Back to Journals » Infection and Drug Resistance » Volume 15
Antimicrobial Susceptibility Trends Among Gram-Negative Bacilli Causing Bloodstream Infections: Results from the China Antimicrobial Resistance Surveillance Trial (CARST) Program, 2011–2020
Authors Yan M ![]() , Zheng B, Li Y, Lv Y
, Zheng B, Li Y, Lv Y
Received 24 January 2022
Accepted for publication 26 March 2022
Published 29 April 2022 Volume 2022:15 Pages 2325—2337
DOI https://doi.org/10.2147/IDR.S358788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Mengyao Yan, Bo Zheng, Yun Li, Yuan Lv
Institute of Clinical Pharmacology, Peking University First Hospital, Beijing, People’s Republic of China
Correspondence: Yun Li; Yuan Lv, Institute of Clinical Pharmacology, Peking University First Hospital, Xueyuan Road 38, Haidian District, Beijing, 100191, People’s Republic of China, Tel +86-10-82802315, Fax +86-10-62072817, Email [email protected]; [email protected]
Purpose: The antimicrobial resistance profiles of gram-negative bacilli causing bloodstream infections have changed over time, while comprehensive and real-time surveillance data are limited in China. This study aimed to review the antimicrobial susceptibility trends among main gram-negative bacilli isolated from blood specimens in China.
Methods: From 2011 to 2020, a total of 4352 non-duplicate isolates were collected from 21 tertiary hospitals in 18 provinces or cities across China. Antimicrobial susceptibility testing was conducted by the agar dilution method recommended by the Clinical and Laboratory Standards Institute (CLSI), and the results were interpreted using CLSI criteria.
Results: During this 10-year surveillance period, meropenem and imipenem were the most effective agents against Escherichia coli (resistance remaining < 5%). The proportion of ESBL-producing isolates in carbapenem-susceptible E. coli displayed a decreasing trend (from 72.9% to 51.2%). The resistance rates of Klebsiella pneumoniae to meropenem and imipenem increased from 3.3% and 1.6% in the 2011– 12 period to 15.0% and 15.4% in the 2019– 20 period, respectively. Carbapenems and amikacin were the most active agents against Enterobacter cloacae. The resistance rates of Pseudomonas aeruginosa to meropenem and imipenem increased from 13.1% and 17.7% in the 2015– 16 period to 24.5% and 21.0% in the 2019– 20 period, respectively. Few agents showed activity against Acinetobacter baumannii. The frequency of imipenem-non-susceptible A. baumannii remained stable (remaining ∼ 70%).
Conclusion: The rapid spread of carbapenem-resistant K. pneumoniae has been serious in recent years. Conversely, the prevalence of ESBL-producing isolates was decreased. Carbapenems are still effective against gram-negative bacilli causing BSIs, except for A. baumannii. More attention should be given to A. baumannii, considering its high resistance against different classes of antimicrobials.
Keywords: Enterobacterales, P. aeruginosa, A. baumannii, ESBL, carbapenem-resistance
Introduction
Bloodstream infection (BSI) is one of the most common infectious diseases in hospital practice. It can progress to sepsis due to patient- or pathogen-related factors,1,2 which is associated with extended hospitalization, significant health-care costs, and an increase in mortality.3,4 Although the spectrum of pathogens causing BSIs is everchanging and varies from region to region, the importance of gram-negative bacilli has increased substantially in recent years.4,5 The initial antimicrobial options to treat BSIs are driven mainly by an understanding of these pathogens.
Globally, the rapid spread of antimicrobial resistance among gram-negative bacilli has become a serious threat to public health. To deal with this challenge, broad-spectrum antimicrobials such as third-generation cephalosporins and carbapenems have been overprescribed repeatedly, leading to a vicious cycle with further accumulation of selective resistance profiles.6,7 Patients who develop BSIs caused by extended-spectrum β-lactamase [ESBL]-producing Enterobacteriaceae, carbapenem-resistant Enterobacteriaceae, carbapenem-resistant Pseudomonas aeruginosa and Acinetobacter baumannii, have limited therapeutic options.8,9 Several studies have demonstrated that these pathogens were the main reasons for the high mortality in BSI.5,10,11 To understand the extent of the resistance problem and thus stem the tide of BSIs, continuously monitoring trends in antimicrobial resistance among BSI pathogens is of great importance.
The national surveillance program of China Antimicrobial Resistance Surveillance Trial (CARST) was established by the Institute of Clinical Pharmacology, Peking University, to monitor the antimicrobial activities of broad-spectrum agents and the antimicrobial resistance trends among clinical isolates in China. Currently, there are 20 tertiary teaching hospitals from 18 major cities throughout China selected as CARST monitoring sites. These hospitals were representative of nationwide circumstances, based on geographical distribution, medical skill, and the development level of microbiological diagnostic techniques.12 We previously reported the antimicrobial resistance trends in Enterobacteriaceae isolated from blood in 2004 to 2014 and bacterial susceptibility in bloodstream infections in 2015–2016.13,14 In this study, we report on the antimicrobial susceptibility trends among main gram-negative bacilli isolated from blood specimens from the CARST program between 2011 and 2020.
Materials and Methods
Antimicrobial Agents
Meropenem was purchased from Sumitomo Pharmaceuticals Co., Ltd. (Suzhou, China); imipenem and ertapenem were from Merck and Co., Inc. (Elkton, VA, USA); ampicillin was from INALCO Company (Milan, Italy); piperacillin was from TargetMol Company (Boston, MA, USA); cefepime was from Bristol-Myers Squibb (Shanghai, China); aztreonam was from Shanghai SPH New ASIA Pharmaceutical Co., Ltd. (Shanghai, China); ciprofloxacin was purchased from Shangyu Jingxin Pharmaceutical Co., Ltd. (Hangzhou, Beijing); colistin was from Sigma-Aldrich (Saint Louis, MO, USA); sulbactam was from Guangzhou Baiyunshan Pharmaceutical Co., Ltd. (Guangzhou, China); all other antibiotics were from the National Institute for Food and Drug Control (Beijing, China). Tazobactam was tested in combination with piperacillin at a fixed concentration of 4 µg/mL. Ampicillin-sulbactam were tested in a ratio of 2:1. Cefoperazone-sulbactam were in a ratio of 2:1.
Bacterial Isolates
A total of 4352 non-duplicate BSI isolates, including Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae, P. aeruginosa and A. baumannii, were collected from 21 tertiary hospitals (18 in 2011–12; 19 in 2013–14; 18 in 2015–16; 20 in 2017–18; and 20 in 2019–20, with one or two hospitals added or removed from surveillance during the study period) in 18 provinces or cities across China in 2011 to 2020 as part of the CARST program. All isolates were collected biennially by the CARST program over five consecutive 2-year periods (2011–12; 2013–14; 2015–16; 2017–18; and 2019–20) and were sent to a central laboratory (Institute of Clinical Pharmacology, Peking University First Hospital). All bacteria were isolated from the blood samples of patients. Species were identified by the Analytical Profile Index system (API 20E, 20NE [bioMérieux]).
