")
Back to Journals » Clinical Interventions in Aging » Volume 13
Antibacterial treatment of aspiration pneumonia in older people: a systematic review
Authors Bowerman TJ , Zhang J, Waite LM
Received 10 August 2018
Accepted for publication 14 September 2018
Published 30 October 2018 Volume 2018:13 Pages 2201—2213
DOI https://doi.org/10.2147/CIA.S183344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Timra J Bowerman,1–3 Jan Zhang,2 Louise M Waite4,5
1Department of Aged Care, Psychogeriatrics and Rehabilitation, Bankstown-Lidcombe Hospital, Bankstown, NSW, Australia; 2Department of Geriatric Medicine, Concord Repatriation General Hospital, Concord, NSW, Australia; 3University of New South Wales, Sydney, NSW, Australia; 4Centre for Education and Research on Ageing, Concord Repatriation General Hospital, Concord, NSW, Australia; 5University of Sydney, Sydney, NSW, Australia
Background: Aspiration pneumonia is a common problem in older people with high mortality and increasing prevalence.
Objective: The aims of this paper were to systematically review the literature on the antibacterial treatment of aspiration pneumonia in elderly patients and identify the microbiology of aspiration pneumonia.
Materials and methods: EMBASE, MEDLINE, and Cochrane databases were systematically searched for studies that examined the clinical efficacy of antibiotic treatment in elderly patients with aspiration pneumonia. Information on study design, antibiotic treatment, study population, participants, microbiology, clinical outcomes, adverse events, and mortality was recorded.
Results: There were no definitive clinical trials, placebo-controlled trials, or meta-analyses. Of the eight studies selected for inclusion in the review, the majority utilized and/or compared broad-spectrum antibiotics. No specific antibacterial agent had evidence of superior efficacy. Broad-spectrum antibiotics resulted in the emergence of multiresistant organisms. Anaerobic bacteria were infrequently isolated, suggesting a less important role in the pathogenesis of aspiration pneumonia.
Conclusion: There is limited evidence with regard to the use of antibiotics in older patients with aspiration pneumonia. Research providing an evidence base for the treatment of aspiration pneumonia in older people is required.
Keywords: aspiration pneumonia, antibiotics, antibacterial, antimicrobial, older people
Introduction
The incidence of aspiration pneumonia is difficult to determine, because there are few diagnostic markers for aspiration and most studies do not distinguish between aspiration pneumonia and aspiration pneumonitis.1 Furthermore, studies suggested that as much as 5%–15% of people diagnosed with community-acquired pneumonia (CAP) actually have aspiration pneumonia,2,3 even more so in residential aged-care facility (RACF) residents.2,4 Aspiration pneumonia is becoming more common, with one study showing a 93.5% increase in annual hospitalizations for aspiration pneumonia between 1991 and 1998.5
The most common microorganisms isolated from aspiration pneumonia reflect those found in the oropharynx such as Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, and anaerobes.6 Gram-negative bacilli, S. aureus, and Pseudomonas aeruginosa are more common in institutionalized older people as a result of poor oral hygiene leading to dental decay and gingivitis.7 Pathogenic organisms are also seen in edentulous elderly patients suggesting that coating of the tongue by bacteria also contributes to the risk of aspiration pneumonia.8
Aspiration pneumonia can lead to the development of necrotizing pneumonia or lung abscess, which may require a prolonged course of antibiotics and surgery.9 Aspiration pneumonia can be associated with high mortality with studies reporting figures between 0% and 85%.10 A study of 47 hospitalized patients reported that mortality was 90% if two or more lobes of the lung were involved and 41% if only one lobe was affected.11 Aspiration pneumonia was an independent predictor of 30-day mortality after adjusting for pneumonia category, performance status, severity score, and treatment failure.12
Despite its high incidence and mortality, there has been a lack of research on the treatment of aspiration pneumonia. Hence, the aims of this systematic review were to describe the microbiology of aspiration pneumonia and to determine whether there are data to support optimal antibiotic management in elderly patients.
Materials and methods
Information sources
EMBASE (1980 to April 12, 2018), MEDLINE (1946 to April 14, 2018), and Cochrane (2005 to April 11, 2018) were searched on April 14, 2018, by two independent researchers (TB and JZ). Results were limited to studies in English involving human subjects. Reference lists of full-text papers were hand searched to identify any other relevant studies.
Search terms
Search terms were as follows: aspiration pneumon$.m_titl. or pulmonary aspiration.m_titl. and treatment.mp. or management.mp. or pharmacotherapy.mp. or medication.mp. or antibiotics.mp. or antibacterial.mp. or antimicrobial.mp. Studies were also hand searched for additional relevant publications.
Eligibility criteria
Studies that examined the clinical effectiveness of antibiotic treatment for aspiration pneumonia were selected. All study designs except case reports were included. Studies were excluded if they reported only the treatment of necrotizing pneumonia and lung abscess without a clear history of preceding aspiration or did not include elderly patients (>65 years old). Any discrepancies regarding eligibility or other criteria were resolved by consensus between the two authors, TB and JZ.
Data items
Information on study design and antibiotic treatment including dose and route, study population, number and age of participants, microbiology, clinical efficacy, and any other outcome measures, such as adverse reactions and mortality, was extracted from each study.
Risk of bias assessment
The Cochrane Risk of Bias Assessment Tool13 was used to assess the quality of all included studies.
Results
The database search generated 521 studies of which 354 were reviewed for eligibility after duplicates were removed. After the application of exclusion criteria, eight studies were included in the systematic review (Figure 1).
