Back to Journals » Infection and Drug Resistance » Volume 14
Antibiotic Resistance Genes Among Carbapenem-resistant Enterobacterales (CRE) Isolates of Prapokklao Hospital, Chanthaburi Province, Thailand
Authors Tunyong W, Arsheewa W, Santajit S, Kong-ngoen T, Pumirat P, Sookrung N, Chaicumpa W, Indrawattana N ![]()
Received 9 July 2021
Accepted for publication 7 August 2021
Published 29 August 2021 Volume 2021:14 Pages 3485—3494
DOI https://doi.org/10.2147/IDR.S328521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Witawat Tunyong,1 Weewan Arsheewa,2 Sirijan Santajit,3,4 Thida Kong-ngoen,1 Pornpan Pumirat,1 Nitat Sookrung,5,6 Wanpen Chaicumpa,6 Nitaya Indrawattana1
1Department of Microbiology and Immunology, Faculty of Tropical Medicine, Mahidol University, Bangkok, 10400, Thailand; 2Department of Microbiology, Phrapokklao Hospital, Chanthaburi, 22000, Thailand; 3School of Allied Health Sciences, Walailak University, Nakhon Si Thammarat, 80161, Thailand; 4Research Excellence Center for Innovation and Health Products, Walailak University, Nakhon Si Thammarat, 80161, Thailand; 5Biomedical Research Incubation Unit, Department of Research, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand; 6Center of Research Excellence on Therapeutic Proteins and Antibody Engineering, Department of Parasitology, Faculty of Medicine Siriraj Hospital, Bangkok, 10700, Thailand
Correspondence: Nitaya Indrawattana
Department of Microbiology and Immunology, Faculty of Tropical Medicine, Mahidol University, Bangkok, 10400, Thailand
Tel +66 2 354 9100 Ext. 1598
Fax +66 2 643 5598
Email [email protected]
Background: The global spread of carbapenem-resistant Enterobacterales (CRE) inflicts a severe threat to human health. The CRE infections have resulted in an increased mortality rate in hospitals and other health-care settings worldwide. In this study, the antibiotic-resistance pattern and prevalence of carbapenemase-encoding genes among CRE isolated from patients of one hospital in Thailand were investigated.
Methods: By using conventional biochemical tests, we identified and isolated all species of Enterobacterales from the clinical samples kept at Prapokklao Hospital, Chanthaburi, Thailand, which were collected during 2016– 2017. Multidrug-resistant (MDR) bacteria were determined by disc diffusion method and minimum inhibitory concentration (MIC) test strips. Carbapenemase genes were detected by PCR and confirmed by Sanger sequencing.
Results: Klebsiella pneumoniae complex, Escherichia coli, and Enterobacter spp. were isolated from the specimens. Of 9,564 isolated Enterobacterales, 282 were multidrug-resistance (MDR). The MIC test strips revealed that the MDR CRE were resistant to ertapenem (92.9%) and meropenem (81.3%). All these isolates carried carbapenemase-coding genes, including blaNDM (90%) and blaIMP (71%), the two most commonly found genes among CRE strains. There were 39.2% of the isolates that carried a combination of blaNDM-blaIMP and 22.6% carried combined blaNDM-blaIMP-blaOXA-48-like genes.
Conclusion: This study demonstrates a significantly high prevalence of CRE isolates with the MDR phenotypes. A minority of the isolates carried a single carbapenem-resistant gene, while the majority harbored multiple genes in combination. Regular monitoring of MDR CRE and characterization of their drug resistance are important for guiding treatment, intervention and control of the CRE spread and outbreak in a health-care setting.
Keywords: carbapenemase, CRE, drug resistant, Enterobacterales, nosocomial infections
Introduction
Carbapenem-resistant Enterobacterales (CRE) are gram-negative bacteria that have become pathogens of a major public health concern globally. These bacteria infect hospitalized patients who are under long-term medical care from severe entities, such as those with major surgery/injury or urinary/intravascular/respiratory catheters.1–3 Normally, CRE inhabit the digestive tract of healthy individuals or animals and are nonpathogenic.4 They become pathogens when they are misplaced into other anatomical sites, e.g., the blood stream, urinary tract, or respiratory tract, causing hospital-acquired diseases that encompass pneumonia, sepsis, urinary tract infection, wound infection, meningitis, etc. The infections are difficult to treat as these bacteria have propensity to resist multiple antimicrobial drugs, particularly carbapenem, which is considered the last antibiotic resort for treatment of multidrug-resistant bacterial infections.5,6 Over the past decades, increased CRE infections have been reported worldwide.7–16 The Centers for Disease Control and Prevention (CDC)’s Detect and Protect Against Antibiotic Resistance Initiative (known as the AR Initiative) and the World Health Organization (WHO) have specifically recommended the detection and tracking of CRE as a critical priority of public health.17,18,19 The most common species of CRE causing infections in the clinical settings are Klebsiella pneumoniae and Escherichia coli.20,21 The carbapenemase resistance is usually mediated by mobile genetic elements harboring beta-lactamase encoding genes, which also confer resistance to most penicillin-derivatives and cephalosporins.5 Meropenem, doripenem, ertapenem, and imipenem are the most commonly used carbapenems in the health-care settings.22 Carbapenemase gene products, such as K. pneumoniae carbapenemase (KPC), metallo-β-lactamases, and oxacillinase (OXA-48), are often found in carbapenemase-producing Enterobacterales.23–28 Among them, the blaKPC is the most common gene reported; however, prevalence of other genes, such as blaOXA, blaVIM, blaNDM, and blaIMP, are gradually increasing worldwide.29 Emergence of drug resistant bacteria have led to more severe drug resistance problems.30 In this study, the antibiotic resistance patterns and carbapenem-resistant genes among CRE isolated from the clinical samples kept in a tertiary health-care setting in Thailand were investigated as this kind of information is needed for emergency preparedness and response to outbreaks of MDR organisms in a locality.
