")
Back to Journals » Clinical Interventions in Aging » Volume 17
Anticholinergic Drug Use on Admission and the Risk of In-Hospital Falls in Older Hospitalized Patients
Authors Akgün Ö, Oudshoorn C, Mattace-Raso FUS , Egberts A
Received 11 January 2022
Accepted for publication 5 March 2022
Published 15 March 2022 Volume 2022:17 Pages 277—285
DOI https://doi.org/10.2147/CIA.S357818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Özge Akgün,1 Christian Oudshoorn,1 Francesco US Mattace-Raso,1 Angelique Egberts1,2
1Department of Internal Medicine, Section of Geriatric Medicine, Erasmus MC University Medical Center, Rotterdam, the Netherlands; 2Department of Hospital Pharmacy, Franciscus Gasthuis & Vlietland, Rotterdam & Schiedam, the Netherlands
Correspondence: Angelique Egberts, Section of Geriatric Medicine, Department of Internal Medicine, Erasmus MC University Medical Center, Room Rg-527, PO Box 2040, Rotterdam, CA, 3000, the Netherlands, Tel +31 10 70 35979, Fax +31 10 70 34768, Email [email protected]
Purpose: In-hospital falls, especially among older patients, are a major and underestimated problem. Several studies have suggested a possible association between anticholinergic drug use and falls, but the results are inconclusive and studies focusing on in-hospital falls are scarce. The aim of the present study was to investigate whether anticholinergic drug exposure on admission is associated with in-hospital falls.
Patients and Methods: This retrospective chart review study was conducted in the Erasmus MC University Medical Center, Rotterdam, the Netherlands. Patients aged 65 years and older, who were acutely admitted to the geriatric ward between 2012 and 2015, were included. Anticholinergic drug exposure was determined with the Anticholinergic Risk Scale (ARS), the Anticholinergic Cognitive Burden scale (ACB) and the list of Chew. Logistic regression was used to investigate the possible association between anticholinergic drug exposure and in-hospital falls. Analyses were adjusted for age, sex, fall history, fall as reason for admission, number of drugs on admission, use of a mobility aid and delirium.
Results: A total of 905 patients were included, of which 94 patients experienced one or more in-hospital falls. Each additional anticholinergic drug in use, according to the ARS, was associated with an increased odd of experiencing a fall (OR = 1.49, 95% CI: 1.06– 2.10). Other measures, ie anticholinergic drug use (yes/no) and different categories of anticholinergic drug burden, measured with the ARS, ACB and list of Chew, were all not associated with in-hospital falls.
Conclusion: Anticholinergic drug exposure on admission is possibly not a main risk factor for in-hospital falls among older patients.
Keywords: accidental falls, cholinergic antagonists, inpatients
Introduction
Falls affect approximately 30% of the older population each year, and are very common in hospital settings.1,2 Studies in hospital settings show around 1–9 falls per 1000 patient days and 15–30% of the patients who fall in the hospital, are inclined to fall again.3–5 Moreover, in-hospital falls can cause serious injuries, extended hospitalization, lead to additional costs, and increase the risk for nursing home admission.1 Considering the magnitude of the problem, identifying modifiable risk factors to reduce the risk for in-hospital falls is of paramount interest.
Older persons have an increased fall risk due to age-related physiological changes and high prevalence of comorbidities. Known risk factors for falls are, among others, mobility impairments, a history of falls and Parkinson’s disease.6,7 Additionally, as the number of prescribed medications increases with age, older persons frequently use multiple (fall increasing) drugs (polypharmacy).8,9 Specific drug classes that have been associated with an increased fall risk are benzodiazepines, diuretics, opioids and anticholinergic drugs.10–15
It has been reported that more than half of the hospitalized older population use drugs with anticholinergic activity (≈54%).16,17 Anticholinergics have several side-effects and older persons are sensitive to these effects due to age-related pharmacokinetic and pharmacodynamic changes. Therefore, even drugs with low anticholinergic activity can give serious side effects such as blurred vision, dizziness and an increased risk of delirium. This may lead to an increased risk of falling.6,14,15,18
Several studies have investigated the possible association between anticholinergic drug use and falls but the results are inconsistent.19–22 The methods used to assess anticholinergic drug use differ among the studies which could cause the inconsistency in the results. Also, variations exist in setting and study design. These differences decrease the comparability of observational studies on falls. Given this lack of knowledge, we investigated the association between anticholinergic drug exposure, using three various techniques, and in-hospital falls in older hospitalized patients.
