Back to Journals » Journal of Inflammation Research » Volume 19
ANCA-Associated Vasculitis with Predominant Peripheral and Central Nervous System Involvement: A Case Report
Authors Zhang B ![]() , Jing C, Liu P, Zhang J
, Jing C, Liu P, Zhang J ![]()
Received 5 December 2025
Accepted for publication 17 March 2026
Published 24 March 2026 Volume 2026:19 586113
DOI https://doi.org/10.2147/JIR.S586113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Bing Zhang, Chaoyang Jing, Peipei Liu, Jianlei Zhang
Department of Neurology, Huaihe Hospital of Henan University, Kaifeng, Henan, 475000, People’s Republic of China
Correspondence: Jianlei Zhang, Department of Neurology, Huaihe Hospital of Henan University, Kaifeng, Henan, 475000, People’s Republic of China, Email [email protected]
Background: ANCA-associated vasculitis (AAV) is an immune-mediated multi-system disease. It can present with neurological involvement as its predominant manifestation. We report a case of AAV with predominant peripheral and central nervous system involvement.
Case Presentation: A 62-year-old male presented with fever and asymmetric weakness and pain in the lower limbs. Electrophysiological studies revealed asymmetric axonal damage in both lower limbs. During hospitalization, he developed acute bulbar palsy. Brain MRI confirmed bilateral basal ganglia infarction. Ancillary tests indicated involvement of the lungs, kidneys, and hematological systems, along with positive MPO-ANCA (p-ANCA), confirming the diagnosis of AAV. His symptoms gradually improved following treatment with glucocorticoids and immunosuppressants. At the 6-month follow-up, his symptoms were largely resolved.
Conclusion: The presence of asymmetric axonal neuropathy or atypical non-atherosclerotic cerebral infarction, particularly when accompanied by multisystem involvement, should raise suspicion for AAV. Early diagnosis and prompt treatment significantly improve patient outcomes.
Keywords: ANCA-associated vasculitis, MPA, peripheral neuropathy, central nervous system
Introduction
ANCA-associated vasculitis (AAV) is a necrotizing vasculitis characterized by few or no immune deposits, affecting small-to-medium vessels, and capable of affecting almost any organ.1 AAV encompasses three distinct entities: microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA), and eosinophilic granulomatosis with polyangiitis (EGPA). The pathogenesis of AAV involves antibodies against two principal antigenic targets: leukocyte proteinase 3 (PR3-ANCA) and myeloperoxidase (MPO-ANCA). A recent ultrastructural study demonstrated the importance of neutrophils in the early pathophysiology of MPA.2 Another ultrastructural study in EGPA visualized the behavior of eosinophils and demonstrated tissue damage mediated by both extravascular and intravascular eosinophils.3
Peripheral nerve involvement is common in AAV and typically manifests as asymmetric axonal neuropathy, most frequently in patients with EGPA (60–70%), followed by MPA (20–50%) and GPA (15–50%).4 Central nervous system involvement is rare in AAV, occurring in approximately 1.6–15% of cases, with no significant predisposition for any particular type of vasculitis.4–6 The clinical manifestations are heterogeneous, and presentation as acute cerebral infarction is notably rare. The patients presenting predominantly with peripheral and central nervous system involvement are exceedingly rare. Herein, we report a case of AAV with predominant peripheral and central nervous system involvement.