Materials and Methods
Study Design, Sample Collection, and Ethical Approval
The stored clinical samples were from a cross-sectional study conducted during January 2016 to December 2017 by the Department of Microbiology, Prapokklao Hospital, Chanthaburi Province, located about 226 km Southeast of Bangkok, Thailand. Of the 9,564 Enterobacterales isolates recovered from the specimens, 282 isolates (2.95%) were CRE. They were from different types of the samples from different patients, i.e., 18 blood samples, 8 body fluids, 120 urine samples, 108 sputum samples and 28 pus samples. Unfortunately, the demographic data of the patients were untraceable. This study was approved by the Ethics Committee of Prapokklao Hospital, Chanthaburi Province, Thailand (approval number: CTIREC 041).
Bacterial Isolation and Identification
The stock samples were streaked on McConkey agar and incubated at 37°C for 24 hours. Isolated bacterial colonies on the plates were subjected to conventional biochemical tests31 including oxidase, triple sugar iron utilization, ornithine decarboxylase, indole production, motility, and citrate utilization tests, as well as antimicrobial susceptibility tests.32
Antimicrobial Susceptibility Testing
The antimicrobial susceptible testing was performed based on the Clinical and Laboratory Standards Institute (CLSI) guidelines 2017.33 The Kirby–Bauer disc diffusion method and 16 antimicrobial drugs/drug combinations were used, including ampicillin (10 μg), amoxicillin/clavulanate (20/10 μg), ampicillin/sulbactam (10/10 μg), piperacillin/tazobactam (100/10 μg), cefazolin (30 μg), ceftazidime (30 μg), cefotaxime (30 μg), ceftriaxone (30 μg), ertapenem (10 μg), meropenem (10 μg), imipenem (10 μg), gentamicin (10 μg), amikacin (30 μg), ciprofloxacin (5 μg), trimethoprim/sulfamethoxazole (1.25/23.75 μg), and fosfomycin (200 μg) (Oxoid, Thermo Fisher Scientific, Basingstoke Hampshire, UK). Multidrug-resistance criteria were defined as bacteria resistant to carbapenem and at least three out of five drug groups—cephalosporins, ampicillin, β-lactam/β-lactamase inhibitor combination, fluoroquinolones, folate pathway, and fosfomycin. Extended-spectrum β-lactamase (ESBL) production of all isolates were tested by using a combination disc test of ceftazidime with and without clavulanate, and cefotaxime with and without clavulanate (BD BBL, Identification System, New York, USA). A positive test result was defined as ≥5 mm difference in the clear zone diameter between the discs with and without clavulanate. Criteria of CLSI 2017 were used for interpretation of the antimicrobial-susceptibility results. Carbapenem resistance was determined using Liofilchem® MIC Test Strips (Liofilchem, Roseto degli Abruzzi (TE), Italy). CRE was defined as Enterobacterales organisms showing decreased susceptibility to carbapenems (MIC for imipenem ≥2 μg/mL, meropenem ≥2 μg/mL, or ertapenem ≥1 μg/mL) and resistance to all third-generation cephalosporins, regardless of carbapenemase production.34 All antibiotic susceptibility tests were independently performed in duplicative experiments.
PCR and DNA Sequencing for Detection and Identification of Carbapenemase Genes
The genomic DNA of all CRE isolates was extracted and amplified for bla genes, including blaKPC, blaNDM, blaVIM, blaIMP, and blaOXA-48-like, using specific primers. Briefly, the bacterial isolates were grown on tryptic soy agar plates at 37°C overnight. The single bacterial colony was re-suspended in sterile distilled water and boiled at 100°C for 10 minutes. The lysates were centrifuged at 12,000 ×g for 10 minutes and 1 μL of supernatant was used as DNA template for PCR.35 The amplification reaction (25 μL) contained 10× Taq buffer, 25 mM of MgCl2, 10 mM of dNTPs, 10 μM each of of forward and reverse primers, >50 ng/μL of genomic DNA and 1.25 units/μL of Taq DNA Polymerase (Thermo Scientific, Waltham, MA, USA). The thermal cycles were 94°C for 5 minutes, followed by 35-cycles of denaturing at 94°C, 30 seconds; annealing at a temperature specific for each primer, 30 seconds; and extension at 72°C, 30 seconds, with a final extension at 72°C for 7 minutes.35 PCR products were analyzed using 1.5% (w/v) agarose gel and ethidium bromide staining. Individual genes in representative CRE isolates were verified by DNA sequencing. The nucleotide sequences were analyzed using the BLASTn program, software available at the National Center for Biotechnology Information website (http://www.ncbi.nlm.nih.gov).
Results
Bacterial Identification and CRE Isolates
From a total of 9,567 Enterobacterales isolates, 282 (2.95%) were carbapenem resistant Enterobacterales (CRE). They were 187 (66%) K. pneumoniae complex, 81 (29%) E. coli, and 14 (5%) Enterobacter spp., 11 (4%) E. cloacae and 3 (1%) E. aerogenes (Figure 1).