Antimicrobial Susceptibility Testing
MICs were determined by the agar dilution method, with the exception of colistin, which was determined by the broth microdilution method.15 The interpretative breakpoint criteria were in accordance with those recommended by the Clinical and Laboratory Standards Institute (CLSI) guidelines.16 Bacterial suspensions were obtained by inoculation with 104 CFU of each bacterium via a multipoint inoculator. Disc diffusion was performed to identify ESBL-producing isolates among E. coli and K. pneumoniae, as recommended by CLSI.16 If the cefotaxime (30 μg) zone was ≤27 mm or the ceftazidime (30 μg) zone ≤22 mm, ESBL production was defined as a ≥5 mm increase in a zone diameter for cefotaxime (30 μg) or ceftazidime (30 μg) tested in combination with clavulanic acid (10 μg) compared to the zone diameter of the agent when tested alone. Isolates of P. aeruginosa and A. baumannii were classified as imipenem-susceptible (IPM-S, MIC ≤2 µg/mL) and imipenem-non-susceptible (IPM-NS, MIC >2 µg/mL). E. coli ATCC (American Type Culture Collection) 25922, K. pneumoniae ATCC 700603, and P. aeruginosa ATCC 27853 were used as quality control reference strains.
Data Analysis
All data, including patient and microbiological information, were analyzed using Statistical Package for the Social Sciences 26.0 software (SPSS, Inc., Chicago, IL, USA).
Results
Distribution of Isolates
Among the 4352 BSI gram-negative bacilli collected from 2011 to 2020, the most common pathogens overall were E. coli (1655), followed by K. pneumoniae (1074), A. baumannii (723), P. aeruginosa (622) and E. cloacae (278). The majority of isolates came from non-intensive care patients (E. coli, 88.3%; K. pneumoniae, 79.9%; E. cloacae, 82.7%; P. aeruginosa, 77.2%; and A. baumannii, 50.1%).
Changes in Antimicrobial Susceptibility of E. coli
During the 10-year study period, the susceptibility profiles for E. coli remained stable for most antibiotic agents (Table 1). Carbapenems and amikacin were still the most effective agents against E. coli (susceptibility remaining >95%). From 2011–12 to 2019–20, the MIC50 and MIC90 values of carbapenems against E. coli all varied within ± one 2-fold dilution step. Although the susceptibilities of meropenem (97.0% susceptible) and imipenem (97.0% susceptible) in the 2019–20 period showed slight declines compared to previous study periods, both agents displayed superior in vitro activities. β-Lactam combination agents, including piperacillin-tazobactam and cefoperazone-sulbactam, were also active agents, against which 88.3–92.3% and 75.0–80.6% of E. coli, were susceptible, respectively. Although the susceptibility rate has been increasing over