Back to Journals » Advances in Medical Education and Practice » Volume 17
Anesthesiology Residents’ Eliciting of Patient Questions During Informed Consent with a Patient in Pain
Authors Blanch-Hartigan D ![]() , Meyer EC, Ruben MA, Henig A, Jeong S, Waisel DB, Blum RH
, Meyer EC, Ruben MA, Henig A, Jeong S, Waisel DB, Blum RH ![]()
Received 31 January 2026
Accepted for publication 2 May 2026
Published 11 June 2026 Volume 2026:17 595845
DOI https://doi.org/10.2147/AMEP.S595845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Danielle Blanch-Hartigan,1 Elaine C Meyer,2 Mollie A Ruben,3 Ariel Henig,4 Sunny Jeong,5 David B Waisel,6 Richard H Blum7
1Department of Natural and Applied Sciences, Bentley University, Waltham, MA, USA; 2Department of Psychiatry and Behavioral Sciences, Boston Children’s Hospital and Center for Bioethics, Harvard Medical School, Boston, MA, USA; 3Department of Psychology, University of Rhode Island, Kingston, RI, USA; 4Department of Medicine, Mount Sinai Morningside/West Hospitals, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 5Medical School, University of Western Australia, Nedlands, WA, Australia; 6Private Practice, Waisel Anesthesiology, New Haven, CT, USA; 7Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children’s Hospital, Boston, MA, USA
Correspondence: Danielle Blanch-Hartigan, Department of Natural and Applied Sciences, Bentley University, 175 Forest Street, Waltham, MA, 02452, USA, Tel +17818912066, Email [email protected]
Purpose: Informed consent is a cornerstone of ethical practice. Eliciting patient questions during informed consent increases patient engagement and understanding, thus enhancing integrity of the consent process. However, a patient in visible pain can add an additional challenge to the informed consent process. The purpose of this research was to examine if and how anesthesiology residents ask for questions from a patient displaying severe pain during an informed consent simulation.
Methods: Anesthesiology residents recruited from three anesthesia residency programs were video recorded performing an informed consent with a 52-year-old White male simulated patient awaiting urgent repair of a perforated gastric ulcer who was displaying verbal and nonverbal signs of pain. Two independent coders evaluated whether, when and how residents elicited patient questions during the informed consent process.
Results: Among a sample of 65 first- and third-year anesthesiology residents, more than 20% of residents did not elicit questions during the informed consent encounter. Those who elicited questions typically did so late in the process, with approximately 10% inviting questions only after the consent form had been signed. Most questions were closed-ended (yes/no questions). Although residents did not typically incorporate the patient’s name when eliciting questions, most residents demonstrated eye contact. There were no differences in the number or characteristics of questions elicited based on resident gender or level of training.
Conclusion: Our findings suggest there is a need for increased education regarding the purpose and approach to eliciting patient questions during the informed consent process, especially for patients who are experiencing pain.
Plain Language Summary: When a patient is about to have surgery, they talk with their doctor about what to expect. Then they must agree to have the surgery and agree to the anesthesia needed for the surgery. This is known as the informed consent process. Patients who are about to have surgery may have a lot of questions for their doctor. It is important for the doctor to ask the patient if they have any questions. This study looked at videos of a training session for anesthesiology residents, who are doctors in advanced training to give anesthesia. In this training session, the anesthesiology residents were asked to get informed consent from a patient. The patient was an actor pretending to be in a lot of pain. This study looked at whether the anesthesiology resident ever asked the patient if he had any questions. Our results show that sometimes the doctors did not ask if the patient had questions. Sometimes the doctors ask after the consent form has been signed. We need to train anesthesiology residents to always ask if the patient has questions before the patient agrees to the surgery and the anesthesia.
