Back to Journals » Risk Management and Healthcare Policy » Volume 16
Analyzing the Effectiveness of Data-Linked Projects for Health Promotion in Public Health Centers of South Korea
Authors Yoon K, Kim HK, Choi M, Lee M ![]() , Jakovljevic M
, Jakovljevic M ![]()
Received 12 April 2023
Accepted for publication 10 June 2023
Published 16 June 2023 Volume 2023:16 Pages 1101—1117
DOI https://doi.org/10.2147/RMHP.S413630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Kichan Yoon,1 Han-Kyoul Kim,2,3 Mankyu Choi,4,5,* Munjae Lee,6,* Mihajlo Jakovljevic7– 9
1The Institute for Democracy, Seoul, Republic of Korea; 2Department of Rehabilitation Medicine, Seoul National University Hospital, Seoul, Republic of Korea; 3National Traffic Injury Rehabilitation Research Institute, National Traffic Injury Rehabilitation Hospital, Yang-Pyeong, Republic of Korea; 4Department of Health Policy & Management, College of Health Science, Korea University, Seoul, Republic of Korea; 5BK21 FOUR R&E Center for Learning Health Systems, Korea University, Seoul, Republic of Korea; 6Department of Medical Science, Ajou University School of Medicine, Suwon, Republic of Korea; 7Institute of Advanced Manufacturing Technologies, Peter the Great St. Petersburg Polytechnic University, St Petersburg, 195251, Russia; 8Institute of Comparative Economic Studies, Hosei University, Tokyo, 194-0298, Japan; 9Department of Global Health Economics and Policy, University of Kragujevac, Kragujevac, 34000, Serbia
*These authors contributed equally to this work
Correspondence: Munjae Lee, Department of Medical Science, Ajou University School of Medicine, Suwon, Republic of Korea, Email [email protected] Mankyu Choi, Department of Health Policy & Management, College of Health Science, Korea University, Seoul, Republic of Korea, Email [email protected]
Purpose: The purpose of this study lies in verifying the effectiveness of the health promotion project which the public health center at the local level conducted by systematically linking the health examination results from the Health Insurance Corporation. We intend to emphasize the importance of linking the health-related public data.
Methods: A survey was conducted to measure the effect of improving health behavior using EQ-5D-5L and demographic variables.
Results: As a result of the analysis, the residents (3.13) who had experienced the use of public health centers recognized more necessity for the service linked systematically with health checkup data than those (2.93) who had not. In addition, the residents who had experienced the use of public health centers responded that their chronic diseases had improved compared to a year ago (2.78→ 2.93). Next, those (3.04) who had experienced the services linked with health checkup data recognized that their chronic diseases and health conditions had been improved compared to those (2.81) who had not. However, in EQ-5D-5L, after using the service, mobility showed no difference between those who had used the service and those who had not. Furthermore, even in terms of self-management, daily life, etc., the management ability was further improved compared to those who had not used it, before using the service.
Conclusion: This study showed the improved health level when the health promotion service of the public health center was provided by systematically linking the health checkup data of the Health Insurance Corporation in Korea. In order to increase the effectiveness of health data-linked projects, it is necessary to prepare guidelines for linking the public health data and to expand the data-linked project. It will be needed to further subdivide the health checkup results to provide customized services, and to secure dedicated personnel to reinforce the system link.