time, the sensitivity of E. coli to third-generation cephalosporins, aztreonam and gentamicin remained low. The susceptibility rates to ceftazidime were much higher than those to cefotaxime and ceftriaxone. The proportion of ESBL-producing isolates in carbapenem-susceptible E. coli displayed a discernible decreasing trend overall and in different regions of China during the surveillance period (overall from 72.9% in 2011–12 to 51.2% in 2019–20) (Figure 1A). As expected, the susceptibility rates of ESBL-producing E. coli to meropenem and imipenem were both ~100% during the study period.
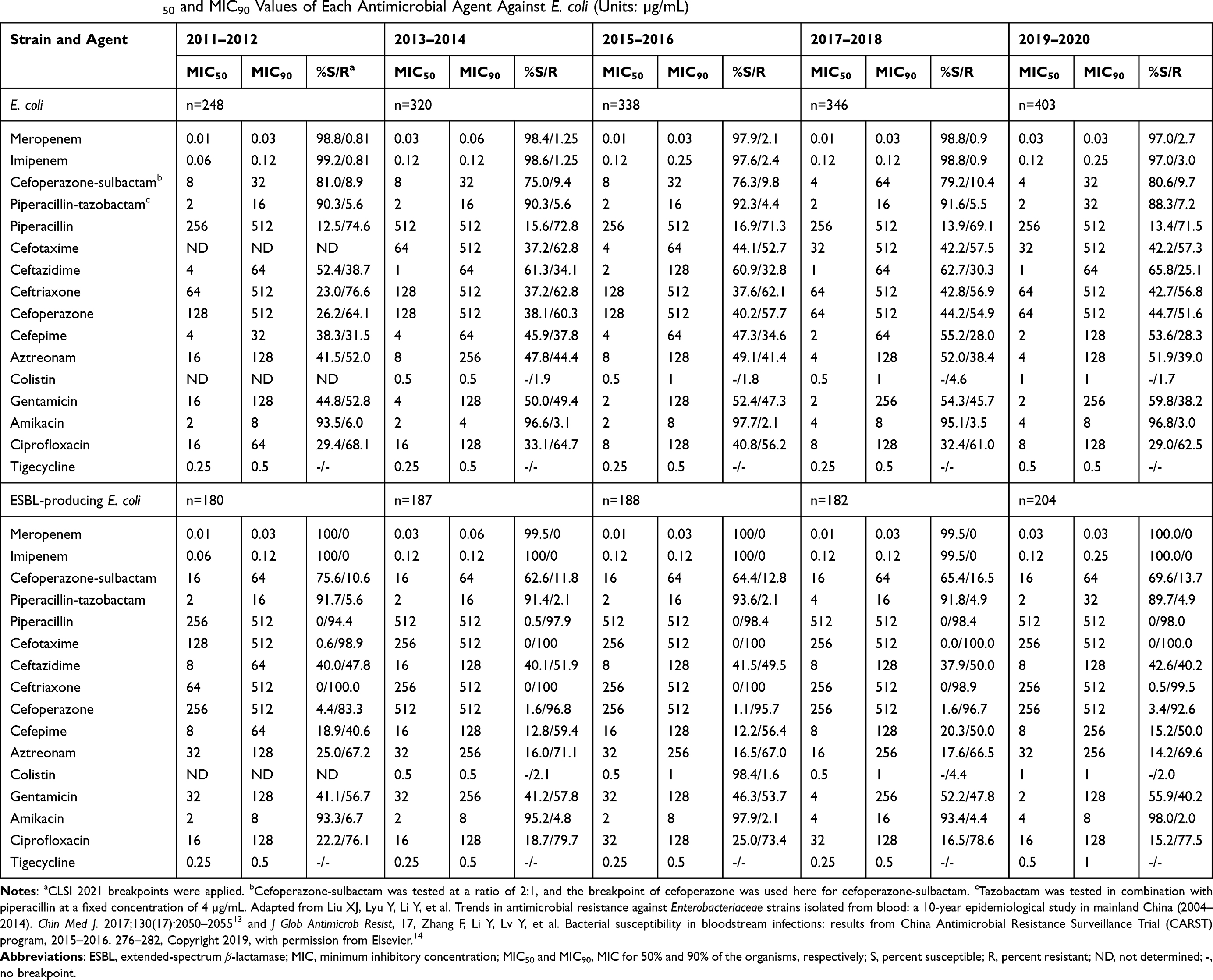 |
Table 1 Change in MIC50 and MIC90 Values of Each Antimicrobial Agent Against E. coli (Units: µg/mL) |
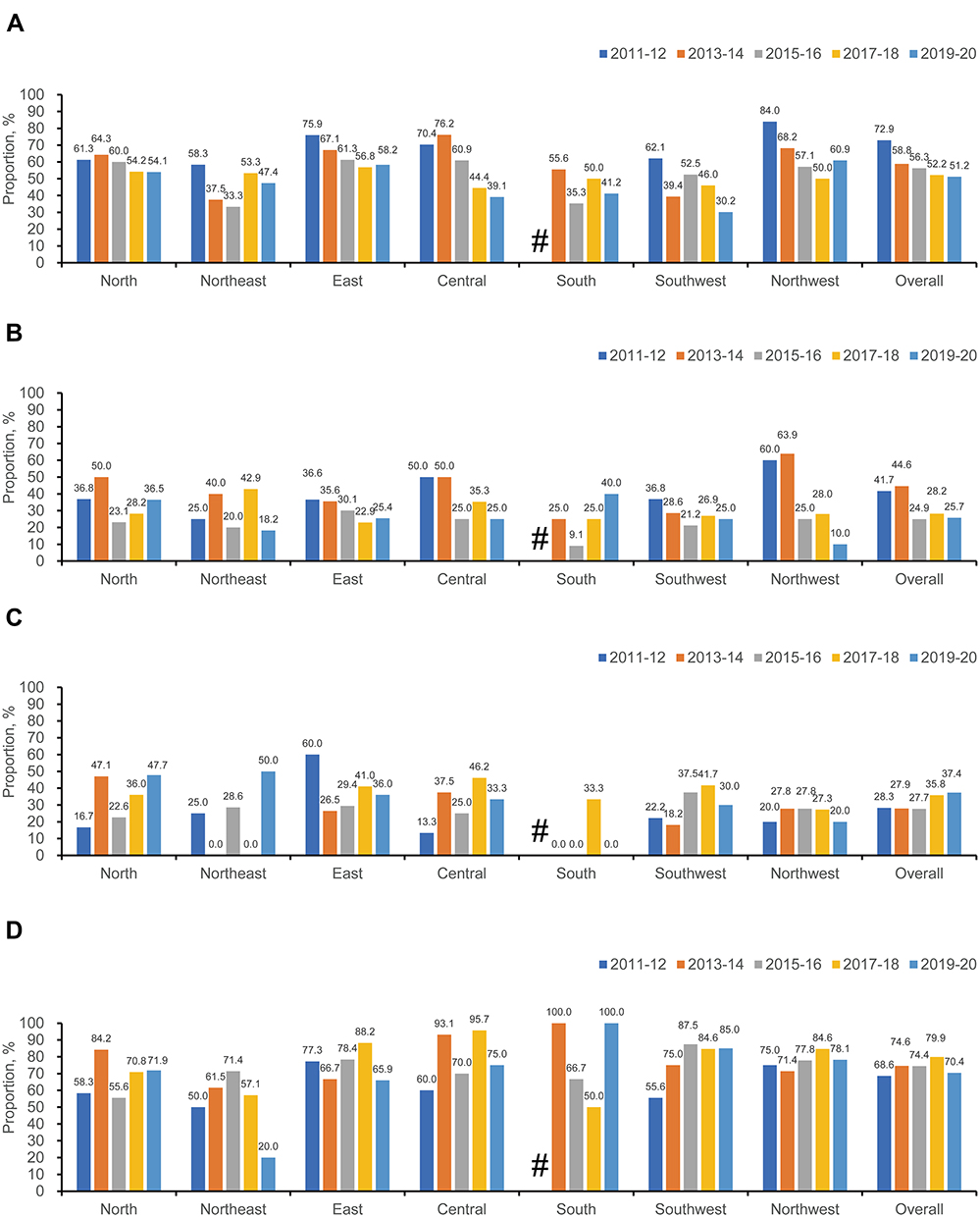 |
Figure 1 Changes over time in the prevalence of ESBL-producing EC in CSEC (A), ESBL-producing KP in CSKP (B), Imipenem-NS PA (C) and Imipenem-NS AB (D) overall and in different regions of China (2011–2020). Abbreviations: ESBL, extended-spectrum β-lactamase; EC, Escherichia coli; CSEC, carbapenem-susceptible Escherichia coli; KP, Klebsiella pneumoniae; CSKP, carbapenem-susceptible Klebsiella pneumoniae; Imipenem-NS, imipenem-non-susceptible; PA, Pseudomonas aeruginosa; AB, Acinetobacter baumannii. Notes: #Means that data in South China in the 2011–12 period were not available. |
Changes in Antimicrobial Susceptibility of K. pneumoniae
The susceptibility profiles of K. pneumoniae were similar to those of E. coli (Table 2). Carbapenems and amikacin were the most active agents against K. pneumoniae. However, the susceptibility rates of K. pneumoniae to meropenem and imipenem decreased from 96.7% and 98.4% in the 2011–12 period to 84.6% and 84.6% in the2019–20 period, respectively. The sensitivity of K. pneumoniae to piperacillin-tazobactam was slightly higher than that to cefoperazone-sulbactam. The susceptibility rates to third-generation cephalosporins, aztreonam, gentamicin and ciprofloxacin fluctuated slightly and were low. An ESBL phenotype was less frequently observed in K. pneumoniae than in E. coli. The nationwide proportion of ESBL-producing isolates in carbapenem-susceptible K. pneumoniae during the study period fluctuated around 24.9% and 44.6%, but overall displayed a decreasing tendency (Figure 1B). The proportion of ESBL-producing isolates in carbapenem-susceptible K. pneumoniae decreased in all regions of China from 2011 to 2016, and fluctuated differently thereafter (Figure 1B). The susceptibility rates of ESBL-producing K. pneumoniae to meropenem and imipenem were both ~95% from 2011 to 2018; however, the susceptibility rates both decreased to ~85% in the last surveillance period.