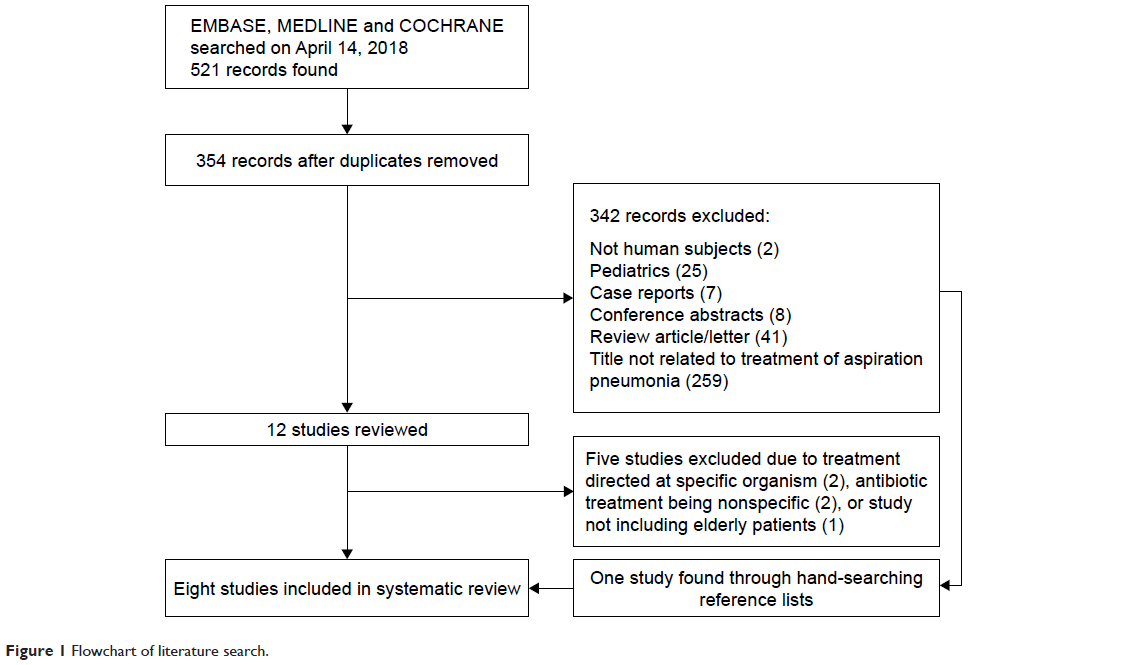 | Figure 1 Flowchart of literature search. |
Microbiology
Table 1 summarizes the microbiological sampling techniques used and the organisms found in the eight studies.
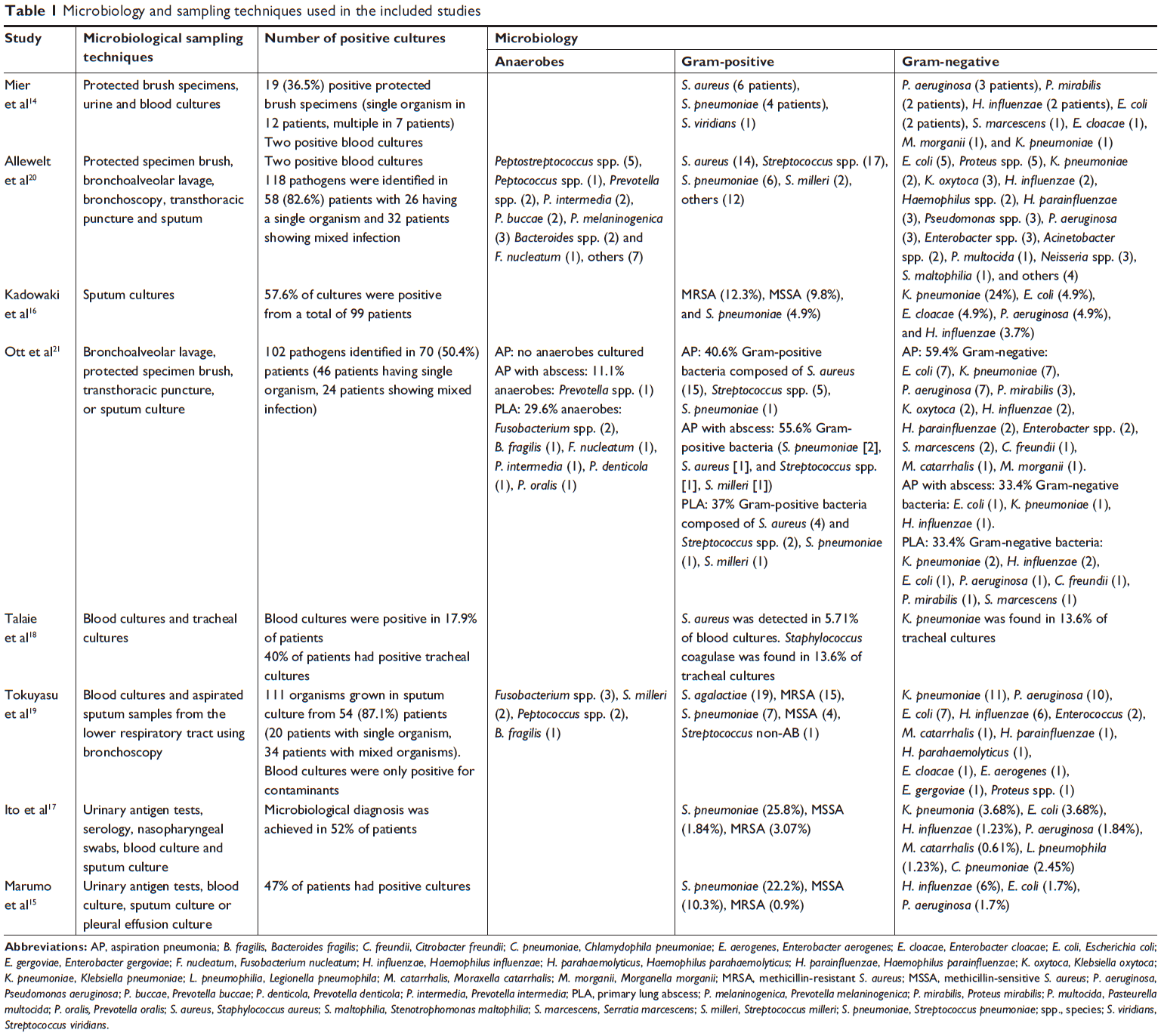 | Table 1 Microbiology and sampling techniques used in the included studies |
Mier et al14 took protected brush specimens from 52 patients as well as urine and blood cultures. There were two positive blood cultures with one patient having S. aureus in both the blood culture and protected brush specimen. The other patient grew S. pneumoniae in their blood culture with a negative protected brush specimen. It should be noted that brush specimens were taken after the administration of antibiotics which might reduce the identification of anaerobes.