Keywords: subjective quality of life, EQ-5D-5L, regional health institutions, public data-linked services, South Korea
Introduction
Widespread population aging in Asia began to accelerate over the past few decades creating a serious challenge to health insurance, pension and retirement policies throughout the region.1,2 As of 2020, South Korean society has begun to age at a rate where the proportion of the elderly population has exceeded 14%; subsequently, public interest and demand for healthcare has increased. Particularly, in rural areas, the role played by regional health and medical institutions as public health centers is becoming increasingly prominent; the medical infrastructure needed to meet the healthcare needs is insufficient.3–5 Regional health and medical institutions are established and operated based on the Regional Public Health Act and the Act on Special Measures for Health and Medical Care in Rural Areas. The Regional Public Health Act regulates functioning of public health centers, health and medical centers, branch offices of health centers, health life-supporting centers, and so on; healthcare centers and other similar institutions have been established in accordance with the Act on Special Measures for Health and Medical Care in Rural Areas.6–9
Public health centers and health care centers function as regional health and medical institutions: the former mainly perform health promotion, disease management, and preventive activities for local residents; the latter are established in vulnerable healthcare areas, where they contribute to the health promotion of local residents.10,11 In particular, public health centers aid the implementation of 22 integrated health promotion projects regarding smoking prohibition, sobriety, nutrition, preventive management of obesity, maternal and child health, dementia management, and so on;12–14 all the data related to the project are being accumulated through the Public Health Information System. As of December 2019, the number of users of regional health and medical institutions, including public health centers was 6,394,510, or 12% of the total population.15
In 2018, owing to the national health-checkup project conducted by the National Health Insurance Corporation, the need for follow-up management in health and medical institutions increased, as 3.62 million people were suspected of having a disease. Accordingly, persons suspected of having a disease after a medical examination were linked to the Regional Public Health Information System, which, in turn, connected them to six kinds of public health center projects, including a cardio-cerebrovascular disease project, visiting healthcare projects, and so on.16–18 In March 2019, only 74 regional health and medical institutions utilized the medical checkup results. However, system function was improved so that the medical checkup results could be used when promoting the health promotion project at the public health center; therefore, 124 regional health and medical institutions began to implement the data-linked services. As of the end of December 2020, it was found that the relevant services had been provided to 169,391 out of the 1,591,827 health checkup result cases.19–23
At the community level, regional health and medical institutions play an important role in reducing disease and enhancing health levels. Furthermore, the data linkage between each system can be effectively utilized because it has no data collection cost or responding burden.24 Such programs have been introduced in other parts of the world as well; for instance, in British Columbia, Canada, the PopData BC (population data) is preparing policies to improve the health of local residents by linking medical services, population health, various data, and so on.25–28 Additionally, South Korea is building big-data platforms that can be linked with health data through next-generation health and medical information systems.29 Prioritization in artificial intelligence and big data investment is clearly visible through most major science and innovation funding agencies in Asia-Pacific region.30,31
Accordingly, this study concluded that it is necessary to assess the effectiveness of data-linked services in regional health and medical institutions when considering the importance of customized health services and linking data at the local community level. In other words, health promotion projects conducted through the linking of the regional health-checkups (PHIS) of regional health and medical institutions with the health checkup system of the National Health Insurance Corporation may measure effectiveness of these services. The purpose of this study is to analyze how much the health level of subjects has improved when the local public health centers link with the health checkup result data in the Health Insurance Corporation system while promoting health promotion projects. To this end, the necessity for health data-linked services, subjective health-improvement level, quality of life, improvement level of chronic diseases, and health satisfaction of the residents who had used the health data-linked services were compared with the cases of those who had not used. Here, the EQ-5D-5L scale, which is being used in more than 50 countries, was used to measure the subjective health-level.
Materials and Methods
While numerous tools are available to measure changes in health levels, ED-5D-3L and EQ-5D-5L have been widely used to assess quality of life in clinical research. EQ-5D-3L is the most widely used quality-of-life evaluation tool in clinical research, and it has been translated into more than 130 languages worldwide. EQ-5D-3L is a general health measurement tool used for evaluating health status in patients and in the general population. It comprises five areas: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The questionnaire response level encompasses three levels (no problem, slight problem, and serious problem). However, while the feasibility of EQ-5D-3L as a simple questionnaire tool has been validated among a wide range of patients, it has one limitation (ceiling effect) in its ability to distinguish differences in health or small individual-level changes over time among patients as well as the general population.
However, EQ-5D-5L was developed to improve the sensitivity and ceiling effect of EQ-5D-3L, where the five areas were the same, but each area included five levels. Official versions of EQ-5D-5L are available in more than 50 countries; the area name of motor ability has been changed to mobility. Specifically, it includes the indexes that ask each five level for the five areas: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.
To measure the effectiveness of the health-behavior improvements, this study used the EQ-5D-5L, the questionnaire for assessing health status and quality of life, which has been improved recently. In short, the five indices were utilized for measuring the effectiveness of the post-services linked to the medical checkup result data; the five-point Likert scale was used to analyze each health level (Table 1).