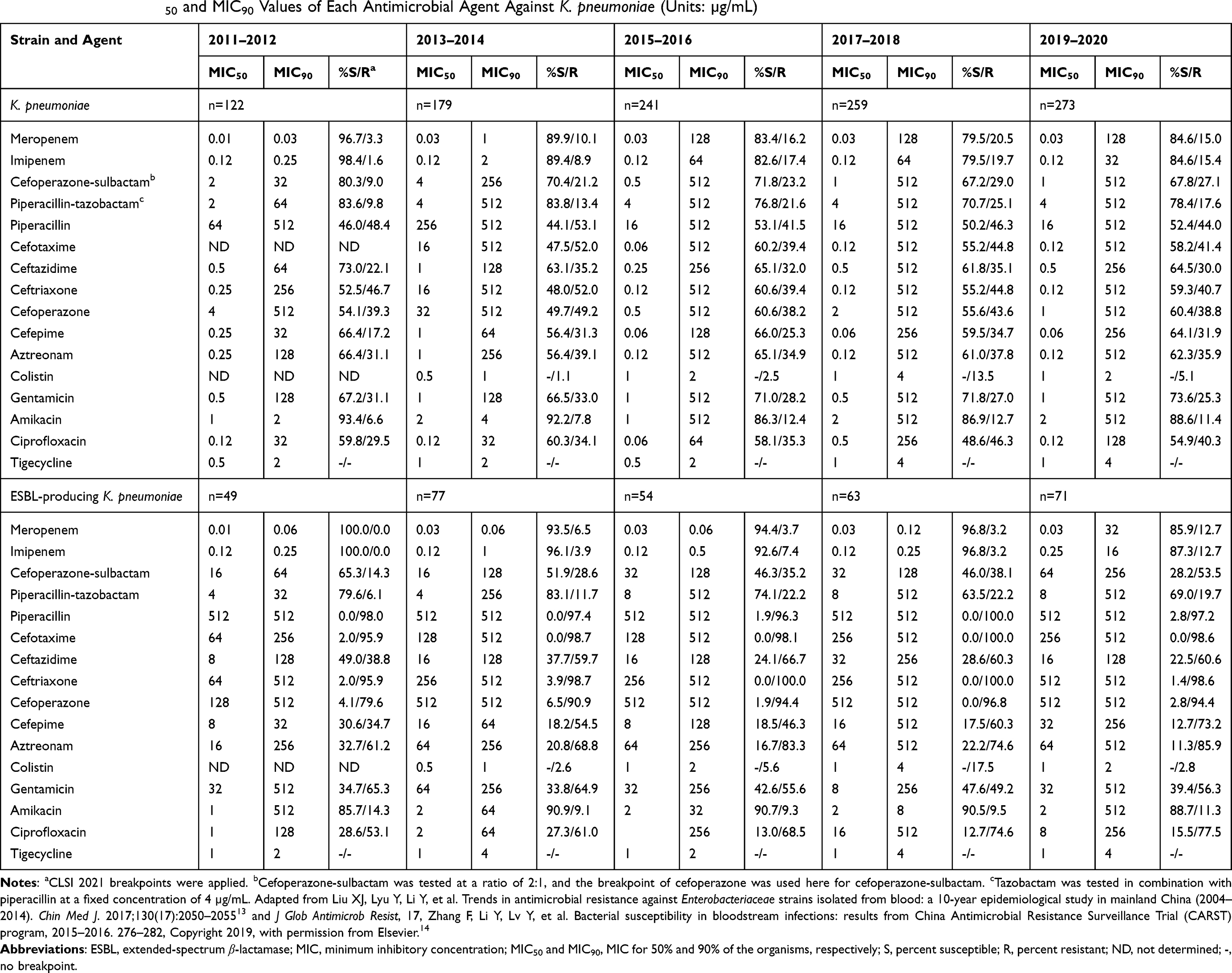 |
Table 2 Change in MIC50 and MIC90 Values of Each Antimicrobial Agent Against K. pneumoniae (Units: µg/mL) |
Changes in Antimicrobial Susceptibility of E. cloacae
Carbapenems and amikacin were the most active agents against E. cloacae (Table 3). Susceptibility rates of E. cloacae to meropenem and imipenem were higher than those to ertapenem. The sensitivity to piperacillin-tazobactam was similar to that to cefoperazone-sulbactam. The susceptibility rates to piperacillin, third-generation cephalosporins and aztreonam were always low, while sensitivity to cefepime was much higher than that to third-generation cephalosporins. The sensitivity of E. cloacae to gentamicin (susceptibility remaining >85% from 2013 to 2020) was higher than those of E. coli and K. pneumoniae.
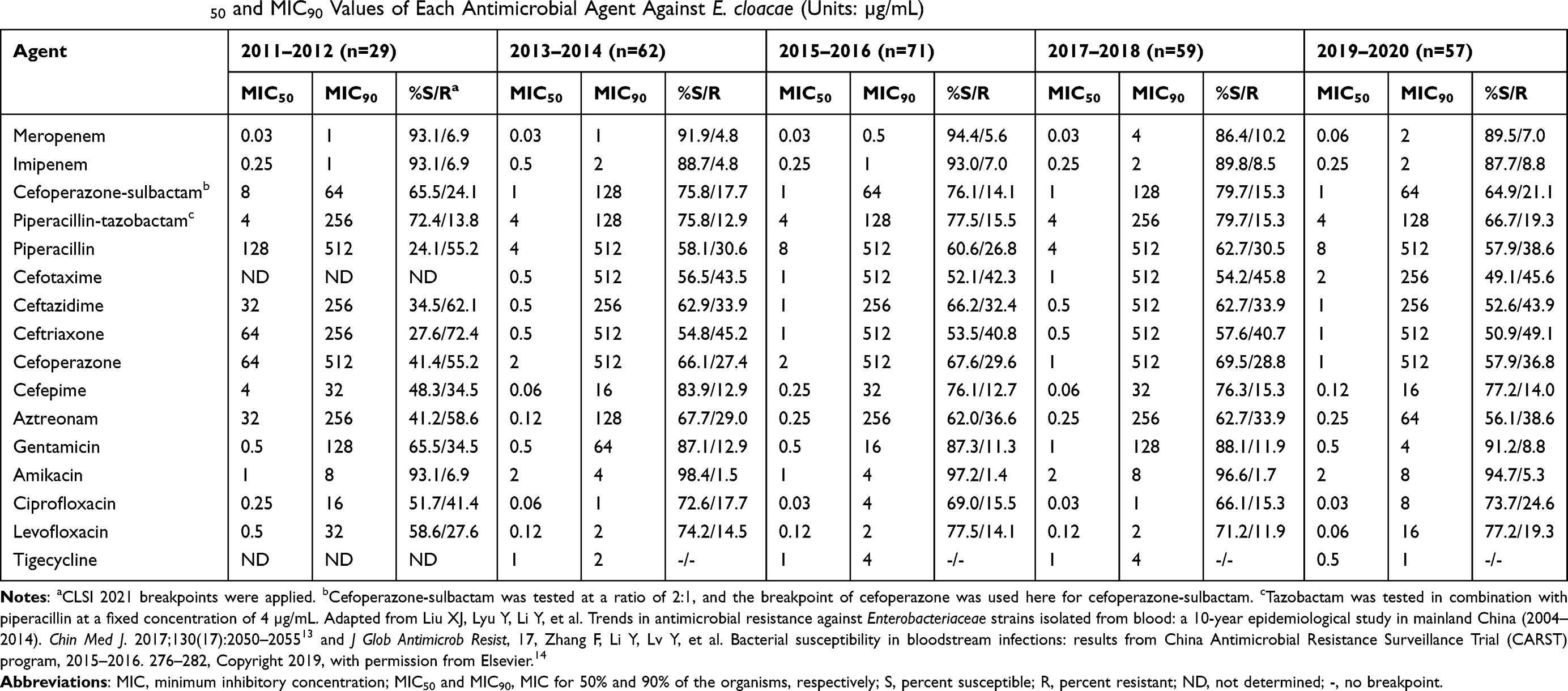 |
Table 3 Change in MIC50 and MIC90 Values of Each Antimicrobial Agent Against E. cloacae (Units: µg/mL) |
Changes in Antimicrobial Susceptibility of P. aeruginosa
The susceptibility rates of P. aeruginosa to meropenem and imipenem decreased from 80.8% and 72.3% in the 2015–16 period to 69.7% and 62.6% in the 2019–20 period, respectively (Table 4). A similar trend was observed in the sensitivity of P. aeruginosa to piperacillin-tazobactam (susceptibility rate from 80.0% in 2015–16 to 73.5% in 2019–20) and cefoperazone-sulbactam (susceptibility rate from 80.8% in 2015–16 to 68.4% in 2019–20). Ceftazidime and cefepime maintained high activities against P. aeruginosa, with >70% of isolates being susceptible over the study period. The susceptibility rates to amikacin were higher than those to gentamicin. The overall IPM-NS P. aeruginosa frequency increased during the study period, and the greatest increase occurred between the 2015–16 period and 2017–18 period, with the frequency increased from 27.7% in the 2015–16 period to 35.8% in the 2017–18 period (Figure 1C). Trends in the prevalence of IPM-NS P. aeruginosa varied widely among different regions of China from 2011 to 2020 (Figure 1C). During the surveillance period, a marked increase was observed in the sensitivity of IPM-NS P. aeruginosa to amikacin (54.5% susceptible in the 2011–12 period; 91.4% susceptible in the 2019–20 period).
