Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Anti-Diabetic Effect of Telmisartan Through its Partial PPARγ-Agonistic Activity
Authors Ayza MA ![]() , Zewdie KA
, Zewdie KA ![]() , Tesfaye BA
, Tesfaye BA ![]() , Gebrekirstos ST
, Gebrekirstos ST ![]() , Berhe DF
, Berhe DF ![]()
Received 31 May 2020
Accepted for publication 10 September 2020
Published 12 October 2020 Volume 2020:13 Pages 3627—3635
DOI https://doi.org/10.2147/DMSO.S265399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Muluken Altaye Ayza, Kaleab Alemayehu Zewdie, Bekalu Amare Tesfaye, Selamawit Tesfamariam Gebrekirstos, Derbew Fikadu Berhe
Department of Pharmacology and Toxicology, School of Pharmacy, Mekelle University, Mekelle, Ethiopia
Correspondence: Muluken Altaye Ayza Tel +251-916707913 Email [email protected]
Abstract: Telmisartan is an angiotensin II receptor antagonist, which selectively inhibits the angiotensin II type 1 receptor. Thus, it is widely used for hypertension management. Nowadays, telmisartan’s effect on peroxisome proliferator-activated receptors (PPARs) is gaining wider attention. PPARs are ligand-activated transcription factors that belong to the nuclear hormone receptor superfamily. Telmisartan is reported to have a partial PPARγ-agonistic effect while avoiding the safety concerns found with full PPARγ agonists (thiazolidinediones). Telmisartan could be an alternative treatment option, with dual benefit for diabetes mellitus (DM) and hypertension. This review summarizes the anti-diabetic activity of telmisartan via its partial PPARγ-agonistic activity.
Keywords: diabetes mellitus, hypertension, peroxisome proliferator-activated receptors, telmisartan
Introduction
Telmisartan
Telmisartan is a selective angiotensin II type 1 receptor antagonist (angiotensin receptor blocker [ARB]) which does not affect the other receptor systems involved in cardiovascular regulation.1,2 It is a more lipophilic compound than other ARBs, which facilitates oral absorption and benefits tissue and cell penetration.3 The drug is used for the management of hypertension, either as monotherapy or as combination therapy with other antihypertensive agents.1,4 It is considered as a first-line drug in mild-to-moderate hypertension with an excellent safety profile, and is used for the treatment of hypertension-related cardiovascular end-organ damage.5 A number of studies have shown that telmisartan has partial PPARγ-agonist activity, activating 25–30% of the receptor compared to the full PPARγ agonists.6–8
Peroxisome Proliferator-Activated Receptors (PPARs)
PPARs are ligand-activated transcription factors that belong to the nuclear hormone receptor superfamily.9 PPARs comprise three subtypes, namely PPARα, PPARγ, and PPARβ/δ.10
Among the three subtypes, PPARγ is the most studied nuclear receptor and is involved in the control of energy balance, glucose and lipid homeostasis.11 Thiazolidinediones, including rosiglitazone and pioglitazone, are anti-diabetic drugs acting on PPARγ.12 Thiazolidinediones promote insulin sensitization and improve dyslipidemia in diabetic patients.13 It has been reported that PPARγ agonists may have various therapeutic advantages in addition to anti-diabetic activity. Rosiglitazone decreased arterial stiffness and clinical inflammatory responses in diabetic patients with coronary artery disease.14,15 Despite the beneficial effects of thiazolidinediones on the heart, they are also associated with several adverse effects, including cardiac dysfunction and ventricular fibrillation.16,17
Challenges with Full-PPARγ Agonists
Full PPARγ agonists are associated with a number of side effects, including weight gain, fluid retention (edema), and cardiac toxicity.18 The first approved drug from the thiazolidinedione class was troglitazone, which was withdrawn from the market in 2000 owing to its fatal hepatotoxicity.19 This idiosyncratic hepatotoxicity is mediated through oxidative stress and involves mitochondrial dysfunction.20,21 Other thiazolidinediones are also associated with adverse effects, including weight gain (adiposity), increased rate of bone fracture, anemia, and hepatic damage.22
Rosiglitazone is associated with granulomatous hepatitis.23,24 It has also been reported to increase cardiovascular risk.25 Hypertension, myocardial ischemia, heart failure, upper respiratory tract infection, and diarrhea were also reported with rosiglitazone use.26 Owing to its cardiovascular side effects and adverse effects on the lipid profile, rosiglitazone was banned in India in 2010.27
Clinical use of pioglitazone is also limited by undesirable adverse effects, including weight gain, precipitation of heart failure, peripheral edema, and an increase in bone fractures.28,29 Pioglitazone is also reported to induce hepatic damage.30,31 Although the severity depends on the dose administered, subchronic administration of pioglitazone in mice resulted in nephrotoxicity, hepatotoxicity, cardiotoxicity, and hematological disorders, which were supported by biochemical abnormalities and histopathological changes.32 For this reason, new PPARγ ligands with increased therapeutic efficacy and reduced adverse effects are needed. Partial PPARγ modulators are one of the promising classes in this regard.33
Advantages of Partial PPARγ Agonists
PPARγ partial agonists selectively modify the expression of genes needed only for insulin sensitization without activating the genes responsible for weight gain and edema.34 This makes partial PPARγ agonists preferable to full agonists.35 Adverse effects including weight gain and edema may lead to heart failure, and other adverse effects may also be avoided by selective modulation of the PPARγ receptor.36
The partial PPARγ agonist balaglitazone showed fewer untoward effects, including fluid and fat accumulation, compared to the full PPARγ agonist pioglitazone.37 Another selective partial activator of PPARγ (PAR-1622) showed anti-diabetic activity with a broader safety margin against fluid retention in comparison with rosiglitazone.38 PAM-1616 is also a selective modulator of PPARγ with anti-hyperglycemic properties and an improved side effect profile compared to rosiglitazone.39 KR-62980 is a selective PPARγ modulator with anti-diabetic and anti-adipogenic activity with an improved side effect profile.40,41 CMHX008, a partial PPARγ modulator, showed comparable insulin-sensitizing effects with lower adipogenic capacity and lower risk of bone loss compared to rosiglitazone, and it could be an effective agent for the management of DM and other metabolic disorders.42,43 GQ-16 and L312, PPARγ partial agonists, also showed a promising anti-diabetic effect with an improved side effect profile.44,45 There are several partial PPARγ agonists under investigation, with an insulin sensitization action and fewer adverse effects, including a reduced tendency to cause weight gain, adipose tissue gain, and fluid retention.46
PPARγ partial activation may have an important endothelial defensive action through activating eNOS, generating nitric oxide (NO) and enhancing NO bioavailability, reducing oxidative stress, and preventing the adhesion cascade and vascular inflammation.47 Partial PPARγ agonists may offer beneficial effects for the management of type II DM (T2DM) with attenuated adverse effects such as fluid retention and cardiac hypertrophy.34
Patients with hypertension and T2DM may obtain a dual benefit from drugs such as telmisartan with multiple targets (AT1R and PPARγ). That would potentially reduce the pill burden and side effects of multiple medication use, and hence improve medication adherence. This review focuses on the anti-diabetic effects of telmisartan mediated through PPARγ.