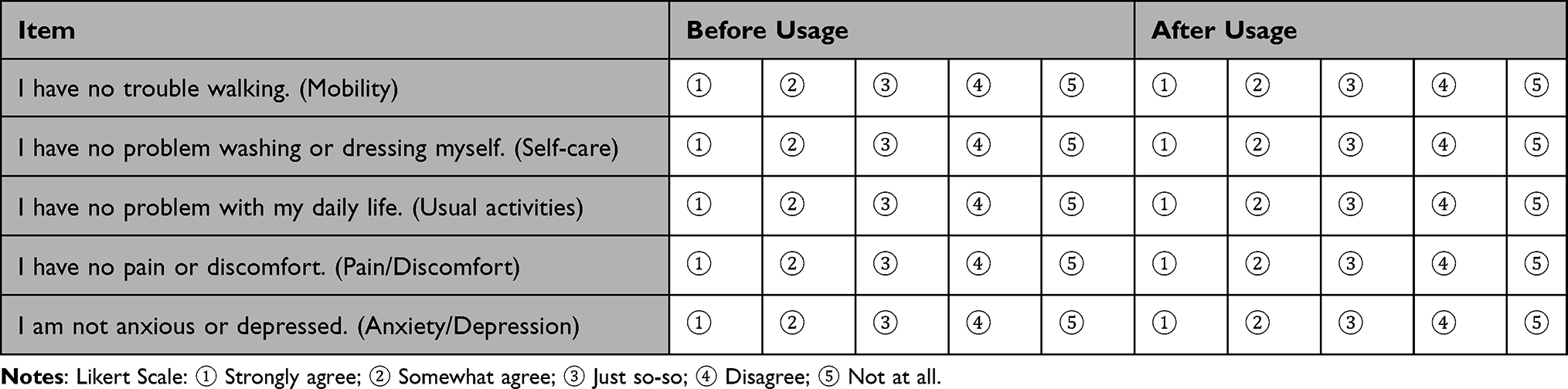 |
Table 1 Questionnaire for Measuring Subjective Quality of Life |
In this study, not only were questions about the official scale EQ-5D-5L added to ask for subjective quality of life, but questions were also added to ask for the necessity for health data-linked services, the subjective health-improvement level, the health satisfaction, and the chronic disease improvement level. Furthermore, demographic variables were used for examining the user characteristics of regional health and medical institutions. The user properties in health and medical institutions were investigated considering gender, age, marital status, educational background, health insurance type, monthly income level, number of household members, and so on.
To measure the effectiveness of the health data-linked service, the population group was divided according to whether to use local public health centers, whether there are those who had experienced the linked services among the center users, etc. Furthermore, in order to investigate the improvement level of health status, the questionnaire was designed to make the subjects respond by mutually comparing the current health conditions with a year ago. As for the analysis method, the two group mean comparison (t=test) was utilized to investigate the difference between users and non-users, experienced users and non-experienced users of the linked service, a-year-ago and now. And to verify the difference in health level according to the number of their having chronic diseases, one-way analysis of variance (ANOVA) was applied.
Specifically, a survey was conducted to measure the effectiveness of the linked service of public health centers, in which the data of health checkups – implemented annually by the National Health Insurance Corporation – were linked with the Regional Public Health Information System (PHIS). The questionnaire consists of a total of 18 questions, divided into a-year-ago and now, of 6 questions asking about whether to have the experience of using local public health centers, whether to have the usage experience of the medical checkup result data-linked service, the necessity for the linked service, the health satisfaction level, the number of chronic diseases, and the health status; of 7 demographic questions asking for gender, age, marriage, insurance type, monthly income, number of family members, and residence area; and of 5 questions asking about the health-related quality of life (EQ-5D-5L).
We commissioned Company B, a professional survey agency, to conduct the survey for one week from November 12, 2020 onward. For sampling, random panel surveys were conducted until 300 people who had experience in using health and medical institutions and 150 people who had experience in utilizing the post-services attached to the health checkup result were selected from among the survey agency’s 130,000 panels.
Results
Demographic Characteristics
To achieve the purpose of this study, 300 users and 200 non-users of public health centers were extracted by priority and then, 150 users and 150 non-users of data-linked services were extracted as well among public health center users. More than 10,000 panels were utilized to extract the survey subjects according to whether or not they had used them. Nevertheless, it is necessary to expand the number of survey subjects through additional researches in order to generalize the research results. The results revealed the following socio-demographic characteristics.
First, to a question regarding experience of using regional health and medical institutions, 300 people (59.4%) answered that they had some experience; 200 (40.6%) said they had no experience.
Second, for a question regarding experience of using post-services from health checkup results, 150 answered that they had experience, accounting for 50% of the 300 people who had experience in using health and medical institutions.
Third, among the survey subjects, 175 people (35.0%) answered “Not at all” to the question on the number of chronic diseases they had during the survey period; 38.8% (the highest; 194 people) answered “One chronic disease”. Furthermore, 131 (26.2%) were suffering from two or more chronic diseases.
Fourth, 242 participants were men (48.4%) and 258 were women (51.6%).
Fifth, the study age group was limited to those in their 40s or older due to the characteristics of chronic diseases. The survey results showed that 233 people (58.6%) were in their 40s, followed by 153 (30.6%) in their 50s, 54 (10.8%) in their 60s or older, and others.
Sixth, to a question on marital status, 81.7% (407 people) answered that they had been married, and 91 people (18.3%) answered that they were single.