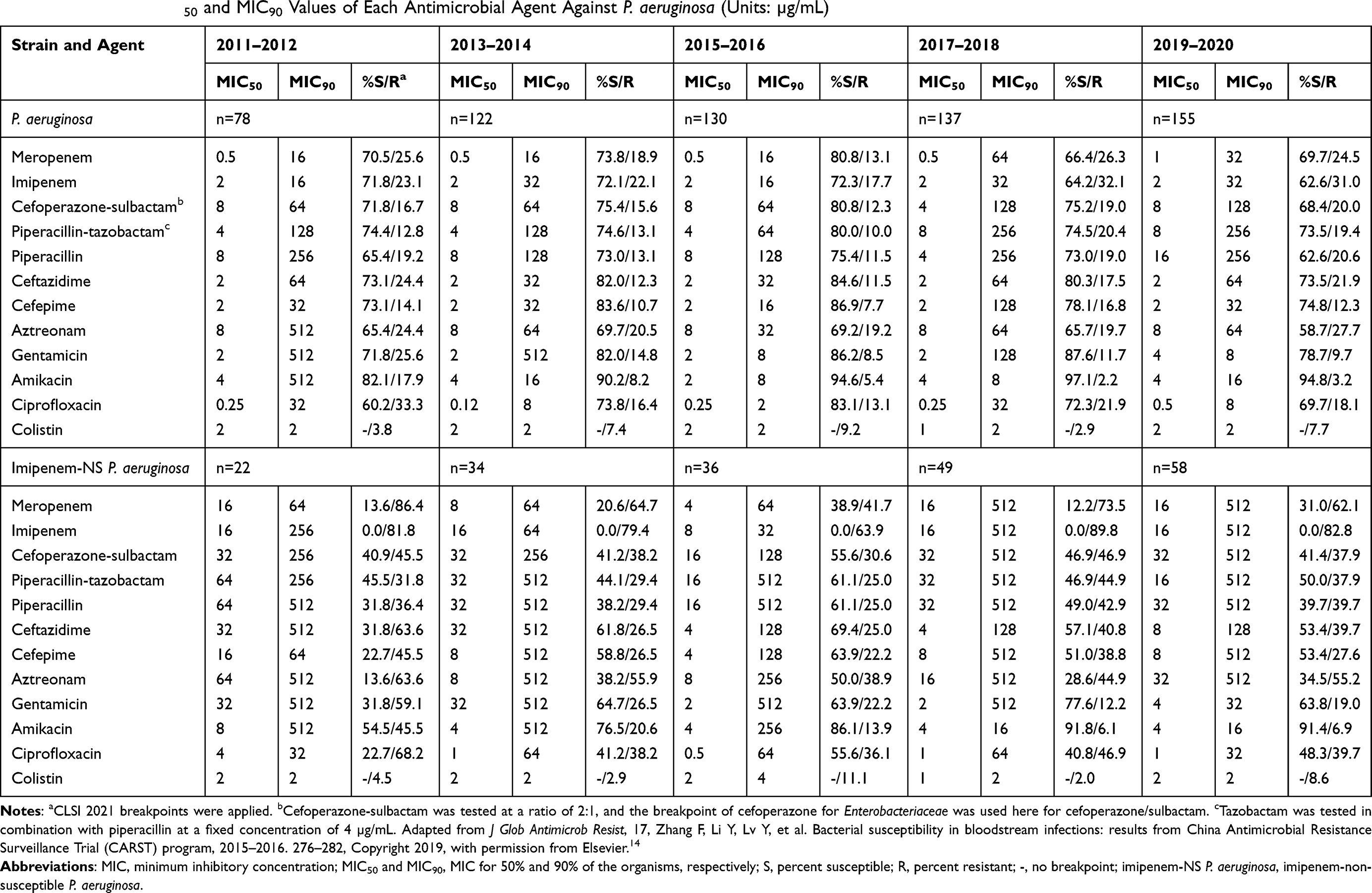 |
Table 4 Change in MIC50 and MIC90 Values of Each Antimicrobial Agent Against P. aeruginosa (Units: µg/mL) |
Changes in Antimicrobial Susceptibility of A. baumannii
Few agents showed in vitro activity against A. baumannii, with colistin and tigecycline being the two agents with low MIC90 values during the 10-year study period (Table 5). The susceptibility rates of A. baumannii to carbapenems were ≤30%. The susceptibility rates to the β-lactam combination agent cefoperazone-sulbactam were also low, with only ~30% of isolates being susceptible in each of the study periods. Although amikacin was the most effective agent apart from colistin and tigecycline, the susceptibility rates to amikacin were <50%, with the highest values of 47.3% in the 2019–20 study period. The MIC50 and MIC90 values of tigecycline against A. baumannii were higher than those against Enterobacteriaceae. In general, the frequency of IPM-NS A. baumannii remained high and stable over the course of the study, with the proportion remaining ~70% (Figure 1D). Trends in the prevalence of IPM-NS A. baumannii varied among different regions in China, but almost all regions showed the high prevalence from 2011 to 2020 (Figure 1D). The susceptibility rates of IPM-NS A. baumannii to most agents were <5%, and the resistance was serious.