In the study by Marumo et al,15 anaerobic cultures were not undertaken on sputum specimens.15 This study identified specific pathogens in 55 patients (47%) using urinary antigen test, blood, sputum, or pleural effusion culture, with S. pneumoniae being the most frequently isolated organism identified in 26 patients (22.2%), followed by methicillin-sensitive S. aureus (MSSA; 10.3%) and H. influenzae (6%; Table 1).
Kadowaki et al16 only used sputum cultures and did not identify any anaerobic bacteria. Of the 100 patients, they obtained sputum samples from 99 patients. 42.4% of these cultures were negative. Gram-negative bacilli accounted for the majority of organisms (48.1%) and Gram-positive bacteria for 40.7% (Table 1). This study also examined the disappearance of these organisms from the sputum following antibiotic treatment and found that some bacteria remained detectable. Methicillin-resistant S. aureus (MRSA) emerged in patients who were administered all antibiotic regimens (22.7% in 3 g ampicillin/sulbactam, 25% in 6 g ampicillin/sulbactam, and 34.8% in panipenem/betamiprom [PAPM/BP]) except clindamycin.16
Ito et al17 utilized urinary antigen tests, serology, nasopharyngeal swabs, and blood and sputum culture and identified a microbial diagnosis in 52% of patients. While Gram-positive bacteria, Gram-negative bacteria, and viruses were all isolated, no anaerobes were cultured. It is interesting to note that mixed infection with other bacteria and nonbacterial pathogens occurred in nine patients who were culture positive for S. pneumoniae.17
While the absence of anaerobes isolated on sputum culture is not surprising, the tracheal and blood cultures performed on all patients enrolled in the study by Talaie et al18 also failed to yield any anaerobic bacteria. Their results showed a positive blood culture in 18.6% of patients in the ceftriaxone/clindamycin treatment arm, with 4.3% of cultures positive for S. aureus. In the cefepime/clindamycin group, 17.1% of blood cultures were positive including 7.1% positive for S. aureus. Tracheal cultures were positive in 38.6% and 41.4% of these patients, respectively. A combination of Klebsiella pneumoniae and Staphylococcus coagulase was found in 12.9% and 14.3%, respectively.18
Tokuyasu et al19 used bronchoscopy to obtain aspirated sputum samples from the lower respiratory tract and isolated anaerobic organisms in 27.4% and Gram-negative rods in 51.6% of patients. The Gram-positive organisms isolated were Streptococcus agalactiae, MRSA, S. pneumoniae, MSSA, and Streptococcus non AB, and 54.8% of patients had mixed growth (Table 1).19
All 70 enrolled participants in the study by Allewelt et al20 had microbiological sampling through either protected specimen brush, bronchoalveolar lavage, sputum, transthoracic puncture, or bronchoscopically obtained bronchial secretions. Bacteria were identified in 58 patients, with mixed infection present in 32 of these patients. Anaerobes were found in 25 cases from protected specimen brush and bronchoalveolar lavage. The largest group of organisms isolated was Gram-positive bacteria, which accounted for 51 cases while Gram-negative bacteria were responsible for 42 cases (Table 1).20
Ott et al21 used more invasive procedures to obtain microbiological samples including bronchoalveolar lavage, protected specimen brush, and transthoracic puncture. Of 139 patients, 70 patients had positive cultures. Multiple organisms were found in 24 of these patients. In patients with aspiration pneumonia, no anaerobes were cultured from their specimens. The aerobes consisted of 40.6% Gram-positive bacteria and 59.4% Gram-negative bacteria (Table 1). Patients with aspiration pneumonia with lung abscess grew both anaerobic and aerobic bacteria; however, the only anaerobes isolated were Prevotella spp. The Gram-positive bacteria were more frequent than Gram-negative bacteria (55.6% vs 33.4%). It is important to note that some patients were treated with antibiotics prior to enrollment in this study.21
All eight studies used different, and some multiple, sampling techniques to identify microorganisms. Invasive techniques, such as bronchoscopy, recovered more anaerobic bacteria than less invasive techniques, such as sputum and blood cultures which isolated mainly aerobic bacteria. The most common Gram-negative organisms were Escherichia coli, K. pneumoniae, and P. aeruginosa, and the most common Gram-positive organisms were S. aureus and S. pneumoniae. Many studies reported mixed growth. The results are limited by the poor sensitivity and specificity of respiratory isolates22 and the prior administration of antibiotics in some studies.
Antibacterial treatment of aspiration pneumonia
Study characteristics are summarized in Table 2. Studies identified participants for inclusion in the studies based on both clinical and radiological evidence of aspiration pneumonia. The eight studies included are of reasonable quality, and the majority have used comparative and prospective design protocols.