Seventh, to a question on health insurance types, 335 people indicated that they had workplace insurance—about 38.0% more than 147 regional insurance holders. Eighth, to a question on monthly income, 8.4% (42 people) indicated they were earning less than 2 million won based on the median income of about 4.8 million. Those earning between 2 million won or more and less than 4 million won accounted for 33.8% (the highest; 169 people), followed by 166 people (33.2%) earning between 4 million won or more and less than 6 million won, and 123 (24.6%) earning 6 million won or more.
Ninth, in terms of the number of family members, 355 people said they had more than three family members, accounting for 71.0% (the highest). It was followed by 86 people (17.2%) with two family members, and 10 (2.0%) without any family members.
Finally, for a question on residential areas, 203 people said they were living in metropolitan areas, accounting for 40.6%. People living in rural areas were 297 (59.4%) (Table 2).
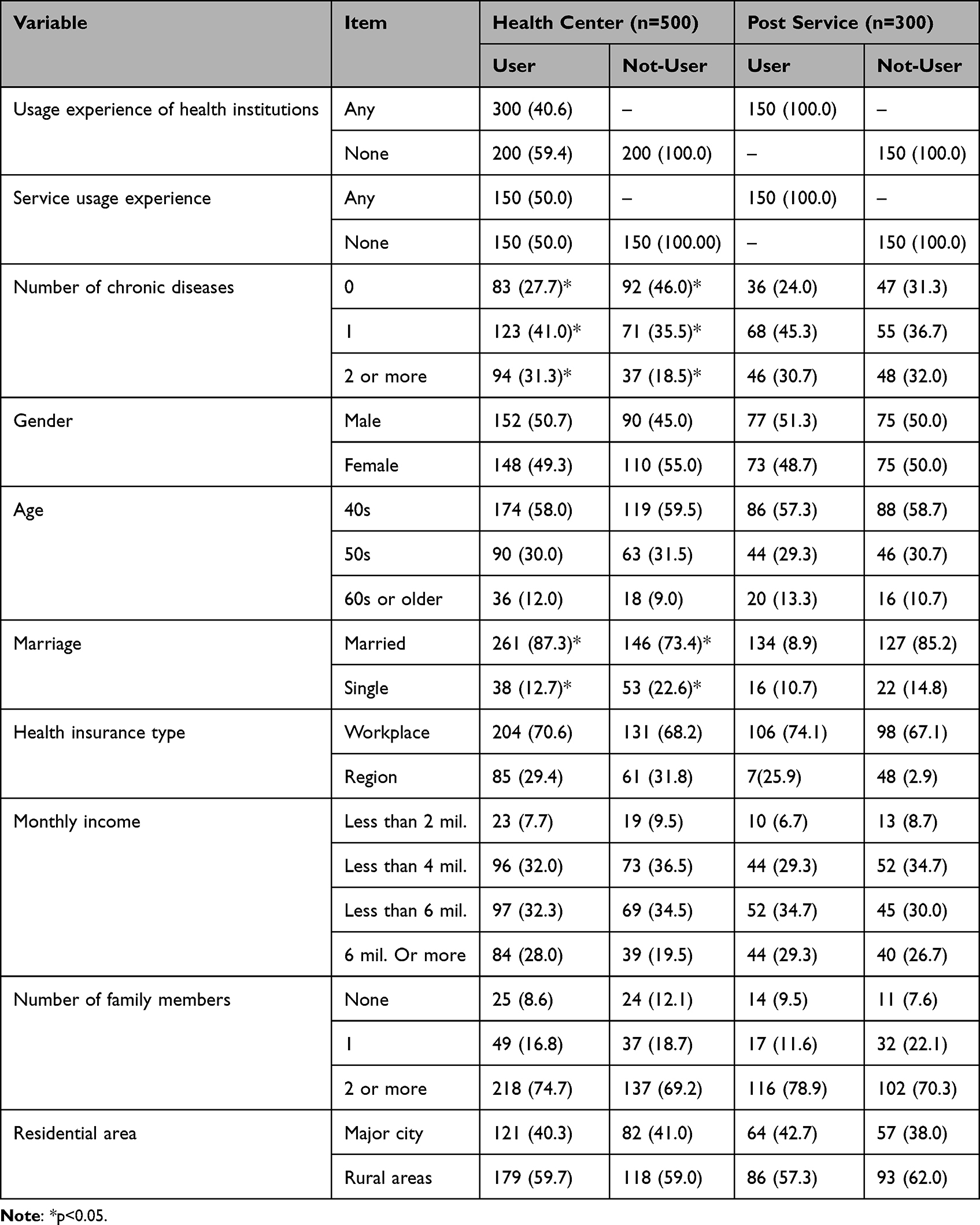 |
Table 2 Socio-Demographic Properties of Study Subjects (Unit: Persons, %) |
Mean Difference Analysis Based on Usage Experience Regarding Public Health Centers
Regarding the performance of health checkup result-related data-linked post-services of regional health and medical institutions, the mean difference was analyzed based on experience of using regional health and medical institutions and health checkup result-related data-linked post-services. Consequently, the results showed that those (3.13) who had experience in using regional health and medical institutions were more deeply aware of the need for post-services than those (2.93) who did not have such experiences. This represented a statistically significant value at the 95% confidence level. Furthermore, those who had experience in using regional health and medical institutions had an average of 2.11 chronic diseases, thus showing a statistically significant difference compared to the average number (1.75) of chronic diseases that people without experience were found to have.