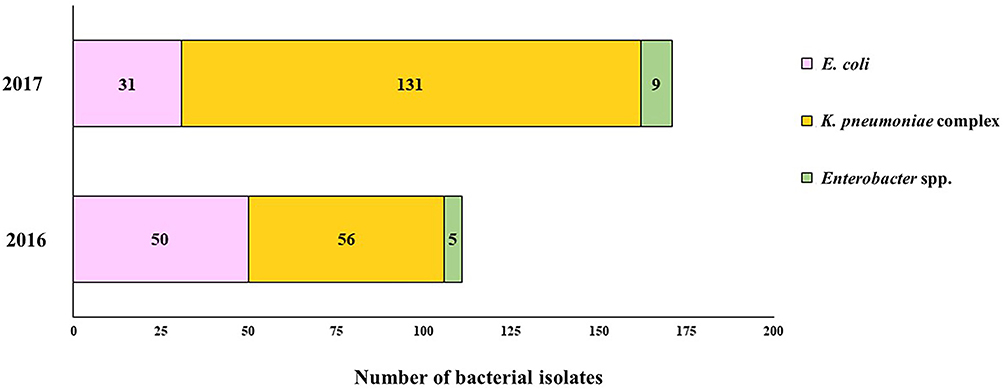 |
Figure 1 Number of carbapenem-resistant Enterobacterales isolates during 2016–2017. |
Antimicrobial Susceptibility Testing
Antimicrobial pattern of carbapenem-resistant Enterobacterales isolates are shown in Table 1. The 2016 CRE isolates showed high resistance to third-generation cephalosporin (100%); carbapenem: ertapenem 99%, meropenem 94.6%, imipenem 81.9%; β-lactam/β-lactamase inhibition combination: amoxicillin/clavulanate 100%, ampicillin/sulbactam 99%, piperacillin/tazobactam 88.3%; and ampicillin 99%. Resistance to other antibiotics was observed—ciprofloxacin 82.9%, trimethoprim-sulfamethoxazole 90%, amikacin 61.3%, gentamicin 21.6%, and fosfomycin 18%. The results of the MIC test strips showed resistance to ertapenem and meropenem at 85.6 and 78.4%, respectively. The MIC ranges of CRE isolates, i.e., E. coli, K. pneumoniae complex, and Enterobacter spp., for ertapenem were 0.5–32, 0.064–32, and 1–32 µg/mL, respectively, and for meropenem were 0.032–32, 0.047–32 and 2–32 µg/mL, respectively. The CRE isolates were positive for extended-spectrum β-lactamase (ESBL); the values for ceftazidime and cefotaxime were 85.5 and 71.4%, respectively (Figure 2).
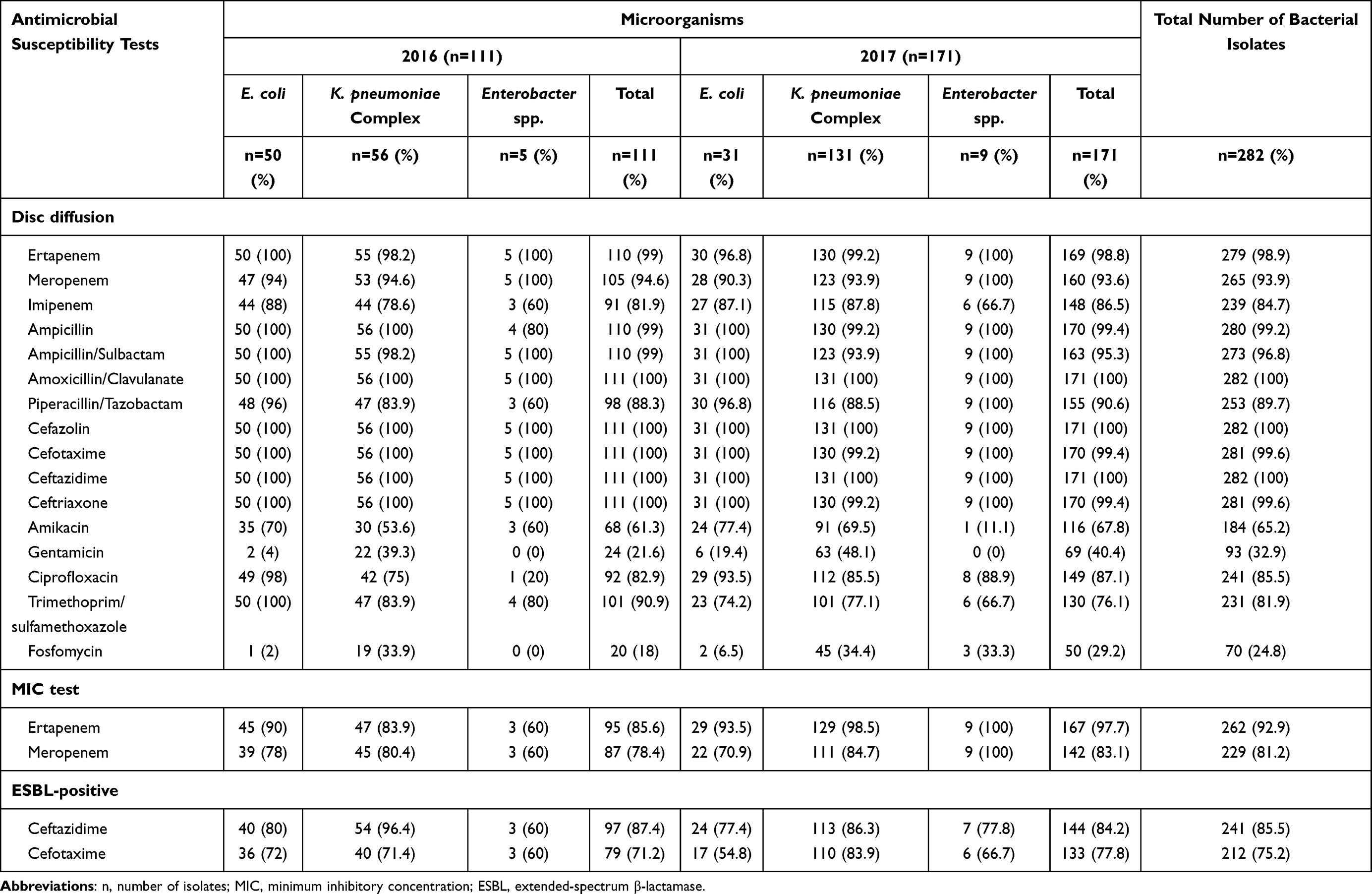 |
Table 1 Antimicrobial Pattern of Carbapenem-Resistant Enterobacterales Isolates |
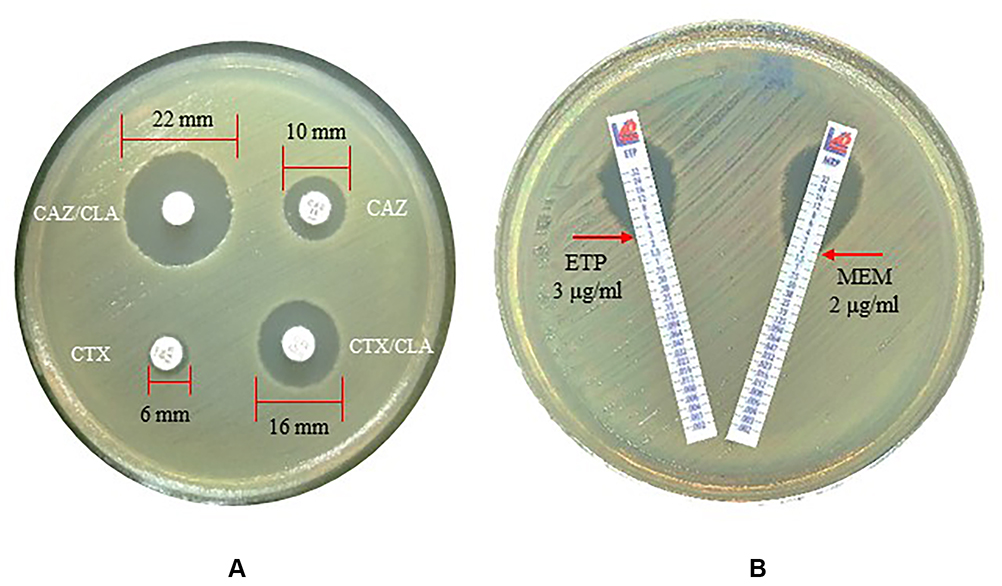 |
Figure 2 Antimicrobial susceptibility test. (A) Extended-spectrum β-lactamase (ESBL) production was determined by the combination disc test. (B) Carbapenem resistance test by MIC test strips. Abbreviations: CAZ/CLA, ceftazidime + clavulanate; CAZ, ceftazidime + cefotaxime; CTX, cefotaxime; CTX/CLA, cefotaxime + clavulanate; ETP, ertapenem; MEM, meropenem. |
The 2017 CRE isolates were highly resistant to third-generation cephalosporin (cefazolin 100%, ceftazidime 100%, cefotaxime 99.4%, ceftriaxone 99.4%); carbapenem (ertapenem 98.8%, meropenem 93.6%, imipenem 86.5%); β-lactam/β-lactamase inhibition combination (amoxicillin/clavulanate 100%, ampicillin/sulbactam 96.8%, piperacillin/tazobactam 89.7%); and ampicillin (99.2%). Resistance to other antibiotics were—ciprofloxacin (87.1%), trimethoprim-sulfamethoxazole (76.1%), amikacin (67.8%), gentamicin (40.4%), and fosfomycin (29.2%). The MIC test strips that demonstrated resistance to ertapenem and meropenem were 97.7 and 83.1%, respectively. These CRE isolates were positive for ESBL; the values for ceftazidime and cefotaxime were 84.2 and 77.8%, respectively.