Telmisartan for Diabetes Mellitus
Current management of DM is associated with major hurdles, comprising polypharmacy, striving for glycemic targets, patient adherence, and clinical inertia.48 In spite of many anti-diabetic drugs being available, adequate control of diabetic hyperglycemia often remains difficult to achieve.49 In T2DM, intense control of glycemia generally requires the addition of insulin to oral agents, which is consistently accompanied by weight gain. Furthermore, increased hypoglycemia carries a risk of cerebral damage, mental disorders and stroke, cognitive damage, hypertension, and renal disease.50 The adverse effects associated with currently available drugs include GI adverse effects and lactic acidosis with metformin,51,52 weight gain and hypoglycemia with sulfonylureas, and fluid retention and weight gain with thiazolidinediones.53 Since the available agents are associated with various adverse effects, it is important to discover an alternative agent that is more effective and safer to use in the treatment of T2DM.53,54
As telmisartan is reported to have partial PPARγ-agonistic effect, the drug can regulate glucose and lipid metabolism, and improve insulin resistance.55 PPARγ phosphorylation and its downstream gene expression may be regulated by telmisartan, promoting glucose uptake and acting as an insulin-sensitizing agent in adipocytes.56 Telmisartan augments glucose transporter-4 protein expression and 2-deoxyglucose uptake in the basal and insulin-stimulated states of adipocytes.57 It further increases glucose transporter-4 localization to the plasma membrane and enhances glucose uptake through PPARγ in adipocytes. Thus, telmisartan could be an effective therapy for metabolic syndrome.58
Different mechanisms have been postulated for the glucose-lowering potential of telmisartan. It may occur through the suppression of reactive oxygen species and an agonistic effect on PPARγ.59 Telmisartan decreased malondialdehyde and increased glutathione, catalase, and superoxide dismutase levels in STZ-induced type 2 diabetic rats, and prevented cardiovascular complications.60 Furthermore, telmisartan was shown to increase serum adiponectin and improved both oxidative stress and insulin resistance in type 2 diabetic patients.61 Also, in diabetic patients with hypertension, telmisartan increased high-molecular-weight adiponectin levels and improved insulin resistance, through partial PPARγ activation.62 Adiponectin, through binding to its receptors, mediates the insulin-sensitizing effect, which is important in DM patients.63
In addition, interruption of the renin–angiotensin–aldosterone system (RAAS) may improve glycemic control in T2DM, since the RAAS is implicated in the development of T2DM.64 Owing to the ability of telmisartan, partial activation of PPARγ and ARB blockade may have additional importance not merely in the management of metabolic syndrome and prevention of T2DM but also in the prevention and treatment of atherosclerotic cardiovascular disease.65
Telmisartan improves insulin sensitivity in hypertensive patients with insulin resistance or T2DM.66 Telmisartan treatment of hypertensive patients with T2DM not only improved blood pressure, glucose and lipid metabolism, but also improved endothelial function for the prevention of atherosclerosis.67 Through activating PPARγ, telmisartan reduces cardiac fibrosis and hypertrophy, thus preventing unfavorable cardiac remodeling.7 In addition to PPARγ activation, telmisartan improves hyperglycemia-induced cardiac fibrosis through PPARδ activation.68,69 Telmisartan may be important in preventing diabetic cardiomyopathy and it could be used to treat both hemodynamic and metabolic aberrations.70,71 These cardioprotective effects of telmisartan may be due to improvement of endothelial function, which is associated with PPARγ-eNOS, oxidative stress, and the Rho-kinase pathway.72 Targeting both angiotensin type 1 receptor and PPARγ may be important in treating hyperlipidemia, insulin resistance, hypertension, and stroke, and ultimately mitigating the burden of cerebrovascular and cardiovascular disease.73
Patients with uncomplicated hypertension and mild dyslipidemia can be effectively treated with telmisartan.74 Both animal and human studies showed improvements in the lipid profile with telmisartan treatment. In high-fat diet-induced dyslipidemic guinea pigs, telmisartan markedly decreased triglyceride and slightly increased high-density lipoprotein cholesterol levels.75 In a prospective open-label study, telmisartan significantly increased high-density lipoprotein and decreased triglyceride and total cholesterol in hypertensive patients with dyslipidemia.76 Telmisartan may have hepatic partial PPARα agonist activity and it increases lipoprotein lipase expression via a PPARα-dependent pathway, which could explain telmisartan’s anti-dyslipidemic actions.77,78
Telmisartan has the additional benefit of renoprotection in patients diagnosed with diabetes and hypertension. In a randomized, multicenter, double-blind, placebo-controlled trial, telmisartan reduced the transition from incipient to overt nephropathy and induced remission of albuminuria in Japanese patients with T2DM; telmisartan achieved superior renoprotection.79 In addition, in a multicenter, prospective, double-blind, forced-titration, randomized study, telmisartan and ramipril both increased nitric oxide activity of the renal endothelium significantly, which in turn may support the preservation of cardiovascular and renal function in patients with T2DM.80
A number of preclinical and clinical studies have shown a decrease in blood glucose and improvement in diabetic complications after treatment with telmisartan (Table 1).
