Back to Journals » Clinical Ophthalmology » Volume 16
Anti-Vascular Endothelial Growth Factor Treatment for Macular Edema in Eyes with Branch Retinal Vein Occlusion with vs Without Glaucoma – Does Glaucoma Affect Visual Outcome in Eyes with BRVO-ME After antiVEGF Injections?
Authors Asami S, Sugimoto M ![]() , Tsukitome H, Kato K, Matsubara H, Kondo M
, Tsukitome H, Kato K, Matsubara H, Kondo M
Received 1 January 2022
Accepted for publication 7 June 2022
Published 15 July 2022 Volume 2022:16 Pages 2275—2283
DOI https://doi.org/10.2147/OPTH.S356727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Shin Asami, Masahiko Sugimoto, Hideyuki Tsukitome, Kumiko Kato, Hisashi Matsubara, Mineo Kondo
Department of Ophthalmology, Mie University Graduate School of Medicine, Tsu, Mie, Japan
Correspondence: Masahiko Sugimoto, Department of Ophthalmology, Mie University Graduate School of Medicine, 2-174 Edobashi, Tsu, Mie, 514-8507, Japan, Tel +81-59-231-5027, Fax +81-59-231-3036, Email [email protected]
Purpose: To compare the therapeutic effects of anti-vascular endothelial growth factor (anti-VEGF) agents in eyes with macular edema associated with branch retinal vein occlusion (BRVO-ME) with glaucoma to those without glaucoma.
Patients and Methods: This retrospective study was conducted using the medical records of Mie University Hospital from 2013 to 2017. Patients were recruited if they had received anti-VEGF agents for BRVO-ME treatment and included 30 patients (30 eyes) without glaucoma (G[-] group) and 27 patients (27 eyes) with glaucoma (G[+] group). The central retinal thickness (CRT) and best-corrected visual acuity (BCVA) at 3 months after a single injection of anti-VEGF agents were compared between the two groups.
Results: Before treatment, the mean±standard deviation of the CRT was 514.2± 117.3 μm for the G[-] group, which was not significantly different from that for the G[+] group (533.4± 171.4 μm). The CRT in the G[-] and G[+] groups significantly reduced to 321.1± 114.6 μm and 347.8± 134.7 μm, respectively, at 1 month after the injection and to 360.4± 159.5 μm and 352.4± 151.9 μm, respectively, at 3 months after the injection (P< 0.01 for each group). The difference in the degree of CRT reduction between the two groups was not significant. Before treatment, the BCVA was 0.42± 0.32 logMAR units in the G[-] group and 0.57± 0.33 logMAR units in the G[+] group, showing no significant difference. The BCVA in the G[-] and G[+] groups improved significantly to 0.27± 0.26 logMAR units and 0.34± 0.42 logMAR units, respectively, at 1 month, and to 0.18± 0.20 logMAR units and 0.39± 0.34 logMAR units, respectively, at 3 months (P< 0.01). The BCVA in the G[-] group was significantly better than that in the G[+] group at 3 months (P=0.02).
Conclusion: The therapeutic response of anti-VEGF agents for BRVO-ME is affected by the presence of glaucoma.
Keywords: anti-vascular endothelial growth factor treatment, branch retinal vein occlusion, glaucoma, macular edema
Introduction
Branch retinal vein occlusion (BRVO) is a relatively common retinal vascular disorder with a prevalence of 4.42/1000 individuals.1 Hemodynamic changes, including venous stasis, conformational damage of the vessel walls, and blood hypercoagulability, are important signs of the pathogenesis of BRVO. Various systemic and ophthalmic risk factors are associated with the development of BRVO. Systemic risk factors include systemic hypertension, diabetes mellitus, hyperlipidemia, atherosclerotic-associated diseases, ischemic heart disease, and obesity. An important ophthalmic risk factor for BRVO is glaucoma.2,3 And there is a possibility of a common pathological mechanism for these two disorders.4,5
Macular edema associated with BRVO (BRVO-ME) is a major cause of vision reduction that occurs in 30% of BRVO patients.2 There are many treatment options for BRVO-ME, including grid laser photocoagulation, vitrectomy, and administration of steroid agents. At present, anti-vascular endothelial growth factor (VEGF) treatment is the primary treatment option for BRVO-ME.6 This is because vascular occlusion induces upregulation of VEGF, which results in an increase in vascular permeability and subsequent macular edema (ME). Many clinical studies have shown the beneficial effects of anti-VEGF treatment in eyes with BRVO-ME by using bevacizumab (Avastin®, Genentech, San Francisco, CA, USA), ranibizumab (Lucentis®, Genentech)7 and aflibercept (Eylea®, Regeneron Pharmaceuticals, Tarrytown, NY, USA).8 These anti-VEGF agents have well-established efficacy and safety profiles.