Carbapenemase Coding Genes Among the Carbapenem-resistant Enterobacterales
The PCR amplicon sizes of the resistant genes, ie, blaKPC, blaVIM, blaIMP, blaNDM, and blaOXA-48-like were 489, 382, 188, 490, 218 and 743 bp, respectively (Supplementary Data 1).
Of the 282 CRE isolates, 256 (90%) carried blaNDM; 203 (72%) and 134 (48%) isolates were positive for blaIMP and blaOXA-48-like, respectively. There were five (1.8%) isolates carried blaVIM and one (0.4%) isolate with blaKPC.
Distribution of the carbapenemase genes was also analyzed. Among 282 isolates, 31 were singly positive for blaNDM (22 isolates, 7.8%) and blaIMP (9 isolates, 3.2%). The others 251 isolates (89%) had combination of different genes. The predominant combination was blaNDM and blaIMP (111 isolates, 39.2%), followed by combined blaNDM, blaIMP, and blaOXA-48-like (64 isolates, 22.6%) and combined blaNDM and blaOXA-48-like (55 isolates, 19.4%). Other combination types were the blaIMP and blaOXA-48-like (15 isolates, 5.3%), blaNDM, blaIMP and blaOXA-48-like (3 isolates, 1.1%), blaNDM and blaVIM combination (2 isolates, 0.7%), and blaKPC, blaIMP, and blaOXA-48-like (1 isolate, 0.4%). The orthologues of the antibiotic-resistant gene PCR amplicons are shown in Supplementary Data 2.
Among carbapenem-resistant bacteria, the highest prevalence of the drug-resistant gene was blaNDM, which was found in 165 isolates (58.5%) of K. pneumoniae complex; followed by 78 isolates (27.7%) of E. coli. The second most prevalent resistant gene was blaIMP gene, which was found in 151 (53.5%) of K. pneumoniae complex and in 46 (29.1%) of E. coli isolates. The blaOXA-48-like gene was found in 82 isolates (29.1%), and 44 isolates (15.6%); the blaVIM gene was found in 4 (1.4%) E. coli isolates and 1 (0.4%) K. pneumoniae complex isolate; and the blaKPC gene was found in 1 (0.4%) K. pneumoniae complex isolate. For Enterobacter spp., the predominant resistant gene was blaNDM (13 isolates, 4.6%; 11 E. cloacae isolates and 2 E. aerogenes isolates). Others genes were blaOXA-48-like (8 isolates, 3%; 5 E. cloacae isolates and 3 E. aerogenes isolates) and blaIMP (6 isolates, 2%; 5 E. cloacae isolates and 1 E. aerogenes isolate) (Table 2 and Figure 3).