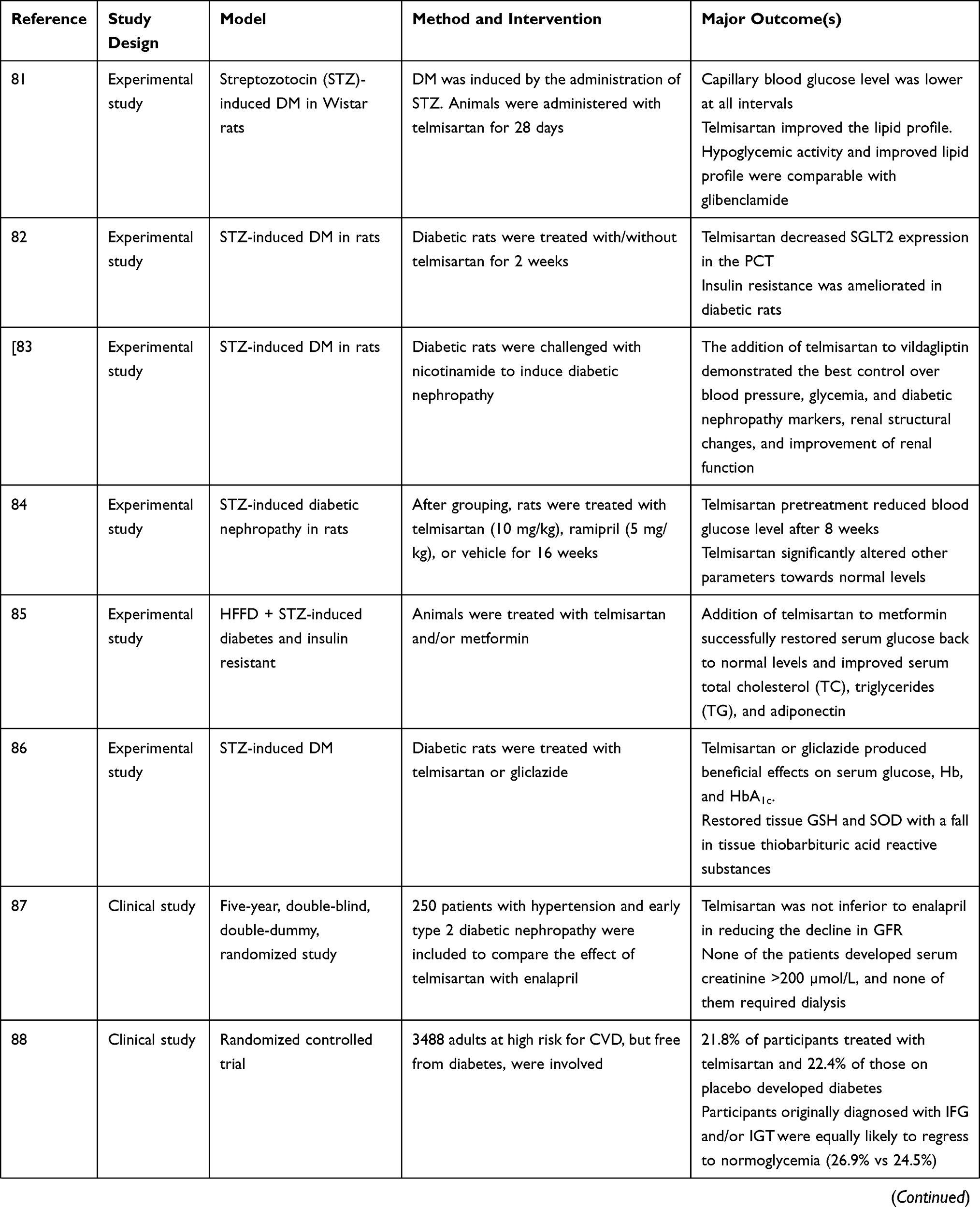 | 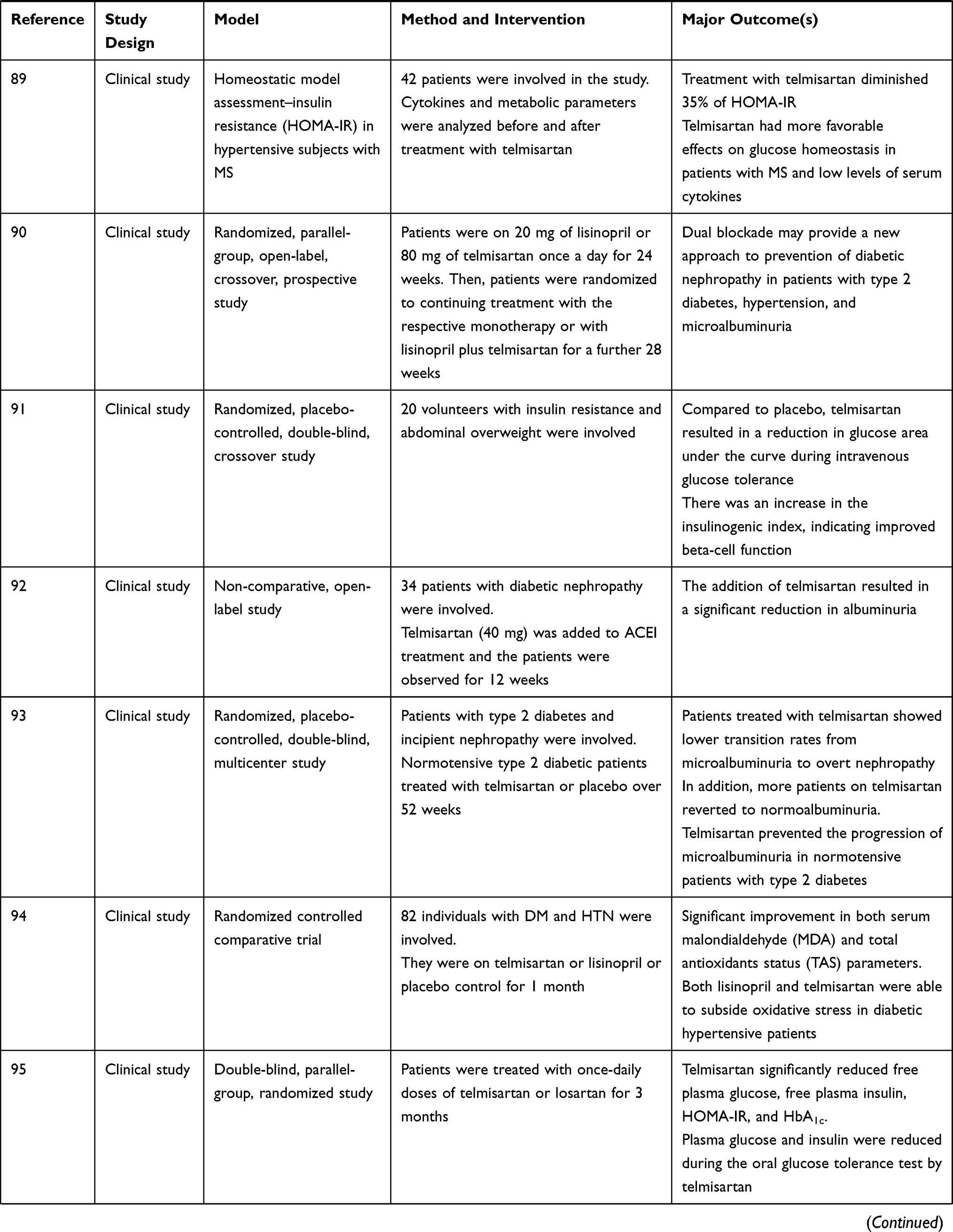 | 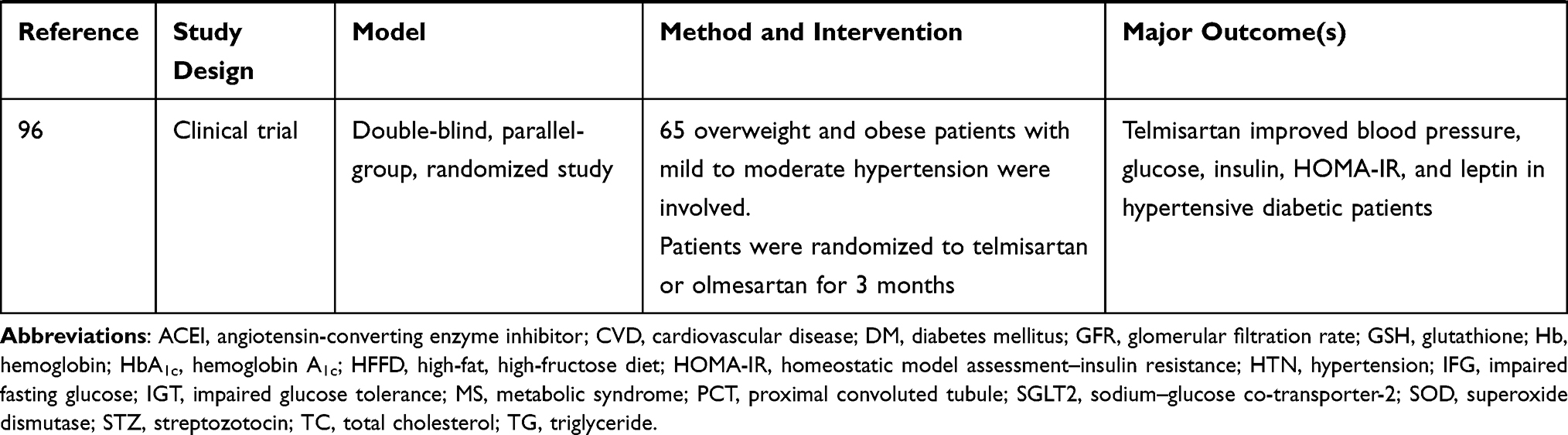 |
Table 1 Effects of Telmisartan in Diabetes Mellitus and Associated Complications |
Conclusion
Telmisartan is a well-known anti-hypertensive drug, which is currently in clinical use. The partial PPARγ-agonistic activity and angiotensin receptor blockade activity of telmisartan have been shown to have multiple clinical benefits, including anti-diabetic and cardiovascular effects. In addition, telmisartan is reported to have PPARα and PPARδ agonist activity. Telmisartan would be an ideal alternative dual-purpose medication for patients with T2DM, hypertension and other cardiovascular disorders. However, this requires further detailed understanding of the therapeutic efficacy and molecular mechanism of telmisartan and other partial PPARγ-agonist drugs.
