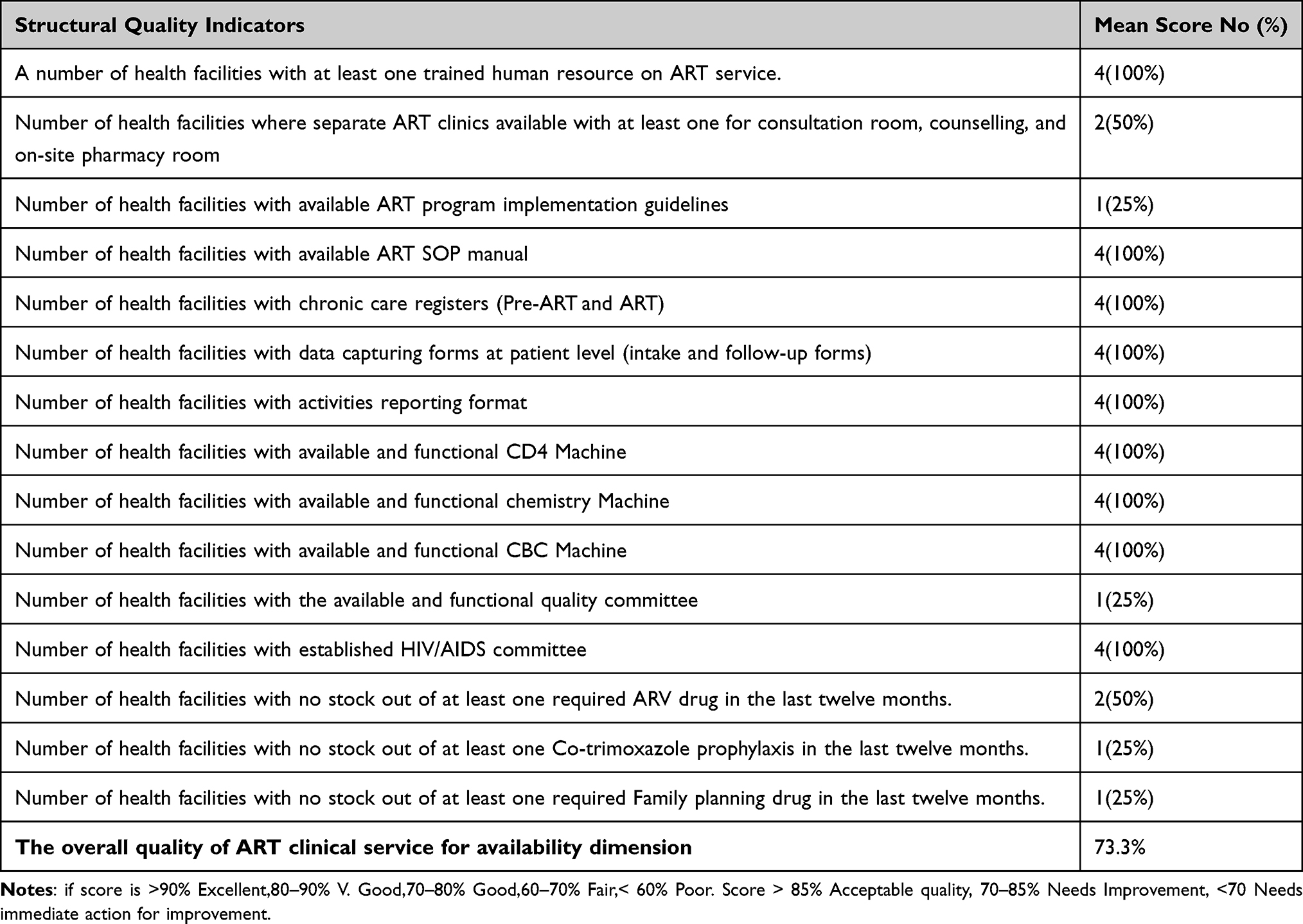 |
Table 2 Summary of the Structural Quality of ART Clinical Service in Selected Addis Ababa Public Hospitals, 2021 |
Compliance Dimension (Process Quality Indicators)
A total of 357 client folders who were enrolled and started ART were reviewed from four public hospitals providing the service. Of those clients 238 (66.7%) were women. The mean age of the clients was 44.2 (SD 9.6). One hundred nine were secondary (9–12) educated, 108 (30.3%), 68 (19%), 56 (15.7%),16 (4.5%) were elementary (1_8) school, college and above, unable to read and write, and 16 (4.5%) were only read and write respectively. The majority of the participants 149 (41.7%) were married and 103 (28.9%) were unemployed. The quality of ART clinical service in terms of HIV/AIDS service providers with the national standard was measured to be 79.5% which is good but needs improvement (Table 3).
