Back to Journals » Biologics: Targets and Therapy » Volume 19
Antibody-Based Therapeutics for Hypercholesterolemia
Authors Tomlinson B ![]() , Chan P
, Chan P ![]()
Received 30 June 2025
Accepted for publication 13 October 2025
Published 27 October 2025 Volume 2025:19 Pages 631—649
DOI https://doi.org/10.2147/BTT.S500456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Brian Tomlinson,1 Paul Chan2
1Faculty of Medicine, Macau University of Science & Technology, Macau, 999078, People’s Republic of China; 2Division of Cardiology, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei City, Taiwan
Correspondence: Brian Tomlinson, Faculty of Medicine, Macau University of Science & Technology, Avenida Wai Long, Taipa, Macau, 999078, People’s Republic of China, Email [email protected]
Abstract: Statins have provided the first line treatment for hypercholesterolemia for over two decades with the addition of ezetimibe if low-density lipoprotein (LDL) cholesterol targets are not achieved with statins alone. However, treatment with statins and other oral small molecules is often insufficient to attain the target levels of LDL cholesterol. This review describes the monoclonal antibodies (mAbs) that have been produced to overcome the residual cardiovascular risk related to uncontrolled LDL cholesterol. In recent years the mAbs, alirocumab and evolocumab, targeting proprotein convertase subtilisin/kexin type 9 (PCSK9) have become established worldwide as an additional treatment for patients not achieving LDL cholesterol goals on statins and ezetimibe, or sometimes as an alternative treatment in those with statin intolerance. They have been shown to be safe and effective in reducing cardiovascular events in patients at high cardiovascular risk. More recently, four new mAbs targeting PCSK9 have been developed and approved in China. Some of these mAbs offer the benefit of less frequent subcutaneous dosing and some are humanized mAbs and it remains to be seen whether their efficacy will be retained with long term use. New drug targets were identified to potentially reduce elevated triglyceride levels and the mAb angiopoietin-like 3 (ANGPTL3) inhibitor, evinacumab, was found to be effective in reducing LDL cholesterol in patients with homozygous familial hypercholesterolemia (FH) and has been approved for that indication. SHR-1918 is another mAb targeting ANGPTL3 being developed in China which may also be effective to treat homozygous FH. These drugs are expensive and may not be suitable for a wider indication and there are antisense oligonucleotides and small interfering RNA treatments in development which may prove more cost effective. Another mAb at an early stage of development is MAR001 targeting angiopoietin-like 4 (ANGPTL4). The role for this remains to be established.
Keywords: angiopoietin-like 3, atherosclerotic cardiovascular disease, familial hypercholesterolemia, monoclonal antibody, proprotein convertase subtilisin/kexin type 9
Introduction
Atherosclerotic cardiovascular disease (ASCVD) continues to be a major cause of morbidity and mortality in the United States and the rest of the world, fueled by ongoing increases in hypertension, obesity, type 2 diabetes and other major risk factors, according to the American Heart Association’s (AHA) 2025 Heart Disease and Stroke Statistics.1 Hypercholesterolemia, and in particular elevated low-density lipoprotein (LDL) cholesterol, is a major contributing factor to ASCVD, as shown by evidence from epidemiologic, genetic, and clinical studies.2
Statins, which inhibit 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase, the rate-limiting enzyme in the endogenous synthesis of cholesterol in the liver, have been the primary treatment to reduce LDL cholesterol for over 2 decades.3 A meta-analysis of clinical trials with statins showed that greater reductions in LDL cholesterol resulted in greater reductions in cardiovascular events.4 Statins are generally well tolerated, although there is increasing awareness of muscle symptoms in patients taking statins, which may not always be related to the drug itself.5 It has also been established that there is a small increase in the risk for new onset diabetes with statin therapy, particularly in people with prediabetes or other factors predisposing to diabetes, and usually related to higher intensity statin treatment.6 Other adverse effects attributed to statins, such as cognitive impairment, renal and hepatic damage, hemorrhagic stroke and cataract, have largely been disproven.7
Many observational studies show that the majority of patients do not achieve their LDL cholesterol goals despite the general availability of statins and other treatments.8,9 There are many reasons for this including prescription inertia and poor adherence to statin therapy which may be related to perceived adverse effects or general reluctance to being treated with statins.10 LDL cholesterol goals can be achieved more often with the use of combination therapy but studies show this is not used very frequently.11
Ezetimibe, which inhibits intestinal absorption of cholesterol and plant sterols by the Niemann-Pick C1-Like 1 (NPC1L1) transporter, is recommended as the next treatment to add if the LDL cholesterol goal is not achieved with statin treatment.12,13 Oral ezetimibe monotherapy at 10 mg once daily reduces LDL cholesterol by about 15–22% and when used in combination with statins the reduction in LDL cholesterol is usually slightly greater.14 In patients with acute coronary syndromes (ACS) in the IMProved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), ezetimibe in combination with high-dose statin reduced the combined cardiovascular endpoint especially in patients with diabetes mellitus.15,16
Recently, bempedoic acid has emerged as another oral drug that can be used as an alternative or addition to statin therapy. It acts by inhibiting ATP-citrate lyase (ACL), an enzyme higher than HMG-CoA in the cholesterol synthesis pathway, and it can reduce LDL cholesterol about 20% in addition to statin therapy or 30% when used as monotherapy.17 It is unlikely to cause muscle symptoms as it is activated selectively in the liver and not in skeletal muscle. In the CLEAR (Cholesterol Lowering via Bempedoic Acid [ECT1002], an ACL-Inhibiting Regimen) Outcomes study, it reduced the primary endpoint of combined cardiovascular events by 13% (p = 0.004) in statin intolerant patients who had, or were at high risk for, cardiovascular disease.18
Proprotein Convertase Subtilisin/Kexin Type 9 Inhibitors
The discovery in 2003 of proprotein convertase subtilisin/kexin type 9 (PCSK9), also known initially as neural apoptosis-regulated convertase 1 (NARC-1), provided a new target for drug development to reduce LDL cholesterol.19,20 Gain-of-function mutations in the PCSK9 gene were found to cause autosomal dominant familial hypercholesterolemia (FH),19 whereas loss-of-function variants were associated with lower levels of LDL cholesterol and reduced cardiovascular events and people with homozygous mutations causing absence of PCSK9 appeared healthy.21–23 Therefore, inhibition of PCSK9 appeared a promising alternative approach to reduce LDL cholesterol and cardiovascular events.
The first drugs to inhibit PCSK9 that were brought to the market were evolocumab and alirocumab which are fully human monoclonal antibodies (mAbs) that reduce LDL cholesterol by about 60% in most patients. Bococizumab was a humanized mAb targeting PCSK9, but it was withdrawn from development because of the formation of antidrug antibodies in some patients, which reduced its efficacy.24 Other mAbs have being developed and in the last two or three years, four other mAbs have been developed and approved for use in China (Table 1). In this article we provide a comprehensive review of all the mAbs in advanced development targeting PCSK9.
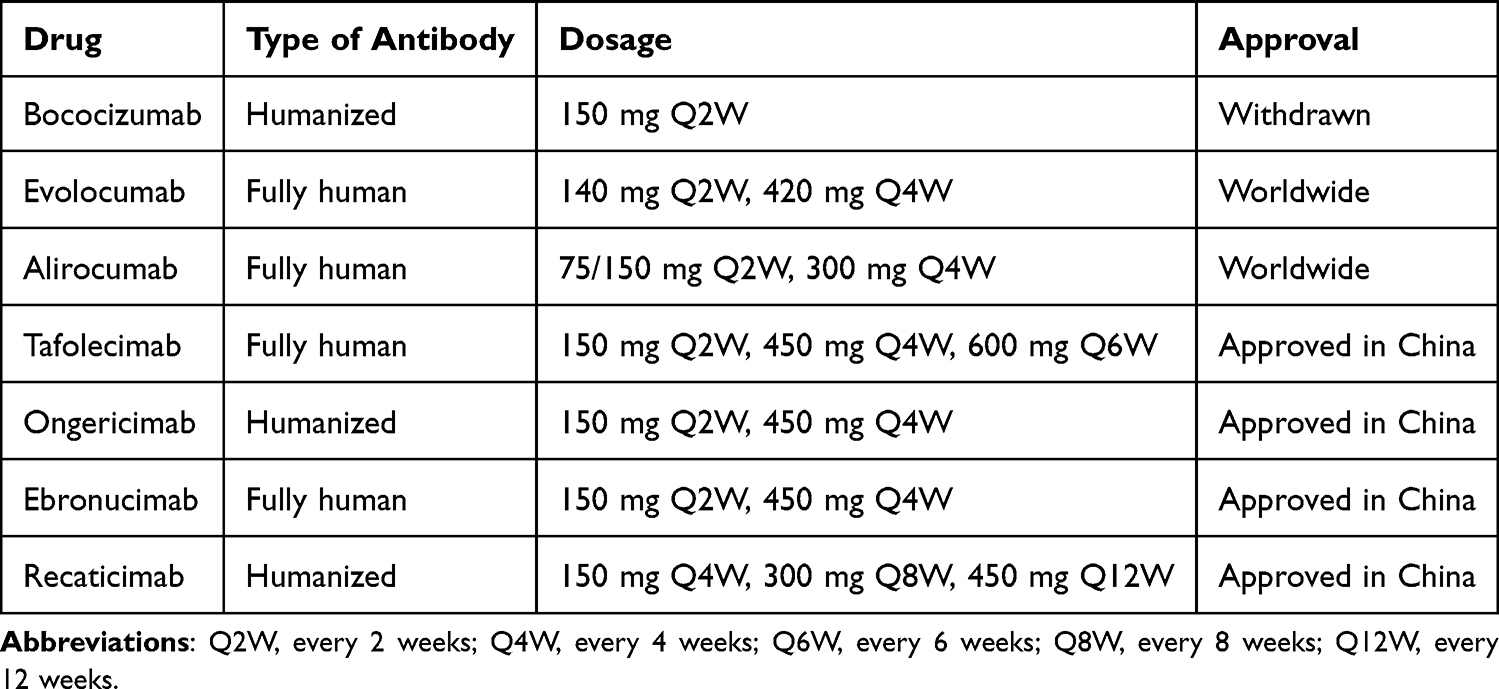 |
Table 1 Monoclonal Antibodies Targeting Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) |
Alirocumab and evolocumab were followed by the small interfering RNA (siRNA) inclisiran (Leqvio®, Novartis) which can be administered subcutaneously (SC) every 6 months and resulted in approximately 50% reductions in LDL cholesterol in the ORION-10 and ORION-11 trials.25,26 Inclisiran was approved for use in the European Union in 2020 and by the United States Food and Drug Administration (FDA) in 2021 before the results of cardiovascular outcome studies were available. It is currently being evaluated in the ORION-4 (NCT3705234) and VICTORION-2P (NCT05030428) cardiovascular outcome studies.
Several other types of pharmacotherapy to inhibit PCSK 9 are currently at various stages of development (Figure 1). There are two oral drugs in development, enlicitide decanoate (MK-0616, Merck) and AZD0780 (AstraZeneca). Enlicitide decanoate is a potent, oral macrocyclic peptide co-formulated with an oral absorption enhancer that can reduce LDL cholesterol in a dose-dependent manner by up to about 60%.27 It is currently being evaluated in three phase 3 trials CORALreef Lipids (NCT05952856), CORALreef HeFH (NCT05952869) and CORALreef Outcomes (TIMI 77) (NCT06008756).
 |
Figure 1 Action of drugs which increase or inhibit proprotein convertase subtilisin/kexin type 9 (PCSK9). The drugs in red font increase the expression of the LDL receptor and also increase PCSK9. The drugs in green font reduce PCSK9 through various mechanisms. Abbreviations: LDL, low-density lipoprotein; MTP, microsomal triglyceride transfer protein; VLDL, very low-density lipoprotein. |
The recent phase 2 PURSUIT study (NCT06173570) of oral AZDO780 showed a dose-dependent placebo-corrected reduction in LDL cholesterol up to 50.7% with the 30 mg dose.28
Lerodalcibep (LIB003) is a recombinant fusion protein comprising an adnectin PCSK9 binding domain and human serum albumin that is being developed by LIB Therapeutics. It was well tolerated in early phase trials and reduced LDL cholesterol by more than 60%. In the phase 3 LIBerate-HeFH trial (NCT04797104) in heterozygous FH patients, lerodalcibep 300 mg SC monthly given in 1.2 mL SC injections, reduced LDL cholesterol by 58.61% compared with placebo and had a safety profile similar to placebo apart from mild injection site reactions.29 The LIBerate-CVD study (NCT04797247) demonstrated the efficacy and safety of lerodalcibep in patients with ASCVD.30
A CRISPR base-editing therapy, VERVE-101 (Verve Therapeutics Inc), was developed to alter a single DNA base in the PCSK9 gene and permanently prevent hepatic PCSK9 production.31 This was used in the phase Ib Heart-1 (NCT05398029) study in heterozygous FH patients with established ASCVD but there were some adverse events and the product was modified to VERVE-102 which is being assessed in the Heart-2 trial (NCT06164730).