Abbreviations
ARB, angiotensin receptor blocker; DM, diabetes mellitus; GC, glibenclamide; GSH, glutathione; HbA1c, hemoglobin A1c; HOMA-IR, homeostatic model assessment–insulin resistance; MDA, malondialdehyde; PCT, proximal convoluted tubule; RAAS, renin–angiotensin–aldosterone system; SOD, superoxide dismutase; STZ, streptozotocin; T2DM, type 2 diabetes mellitus; TAS, total antioxidant status.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wienen W, Entzeroth M, van Meel JC, et al. A review on telmisartan: a novel, long‐acting angiotensin II‐receptor antagonist. Cardiovasc Drug Rev. 2000;18(2):127–154. doi:10.1111/j.1527-3466.2000.tb00039.x
2. Sharpe M, Jarvis B, Goa KL. Telmisartan. Drugs. 2001;61(10):1501–1529. doi:10.2165/00003495-200161100-00009
3. Galzerano D, Capogrosso C, Di Michele S, et al. New standards in hypertension and cardiovascular risk management: focus on telmisartan. Vasc Health Risk Manag. 2010;6:113–133. doi:10.2147/VHRM.S7857
4. Battershill AJ, Scott LJ. Telmisartan. Drugs. 2006;66(1):51–83. doi:10.2165/00003495-200666010-00004
5. Borém LMA, Neto JFR, Brandi IV, Lelis DF, Santos SHS. The role of the angiotensin II type I receptor blocker telmisartan in the treatment of non-alcoholic fatty liver disease: a brief review. Hypertens Res. 2018;41(6):394–405. doi:10.1038/s41440-018-0040-6
6. Haraguchi T, Iwasaki K, Takasaki K, et al. Telmisartan, a partial agonist of peroxisome proliferator-activated receptor γ, improves impairment of spatial memory and hippocampal apoptosis in rats treated with repeated cerebral ischemia. Brain Res. 2010;1353:125–132. doi:10.1016/j.brainres.2010.07.017
7. Maejima Y, Okada H, Haraguchi G, et al. Telmisartan, a unique ARB, improves left ventricular remodeling of infarcted heart by activating PPAR gamma. Lab Invest. 2011;91(6):932–944. doi:10.1038/labinvest.2011.45
8. Amano Y, Yamaguchi T, Ohno K, et al. Structural basis for telmisartan-mediated partial activation of PPAR gamma. Hypertens Res. 2012;35(7):715–719. doi:10.1038/hr.2012.17
9. Rakhshandehroo M, Knoch B, Müller M, Kersten S. Peroxisome proliferator-activated receptor alpha target genes. PPAR Res. 2010;2010:612089. doi:10.1155/2010/612089
10. Tyagi S, Gupta P, Saini AS, Kaushal C, Sharma S. The peroxisome proliferator-activated receptor: A family of nuclear receptors role in various diseases. J Adv Pharm Technol Res. 2011;2(4):236. doi:10.4103/2231-4040.90879
11. Zieleniak A, Wójcik M, Woźniak LA. Structure and physiological functions of the human peroxisome proliferator-activated receptor γ. Arch Immunol Ther Exp. 2008;56(5):331. doi:10.1007/s00005-008-0037-y
12. Duan SZ, Usher MG, Mortensen RM. Peroxisome proliferator-activated receptor-gamma-mediated effects in the vasculature. Circ Res. 2008;102(3):283–294. doi:10.1161/CIRCRESAHA.107.164384
13. Fogo AB. Potential for peroxisome proliferator-activated receptor-gamma agonists in progression: beyond metabolism. Curr Opin Nephrol Hypertens. 2008;17(3):282–285. doi:10.1097/MNH.0b013e3282f9b1c0
14. Wang G, Wei J, Guan Y, Jin N, Mao J, Wang X. Peroxisome proliferator-activated receptor-gamma agonist rosiglitazone reduces clinical inflammatory responses in type 2 diabetes with coronary artery disease after coronary angioplasty. Metabolism. 2005;54(5):590–597. doi:10.1016/j.metabol.2004.11.017
15. Yu J, Jin N, Wang G, Zhang F, Mao J, Wang X. Peroxisome proliferator-activated receptor gamma agonist improves arterial stiffness in patients with type 2 diabetes mellitus and coronary artery disease. Metabolism. 2007;56(10):1396–1401. doi:10.1016/j.metabol.2007.05.011
16. Psaty BM, Furberg CD. Rosiglitazone and cardiovascular risk. Mass Med Soc. 2007.
17. Palee S, Weerateerangkul P, Chinda K, Chattipakorn SC, Chattipakorn N. Mechanisms responsible for beneficial and adverse effects of rosiglitazone in a rat model of acute cardiac ischaemia-reperfusion. Exp Physiol. 2013;98(5):1028–1037. doi:10.1113/expphysiol.2012.070433
18. Liberato MV, Nascimento AS, Ayers SD, et al. Medium chain fatty acids are selective peroxisome proliferator activated receptor (PPAR) γ activators and pan-PPAR partial agonists. PLoS One. 2012;7(5):e36297–e. doi:10.1371/journal.pone.0036297
19. Wang L, Waltenberger B, Pferschy-Wenzig E-M, et al. Natural product agonists of peroxisome proliferator-activated receptor gamma (PPARγ): a review. Biochem Pharmacol. 2014;92(1):73–89. doi:10.1016/j.bcp.2014.07.018
20. Julie NL, Julie IM, Kende AI, Wilson GL. Mitochondrial dysfunction and delayed hepatotoxicity: another lesson from troglitazone. Diabetologia. 2008;51(11):2108–2116.
21. Yokoi T. Troglitazone. In: Uetrecht J, editor. Adverse Drug Reactions. Berlin: Springer; 2010:419–435.
22. Bhalla K, Hwang BJ, Choi JH, et al. N-Acetylfarnesylcysteine is a novel class of peroxisome proliferator-activated receptor γ ligand with partial and full agonist activity in vitro and in vivo. J Biol Chem. 2011;286(48):41626–41635. doi:10.1074/jbc.M111.257915
23. Dhawan M, Agrawal R, Ravi J, et al. Rosiglitazone-induced granulomatous hepatitis. J Clin Gastroenterol. 2002;34(5):582–584. doi:10.1097/00004836-200205000-00021
24. Bonkovsky HL, Azar R, Bird S, Szabo G, Banner B. Severe cholestatic hepatitis caused by thiazolidinediones: risks associated with substituting rosiglitazone for troglitazone. Dig Dis Sci. 2002;47(7):1632–1637. doi:10.1023/A:1015895925374
25. Wallach JD, Wang K, Zhang AD, et al. Updating insights into rosiglitazone and cardiovascular risk through shared data: individual patient and summary level meta-analyses. BMJ. 2020;368:l7078. doi:10.1136/bmj.l7078
26. Rodriguez BSQ, Correa R. Rosiglitazone. StatPearls [Internet]. StatPearls Publishing; 2019.
27. Chinnam P, Mohsin M, Shafee LM. Evaluation of acute toxicity of pioglitazone in mice. Toxicol Int. 2012;19(3):250–254. doi:10.4103/0971-6580.103660
28. Shah P, Mudaliar S. Pioglitazone: side effect and safety profile. Expert Opin Drug Saf. 2010;9(2):347–354. doi:10.1517/14740331003623218
29. Zou C, Hu H. Use of pioglitazone in the treatment of diabetes: effect on cardiovascular risk. Vasc Health Risk Manag. 2013;9:429.