The most important clinical problem in anti-VEGF treatment for BRVO-ME is that it does not improve the visual function of all patients equally. In addition, patients frequently show recurrence, necessitating repeated injections that impose a major financial burden on the patients. We make a hypothesis that the similarities in the vascular pathological mechanisms and structural abnormalities shared by BRVO and glaucoma can influence the effectiveness or clinical course of anti-VEGF treatment for eyes with BRVO-ME with or without glaucoma.
Thus, the aim of this study was to compare the recovery of visual acuity and central retinal thickness after anti-VEGF treatment in patients diagnosed with BRVO-ME with and without glaucoma.
Patients and Methods
This was a retrospective, single-center, case control study. Patients’ data were recorded in the electronic database of Mie University Hospital. All patients were diagnosed with BRVO-ME between January 2013 and December 2017 and had received anti-VEGF treatment. This database contains medical claims data for 377,552 individuals as defined by the Medical Information System Development Center and mapped to the International Classification of Diseases (ICD)-10 codes with a diagnosis of BRVO (20077100), BRVO-ME (20099742), and glaucoma (20055896, 20060425, 20065219, 20066639, and 20077777). All patients were referred after the onset of BRVO-ME.
Each patient underwent a comprehensive ophthalmological examination, including measurements of the best-corrected visual acuity (BCVA) and IOP, examination of the anterior segment by slit-lamp biomicroscopy, examination of the fundus by indirect ophthalmoscopy, and measurement of the central retinal thickness (CRT) in spectral-domain optical coherence tomography (SD-OCT) images.
The inclusion criteria were age ≥20 years, presence of BRVO-ME diagnosed by clinical findings, CRT > 300 μm in the SD-OCT images, and BCVA ≥ 20/320 before treatment. The exclusion criteria at the time of the initial anti-VEGF treatment were as follows: prior ocular surgery, including cataract surgery within 6 months or during the observation period, prior macular laser photocoagulation, and intravitreal or sub-tenon steroid injections within 3 months of the beginning of the study. In addition, eyes with ocular inflammation, drusen, severe proliferative changes, retinal hemorrhage that involved the fovea, presence of an epiretinal membrane, prior pars plana vitrectomy, and media opacities that would have disturbed the OCT images and significantly affected the BCVA, such as vitreous hemorrhage, vitreous opacity, severe cataract, and corneal opacity, were excluded. Patients with uncontrolled systemic medical conditions or a history of thromboembolic events were also excluded.
Definition of Glaucoma
Patients fulfilled the following criteria for the diagnosis of glaucoma before the onset of BRVO-ME at the referral clinic: an open-angle, glaucomatous optic disc appearance such as diffuse or localized rim thinning, a notch in the rim, a vertical cup-to-disc (CD) ratio >0.6 or greater by 0.2 than that of the fellow eye, and glaucomatous VF defects before the onset of the BRVO evaluated at the referral clinic. Thus, we could not collect VF data completely from the referral clinic.
Intravitreal Anti-VEGF Injections
Intravitreal injection of the anti-VEGF agent was performed under subconjunctival or topical anesthesia. Each patient received 0.05 mL of anti-VEGF agent intravitreally with a 30-gauge needle inserted 4 mm posterior to the corneal limbus under sterile conditions. All patients received topical levofloxacin hydrate (1.5% Cravit Ophthalmic Solution ®) for 1 week after the injection. One of three anti-VEGF agents, bevacizumab, ranibizumab, and aflibercept, was used as the anti-VEGF agent. When a recurrence of BRVO-ME was identified on the basis of the OCT images or a worsening of the vision, additional injections of the same agent were administered under a pro re nata (PRN) regimen.
Measurements of BCVA
BCVA was measured using a Landolt chart at every visit. The decimal BCVA values were converted to logarithm of the minimum angle of resolution (logMAR) units for statistical analyses.
Optical Coherence Tomography
CRT measurements were made on the images recorded by the Heidelberg Spectralis OCT instrument (Heidelberg Engineering Inc., Heidelberg, Germany). Because image quality is affected by media opacity, we excluded patients with media opacity, as described above. In addition, because operator skills also affect image quality, trained orthoptists use OCT to guarantee image quality. Finally, properly aligned scans with the best quality were chosen for analysis from the acquired scans. For qualitative and quantitative analyses of the OCT images, the fast macular protocol was used to obtain images with an automatic real-time mean value of 9, which acquired 25 horizontal lines consisting of 1024 A-scans/line. CRT was defined as the thickness between the two boundaries (internal limiting membrane and the highly reflective retinal pigment epithelial line) at the fovea along each A-scan using the attached software, which automatically detects the vitreoretinal junction as the inner retinal boundary and the chorioretinal junction as the outer retinal boundary. This value was automatically calculated from the central retinal thickness map using the attached software.