However, it was found that those (3.03 and 3.06, respectively) who had no experience in using regional health and medical institutions had better health status—a year ago (3.27) and at present (3.26)—than those who had such experience. This indicated that the users of regional health and medical institutions belonged to many social brackets that were relatively vulnerable in terms of health (Table 3).
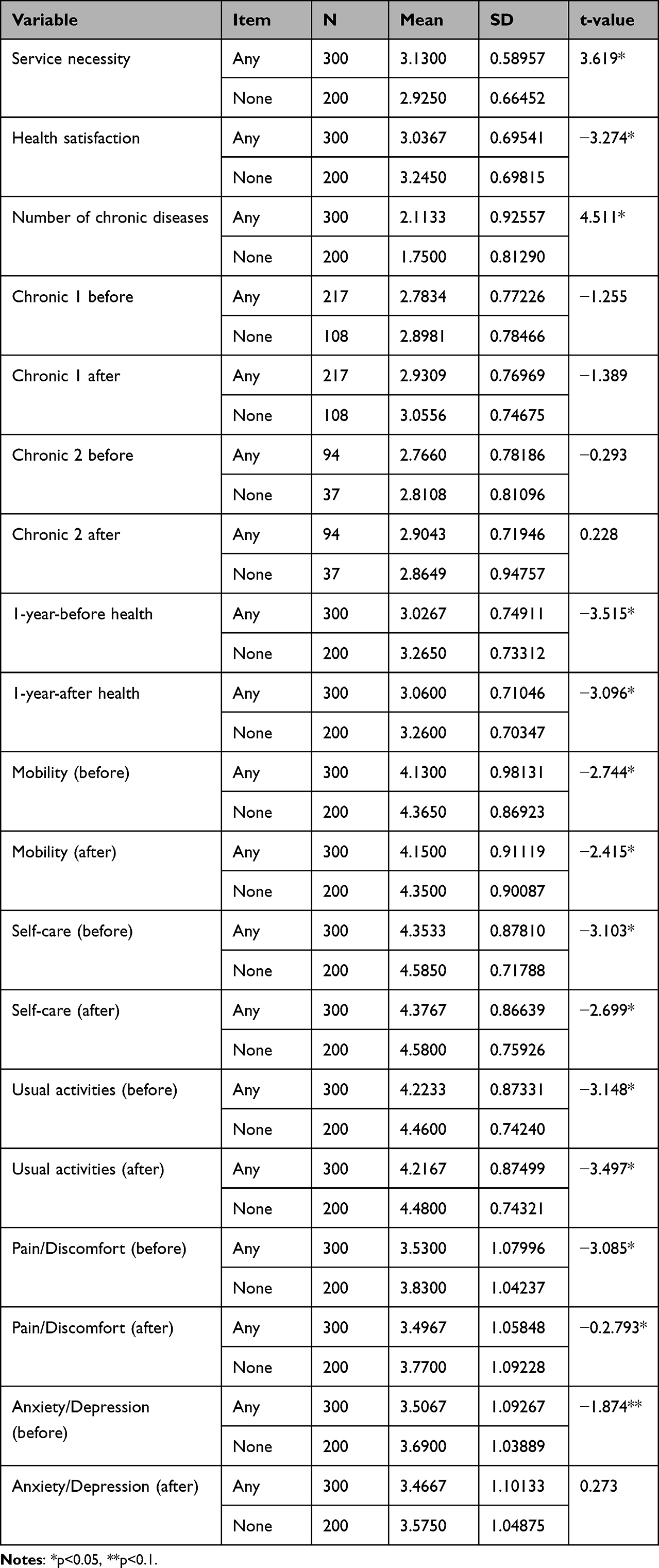 |
Table 3 Mean Difference Analysis Based on the Experience of Using Health and Medical Institutions |
Furthermore, in terms of health-related quality of life indicators (eg, mobility, self-care, usual activities, and pain/discomfort), those who had no experience in using health and medical institutions perceived themselves as being healthier—a year ago and during the survey—compared to those who had such experience. This suggests a statistically significant difference between the two camps. Moreover, regarding anxiety/depression, they exhibited no differences at the perception level regardless of whether they had the usage experience. That is, those who used anxiety/depression healthcare services had a mean of 3.47, while those who had no such experience reported a mean of 3.58, thus suggesting no statistically significant difference between the two camps.