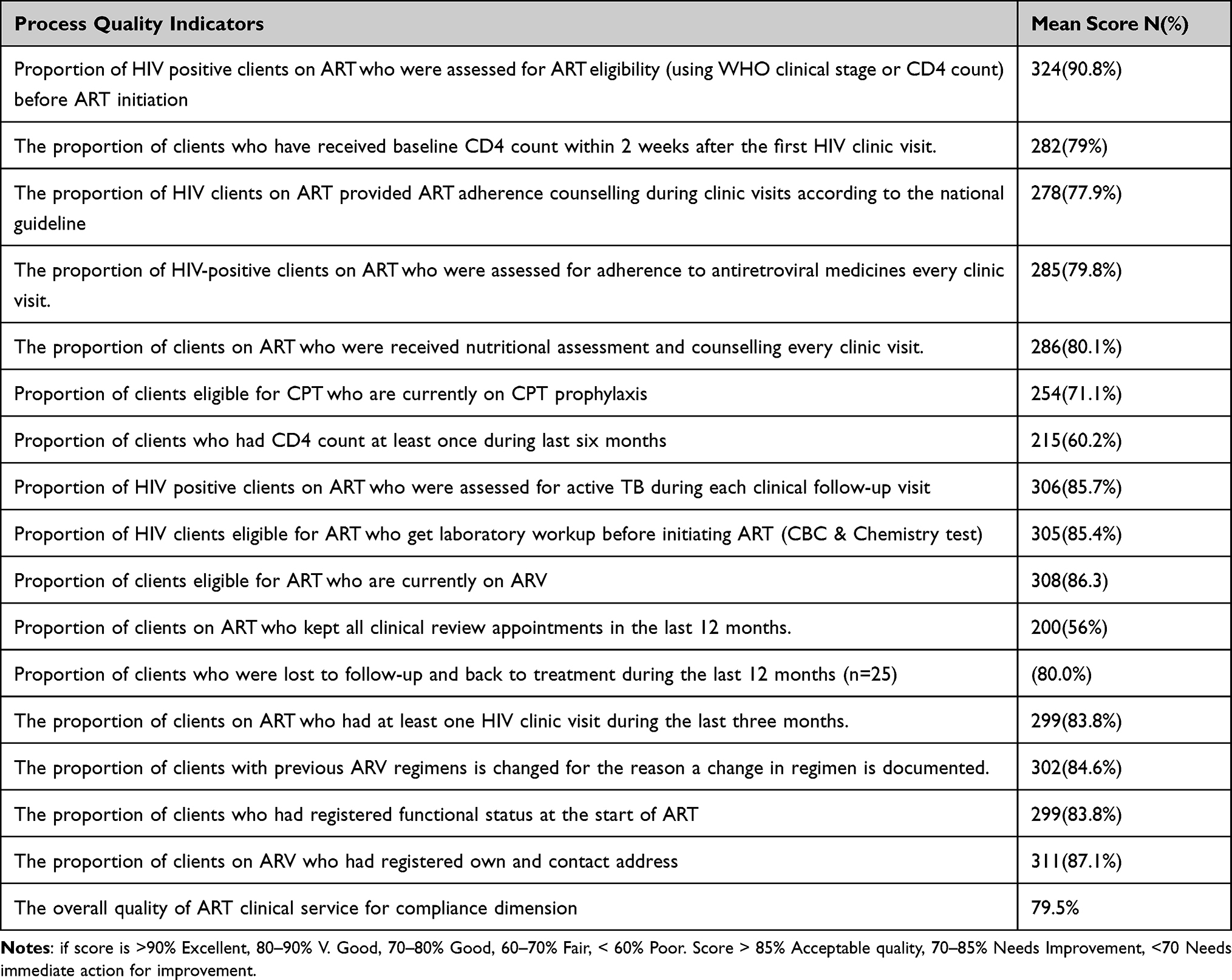 |
Table 3 Quality of ART Clinical Service with Compliance of Service Providers in Selected Addis Ababa Public Hospitals, 2021 (n=357) |
Client Satisfaction on Quality of HIV/AIDS Clinical Services
In total, 86.4% with CI (82.8%-89.6%) overall quality of HIV/AIDS clinical service in terms of client satisfaction could be explained by the Donabedian model was very good and acceptable quality (Table 4).