30. Belcher G, Matthews D. Safety and tolerability of pioglitazone. Exp Clin Endocrinol Diabetes. 2000;108(Sup.2):267–273. doi:10.1055/s-2000-8529
31. Nagasaka S, Abe T, Kawakami A, et al. Pioglitazone-induced hepatic injury in a patient previously receiving troglitazone with success. Diabet Med. 2002;19(4):347–348. doi:10.1046/j.1464-5491.2002.00712_4.x
32. Elshama SS, El-Kenawy AE-M, Osman H-EH. Toxicological evaluation of subchronic use of pioglitazone in mice. Iran J Basic Med Sci. 2016;19(7):712–719.
33. Guasch L, Sala E, Castell-Auví A, et al. Identification of PPARgamma partial agonists of natural origin (I): development of a virtual screening procedure and in vitro validation. PLoS One. 2012;7(11):e50816. doi:10.1371/journal.pone.0050816
34. Chang CH, McNamara LA, Wu MS, et al. A novel selective peroxisome proliferator-activator receptor-γ modulator—SPPARγM5 improves insulin sensitivity with diminished adverse cardiovascular effects. Eur J Pharmacol. 2008;584(1):192–201. doi:10.1016/j.ejphar.2007.12.036
35. Agrawal R, Jain P, N Dikshit S. Balaglitazone: a second generation peroxisome proliferator-activated receptor (PPAR) gamma (γ) agonist. Mini Rev Med Chem. 2012;12(2):87–97. doi:10.2174/138955712798995048
36. Burgermeister E, Schnoebelen A, Flament A, et al. A novel partial agonist of peroxisome proliferator-activated receptor-γ (PPARγ) Recruits PPARγ-Coactivator-1α, prevents triglyceride accumulation, and potentiates insulin signaling in vitro. Mol Endocrinol. 2006;20(4):809–830. doi:10.1210/me.2005-0171
37. Henriksen K, Byrjalsen I, Qvist P, et al. Efficacy and safety of the PPARgamma partial agonist balaglitazone compared with pioglitazone and placebo: a Phase III, randomized, parallel-group study in patients with type 2 diabetes on stable insulin therapy. Diabetes Metab Res Rev. 2011;27(4):392–401. doi:10.1002/dmrr.1187
38. Kim MK, Chae YN, Kim HS, et al. PAR-1622 is a selective peroxisome proliferator-activated receptor γ partial activator with preserved antidiabetic efficacy and broader safety profile for fluid retention. Arch Pharm Res. 2009;32(5):721–727. doi:10.1007/s12272-009-1511-8
39. Kim MK, Chae YN, Choi SH, et al. PAM-1616, a selective peroxisome proliferator-activated receptor γ modulator with preserved anti-diabetic efficacy and reduced adverse effects. Eur J Pharmacol. 2011;650(2–3):673–681. doi:10.1016/j.ejphar.2010.10.044
40. Kim KR, Lee JH, Kim SJ, et al. KR-62980: a novel peroxisome proliferator-activated receptor gamma agonist with weak adipogenic effects. Biochem Pharmacol. 2006;72(4):446–454. doi:10.1016/j.bcp.2006.05.005
41. Jung H, Lee MS, Jang EJ, et al. Augmentation of PPARgamma-TAZ interaction contributes to the anti-adipogenic activity of KR62980. Biochem Pharmacol. 2009;78(10):1323–1329. doi:10.1016/j.bcp.2009.07.001
42. Ming Y, Hu X, Song Y, et al. CMHX008, a novel peroxisome proliferator-activated receptor γ partial agonist, enhances insulin sensitivity in vitro and in vivo. PLoS One. 2014;9(7):e102102–e. doi:10.1371/journal.pone.0102102
43. Hou Y, Cao X, Hu X, et al. CMHX008, a PPARγ partial agonist, enhances insulin sensitivity with minor influences on bone loss. Genes Dis. 2018;5(3):290–299. doi:10.1016/j.gendis.2018.05.004
44. Amato AA, Rajagopalan S, Lin JZ, et al. GQ-16, a novel peroxisome proliferator-activated receptor γ (PPARγ) ligand, promotes insulin sensitization without weight gain. J Biol Chem. 2012;287(33):28169–28179. doi:10.1074/jbc.M111.332106
45. Xie X, Zhou X, Chen W, et al. L312, a novel PPARγ ligand with potent anti-diabetic activity by selective regulation. BBA - Gen Subjects. 2015;1850(1):62–72. doi:10.1016/j.bbagen.2014.09.027
46. Chigurupati S, Dhanaraj SA, Balakumar P. A step ahead of PPARγ full agonists to PPARγ partial agonists: therapeutic perspectives in the management of diabetic insulin resistance. Eur J Pharmacol. 2015;755:50–57. doi:10.1016/j.ejphar.2015.02.043
47. Balakumar P, Kathuria S. Submaximal PPARγ activation and endothelial dysfunction: new perspectives for the management of cardiovascular disorders. Br J Pharmacol. 2012;166(7):1981–1992.
48. Khan NM, Ahmad A, Tiwari K, A Kamal M, Mushtaq G, M Ashraf G. Current challenges to overcome in the management of type 2 diabetes mellitus and associated neurological disorders. CNS Neurol Disord Drug Targets. 2014;13(8):1440–1457.