Methods
This (retrospective) observational chart review study was performed with a dataset previously used to investigate the association between anticholinergic drug exposure on admission and delirium, length of hospital stay, postdischarge institutionalization and in-hospital mortality.23 This dataset contained all acutely ill patients aged 65 and older, hospitalized to the ward of geriatrics of the Erasmus MC University Medical Center, Rotterdam, The Netherlands between January 1, 2012 and December 31, 2015. Acutely ill patients were defined as patients with an acute condition that needed hospital admission to be treated. Due to the aim of the previous study, patients hospitalized for ≤ 2 days, admitted for elective (diagnostic) procedures and those with missing data on drug use or outcome measures were excluded from the dataset.23 In the present study, we included all patients enrolled in the dataset.
The study was conducted in accordance with the principles expressed in the Declaration of Helsinki. In The Netherlands, ethical approval and patient consent are not required for retrospective chart review studies in which data collected during routine clinical care are extracted and analyzed anonymously.
Data Collection
All data was collected from medical records. Variables that may contribute to the occurrence of falls were collected and included age, sex, body mass index (BMI), use of walking, hearing or visual aids, the presence of Parkinson’s disease, fall history, fall as reason for admission, prescribed drug use at the time of admission and the occurrence of delirium. The severity of comorbidities was calculated with the Charlson Comorbidity Index (CCI), which includes 19 medical conditions scored from one to six, with total scores ranging from 0–37.24 The higher the score, the more severe the burden of comorbidities. Also length of hospital stay, place of residence before admission and after discharge, and in-hospital mortality were documented.
Anticholinergic Drug Measurement
In the present study, we focused on anticholinergic drug use at the time of admission. Dispensing records from the community pharmacy were used to register all prescribed drugs in use by the patient. If this information was unavailable, correspondence letters of general practitioners or other referrers, or the medication history from the hospital medical record were used.23
Several anticholinergic drug scales are available that rank drugs based on their anticholinergic properties. In the present study, we used the Anticholinergic Risk Scale (ARS),25 the Anticholinergic Cognitive Burden scale (ACB, version of 2012)26 and the list of Chew et al.27 These lists were chosen because they are simple and quick to use, and contain different anticholinergic drugs.
On the ARS, drugs are ranked based on their anticholinergic side effects, both central and peripheral, possibly leading to cognitive dysfunction. It has a total of 49 drugs divided with a score of 1 to 3, 1 meaning moderate anticholinergic potential and 3 meaning high anticholinergic potential.25 The ACB includes 99 drugs that are ranked with a score ranging between 1 to 3, based on their potential to have a negative effect on cognition. Drugs with a score of 3 have also associations with delirium.26 Finally, the 39 drugs on the list of Chew are ranked based on in vitro anticholinergic activity. They are scored from 0.5–3 which means low to high anticholinergic activity.27
In the present study, anticholinergic drug exposure on admission was defined as the use of anticholinergic drugs (no/yes), total number of anticholinergic drugs, and categories of anticholinergic drug burden (ADB), all measured with the ARS, ACB and list of Chew. ADB is the sum of scores assigned to each drug prescribed to the patient.
Study Outcome
The primary outcome measure was the occurrence of falls during the hospital stay. A fall was defined as an unintentional change in body position. These data were collected from medical records in the hospital and subsequently compared with the recorded falls from the incident monitoring reporting system to verify the completeness of the data.
Statistical Analysis
All data was analyzed using Statistical Package for the Social Sciences (SPSS version 25.0 IBM Corp., Armonk, NY, USA) and results were assumed statistically significant at a two-sided P<0.05. Possible differences in characteristics between fallers and non-fallers were compared using the Chi-square test or Fisher’s exact test for categorical variables and the Mann–Whitney U-test or Student’s t-test for continuous variables, depending on the distribution of the data.