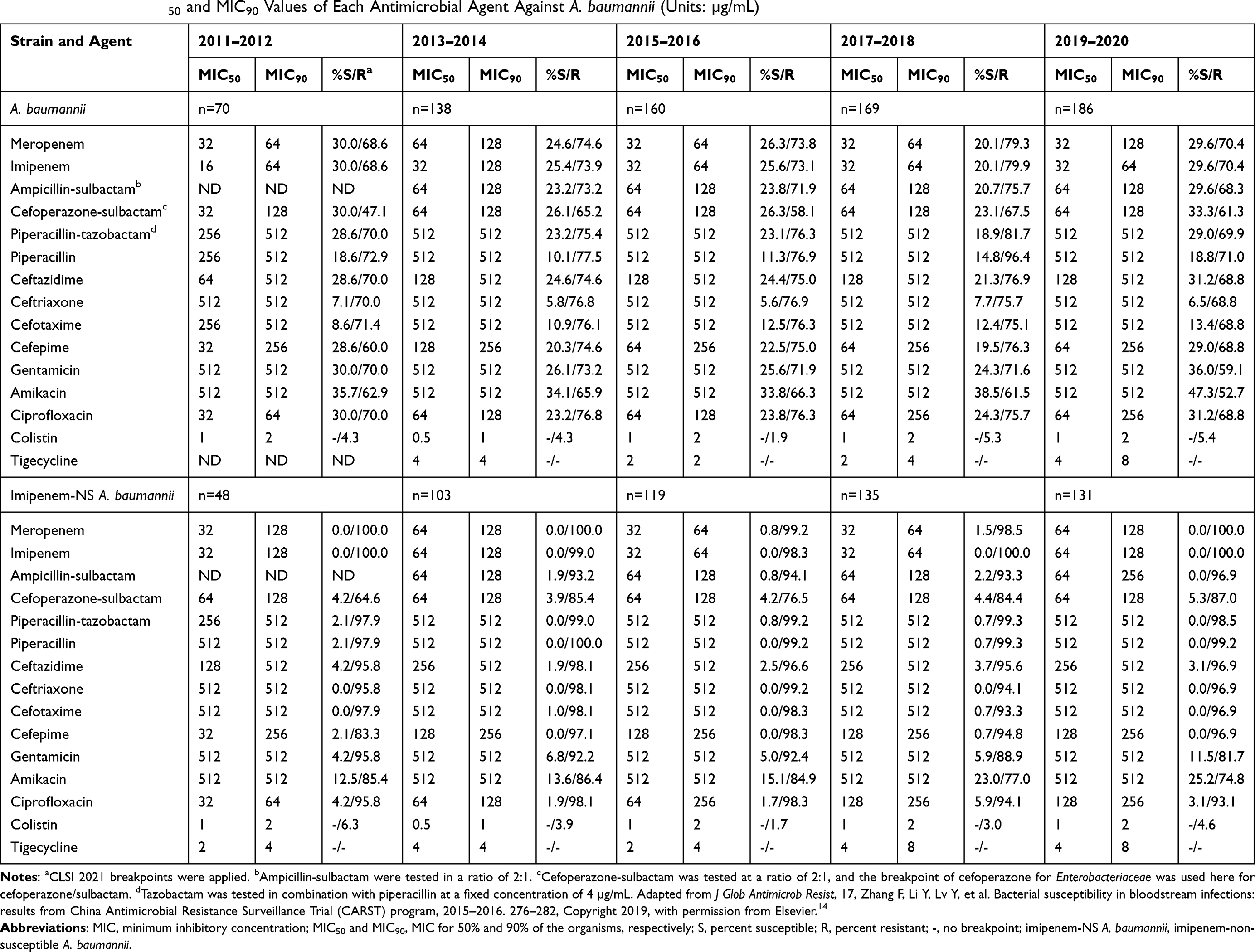 |
Table 5 Change in MIC50 and MIC90 Values of Each Antimicrobial Agent Against A. baumannii (Units: µg/mL) |
Discussion
BSIs are caused by a wide variety of pathogens, mainly Staphylococcus aureus and E. coli.5,8,14 However, many surveillance programs show an ongoing increase in the detection of gram-negative bacilli, many of which are multidrug-resistant (MDR), in BSI, worldwide.17,18 Majority of the gram-negative bacteria in these studies have been E. coli, K. pneumoniae and P. aeruginosa.19,20 Early empirical and adequate agents against these pathogens are essential to reduce the occurrence of bacterial resistance and thus improve patient outcomes. In recent years, the rising resistance rate of gram-negative bacilli has been a serious problem globally. The antimicrobial resistance profiles of gram-negative bacilli causing bloodstream infections have changed over time, while comprehensive and real-time surveillance data are limited in China. In the present study, we evaluated the susceptibility profiles of the most common gram-negative bacteria isolated from blood specimens to antimicrobial agents that are regularly used clinically.
E. coli was the most common BSI-associated bacteria. Data from the SENTRY Antimicrobial Surveillance Program showed that E. coli was more prominent than S. aureus and contributed to 24.0% of BSIs worldwide from 2013 to 2016.5 A study in Southwest China also indicated that E. coli (accounting for 32.03% of BSIs) was the most frequently isolated bacteria causing BSIs.9 Similar to previous reports, rates of resistance in E. coli remained relatively stable for many antibiotic agents in China from 2011 to 2020.21,22 During the study period, cefotaxime resistance rates in E. coli were always higher than those of ceftazidime. In China, blaCTX-M was the most common ESBL genotype and was widespread throughout the country.23,24 The CTX-M β-lactamases with the ability to hydrolyze cefotaxime and ceftriaxone were responsible for the high cefotaxime resistance rates.25 A decreasing trend in the resistance rates of E. coli to third-generation cephalosporins was observed during the 10-year period. The possible explanation underlying this was that the use of third-generation cephalosporins was decreased and carbapenems became the important choice in the empirical treatment of BSIs due to the widespread of ESBL in nosocomial infections. Although the detection rates of carbapenem-non-susceptible E. coli remained low in the 10-year period, the treatments for infections caused by this pathogen are a challenging problem in clinics. Carbapenemases, particularly metallo-β-lactamase (MBL), are the primary causes of carbapenem resistance in E. coli in China.26 β-Lactam-β-lactamase inhibitor combinations (BL-BLIs) are some of the efficacious antibiotic agents against carbapenem-resistant bacteria. However, the currently approved combinations possess activity against serine-β-lactamases, and clinical BL-BLIs approved for metallo-β-lactamases are not available.27
K. pneumoniae was the second most frequent cause of BSI among gram-negative bacteria and contributed to ~10% of BSIs worldwide.5 Data from China showed that K. pneumoniae accounted for 11.1% of BSIs in China.9 In the past decade, the utilization of carbapenems in clinical treatments has become necessary due to the proliferation of MDR pathogens in clinical settings. Such an increase in carbapenem consumption has been accompanied by the emergence of carbapenem-resistant gram-negative pathogens. A significant increase in the detection rate of carbapenem-resistant K. pneumoniae (CRKP) was observed during the 10-year period. Other studies also demonstrated that CRKP increased seriously in China and few agents were effective against these pathogens. In China, Klebsiella pneumoniae carbapenemase-2 (KPC-2) is responsible for phenotypic resistance in most CRKP strains.26,28 Novel β-lactamase inhibitor combinations display activities against CRKP, including ceftazidime-avibactam, meropenem-vaborbactam and imipenem-relebactam, which are currently approved or in late stages of development.29 In addition, the resistance rates of K. pneumoniae to ciprofloxacin have been increasing and ciprofloxacin is not an appropriate choice in the treatment of K. pneumoniae BSIs.
Among all Enterobacteriaceae, E. cloacae ranks third in its ability to cause bloodstream infections.5,20 In China, MBL genes and KPC genes were both detected in E. cloacae in previous studies.30,31 Carbapenem resistance genes might be shared between bacterial species via horizontal transfer. In general, the ciprofloxacin activities against E. cloacae showed a trend to increase, and the agent continued to be an effective choice.