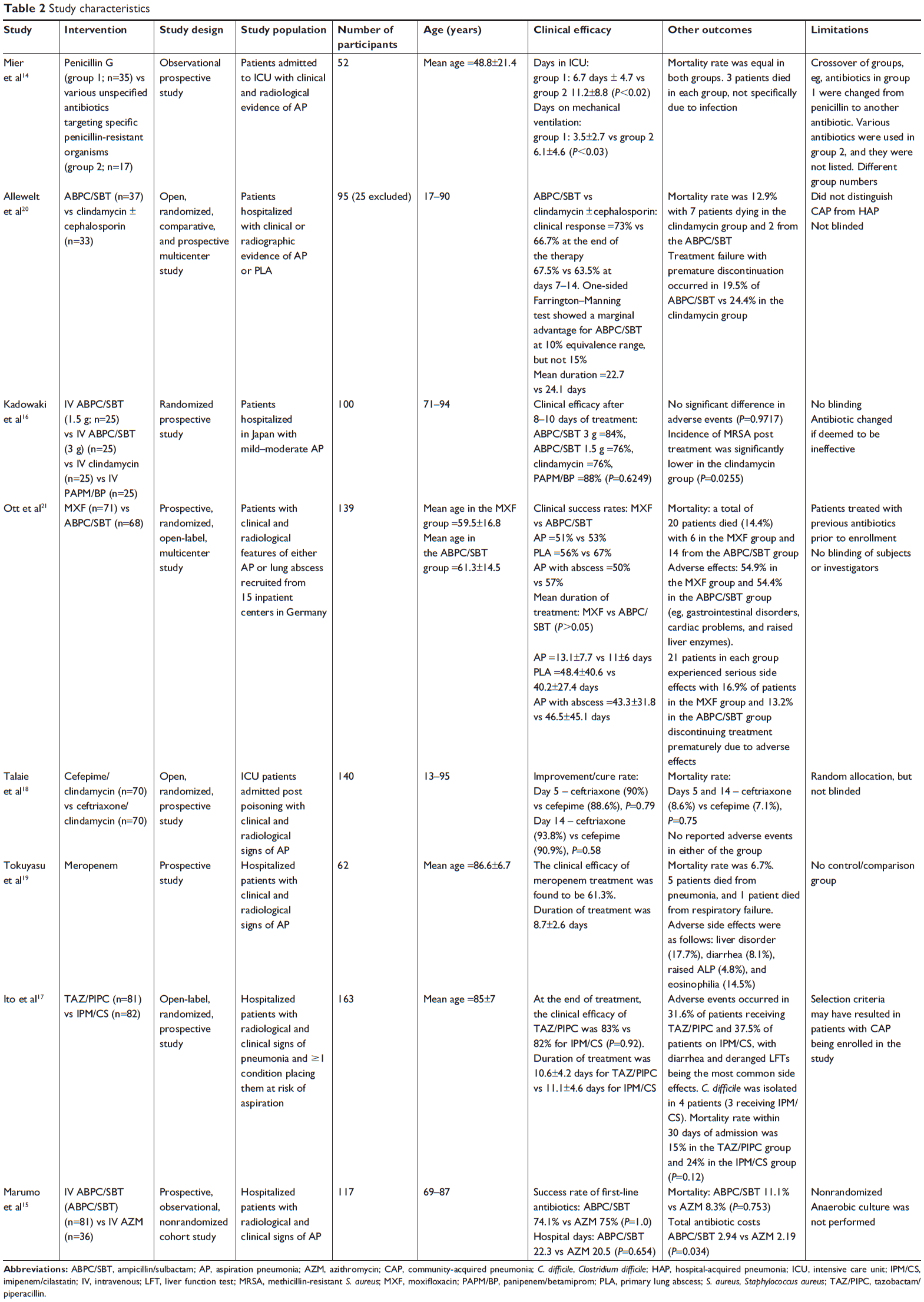 | Table 2 Study characteristics |
Mier et al14 examined the use of penicillin G as an initial antibiotic treatment in patients admitted to the intensive care unit (ICU), with treatment amended if the organism was resistant to penicillin. The patients were thus divided into two groups; with group one receiving penicillin and group 2 receiving tailored antibiotic therapy, although antibiotic class and regimen was not specified. There were significant differences in patient characteristics between the groups: those from group 2 were older, more unwell (lower blood pressure, higher creatinine), and admitted from another hospital ward rather than the community. Patients in group 2 spent longer time in ICU (6.7±4.7 vs 11.2±8.8 days, P≤0.02) and on mechanical ventilation (3.5±2.7 vs 6.1±4.6 days, P=<0.03), but there was no significant difference in mortality.
Allewelt et al20 randomized patients with aspiration pneumonia and primary lung abscess into treatment with either ampicillin/sulbactam or clindamycin ± cephalosporin, with 72.7% of the clindamycin group receiving a cephalosporin. Cephalosporins included cefotiam (n=12), cefuroxime (n=6), cefazolin (n=2), ceftazidime (n=2), cefotaxime (n=1), and ceftriaxone (n=1). Twenty-five subjects were excluded from the final analysis because of the violation of exclusion criteria, receiving antibiotics not in the treatment protocol or loss to follow-up. The final two groups were similar in baseline characteristics, with the only significant difference being a greater majority of males in the ampicillin/sulbactam group (86.5% vs 63.6%, P=0.05). The study found that, in patients treated with ampicillin/sulbactam, improvement occurred in 73% of patients at the end of therapy and in 67.5% by the final examination. In 66.7% of patients treated with clindamycin, there was an improvement at the end of therapy and 63.6% had improved by the final examination. Statistical analysis with a one-sided Farrington–Manning test showed an advantage for ampicillin/sulbactam over clindamycin at the 10% equivalence range, but the antibiotics were equally effective at the 15% equivalence range. However, treatment failure and a higher discontinuation rate were seen in the ampicillin/sulbactam group (24.4% vs 19.5%), while the 12.9% mortality rate was composed mainly of patients in the clindamycin group, perhaps suggesting that patients in the clindamycin group had more severe disease. The limitations of this study were the absence of blinding and administration of antibiotics prior to study inclusion, thus selecting for more resistant organisms. The authors concluded that this study suggests a possible, albeit very weak, advantage of ampicillin/sulbactam over clindamycin.
Kadowaki et al16 examined the use of ampicillin/sulbactam and clindamycin in patients with aspiration pneumonia aged between 71 and 94 years. This unblinded study compared three different antibiotics and different doses of ampicillin/sulbactam that were adjusted according to response. The study found no significant difference in the clinical efficacy, side effects, or treatment duration (Table 2) between the four groups. Patients on the full dose of ampicillin/sulbactam were noted to suffer from more diarrhea and blood-stained bowel discharge compared to patients receiving the half dose. The study was terminated early because MRSA emerged in all treatment groups, except clindamycin. Therefore, this study showed no difference in antibiotic efficacy with the major difference being adverse effect profiles.