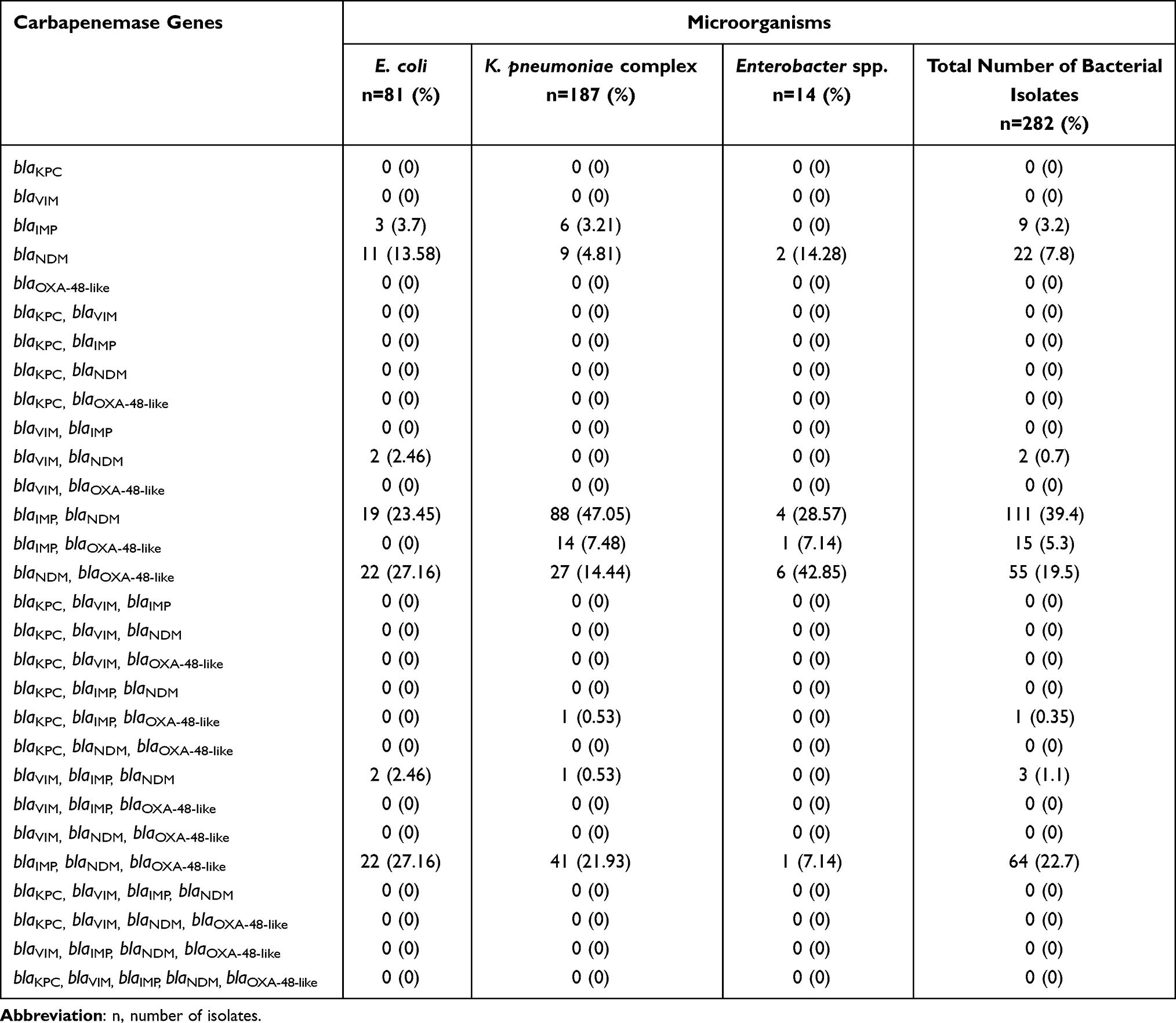 |
Table 2 Distribution of Carbapenemase-encoding Genes Among Carbapenemase-producing Carbapenem-resistant Enterobacterales Isolates by PCR |
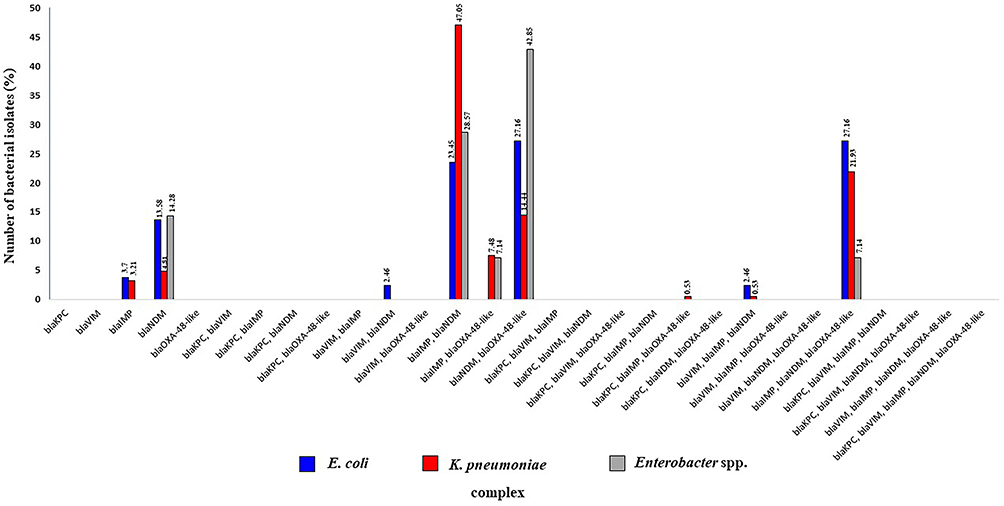 |
Figure 3 Percentage of carbapenemase-encoding genes among carbapenemase-producing carbapenem-resistant Enterobacterales, based on PCR analysis. |
Discussion
Carbapenem-resistant Enterobacterales (CRE) are considered nowadays as a public health threat worldwide because they are one of the major causes of death among patients with hospital-acquired infections. Regular monitoring of CRE in a particular health-care setting is rational to guide effective treatment of the infection. This study assessed the antibiotic-resistance pattern and the prevalence of the carbapenem-resistant genes among CRE isolated from clinical specimens of patients kept at Prapokklao Hospital which is one of the tertiary care hospitals in Southeastern Thailand. Our study demonstrates a high prevalence of CRE that carried a variety of carbapenem-resistance coding genes. Three species of Enterobacterales, i.e., K. pneumoniae complex, E. coli, and Enterobacter spp. were predominant among the CRE isolates (282 of 9,567 Enterobacterales isolates). Five families of carbapenemase genes including blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA-48-like were identified by PCR and DNA sequencing.