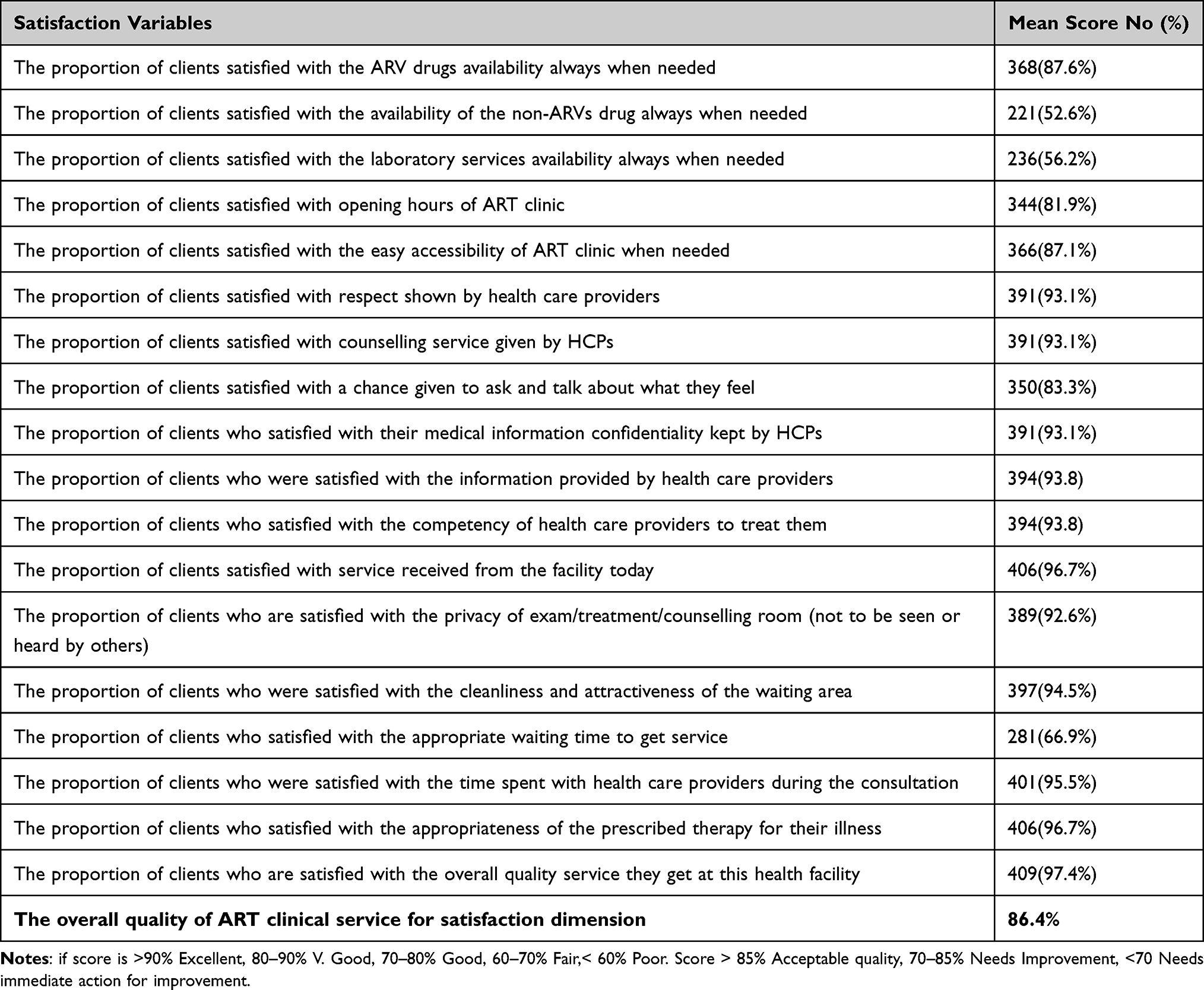 |
Table 4 Summary Clients Satisfaction (Outcome Quality) of ART Clinical Service in Selected Addis Ababa Public Hospitals, 2021 (n=420) |
Factors Associated with Client Satisfaction
Bivariate logistic regression analysis indicated that age category, education, occupation, patients who knew their partner’s HIV status, a patient who disclosed their HIV status, months of ART, and consultation time were variables that satisfied the assumption (p≤0.25) were considered as candidates for multivariate analysis. Multivariable logistic regression analysis indicated that Age, disclosure of HIV status, months of ART, and consultation time were associated with patient satisfaction with ART clinical services.
Patients who disclosed their HIV status were 10.7 times more likely to be satisfied when compared to those who were not disclosed [AOR 10.7, 95% CI: 5.2–22]. Patients who were on follow-up for 2 years and above were 10.4 times more likely to be satisfied compared to those on treatment for less than 2 years [AOR 10.4, 95% CI: 3.89–27.8]. Similarly, patients who received advice for more than 10 min were 3.5 times more likely to be satisfied when compared with those who received advice of less than 10 min [AOR 3.5, 95% CI: 1.6–7.35]. Study participants who belonged to the age groups of 34–44, 45–55, and 56–76 years were 5.1, 8.1, and 5 times more likely to be satisfied than those who were in the age group 23–33 years[AOR 5.1,95% CI:1.2–22, AOR 8.1,95% CI:1.9–35.5, AOR 5.0, 95% CI:2.97–9.44] respectively (Table 5).