Keywords: anesthesiology, doctor-patient interaction, informed consent, pain, resident education, simulation
Introduction
Informed consent is a widely accepted legal, ethical and regulatory requirement for clinical and research encounters.1 Informed consent is rooted in the bioethical principle of respect for autonomy whereby patients provide consent freely, intentionally, and with accurate understanding. Historically, informed consent meant a physician’s obligation to disclose information, however, the focus has shifted to embrace the patient’s understanding and experience.2
The importance and value of eliciting patients’ questions have long been established as an essential component of the clinician’s skill set. Eliciting questions in this context refers to the clinician asking or probing whether the patient has any questions if the patient has not asked any questions or solicits additional questions. For anesthesiologists, eliciting questions promotes patient comprehension, confirms understanding, and upholds integrity of informed consent.3 The American Board of Anesthesiology (ABA) considers eliciting questions during informed consent of sufficient importance to include in the Objective Structure Clinical Exam required to achieve Diplomate status (https://www.theaba.org/pdfs/OSCE_Content_Outline.pdf). Obtaining informed consent is a central responsibility of anesthesiologists; yet anesthesiology residents report inadequate preparation to address ethical, practical, and relational challenges.4 Learning to conduct informed consent is often happenstance, occurring through observation and imitation of senior practitioners.
Patients afforded opportunities to ask questions are more likely to receive beneficial information which can positively influence health outcomes.5 Patients report wanting more information,6 but not having adequate opportunities to ask questions.7 Given the inherent hierarchy, patients may not feel empowered to initiate questions, and may seek verbal and nonverbal signals that question-asking is appropriate and welcomed.8
Patients actively experiencing pain during the informed consent process provides an additional challenge. Pain makes it harder for patients to process information and make decisions.9 Both patients and clinicians may want to accelerate the informed consent process to focus instead on intervening for the pain. Anesthesiologists who are discussing informed consent with a patient in pain often wait until after the informed consent is completed to address the patient’s pain.3 While studies have explored patient questions during the informed consent process about pain10 (eg will the procedure be painful?), less research has examined how the patient being in a state of pain can impact the informed consent process. Patients in pain may be particularly less likely to bring up questions during informed consent process and therefore be more reliant on their clinicians actively eliciting questions.
Given the importance of the informed consent discussion and to identify opportunities for education, the present study examined whether anesthesiology residents elicited questions during perioperative informed consent of a simulated patient in visible state of pain. In addition to understanding if the resident elicited questions, we explored the timing of when the resident asked the patient if they had any questions and how the elicitation of questions was worded by the resident.
Materials and Methods
This observational study was part of a research program assessing anesthesiology resident competence across three Harvard Medical School-affiliated anesthesiology residency programs.3 A convenience sample was video-recorded during participation in the validated Harvard Anesthesia Resident Performance Assessment (HARP).11,12 The Office of Clinical Investigations at Boston Children’s Hospital approved the protocol (X07-09-0395) and residents completed an informed consent.
The HARP scenario depicted a 52-year-old White man simulated patient (SP) awaiting urgent repair of a perforated gastric ulcer.3 The SP was medically stable but instructed to demonstrate acute abdominal pain through multiple standardized verbal and nonverbal pain cues and to express concern about post-operative nausea and vomiting because of previous negative anesthetic experience. Residents were instructed to obtain informed consent. Residents were told the surgeon wished to proceed urgently to the operating room, creating realistic time pressure. Residents were not made aware of the goal of this research or specifically instructed on asking or answering questions before the simulated encounter.
The coding of whether, when, and how residents elicited questions from the SPs included: whether any questions were elicited (yes/no); the number of times a question was elicited; length of time to first question to be elicited; when the first question was elicited relative to handing consent form to SP (before, during, after); when the first question was elicited relative to signing consent form (before, during, after); whether question elicitation was open-ended (eg, What questions do you have?) or closed-ended (eg, Do you have any questions?); whether question elicitation was personal (eg, incorporates patient’s name and/or includes the physician’s reference to self) or impersonal; and whether the resident made eye contact during question elicitation (yes/no).
Two coders independently coded the videos and reached consensus on discrepancies through reviewing the video and discussion.13 Overall Kappa statistic prior to consensus discussions was .86 for all codes, indicating acceptable inter-rater reliability.
Descriptive statistical analyses included frequency counts and percentages. One-way ANOVA compared the number of questions, when, and how the questions were elicited by resident gender and anesthesiology residency year (first-year vs third-year).
Results
A total of 65 anesthesiology residents participated, including 28 (43.1%) men and 37 (56.9%) women, with 49 (75.4%) first-year and 16 (24.6%) third-year residents. Residents represented three accredited anesthesiology residency programs including Beth Israel Deaconess Medical Center (n = 20, 30.8%), Brigham and Women’s Hospital (n = 25, 38.5%) and Massachusetts General Hospital (n = 20, 30.8%). On average, simulated informed consent encounters lasted 9.8 (SD = 2.1) minutes and ranged from 5.3–15.9 minutes in length.