Statistical Analyses
The results are presented as mean ± standard deviation (SD) values. Kruskal–Wallis one-way analysis of variance was used to determine the significance of the differences during the observations for each group. Mann–Whitney U-tests were used to determine the significance of the differences between the groups. Chi-square tests were used to determine the significance of the differences among the groups. Two-tailed P values of <0.05 were considered significant. Statistical evaluations were performed using the Statcel 4 Statistical Program (Statcel; OMC, Saitama, Japan).
Results
Patient data were extracted from the electronic database of our hospital between January 2013 and December 2017. We evaluated the findings for 27 BRVO-ME eyes with glaucoma (G [+] group) and 30 eyes with BRVO-ME without glaucoma (G [-] group).
Baseline Characteristics
The clinical characteristics of the patients are summarized in Table 1. None of the patients had a mixed arteriovenous occlusion. For the G [-] group, the average age was 69.8 ± 11.1 years, BCVA was 0.42 ± 0.32 logMAR units, CRT was 514.2 ± 117.3 µm, and intraocular pressure (IOP) was 12.7 mmHg. Five eyes received aflibercept, one received bevacizumab, and 24 received ranibizumab. For the G [+] group, the average age was 72.0 ± 10.9 years, BCVA was 0.57 ± 0.33 logMAR units, CRT was 533.4 ± 171.4 µm, and IOP was 15.8 mmHg. Mean CD ratio was 0.76 and 13 eyes received prostaglandin analogues for G [+] group. Three eyes received aflibercept, 10 received bevacizumab, and 14 received ranibizumab. No significant differences in baseline values were found between the two groups before anti-VEGF treatment. The type of anti-VEGF agent used in the two groups was significantly different, with a higher rate of ranibizumab usage in the G [-] group (P = 0.02; Chi-square test).
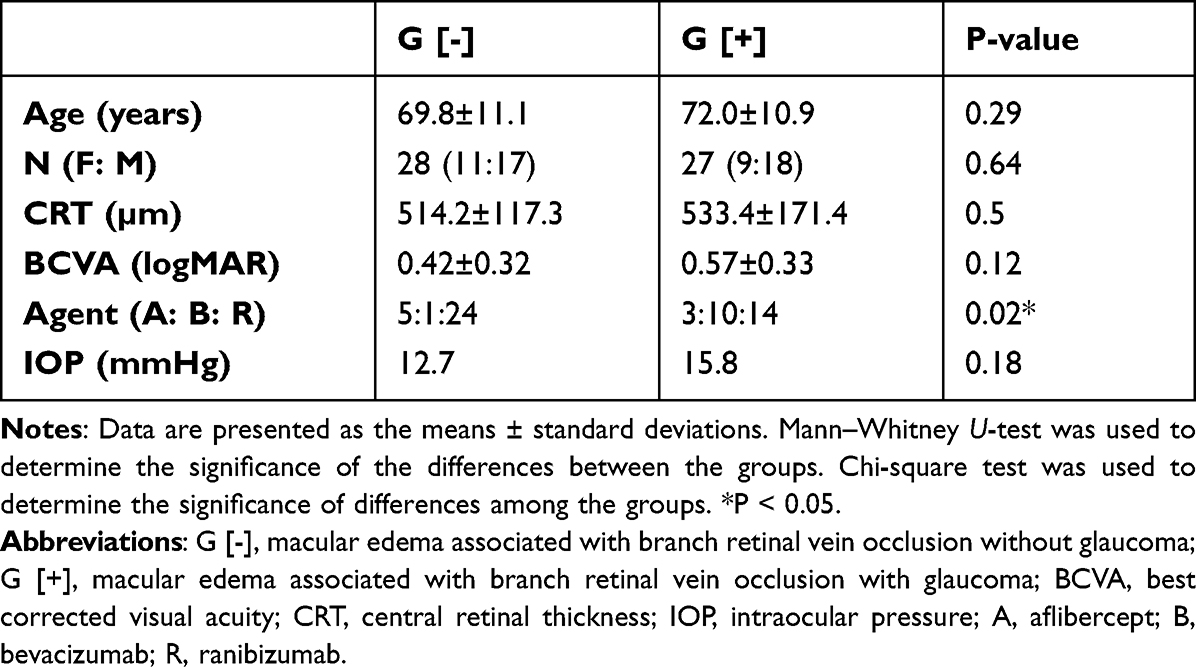 |
Table 1 Baseline Characteristics of the Patients |
Changes in BCVA and CRT During Anti-VEGF Treatment
We analyzed the changes in BCVA and CRT at 1 and 3 months after a single anti-VEGF injection. For the G [-] group, the BCVA significantly improved to 0.27 ± 0.26 logMAR units at 1 month (P = 0.0012; Kruskal–Wallis one-way analysis of variance, Figure 1A) and to 0.18 ± 0.20 logMAR units at 3 months after the injection (P < 0.001, Figure 1A). For the G [+] group, the BCVA significantly improved to 0.34 ± 0.42 logMAR units at 1 month (P < 0.001; Kruskal–Wallis one-way analysis of variance, Figure 1A) and to 0.39 ± 0.34 logMAR units at 3 months after the injection (P < 0.001, Figure 1A).