Logistic regression was performed to obtain the odds ratio (OR) and 95% confidence interval (CI) for in-hospital falls (dependent variable) according to different measures of anticholinergic drug exposure (exposure no/yes, total number of anticholinergic drugs and categories of ADB quantified with the ARS, the ACB and the Chew). Number of anticholinergic drugs was treated as a continuous variable. ADB was divided into three categories: no ADB (for all scales score 0), moderate ADB (ARS and ACB score 1–2; Chew score 0.5–1.0) and high ADB (ARS and ACB score ≥3; Chew score ≥1.5); the first category was used as reference. Adjustments have been made for characteristics with a P<0.10 and which were available for all patients (fall history, fall as reason for admission, number of drugs on admission, use of a mobility aid and delirium) and for standard covariates (age and sex) through multivariate logistic regression.
Results
A total of 1193 patients were admitted to the geriatric ward during the study period of whom 905 were included (165 did not meet the inclusion criteria, 119 were excluded because they were hospitalized for ≤ 2 days and 4 had missing data with regard to drug use or outcome measures). A detailed flow chart of the study sample selection can be found in a previous publication.23 No statistically significant differences were found in sex distribution and age between included and excluded patients.23
Table 1 shows the baseline and discharge characteristics of the overall sample, of which 10.4% (94 patients) experienced at least one fall in the hospital. The median age of the patients was 81 (interquartile range: 76–85) and 48.3% were male. Patients who fell were more likely to be male (60.6% vs 46.9%, P=0.011), more frequently had a positive fall history (76.6% vs 43.8%, P<0.001), were more likely to have a fall as the primary reason for admission (10.6% vs 4.7%, P=0.025) and had less prescribed drugs on admission (median 7 vs 8, P=0.015) than non-fallers. Furthermore, patients who fell during hospital stay were more likely to have a delirium during their admission (56.4% vs 25.5%, P<0.001), had a longer length of hospital stay (median 13 vs 7 days, P<0.001) and were more likely to be admitted to an institutional care facility after discharge (73.9% vs 43.5%, P<0.001) than patients who did not fall. Figure 1 shows that most patients fell within the first week of hospitalization.
 |
Table 1 Characteristics of the Overall Study Sample |
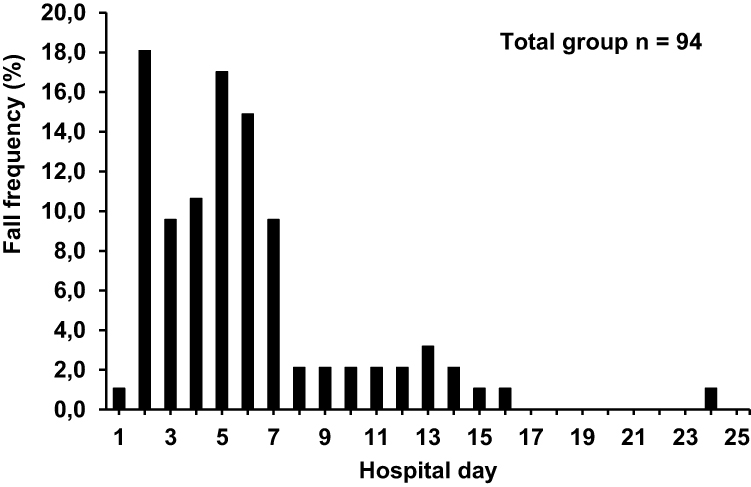 |
Figure 1 Frequency distribution of falls per hospital day. |
Anticholinergic Drug Use and Falls
Table 2 shows the characteristics with regard to anticholinergic drug exposure. The percentage of patients that used at least one anticholinergic drug, was 28.3% based on the ARS, 71.2% based on the ACB, and 57.8% based on the Chew. The median anticholinergic drug burden was 1 or lower for the overall sample, fallers and non-fallers.