Of the 65 residents, 51 (78.5%) elicited questions from the SP and 14 (21.5%) did not (Table 1). Of those 51 residents who elicited questions, 29 (56.9%) inquired once if the SP had any questions and 22 (43.1%) inquired two or more times. The first elicitation of questions typically occurred toward the end of obtaining informed consent, an average of 8.3 minutes (SD = 2.3) into the interaction, such that questions were elicited after 83.4% of the encounter had elapsed. Of those who elicited questions, most residents (n = 39, 76.5%) elicited SP questions for the first time before handing the consent form to the SP to sign, a few (n = 3, 5.9%) elicited questions while handing the form, and the remaining (n = 9, 17.6%) elicited questions only after handing the form to the SP. Similarly, most residents (n = 46, 90.2%) elicited questions before the SP had signed the consent form, but 5 (9.8%) elicited questions for the first time only after the SP had already signed the consent form.
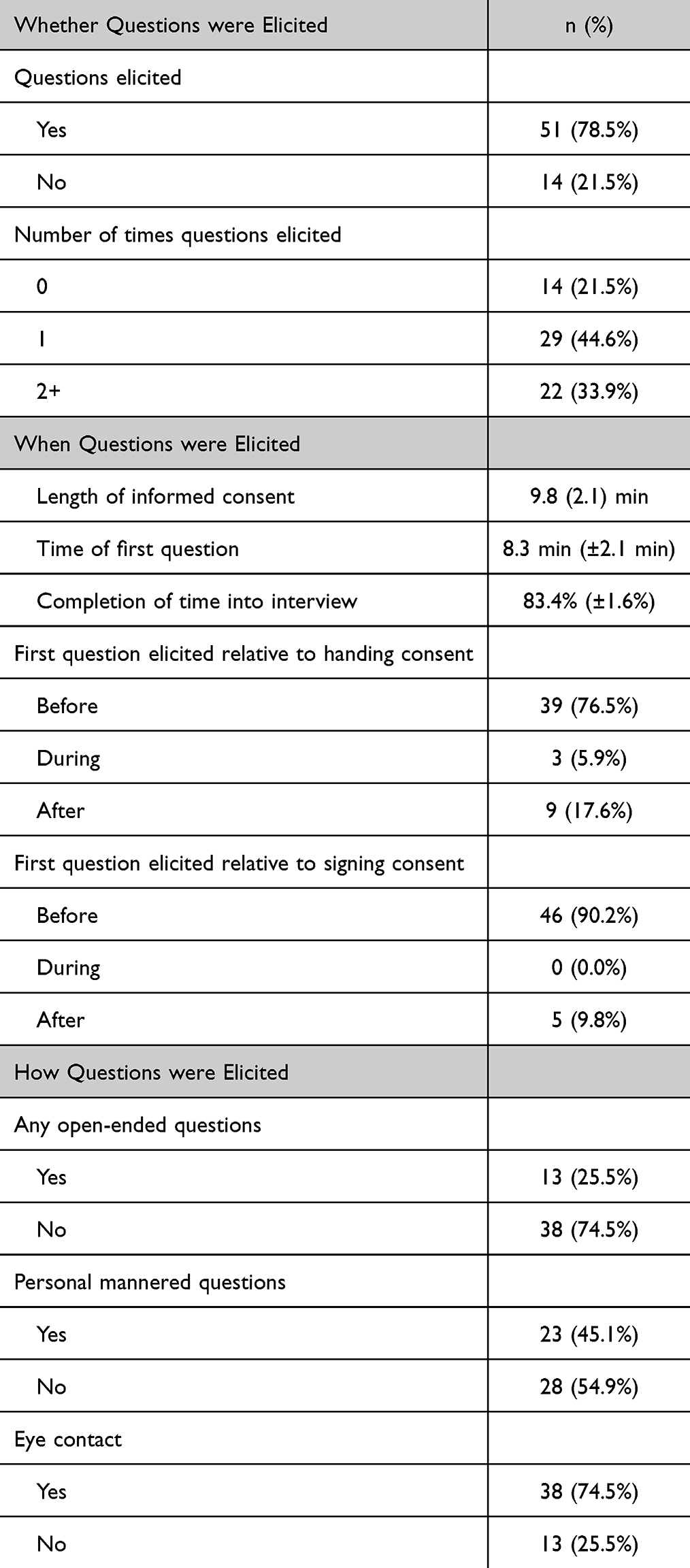 |
Table 1 Whether, When and How Patient Questions Were Elicited During Anesthesia Informed Consent Encounters |
Among residents who elicited questions, most (n = 38, 74.5%) asked closed-ended questions. Just under half (n = 23, 45.1%) asked personalized questions, incorporating the patient’s name and/or the physician’s reference to self (eg, “Mr. Smith, what questions do you have for me?”). Most residents (n = 38, 74.5%), made eye contact while eliciting questions.