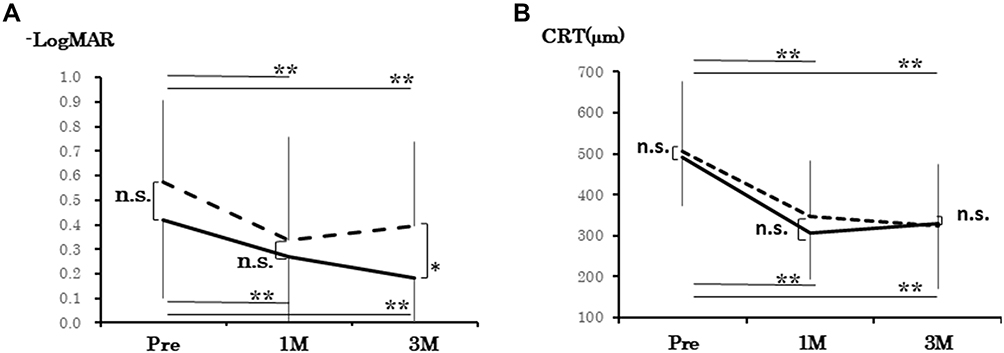 |
Figure 1 The best-corrected visual acuity (BCVA) and central sub-retinal thickness (CRT) at 3 months after a single anti-VEGF injection for eyes without glaucoma (G [-]) and with glaucoma (G [+]). BCVA and CRT significantly improved in both groups during the experimental period. Baseline BCVA did not differ significantly between the two groups (A and B). The two groups showed no significant difference at 1 month after treatment, but the BCVA was significantly worse in the G [+] group than in the G [-] group at 3 months after treatment (P = 0.02). Abbreviations: G [-], macular edema associated with BRVO without glaucoma; G [+], macular edema associated with BRVO with glaucoma; BCVA, best-corrected visual acuity; BRVO, branch retinal vein occlusion; CRT, central retinal thickness; VEGF, vascular endothelial growth factor; ns, not significant. Notes: Line: BRVO without glaucoma, broken line: BRVO with glaucoma.*P < 0.05, **P < 0.01. |
No significant difference was observed in the BCVA between the two groups at 1 month after the injection (P = 0.37; Mann–Whitney U-test), but the BCVA was significantly worse in the G [+] group than in the G [-] group at 3 months after the treatment (P = 0.02, Figure 1A). No significant difference was observed with IOP (P = 0.39).
In the G [-] group, the CRT also significantly reduced to 321.1 ± 114.6 µm at 1 month (P < 0.001, Figure 1B) and to 360.4 ± 159.5 µm at 3 months after the treatment (P < 0.001, Figure 1B). In the G [+] group, the CRT significantly reduced to 347.8 ± 134.7 µm at 1 month (P = 0.001, Figure 1B) and to 352.4 ± 151.9 µm at 3 months after the treatment (P < 0.001, Figure 1B). No significant difference was observed in the CRT between the two groups at 1 and 3 months (P = 0.48 at 1 month and P = 0.95 at 3 months). No significant difference was observed with IOP (P = 0.40).
All patients were treated with additional anti-VEGF injections with the PRN regimen according to the physician’s decision. The mean number of injections during the 1-year follow-up period was 2.1 ± 1.4 for the G [-] group and 2.1 ± 1.3 for the G [+] group (P = 0.68; Chi-square test). Re-injection was performed at 3.6 months (median 3.0 months) in the G [-] group and 4.9 months (median 4.0 months) in the G [+] group without statistically significant difference (P = 0.31).
Discussion
Anti-VEGF agents have become the first-line treatment for BRVO-ME, although there is no standard protocol for the use of these agents. Moreover, these agents are not effective in all cases, and it is still not clear what types of ME cases require additional anti-VEGF treatment or other treatments, including steroid agents or vitrectomy, when anti-VEGF treatment is ineffective. Our findings showed that anti-VEGF agents were effective in the eyes of BRVO-ME patients with or without glaucoma. However, because earlier reduction in BCVA were observed in BRVO-ME with glaucoma compared with those without glaucoma, a glaucomatous background may affect the maintenance of visual function after anti-VEGF treatment.
The Therapeutic Effectiveness of Anti-VEGF Agents for BRVO-ME is Affected by the Presence of Glaucoma
The structural abnormalities of the optic nerve in eyes with BRVO and glaucoma show some relationships,9 and other studies have reported that glaucomatous eyes with unilateral BRVO show faster progression of the visual field defects than the fellow eye.10 An elevated IOP may cause physical compression of the central retinal vein at the lamina cribrosa, which would lead to blood flow disturbances at the optic disc and thrombus formation related to BRVO.11 Vascular abnormalities are another aspect that need to be considered as a risk factor for the development of BRVO in glaucoma patients.12 Different vascular risk factors have been reported for the development of BRVO in glaucoma patients, including reduced ocular blood flow,13 local vasospasm,14 and unstable ocular perfusion pressure.15 Especially, the role of choriocapillaris which shown to be affected in BRVO,16,17 because fellow eyes of patients with unilateral retinal vein occlusion, demonstrates a substantial decrease of perfusion or vascular abnormalities in choriocapillaris. Considering these background factors with our results, there is an urgent need to establish a customized treatment protocol for BRVO-ME with glaucoma.