Treatments targeting PCSK9 are generally effective in patients with heterozygous FH (HeFH), which is a relatively common condition occurring in about 1:250 to 1:300 people in most populations.32 Homozygous FH (HoFH) has a prevalence ranging from 1:250,000 to 1:360,000 and does not respond well to PCSK9 inhibitors except in those subjects with gain-of-function mutations in the PCSK9 gene.33 It may be treated with lipoprotein apheresis in centers where that is available.
Bococizumab
Bococizumab (RN316/PF-04950615, Pfizer) is a humanized IgG2Δa mAb that recognizes and binds to the LDL receptor (LDLR)-binding domain of PCSK9, which was undergoing development by Pfizer, Inc (New York, NY) in the Studies of PCSK9 Inhibition and the Reduction of vascular Events (SPIRE) program.34 In a phase 2b 24-week dose-ranging study (NCT01592240) in 351 subjects with hypercholesterolemia on stable doses of statin, bococizumab significantly reduced LDL cholesterol levels across all doses with 150 mg SC every 2 weeks (Q2W) producing placebo-adjusted reductions in LDL cholesterol at week 12 of 53.1%.35 Some subjects had dose reductions because of very low LDL cholesterol. Positive antidrug antibody (ADA) titers were detected in about 7% of subjects treated with bococizumab and LDL cholesterol lowering was reduced in one of those subjects (0.4% of those treated with bococizumab subjects).
The SPIRE-1 (NCT01975376) and SPIRE-2 (NCT01975389) cardiovascular outcome studies were stopped early after a median follow-up of 10 months because of the development of high rates of ADAs in other studies in the program.36 The placebo adjusted reduction in LDL cholesterol at 14 weeks was 59.0% with bococizumab 150 mg SC Q2W. In the higher-risk, longer-duration trial (SPIRE-2), major cardiovascular events were significantly reduced (hazard ratio, 0.79; 95% confidence intervals [CI], 0.65 to 0.97; P=0.02), but there was no effect on major cardiovascular events in the lower-risk, shorter-duration trial (SPIRE-1).36 In a review of 6 clinical trials with bococizumab, ADAs developed in a large proportion of the patients which significantly reduced the lowering of LDL cholesterol levels and there was also a wide variation in the relative reduction in LDL cholesterol levels among patients in whom ADAs did not develop.24 Combining all SPIRE study results, the LDL cholesterol reduction related to bococizumab was 54.2% at 12 weeks and 40.4% at 52 weeks.37 ADAs generally developed after 12 weeks treatment and were associated with more frequent injection-site reactions.
A genome-wide association study of the ADA response to bococizumab identified specific amino acid substitutions at the HLA DRB1 and HLA DQB1 loci which were thought to be potentially generalizable to the response to other therapeutic mAbs.38
Evolocumab
Evolocumab (AMG 145, Repatha®, Amgen) is a fully human IgG2 mAb given in SC doses of 140 mg Q2W or 420 mg every month (Q1M) that reduce LDL cholesterol up to a maximum of about 64%.39,40 Evolocumab was approved by the European Commission (EC) in July 2015 followed by FDA approval in August 2015 and was the first PCSK9 inhibitor to be approved anywhere in the world. The comprehensive clinical development program of evolocumab called the “Program to Reduce LDL cholesterol and Cardiovascular Outcomes Following Inhibition of PCSK9 In Different Populations (PROFICIO)” included 20 clinical trials and a combined enrollment of about 30,000 patients.41
Evolocumab binds to circulating PCSK9 and over the dose range of 21 to 140 mg the plasma concentration did not increase in direct proportion to the dose, but in doses from 140 mg to 420 mg the pharmacokinetics became linear.42 The time to median peak serum concentrations (Tmax) following single SC doses of 140 or 420 mg in healthy adults was 3 to 4 days and the estimated absolute bioavailability was 72%.43 The elimination of evolocumab follows two phases involving predominantly saturable binding to the target protein, PCSK9, at low concentrations and through a non-saturable proteolytic pathway at higher concentrations and the estimated effective half-life (t1/2) is 11 to 17 days.43
Maximum suppression of circulating unbound PCSK9 was seen within 4 hours with single SC doses of 140 mg or 420 mg of evolocumab and compared to placebo, LDL cholesterol was reduced in a dose-dependent manner up to a maximum of 64%.42 The LDL cholesterol reduction was achieved as early as one week and the maximum responses were generally seen within two weeks of SC doses. There were also significant decreases in other lipid parameters with evolocumab, which included total cholesterol (TC), non-high-density lipoprotein (non-HDL) cholesterol, apolipoprotein B (apoB), triglycerides, and lipoprotein(a) [Lp(a)].42
Optimal dosing regimens with evolocumab were identified in the clinical development program in the phase 1 and 2 studies and these were applied in a large series of phase 3 studies. The two dosing regimens of evolocumab 140 mg Q2W or 420 mg Q1M were shown to have almost identical effects. The maximum reduction in LDL cholesterol produced by these doses varies from about 50% to over 60% in different patient groups, being slightly greater in patients on statin treatment. In the TESLA Part B (NCT01588496) and the TAUSSIG (NCT01624142) studies, which included patients with HoFH, the reduction of LDL cholesterol was attenuated in patients with LDL receptor-defective mutations and there was no response in those with receptor-negative mutations.44,45 Having some functioning LDLRs is necessary for the reduction of circulating LDL cholesterol with PCSK9 inhibitors or statins.
In the FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk, NCT01764633) trial in patients with stable cardiovascular disease, evolocumab was given SC as 140 mg Q2W or 420 mg Q1M and this reduced LDL cholesterol levels as compared with placebo by 59%, and reduced the composite cardiovascular primary endpoint by 15% compared to placebo for a median duration of follow-up of 2.2 years.46
The EBBINGHAUS (Evaluating PCSK9 Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects, NCT02207634) trial was a sub study of FOURIER to determine if the addition of evolocumab to background statin therapy and the attainment of very low LDL cholesterol levels had any adverse effects on cognitive function.47 No significant effects on cognitive function were observed for a median of 19 months.
Alirocumab
Alirocumab (REGN727, SAR236553, Praluent®, Sanofi/Regeneron) is a fully human IgG1 mAb that is given in SC doses of 75 or 150 mg Q2W and lowers LDL cholesterol by 45–62%.48,49 It was approved for medical use by the FDA and the EC in 2015. Like evolocumab, it also lowers other atherogenic lipid parameters, including TC, non-HDL cholesterol, apoB, triglycerides, and Lp(a), and there were increases in HDL cholesterol and apoA-I in some studies.48 The dose of 300 mg Q4W was approved by the FDA and the EC in 2017 and can be used as a starting dose as an alternative to 75 mg Q2W.
After SC injections of single doses, the Tmax for alirocumab is a median of about 3–7 days and the absolute bioavailability after SC administration is about 85%.50 At low concentrations, the elimination of alirocumab is predominately through saturable binding to PCSK9, while at higher concentrations alirocumab is largely eliminated through a non-saturable proteolytic pathway. The median apparent t1/2 of alirocumab was 17 to 20 days in patients receiving alirocumab at SC doses of 75 mg Q2W or 150 mg Q2W at steady state.50 When administered with a statin, the median apparent t1/2 of alirocumab is reduced to 12 days, presumably because the production of PCSK9 increases during statin treatment and this potentiates target-mediated clearance of alirocumab.
In the phase 3 program called ODYSSEY, alirocumab was compared with placebo or active control in a series of randomized, double-blind studies including patients with HeFH or with primary hypercholesterolemia with moderate to very high cardiovascular risk.51 In the ODYSSEY OUTCOMES cardiovascular outcomes study in patients with ACS, the dose of alirocumab was adjusted between 75 mg and 150 mg Q2W to achieve an LDL cholesterol level of 25–50 mg/dl (0.65–1.3 mmol/L) and there was a 15% reduction (p < 0.001) in the primary composite cardiovascular endpoint.52 In the phase 3 ODYSSEY program, the safety profile of alirocumab was generally comparable to placebo,49 and in the ODYSSEY OUTCOMES study, adverse events had a similar incidence in the alirocumab and the placebo groups, except that local injection-site reactions were more frequent in the alirocumab group than in the placebo group (3.8% versus 2.1%).52
No evidence of differences in cognitive tests was found by achieved lowest levels of LDL cholesterol, even <25 mg/dL.53 A pooled data analysis from 14 trials of the ODYSSEY program reported that in alirocumab-treated patients, LDL cholesterol levels <25 or <15 mg/dL were not associated with an increase in neurocognitive events.54
In the global safety pool, ADAs were detected in 4.8% of alirocumab-treated patients compared to 0.6% in control groups using a highly sensitive assay.51 These generally developed after a median of 12 weeks treatment and were only transient. Neutralizing antibodies were identified in only 1.2% of alirocumab-treated patients and these did not appear to correlate with safety outcomes or lipid-lowering efficacy. However, patients with positive ADAs response had more frequent injection-site reactions than those who did not develop this (10.2% vs 5.2%).51
Tafolecimab
Tafolecimab (IBI306, Sintbilo®) is a fully human IgG2 PCSK9 mAb developed by Innovent Biologics (Suzhou) Co. Ltd. It has potential long-acting effects as it is said to possess greater binding affinity for PCSK9 and a longer duration of LDL cholesterol reduction than other mAbs such as evolocumab.55 It was approved in August 2023 by the National Medical Products Administration (NMPA) in China as “An adjunct to diet, in combination with a statin or statin with other LDL cholesterol-lowering therapies, for the treatment of adults with primary hyperlipidemia [including heterozygous familial hypercholesterolemia (HeFH) and non-familial hypercholesterolemia (non-FH)] and mixed dyslipidemia who have failed to achieve LDL cholesterol goals despite moderate or higher doses of statins, to reduce LDL cholesterol, TC, and apoB levels”.56
Tafolecimab was given in intravenous (IV) and SC doses in phase 1a (NCT03366688) and phase 1b/2 (NCT03815812) dose finding studies in healthy volunteers or subjects with hyperlipidemia.55 Reductions in LDL cholesterol levels persisted for six weeks with higher doses and it was well tolerated. Tafolecimab was studied in a series of phase 3 studies called CREDIT (Clinical Research of Developing PCSK9 Inhibitor as Cholesterol-lowering Therapy in Chinese Patients with Dyslipidemia) that included patients at high cardiovascular risk with and without FH.
CREDIT-1 (NCT04289285) was a phase 3 48-week trial in Chinese patients with non-FH with SC tafolecimab 450 mg Q4W or tafolecimab 600 mg Q6W which showed reductions in LDL cholesterol of 65.0% and 57.3%, respectively, and the drug was well tolerated.57 Injection site reactions were more frequent with tafolecimab than with placebo (7.3% vs 2.5%).
CREDIT-2 (NCT04179669) was a phase 3 trial of tafolecimab in Chinese patients with HeFH who were on stable lipid lowering therapy.58 Tafolecimab 150 mg Q2W, tafolecimab 450 mg Q4W, or a placebo were given during a 12-week double-blind treatment phase, followed by a 12-week open-label period with tafolecimab administration. The least squares mean reductions in LDL cholesterol levels relative to placebo at week 12 were 57.4% with 150 mg Q2W and 61.9% with 450 mg Q4W (both p < 0.0001). The concentrations of non-HDL cholesterol, apoB-100, and Lp(a) were also markedly decreased with tafolecimab by week 12 and these effects were maintained until week 24.58
CREDIT-3 (NCT04031742) is a phase 2b/3 study to assess the efficacy and safety of IBI306 in subjects with homozygous FH. It appears to have been completed in 18 subjects, but results have not been published yet.
CREDIT-4 (NCT04709536) included 303 patients with HeFH or at high or very high cardiovascular risk with non-FH and with screening LDL cholesterol ≥1.8 mmol/L randomized to tafolecimab 450 mg Q4W or placebo for a 12-week double-blind treatment period.59 The least squares mean placebo corrected reduction in LDL cholesterol at week 12 was 63.0%, p < 0.0001 and there were marked reductions in non-HDL cholesterol, apoB, and Lp(a) levels.59 The phase 3 studies with tafolecimab are summarized in Table 2.