In this study, the prevalence of CRE isolated during 2016–2017 showed marked increase compared to those of 2012–2013 study in the same hospital, Prapokklao Hospital.36 The National Antimicrobial Resistance Surveillance Center, Thailand (NARST), reported that between January and December 2017, 13% of K. pneumoniae complex isolates and 1% of E. coli isolates were resistant to carbapenems.20 In this study, 66% of the K. pneumoniae complex accounted for the largest percentage of CRE isolates (50% in 2016 and 77% in 2017), 29% of the E. coli and 5% of the Enterobacter spp., respectively.
Most resistance to carbapenem agents is caused by carbapenemase and the presence of other resistance mechanisms, such as extended-spectrum beta-lactamases (ESBLs), porin mutations, and/or the presence of efflux pumps.37 While our antimicrobial susceptibility testing results showed that carbapenem-resistant Enterobacterales strains exhibited resistance to many antimicrobial agents including third generation cephalosporin, carbapenem, the β-lactam/β-lactamase inhibition combination, ampicillin, ciprofloxacin, trimethoprim sulfamethoxazole, and amikacin, most CRE strains are still sensitive to gentamicin and fosfomycin which conformed to the results of previous studies.38–41 The results of this study showed that CRE isolates were highly resistant to carbapenem agents. The isolates were resistant to ertapenem (93%) which was more than meropenem (81%). The prevalence of ESBL-producing isolates (75–85%) in this study was higher than that observed in a previous study among Thai community volunteers (32.0–66.5%).36
Among the CRE isolates of this study, the prevalence of three carbapenemase genes was high—blaNDM, followed by blaIMP and blaOXA-48-like. The blaVIM and blaKPC genes were found in smaller numbers in this study, even though this gene has been reported to spread rapidly worldwide. In Thailand, blaNDM, blaOXA-48-like, and blaIMP-14 were frequently detected in clinical Enterobacterales isolates,42 while the prevalence of blaKPC in the country remained low; the latest study reported 0.02% of blaKPC-13-carrying isolates among Enterobacterales and 1.7% among CRE isolates.43 The prevalence of CRE in Asia and South East Asia showed an increasing trend and is mainly caused by carbapenem-hydrolyzing β-lactamases, including NDM and IMP-type enzymes.23,44 In this study, the blaNDM gene was found to be the most common carbapenemase gene, i.e., carried by about 90% of the tested isolates. The other most common carbapenemase genes were blaIMP, carried by 203 isolates (71%) and frequently found in K. pneumoniae complex (53%); the blaOXA-48-like gene, was found in 134 isolates (48%) and 29% among the K. pneumoniae complex. There are limited data on blaIMP and blaOXA-48-like in relation to CRE prevalence in Thailand. However, Rimrang et al43 reported in 2012 that two isolates of K. pneumoniae complex out of 4,818 from clinical Enterobacterales isolates were blaIMP. In addition, our results also demonstrated that 89% of the CRE contained combinations of genes. The most commonly found were the blaNDM and blaIMP gene combination (39.2%), followed by the blaNDM and blaOXA-48-like combination, and the blaIMP and blaOXA-48-like combination. In addition, we observed the triple combination of blaNDM, blaIMP and blaOXA-48-like (22.6%), and 11% of the CRE isolates with single gene, i.e., blaNDM (7.8%) and blaIMP (3.2%).
The high prevalence of CRE harboring the carbapenemase-coding genes along with multiple drug-resistant phenotypes signals a decreasing therapeutic efficacy of the currently available antimicrobial agents. Thus, an effective alternative option to combat these drug resistant bacteria is urgently needed. Natural products with antibacterial activities against various gram-positive and gram-negative bacterial pathogens have been used with some success, such as essential oils (Melaleuca alternifolia, Thymus vulgaris, Mentha piperita, and Rosmarinus officinalis), a commercial ophthalmic solution containing povidone-iodine 0.6% (IODIM®), hexamidine diisethionate 0.05% (Keratosept).45–48 These products should be studied further along with other novel synthetic drugs toward clinical use against the MDR CRE.
Conclusion
We have demonstrated a significantly high prevalence of carbapenem-resistant Enterobacteriales (CRE) isolates with the multidrug-resistant (MDR) phenotypes isolated from clinical samples of patients of one of the tertiary care hospitals in Thailand. The MDR CRE isolates carried carbapenem-resistant genes either singly (minority) or multiple genes in combination (majority). Regular monitoring of the MDR CRE is needed regularly for guiding treatment, intervention and control of the spread and outbreak of these superbugs.
Acknowledgments
This work was supported by the Tropical Medicine Grants 2017 from Faculty of Tropical Medicine, Mahidol University to Witawat Tunyong. We would like to thank Mr Paul Adams, Research Administrator of Faculty of Tropical Medicine, Mahidol University, for editing English of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elbadawi LI, Borlaug G, Gundlach KM, et al. Carbapenem-resistant Enterobacteriaceae transmission in health care facilities-Wisconsin, February-May 2015. Morbid Mortal Wkly Rep. 2016;65(34):906–909. doi:10.15585/mmwr.mm6534a5
2. Suay-García B, Pérez-Gracia MT. Present and future of carbapenem resistant Enterobacteriaceae (CRE) infections. Antibiotics. 2019;8(3):122. doi:10.3390/antibiotics8030122
3. Sheu CC, Chang YT, Lin SY, Chen YH, Hsueh PR. Infections caused by carbapenem-resistant Enterobacteriaceae: an update on therapeutic options. Front Microbiol. 2019;10:80. doi:10.3389/fmicb.2019.00080
4. Jacob JT, Klein E, Laxminarayan R, et al. Vital signs: carbapenem-resistant Enterobacteriaceae. Morbid Mortal Wkly Rep. 2013;62(9):165.