The previous studies revealed that P. aeruginosa was the most common non-fermentative gram-negative bacteria causing BSIs and contributed to ~5% of BSIs worldwide.5 The prevalence of P. aeruginosa in BSIs was ~3% in China.9 In general, the resistance profiles for P. aeruginosa displayed a first decrease and then increase for most agents during the study period. The increased use of carbapenems in recent years was related to the increased rates of IPM-NS P. aeruginosa in the last two surveillance periods. Imipenem resistance cannot cause resistance against other antibiotics but may be indicative of rising MDRs based on previous data.32 MDR in P. aeruginosa is a growing public health problem and is challenging to treat. Institutions and researchers have been paying increased attention to new treatments for carbapenem-resistant and MDR P. aeruginosa, and several studies reported that combination therapy might be an effective strategy, exemplified by colistin-based combination therapy.33 In addition, aminoglycosides could be considered as a therapeutic option since they retained activity against MDR P. aeruginosa.
A. baumannii was another most common non-fermentative gram-negative bacteria causing BSIs and accounted for 2% of BSIs worldwide in the past 20 years.5 A similar prevalence was observed in a Chinese surveillance program.9 Infections caused by A. baumannii are problematic for patients due to this pathogen’s resistance against different classes of antibiotics. The level of MDR for A. baumannii is higher than that observed in K. pneumoniae and P. aeruginosa globally.34 Carbapenems are considered to be a front-line option for infections caused by MDR, but carbapenem resistance is serious in A. baumannii. Tigecycline and colistin could be potentially used for MDR A. baumannii infections.35 However, resistance to colistin is also emerging.36 The high trend of resistance in A. baumannii is a crisis to the public health considering its ability to survive in harsh environments, predilection for the seriously ill within intensive care units, and a wide variety of resistance mechanisms. Strict antimicrobial management and effective infection control policy should be enforced to reduce the production and spread of resistance.
Conclusion
In summary, our study generated a complete picture of variation in pathogen frequency and antibiotic resistance trends among gram-negative bacilli causing BSI. The susceptibility profiles for E. coli, the major cause of BSIs, remained constant during the 10 years. The prevalence of ESBL-producing isolates in E. coli and K. pneumoniae were both decreased. However, a significant increase in the carbapenem resistance rates in K. pneumoniae has been observed. The resistance profiles for P. aeruginosa have displayed a trend to increase for most agents in recent years. Carbapenems are still the effective options against gram-negative bacilli, except for A. baumannii. The resistance trend in A. baumannii was serious and few agents were effective against these pathogens. The last-resort antibiotics such as tigecycline and colistin could be potentially used for MDR A. baumannii BSIs. The spread control of A. baumannii within the hospital environment is of great urgency.
Ethics Approval and Consent to Participate
Since the project falls under the category observational study and all bacterial strains were from residual samples used in clinical diagnosis or were strains from their subcultures, it has been determined they meet the criteria for exemption. This project does not involve any patient information nor does it affect the normal diagnosis and treatment of patients, and after consultation with the human research ethics committee of the Institutional Review Board of Peking University First Hospital, ethical approval was waived and written patient consent was not required.
Acknowledgments
The following hospitals contributed to this study: (1) the Institute of Clinical Pharmacology, Peking University First Hospital, Beijing; (2) Beijing Hospital, Beijing; (3) The Second Hospital of Jilin University, Changchun; (4) Tianjin Medical University General Hospital, Tianjin; (5) The Second Hospital of Hebei Medical University, Shijiazhuang; (6) The First Affiliated Hospital with Nanjing Medical University, Nanjing; (7) Zhongshan Hospital, Fudan University, Shanghai; (8) Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou; (9) Guangzhou Women and Children’s Medical Center, Guangzhou; (10) Renmin Hospital of Wuhan University, Wuhan; (11) Xiangya Hospital Central South University, Changsha; (12) Kunming First People’s Hospital, Kunming; (13) The Affiliated Hospital of Guizhou Medical University, Guiyang; (14) The First Hospital Affiliated to Army Medical University, Chongqing; (15) Air Force Military Medical University, Xijing Hospital, Xi’an; (16) Jinan Central Hospital Affiliated to Shandong University, Jinan; (17) Lanzhou University Second Hospital, Lanzhou; (18) The First Teaching Hospital of Xinjiang Medical University, Urumqi; (19) Hanzhong Center Hospital, Hanzhong; (20) Hainan General Hospital, Haikou; and (21) Children’s Hospital of Shanxi, Shanxi.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Key Research and Development Program of China (2018YFC1200100 and 2018YFC1200105). This study also received funding from Sumitomo Pharmaceuticals Co., Ltd. (Suzhou, China).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cecconi M, Evans L, Levy M, et al. Sepsis and septic shock. Lancet. 2018;392:75–87. doi:10.1016/S0140-6736(18)30696-2
2. Qu J, Feng C, Li H, et al. Antibiotic strategies and clinical outcomes for patients with carbapenem-resistant Gram-negative bacterial bloodstream infection. Int J Antimicrob Agents. 2021;57:106284. doi:10.1016/j.ijantimicag.2021.106284
3. McNamara JF, Righi E, Wright H, et al. Long-term morbidity and mortality following bloodstream infection: a systematic literature review. J Infect. 2018;77:1–8. doi:10.1016/j.jinf.2018.03.005
4. Kern WV, Rieg S. Burden of bacterial bloodstream infection-a brief update on epidemiology and significance of multidrug-resistant pathogens. Clin Microbiol Infect. 2020;26:151–157. doi:10.1016/j.cmi.2019.10.031
5. Diekema DJ, Hsueh P-R, Mendes RE, et al. The microbiology of bloodstream infection: 20-year trends from the SENTRY antimicrobial surveillance program. Antimicrob Agents Chemother. 2019;63:e00355–19. doi:10.1128/AAC.00355-19
6. Al-Orphaly M, Hadi HA, Eltayeb FK, et al. Epidemiology of multidrug-resistant Pseudomonas aeruginosa in the Middle East and North Africa region. mSphere. 2021;6:e00202–21. doi:10.1128/mSphere.00202-21
7. Bassetti M, De Waele JJ, Eggimann P, et al. Preventive and therapeutic strategies in critically ill patients with highly resistant bacteria. Intensive Care Med. 2015;41:776–795. doi:10.1007/s00134-015-3719-z
8. Akova M. Epidemiology of antimicrobial resistance in bloodstream infections. Virulence. 2016;7:252–266. doi:10.1080/21505594.2016.1159366
9. Yang S, Xu H, Sun J, et al. Shifting trends and age distribution of ESKAPEEc resistance in bloodstream infection, Southwest China, 2012–2017. Antimicrob Resist Infect Control. 2019;8:61. doi:10.1186/s13756-019-0499-1
10. Falagas ME, Tansarli GS, Karageorgopoulos DE, et al. Deaths attributable to carbapenem-resistant Enterobacteriaceae infections. Emerg Infect Dis. 2014;20:1170–1175. doi:10.3201/eid2007.121004
11. Stewardson AJ, Allignol A, Beyersmann J, et al. The health and economic burden of bloodstream infections caused by antimicrobial susceptible and non-susceptible Enterobacteriaceae and Staphylococcus aureus in European hospitals, 2010 and 2011: a multicentre retrospective cohort study. Euro Surveill. 2016;21:
12. Liu X, Wang Y, Cui L, et al. A retrospective study on mcr-1 in clinical Escherichia coli and Klebsiella pneumoniae isolates in China from 2007 to 2016. J Antimicrob Chemother. 2018;73:1786–1790. doi:10.1093/jac/dky092
13. Liu XJ, Lyu Y, Li Y, et al. Trends in antimicrobial resistance against Enterobacteriaceae strains isolated from blood: a 10-year epidemiological study in mainland China (2004–2014). Chin Med J. 2017;130(17):2050–2055. doi:10.4103/0366-6999.213407.