Whether or not residents solicited questions, when in the encounter the question was solicited, or whether open or closed questions were asked did not significantly differ based on resident gender (p = 0.15, p = 0.57, p = 0.52, respectively) or residency year (p = 0.96, p = 0.83, p = 0.48, respectively).
Discussion
Patients’ fears about anesthesia are well-documented14–16 and their retention of information during informed consent can be limited.17 Patients’ difficultly processing information during informed consent may be exacerbated by being in a state of pain.9 Eliciting questions during informed consent promotes patient engagement, trust, mutual understanding, and reassurance.5,18
This observational study of anesthesiology residents indicates opportunities for improving question elicitation during informed consent since more than 20% of the residents did not elicit questions. Nearly a quarter of residents who elicited questions did so during or after the consent form had been handed to be signed. Emphasis on the form itself could disrupt a natural question-and-answer exchange or convey that signing the form was more important than patient questions. Moreover, most residents failed to ask open-ended questions, which are known to encourage patients to share more information.19,20
Anesthesia informed consent poses unique challenges since most anesthesiologists meet patients on the day of surgery and have limited time to obtain informed consent.21 Patients may be experiencing perioperative pain. In busy practice environments, waiting until all the information has been provided before inviting patients’ questions may be deemed most efficient since questions could presumably be addressed over the course of the discussion. However, open-ended elicitation of patient concerns early in a visit can actually reduce time spent on concerns later in the visit and even improve health outcomes.22,23 Further, setting a tone early of eliciting questions can assuage patient anxiety, facilitate patient-centeredness, and generate greater patient satisfaction.
Based on these results, we encourage anesthesiology training programs to incorporate more explicit guidance, practice and feedback on how and when patient questions can be elicited during informed consent. Practical educational examples could include embedding learning opportunities to encourage and provide time for students to ask patients what questions they have during informed consent encounters. If incorporating simulation, standardized patients could be engaged to portray various patient styles ranging from asking no questions (and how to address this through modeling and offering answers to commonly asked questions), to asking very detailed questions. Training should also include how to recognize and respond to patient pain24 and then how best to elicit questions when a patient is in a state of pain. Since patient characteristics such as age, race/ethnicity, language barriers, literacy level, educational attainment, and previous anesthetic and healthcare experiences can influence patient question-asking, training residents to elicit questions early and proactively during informed consent may be particularly important for ensuring ethical and equitable care in vulnerable patient populations.25
Several limitations exist in this observational study. Data was collected during simulated informed consent evaluation. This may have motivated residents to elicit more questions or not represented typical practice. The SP was a White adult man awaiting urgent surgery and expressing pain. It is reasonable that eliciting questions varies depending on multiple factors including patient characteristics, urgency of surgery, and/or presentation of pain. Anesthesiology residents were studying in the same northeastern city, limiting generalizability.
Future research on eliciting questions during informed consent could examine patient priorities regarding question-asking, how elicitation of questions impacts retention of information and decision-making, and the concurrent effects of busy clinical environments. Examining naturally occurring clinical approaches to eliciting questions would be worthwhile, such as optimal timing and phrasing in different clinical situations, including for patients in pain. Alternate approaches could be compared regarding time requirements, patient experience and outcomes, and satisfaction with care. Finally, research should assess whether eliciting questions leads to improved physician engagement and well-being.