5. Tängdén T, Giske CG. Global dissemination of extensively drug‐resistant carbapenemase‐producing Enterobacteriaceae: clinical perspectives on detection, treatment and infection control. J Intern Med. 2015;277(5):501–512. doi:10.1111/joim.12342
6. Li X, Ye H. Clinical and mortality risk factors in bloodstream infections with carbapenem-resistant Enterobacteriaceae. Can J Infect Dis Med Microbiol. 2017. doi:10.1155/2017/6212910
7. Nordmann P, Naas T, Poirel L. Global spread of carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis. 2011;17(10):1791. doi:10.3201/eid1710.110655
8. Shahid M, Sobia F, Singh A, Khan HM, Malik A, Shukla I. Molecular epidemiology of carbapenem-resistant Enterobacteriaceae from a North Indian Tertiary Hospital. N Z J Med Lab Sci. 2012;66(1):5.
9. Guh AY, Bulens SN, Mu Y, et al. Epidemiology of carbapenem-resistant Enterobacteriaceae in 7 US communities, 2012–2013. JAMA. 2015;314(14):1479–1487. doi:10.1001/jama.2015.12480
10. Okoche D, Asiimwe BB, Katabazi FA, Kato L, Najjuka CF. Prevalence and characterization of carbapenem-resistant Enterobacteriaceae isolated from Mulago National Referral Hospital, Uganda. PLoS One. 2015;10(8):e0135745. doi:10.1371/journal.pone.0135745
11. Xu Y, Gu B, Huang M, et al. Epidemiology of carbapenem resistant Enterobacteriaceae (CRE) during 2000–2012 in Asia. J Thorac Dis. 2015;7(3):376.
12. Alotaibi FE, Bukhari EE, Al-Mohizea MM, Hafiz T, Essa EB, AlTokhais YI. Emergence of carbapenem-resistant Enterobacteriaceae isolated from patients in a university hospital in Saudi Arabia. Epidemiology, clinical profiles and outcomes. J Infect Public Health. 2017;10(5):667–673. doi:10.1016/j.jiph.2017.05.004
13. Almugadam BS, Ali NO, Ahmed AB. Prevalence and antibiotics susceptibility patterns of carbapenem resistant Enterobacteriaceae. J Bacteriol Mycol Open Access. 2018;6(3):187–190.
14. Chotiprasitsakul D, Srichatrapimuk S, Kirdlarp S, Pyden AD, Santanirand P. Epidemiology of carbapenem-resistant Enterobacteriaceae: a 5-year experience at a tertiary care hospital. Infect Drug Resist. 2019;12:461. doi:10.2147/IDR.S192540
15. Kang JS, Yi J, Ko MK, Lee SO, Lee JE, Kim KH. Prevalence and risk factors of carbapenem-resistant Enterobacteriaceae acquisition in an emergency intensive care unit in a tertiary hospital in Korea: a Case-Control Study. J Korean Med Sci. 2019;34(18):18. doi:10.3346/jkms.2019.34.e140
16. Tran DM, Larsson M, Olson L, et al. High prevalence of colonisation with carbapenem-resistant Enterobacteriaceae among patients admitted to Vietnamese hospitals: risk factors and burden of disease. J Infect. 2019;79(2):115–122. doi:10.1016/j.jinf.2019.05.013
17. Lutgring JD, Limbago BM, Kraft CS. The problem of Carbapenemase-producing-carbapenem-resistant-Enterobacteriaceae detection. J Clin Microbiol. 2016;54(3):529–534. doi:10.1128/JCM.02771-15
18. Kost K, Yi J, Rogers B, Jerris R. Comparison of clinical methods for detecting carbapenem-resistant Enterobacteriaceae. Pract Lab Med. 2017;8:18–25. doi:10.1016/j.plabm.2017.03.002
19. Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–327. doi:10.1016/S1473-3099(17)30753-3
20. NARST. National antimicrobial resistance surveillance center, Thailand. Available from:http://narst.dmsc.moph.go.th/data/AMR%202000-2020-12M.pdf. Accessed July 30, 2021. Thai.
21. Partridge SR, Kwong SM, Firth N, Jensen SO. Mobile genetic elements associated with antimicrobial resistance. Clin Microbiol Rev. 2018;31(4):e00088–17. doi:10.1128/CMR.00088-17
22. Nicolau DP. Carbapenems: a potent class of antibiotics. Expert Opin Pharmacother. 2008;9(1):23–37. doi:10.1517/14656566.9.1.23
23. Logan LK, Weinstein RA. The epidemiology of carbapenem-resistant Enterobacteriaceae: the impact and evolution of a global menace. J Infect Dis. 2017;215(suppl_1):S28–S36. doi:10.1093/infdis/jiw282
24. Rhodes NJ, Wagner JL, Davis SL, et al. Trends in and predictors of carbapenem consumption across North American hospitals: results from a multicenter survey by the MAD-ID research network. Antimicrob Agents Chemother. 2019;63(7):e00327–19. doi:10.1128/AAC.00327-19
25. Bakthavatchalam YD, Anandan S, Veeraraghavan B. Laboratory detection and clinical implication of oxacillinase-48 like carbapenemase: the hidden threat. J Glob Infect Dis. 2016;8(1):41. doi:10.4103/0974-777X.176149
26. Lee CR, Lee JH, Park KS, Kim YB, Jeong BC, Lee SH. Global dissemination of carbapenemase-producing Klebsiella pneumoniae: epidemiology, genetic context, treatment options, and detection methods. Front Microbiol. 2016;7:895.