Case Presentation
A 62-year-old male presented with 20-day histories of fever and bilateral lower limb weakness, and 15-day histories of bilateral lower limb edema and pain, under suspicion of Guillain-Barré syndrome (GBS). 20 days prior to admission, he developed fever (approximately 37.5°C), cough, productive sputum, and bilateral lower limb weakness (maintaining independent ambulation). No significant improvement was observed following antibiotic treatment. 15 days prior to admission, he developed bilateral lower limb edema and severe pain in the posterior calf muscles. Chest CT at a local hospital revealed bronchiectasis with bilateral pulmonary inflammation and minimal pericardial effusion. Following treatment for suspected pneumonia and cardiac insufficiency, the edema partially resolved. However, he experienced persistent fever with progressive worsening of lower limb weakness and pain, particularly in the left limb manifesting as: (1) inability to ambulate independently; (2) intolerable pain triggering episodes of crying. Nerve conduction studies demonstrated axonal damage in bilateral femoral, tibial, common peroneal, superficial peroneal, and sural nerves (more pronounced on the left). Additionally, needle electromyography revealed neurogenic changes in the vastus medialis, tibialis anterior, and gastrocnemius muscles bilaterally. His medical history included bronchiectasis for 40 years, diabetes mellitus for 15 years, and rheumatoid arthritis for 10 years, with no history of asthma or nasal involvement. Clinical examination revealed weakness in both lower extremities (4/5 on the modified Research Council (MRC) scale on the right, 4-/5 on the left), hypoalgesia below both ankles, and impaired vibration sense and kinesthesia in the left foot. Cerebrospinal fluid (CSF) analysis showed normal routine and biochemical parameters. Blood routine examination revealed leukocytosis (11.04 × 109/L), neutrophilia (8.74 × 109/L), mild anemia (hemoglobin 120 g/L, N: 130~175), and a normal eosinophil count (0.06 × 109/L). Elevated plasma free hemoglobin (99.3 mg/L, N <40) suggesting intravascular hemolysis. Urinalysis showed proteinuria (1+) and hematuria (3+), with elevated 24-hour urinary protein excretion of 1.85 g/24h (N <0.20). Blood biochemistry demonstrated hypoalbuminemia (24.6 g/L), fasting hyperglycemia (7.38 mmol/L) and elevated HbA1c (8.30%). Autoimmune serology revealed: positive rheumatoid factor (474 IU/mL, N <18), positive anti-CCP antibody (474 U/mL, N <25), positive myeloperoxidase (MPO-ANCA) (98.68 AU/mL, N <20), positive perinuclear (p-ANCA) (1:32, N <1:10), negative proteinase 3 (PR3-ANCA) and cytoplasmic (c-ANCA). Additionally, all three laboratory parameters were markedly elevated: erythrocyte sedimentation rate (ESR) 93 mm/h, C-reactive protein (CRP) 224.00 mg/L, and D-dimer 5169 ug/L (N <232). Serological testing revealed no abnormalities in: antinuclear antibody (ANA), anticardiolipin antibody, anti-glomerular basement membrane antibody, hepatitis B/C, HIV, syphilis, tumor markers, folate, and vitamin B12 levels.
On day 7 of admission, the patient developed headache and dysphagia. Brain MRI demonstrated multifocal abnormalities in the bilateral putamina (hypointensity on T1-weighted images, hyperintensity on T2-weighted images, and hyperintensity on both FLAIR and DWI sequences) (Figure 1). These findings collectively suggested acute cerebral infarction due to cerebral small vessel disease secondary to ANCA-associated vasculitis (AAV).
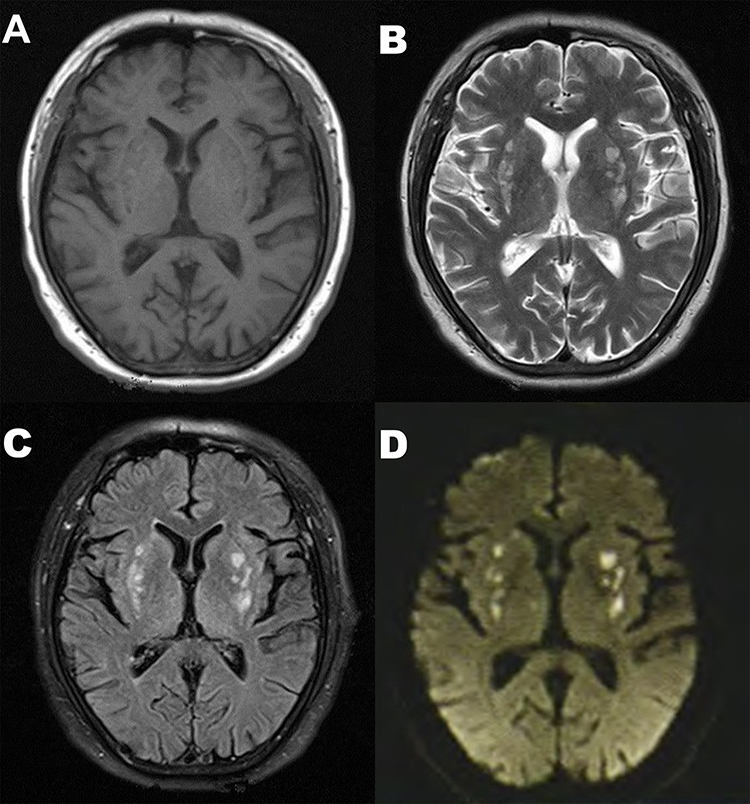 |
Figure 1 Brain MRI demonstrating multifocal abnormalities in the bilateral putamina. (A) hypointensity on T1-weighted images; (B) hyperintensity on T2-weighted images; (C) hyperintensity on FLAIR sequences; (D) hyperintensity on DWI sequences. |
The patient was diagnosed with AAV involving both peripheral and central nervous systems. Treatment with glucocorticoids, cyclophosphamide, and mycophenolate mofetil resulted in: resolution of fever, improvement in limb weakness/pain and dysphagia. Following discharge, maintenance immunosuppression with glucocorticoids and mycophenolate mofetil was continued. At 6-month follow-up, the patient achieved: independent ambulation, near-complete resolution of limb pain and dysphagia.