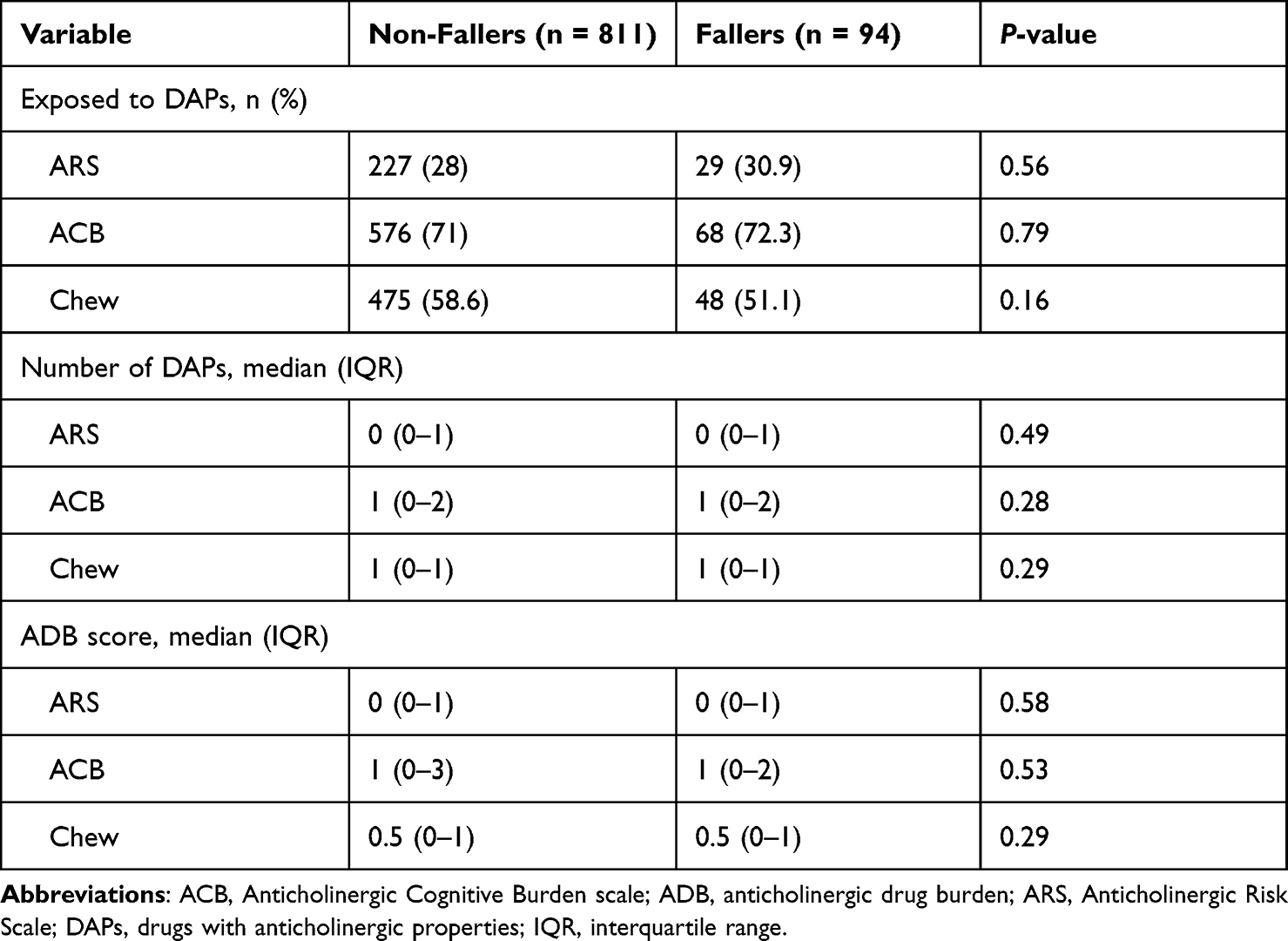 |
Table 2 Characteristics with Regard to Anticholinergic Drug Exposure |
Table 3 shows the ORs and corresponding 95% CIs for in-hospital falls based on different measures of anticholinergic effect. In adjusted models, we found that each additional anticholinergic drug in use by a patient according to the ARS was associated with a 49% increase in odds of experiencing a fall during the hospital stay (OR = 1.49 (95% CI 1.06–2.10)). However, this association seems to be caused by a small group of four patients who used four anticholinergic drugs. In this group, the fall frequency was 50%, while it was around 10% in patients using 0 to 3 anticholinergic drugs. Anticholinergic drug exposure (yes/no) and ADB, measured with the ARS, ACB and list of Chew, were not associated with in-hospital falls.