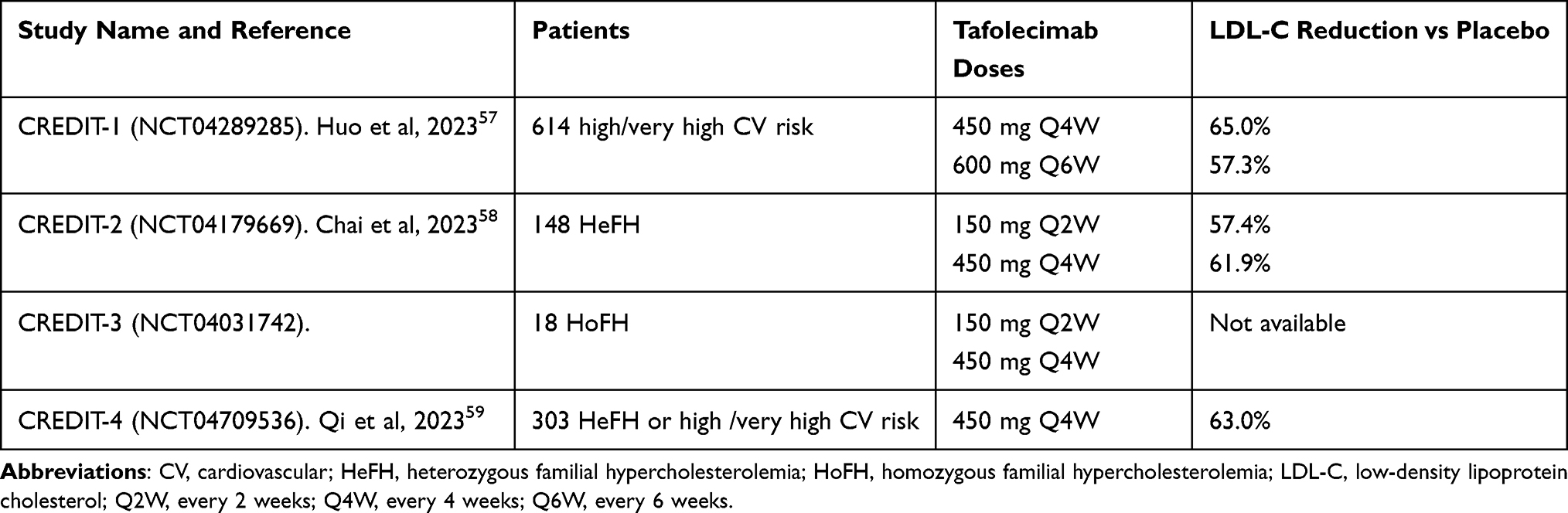 |
Table 2 Phase 3 Studies with Tafolecimab |
Pharmacokinetic data show that the median Tmax of tafolecimab was ≈ 4.7–7.5 days and the absolute bioavailability was about 58% after single SC doses of tafolecimab 150 mg, 450 mg, and 600 mg.56 The mean volume of distribution of tafolecimab at steady state was 5.7 L, the mean clearance was 0.162 L/day and the mean t1/2 was 26.1 days. Maximal reductions in PCSK9 levels from baseline (89.6–100%) were seen at 4–24 h after single SC or IV doses of tafolecimab and the duration of the reduction of PCSK9 was dose-dependent.55
A meta-analysis of the available randomized controlled trials (RCTs) with tafolecimab included three that evaluated the efficacy of tafolecimab 450 mg Q4W in 462 patients in comparison with placebo (N= 224) and indicated that tafolecimab resulted in a substantial decrease in LDL cholesterol at 12 weeks in comparison to placebo (mean difference = −63.8%, 95% CI −65.9% to −61.7%, p<0.00001).60 A greater number of patients in the tafolecimab cohort attained ≥50% decrease in LDL cholesterol and LDL cholesterol values below 1.8 mmol/L compared to the placebo cohort at week 12 and tafolecimab showed marked decreases in non-HDL cholesterol, apoB-100, and Lp(a) levels.
A review of the published literature on tafolecimab concluded that the efficacy data in a range of patients at high cardiovascular risk was satisfactory and the safety profile was good but the effect on cardiovascular outcomes remains to be elucidated.61 The recommended dosage of tafolecimab is 150 mg Q2W, 450 mg Q4W, or 600 mg Q6W. Whether the duration of action over six weeks is related to greater binding activity to PCSK9 or just the higher dose used has not been established.
Ongericimab
Ongericimab (JS002, Junshida®) is a recombinant anti-PCSK9 mAb developed by Junshi Biosciences. It is described as humanized in the publications but as fully human in the Approved for Marketing website. In October 2024 it was approved for marketing in China by the NMPA “for the treatment of adult patients with primary hypercholesterolemia (non-familial) and mixed dyslipidemia, who cannot achieve the recommended target of low-density lipoprotein cholesterol (LDL cholesterol) even after receiving moderate or high doses of statin therapy”. Not all the clinical trial results with ongericimab have been published.
Ongericimab was studied in a phase 1a single SC and IV dose study (JS002-001, NCT04197817) and a phase 1/2 multiple dose study (JS002-002, NCT04469673) to examine the pharmacokinetics and pharmacodynamics.62 Ongericimab exhibited non-linear kinetics, and as the dosage increased, the apparent clearance decreased, with terminal t1/2 values of 4.5–6.5 days.
A phase 3 trial (JS002-003, NCT04781114) was conducted in 806 Chinese patients with primary hypercholesterolemia or mixed dyslipidemia to evaluate the efficacy and safety of ongericimab as an additional treatment to stable and optimized lipid-lowering therapy.63 The patients were randomized to receive ongericimab 150 mg Q2W, ongericimab 300 mg Q4W or matching placebos for 52 weeks. The least-squares mean difference of percentage reduction in LDL cholesterol from baseline to week 24 compared to placebo for ongericimab 150 mg Q2W was 67.7% (p<0.0001) and for ongericimab 300 mg Q4W 61.2% (p<0.0001). These reductions were sustained up to week 52. No data on ADAs was reported. In addition, treatment with ongericimab had favorable effects on other lipid parameters including significant reductions in levels of non–HDL-C, apoB, and Lp(a) levels (45–68%) and increases in levels of HDL-C and apoA-1.
A phase 2 single arm, open label study (JS002-004, NCT04515927) was performed in 31 patients with HoFH diagnosed by clinical or genetic criteria, who were on stable lipid-lowering therapies for ≥4 weeks.64 Ongericimab 450 mg SC Q4W reduced LDL cholesterol from baseline overall by 12.6% (p=0.001) at week 12, and the mean (SD) LDL cholesterol reduction from baseline was 21.7 (28.0)% in 14 patients with defective LDLRs and 1.4 (9.6)% in 7 patients with negative LDLR. No serious adverse effects were reported.
In a phase 3 clinical trial (JS002-005, NCT05325203) in Chinese patients with definite HeFH according to Dutch Lipid Clinical Network criteria who were receiving stable lipid-lowering therapy, 135 patients were randomized to receive either ongericimab 150 mg Q2W, ongericimab 450 mg Q4W or the matching placebos for a total of 24 weeks.65 Compared to respective matching placebo groups, the least-squares mean reduction in LDL cholesterol for the ongericimab 150 mg Q2W group was 69.4% (p < 0.0001), and for the ongericimab 450 mg Q4W group it was 80.6% (p < 0.0001).65 Ongericimab showed favorably reductions in other lipid parameters including 50.0% reduction in Lp(a) levels.
The phase 3 study (JS002-006, NCT05532800) assessed the effectiveness and safety of SC ongericimab 150 mg Q2W administered by prefilled syringe (PFS) or autoinjector (AI) in 255 Chinese patients with primary hypercholesterolemia or mixed dyslipidemia on stable optimized lipid-lowering therapy.66 Compared to the respective matching placebo groups, the least squares mean percent reductions at week 12 were 72.7% (3.9%) for PFS and 71.1% (3.8%) for AI (both p < 0.001).66 Adverse events were similar with ongericimab compared with placebo.
There is an ongoing phase 3 study (JS002-007, NCT05621070) of ongericimab as monotherapy in patients with primary hypercholesterolemia or mixed dyslipidemia, which plans to recruit 582 subjects who will be randomized to SC ongericimab 150 mg Q2W or 450 mg Q4W or placebo comparators for a total of 52 weeks. Another phase 1 pharmacokinetic study (JS002-008-BE, NCT05859529) is comparing different delivery syringe devices. Ongericimab is a humanized mAb but there have been no reports of the development of ADAs or the attenuation of LDL cholesterol lowering effects in the clinical trials, some of which have continued for 52 weeks.
Ebronucimab
Ebronucimab (AK102) is a fully human IgG1 mAb targeting PCSK9 that was developed by Akeso Biopharma and AD Pharmaceuticals. It was approved by the NMPA in China “for treatment of primary hypercholesterolemia and mixed hyperlipidemia and heterozygous familial hypercholesterolemia in combination with statins or statins and other lipid-lowering therapies”, in September 2024.67
A phase 1 study (AK102-101, NCT04169386) in 32 healthy subjects involved single SC doses of ebronucimab (75, 150, 300 or 500 mg) or matching placebo.68 The median Tmax ranged from 2.0 to 6.0 days, t1/2 was within 4.11 to 5.01 days and maximum plasma concentration (Cmax), area under the plasma concentration time curve (AUC)0-t, and AUC0-∞ increased approximately in a dose-proportional manner. A total of 3 subjects were tested ADA positive at least once during the study.
A phase 2 dose finding and safety study (AK102-203, NCT04358432) was performed in patients with hyperlipidemia.69 A phase 2 study (AK102-202, NCT03933293) with ebronucimab in 10 patients with HoFH has been completed but has not been reported.
In a phase 3 trial (NCT05255094), 464 Chinese patients with primary hypercholesterolemia, including HeFH, or mixed dyslipidemia, were randomized to receive ebronucimab 450 mg Q4W, or 150 mg Q2W or matching placebos.70 The least squares mean reduction in LDL cholesterol from baseline to week 12 with ebronucimab 450 mg Q4W and ebronucimab 150 mg Q2W versus placebo was 59.13% (Adjusted p <0.0001) and 60.43% (Adjusted p <0.0001), respectively.71 The only treatment-associated adverse events that occurred more frequently in the ebronucimab dose groups were injection site reactions. Treatment emergent positive ADAs occurred in 4.9% (15/305), and neutralizing antibodies were positive in 3.9% (12/305). A number of other studies have been completed or are ongoing, but they have not been reported yet.
Recaticimab
Recaticimab (SHR-1209) is a humanized IgG1 mAb against PCSK9 that was developed by Jiangsu Hengrui Pharmaceuticals Co., Ltd. It was approved by the NMPA in China in January 2025. It features a preferred IgG1 protein subtype incorporating the YTE motif in the Fc region. This design enhances the drug’s specificity and affinity for PCSK9 while significantly extending its t1/2 in vivo. The YTE motif (M252Y/S254T/T256E) at the CH2-CH3 interface in the IgG1 Fc region is a prototypical example of a mutant in the Fc region of the antibody to increase association with the neonatal Fc receptor (FcRn), which leads to antibody recycling and minimal endosomal degradation.72 The benefit of incorporation of the YTE motif was first shown with motavizumab, an anti-respiratory syncytial virus monoclonal antibody, where the YTE Fc-modified antibody had a 2- to 4-fold increase in t1/2 compared to the original antibody and the t1/2 was extended up to 100 days in humans.73
The pharmacokinetics of recaticimab were studied in the phase 1b/2 trial (NCT03944109).74 The median Tmax ranged from 6.0 to 9.0 days after first administration of recaticimab and did not vary with the dose. The plasma t1/2 ranged from 18.6 to 22.1 days with the majority of doses and schedules, except with the 450 mg 12-weekly dose the geometric mean t1/2 was 27.4 days. There were no observable differences in the apparent total clearance (0.3 to 0.4 L/day) or the apparent volume of distribution (7.2 to 12.0 L) with different doses and schedules. The t1/2 of recaticimab was comparatively longer than that of evolocumab or alirocumab (evolocumab 11–17 days, alirocumab: 17–20 days).