Ott et al21 compared ampicillin/sulbactam to moxifloxacin in patients with aspiration pneumonia, primary lung abscess, and aspiration pneumonia with cavitation. The two groups were comparable in characteristics and dropout rate (32.4% vs 29.4%), and there was similar efficacy between the groups (moxifloxacin 52% vs ampicillin/sulbactam 57%). The incidence of treatment side effects was equivalent (moxifloxacin 54.9% vs ampicillin/sulbactam 54.4%). Treatment failure resulting in premature discontinuation occurred in 22.1% in the ampicillin/sulbactam group compared to 15.5% of the moxifloxacin group. The mortality rate was 14.4%, being composed of 14 patients from the ampicillin/sulbactam group and six patients from the moxifloxacin group. The main limitations were the absence of blinding and the inclusion of patients who had received antibiotics prior to recruitment.
Marumo et al15 compared ampicillin/sulbactam to azithromycin in patients admitted to hospital from an RACF or long-term care hospital with aspiration pneumonia. This study showed that there was no difference in the success rate of first-line antibiotics between the ampicillin/sulbactam and azithromycin groups (74.1% vs 75%). There was no significant difference in mortality (11.1% vs 8.3%) or length of hospital stay (22.3±7.3 vs 20.5±8.1 days), although the length of stay was protracted. The participants were not randomized in this study, but patient characteristics were similar between groups, including the severity of pneumonia.
Ito et al17 evaluated the use of tazobactam/piperacillin and imipenem/cilastatin in the treatment of moderate-to-severe pneumonia in patients with at least one risk factor for aspiration pneumonia. Patients were recruited from the community or RACF. Baseline characteristics of the groups were not significantly different. At the end of treatment, resolution of pneumonia for tazobactam/piperacillin was 80% vs 79% (not significant) for imipenem/cilastatin in the modified intention-to-treat population and 83% vs 82% (ns) in those who adhered to the study protocol. However, the tazobactam/piperacillin group showed more prompt improvement with lower white cell count and temperature at day 4. In post hoc subgroup analyses, when antibiotics were analyzed against microbiological data, tazobactam/piperacillin was better at improving outcomes in patients with Gram-positive bacteria with and without mixed infection (96% vs 73%, P=0.03). There was no significant difference in adverse events (24 vs 32 events), with diarrhea being the most frequent adverse event in both groups. Clostridium difficile was isolated in four cases, with three cases in patients on imipenem/cilastatin. The mortality rate was 15% in the tazobactam/piperacillin group compared to 24% on imipenem/cilastatin, which was not statistically significant. The main limitation of this study was the fact that patients without aspiration pneumonia may have been enrolled due to the inclusion criteria stipulating that patients only had to have one risk factor for aspiration pneumonia. Some patients had positive viral cultures which was not consistent with bacterial aspiration pneumonia. Patients were not blinded to their treatment.
Tokuyasu et al19 examined the use of carbapenems for the treatment of aspiration pneumonia in patients ≥75 years old in a small prospective study. Participants had an average age of 86.6 years, 56% were from an RACF, 93.5% were bedbound, 50% were being fed with enteral feeding tubes, and 77.4% had at least one comorbidity. The duration of treatment with meropenem was 8.7±2.6 days, and the main adverse side effects experienced were mild and included liver dysfunction, diarrhea, and eosinophilia. The efficacy rate was 61.3% with a mortality rate of 9.7% directly related to the aspiration pneumonia. Efficacy of treatment was lower in patients with percutaneous endoscopic gastrostomy (PEG) feeding (44.8%) compared to the non-PEG group (75.8%; P≤0.05). This reflects patients with PEG tubes having a more severe pneumonia (89.7% vs 69.7%, P=0.05), as classified by the Japanese Respiratory Society (JRS) classification. There was no comparison or control group. There was a high rate of adverse events, and 33 (53%) patients grew new MRSA infections after receiving meropenem.
Talaie et al18 studied cefepime/clindamycin vs ceftriaxone/clindamycin in overdose patients with the evidence of aspiration pneumonia admitted to ICU with the majority requiring mechanical ventilation. The average age of patients in this study was approximately 32 years, but it included patients up to the age of 95 years and hence was included in this systematic review. The clinical response between the cefepime and ceftriaxone groups was not statistically significant at day 5 (88.6% vs 90%, P=0.79) or day 14 (90.9% vs 93.8%, P=0.58). No patients experienced any adverse reactions. The mortality rate was not statistically significant between the groups with 7.1% in the cefepime group and 8.6% in the ceftriaxone group (P=0.75). The high success rate seen in this study compared to previous studies is likely due to the young average age and the possible inclusion of patients with aspiration pneumonitis that may have improved without antibiotic treatment. Furthermore, the investigators were not blinded to the treatment groups. Extrapolation of these data to the older population is therefore problematic.
In summary, the antibiotics studied have predominantly been broad spectrum, covering both Gram-positive and Gram-negative bacteria, with the exception of penicillin and clindamycin that have relatively poor Gram-negative activity.23 Inclusion of anaerobic cover was not universal, with only the following antibiotics having anti-anaerobic activity: clindamycin, moxifloxacin, carbapenems, and ampicillin/sulbactam.23 Hence, these antibiotics covered the majority of the pathogens isolated through microbiological sampling, and similar efficacy rates were seen in all comparative trials. The most significant differences arose in side effect profiles and the development of resistant organisms. Studies were limited by the absence of blinding, lack of randomization, and participants receiving antibiotic treatment prior to enrollment.
Risk of bias within studies
All eight studies were assessed for the risk of bias using the Cochrane Risk of Bias Tool (Table S1). Performance and detection bias were found to be high in most studies due to the absence of blinding. Only three studies described randomization of subjects.16,18,21 High attrition bias was suspected in the study by Allewelt et al20 which analyzed outcomes of the “according-to-protocol” group with missing data from the “intention-to-treat” group due to participants either dropping out or being excluded from the study due to protocol violations. The absence of data on clinical efficacy,14 bacteriological response,21 and adverse events15 in three studies was suggestive of selective outcome reporting.
Discussion
There was a predominance of both Gram-negative and Gram-positive bacteria, while anaerobes were infrequently identified. This may reflect methodological issues related to the collection of samples, the use of anaerobic culture techniques, or prior administration of antibiotics. However, the consistency between the studies does seem to suggest that anaerobes are an infrequent cause of aspiration pneumonia. Negative cultures and results showing mixed growth were frequent.