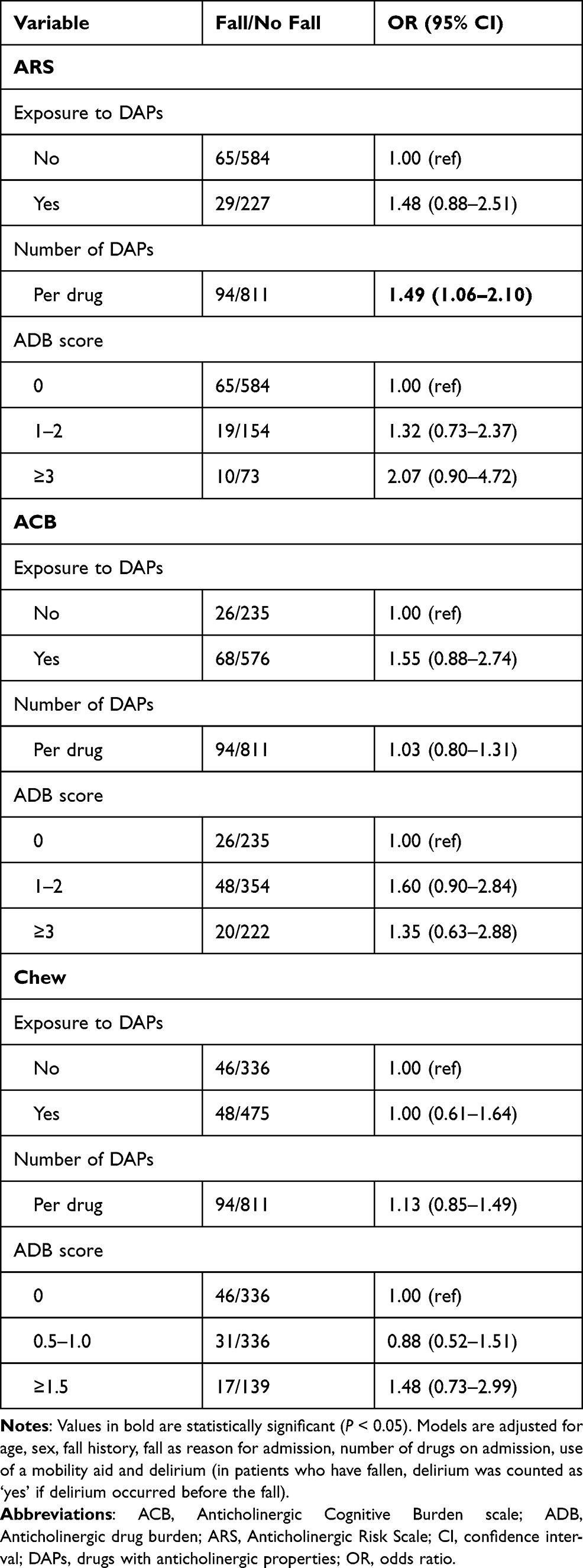 |
Table 3 Odds Ratios for in-Hospital Falls According to Different Measures of Anticholinergic Drug Exposure |
Discussion
In this study, we found that each additional anticholinergic drug in use by an older patient, according to the ARS, is associated with a 49% increase in odds of experiencing a fall during the hospital stay. This association was caused by a very small group of patients using four anticholinergic drugs and might be an overestimation. Other measures of anticholinergic drug use, ie anticholinergic drug burden and exposure, measured with the ARS, ACB and list of Chew were not associated with an increased risk of falling. This is the first study investigating the association between anticholinergic drug use, measured with the ARS, ACB and list of Chew, and in-hospital falls.