A phase 1a study in 32 healthy volunteers (NCT03634436) showed that single doses of 51 to 450 mg recaticimab produced 50 to 65% reductions in LDL-C levels and was safe and well-tolerated.74 A phase 1b/2 study (NCT03944109) was performed in patients receiving a stable dose of atorvastatin and recaticimab reduced LDL cholesterol by up to 59.51%.74 Another phase 1 phase study (NCT05370950) in healthy subjects showed that single SC doses of 450 mg recaticimab given into different sites had similar pharmacokinetics and pharmacodynamics.75
The REMAIN-1 (REcaticimab MonotherApy in patIents with Nonfamilial hypercholesterolaemia and mixed hyperlipaemia; NCT04849000) was a phase 3 study of monotherapy with recaticimab in patients with non-FH hypercholesterolemia or mixed hyperlipidemia with a fasting LDL cholesterol level of ≥2.6 to <4.9 mmol/L, and a fasting triglyceride level of ≤5.6 mmol/L.76 Therapy with recaticimab at doses of 150 mg Q4W, 300 mg Q8W, and 450 mg Q12W or placebo was given for 24 weeks and reduced LDL cholesterol relative to placebo by 49.6%, 52.8% and 45.0%, respectively.
In the REMAIN-2 (Recaticimab Add-On Therapy in Patients with Non-Familial Hypercholesterolaemia and Mixed Hyperlipidemia, NCT04885218) phase 3 trial in 689 participants on stable moderate or high-intensity statin, with or without ezetimibe or fenofibrate for at least 4 weeks and with LDL cholesterol levels of ≥1.8 mmol/L with ASCVD or ≥2.6 mmol/L without ASCVD, recaticimab 150 mg Q4W, 300 mg Q8W, or 450 mg Q12W or placebo were given for 48 weeks.77 The mean reductions in LDL cholesterol compared to placebo at 24 weeks were 62.2%, 59.7%, and 53.4%, respectively, and the effects were maintained through week 48. The drug was well tolerated over a period of 48 weeks.
REMAIN-3 (NCT04844125) was a phase 3 study of recaticimab in 143 patients with heterozygous FH and poorly controlled LDL cholesterol on intensive lipid-lowering therapy.78 143 participants were randomized to receive recaticimab 150 mg SC Q4W or placebo for 12 weeks. The mean reduction in LDL cholesterol was 54.4% with the recaticimab group and 4.5% with placebo at 12 weeks with a treatment difference of 49.8% (p<0.0001). Recaticimab also reduced non-HDL cholesterol by 46.4%, apoB by 43.9% and Lp(a) by 36.9% relative to placebo. There was no significant effect on triglycerides.
The phase 3 studies with recaticimab are summarized in Table 3. There may be concern about the development of ADAs with this humanized mAb, but it appears this has not been a problem so far in the studies up to 24 weeks.
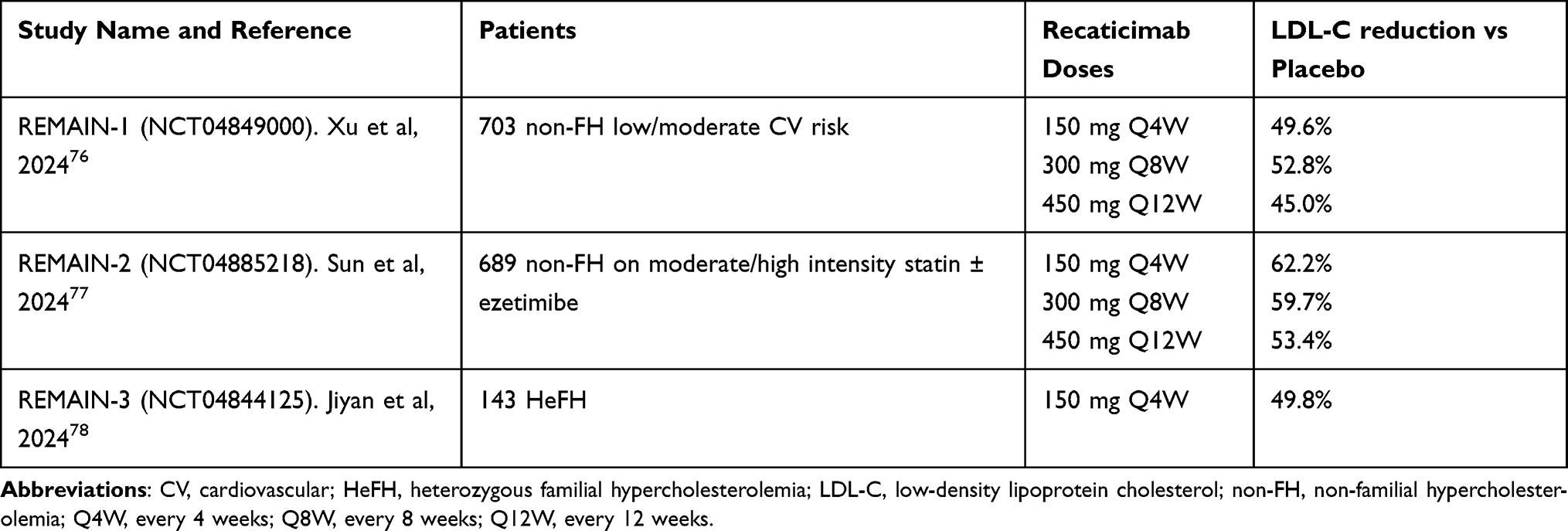 |
Table 3 Phase 3 Studies with Recaticimab |
Angiopoietin-Like 3 (ANGPTL3) Inhibitors
Angiopoietin-like proteins (ANGPTLs) control the relative activity of lipoprotein lipase (LPL) in various tissues and influence the distribution of lipoprotein-derived fatty acids between sites of fat storage or oxidation during feeding and fasting.79 In the Dallas Heart Study population, rare loss-of-function mutations in ANGPTL3, ANGPTL4, or ANGPTL5 were associated with low plasma triglyceride concentrations.79 Nonsense mutations in ANGPTL3 were also found in patients with combined hypolipidemia with extremely low levels of LDL cholesterol, HDL cholesterol, and triglycerides.80 ANGPTL8 is produced in the liver and adipose tissue and levels increase during feeding forming ANGPTL3/ANGPTL8 complexes that increase the inhibitory effect of ANGPTL3 on LPL in muscle. The effects of ANGPTL3/8 on LPL activity and LPL cleavage are much stronger than those of ANGPTL3 or ANGPTL8 alone.81 At the same time through formation of ANGPTL4/ANGPTL8 complexes ANGPTL8 blocks the inhibitory effect of ANGPTL4 on adipose tissue LPL, thereby increasing the uptake of fatty acids in adipose tissue in the postprandial state and reducing uptake in skeletal muscle.82
Familial combined hypolipidemia due to loss-of function mutations in the ANGPTL3 gene was shown to be inherited in a codominant manner and was associated with a substantial reduction of all plasma lipoproteins except for Lp(a).83 Genetic studies of loss-of-function variants in ANGPTL3 and therapeutic antagonism of Angptl3 with evinacumab in mice were associated with decreased lipid levels including triglycerides, LDL cholesterol, and HDL cholesterol and decreased odds of ASCVD.84 ANGPTL3 has therefore been recognized as a novel therapeutic target for lowering not only plasma triglycerides but also plasma LDL cholesterol.85
The mechanism by which reduced serum levels of ANGPTL3 reduce LDL cholesterol is not completely understood but it was assumed that neutralizing ANGPTL3 with a mAb might decrease hepatic very-low-density lipoprotein (VLDL) secretion and increase conversion of circulating triglyceride rich lipoproteins (TGRLs) to smaller particles that could be cleared by lipoprotein receptors other than the LDLR that include the LDL receptor-related protein, the remnant lipoprotein receptor, and the proteoglycan syndecan-1.86 Hepatic uptake of lipid particles via an endothelial lipase (EL) based mechanism has also been suggested, as ANGPTL3 inhibits EL.87
Various pharmacological strategies have been developed to inhibit ANGPTL3 for the treatment of dyslipidemia. These include the mAbs, evinacumab and SHR-1819, the antisense oligonucleotide (ASO), vupanorsen, the small interfering RNA (siRNA) molecules, zodasiran and solbinsiran, and a CRISPR genome editing system (Figure 2).88 It may be possible to develop oral small-molecule inhibitors in the future.
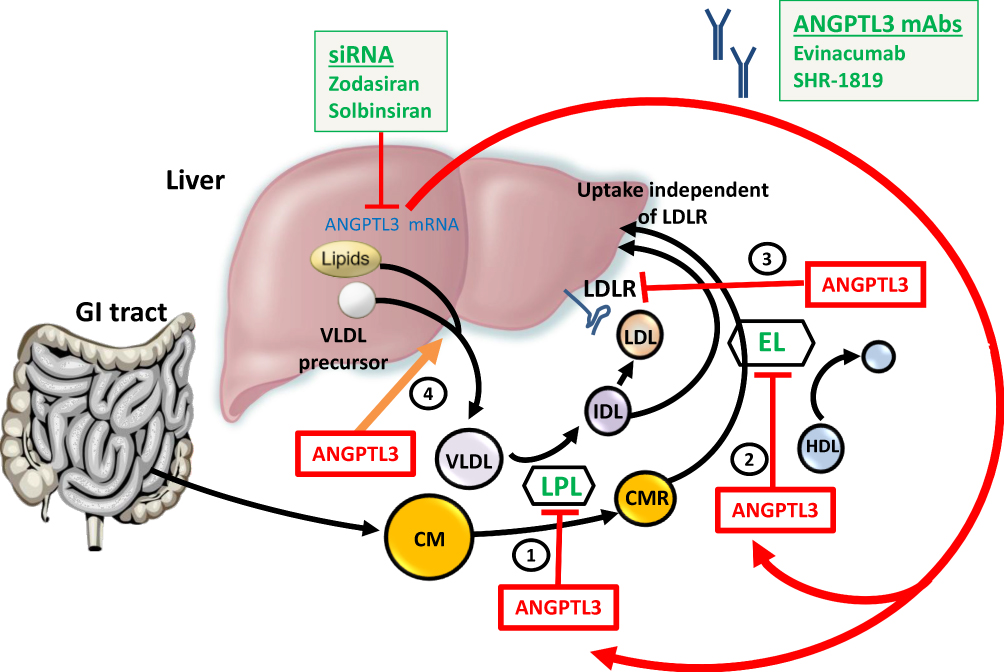 |
Figure 2 Action of angiopoietin-like protein 3 (ANGPTL3) in lipoprotein metabolism. ANGPTL3 inhibits 1) lipoprotein lipase and 2) endothelial lipase. It may also 3) inhibit the liver uptake of LDL particles and 4) stimulate release of VLDL particles from the liver. Inhibition of ANGPTL3 in the absence of functioning LDL receptors facilitates uptake by the liver of remnant particles and LDL via an endothelial lipase-dependent mechanism. Abbreviations: ANGPTL3, angiopoietin-like 3; CM, chylomicron; CMR, chylomicron remnant; EL, endothelial lipase; HDL, high-density lipoprotein; IDL, intermediate-density lipoprotein; LDL, low-density lipoprotein; LDLR, low-density lipoprotein receptor; LPL, lipoprotein lipase; VLDL, very low-density lipoprotein. |
Inhibiting ANGPTL3 or apolipoprotein C3 (apoC3) was expected to be effective in reducing triglyceride levels rather than LDL cholesterol.89 However, the effects of inhibiting ANGPTL3 appear to vary with the lipid phenotype of the patients involved and probably with the degree of ANGPTL3 inhibition. Vupanorsen looked promising in early phase studies but in the phase 2b Vupanorsen in Statin-Treated Patients With Elevated Cholesterol: TaRgeting ANGPTL3 with an aNtiSense oLigonucleotide in AdulTs with dyslipidEmia (TRANSLATE-TIMI 70, NCT04516291) study in patients on statin therapy with combined hyperlipidemia, there were only modest reductions in LDL cholesterol of 7.9 to 16.0% and in apoB of 6.0 to 15.1%, and there were dose-dependent increases in liver fat, and higher doses were associated with elevations in liver enzymes.90 In January 2022, the clinical development program for vupanorsen led by Pfizer was terminated.91
The siRNA ANGPTL3 inhibitor zodasiran showed favorable lipid effects in patients with mixed hyperlipidemia in the phase 2b ARCHES-2 trial (NCT04832971).92 However, the manufacturer, Arrowhead Pharmaceuticals, decided to limit development of zodasiran in favor of plozasiran, which inhibits apoC3, which may have a wider application.93 Zodasiran is being investigated in HoFH.