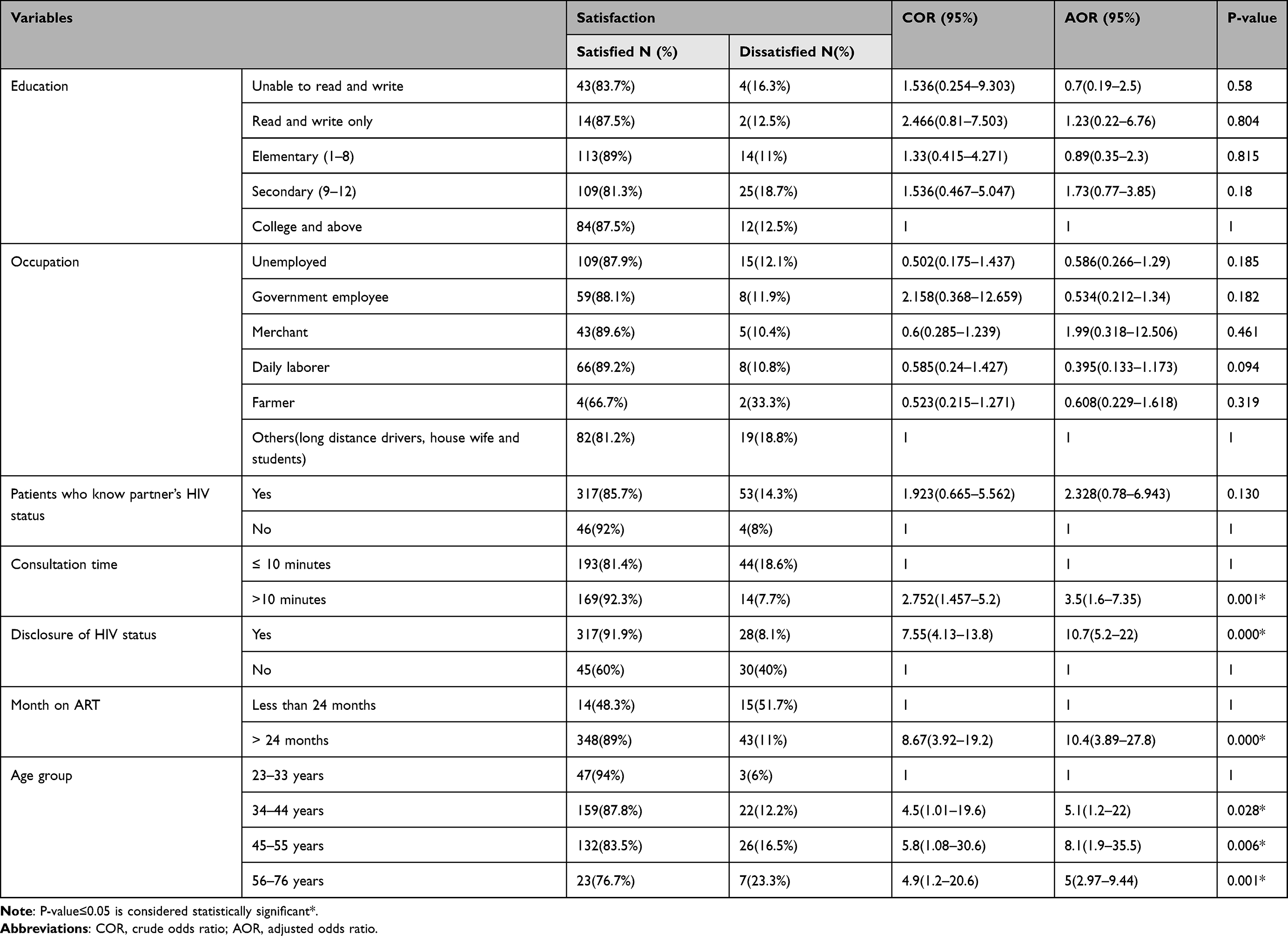 |
Table 5 Bivariate and Multivariate Analysis of Satisfaction Rate of Clients on the Overall Quality of ART Clinical Service in Selected Addis Ababa Public Hospitals, 2021 |
Qualitative Results (Key Informant Interview on Overall ART Clinical Service Quality)
The key informant interview results indicated space problems.
It is not possible to provide quality service without improving infrastructure. We are providing two or three patients in one room at the same time and difficult to maintain confidentiality and privacy for HIV positive people in our hospital. [Key informant 4, Key informant 5]
The overall process implementation of ART clinical service quality was measured in three dimensions and needs some improvement. The key informant interview indicated that service quality should be improved by integrating and mentioning quality improvement as routine work, availability of resources trained, and committed staff acting according to the guidelines and patient-centered care.
Quality should be improved if the availability of resources and health care provider compliance with the guideline and long consultation time to talk about their illness. [KI5, KI3, KI4, KI1]
Overall quality should be improved if there is the availability of all resources needed for HIV service, establishing functional quality improvement committee, and integration and minimization of many and bulky registers. [KI1, KI3]
Integration of Results
Qualitative data from key informant interviews and quantitative results show the quality of ART clinical service in terms of program resource availability (structure) and quality of ART clinical service in terms of HIV/AIDS service providers with the national standard(process) needs improvement. The overall quality of HIV/AIDS clinical service in terms of outcome (client satisfaction) was very good and acceptable.
Discussions
This study focused on the quality of ART clinical service program implementation in selected public Addis Ababa Hospitals. The researcher used Donabedian’s structure–process–outcome model of ART health care quality examining health services and evaluating the quality of health care. According to the model, information about the quality of care can be drawn from three categories: structure describing the context in which care is delivered, including hospital buildings, staff, financing, and equipment, process denotes the transactions between patients and providers throughout the delivery of healthcare and, outcomes refer to the effects of healthcare on the health status of patients and populations.