To date, there have been no large, double-blinded, randomized control trials comparing different antibiotics commonly used to treat aspiration pneumonia. The majority of studies have been prospective in nature with randomization of groups, but minimal blinding and relatively small numbers of patients. They have utilized broad-spectrum antibiotics to cover Gram-positive, Gram-negative, and at times, anaerobic bacteria. For example, Talaie et al18 compared two groups of broad-spectrum cephalosporins. Both groups received clindamycin as well and the response rates in these groups (90.9% vs 93.8%) were higher compared to the study by Allewelt et al,20 which used mainly moderate-spectrum cephalosporins. Carbapenems were the broadest spectrum antibiotics studied, but the study by Tokuyasu et al19 showed a very low clinical efficacy of 61.3%, especially when compared to the efficacy of 88% achieved with PAPM/BP in the study by Kadowaki et al16 and 82% in the study by Ito et al.17 This is likely due to the population studied, which included patients ≥75 years old with the majority being from RACFs with poor functional status, some receiving enteral feeding and many having multiple comorbidities. Nevertheless, the mortality rate was 9.7%,19 which is comparable with other studies.20,21 However, the most worrying and not unexpected result in these studies was the emergence of resistant organisms16,19 and C. difficile.17
The other five studies examined the clinical efficacy of penicillin with no significant difference found between the comparison groups. Four studies examined beta-lactam/beta-lactam inhibitors, but only one paper examined the use of narrow-spectrum penicillin G in the treatment of aspiration pneumonia. Unfortunately, this study by Mier et al14 was flawed as all patients received an initial dose of penicillin G and then their antibiotic was changed depending on the culture results. Another study that examined the use of penicillin G was unable to be included in this literature review as the age range of the participants was not specified and only an average range of 50–55 years was given.24 The study by Bartlett and Gorbach24 showed a comparable efficacy of penicillin G (75%) to clindamycin (84%) in patients with aspiration pneumonia and primary lung abscess.
Therapeutic guidelines in Australia support first-line treatment with penicillin, clindamycin, or cephalosporins depending on severity, with piperacillin/tazobactam used as the second-line treatment if resistant Gram-negative organisms are thought to be present.25 Metronidazole is added to the treatment regimen if there is evidence of anaerobic organisms,25 despite the lack of evidence to support this recommendation.26 While metronidazole has good in vitro activity against anaerobes, clinically it does not appear to be useful in anaerobic pulmonary infections.27,28
The JRS, British Thoracic Society, and American Thoracic Society/Infectious Disease Society of America (ATS/IDSA) guidelines recommend initial treatment with ampicillin/sulbactam,6,29,30 which is supported by four of the studies.15,16,20,21 ATS/IDSA also supports the use of clindamycin and carbapenam,30 in which Kadowaki et al16 showed to be as efficacious as ampicillin/sulbactam.
The duration of antibacterial treatment and clinical outcomes in these studies may have been affected by other factors such as length of time patients remained nil per os (NPO), as Maeda et al31 showed that patients who were NPO for shorter periods had better nutritional status, shorter antibiotic duration, and less impaired swallowing ability. While this was not evident in Tokuyasu et al19 who demonstrated longer fasting periods in the non-PEG group, but no significant difference in the nutritional status or antibiotic duration between the groups, this could be due to the PEG group having greater pneumonia severity. Only two other studies commented on the introduction of oral intake, but no specific timeframes were given.15,16 Introduction of oral intake by Marumo et al15 was based on the decision of the physician, which is known to be highly variable and usually longer than necessary.32 However, patients in the study by Kadowaki et al16 were permitted oral intake only after a period of swallowing rehabilitation and comprehensive oral care, two strategies known to prevent relapse of aspiration pneumonia.33 The fact that only one study implemented preventative measures is in keeping with current data demonstrating that recurrence prevention of aspiration pneumonia by physicians is poor.34
This is the only systematic review that has analyzed the antibacterial treatment of aspiration pneumonia in the older person. However, it is limited by including studies only in English. The lack of randomized control trials and the heterogeneity between the eight studies meant that a meta-analysis could not be performed. This study examined only the treatment of aspiration pneumonia and not prevention, which is an important consideration given that aspiration pneumonia is usually a recurrent problem.33,34 Randomized controlled trials need to be performed now, so that a more evidence-based treatment algorithm can be designed. For example, it would be beneficial to compare intravenously (IV) to orally administered ampicillin/sulbactam and penicillin G to ampicillin/sulbactam.
Conclusion
This literature review highlights the paucity of data guiding the treatment of aspiration pneumonia. Given the rapidly aging population and the high incidence and mortality associated with aspiration pneumonia, more research needs to be directed toward both prevention and treatment. Existing evidence supports the use of broad-spectrum antibiotics, but consideration needs to be given to the rapidly emerging problem of antibacterial resistance juxtaposed with the slow development of new antibacterial agents, calling for judicious, evidence-based prescribing. Research now needs to be directed toward comparing these agents to more narrow-spectrum antibiotics to determine whether there is a difference in therapeutic outcomes.
Acknowledgments
We thank Professor David Le Couteur for his advice and comments in preparing this manuscript for publication. This paper was presented at the Australian and New Zealand Society for Geriatric Medicine Annual Scientific Meeting as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in the Australasian Journal of Ageing 2016;35(Suppl S1):42; https://doi.org/10.1111/ajag.12338.
Disclosure
The authors report no conflicts of interest in this work.