A previous study has investigated the same issue in older hospitalized patients, but used the Drug Burden Index (DBI) to measure anticholinergic drug burden.19 Dauphinot et al19 found that an increase in DBI during admission resulted in a three-fold higher risk of falling. However, the DBI measures the total exposure to anticholinergic and sedative drugs,28 and therefore, the association can also be caused by sedative drugs. Moreover, in line with our findings, they found no difference in DBI between fallers and non-fallers when the DBI was calculated on hospital admission.19
Other studies have investigated the association between anticholinergic drug exposure and falls outside the hospital. Landi et al20 found a positive association between ARS score and rate of falls during 1-year follow-up in older persons living in nursing homes. In the present study, no association was found between categories of ADB, measured with the ARS, and falls, although patients with a high ADB tended to fall more frequently than those with a low ADB. The difference in findings can be caused by the difference in population. Landi et al20 included nursing home residents and these persons may be more vulnerable than the patients included in our study. As a result, those persons may already have a higher chance of falling.
Machado-Duque et al29 found that a moderate and high ARS score (total score of 2 or ≥3 respectively) were associated with increased odds for hip fracture in persons aged 60 years and older. In contrast to our study, more persons used at least one drug with anticholinergic properties (61.9% compared to 28.3% in our study) and more persons had a total ARS score of 2 (12.8% compared to 5.4% in our study) or ≥3 (24.2% compared to 9.2% in our study). In our study, the median ARS score was relatively low. It is possible that patients with high ARS scores are more vulnerable to experience a fall or hip fracture than patients with low ARS scores, but that the number of patients with high ARS scores in our study was too low to detect such an effect.
Other studies have used the ACB. Zia et al30 found that an ACB score ≥ 1 was associated with recurrent and injurious falls in older community-dwelling persons, but this association did not remain statistically significant after adjustment for gait and balance impairment. Squires et al31 also examined the association between ACB scores and injurious falls in older community-dwelling persons and found that persons with a high ACB score had an increased risk for injurious falls over an average follow-up of 2.6 years. In contrast to our study, they only investigated falls resulting in a fracture or injury requiring hospitalization, while we also examined falls that did not result in injury.
Suehs et al22 found that anticholinergic drug exposure, measured with the ACB, was associated with an increased risk of a combined falls/fractures endpoint in older persons with overactive bladder. However, most of the drugs which showed an association with falls and fractures were the anticholinergic drugs used for the treatment of overactive bladder. Therefore, study findings may not be generalizable to other populations where anticholinergic drug use patterns are different.
Considering that in-hospital falls are multifactorial, other factors than anticholinergic drug exposure could play a bigger role in the occurrence of falls. In line with previous studies,7,32 we found that patients with a history of falls, those who had a fall as primary reason for admission and those who had delirium were at increased risk of in-hospital falls. Moreover, we found that the total number of drugs on admission was lower among patients who experienced an in-hospital fall than in those who did not fall. Dauphinot et al19 also showed a statistically significantly higher risk of falling when the number of drugs on admission is low. However, it can be speculated that the therapeutic classes of the drugs have a greater effect on the occurrence of an adverse event, in this case in-hospital falls, than the number of drugs.19
A potential reason why we could not find a clear association between anticholinergic drug use and falls is that we focused on in-hospital falls, which means that only falls that occurred during admission (in a couple of days) were used for the analysis. In previous studies, data on falls was collected by following patients for several months to years.20,22,31 Following patients for a longer period of time increases the risk and amount of falling. Moreover, many patients in our study were exposed to anticholinergic drugs, but the median ADB score per patient was relatively low. This means that a lot of patients used anticholinergics, but these were drugs that have a minimal anticholinergic effect. It might be possible that patients with a high ADB are more vulnerable to fall than patients with a low ADB.
Strengths and Limitations
This study has several strengths. To the best of our knowledge, this is the first study in which three anticholinergic drug scales were used and compared to investigate the association between anticholinergic drug exposure and falls. Moreover, this study focused on in-hospital falls, while most other studies focused on falls in community dwelling or nursing home patients. Also, the results were obtained in a relatively large sample (approximately three times larger than that of Dauphinot et al19). Lastly, not only data from the incident monitoring reporting system were used, but also data from medical records, which reduces the possibility of underestimating the number of falls considerably.
There are also some limitations. First, the anticholinergic drug scales used in this study do not take into account treatment duration and drug dose, while these factors also determine the amount of anticholinergic exposure and thus the severity of side-effects. Second, we measured anticholinergic drug exposure on hospital admission and did not collect data on changes in drug exposure during the hospital stay. This limits the ability to draw conclusions on causality. However, most falls occurred in the first week of hospitalization, and therefore, even when anticholinergic drugs were stopped after admission these drugs could still have had an effect based on the elimination half-life of the drug. Third, there are other drug classes, such as benzodiazepines, which can increase the risk of falling. In the present study, we have adjusted for the number of drugs in use per patient on admission, but not for the type of drugs in use.