Another GalNAc-conjugated siRNA targeting ANGPTL3 developed by Eli Lilly, solbinsiran, was recently shown to result in durable reductions in serum ANGPTL3, apoB, triglyceride, VLDL cholesterol, non-HDL cholesterol and in hepatic fat fraction in adults with mixed dyslipidemia in the phase 2 PROLONG-ANG3 trial (NCT05256654).94
CRISPR Therapeutics’ CTX310 is a CRISPR/Cas9 gene editing treatment designed to target hepatic expression of ANGPTL3. It consists of Cas9 mRNA and guide RNA (gRNA) which target ANGPTL3 encapsulated into lipid nanoparticles.95 It showed reductions of more than 80% in LDL cholesterol and triglycerides after a single dose in a trial involving patients with certain conditions associated with elevated lipid levels. VERVE-201 is a gene editing therapy composed of an mRNA encoding an adenine base editor and a guide RNA targeting the ANGPTL3 gene packaged in a GalNAc lipid nanoparticle developed by Verve Therapeutics.96
Evinacumab
Evinacumab (REGN1500, Evkeeza®, Regeneron Pharmaceuticals, Inc.) is a fully human mAb with a human IgG4 constant region. It was designed using Regeneron’s Velocimmune® technology platform.97 It shows high affinity to ANGPTL3 from mouse, rat, monkey, and humans. Evinacumab binds to ANGPTL3 in the circulation to create immune complexes and the primary mechanism of action is likely to be potentiation of LPL activity.98 It is also able to bind to the ANGPTL3/ ANGPTL8 complex although with less potency than an anti-ANGPTL3/8 antibody.99 ANGPTL3 circulates at about 200 ng/mL whereas ANGPTL3/8 complexes are approximately 20 ng/mL, therefore the dose of evinacumab required would be higher than that for a specific anti-ANGPTL3/8 antibody.99
Early phase studies showed that evinacumab was not only effective in reducing triglycerides but was also able to lower LDL cholesterol in patients with HoFH. It was approved by the FDA for HoFH in February 2021.100 It was approved for medical use in the European Union in June 2021. In 2021, Regeneron announced that the annual wholesale cost of the drug given by IV infusion every 4 weeks would be $450 000 on average, therefore additional indications in lower risk subjects may be difficult to support.100
A phase 1 single ascending dose (SAD) study (NCT01749878) included 83 human volunteers with moderately high triglycerides (>1.7 but ≤5.1 mmol/L, >150 but ≤450 mg/dL) and/or LDL cholesterol (≥2.6 mmol/L, ≥100 mg/dL) and showed dose-dependent reductions in triglycerides up to 76%, in LDL cholesterol up to 23% and in HDL cholesterol up to 25% with evinacumab compared to placebo.84 The SAD study results in 83 subjects and a phase 1 multiple ascending dose (MAD) study in 56 dyslipidemic subjects (NCT02107872) were reported in 2019.101 Evinacumab 150, 300 or 450 mg Q1W, and 300 or 450 mg Q2W was given by SC injection or 20 mg/kg Q4W by IV injection. The maximum reduction in triglycerides was 83.1% at day 2 with 20 mg/kg IV Q4W.101 The reductions in LDL cholesterol were up to 25.1% in the MAD study and HDL cholesterol was also reduced to a variable extent versus placebo with the SC doses and by 6.2% with evinacumab IV at 20 mg/kg Q4W.
In a phase 1 study which compared the pharmacokinetics, pharmacodynamics, safety, and tolerability of evinacumab in four dose cohorts between healthy Japanese and Caucasian adults with baseline LDL cholesterol ≥2.6 and <4.1 mmol/L (≥100 and <160 mg/dL), the pharmacokinetic profiles for both SC and IV doses of evinacumab were comparable in both ethnic groups and evinacumab was generally well tolerated and the dose-related reductions in LDL cholesterol and triglycerides were similar in both groups.102
In a phase 2 open-label, proof-of-concept study (NCT02265952) that included 9 adults with HoFH taking aggressive lipid-lowering therapy, evinacumab was administered as 250 mg SC on day 1, 15 mg/kg IV on day 15, and 450 mg SC Q1W x 4, starting from day 85.103 The mean (±SD) reductions in lipids levels at week 4 were 49±23% in LDL cholesterol, 46±18% in apoB, 49±22% in non-HDL cholesterol, 36±16% in HDL cholesterol and a median reduction of 47% in triglycerides. An additional analysis of this study showed that evinacumab was effective in lowering LDL cholesterol in the HoFH patients regardless of the type of mutation in the LDLR and LDLR activity was not affected so the mechanism appeared to be independent of the LDLR.101
A phase 2 trial in patients with severe hypertriglyceridemia (fasting triglyceride ≥500 mg/dL) who had a history of hospitalization for acute pancreatitis (NCT03452228) included 17 patients with familial chylomicronemia syndrome (FCS), 15 patients with multifactorial chylomicronemia syndrome who had heterozygous loss-of-function mutations in the LPL pathway and 19 patients with multifactorial chylomicronemia syndrome without mutations in the LPL pathway.104 Evinacumab treatment at 15 mg /kg IV Q4W for 12 weeks reduced triglycerides by a variable extent among the 3 cohorts. It had the greatest effect versus placebo in those with no LPL mutations (median 81.7% reduction versus increase of 80.9%), a smaller effect in those with heterozygous LPL pathway mutations (64.8% reduction versus increase of 9.4%), and no significant effect in those with FCS (27.7% reduction versus 22.9% reduction).104 LDL cholesterol tended to increase with evinacumab treatment but this was not significant compared to placebo in any of the three groups of patients with hypertriglyceridemia.
In the phase 3 ELIPSE HoFH (Efficacy and Safety of Evinacumab in Patients With Homozygous Familial Hypercholesterolemia) trial (NCT03399786), evinacumab was evaluated in 65 patients with HoFH on multiple lipid-lowering therapies.105 Evinacumab given at 15 mg/kg IV Q4W reduced LDL cholesterol compared with placebo by a mean of 49% after 24 weeks. Triglyceride levels also decreased by 55% with evinacumab compared to a 4.6% reduction in the placebo group and there was a 30% reduction in HDL cholesterol levels with evinacumab. The effects on LDL cholesterol were similar in the patients with complete LDLR deficiency (null-null) compared to those with residual LDLR activity (non-null). The rates of adverse events were similar in the evinacumab group compared to the placebo group.
A substudy from ELIPSE HoFH (NCT04722068), included four patients with HoFH who underwent apoB kinetic analyses. This showed an increase in the fractional catabolic rate of intermediate-density lipoprotein (IDL)-apoB and LDL-apoB, suggesting that evinacumab lowers LDL cholesterol predominantly by increasing the clearance of apoB-containing lipoprotein from the circulation.106 Another substudy involved two severely affected young HoFH patients who had coronary computed tomography angiography (CCTA) before and after 6 months of treatment, showed substantial reduction of plaques after intensive lipid lowering therapy including statins, ezetimibe, LDL apheresis, and evinacumab.107
In an open-label treatment period of the ELIPSE HoFH study in 65 patients with HoFH who continued treatment with evinacumab 15 mg/kg IV Q4W for 48 weeks, the mean reduction in LDL cholesterol was 46.3% and evinacumab was generally well tolerated.108
In a single-arm, open-label, phase 3 trial (NCT03409744) in 116 patients with HoFH, including 102 adults and 14 adolescents, treated with IV evinacumab 15 mg/kg Q4W for a median of 104.3 weeks, the mean reduction in LDL cholesterol at 24 weeks was 43.6% and evinacumab was generally well tolerated.109
In a phase 3 open-label study in 6 pediatric patients with mean age 8.8 years given a single dose of IV evinacumab 15 mg/kg, and 14 pediatric patients aged 5 to 11 years treated with IV evinacumab 15 mg/kg Q4W, all with genetically proven HoFH (NCT04233918), the mean reduction in LDL cholesterol at 8 weeks after the single dose was 41.6% and at 24 weeks of multiple dosing the reductions were LDL cholesterol 48.3%, apoB 41.3%, non-HDL cholesterol 48.9% and TC 49.1%.110
Evinacumab tended to reduce HDL cholesterol in some of the studies and this was significant in a meta-analysis of five of the early randomized controlled trials.111 The main phase 2 and phase 3 trials with evinacumab are summarized in Table 4.
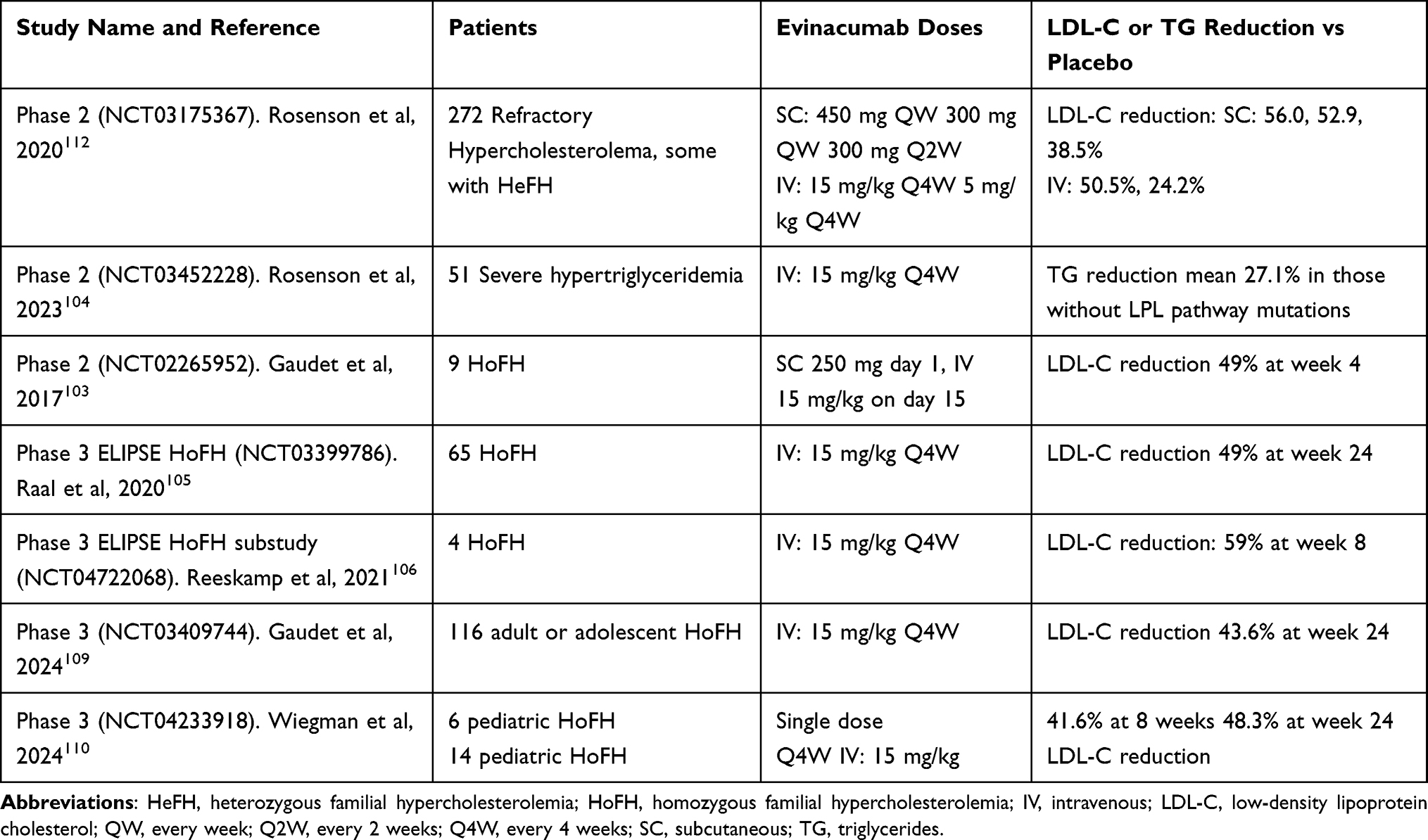 |
Table 4 Phase 2 and 3 Studies with Evinacumab |
SHR-1918
SHR-1918 is a fully human mAb targeting ANGPTL3 developed by Jiangsu Hengrui Pharmaceuticals Co., Ltd and Beijing Suncadia Pharmaceuticals Co., Ltd. It received breakthrough therapy designation (BTD) from the Chinese NMPA in September 2024 for the treatment of HoFH.