The overall quality of ART clinical service was 73.3% for the(structure) availability of resources, 79.5% for(process) healthcare providers’ compliance with the national guidelines, and 86.4% for client satisfaction. Of course, the donabedian model has limitations of linear sequential progression from structure to process to the outcome and how the three domains influence and interact with each other, the finding indicates that the overall quality of ART clinical services requires improvement in structural and process quality measures.
The findings of this study indicated that not all facilities met the minimum standard set by the Federal Ministry of Health for facilities designed to provide ART clinical services. Non-availability of resources, stock of some 2nd line antiretroviral drugs, and family planning drugs have been reported.
In this study, the compliance of health care providers with guidelines needs improvement. A significant proportion of clients did not receive the important components of care recommended by the national guidelines.
This study revealed that the overall level of client satisfaction with the quality of ART clinical services was 86.4%, which is an acceptable quality because of the good availability of resources and compliance of health care providers. These findings are lower than those reported in the Tigray regional state, where the overall satisfaction level of 89.6%20 and a similar study was done in Cameroon Bamenda Regional Hospital overall satisfaction with HIV services was 91.2%.21 Problems in the availability, infrastructure, and shortage of trained human power might be a reason for the lower satisfaction levels in this study. This was higher than the report of a study conducted in Midre-genet Hospital Tigray, Northern Ethiopia, which reported patient satisfaction to be 75.2%,22 Hossana town, Southern Ethiopia 70.10%,6 a study conducted in Gondar Town Health Center, Northwest Ethiopia, 75.4%,23 a study done in Debre Berhan Referral Hospital, North Shoa, 57.7%24 and a study conducted in Mizan-Tepi University Teaching Hospital, Southwest Ethiopia, 55.2%25 patients satisfied with HIV and AIDS services. This may be due to efforts made to improve the service delivery process, availability, and compliance of health professionals to the standard guidelines. This finding is also supported by an in-depth interview with health providers that improved the service delivery process compared to previous years, especially on the availability of ART drugs and supplies, welcoming, respect, close relationship given to ART clients, and the separation of ART clinics from the hospital which has increased their privacy.
This study revealed that clients who disclosed their HIV status to their parents were 10.7 times more satisfied with ART services compared to clients who did not disclose. This is in line with a study conducted in Hossana Town that disclosed their HIV status was associated with satisfaction with HIV and AIDS.6 This might be because respondents who disclosed their HIV status received more family support and did not shame taking their ART drug at any time and family remind taking the drug at the prescribed time.
Patients who had been advised 10 min and above were 3.5 times more satisfied than those who were advised for less than 10 min in this study. This is similar to a study from the Mizan-Tepi University Teaching Hospital, Southwest Ethiopia, which showed that a consultation time of 10 minutes or more was associated with a high satisfaction score.25 This might be due to the patient, physician discussing the disease and treatment, taking enough time to adherence counselling, and different issues would be clarified for the patient.
Patients who take medication 2 years and above were 10.4 times more satisfied than those who take less than 2 years. This might be patients taking treatment for more than 2 years may adopt the clinical service environment and know the more services provided. Patients who were older than 34 years were associated with satisfaction with ART services compared to younger ones. This is similar to a study conducted in Midre-genet Hospital Tigray and Gondar Town Health Center.22,23 This could be due to age increases, social interactions, and interpersonal relationships among clients and health providers increased, emotionally and psychologically stable, and satisfied with ART services provided.
Strengths of the Study
This research used three dimensions to determine the quality of ART clinical service implementation which makes it more valid than measuring the process by a single dimension. Using mixed methods of data collection method helped us get accurate and detailed results.
Limitations of the Study
Limitation of the study: In the case of client satisfaction, the study design was a cross-sectional study and therefore it does not show a causal relationship. The researcher used five points Likert scale, this may not precisely be told us to say so. The improper registration of all of the services delivered was an additional limitation for the assessment of health care providers’ compliance.