Because ME does not develop in all BRVO patients,2 it is not clear whether glaucoma is a risk factor for the development of ME and whether it alters the effectiveness of anti-VEGF treatment. Although there are relationships in the pathological signs between BRVO and glaucoma, VEGF is strongly associated with the development of BRVO-ME, and anti-VEGF agents are effective for its treatment. Earlier comparative studies between patients with BRVO-ME and those without normal tension glaucoma (NTG) showed elevation of aqueous endothelin-1 (ET-1) levels in eyes with NTG. However, the aqueous VEGF levels were not significantly different between the two groups, and the authors concluded that the presence of NTG and higher ET-1 concentrations may limit the degree of visual recovery.18 ET-1 is a potent vasoconstrictor that regulates the blood-retinal barrier, stimulates the growth and migration of cells, and regulates axoplasmic transport. It is essential for the maintenance of cardiovascular homeostasis.19 ET-1 was also reported to be important for the development of BRVO-ME,20 thus the biological differences between BRVO and glaucoma, such as the level of ET-1, may contribute to the different rates of BCVA recovery for BRVO-ME irrespective of the presence of glaucoma.
Glaucomatous eyes show specific changes due to previous damage, including visual field defects, enlargement of the cup-disc ratio, and reduction of peripapillar/perifoveal retinal nerve fiber layer (RNFL) thickness. However, similar changes were also observed in the BRVO eye as a result of ischemic damage. In a large cohort consisting of 6173 eyes, optic nerve head morphology was reported to be associated with BRVO, even in non-glaucomatous eyes, which implies that it plays a role in BRVO pathogenesis.21 The visual field sensitivity reduction reflects the non-perfusion region caused by ischemic damage in BRVO with a strong correlation.22 Moreover, several reports have mentioned RNFL reduction in eyes with BRVO, which implies degeneration of retinal ganglion cells.23,24 Although we considered the possibility of some relationships between BRVO and glaucoma, since the present study was based on a retrospective medical record review, there was no systematic information other than the open-angle glaucoma diagnosis before the onset of BRVO-ME. Thus, the exact examination data, including visual field test results and the RNFL data before onset, were not available to follow the progression of glaucomatous damage. To resolve this limitation, a prospective study with a strict protocol should be conducted in the future.
Discrepancies in BCVA and CRT Recovery
Shin et al reported a significant improvement in BRVO-ME after bevacizumab treatment, irrespective of the presence of NTG.18 In addition, they reported, as we found, that the BCVA was significantly worse at 6 months in the presence of NTG than in eyes without NTG, even though both groups showed a similar reduction in the central macular thickness. They also reported that the recurrence rate and the mean number of injections were not significantly different between the two groups, irrespective of the presence of NTG.16 Such discrepancies in the recovery of the CRT and BCVA were also found in our patients. One possible explanation for the discrepancy between the functional and anatomical changes was provided in the context of diabetic ME by the Diabetic Retinopathy Clinical Research Network.25 They stated,
Although OCT measurements of retinal thickness represent an important tool in clinical evaluation, they cannot substitute reliably as a surrogate for visual acuity at a given point in time.
This is because visual acuity is also affected by the status of photoreceptors reflected as status of ellipsoid line and external limiting membrane. Thus, there may also exist a dissociation between BCVA and CRT in eyes with BRVO-ME. In addition, we suggest that the mechanisms related to morphological improvement are not necessarily the same as the mechanisms that affect visual function, as represented by the BCVA and visual prognosis might be limited in glaucoma due to pre-existing visual field defects affecting central vision. So, we need further investigation for multiple cofounders.
Limitations
The main limitations of this study were the small number of patients, its retrospective nature, and the single-center design. As a result, we could not divide and analyze the patients accordingly to the type of BRVO, eg, major BRVO or macular BRVO,26 nor could evaluate the disc morphology and presence of macular ischemia before and after treatment by using fluorescein angiography or OCT angiography, which is an important prognostic factor for the final BCVA6 though CD ratio did not alter during this short time observation. In addition, the importance of arteriovenous (AV) crossing and hyperreflective material have also been reported. In particular, because occlusion occurs most frequently at the AV crossing27 and its variation pattern may have a role in the clinical distribution of BRVO,28 it is important to evaluate the AV crossing pattern. The presence of hyperreflective material in BRVO is associated with poorer vision.29 Prospective studies are needed to determine whether these factors also affect the treatment pattern of BRVO-ME associated with glaucoma.