Conclusion
Our findings demonstrate variability and practice lapses among residents regarding elicitation of patient questions during anesthesia informed consent with a standardized patient in pain. We advocate that the purpose and specifics of eliciting questions be incorporated into learning paradigms for anesthesia informed consent. Effectiveness of anesthesiology training approaches to improve question-elicitation and other aspects of the informed consent process should also be rigorously evaluated in future research. Multifaceted informed consent educational programs including didactics, role-play, simulation, and practice-based experiences may have advantages over more traditional educational approaches.26–29 Systems-level strategies and organizational support, such as more time and greater privacy, to encourage anesthesiologists to elicit questions within the informed consent process should also be considered.
Conceptualizing question elicitation as an expression of patient-centered anesthesiology and as opportunities for patients to exercise autonomy and shape conversations in personally meaningful ways highlights the value of high-quality informed consent discussions beyond mere conveyance of information and consent form signing.
Declaration of Generative AI in Scientific Writing
No generative AI or AI-assisted technologies were used in the scientific writing of this manuscript.
Data Sharing Statement
De-identified data and any requests for access to the videos used in this study can be made available by contacting the corresponding author.
Ethics Approval and Informed Consent
The Office of Clinical Investigations at Boston Children’s Hospital approved the protocol through expedited review on 09/25/2007. Protocol Number: X07-09-0395. Residents completed an informed consent.
Acknowledgments
This work was supported by the Cathedral Fund, Newton Centre, MA and the Branta Foundation, New York, New York, USA. Work on this paper by the first author (DBH) was supported by the Bentley Center for Health and Business. Work on this paper by the third author (MAR) was supported by the National Institute of Health on Minority Health and Disparities K01MD020123.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Grady C. Enduring and emerging challenges of informed consent. N Engl J Med. 2015;372:855–7. doi:10.1056/NEJMra1411250
2. Beauchamp TL, Childress JF. Principles of Biomedical Ethics. Edicoes Loyola; 1994.
3. Waisel DB, Ruben MA, Blanch-Hartigan D, Hall JA, Meyer EC, Blum RH. Compassionate and clinical behavior of residents in a simulated informed consent encounter. Anesthesiology. 2020;132:159–169. doi:10.1097/ALN.0000000000002999
4. Waisel DB, Lamiani G, Sandrock NJ, Pascucci R, Truog RD, Meyer EC. Anesthesiology trainees face ethical, practical, and relational challenges in obtaining informed consent. J Am Soc Anesthesiologists. 2009;110:480–486.
5. Greene J, Hibbard JH. Why does patient activation matter? An examination of the relationships between patient activation and health-related outcomes. J Gen Intern Med. 2012;27:520–526. doi:10.1007/s11606-011-1931-2
6. Beisecker AE, Beisecker TD. Patient information-seeking behaviors when communicating with doctors. Med Care. 1990;28:19–28. doi:10.1097/00005650-199001000-00004
7. Négrier S, Lanier-Demma F, Lacroix-Kante V, et al. Evaluation of the informed consent procedure in cancer patients candidate to immunotherapy. Eur J Cancer. 1995;31:1650–1652. doi:10.1016/0959-8049(95)00329-H
8. Murtagh GM, Furber L, Thomas AL. Patient-initiated questions: how can doctors encourage them and improve the consultation process? A qualitative study. BMJ Open. 2013;3:e003112. doi:10.1136/bmjopen-2013-003112
9. Khera T, Rangasamy V. Cognition and pain: a review. Front Psychol. 2021;12:673962. doi:10.3389/fpsyg.2021.673962
10. Paci E, Barneschi MG, Miccinesi G, Falchi S, Metrangolo L, Novelli GP. Informed consent and patient participation in the medical encounter: a list of questions for an informed choice about the type of anaesthesia. Eur J Anaesthesiol. 1999;16:160–165. doi:10.1097/00003643-199903000-00004