Conclusion
The overall quality of ART service was good, although with the availability of resources and compliance health care provider needs improvement. All resources recommended by the national antiretroviral therapy implementation guideline including separated counselling room, some second-line drugs were not continuously available. Compliance of health care providers with standard guidelines needs improvement. The overall quality of ART service in terms of client satisfaction was 86.4% explained by the Donabedian model which is good. Patients who disclose their HIV status, months of ART, age, and consultation time were factors associated with client satisfaction.
Recommendation
Based on these findings observed from this study the following recommendations were drawn.
For FMOH, AARHB for Non-Governmental Organizations (ICAP, CDC …)
An expert from higher bodies should provide regular supportive supervision for the respective hospitals. Program resources should be consistently available and supplied for the facilities. The sustainability of quality ART service should strengthen.
For Hospitals
Necessary infrastructures should be constructed like a separate clinic with adequate rooms as per the guidelines. Pharmaceuticals and medical supplies systems should be strengthened and continuous monitoring and performance measurement should be in place to see the performance whether is based on a national guideline or not.
For Program Managers
A functional quality team should be established in the clinic, integration, and maintenance of quality as routine care. On-job training and orientation on quality improvement and providers’ compliance with the guidelines.
For Health Care Providers
The health care provider should adhere to the standard guideline. Patient-provider interaction and discussion about the care provided should be strengthened. More time should give to clients during the consultation time. Health care providers work on strengthening the younger age service satisfaction, helping in disclosure of HIV status.
Abbreviations
ART, Antiretroviral Therapy; ARV, Antiretroviral; BSc, Bachelor of Science; CD4, Cluster of differentiation 4; CDC, Communicable Disease Control; CPT, Co-trimoxazole Preventive Therapy; CTX, Co-trimoxazole prophylaxis; EDHS, Ethiopian Demographic and Health Survey; ELISA, Enzyme-Linked Immunosorbent Assay; FHAPCO, Federal HIV/AIDS Prevention and Control Office; HAART, Highly Active Antiretroviral Therapy; HIV, Human Immunodeficiency Virus; IOs, Opportunistic Infections; FMOH, Federal Ministry of Health; PMTCT, Prevention of Mother to Child Transmission; SPSS, Statistical Package for Social Science; TB, Tuberculosis; UNAIDS, Joint United Nations Program on HIV/AIDS; WHO, World Health Organization.
Acknowledgments
First, I would like to thank almighty God. Next, Kotebe Metropolitan University Menelik II Medical and Health Science College, My thanks go to my advisor for the fastest response and Guidance as well as valuable comments and criticism throughout the process of this research. Our appreciation also goes to the data collectors and supervisors for their unreserved contribution.
Besides, I would like to thank all staff members working at Alert Hospital, Zewditu Hospital, Yekatit 12 Hospital, and St Peter Hospital for their cooperativeness. Last, but not least, my deepest gratitude goes to my family for giving me constructive ideas, encouragement, and motivation during my studies.
Author Contributions
All authors made substantial contributions to the work reported in the conception and design, execution, acquisition of data, or analysis and interpretation of data; took part in drafting the article, revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared that have no competing interests in this work.
References
1. UNAIDS. The Global HIV/AIDS Epidemic; 2019.
2. UNAIDS. HIV and AIDS Estimates of Ethiopia; 2019.
3. WHO. HIV/AIDS Fact Sheets; 2020.
4. Aldomoro Burua1 FNaPW. Adherence to standards of quality HIV/AIDS care and antiretroviral therapy in the West Nile Region of Uganda. BMC Health Serv Res. 2014;14:521.
5. FMoH. National HIV Service Quality Improvement Tool Kit. 2018:9
6. Doyore F, Moges B. Client satisfaction to antiretroviral treatment services and associated factors among clients attending ART clinics in Hossana town, southern Ethiopia. Clin Res. 2016;2(6):6.
7. Eshetu A, Gobena T, Mengeste B, Semahegn A. Quality of Clinical Care for People Living With HIV/AIDS in Dil Chora Referral Hospital, Dire Dawa, East Ethiopia. Pharma Innovation. 2013;2(9, Part A):1.