Regarding the anxiety/depression for one year, those (3.51) who had experience in using public health centers were slightly fewer in number than those (3.69) who had no experience in using them, thus indicating no difference between the two. Those who used public health centers may experience greater emotional stability after visiting these centers. This feeling is based on certain psychological factors, which are roused by the service users’ sense of relief that they are being protected by a regional health and medical institution.
More specifically, the study examined the differences in perceptions of health status among those with experience using health and medical institutions and those without it. First, those with experience in using public health centers acknowledged that a chronic disease they were suffering from had improved to some extent in the present (2.93) than one year ago (2.78), owing to public health centers. Moreover, questions assessing health-related quality of life found no statistically significant difference based on experience of using public health centers (Table 4).
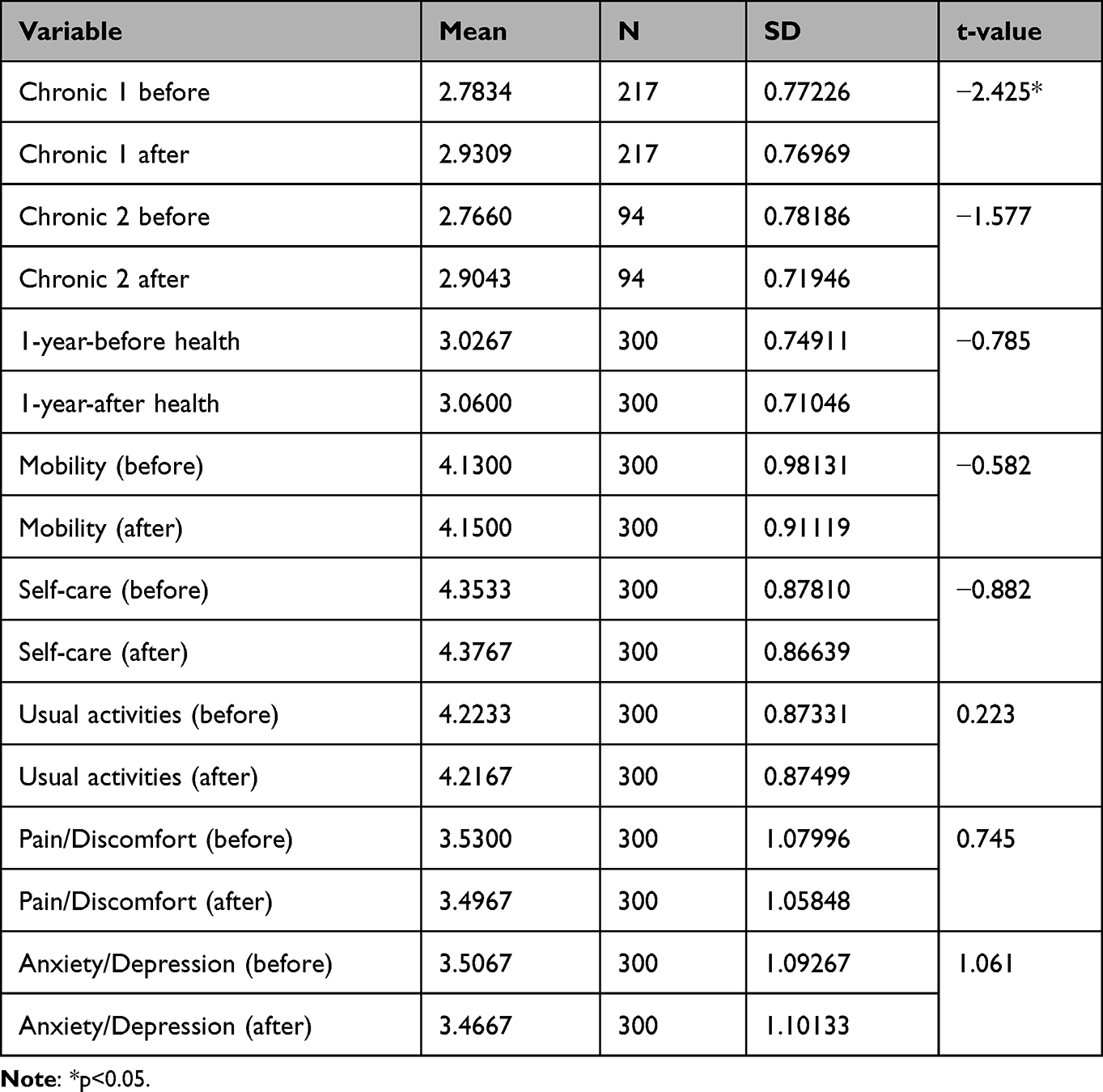 |
Table 4 Mean Difference Analysis in the Health Status of Users of Health and Medical Institutions |
However, those who did not use health and medical institutions perceived that a chronic disease they suffered from had been improved compared to a year ago, whereas their degree of anxiety/depression worsened compared to what it had been a year ago (3.69). Both showed a statistically significant difference. It is judged that the provision of public health center and health data-linked services has the effect of reducing the anxiety and depression of local residents (Table 5).