References
Marik PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001;344(9):665–671. | ||
Marrie TJ, Durant H, Yates L. Community-acquired pneumonia requiring hospitalization: 5-year prospective study. Rev Infect Dis. 1989;11(4):586–599. | ||
Torres A, Serra-Batlles J, Ferrer A, et al. Severe community-acquired pneumonia. Epidemiology and prognostic factors. Am Rev Respir Dis. 1991;144(2):312–318. | ||
Reza Shariatzadeh M, Huang JQ, Marrie TJ. Differences in the features of aspiration pneumonia according to site of acquisition: community or continuing care facility. J Am Geriatr Soc. 2006;54(2):296–302. | ||
Baine WB, Yu W, Summe JP. Epidemiologic trends in the hospitalization of elderly Medicare patients for pneumonia, 1991–1998. Am J Public Health. 2001;91(7):1121–1123. | ||
Japanese Respiratory Society. Aspiration pneumonia. Respirology. 2009;14(Suppl 2):S59–S64. | ||
El-Solh AA, Pietrantoni C, Bhat A, et al. Colonization of dental plaques: a reservoir of respiratory pathogens for hospital-acquired pneumonia in institutionalized elders. Chest. 2004;126(5):1575–1582. | ||
Abe S, Ishihara K, Adachi M, Okuda K. Tongue-coating as risk indicator for aspiration pneumonia in edentate elderly. Arch Gerontol Geriatr. 2008;47(2):267–275. | ||
Lode H. Microbiological and clinical aspects of aspiration pneumonia. J Antimicrob Chemother. 1988;21(Suppl C):83–90. | ||
Hickling KG, Howard R. A retrospective survey of treatment and mortality in aspiration pneumonia. Intensive Care Med. 1988;14(6):617–622. | ||
Cameron JL, Mitchell WH, Zuidema GD. Aspiration pneumonia. Clinical outcome following documented aspiration. Arch Surg. 1973;106(1):49–52. | ||
Komiya K, Ishii H, Umeki K, et al. Impact of aspiration pneumonia in patients with community-acquired pneumonia and healthcare-associated pneumonia: a multicenter retrospective cohort study. Respirology. 2013;18(3):514–521. | ||
Higgins JPT, Altman DG, Sterne JAC [homepage on the Internet]. Chapter 8: assessing risk of bias in included studies. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration; 2011. Available from: www.handbook.cochrane.org. Accessed September 26, 2018. | ||
Mier L, Dreyfuss D, Darchy B, et al. Is penicillin G an adequate initial treatment for aspiration pneumonia? A prospective evaluation using a protected specimen brush and quantitative cultures. Intensive Care Med. 1993;19(5):279–284. | ||
Marumo S, Teranishi T, Higami Y, Koshimo Y, Kiyokawa H, Kato M. Effectiveness of azithromycin in aspiration pneumonia: a prospective observational study. BMC Infect Dis. 2014;14:685. | ||
Kadowaki M, Demura Y, Mizuno S, et al. Reappraisal of clindamycin IV monotherapy for treatment of mild-to-moderate aspiration pneumonia in elderly patients. Chest. 2005;127(4):1276–1282. | ||
Ito I, Kadowaki S, Tanabe N, et al. Tazobactam/piperacillin for moderate-to-severe pneumonia in patients with risk for aspiration: comparison with imipenem/cilastatin. Pulm Pharmacol Ther. 2010;23(5):403–410. | ||
Talaie H, Jabari HR, Shadnia S, Pajouhmand A, Nava-Ocampo AA, Youssefi M. Cefepime/clindamycin vs. ceftriaxone/clindamycin for the empiric treatment of poisoned patients with aspiration pneumonia. Acta Biomed. 2008;79(2):117–122. | ||
Tokuyasu H, Harada T, Watanabe E, et al. Effectiveness of meropenem for the treatment of aspiration pneumonia in elderly patients. Intern Med. 2009;48(3):129–135. | ||
Allewelt M, Schüler P, Bölcskei PL, Mauch H, Lode H; Study Group on Aspiration Pneumonia. Ampicillin + sulbactam vs clindamycin +/− cephalosporin for the treatment of aspiration pneumonia and primary lung abscess. Clin Microbiol Infect. 2004;10(2):163–170. | ||
Ott SR, Allewelt M, Lorenz J, Reimnitz P, Lode H; German Lung Abscess Study Group. Moxifloxacin vs ampicillin/sulbactam in aspiration pneumonia and primary lung abscess. Infection. 2008;36(1):23–30. | ||
Reimer LG, Carroll KC. Role of the microbiology laboratory in the diagnosis of lower respiratory tract infections. Clin Infect Dis. 1998;26(3):742–748. | ||