Discussion
Classic Guillain-Barré syndrome (GBS) typically presents as a post-infectious, symmetrical polyneuropathy, which may be accompanied by muscle pain. The patient primarily presented with a painful asymmetric axonal polyneuropathy predominantly affecting both lower limbs, accompanied by persistent fever. While atypical GBS variants may demonstrate similar manifestations, differentiation from other infectious or inflammatory peripheral neuropathies is essential. He exhibited multisystem involvement (lungs, kidneys, and hematological systems) without cerebrospinal fluid inflammatory changes. Serologic screening revealed positive MPO-ANCA (p-ANCA). Based on the clinical signs and ancillary test results, he fulfilled the 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR) classification criteria for MPA.7–9 He was diagnosed with AAV involving the peripheral nervous system.
Peripheral nervous involvement is common in AAV and may serve as the initial manifestation of the disease. Reported frequencies of peripheral neuropathy in AAV range from 10% to 80%, with higher rates observed in eosinophilic granulomatosis with polyangiitis (EGPA) (60–70%) and microscopic polyangiitis (MPA) (20–50%).4–6,10 The pathophysiological mechanism of peripheral nerve involvement in AAV involves inflammatory vasculitis affecting the epineurial or perineurial vessels, leading to ischemic axonal degeneration. This process is accompanied by destruction of the vascular layers and/or obstruction of the lumen.11 Peripheral nerve involvement in AAV is similar to other vasculitic neuropathies, typically presenting with the acute-to-subacute onset of painful sensory or sensorimotor neuropathy that is generally more pronounced in the lower limbs. Electrophysiological studies typically reveal patchy or multifocal axonal degeneration involving sensory and motor nerves. Asymmetric, non-length-dependent axonal neuropathy is highly suggestive of vasculitis.12
During hospitalization, the patient developed acute bulbar palsy and headache. MRI revealed acute bilateral basal ganglia lesions, leading to a diagnosis of acute cerebral infarction secondary to AAV. AAV should be suspected in multifocal cerebral infarcts from small-medium vessel vasculitis. Given AAV’s dual risks of infarction and hemorrhage, intravenous thrombolysis or antithrombotic therapy requires rigorous bleeding risk assessment.
Central nervous system (CNS) involvement is rare in AAV, occurring in approximately 1.6–15% of cases, with no significant predisposition to any particular type of vasculitis.4–6 Furthermore, various factors such as involvement of other organ systems, drug-related adverse events, infections, and comorbidities can mimic CNS involvement in patients with AAV. After ruling out these mimicking conditions, a 2025 study reported that the frequency of true CNS involvement in AAV was only 1.6%.6 Patients presenting predominantly with peripheral and central nervous system involvement are exceedingly rare. In contrast to the characteristic patterns of peripheral nervous involvement in AAV, CNS involvement in AAV is heterogeneous, including ischemic/hemorrhagic strokes, hypertrophic pachymeningitis, pituitary dysfunction, and posterior reversible encephalopathy syndrome.5 The pathophysiological mechanism of CNS involvement in AAV encompasses two principal processes: necrotizing inflammation of small-to-medium vessels and granulomatous inflammation. In general, dural or pituitary lesions are mainly attributed to granulomatous inflammation, while parenchyma pathologies are mediated by vasculitis. It is noteworthy that MPA does not feature granulomatous inflammation.
Active AAV is characterized by elevated ESR and CRP, and is often associated with a hypercoagulable state.1 In this patient, significantly elevated laboratory markers strongly support the diagnosis. The markedly increased D-dimer and plasma free hemoglobin levels suggest intravascular hemolysis due to microthrombosis. We speculate that microvascular thrombosis may also constitute a key pathophysiological mechanism underlying his central and peripheral nerve damage.
Differential diagnoses include diabetic peripheral neuropathy and rheumatoid vasculitis. The patient presented with acute asymmetric polyneuropathy, and both the clinical manifestations and electromyography findings were inconsistent with diabetic asymmetric peripheral neuropathy (encompassing diabetic radiculopathy, mononeuropathy, and cranial neuropathy).13 The patient presented with no joint pain or swelling at the time of evaluation; therefore, the neurological manifestations were not attributed to rheumatoid vasculitis. A previous study indicated that ANCA-associated vasculitis may develop during the disease course in some patients with rheumatoid arthritis; however, the relationship between these two conditions requires further elucidation.14
The study has several limitations. The main limitation is the lack of pathological data confirming neurological and renal involvement. Other limitations include the incomplete evaluation of other stroke etiologies, particularly the lack of magnetic resonance angiography and high-resolution vessel wall MRI, as well as the speculative discussion regarding microvascular thrombosis.