In a phase 1 SAD study (SHR-1918-101, NCT05432544) in 72 healthy subjects, SC doses of SHR-1918 from 100 to 1200 mg produced maximum reductions in LDL cholesterol from baseline ranging from 46.5% to 49.1%, and the maximum reduction in triglycerides ranged from 67.4% to 82.8%. The reduction in LDL cholesterol remained at 36.9% to 39.0% on Day 85 and for the higher doses, the reduction in triglycerides was 59.9% to 79.1%.113
In a phase 2 study (SHR-1918-201, NCT06109831) in 333 patients with hyperlipidemia at moderate or higher risk of ASCVD who were mainly on a moderate-intensity dose of statin and not at target LDL cholesterol levels, the patients were randomized to receive SC doses of SHR-1918 150, 300, or 600 mg Q4W or 600 mg Q8W or matching placebos for a total of 16 weeks.114 SHR-1918 reduced serum LDL cholesterol by 22% to 30%, as well as triglyceride levels by 52% to 63% with the effect being dose and frequency dependent. There were also reductions in TC, non-HDL cholesterol, HDL cholesterol, apoA-I but not Lp(a).
A phase 2 open-label, single-arm study (SHR-1918-202, NCT06009393) to evaluate the efficacy and safety of SHR-1918 in 20 patients with HoFH appears to have been completed but not published. A phase 2 study in 44 subjects with hyperlipidemia (SHR-1918-203, NCT06471218) using 2 doses of SHR-1918 over 24 weeks is underway.
A phase 3 randomized, double-blind, placebo-controlled, multicenter clinical trial (SHR-1918-301, NCT06723652) in 45 patients with HoFH has been launched to evaluate the efficacy and safety of SHR-1918 in this condition. Participants will switch from placebo to SHR-1918 after 12 weeks and continue for a total of 24 weeks. The primary endpoint is the percentage change in LDL cholesterol levels from baseline at week 12.
Other ANGPTL Inhibitors
ANGPTL4 has been considered as another target for therapy as carriers of ANGPTL4 gene inactivating mutations had lower levels of triglycerides and a lower risk of coronary heart disease (CHD) than did noncarriers.115 Inhibition of Angptl4 in mice and monkeys with the human mAb REGN1001 also resulted in reductions in triglyceride values, but this was associated with lipid accumulation in the mesenteric lymph nodes and abdominal lymphadenopathy secondary to granulomatous lipid accumulation.115 Previous studies of Angptl4 knockout mice or mice treated with the anti-Angptl4 mAb 14D12 also showed lipogranulomatous lesions of the intestines and their draining lymphatics and mesenteric lymph nodes.116 These findings might suggest that ANGPTL4 may not be a useful therapeutic target, but Mendelian randomization analysis showed genetic mimicry of inhibition of ANGPTL4 and enhancement of LPL have similar systemic metabolic effects and were associated with a lower risk of type 2 diabetes and CHD.117
MAR001
MAR001, developed by Marea Therapeutics, Inc., is a first-in-class humanized mAb targeting ANGPTL4, which is highly expressed in adipose tissue. Studies in hypertriglyceridemic non-human primates showed that single doses of MAR001 reduced plasma triglycerides by up to 58%, non-HDL cholesterol by 38% and apoB by 30%.118 Animals fed a high-saturated-fat diet showed only minimal to moderate foamy macrophage formation in mesenteric lymph nodes, and these histological changes did not progress to degeneration, necrosis, inflammation, fibrosis, or other reactive changes, and there was no evidence of systemic inflammation.
MAR001 was evaluated in a single-ascending-dose phase 1 study in 3 groups of participants, 32 healthy participants, 12 subjects with high BMI (30–40 kg/m²) and 12 subjects with fasting triglycerides in the range of 200–500 mg/dL.119 The doses of SC MAR001 given to healthy participants were 15, 50, 150 or 450 mg and only 450 mg and placebo were used in the other groups. In the high triglyceride cohort, placebo-adjusted mean reductions in fasting triglyceride were 68·6% on day 15.
In the phase 1b/2a multidose randomized, double-blind, placebo-controlled study (NCT05896254), 55 participants with metabolic dysfunction were randomized to receive seven SC injections of placebo or doses of MAR001 at 150, 300 or 450 mg Q2W, followed by a 12-week safety follow-up period.119 At week 12, the placebo adjusted mean reduction in triglycerides was 52·7% and in remnant cholesterol 52·5% with MAR001 450 mg. No treatment-related systemic inflammatory biomarker elevations were seen and no changes in mesenteric lymph node size or inflammation assessed by MRI were observed.119
LY3475766 is a mAb targeting the ANGPTL3/8 complex developed by Eli Lilly. A phase 1 study in subjects with mixed hyperlipidemia showed that single doses of LY3475766 of 10–30 mg IV or 100, 300 and 600 mg SC, dose-dependently reduced plasma triglycerides and LDL cholesterol levels up to 70% and 35%, respectively, and increased HDL cholesterol levels up to 25%.120
Conclusion
The fully human mAbs targeting PCSK9, evolocumab and alirocumab, are well established with a good long-term safety record and with evidence for reduction of cardiovascular events. They are particularly useful in patients with HeFH but have limited effect in lowering LDL cholesterol in the rare patients with HoFH. Tafolecimab and ebronucimab are fully human mAbs and ongericimab and recaticimab are humanized mAbs targeting PCSK9 developed and approved in China. They have not been subjected to cardiovascular outcome studies. Recaticimab has a longer duration of action compared to alirocumab and evolocumab, which is probably related to the YTE motif in the Fc region. This provides the advantage of less frequent dosing. Whether the humanized mAbs will result in ADAs causing reduced function as with bococizumab is not certain. This does not appear to be a problem with the results currently available, but there is limited information on long-term usage. It is not known if these new mAbs will be approved in other countries in addition to China.
The mAbs targeting PCSK9 are highly efficacious but generally quite expensive, which limits their use in many parts of the world. Having more options is likely to make the drugs more affordable and this will apply in China but not elsewhere at present. The siRNA inclisiran can be given twice yearly in the long term, which should improve adherence to therapy considerably. However, the yearly cost is similar to that of the mAbs and it is not currently available in all countries. If the oral drugs inhibiting PCSK9 prove to have satisfactory long-term safety and efficacy in reducing cardiovascular events, they may offer an attractive alternative to the mAbs depending on the cost.
ANGPTL3 has been identified as a target for the treatment of HoFH. Evinacumab has been approved for this indication and SHR-1918 is being developed in China with the same target. These mAbs can reduce LDL cholesterol by about 50% in patients with HoFH and although this may not be adequate to reach LDL cholesterol targets it will usually reduce the requirement for lipoprotein apheresis. Evinacumab is expensive and is unlikely to be used for other indications although it may be useful in hypertriglyceridemia and mixed hyperlipidemia. SHR-1918 appears to have effects similar to evinacumab and could be used for much wider indications depending on the cost. It is likely to be approved in China and could be launched in other countries. MAR001, a humanized mAb targeting ANGPTL4, is at a very early stage of development and its role remains to be established.
Acknowledgments
This paper was funded partially from research funding from Macau University of Science and Technology. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Martin SS, Aday AW, Allen NB, et al. 2025 heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2025;151(8):e41–e660. doi:10.1161/CIR.0000000000001303
2. Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European atherosclerosis society consensus panel. Eur Heart J. 2017;38(32):2459–2472. doi:10.1093/eurheartj/ehx144
3. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366(9493):1267–1278. doi:10.1016/S0140-6736(05)67394-1
4. Baigent C, Blackwell L; Cholesterol Treatment Trialists C. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670–1681. doi:10.1016/S0140-6736(10)61350-5
5. Stroes ES, Thompson PD, Corsini A, et al. Statin-associated muscle symptoms: impact on statin therapy-European atherosclerosis society consensus panel statement on assessment, aetiology and management. Eur Heart J. 2015;36(17):1012–1022. doi:10.1093/eurheartj/ehv043
6. Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet. 2010;375(9716):735–742. doi:10.1016/S0140-6736(09)61965-6
7. Mach F, Ray KK, Wiklund O, et al. Adverse effects of statin therapy: perception vs. the evidence - focus on glucose homeostasis, cognitive, renal and hepatic function, haemorrhagic stroke and cataract. Eur Heart J. 2018;39(27):2526–2539. doi:10.1093/eurheartj/ehy182
8. De Backer G, Jankowski P, Kotseva K, et al. Management of dyslipidaemia in patients with coronary heart disease: results from the ESC-EORP EUROASPIRE V survey in 27 countries. Atherosclerosis. 2019;285:135–146. doi:10.1016/j.atherosclerosis.2019.03.014
9. Ray KK, Molemans B, Schoonen WM, et al. EU-wide cross-sectional observational study of lipid-modifying therapy use in secondary and primary care: the DA VINCI study. Eur J Prev Cardiol. 2021;28(11):1279–1289. doi:10.1093/eurjpc/zwaa047
10. Mach F, Koskinas KC, Roeters van Lennep JE, et al. 2025 focused update of the 2019 ESC/EAS guidelines for the management of dyslipidaemias: developed by the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J. 2025. doi:10.1093/eurheartj/ehaf190
11. Ray KK, Aguiar C, Arca M, et al. Use of combination therapy is associated with improved LDL cholesterol management: 1-year follow-up results from the European observational SANTORINI study. Eur J Prev Cardiol. 2024;31(15):1792–1803. doi:10.1093/eurjpc/zwae199
12. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41:111–188. doi:10.1093/eurheartj/ehz455
13. Virani SS, Akeroyd JM, Smith SC, et al. Very high-risk ASCVD and eligibility for nonstatin therapies based on the 2018 AHA/ACC cholesterol guidelines. J Am Coll Cardiol. 2019;74(5):712–714. doi:10.1016/j.jacc.2019.05.051
14. Davis HR, Veltri EP. Zetia: inhibition of Niemann-Pick C1 Like 1 (NPC1L1) to reduce intestinal cholesterol absorption and treat hyperlipidemia. J Atheroscler Thromb. 2007;14(3):99–108. doi:10.5551/jat.14.99
15. Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372(25):2387–2397. doi:10.1056/NEJMoa1410489
16. Giugliano RP, Cannon CP, Blazing MA, et al. Benefit of adding ezetimibe to statin therapy on cardiovascular outcomes and safety in patients with versus without diabetes mellitus: results from IMPROVE-IT (Improved Reduction of Outcomes: vytorin Efficacy International Trial). Circulation. 2018;137(15):1571–1582. doi:10.1161/CIRCULATIONAHA.117.030950
17. Ballantyne CM, Bays H, Catapano AL, Goldberg A, Ray KK, Saseen JJ. Role of bempedoic acid in clinical practice. Cardiovasc Drugs Ther. 2021;35(4):853–864. doi:10.1007/s10557-021-07147-5
18. Nissen SE, Lincoff AM, Brennan D, et al. Bempedoic acid and cardiovascular outcomes in statin-intolerant patients. N Engl J Med. 2023;388(15):1353–1364. doi:10.1056/NEJMoa2215024