Australian Medicines Handbook 2018 (online). Adelaide: Australian Medicines Handbook Pty Ltd; 2018 July. Available from: https://amhonline.amh.net.au/. Accessed June 7, 2018. | ||
Bartlett JG, Gorbach SL. Treatment of aspiration pneumonia and primary lung abscess. Penicillin G vs clindamycin. JAMA. 1975;234(9):935–937. | ||
eTG complete [Internet]. Melbourne: Therapeutic Guidelines Limited; 2018 July. Available from: https://tgldcdp.tg.org.au/etgcomplete. Accessed July 18, 2018. | ||
Kwong JC, Howden BP, Charles PG. New aspirations: the debate on aspiration pneumonia treatment guidelines. Med J Aust. 2011;195(7):380–381. | ||
Perlino CA. Metronidazole vs Clindamycin Treatment of Anaerobic Pulmonary Infection. Arch Intern Med. 1981;141(11):1424–1427. | ||
Sanders CV, Hanna BJ, Lewis AC. Metronidazole in the treatment of anaerobic infections. Am Rev Respir Dis. 1979;120(2):337–343. | ||
Lim WS, Baudouin SV, George RC, et al ; Pneumonia Guidelines Committee of the BTS Standards of Care Committee. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009;64(Suppl 3):iii1–iii55. | ||
Mandell LA, Wunderink RG, Anzueto A, et al; Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–S72. | ||
Maeda K, Koga T, Akagi J. Tentative nil per os leads to poor outcomes in older adults with aspiration pneumonia. Clin Nutr. 2016;35(5):1147–1152. | ||
Kenzaka T, Kosami K, Matsuoka Y, Noda A, Kumabe A. The Difference between Ideal and Actual Fasting Duration in the Treatment of Patients with Aspiration Pneumonia: A Nationwide Survey of Clinicians in Japan. Tohoku J Exp Med. 2016;240(3):227–233. | ||
Kohno S, Imamura Y, Shindo Y, et al. Clinical practice guidelines for nursing- and healthcare-associated pneumonia (NHCAP) [complete translation]. Respir Investig. 2013;51(2):103–126. | ||
Kenzaka T, Kumabe A, Kosami K, et al. Bacteriological testing and recurrence prevention efforts in the diagnosis and treatment of nursing- and healthcare-associated pneumonia and aspiration pneumonia: A questionnaire survey of hospitals across Japan. Respir Investig. 2018;56(2):150–157. |
Supplementary material
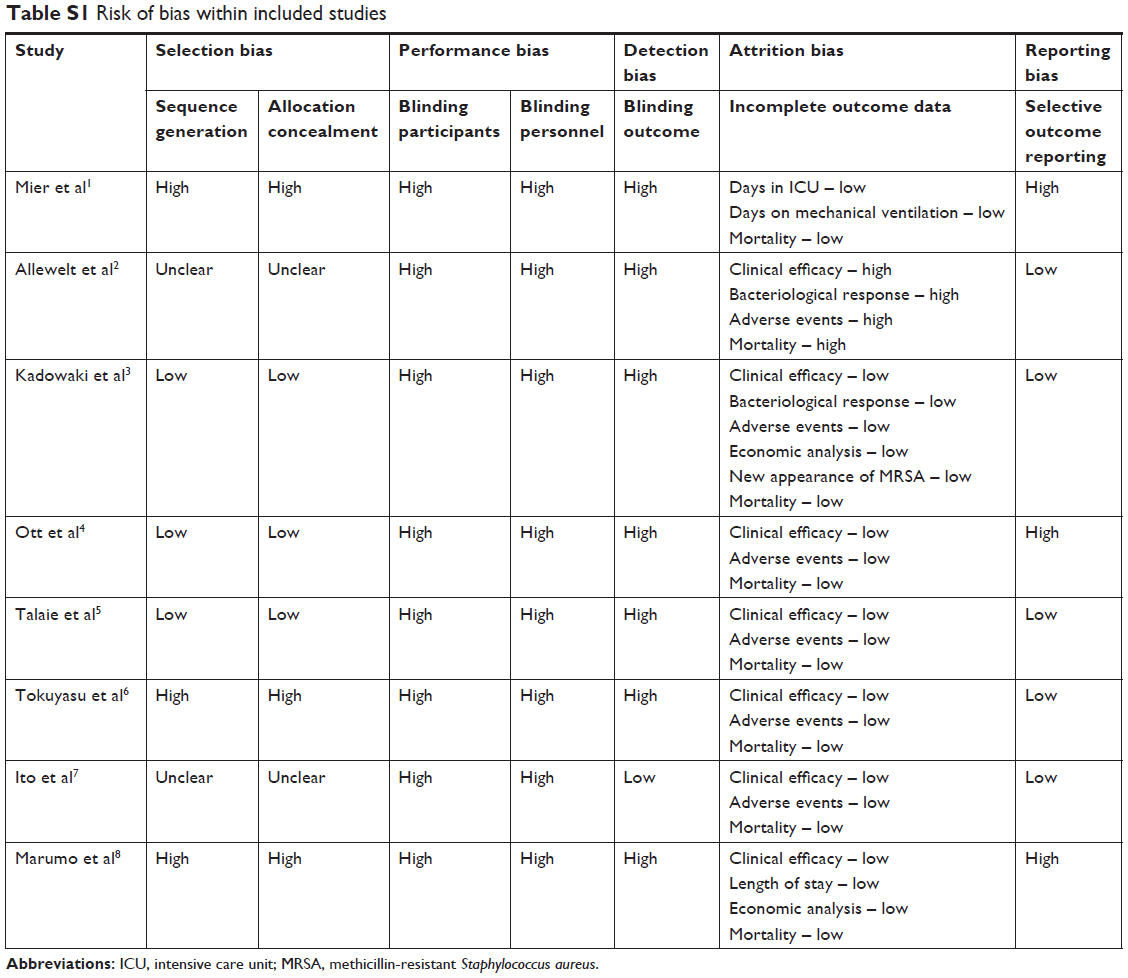 | Table S1 Risk of bias within included studies |
References
Mier L, Dreyfuss D, Darchy B, et al. Is penicillin G an adequate initial treatment for aspiration pneumonia? A prospective evaluation using a protected specimen brush and quantitative cultures. Intensive Care Med. 1993;19(5):279–284. | ||
Allewelt M, Schüler P, Bölcskei PL, Mauch H, Lode H; Study Group on Aspiration Pneumonia. Ampicillin + sulbactam vs clindamycin +/− cephalosporin for the treatment of aspiration pneumonia and primary lung abscess. Clin Microbiol Infect. 2004;10(2):163–170. | ||
Kadowaki M, Demura Y, Mizuno S, et al. Reappraisal of clindamycin IV monotherapy for treatment of mild-to-moderate aspiration pneumonia in elderly patients. Chest. 2005;127(4):1276–1282. | ||
Ott SR, Allewelt M, Lorenz J, Reimnitz P, Lode H; German Lung Abscess Study Group. Moxifloxacin vs ampicillin/sulbactam in aspiration pneumonia and primary lung abscess. Infection. 2008;36(1):23–30. | ||
Talaie H, Jabari HR, Shadnia S, Pajouhmand A, Nava-Ocampo AA, Youssefi M. Cefepime/clindamycin vs. ceftriaxone/clindamycin for the empiric treatment of poisoned patients with aspiration pneumonia. Acta Biomed. 2008;79(2):117–122. | ||
Tokuyasu H, Harada T, Watanabe E, et al. Effectiveness of meropenem for the treatment of aspiration pneumonia in elderly patients. Intern Med. 2009;48(3):129–135. | ||
Ito I, Kadowaki S, Tanabe N, et al. Tazobactam/piperacillin for moderate-to-severe pneumonia in patients with risk for aspiration: comparison with imipenem/cilastatin. Pulm Pharmacol Ther. 2010;23(5):403–410. | ||
Marumo S, Teranishi T, Higami Y, Koshimo Y, Kiyokawa H, Kato M. Effectiveness of azithromycin in aspiration pneumonia: a prospective observational study. BMC Infect Dis. 2014;14:685. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.