Second, we used different anti-VEGF agents for the treatment and did not evaluate the differences among the agents. There was a significant difference in the distribution of anti-VEGF agents between the G [-] and G [+] groups, as shown in Table 1. Many patients received bevacizumab in the G [+] group and ranibizumab in the G [-] group. This imbalance may have influenced our results. The LEAVO study compared intravitreal aflibercept or bevacizumab with ranibizumab for eyes with CRVO-related ME, and they reported a noninferior mean change in vision. However, in that study, there were fewer anti-VEGF injections in the aflibercept group than in the ranibizumab group.30 In contrast, a meta-analysis of 18 articles reported no statistically significant differences in any outcomes among bevacizumab, ranibizumab, and aflibercept for treatment of BRVO-ME, although all of these agents were significantly superior to sham injection.31 Considering these discrepancies, further investigations with large number of cases are essential.
Third, we followed patients for only a short term with a single-injection, 1+ PRN (PRN) regimen, although most randomized clinical trial (RCT) protocols involved multiple initial monthly injections. In the BRAVO trial, patients received six monthly ranibizumab injections in the first six months (6+PRN).32 However, several studies have reported that the improvement in visual outcomes and CRT were similar between single injections and three-monthly injections.33–35 Although it is difficult to compare the previous RCT with other studies, including our study, due to the differences in inclusion criteria, these results suggest that the 1+PRN regimen may be a useful protocol for BRVO-ME with fewer injections. However, since our study was a retrospective study, we could not define strict re-injection criteria. For the 1-year follow-up period of our study, re-injection was performed at 3.6 months (median, 3.0 months) for the G [-] group and 4.9 months (median 4.0 months) for the G [+] group with no significance. Because we observed cases that did not require re-injection within 3 months after initial injection, there is a possibility that more frequent injections could clarify the difference between the two groups. Additional examinations are needed to clarify this point.
Fourth, there are possibilities that anti-VEGF injection itself cause acute or longitude IOP rise which affect glaucoma progression.36,37 Here, we did not perform paracentesis and there may occur acute IOP elevation. Though acute IOP elevation continue short time and paracentesis is useful, we need attention for such injection-related IOP elevation.
Fifth, though IOP maintained lower than 20mmHg for G [+] group, 13 eyes among 27 eyes (48.1%) received prostaglandin analogues. There is a possibility that prostaglandin analogues affect ME formation.38 But its incidence was not high (between 1.2% and 5% during latanoprost treatment) and all patients did not cause ME before BRVO onset though they used prostaglandin analogue before onset. We need attention for IOP reduction and side effect of prostaglandin analogue carefully.
Finally, CRT was not evaluated as a sector region. Some reports have shown that RNFL in the superior or inferior quadrant is affected by glaucomatous damage.39,40 Such fundamental differences related to glaucoma severity may affect CRT improvement in BRVO-ME with glaucoma.
Conclusions
In conclusion, we found that anti-VEGF treatment is effective for BRVO-ME, regardless of whether the eye is glaucomatous. However, the therapeutic response of anti-VEGF agents for BRVO-ME is affected by the presence of glaucoma and glaucoma is considered as a negative prognostic factor for BCVA improvement with BRVO-ME.
Abbreviations
BCVA, Best-corrected visual acuity; BRVO, Branch retinal vein occlusion; CRT, Central retinal thickness; IOP, Intraocular pressure; ME, Macular edema; NTG, Normal tension glaucoma; OCT, Optical coherence tomography; PRN, Pro re nata; RCT, Randomized clinical trial; RNFl, Retinal nerve fiber layer; RNFLT, Retinal nerve fiber layer thickness; SD, Standard deviation; VEGF, Vascular endothelial growth factor; VF, Visual field.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The procedures used in this study were approved by the Institutional Ethics Review Board of Mie University Hospital (H2019-065), and the study was registered at http://www.umin.ac.jp (UMIN ID 000037679). This study was conducted in accordance with the World Medical Association Declaration of Helsinki. Informed consent was obtained from all subjects involved in the study using the opt-out approach.
Acknowledgments
We thank Professor Emeritus Duco Hamasaki of the Bascom Palmer Eye Institute of the University of Miami for critical discussions and final manuscript revisions. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Masahiko Sugimoto has the following interests to declare:
[Financial support] Alcon Pharma and Bayer.
[Other (lecture fee)] Alcon Pharma, Kowa Pharma, Senjyu Pharma, Daiichi Yakuhin Sangyo, Bayer, Wakamoto Pharma.
The sponsors had no role in the design, execution, interpretation, or writing of the study. The authors report no conflicts of interest in this work.