19. Abifadel M, Varret M, Rabes JP, et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet. 2003;34(2):154–156. doi:10.1038/ng1161
20. Seidah NG, Benjannet S, Wickham L, et al. The secretory proprotein convertase neural apoptosis-regulated convertase 1 (NARC-1): liver regeneration and neuronal differentiation. Proc Natl Acad Sci U S A. 2003;100(3):928–933. doi:10.1073/pnas.0335507100
21. Hobbs HH, Cohen JC, Horton JD. PCSK9: from nature’s loss to patient’s gain. Circulation. 2024;149(3):171–173. doi:10.1161/CIRCULATIONAHA.123.064498
22. Cohen JC, Boerwinkle E, Mosley TH Jr, Hobbs HH. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006;354(12):1264–1272. doi:10.1056/NEJMoa054013
23. Cohen J, Pertsemlidis A, Kotowski IK, Graham R, Garcia CK, Hobbs HH. Low LDL cholesterol in individuals of African descent resulting from frequent nonsense mutations in PCSK9. Nat Genet. 2005;37(2):161–165. doi:10.1038/ng1509
24. Ridker PM, Tardif JC, Amarenco P, et al. Lipid-reduction variability and antidrug-antibody formation with bococizumab. N Engl J Med. 2017;376(16):1517–1526. doi:10.1056/NEJMoa1614062
25. Tomlinson B, Chow E, Chan P, Lam CWK. An evaluation of the pharmacokinetics of inclisiran in the treatment of atherosclerotic cardiovascular disease. Expert Opin Drug Metab Toxicol. 2021;17(12):1353–1361. doi:10.1080/17425255.2021.2029402
26. Ray KK, Wright RS, Kallend D, et al. Two phase 3 trials of inclisiran in patients with elevated LDL cholesterol. N Engl J Med. 2020;382(16):1507–1519. doi:10.1056/NEJMoa1912387
27. Ballantyne CM, Banka P, Mendez G, et al. Phase 2b randomized trial of the oral PCSK9 inhibitor MK-0616. J Am Coll Cardiol. 2023;81(16):1553–1564. doi:10.1016/j.jacc.2023.02.018
28. Koren MJ, Vega RB, Agrawal N, et al. An oral PCSK9 inhibitor for treatment of hypercholesterolemia. J Am Coll Cardiol. 2025;85(21):1996–2007. doi:10.1016/j.jacc.2025.03.499
29. Raal F, Fourie N, Scott R, et al. Long-term efficacy and safety of lerodalcibep in heterozygous familial hypercholesterolaemia: the LIBerate-HeFH trial. Eur Heart J. 2023;44(40):4272–4280. doi:10.1093/eurheartj/ehad596
30. Kereiakes D, Fourie N, Engelbrecht J, et al. Long term efficacy and safety of lerodalcibep in patients with atherosclerotic cardiovascular disease (liberate-CVD). Atherosclerosis. 2024:395. doi:10.1016/j.atherosclerosis.2024.118513
31. Hooper AJ, Tang XL, Burnett JR. VERVE-101, a CRISPR base-editing therapy designed to permanently inactivate hepatic PCSK9 and reduce LDL-cholesterol. Expert Opin Investig Drugs. 2024;33(8):753–756. doi:10.1080/13543784.2024.2369747
32. Gidding SS, Champagne MA, de Ferranti SD, et al. The agenda for familial hypercholesterolemia: a scientific statement from the American Heart Association. Circulation. 2015;132(22):2167–2192. doi:10.1161/CIR.0000000000000297
33. Cuchel M, Raal FJ, Hegele RA, et al. 2023 update on European atherosclerosis society consensus statement on homozygous familial hypercholesterolaemia: new treatments and clinical guidance. Eur Heart J. 2023;44(25):2277–2291. doi:10.1093/eurheartj/ehad197
34. Ridker PM, Amarenco P, Brunell R, et al. Evaluating bococizumab, a monoclonal antibody to PCSK9, on lipid levels and clinical events in broad patient groups with and without prior cardiovascular events: rationale and design of the studies of PCSK9 Inhibition and the Reduction of vascular Events (SPIRE) lipid lowering and SPIRE cardiovascular outcomes trials. Am Heart J. 2016;178:135–144. doi:10.1016/j.ahj.2016.05.010
35. Ballantyne CM, Neutel J, Cropp A, et al. Results of Bococizumab, A monoclonal antibody against proprotein convertase subtilisin/kexin type 9, from a randomized, placebo-controlled, dose-ranging study in statin-treated subjects with hypercholesterolemia. Am J Cardiol. 2015;115(9):1212–1221. doi:10.1016/j.amjcard.2015.02.006
36. Ridker PM, Revkin J, Amarenco P, et al. Cardiovascular efficacy and safety of bococizumab in high-risk patients. N Engl J Med. 2017;376(16):1527–1539. doi:10.1056/NEJMoa1701488
37. Ferri N, Corsini A, Sirtori CR, Ruscica M. Bococizumab for the treatment of hypercholesterolaemia. Expert Opin Biol Ther. 2017;17(7):909–910. doi:10.1080/14712598.2017.1330849
38. Chasman DI, Hyde CL, Giulianini F, et al. Genome-wide pharmacogenetics of anti-drug antibody response to bococizumab highlights key residues in HLA DRB1 and DQB1. Sci Rep. 2022;12(1):4266. doi:10.1038/s41598-022-07997-5
39. Tomlinson B, Hu M, Zhang Y, Chan P, Liu ZM. Evolocumab for the treatment of hypercholesterolemia. Expert Opin Biol Ther. 2017;17(11):1447–1461. doi:10.1080/14712598.2017.1365134
40. Stein EA, Giugliano RP, Koren MJ, et al. Efficacy and safety of evolocumab (AMG 145), a fully human monoclonal antibody to PCSK9, in hyperlipidaemic patients on various background lipid therapies: pooled analysis of 1359 patients in four phase 2 trials. Eur Heart J. 2014;35(33):2249–2259. doi:10.1093/eurheartj/ehu085
41. Langslet G, Emery M, Wasserman SM. Evolocumab (AMG 145) for primary hypercholesterolemia. Expert Rev Cardiovasc Ther. 2015;13(5):477–488. doi:10.1586/14779072.2015.1030395
42. Stein EA, Wasserman SM, Dias CS, Scott R, Raal F. AMG-145. Drugs Future. 2013;38(7):451–459. doi:10.1358/dof.2013.038.07.1981967
43. Repatha (evolocumab) injection prescribing information 2015. August 27, 2015. Amgen. Available from: http://pi.amgen.com/united_states/repatha/repatha_pi_hcp_english.pdf.
44. Raal FJ, Honarpour N, Blom DJ, et al. Inhibition of PCSK9 with evolocumab in homozygous familial hypercholesterolaemia (TESLA Part B): a randomised, double-blind, placebo-controlled trial. Lancet. 2015;385(9965):341–350. doi:10.1016/S0140-6736(14)61374-X
45. Raal FJ, Hovingh GK, Blom D, et al. Long-term treatment with evolocumab added to conventional drug therapy, with or without apheresis, in patients with homozygous familial hypercholesterolaemia: an interim subset analysis of the open-label TAUSSIG study. Lancet Diabetes Endocrinol. 2017;5(4):280–290. doi:10.1016/S2213-8587(17)30044-X
46. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722. doi:10.1056/NEJMoa1615664
47. Giugliano RP, Mach F, Zavitz K, et al. Cognitive function in a randomized trial of evolocumab. N Engl J Med. 2017;377(7):633–643. doi:10.1056/NEJMoa1701131
48. Roth EM, Diller P. Alirocumab for hyperlipidemia: physiology of PCSK9 inhibition, pharmacodynamics and Phase I and II clinical trial results of a PCSK9 monoclonal antibody. Future Cardiol. 2014;10(2):183–199. doi:10.2217/fca.13.107
49. Tomlinson B, Hu M, Zhang Y, Chan P, Liu ZM. Alirocumab for the treatment of hypercholesterolemia. Expert Opin Biol Ther. 2017;17(5):633–643. doi:10.1080/14712598.2017.1305354
50. Praluent. Highlights of prescribing information. 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/125559s001lbl.pdf.
51. Roth EM. Alirocumab for hyperlipidemia: ODYSSEY Phase III clinical trial results and US FDA approval indications. Future Cardiol. 2016;12(2):115–128. doi:10.2217/fca.15.78
52. Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. 2018;379(22):2097–2107. doi:10.1056/NEJMoa1801174
53. Robinson JG, Rosenson RS, Farnier M, et al. Safety of very low low-density lipoprotein cholesterol levels with alirocumab: pooled data from randomized trials. J Am Coll Cardiol. 2017;69(5):471–482. doi:10.1016/j.jacc.2016.11.037
54. Jones PH, Bays HE, Chaudhari U, et al. Safety of Alirocumab (A PCSK9 Monoclonal Antibody) from 14 randomized trials. Am J Cardiol. 2016;118(12):1805–1811. doi:10.1016/j.amjcard.2016.08.072
55. Cui Y, Zhao X, Qi L, et al. A potential long-acting LDL-cholesterol–lowering PCSK9 monoclonal antibody. JACC. 2021;1(3):411–415. doi:10.1016/j.jacasi.2021.09.002
56. Keam SJ. Tafolecimab: first Approval. Drugs. 2023;83(16):1545–1549. doi:10.1007/s40265-023-01952-y
57. Huo Y, Chen B, Lian Q, et al. Tafolecimab in Chinese patients with non-familial hypercholesterolemia (CREDIT-1): a 48-week randomized, double-blind, placebo-controlled phase 3 trial. Lancet Reg Health West Pac. 2023;41:100907. doi:10.1016/j.lanwpc.2023.100907
58. Chai M, He Y, Zhao W, et al. Efficacy and safety of tafolecimab in Chinese patients with heterozygous familial hypercholesterolemia: a randomized, double-blind, placebo-controlled phase 3 trial (CREDIT-2). BMC Med. 2023;21(1):77. doi:10.1186/s12916-023-02797-8
59. Qi L, Liu D, Qu Y, et al. Tafolecimab in Chinese patients with hypercholesterolemia (CREDIT-4): a randomized, double-blind, placebo-controlled phase 3 trial. JACC Asia. 2023;3(4):636–645. doi:10.1016/j.jacasi.2023.04.011
60. Fatima E, Qureshi Z, Khanzada M, Safi A, Rehman OU, Altaf F. The efficacy of tafolecimab in chinese patients with hypercholesterolemia: a systematic review and meta-analysis. Am J Cardiovasc Drugs. 2024;24(5):641–650. doi:10.1007/s40256-024-00654-4
61. Tafolecimab LJJ. A novel member of PCSK9 monoclonal antibodies, is worth expecting in a chinese population. JACC Asia. 2023;3(4):646–648. doi:10.1016/j.jacasi.2023.06.002
62. Jiang J, Xu L, Chai L, et al. Clinical pharmacokinetics and pharmacodynamics of ongericimab: a potential long-acting PCSK9 monoclonal antibody in healthy subjects and patients with hypercholesterolemia: randomized, double-blind, placebo-controlled phase Ia and Ib/II studies. Clin Transl Sci. 2024;17(11):e70061. doi:10.1111/cts.70061
63. Wang X, Qiu M, Cheng Z, et al. Efficacy and safety of ongericimab in chinese patients with primary hypercholesterolemia and mixed dyslipidemia. J Am Heart Assoc. 2024;13(11):e033669. doi:10.1161/JAHA.123.033669
64. Lin J, Chen J, Zhang R, et al. Abstract 10921: efficacy and safety of ongericimab in chinese patients with homozygous familial hypercholesterolemia. Circulation. 2022;146(Suppl_1):A10921–A10921. doi:10.1161/circ.146.suppl_1.10921
65. Lin J, Ji Y, Wang G, et al. Efficacy and safety of ongericimab in Chinese patients with heterozygous familial hypercholesterolemia: a randomized, double-blind, placebo-controlled phase 3 trial. Atherosclerosis. 2025;403:119120. doi:10.1016/j.atherosclerosis.2025.119120
66. Zhao W, Cheng Z, Ji X, et al. Efficacy and safety of ongericimab given by prefilled syringe or autoinjector in primary hypercholesterolemia and mixed hyperlipidemia. Nutr Metab Cardiovasc Dis. 2024;34(9):2217–2225. doi:10.1016/j.numecd.2024.04.011
67. Blair HA. Ebronucimab: first approval. Drugs. 2025;85(3):437–441. doi:10.1007/s40265-025-02146-4
68. Chen R, Tian Z, Tang X, et al. The safety, pharmacokinetics, pharmacodynamics and immunogenicity of ebronucimab in healthy volunteers: result from a Phase I, randomized, double-blind, placebo-controlled, single dose-escalation study. Circulation. 2022;146(Suppl_1):A9318–A9318. doi:10.1161/circ.146.suppl_1.9318
69. Zhen W, Pei Z, Chen J, et al. Efficacy and safety of ebronucimab, a monoclonal antibody against Pcsk9, in patients with hyperlipidemia: result from a phase 2, randomized, double-blind, placebo-controlled study. Circulation. 2022;146(Suppl_1):A10451–A10451. doi:10.1161/circ.146.suppl_1.10451
70. Zhang Y, Pei Z, Chen B, et al. Ebronucimab in Chinese patients with hypercholesterolemia-A randomized double-blind placebo-controlled phase 3 trial to evaluate the efficacy and safety of ebronucimab. Pharmacol Res. 2024;207:107340. doi:10.1016/j.phrs.2024.107340