11. Blum RH, Muret-Wagstaff SL, Boulet JR, et al; Harvard Assessment of Anesthesia Resident Performance Research Group. Simulation-based assessment to reliably identify key resident performance attributes. Anesthesiology. 2018;128:821–831. doi:10.1097/ALN.0000000000002091
12. Blum RH, Boulet JR, Cooper JB, Muret-Wagstaff SL; Harvard Assessment of Anesthesia Resident Performance Research Group. Simulation-based assessment to identify critical gaps in safe anesthesia resident performance. Anesthesiology. 2014;120:129–141. doi:10.1097/ALN.0000000000000055
13. Blanch-Hartigan D, Ruben MA, Hall JA, Schmid Mast M. Measuring nonverbal behavior in clinical interactions: a pragmatic guide. Patient Educ Couns. 2018;101:2209–2218. doi:10.1016/j.pec.2018.08.013
14. Cheng JYJ, Wong BWZ, Chin YH, et al. Preoperative concerns of patients undergoing general surgery. Patient Educ Couns. 2021;104:1467–1473. doi:10.1016/j.pec.2020.11.010
15. Mavridou P, Dimitriou V, Manataki A, Arnaoutoglou E, Papadopoulos G. Patient’s anxiety and fear of anesthesia: effect of gender, age, education, and previous experience of anesthesia. A survey of 400 patients. J Anesth. 2013;27:104–108. doi:10.1007/s00540-012-1460-0
16. Burkle CM, Mann CE, Steege JR, Stokke JS, Jacob AK, Pasternak JJ. Patient fear of anesthesia complications according to surgical type: potential impact on informed consent for anesthesia. Acta Anaesthesiol Scand. 2014;58:1249–1257. doi:10.1111/aas.12413
17. Bai JW, Abdallah FW, Cohn M, Ladowski S, Madhusudan P, Brull R. Say what? Patients have poor immediate memory of major risks of interscalene block disclosed during the informed consent discussion. Reg Anesth Pain Med. 2019;44:981–985. doi:10.1136/rapm-2019-100858
18. Street RL. Information-giving in medical consultations: the influence of patients’ communicative styles and personal characteristics. Soc Sci Med. 1991;32:541–548. doi:10.1016/0277-9536(91)90288-N
19. Kindler CH, Szirt L, Sommer D, Hausler R, Langewitz W. A quantitative analysis of anaesthetist-patient communication during the pre-operative visit. Anaesthesia. 2005;60:53–59. doi:10.1111/j.1365-2044.2004.03995.x
20. Takemura Y, Sakurai Y, Yokoya S, et al. Open-ended questions: are they really beneficial for gathering medical information from patients? Tohoku J Exp Med. 2005;206:151–154. doi:10.1620/tjem.206.151
21. Tait AR, Teig MK, Voepel-Lewis T. Informed consent for anesthesia: a review of practice and strategies for optimizing the consent process. Can J Anaesth. 2014;61:832–842. doi:10.1007/s12630-014-0188-8
22. Marvel MK, Epstein RM, Flowers K, Beckman HB. Soliciting the patient’s agenda: have we improved? JAMA. 1999;281:283–287. doi:10.1001/jama.281.3.283
23. Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Family Med. 2011;24:229–239. doi:10.3122/jabfm.2011.03.100170
24. Ruben MA, Blanch-Hartigan D, Laquidara J, et al. How responsive are anesthesiologists to patient pain? Residents’ verbal and nonverbal responses to standardized patient pain cues. J Nonverbal Behav. 2021:1–18.
25. Eggly S, Harper FWK, Penner LA, Gleason MJ, Foster T, Albrecht TL. Variation in question asking during cancer clinical interactions: a potential source of disparities in access to information. Patient Educ Couns. 2011;82:63–68. doi:10.1016/j.pec.2010.04.008
26. Lee SC, Nguyen V, Nguyen A, Minard CG, Rajagopalan S. Teaching anesthesiology residents how to obtain informed consent. J Educ Perioper Med. 2019;21:E632.
27. Bashir MA, Khan AA, Khan SA. Assessment of informed consent and the impact of simulation on anesthesia trainees. Cureus. 2021;13. doi:10.7759/cureus.19787
28. Koller SE, Moore RF, Goldberg MB, et al. An informed consent program enhances surgery resident education. J Surg Educ. 2017;74:906–913. doi:10.1016/j.jsurg.2017.02.002
29. Antoniou A, Marmai K, Qasem F, Cherry R, Jones PM, Singh S. Educating anesthesia residents to obtain and document informed consent for epidural labor analgesia: does simulation play a role? Int J Obstet Anesth. 2018;34:79–84. doi:10.1016/j.ijoa.2017.12.005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.