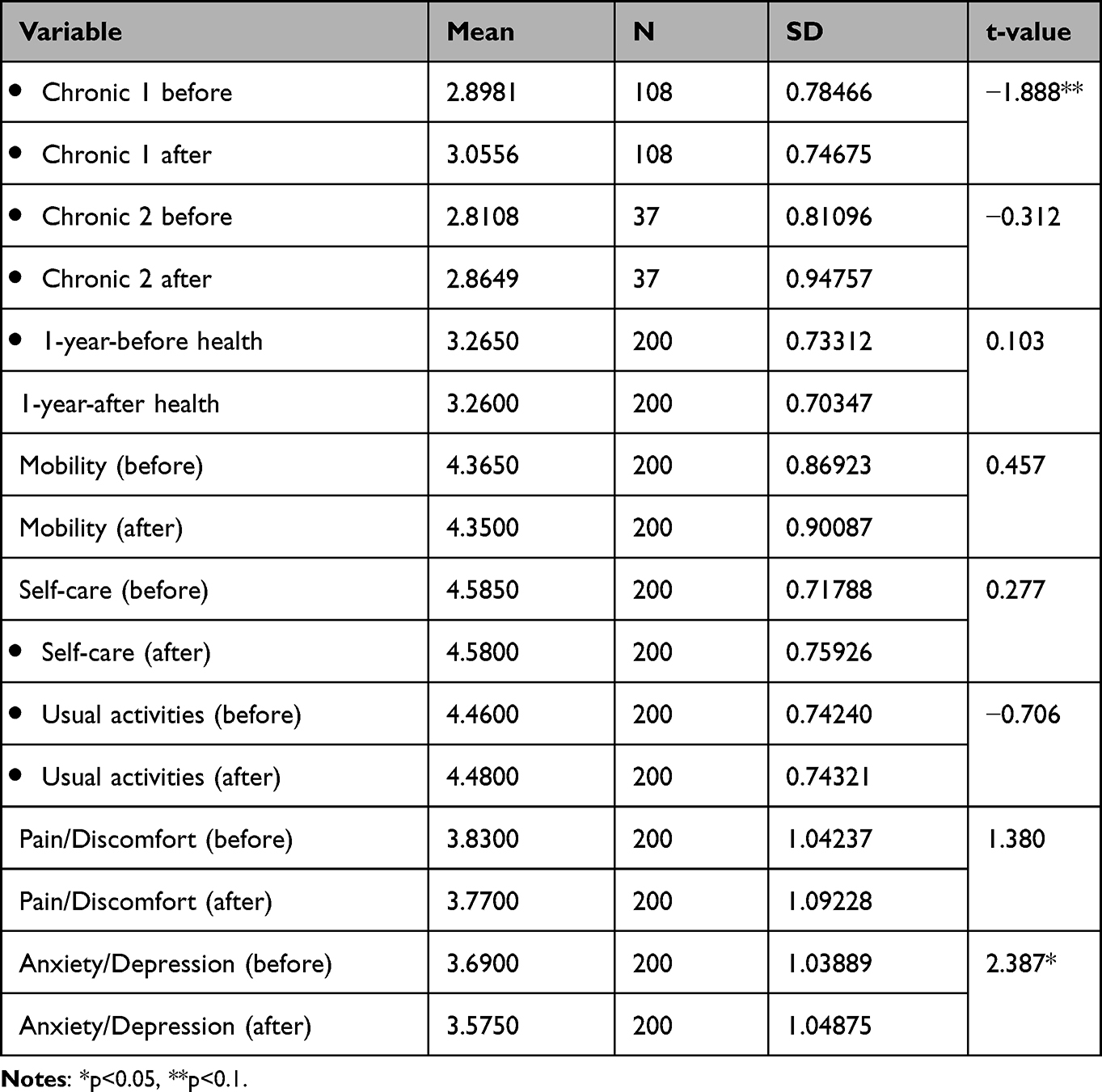 |
Table 5 Mean Difference Analysis of the Health Status of Non-Users of Health and Medical Institutions |
Mean Difference Analysis Based on Experience of Using Data-Linked Post-Services
Next, we investigated differences with regard to health awareness levels based on whether participants had experience in using health checkup result-related data-linked post-services. Regarding “one-year-ago” health status, those with no experience in using such services appeared to have a mean of 3.05; this finding suggested that they perceived themselves to be healthier than those (2.95) who had experience in using such services. Furthermore, regarding the questions on health-related quality of life, those who had no experience in using such services (in terms of mobility, self-care, and usual activities) perceived themselves to be healthier than those who had experience in using such services. These findings suggested a statistically significant difference.