27. Wang Q, Wang X, Wang J, et al. Phenotypic and genotypic characterization of carbapenem-resistant Enterobacteriaceae: data from a longitudinal large-scale CRE study in China (2012–2016). Clin Infect Dis. 2018;67(suppl_2):S196–S205. doi:10.1093/cid/ciy660
28. Park CE. Clinical laboratory aspect of carbapenem-resistant Enterobacteriaceae. Korean J Clin Lab Sci. 2020;52(1):18–27. doi:10.15324/kjcls.2020.52.1.18
29. Chen WK, Yang Y, Tan BH. Increased mortality among carbapenemase producing carbapenem-resistant Enterobacteriaceae carriers who developed clinical isolates of another genotype. Oxford Univ Press. 2019;6(2):ofz006.
30. Netikul T, Kiratisin P. Genetic characterization of carbapenem-resistant Enterobacteriaceae and the spread of carbapenem-resistant Klebsiella pneumoniae ST340 at a university hospital in Thailand. PLoS One. 2015;10(9):e0139116. doi:10.1371/journal.pone.0139116
31. Nordmann P, Gniadkowski M, Giske CG, Poirel L, Woodford N, Miriagou V. European network on carbapenemases. Identification and screening of carbapenemase-producing Enterobacteriaceae. Clin Microbiol Infect. 2012;18(5):432–438. doi:10.1111/j.1469-0691.2012.03815.x
32. Cheesbrough M. District Laboratory Practice in Tropical Countries, Part 2. Cambridge, UK: Cambridge University Press; 2005.
33. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing.
34. Lee HJ, Choi JK, Cho SY, et al. Carbapenem-resistant Enterobacteriaceae: prevalence and risk factors in a single community-based hospital in Korea. Infect Chemother. 2016;48(3):166–173. doi:10.3947/ic.2016.48.3.166
35. Mohamed T, Yousef LM, Darweesh EI, Khalil AK, Meghezel EM. Detection and characterization of carbapenem resistant Enterobacteriacea in Sohag University Hospitals. Egypt J Med Microbiol. 2018;27(4):61–69.
36. Arsheewa W. Prevalence of carbapenemase enzyme in clinical isolates of carbapenem-resistant Enterobacteriaceae from Prapokklao Hospital in 2012–2013. J Prapokklao Hosp Clin Med Educ Cent. 2016;33(4):314–325.
37. AlTamimi M, AlSalamah A, AlKhulaifi M, AlAjlan H. Comparison of phenotypic and PCR methods for detection of carbapenemases production by Enterobacteriaceae. Saudi J Biol Sci. 2017;24(1):155–161. doi:10.1016/j.sjbs.2016.07.004
38. Livermore DM, Warner M, Mushtaq S, Doumith M, Zhang J, Woodford N. What remains against carbapenem-resistant Enterobacteriaceae? Evaluation of chloramphenicol, ciprofloxacin, colistin, fosfomycin, minocycline, nitrofurantoin, temocillin and tigecycline. Int J Antimicrob Agent. 2011;37(5):415–419. doi:10.1016/j.ijantimicag.2011.01.012
39. Yeganeh Sefidan F, Azargun R, Ghotaslou R. Fosfomycin, a therapeutic option for infections produced by multiple drug-resistant Enterobacteriaceae. Microb Res. 2016;7(1):32–36. doi:10.4081/mr.2016.6407
40. Gopichand P, Agarwal G, Natarajan M, et al. In vitro effect of fosfomycin on multi-drug resistant gram-negative bacteria causing urinary tract infections. Infect Drug Res. 2019;12:2005. doi:10.2147/IDR.S207569
41. Mączyńska B, Paleczny J, Oleksy-Wawrzyniak M, Choroszy-Król I, Bartoszewicz M. In vitro susceptibility of multi-drug resistant Klebsiella pneumoniae strains causing nosocomial infections to fosfomycin. a comparison of determination methods. Pathogens. 2021;10(5):512. doi:10.3390/pathogens10050512
42. Rattanaumpawan P, Choorat C, Takonkitsakul K, Tangkoskul T, Seenama C, Thamlikitkul V. A prospective surveillance study for multidrug-resistant bacteria colonization in hospitalized patients at a Thai University Hospital. Antimicrob Resist Infect Control. 2018;7(1):1–11. doi:10.1186/s13756-018-0393-2
43. Rimrang B, Chanawong A, Lulitanond A, et al. Emergence of NDM-1-and IMP-14a-producing Enterobacteriaceae in Thailand. J Antimicrob Chemother. 2012;67(11):2626–2630. doi:10.1093/jac/dks267
44. Kerdsin A, Deekae S, Chayangsu S, et al. Genomic characterization of an emerging blaKPC-2 carrying Enterobacteriaceae clinical isolates in Thailand. Sci Rep. 2019;9(1):1–7. doi:10.1038/s41598-019-55008-x
45. Cannas S, Usai D, Pinna A, et al. Essential oils in ocular pathology: an experimental study. J Infect Dev Ctries. 2015;9(6):650–654. doi:10.3855/jidc.6842
46. Rameshkumar G, Ramakrishnan R, Shivkumar C, et al. Prevalence and antibacterial resistance patterns of extended-spectrum beta-lactamase producing gram-negative bacteria isolated from ocular infections. Indian J Ophthalmol. 2016;64(4):303. doi:10.4103/0301-4738.182943
47. Pinna A, Donadu MG, Usai D, et al. In vitro antimicrobial activity of a new ophthalmic solution containing povidone‐iodine 0.6%(IODIM®). Acta Ophthalmol. 2020;98(2):e178–e180. doi:10.1111/aos.14243
48. Pinna A, Donadu MG, Usai D, Dore S, Boscia F, Zanetti S. In vitro antimicrobial activity of a new ophthalmic solution containing hexamidine diisethionate 0.05%(keratosept). Cornea. 2020;39(11):1415–1418. doi:10.1097/ICO.0000000000002375
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.