Conclusion
In this study, we found that anticholinergic drug exposure on admission, measured with the ARS, ACB and Chew was not associated with an increased fall risk in older hospitalized patients. More research needs to be done, for example in subgroups with a high baseline fall risk, to clarify the possible association between anticholinergic drugs and falls, to reduce as many risk factors for falls as possible.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval/Informed Consent
In the Netherlands, no ethical approval and patient consent are required for retrospective chart review studies in which data collected during routine clinical care are extracted and analyzed anonymously.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; have approved the final version of the article to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No sources of funding were used for the conduct of this study or the preparation of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khow KSF, Visvanathan R. Falls in the aging population. Clin Geriatr Med. 2017;33(3):357–368. doi:10.1016/j.cger.2017.03.002
2. Loke MY, Yen Gan LL, Islahudin F. Awareness of medication related falls and preferred interventions among the elderly. Pak J Pharm Sci. 2018;31(2):359–364.
3. Schwendimann R, Buhler H, De Geest S, Milisen K. Characteristics of hospital inpatient falls across clinical departments. Gerontology. 2008;54(6):342–348. doi:10.1159/000129954
4. Krauss MJ, Nguyen SL, Dunagan WC, et al. Circumstances of patient falls and injuries in 9 hospitals in a Midwestern healthcare system. Infect Control Hosp Epidemiol. 2007;28(5):544–550. doi:10.1086/513725
5. Sato N, Hase N, Osaka A, Sairyo K, Katoh S. Falls among hospitalized patients in an acute care hospital: analyses of incident reports. J Med Invest. 2018;65(1.2):81–84. doi:10.2152/jmi.65.81
6. Deandrea S, Bravi F, Turati F, Lucenteforte E, La Vecchia C, Negri E. Risk factors for falls in older people in nursing homes and hospitals. A systematic review and meta-analysis. Arch Gerontol Geriatr. 2013;56(3):407–415. doi:10.1016/j.archger.2012.12.006
7. Mazur K, Wilczynski K, Szewieczek J. Geriatric falls in the context of a hospital fall prevention program: delirium, low body mass index, and other risk factors. Clin Interv Aging. 2016;11:1253–1261. doi:10.2147/CIA.S115755
8. Ambrose AF, Paul G, Hausdorff JM. Risk factors for falls among older adults: a review of the literature. Maturitas. 2013;75(1):51–61. doi:10.1016/j.maturitas.2013.02.009
9. Kojima T, Akishita M, Nakamura T, et al. Polypharmacy as a risk for fall occurrence in geriatric outpatients. Geriatr Gerontol Int. 2012;12(3):425–430. doi:10.1111/j.1447-0594.2011.00783.x
10. Richardson K, Bennett K, Kenny RA. Polypharmacy including falls risk-increasing medications and subsequent falls in community-dwelling middle-aged and older adults. Age Ageing. 2015;44(1):90–96. doi:10.1093/ageing/afu141
11. de Vries M, Seppala LJ, Daams JG, et al. Fall-risk-increasing drugs: a systematic review and meta-analysis: I. Cardiovascular drugs. J Am Med Dir Assoc. 2018;19(4):371 e371–371 e379. doi:10.1016/j.jamda.2017.12.013
12. Seppala LJ, Wermelink A, de Vries M, et al. Fall-risk-increasing drugs: a systematic review and meta-analysis: II. Psychotropics. J Am Med Dir Assoc. 2018;19(4):371 e311–371 e317.
13. Seppala LJ, van de Glind EMM, Daams JG, et al. Fall-Risk-increasing drugs: a systematic review and meta-analysis: III. Others. J Am Med Dir Assoc. 2018;19(4):372 e371–372 e378.