References
1. Rogers S, McIntosh RL, Cheung N, et al. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology. 2010;117:
2. Rehak M, Wiedemann P. Retinal vein thrombosis: pathogenesis and management. J Thromb Haemost. 2010;8:1886–1894. doi:10.1111/j.1538-7836.2010.03909.x
3. Yau JWY, Lee P, Wong TY, Best J, Jenkins A. Retinal vein occlusion: an approach to diagnosis, systemic risk factors and management. Intern Med J. 2008;38:904–910. doi:10.1111/j.1445-5994.2008.01720.x
4. Ho JD, Liou SW, Lin HC. Retinal vein occlusion and the risk of stroke development: a five-year follow-up study. Am J Ophthalmol. 2009;147:283–290. doi:10.1016/j.ajo.2008.08.006
5. Yin X, Li J, Zhang B, Lu P. Association of glaucoma with risk of retinal vein occlusion: a meta-analysis. Acta Ophthalmol. 2019;97:652–659. doi:10.1111/aos.14141
6. Pulido JS, Flaxel CJ, Adelman RA, et al. Retinal vein occlusions preferred practice pattern guidelines. Ophthalmology. 2016;123:182–208. doi:10.1016/j.ophtha.2015.10.045
7. Brown DM, Campochiaro PA, Bhisitkul RB, et al. Sustained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a Phase III study. Ophthalmology. 2011;118:1594–1602. doi:10.1016/j.ophtha.2011.02.022
8. Campochiaro PA, Clark WL, Boyer DS, et al. Intravitreal aflibercept for macular edema following branch retinal vein occlusion: the 24-week results of the VIBRANT study. Ophthalmology. 2015;122:538–544. doi:10.1016/j.ophtha.2014.08.031
9. Son Y, Lee S, Park J. Measurement of lamina and prelaminar thicknesses of both eyes in patients with unilateral branch retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol. 2017;255:503–508. doi:10.1007/s00417-016-3491-y
10. Park HYL, Jeon S, Lee MY, Park CK. Glaucoma progression in the unaffected fellow eye of glaucoma patients who developed unilateral branch retinal vein occlusion. Am J Ophthalmol. 2017;175:194–200. doi:10.1016/j.ajo.2016.10.009
11. Mac Donald D. The ABCs of RVO: a review of retinal venous occlusion. Clin Exp Optom. 2014;97:311–323. doi:10.1111/cxo.12120
12. Bonomi L, Marchini G, Marraffa M, et al. Vascular risk factors for primary open angle glaucoma: the Egna-Neumarkt Study. Ophthalmology. 2000;107:1287–1293. doi:10.1016/S0161-6420(00)00138-X
13. Flammer J, Orgul S, Costa VP, et al. The impact of ocular blood flow in glaucoma. Prog Retin Eye Res. 2002;21:359–393. doi:10.1016/s1350-9462(02)00008-3
14. Flammer J, Orgul S. Optic nerve blood-flow abnormalities in glaucoma. Prog Retin Eye Res. 1998;17:267–289. doi:10.1016/S1350-9462(97)00006-2
15. Sung KR, Cho JW, Lee S, et al. Characteristics of visual field progression in medically treated normal-tension glaucoma patients with unstable ocular perfusion pressure. Invest Ophthalmol Vis Sci. 2011;52:737–743. doi:10.1167/iovs.10-5351
16. Wang Q, Chan SY, Yan Y, et al. Optical coherence tomography angiography in retinal vein occlusions. Graefes Arch Clin Exp Ophthalmol. 2018;256:1615–1622. doi:10.1007/s00417-018-4038-1
17. Maltsev DS, Kulikov AN, Kazak AA, Burnasheva MA. Status of choriocapillaris in fellow eyes of patients with unilateral retinal vein occlusions. Ophthalmic Surg Lasers Imaging Retina. 2021;52:23–28. doi:10.3928/23258160-20201223-05
18. Sin BH, Song BJ, Park SP. Aqueous vascular endothelial growth factor and endothelin-1 levels in branch retinal vein occlusion associated with normal tension glaucoma. J Glaucoma. 2013;22:104–109. doi:10.1097/IJG.0b013e3182312047
19. Loesch A. Perivascular nerves and vascular endothelium: recent advances. Histol Histopathol. 2002;17:591–597. doi:10.14670/HH-17.591
20. Kida T, Flammer J, Oku H, et al. Suppressed endothelin-1 by anti-VEGF therapy is important for patients with BRVO-related macular edema to improve their vision. EPMA J. 2016;7:18. doi:10.1186/s13167-016-0066-2
21. Chan EW, Wong TY, Liao J, et al. Branch retinal vein occlusion and optic nerve head topographic parameters: the Singapore Indian eye study. Br J Ophthalmol. 2013;97:611–616. doi:10.1136/bjophthalmol-2012-302280
22. Terashima H, Okamoto F, Hasebe H, Ueda E, Yoshida H, Fukuchi T. Optical coherence tomography angiography and Humphrey field analyser for macular capillary non-perfusion evaluation in branch retinal vein occlusion. Sci Rep. 2021;11(1):4583. doi:10.1038/s41598-021-84240-7
23. Kim CS, Shin KS, Lee HI, Jo YJ, Kim JY. Sectoral retinal nerve fiber layer thinning in branch retinal vein occlusion. Retina. 2014;34:525–530. doi:10.1097/IAE.0b013e3182a2e746
24. Alshareef RA, Barteselli G, You O, et al. In vivo evaluation of retinal ganglion cells degeneration in eyes with branch retinal vein occlusion. Br J Ophthalmol. 2016;100:1506–1510. doi:10.1136/bjophthalmol-2015-308106
25. Diabetic Retinopathy Clinical Research Network. Relationship between optical coherence tomography-measured central retinal thickness and visual acuity in diabetic macular edema. Ophthalmology. 2007;114:525–536.