Conclusion
AAV can present with neurological involvement as its primary manifestation. Although AAV with predominant involvement of both the peripheral and central nervous systems is exceedingly rare, clinicians should consider a diagnosis of AAV when a patient presents with asymmetric axonal neuropathy or atypical non-atherosclerotic cerebral infarction. Systematic evaluation for multisystem involvement and early autoantibody testing in such patients facilitate diagnosis and treatment.
Data Sharing Statement
The anonymized data that support the findings of this study are available from the corresponding author (Jianlei Zhang) upon reasonable request.
Ethical Approval and Consent to Participate
This report conforms to the Declaration of Helsinki. Ethical review and approval were waived for this study in accordance with local legislation and institutional requirements. Verbal and written informed consent were obtained from the patient and his caregivers.
Consent to Publish
The patient has given his consent and authorized his clinical data in our report to be published.
Acknowledgments
The authors would like to thank the patient who participated in this study.
This case report was written following the CARE guidelines (for CAse REports) published in 2013 in the Journal of Clinical Epidemiology.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Bing Zhang: Conceptualization, Writing – original draft; Chaoyang Jing: Data curation; Peipei Liu: Data curation; Jianlei Zhang: Conceptualization, Writing – review and editing.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kronbichler A, Bajema IM, Bruchfeld A, Mastroianni Kirsztajn G, Stone JH. Diagnosis and management of ANCA-associated vasculitis. Lancet. 2024;403(10427):683–5. doi:10.1016/S0140-6736(23)01736-1
2. Koike H, Furukawa S, Mouri N, Fukami Y, Iijima M, Katsuno M. Early ultrastructural lesions of anti-neutrophil cytoplasmic antibody- versus complement-associated vasculitis. Neuropathology. 2022;42(5):420–429. doi:10.1111/neup.12821
3. Koike H, Nishi R, Furukawa S, et al. In vivo visualization of eosinophil secretion in eosinophilic granulomatosis with polyangiitis: an ultrastructural study. Allergol Int. 2022;71(3):373–382. doi:10.1016/j.alit.2022.02.009
4. Wludarczyk A, Szczeklik W. Neurological manifestations in ANCA-associated vasculitis - assessment and treatment. Expert Rev Neurother. 2016;16(8):861–863. doi:10.1586/14737175.2016.1165095
5. Zheng Y, Zhang Y, Cai M, Lai N, Chen Z, Ding M. Central nervous system involvement in ANCA-associated vasculitis: what neurologists need to know. Front Neurol. 2019;9:1166. doi:10.3389/fneur.2018.01166
6. Yagiz Ozogul Y, Esatoglu SN, Ozogul M, et al. Central nervous system involvement and mimickers in ANCA associated vasculitis. J Neurol. 2025;272(8):492. doi:10.1007/s00415-025-13203-z
7. Suppiah R, Robson JC, Grayson PC, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for microscopic polyangiitis. Ann Rheum Dis. 2022;81(3):321–326. doi:10.1136/annrheumdis-2021-221796
8. Grayson PC, Ponte C, Suppiah R, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis. Ann Rheum Dis. 2022;81(3):309–314. doi:10.1136/annrheumdis-2021-221794
9. Robson JC, Grayson PC, Ponte C, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for granulomatosis with polyangiitis. Ann Rheum Dis. 2022;81(3):315–320. doi:10.1136/annrheumdis-2021-2217952022
10. Quintero-Giraldo LP, Barahona-Correa J, Corredor-Orlandelli D, García-Alfonso C, Herrera-Leaño N, Fernández-ávila DG. Nervous system involvement in ANCA-associated vasculitis: single center experience from Latin America. Semin Arthritis Rheum. 2025;73:152751. doi:10.1016/j.semarthrit.2025.152751
11. Koike H, Nishi R, Ohyama K, et al. ANCA-associated vasculitic neuropathies: a review. Neurol Ther. 2022;11(1):21–38. doi:10.1007/s40120-021-00315-7
12. Gwathmey KG, Burns TM, Collins MP, Dyck PJ. Vasculitic neuropathies. Lancet Neurol. 2014;13(1):67–82. doi:10.1016/S1474-4422(13)70236-9
13. Sinnreich M, Taylor BV, Dyck PJ. Diabetic neuropathies. Classification, clinical features, and pathophysiological basis. Neurologist. 2005;11(2):63–79. doi:10.1097/01.nrl.0000156314.24508.ed
14. Draibe J, Salama AD. Association of ANCA associated vasculitis and rheumatoid arthritis: a lesser recognized overlap syndrome. Springerplus. 2015;4(1):50. doi:10.1186/s40064-015-0835-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.