14. Zhang F, Li Y, Lv Y, et al. Bacterial susceptibility in bloodstream infections: results from China Antimicrobial Resistance Surveillance Trial (CARST) program, 2015–2016. J Glob Antimicrob Resist. 2019;17:276–282. doi:10.1016/j.jgar.2018.12.016
15. Clinical and Laboratory Standards Institute. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically Ninth Edition: Approved Standard M7-A9. CLSI, Wayne, PA, USA: Clinical and Laboratory Standards Institute; 2012.
16. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Thirty-First Informational Supplement M100-S31. CLSI, Wayne, PA, USA: Clinical and Laboratory Standards Institute; 2021.
17. Zhang Z, Chen M, Yu Y, et al. Antimicrobial susceptibility among gram-positive and gram-negative blood-borne pathogens collected between 2012–2016 as part of the Tigecycline Evaluation and Surveillance Trial. Antimicrob Resist Infect Control. 2018;7:152. doi:10.1186/s13756-018-0441-y
18. Yungyuen T, Chatsuwan T, Plongla R, et al. Nationwide surveillance and molecular characterization of critically drug-resistant Gram-negative bacteria: results of the Research University Network Thailand study. Antimicrob Agents Chemother. 2021;65:e00675–21. doi:10.1128/AAC.00675-21
19. De Angelis G, Fiori B, Menchinelli G, et al. Incidence and antimicrobial resistance trends in bloodstream infections caused by ESKAPE and Escherichia coli at a large teaching hospital in Rome, a 9-year analysis (2007–2015). Eur J Clin Microbiol Infect Dis. 2018;37:1627–1636. doi:10.1007/s10096-018-3292-9
20. Xu A, Zheng B, Xu YC, et al. National epidemiology of carbapenem-resistant and extensively drug-resistant Gram-negative bacteria isolated from blood samples in China in 2013. Clin Microbiol Infect. 2016;22(Suppl 1):S1–8. doi:10.1016/j.cmi.2015.09.015
21. Hu F, Zhu D, Wang F, et al. Current status and trends of antibacterial resistance in China. Clin Infect Dis. 2018;67(suppl_2):S128–S134. doi:10.1093/cid/ciy657
22. Hu F, Guo Y, Yang Y, et al. Resistance reported from China antimicrobial surveillance network (CHINET) in 2018. Eur J Clin Microbiol Infect Dis. 2019;38(12):2275–2281. doi:10.1007/s10096-019-03673-1
23. Yu Y, Ji S, Chen Y, et al. Resistance of strains producing extended-spectrum beta-lactamases and genotype distribution in China. J Infect. 2007;54(1):53–57. doi:10.1016/j.jinf.2006.01.014
24. Xia S, Fan X, Huang Z, et al. Dominance of CTX-M-type extended-spectrum β-lactamase (ESBL)-producing Escherichia coli isolated from patients with community-onset and hospital-onset infection in China. PLoS One. 2014;9(7):e100707. doi:10.1371/journal.pone.0100707
25. Bush K, Bradford PA. Epidemiology of β-lactamase-producing pathogens. Clin Microbiol Rev. 2020;33(2):e00047–19. doi:10.1128/CMR.00047-19
26. Zhang R, Liu L, Zhou H, et al. Nationwide surveillance of clinical carbapenem-resistant Enterobacteriaceae (CRE) strains in China. EBioMedicine. 2017;19:98–106. doi:10.1016/j.ebiom.2017.04.032
27. Mojica MF, Rossi M-A, Vila AJ, et al. The urgent need for metallo-β-lactamase inhibitors: an unattended global threat.. Lancet Infect Dis. 2021;22(1):
28. Yin D, Wu S, Yang Y, et al. Results from the China Antimicrobial Surveillance Network (CHINET) in 2017 of the in vitro activities of ceftazidime-avibactam and ceftolozane-tazobactam against clinical isolates of Enterobacteriaceae and Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2019;63:e02431–18. doi:10.1128/AAC.02431-18
29. Yahav D, Giske CG, Grāmatniece A, et al. New β-lactam-β-lactamase inhibitor combinations. Clin Microbiol Rev. 2021;34:e00115–20. doi:10.1128/CMR.00021-21
30. Xue M, Wang K, Lu L, et al. Characterization of an New Delhi-Metallo-1-producing Enterobacter cloacae ST418 strain from a patient in Guangzhou, China. Microb Drug Resist. 2021;27:706–709. doi:10.1089/mdr.2020.0035
31. Zhao Y, Zhang J, Fu Y, et al. Molecular characterization of metallo-β-lactamase-producing carbapenem-resistant Enterobacter cloacae complex isolated in Heilongjiang Province of China. BMC Infect Dis. 2020;20:94. doi:10.1186/s12879-020-4768-7
32. Shortridge D, Gales AC, Streit JM, et al. Geographic and temporal patterns of antimicrobial resistance in Pseudomonas aeruginosa over 20 years from the SENTRY Antimicrobial Surveillance Program, 1997–2016. Open Forum Infect Dis. 2019;6(Suppl 1):S63–S68. doi:10.1093/ofid/ofy343
33. Horcajada JP, Montero M, Oliver A, et al. Epidemiology and treatment of multidrug-resistant and extensively drug-resistant Pseudomonas aeruginosa infections. Clin Microbiol Rev. 2019;32:e00031–19. doi:10.1128/CMR.00031-19
34. De Oliveira DMP, Forde BM, Kidd TJ, et al. Antimicrobial resistance in ESKAPE pathogens. Clin Microbiol Rev. 2020;33:e00181–19. doi:10.1128/CMR.00181-19
35. Xie R, Zhang XD, Zhao Q, Peng B, Zheng J. Analysis of global prevalence of antibiotic resistance in Acinetobacter baumannii infections disclosed a faster increase in OECD countries. Emerg Microbes Infect. 2018;7(1):31. doi:10.1038/s41426-018-0038-9
36. Cai Y, Chai D, Wang R, Liang B, Bai N. Colistin resistance of Acinetobacter baumannii: clinical reports, mechanisms and antimicrobial strategies. J Antimicrob Chemother. 2012;67(7):1607–1615. doi:10.1093/jac/dks084
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.