26. Hayreh SS. Prevalent mis conceptions about acute retinal vascular occlusive disorders. Prog Retin Eye Res. 2005;24:493–519. doi:10.1016/j.preteyeres.2004.12.001
27. Weinberg D, Dodwell DG, Fern SA. Anatomy of arteriovenous crossings in branch retinal vein occlusion. Am J Ophthalmol. 1990;109:298–302. doi:10.1016/S0002-9394(14)74554-4
28. Feist RM, Ticho BH, Shapiro MJ, Farber M. Branch retinal vein occlusion and quadratic variation in arteriovenous crossings. Am J Ophthalmol. 1992;113:664–668. doi:10.1016/S0002-9394(14)74791-9
29. Venkatesh R, Pereira A, Sangai S, Thomas S, Yadav NK. Prognostic value of hyperreflective material on visual acuity in treatment-naïve BRVO. Ophthalmic Surg Lasers Imaging Retina. 2020;51:320–327. doi:10.3928/23258160-20200603-02
30. Hykin P, Prevost AT, Vasconcelos JC, et al. Clinical effectiveness of intravitreal therapy with ranibizumab vs aflibercept vs bevacizumab for macular edema secondary to central retinal vein occlusion: a randomized clinical trial. JAMA Ophthalmol. 2019;137:1256–1264. doi:10.1001/jamaophthalmol.2019.3305
31. Sangroongruangsri S, Ratanapakorn T, Wu O, Anothaisintawee T, Chaikledkaew U. Comparative efficacy of bevacizumab, ranibizumab, and aflibercept for treatment of macular edema secondary to retinal vein occlusion: a systematic review and network meta-analysis. Expert Rev Clin Pharmacol. 2018;11:903–916. doi:10.1080/17512433.2018.1507735
32. Campochiaro PA, Heier JS, Feiner L, et al. Ranibizumab for macular edema following branch retinal vein occlusion: six month primary end point results of a phase III study. Ophthalmology. 2010;117:1102–1112. doi:10.1016/j.ophtha.2010.02.021
33. Ito Y, Saishin Y, Sawada O, et al. Comparison of single injection and three monthly injections of intravitreal bevacizumab for macular edema associated with branch retinal vein occlusion. Clin Ophthalmol. 2015;9:175–180. doi:10.2147/OPTH.S76261
34. Bayat AH, Çakır A, Özturan ŞG, et al. Comparison of one and three initial monthly intravitreal ranibizumab injection in patients with macular edema secondary to branch retinal vein occlusion. Int J Ophthalmol. 2018;11:1534–1538. doi:10.18240/ijo.2018.09.17
35. Chen X, Hu TM, Zuo J, et al. Intravitreal conbercept for branch retinal vein occlusion induced macular edema: one initial injection versus three monthly injections. BMC Ophthalmol. 2020;20:225. doi:10.1186/s12886-020-01494-x
36. Beato J, Pedrosa AC, Pinheiro-Costa J, et al. Long-term effect of anti-VEGF agents on intraocular pressure in age-related macular degeneration. Ophthalmic Res. 2016;56:30–34. doi:10.1159/000444395
37. de Vries VA, Bassil FL, Ramdas WD. The effects of intravitreal injections on intraocular pressure and retinal nerve fiber layer: a systematic review and meta-analysis. Sci Rep. 2020;10:132. doi:10.1038/s41598-020-70269-7
38. Holló G, Aung T, Cantor LB, Aihara M. Cystoid macular edema related to cataract surgery and topical prostaglandin analogs: mechanism, diagnosis, and management. Surv Ophthalmol. 2020;65:496–512. doi:10.1016/j.survophthal.2020.02.004
39. Dichtl A, Jonas JB, Naumann GO. Retinal nerve fiber layer thickness in human eyes. Grafes Arch Clin Exp Ophthalmol. 1999;237:474–479. doi:10.1007/s004170050264
40. Kubota T, Khalil AK, Honda M, et al. Comparative study of retinal nerve fiber layer damage in Japanese patients with normal- and high-tension glaucoma. J Glaucoma. 1999;8(6):363–366. doi:10.1097/00061198-199912000-00004
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.