49. Opie L. Sodium glucose co-transporter 2 (SGLT2) inhibitors: new among antidiabetic drugs. Cardiovasc Drugs Ther. 2014;28(4):331–334. doi:10.1007/s10557-014-6522-0
50. Opie LH, Yellon DM, Gersh BJ. Controversies in the cardiovascular management of type 2 diabetes. Heart. 2011;97(1):6–14. doi:10.1136/hrt.2010.214031
51. Shurrab NT, Arafa E-SA. Metformin: A review of its therapeutic efficacy and adverse effects. Obes Med. 2020;17:100186. doi:10.1016/j.obmed.2020.100186
52. Alam F, Islam MA, Kamal MA, Gan SH. Updates on managing type 2 diabetes mellitus with natural products: towards antidiabetic drug development. Curr Med Chem. 2018;25(39):5395–5431. doi:10.2174/0929867323666160813222436
53. Bonora E. Antidiabetic medications in overweight/obese patients with type 2 diabetes: drawbacks of current drugs and potential advantages of incretin‐based treatment on body weight. Int J Clin Pract. 2007;61:19–28. doi:10.1111/j.1742-1241.2007.01441.x
54. Chakraborti CK. Exenatide: a new promising antidiabetic agent. Indian J Pharm Sci. 2010;72(1):1–11. doi:10.4103/0250-474X.62228
55. Wang J, Pang T, Hafko R, Benicky J, Sanchez-Lemus E, Saavedra JM. Telmisartan ameliorates glutamate-induced neurotoxicity: roles of AT1 receptor blockade and PPARγ activation. Neuropharmacology. 2014;79:249–261. doi:10.1016/j.neuropharm.2013.11.022
56. Fang T, Di Y, Li G, et al. Effects of telmisartan on TNFalpha induced PPARgamma phosphorylation and insulin resistance in adipocytes. Biochem Biophys Res Commun. 2018;503(4):3044–3049. doi:10.1016/j.bbrc.2018.08.091
57. Fujimoto M, Masuzaki H, Tanaka T, et al. An angiotensin II AT1 receptor antagonist, telmisartan augments glucose uptake and GLUT4 protein expression in 3T3-L1 adipocytes. FEBS Lett. 2004;576(3):492–497. doi:10.1016/j.febslet.2004.09.027
58. Furukawa H, Mawatari K, Koyama K, et al. Telmisartan increases localization of glucose transporter 4 to the plasma membrane and increases glucose uptake via peroxisome proliferator-activated receptor gamma in 3T3-L1 adipocytes. Eur J Pharmacol. 2011;660(2–3):485–491. doi:10.1016/j.ejphar.2011.04.008
59. Zhao S, Chan LKY, Chen L, Cheng TW, Klein T, Leung PS. Combination of telmisartan and linagliptin preserves pancreatic islet cell function and morphology in db/db mice. Pancreas. 2016;45(4):584–592. doi:10.1097/MPA.0000000000000505
60. Goyal BR, Parmar K, Goyal RK, Mehta AA. Beneficial role of telmisartan on cardiovascular complications associated with STZ-induced type 2 diabetes in rats. Pharmacol Rep. 2011;63(4):956–966. doi:10.1016/S1734-1140(11)70611-9
61. Watanabe M, Inukai K, Sumita T, et al. Effects of telmisartan on insulin resistance in Japanese type 2 diabetic patients. Internal Med. 2010;49(17):1843–1847. doi:10.2169/internalmedicine.49.3189
62. Mori H, Okada Y, Arao T, Nishida K, Tanaka Y. Telmisartan at 80 mg/Day Increases High-Molecular-Weight Adiponectin Levels and Improves Insulin Resistance in Diabetic Patients. Adv Ther. 2012;29(7):635–644. doi:10.1007/s12325-012-0032-x
63. Yadav A, Kataria MA, Saini V, Yadav A. Role of leptin and adiponectin in insulin resistance. Clin Chim Acta. 2013;417:80–84. doi:10.1016/j.cca.2012.12.007
64. Khan A, Khan BT, Qayyum A. Comparative study of telmisartan with pioglitazone on insulin resistance in type 2 diabetic mice. Pak Armed Forces Med J. 2017;67(1):31–36.
65. Kurtz TW. New treatment strategies for patients with hypertension and insulin resistance. Am J Med. 2006;119(5 Suppl 1):011. doi:10.1016/j.amjmed.2006.01.011
66. Suksomboon N, Poolsup N, Prasit T. Systematic review of the effect of telmisartan on insulin sensitivity in hypertensive patients with insulin resistance or diabetes. J Clin Pharm Ther. 2012;37(3):319–327. doi:10.1111/j.1365-2710.2011.01295.x
67. Wago T, Yoshimoto T, Akaza I, et al. Improvement of endothelial function in patients with hypertension and type 2 diabetes after treatment with telmisartan. Hypertens Res. 2010;33(8):796–801. doi:10.1038/hr.2010.107
68. Chang W-T, Cheng J-T, Chen Z-C. Telmisartan improves cardiac fibrosis in diabetes through peroxisome proliferator activated receptor δ (PPARδ): from bedside to bench. Cardiovasc Diabetol. 2016;15(1):113. doi:10.1186/s12933-016-0430-5
69. Mikami D, Kimura H, Kamiyama K, et al. Telmisartan activates endogenous peroxisome proliferator-activated receptor-δ and may have anti-fibrotic effects in human mesangial cells. Hypertens Res. 2014;37(5):422–431. doi:10.1038/hr.2013.157
70. Tuck ML. Angiotensin-receptor blocking agents and the peroxisome proliferator-activated receptor-gamma system. Curr Hypertens Rep. 2005;7(4):240–243. doi:10.1007/s11906-005-0019-y
71. Malek V, Gaikwad AB. Telmisartan and thiorphan combination treatment attenuates fibrosis and apoptosis in preventing diabetic cardiomyopathy. Cardiovasc Res. 2019;115(2):373–384. doi:10.1093/cvr/cvy226
72. Kobayashi N, Ohno T, Yoshida K, et al. Cardioprotective mechanism of telmisartan via PPAR-gamma-eNOS pathway in dahl salt-sensitive hypertensive rats. Am J Hypertens. 2008;21(5):576–581. doi:10.1038/ajh.2008.27
73. Towfighi A, Ovbiagele B. Partial peroxisome proliferator-activated receptor agonist angiotensin receptor blockers. Cerebrovasc Dis. 2008;26(2):106–112. doi:10.1159/000139656
74. Vanitha M, Vijayal R. Effect of telmisartan on serum lipid profile in patients with hypertension and dyslipidemia. Int J Med Res Health Sci. 2013;2(4):745–749. doi:10.5958/j.2319-5886.2.4.119
75. Xu C, Fang D, Chen X, et al. Effect of telmisartan on the therapeutic efficacy of pitavastatin in high-fat diet induced dyslipidemic guinea pigs. Eur J Pharmacol. 2015;762:364–371. doi:10.1016/j.ejphar.2015.06.005
76. Jayapriya B, Thamilarasi S, Shanthi M, Jafrin AL. Effect of telmisartan on blood pressure and lipid profile in hypertensive patients with dyslipidemia. Int J Pharm Life Sci. 2013;4(10).