8. Li L, Comulada WS, Lin C, Lan C-W, Cao X, Wu Z. Report on the provider–Client interaction from 68 methadone maintenance clinics in China. Health Commun. 2017;32(11):1368–1375. doi:10.1080/10410236.2016.1221754
9. Hailemeskal MB, Sereda Y, Latypov A, Kiriazova T, Avaliani N. Perceived quality of HIV care and client satisfaction across different service providers in Ukraine. Eur J Public Health. 2020;30(1):23–30. doi:10.1093/eurpub/ckz124
10. FMOH. The Federal Democratic Republic of Ethiopia, Health Sector Transformation Plan. Addis Abeba: Ministry of health; 2015.
11. Donabedian AJJ. The quality of care: how can it be assessed? JAMA. 1988;260(12):1743–1748. doi:10.1001/jama.260.12.1743
12. Mitchell PH, Ferketich S, Jennings BM. Scholarship AAoNEPoQHCJITJoN. Quality Health Outcomes Model. 1998;30(1):43–46.
13. Carayon P, Hundt AS, Karsh B, et al. Work system design for patient safety: the SEIPS model. Quality & Safety in Health Care. 2006;15(suppl 1):i50–i8. doi:10.1136/qshc.2005.015842
14. Donabedian A. “The Definition of Quality and Approaches to Its Assessment. Explorations in Quality Assessment and Monitoring. Ann Arbor, Michigan: Health Administration Press; 1980.
15. Ishtiaq M. Book Review Creswell, JW (2014). Research Design. 2019;12(5):40.
16. Eshetu A, Gobena T, Mengeste B, Semahegn A. Quality of Clinical Care for People Living With HIV/AIDS in Dil Chora Referral Hospital, Dire Dawa, East Ethiopia. Pharma Innovation. 2013;2(9, Part A):1.
17. Pearce NDaM. HQIP Guide to Ensuring Data Quality in Clinical Audits; 2011.
18. Adane S, Adane MM. Assessment of antiretroviral treatment (ART) cares service provision in Tigray Region health centres, North Ethiopia. BMC Health Serv Res. 2015;15:368. doi:10.1186/s12913-015-1032-8
19. Sullivan GM, Artino AR. Analyzing and interpreting data from Likert-type scales. J Grad Med Educ. 2013;5(4):541. doi:10.4300/JGME-5-4-18
20. Tessema SB, Adane MM. Assessment of antiretroviral treatment (ART) cares service provision in Tigray Region health centres, North Ethiopia. BMC Health Serv Res. 2015;15(1):368.
21. Wung BA, Peter NF, Atashili J. Clients’ satisfaction with HIV treatment services in Bamenda, Cameroon: a cross-sectional study. BMC Health Serv Res. 2016;16(1):1–9. doi:10.1186/s12913-016-1512-5
22. Atsebeha KG, Chercos DH. High antiretroviral therapy service delivery satisfaction and its’ associated factors at Midre-genet hospital; Northwest Tigray, Ethiopia. BMC Health Serv Res. 2018;18(1):1–9. doi:10.1186/s12913-018-3055-4
23. Adissu G, Biks GA, Tamirat KS. Patient satisfaction with antiretroviral therapy services and associated factors at Gondar town health centres, Northwest Ethiopia: an institution-based cross-sectional study. BMC Health Serv Res. 2020;20(1):93. doi:10.1186/s12913-020-4934-z
24. Mezemir R, Getachew D, Gebrselassie M. Patients’ satisfaction and its determinants in outpatient Department of Deberebirhan Referral Hospital, North Shoa, Ethiopia. Int J Econ Manag Sci. 2014;3(191):2. doi:10.4172/2162-6359.1000191
25. Nigussie T, Aferu T, Mamo Y, Feyisa M. Patient Satisfaction with HIV and AIDS Services in Mizan-Tepi University Teaching Hospital, Southwest Ethiopia. HIV/AIDS. 2020;12:403.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.