14. Ruxton K, Woodman RJ, Mangoni AA. Drugs with anticholinergic effects and cognitive impairment, falls and all-cause mortality in older adults: a systematic review and meta-analysis. Br J Clin Pharmacol. 2015;80(2):209–220. doi:10.1111/bcp.12617
15. Collamati A, Martone AM, Poscia A, et al. Anticholinergic drugs and negative outcomes in the older population: from biological plausibility to clinical evidence. Aging Clin Exp Res. 2016;28(1):25–35. doi:10.1007/s40520-015-0359-7
16. Lopez-Alvarez J, Sevilla-Llewellyn-Jones J, Anticholinergic A-OL. Drugs in geriatric psychopharmacology. Front Neurosci. 2019;13:1309. doi:10.3389/fnins.2019.01309
17. Vidal X, Agusti A, Vallano A, et al. Elderly patients treated with psychotropic Medicines admitted to hospital: associated characteristics and inappropriate use. Eur J Clin Pharmacol. 2016;72(6):755–764. doi:10.1007/s00228-016-2032-2
18. Nishtala PS, Salahudeen MS, Hilmer SN. Anticholinergics: theoretical and clinical overview. Expert Opin Drug Saf. 2016;15(6):753–768. doi:10.1517/14740338.2016.1165664
19. Dauphinot V, Faure R, Omrani S, et al. Exposure to anticholinergic and sedative drugs, risk of falls, and mortality: an elderly inpatient, multicenter cohort. J Clin Psychopharmacol. 2014;34(5):565–570. doi:10.1097/JCP.0000000000000195
20. Landi F, Dell’Aquila G, Collamati A, et al. Anticholinergic drug use and negative outcomes among the frail elderly population living in a nursing home. J Am Med Dir Assoc. 2014;15(11):825–829. doi:10.1016/j.jamda.2014.08.002
21. Fraser LA, Adachi JD, Leslie WD, et al. Effect of anticholinergic medications on falls, fracture risk, and bone mineral density over a 10-year period. Ann Pharmacother. 2014;48(8):954–961. doi:10.1177/1060028014535363
22. Suehs BT, Caplan EO, Hayden J, Ng DB, Gaddy RR. The relationship between anticholinergic exposure and falls, fractures, and mortality in patients with overactive bladder. Drugs Aging. 2019;36(10):957–967. doi:10.1007/s40266-019-00694-5
23. Egberts A, van der Craats ST, van Wijk MD, Alkilabe S, van den Bemt P, Mattace-Raso FUS. Anticholinergic drug exposure is associated with delirium and postdischarge institutionalization in acutely ill hospitalized older patients. Pharmacol Res Perspect. 2017;5(3):e00310. doi:10.1002/prp2.310
24. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
25. Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168(5):508–513. doi:10.1001/archinternmed.2007.106
26. Campbell N, Maidment I, Fox C, Khan B, Boustani M. The 2012 update to the Anticholinergic Cognitive Burden Scale. J Am Geriatr Soc. 2013;61:S142–S143.
27. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333–1341. doi:10.1111/j.1532-5415.2008.01737.x
28. Hilmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med. 2007;167(8):781–787. doi:10.1001/archinte.167.8.781
29. Machado-Duque ME, Castano-Montoya JP, Medina-Morales DA, Castro-Rodriguez A, Gonzalez-Montoya A, Machado-Alba JE. Drugs with anticholinergic potential and risk of falls with hip fracture in the elderly patients: a case-control study. J Geriatr Psychiatry Neurol. 2018;31(2):63–69. doi:10.1177/0891988718757370
30. Zia A, Kamaruzzaman S, Myint PK, Tan MP. Anticholinergic burden is associated with recurrent and injurious falls in older individuals. Maturitas. 2016;84:32–37. doi:10.1016/j.maturitas.2015.10.009
31. Squires P, Pahor M, Manini TM, Vouri S, Brown JD. Impact of anticholinergic medication burden on mobility and falls in the lifestyle interventions for elders (LIFE) study. J Clin Med. 2020;9(9):2989. doi:10.3390/jcm9092989
32. Oliver D, Britton M, Seed P, Martin FC, Hopper AH. Development and evaluation of evidence based risk assessment tool (STRATIFY) to predict which elderly inpatients will fall: case-control and cohort studies. BMJ. 1997;315(7115):1049–1053. doi:10.1136/bmj.315.7115.1049
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.