77. Clemenz M, Frost N, Schupp M, et al. Liver-specific peroxisome proliferator–activated receptor α target gene regulation by the angiotensin type 1 receptor blocker telmisartan. Diabetes. 2008;57(5):1405–1413. doi:10.2337/db07-0839
78. Yin SN, Liu M, Jing DQ, Mu YM, Lu JM, Pan CY. Telmisartan increases lipoprotein lipase expression via peroxisome proliferator-activated receptor-alpha in HepG2 cells. Endocr Res. 2014;39(2):67–73. doi:10.3109/07435800.2013.828741
79. Makino H, Haneda M, Babazono T, et al. Prevention of transition from incipient to overt nephropathy with telmisartan in patients with type 2 diabetes. Diabetes Care. 2007;30(6):1577–1578. doi:10.2337/dc06-1998
80. Schmieder RE, Delles C, Mimran A, Fauvel JP, Ruilope LM. Impact of telmisartan versus ramipril on renal endothelial function in patients with hypertension and type 2 diabetes. Diabetes Care. 2007;30(6):1351–1356. doi:10.2337/dc06-1551
81. Amoghimath S, Suresha R. Effect of telmisartan on blood glucose levels and blood lipid levels in streptozotocin induced diabetic rats. Biomed Pharmacol J. 2019;12(3):1303–1308. doi:10.13005/bpj/1758
82. Tojo A, Hatakeyama S, Kinugasa S, Nangaku M. Angiotensin receptor blocker telmisartan suppresses renal gluconeogenesis during starvation. Diabetes Metab Syndr Obes. 2015;8:103–113. doi:10.2147/DMSO.S78771
83. Sharma AK, Kanawat DS, Mishra A, et al. Dual therapy of vildagliptin and telmisartan on diabetic nephropathy in experimentally induced type 2 diabetes mellitus rats. J Renin-Angio-Aldo S. 2014;15(4):410–418.
84. Senapaty S, Rath B. Biochemical effects of telmisartan versus ramipril in experimental diabetic nephropathy. Int J Health Sci Res. 2015;5(5):195–202.
85. Salama RM, Schaalan MF, Ibrahim ME, Khalifa AE, Elkoussi AA. Effectiveness of telmisartan as an adjunct to metformin in treating type II diabetes mellitus in rats. Open J Endocr Metab Dis. 2013;3:186–196. doi:10.4236/ojemd.2013.33026
86. Hamed AA, Malek HA. Effect of telmisartan in experimentally induced diabetetes mellitus in rats. Int J Health Sci. 2007;1(2):249.
87. Barnett A. Preventing renal complications in type 2 diabetes: results of the diabetics exposed to telmisartan and enalapril trial. J Am Soc Nephrol. 2006;17(4 suppl 2):S132–S5. doi:10.1681/ASN.2005121326
88. Barzilay JI, Gao P, Rydén L, et al. Effects of telmisartan on glucose levels in people at high risk for cardiovascular disease but free from diabetes: the TRANSCEND study. Diabetes Care. 2011;34(9):1902–1907. doi:10.2337/dc11-0545
89. Muñoz-Torrero JFS, Rivas MD, Costo A, et al. Telmisartan improves insulin resistance in patients with low cytokine levels. J Investig Med. 2011;59(3):602–605. doi:10.2310/JIM.0b013e31820bf26b
90. Sengul AM, Altuntas Y, Kürklü A, Aydın L. Beneficial effect of lisinopril plus telmisartan in patients with type 2 diabetes, microalbuminuria and hypertension. Diabetes Res Clin Pract. 2006;71(2):210–219. doi:10.1016/j.diabres.2005.06.010
91. Nagel JM, Tietz AB, Göke B, Parhofer KG. The effect of telmisartan on glucose and lipid metabolism in nondiabetic, insulin-resistant subjects. Metabolism. 2006;55(9):1149–1154. doi:10.1016/j.metabol.2006.04.011
92. Mazerska M, Myśliwiec M. Telmisartan lowers albuminuria in type 2 diabetic patients treated with angiotensin enzyme inhibitors. Adv Med Sci. 2009;54(1). doi:10.2478/v10039-009-0015-6
93. Makino H, Haneda M, Babazono T, et al. Microalbuminuria reduction with telmisartan in normotensive and hypertensive Japanese patients with type 2 diabetes: a post-hoc analysis of The Incipient to Overt: angiotensin II Blocker, Telmisartan, Investigation on Type 2 Diabetic Nephropathy (INNOVATION) study. Hypertens Res. 2008;31(4):657–664.
94. Al-Hammami FA, Hasan OA. Comparative study of lisinopril versus telmisartan effects on oxidative stress in diabetic type 2 hypertensive patients. Raf J Sci. 2012;23(2E):34–41.
95. Vitale C, Mercuro G, Castiglioni C, et al. Metabolic effect of telmisartan and losartan in hypertensive patients with metabolic syndrome. Cardiovasc Diabetol. 2005;4(1):6. doi:10.1186/1475-2840-4-6
96. De Luis D, Conde R, González-Sagrado M, et al. Effects of telmisartan vs olmesartan on metabolic parameters, insulin resistance and adipocytokines in hypertensive obese patients. Nutr Hosp. 2010;25(2):275–279.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.