71. Huo Y, Zheng B, Xia Y, et al. Efficacy and safety of Ebronucimab, in patients with primary hypercholesterolemia and mixed hyperlipidemia: results from a randomized, double-blind, placebo-controlled phase III clinical study. Atherosclerosis. 2023;379:S198–S199. doi:10.1016/j.atherosclerosis.2023.06.658
72. Booth BJ, Boopathy R, Kristin N, et al. Extending human IgG half-life using structure-guided design. MAbs. 2018;10(7):1098–1110. doi:10.1080/19420862.2018.1490119
73. Robbie GJ, Criste R, Dall’acqua WF, et al. A novel investigational Fc-modified humanized monoclonal antibody, motavizumab-YTE, has an extended half-life in healthy adults. Antimicrob Agents Chemother. 2013;57(12):6147–6153. doi:10.1128/AAC.01285-13
74. Xu M, Zhu X, Wu J, et al. PCSK9 inhibitor recaticimab for hypercholesterolemia on stable statin dose: a randomized, double-blind, placebo-controlled phase 1b/2 study. BMC Med. 2022;20(1):13. doi:10.1186/s12916-021-02208-w
75. Wang Y, Cheng Y, Guo Y, et al. A phase i study to evaluate the relative bioavailability, pharmacodynamics, and safety of a single subcutaneous injection of recaticimab at three different sites in healthy Chinese subjects. Eur J Drug Metab Pharmacokinet. 2025;50(3):265–272. doi:10.1007/s13318-025-00944-5
76. Xu M, Wang Z, Zhang Y, et al. Recaticimab monotherapy for nonfamilial hypercholesterolemia and mixed hyperlipemia: the phase 3 REMAIN-1 randomized trial. J Am Coll Cardiol. 2024;84(20):2026–2036. doi:10.1016/j.jacc.2024.07.035
77. Sun Y, Lv Q, Guo Y, et al. Recaticimab as add-on therapy to statins for nonfamilial hypercholesterolemia: the randomized, phase 3 REMAIN-2 trial. J Am Coll Cardiol. 2024;84(20):2037–2047. doi:10.1016/j.jacc.2024.09.012
78. Jiyan C, Li L, Gao X, et al. PCSK9 monoclonal antibody recaticimab in adult heterozygous familial hypercholesterolemia (REMAIN-3): a multicenter, randomized, double-blind, placebo-controlled phase 3 study. J Am Coll Cardiol. 2024;83(13, Supplement):1707. doi:10.1016/S0735-1097(24)03697-0
79. Romeo S, Yin W, Kozlitina J, et al. Rare loss-of-function mutations in ANGPTL family members contribute to plasma triglyceride levels in humans. J Clin Invest. 2009;119(1):70–79. doi:10.1172/JCI37118
80. Musunuru K, Pirruccello JP, Do R, et al. Exome sequencing, ANGPTL3 mutations, and familial combined hypolipidemia. N Engl J Med. 2010;363(23):2220–2227. doi:10.1056/NEJMoa1002926
81. Jin N, Matter WF, Michael LF, et al. The angiopoietin-like protein 3 and 8 complex interacts with lipoprotein lipase and induces LPL cleavage. ACS Chem Biol. 2021;16(3):457–462. doi:10.1021/acschembio.0c00954
82. Chen YQ, Pottanat TG, Siegel RW, et al. Angiopoietin-like protein 8 differentially regulates ANGPTL3 and ANGPTL4 during postprandial partitioning of fatty acids. J Lipid Res. 2020;61(8):1203–1220. doi:10.1194/jlr.RA120000781
83. Minicocci I, Santini S, Cantisani V, et al. Clinical characteristics and plasma lipids in subjects with familial combined hypolipidemia: a pooled analysis. J Lipid Res. 2013;54(12):3481–3490. doi:10.1194/jlr.P039875
84. Dewey FE, Gusarova V, Dunbar RL, et al. Genetic and pharmacologic inactivation of ANGPTL3 and cardiovascular disease. N Engl J Med. 2017;377(3):211–221. doi:10.1056/NEJMoa1612790
85. Kersten S. ANGPTL3 as therapeutic target. Curr Opin Lipidol. 2021;32(6):335–341. doi:10.1097/MOL.0000000000000789
86. Toth PP. Evinacumab therapy for homozygous familial hypercholesterolemia: driving lipoprotein clearance via the road less taken. JACC Adv. 2023;2(9):100646. doi:10.1016/j.jacadv.2023.100646
87. Tall AR, Thomas DG, Gonzalez-Cabodevilla AG, Goldberg IJ. Addressing dyslipidemic risk beyond LDL-cholesterol. J Clin Invest. 2022;132(1). doi:10.1172/JCI148559
88. Chen PY, Gao WY, Liou JW, Lin CY, Wu MJ, Yen JH. Angiopoietin-Like Protein 3 (ANGPTL3) modulates lipoprotein metabolism and dyslipidemia. Int J Mol Sci. 2021;22(14). doi:10.3390/ijms22147310
89. Reeskamp LF, Tromp TR, Stroes ESG. The next generation of triglyceride-lowering drugs: will reducing apolipoprotein C-III or angiopoietin like protein 3 reduce cardiovascular disease? Curr Opin Lipidol. 2020;31(3):140–146. doi:10.1097/MOL.0000000000000679
90. Bergmark BA, Marston NA, Bramson CR, et al. Effect of vupanorsen on non-high-density lipoprotein cholesterol levels in statin-treated patients with elevated cholesterol: TRANSLATE-TIMI 70. Circulation. 2022;145(18):1377–1386. doi:10.1161/CIRCULATIONAHA.122.059266
91. Pfizer and Ionis announce discontinuation of vupanorsen clinical development program. Avaiable from: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-ionis-announce-discontinuation-vupanorsen.
92. Rosenson RS, Gaudet D, Hegele RA, et al. Zodasiran, an RNAi therapeutic targeting ANGPTL3, for mixed hyperlipidemia. N Engl J Med. 2024;391(10):913–925. doi:10.1056/NEJMoa2404147
93. Arrowhead axes heart disease drug, goes all in on another as pipeline progress drives costs up. June 26, 2024. Available from: https://www.fiercebiotech.com/biotech/arrowhead-axes-1-heart-disease-drug-goes-all-another-pipeline-progress-drives-costs.
94. Ray KK, Oru E, Rosenson RS, et al. Durability and efficacy of solbinsiran, a GalNAc-conjugated siRNA targeting ANGPTL3, in adults with mixed dyslipidaemia (PROLONG-ANG3): a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet. 2025;405(10489):1594–1607. doi:10.1016/S0140-6736(25)00507-0
95. Morrow PK, Chen Y-S, Serwer L, et al. Abstract 16908: CTX310: an investigational in vivo CRISPR-based therapy efficiently and durably reduces ANGPTL3 protein and triglyceride levels in non-human primates after a single dose. Circulation. 2023;148(Suppl_1):A16908–A16908. doi:10.1161/circ.148.suppl_1.16908
96. Lee R, Mazzola A, Denizio J, et al. An investigational in vivo base editing medicine targeting ANGPTL3, VERVE-201, achieves precise and durable liver editing in nonclinical studies. Atherosclerosis. 2024:395. doi:10.1016/j.atherosclerosis.2024.118496
97. Murphy AJ, Macdonald LE, Stevens S, et al. Mice with megabase humanization of their immunoglobulin genes generate antibodies as efficiently as normal mice. Proc Natl Acad Sci U S A. 2014;111(14):5153–5158. doi:10.1073/pnas.1324022111
98. Gusarova V, Alexa CA, Wang Y, et al. ANGPTL3 blockade with a human monoclonal antibody reduces plasma lipids in dyslipidemic mice and monkeys. J Lipid Res. 2015;56(7):1308–1317. doi:10.1194/jlr.M054890
99. Balasubramaniam D, Schroeder O, Russell AM, et al. An anti-ANGPTL3/8 antibody decreases circulating triglycerides by binding to a LPL-inhibitory leucine zipper-like motif. J Lipid Res. 2022;63(5):100198. doi:10.1016/j.jlr.2022.100198
100. Kuehn BM. Evinacumab approval adds a new option for homozygous familial hypercholesterolemia with a hefty price tag. Circulation. 2021;143(25):2494–2496. doi:10.1161/CIRCULATIONAHA.121.055463
101. Ahmad Z, Banerjee P, Hamon S, et al. Inhibition of angiopoietin-like protein 3 with a monoclonal antibody reduces triglycerides in hypertriglyceridemia. Circulation. 2019;140(6):470–486. doi:10.1161/CIRCULATIONAHA.118.039107
102. Harada-Shiba M, Ali S, Gipe DA, et al. A randomized study investigating the safety, tolerability, and pharmacokinetics of evinacumab, an ANGPTL3 inhibitor, in healthy Japanese and Caucasian subjects. Atherosclerosis. 2020;314:33–40. doi:10.1016/j.atherosclerosis.2020.10.013
103. Gaudet D, Gipe DA, Pordy R, et al. ANGPTL3 inhibition in homozygous familial hypercholesterolemia. N Engl J Med. 2017;377(3):296–297. doi:10.1056/NEJMc1705994
104. Rosenson RS, Gaudet D, Ballantyne CM, et al. Evinacumab in severe hypertriglyceridemia with or without lipoprotein lipase pathway mutations: a phase 2 randomized trial. Nat Med. 2023;29(3):729–737. doi:10.1038/s41591-023-02222-w
105. Raal FJ, Rosenson RS, Reeskamp LF, et al. Evinacumab for homozygous familial hypercholesterolemia. N Engl J Med. 2020;383(8):711–720. doi:10.1056/NEJMoa2004215
106. Reeskamp LF, Millar JS, Wu L, et al. ANGPTL3 inhibition with evinacumab results in faster clearance of IDL and LDL apoB in patients with homozygous familial hypercholesterolemia—brief report. Arterioscler Thromb Vasc Biol. 2021;41(5):1753–1759. doi:10.1161/ATVBAHA.120.315204
107. Reeskamp LF, Nurmohamed NS, Bom MJ, et al. Marked plaque regression in homozygous familial hypercholesterolemia. Atherosclerosis. 2021;327:13–17. doi:10.1016/j.atherosclerosis.2021.04.014
108. Raal FJ, Rosenson RS, Reeskamp LF, et al. The long-term efficacy and safety of evinacumab in patients with homozygous familial hypercholesterolemia. JACC Adv. 2023;2(9):100648. doi:10.1016/j.jacadv.2023.100648
109. Gaudet D, Greber-Platzer S, Reeskamp LF, et al. Evinacumab in homozygous familial hypercholesterolaemia: long-term safety and efficacy. Eur Heart J. 2024;45(27):2422–2434. doi:10.1093/eurheartj/ehae325
110. Wiegman A, Greber-Platzer S, Ali S, et al. Evinacumab for pediatric patients with homozygous familial hypercholesterolemia. Circulation. 2024;149(5):343–353. doi:10.1161/CIRCULATIONAHA.123.065529
111. Jin M, Meng F, Yang W, Liang L, Wang H, Fu Z. Efficacy and safety of evinacumab for the treatment of hypercholesterolemia: a meta-analysis. J Cardiovasc Pharmacol. 2021;78(3):394–402. doi:10.1097/FJC.0000000000001073
112. Rosenson RS, Burgess LJ, Ebenbichler CF, et al. Evinacumab in patients with refractory hypercholesterolemia. N Engl J Med. 2020;383(24):2307–2319. doi:10.1056/NEJMoa2031049
113. Xie Z, Ye L, Hu W, Lv C, Zhu M. SHR-1918, a monoclonal antibody against angiopoietin-like 3, in healthy subjects: a randomized, double-blind, placebo-controlled, phase 1 study. Eur Heart J. 2024;45(Supplement_1). doi:10.1093/eurheartj/ehae666.3297
114. Xie X, Shi X, Zhang Y, et al. Angiopoietin-like 3 antibody therapy in patients with suboptimally controlled hyperlipidemia: a phase 2 study. J Am Coll Cardiol. 2025;85(19):1821–1835. doi:10.1016/j.jacc.2025.03.008
115. Dewey FE, Gusarova V, O’Dushlaine C, et al. Inactivating variants in ANGPTL4 and risk of coronary artery disease. N Engl J Med. 2016;374(12):1123–1133. doi:10.1056/NEJMoa1510926
116. Desai U, Lee EC, Chung K, et al. Lipid-lowering effects of anti-angiopoietin-like 4 antibody recapitulate the lipid phenotype found in angiopoietin-like 4 knockout mice. Proc Natl Acad Sci U S A. 2007;104(28):11766–11771. doi:10.1073/pnas.0705041104
117. Wang Q, Oliver-Williams C, Raitakari OT, et al. Metabolic profiling of angiopoietin-like protein 3 and 4 inhibition: a drug-target Mendelian randomization analysis. Eur Heart J. 2021;42(12):1160–1169. doi:10.1093/eurheartj/ehaa972
118. Cummings BB, Bouchard PR, Milton MN, et al. An ANGPTL4 inhibitory antibody safely improves lipid profiles in non-human primates. EBioMedicine. 2025;117:105748. doi:10.1016/j.ebiom.2025.105748
119. Cummings BB, Joing MP, Bouchard PR, et al. Safety and efficacy of a novel ANGPTL4 inhibitory antibody for lipid lowering: results from phase 1 and phase 1b/2a clinical studies. Lancet. 2025;405(10493):1923–1934. doi:10.1016/S0140-6736(25)00825-6
120. Gaudet D, Gonciarz M, Shen X, et al. A first-in-human single ascending dose study of a monoclonal antibody against the ANGPTL3/8 complex in subjects with mixed hyperlipidemia. Atherosclerosis. 2022;355:12. doi:10.1016/j.atherosclerosis.2022.06.034
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.