However, those (3.04) who used the service as well as the information guide on their chronic diseases through the health checkup result-related data-linked post-services recognized that their own chronic diseases had improved compared to those (2.81) who did not use the services. This indicated that their chronic diseases had improved through the post-services. Therefore, the health checkup result-related data-linked post-services could be considered to be effective in improving chronic diseases (Table 6).
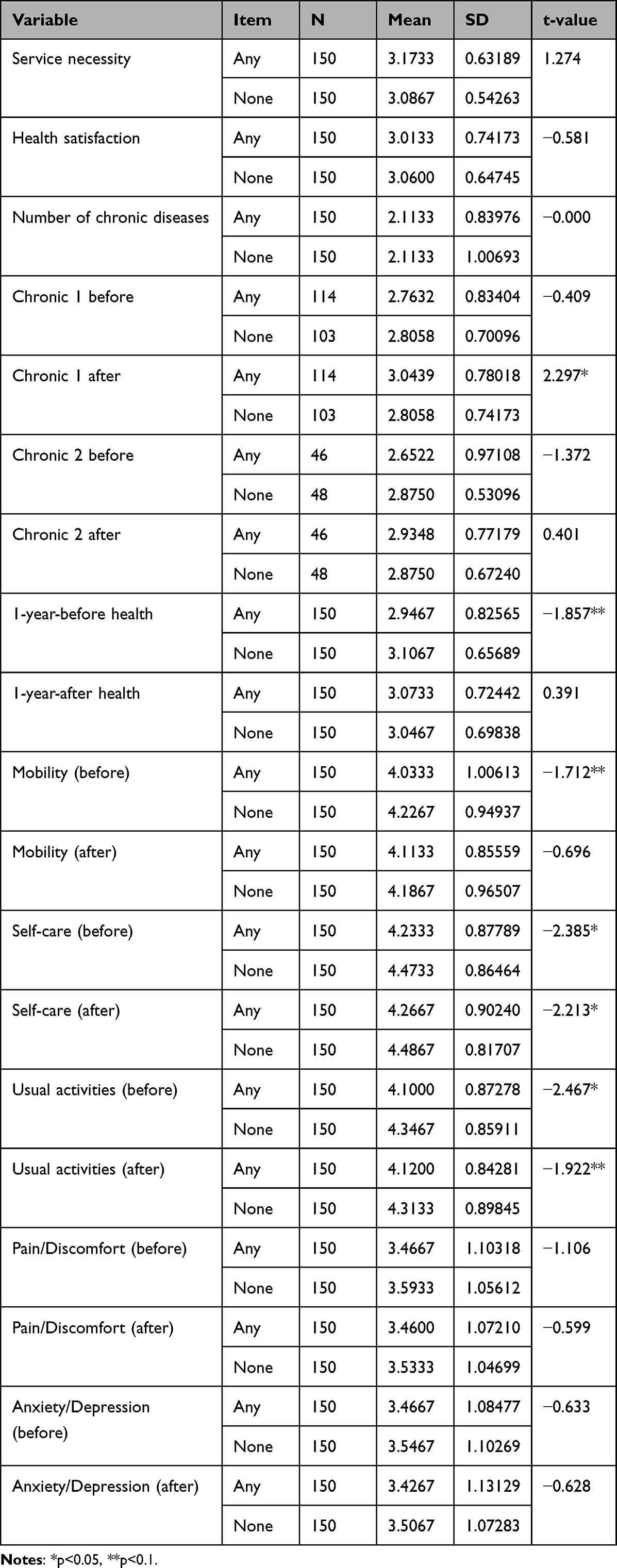 |
Table 6 Mean Difference Analysis Based on Usage Experience of the Post-Services |
More specifically, a comparison of the health improvement levels of those who used the health checkup result-related data-linked post-services with that of the non-users indicated the effectiveness of the post-services. In other words, those who experienced using the post-services recognized that one or two of their chronic diseases had improved compared to those who did not use these services. Furthermore, they perceived an improvement in their current health status (3.07) compared to their “one-year-ago” health status (2.95). This showed a statistically significant difference between those who used these services and those who did not. However, they recognized that there had been no improvement in their health-related quality of life compared to their “one year ago” health-related quality of life status (Table 7).
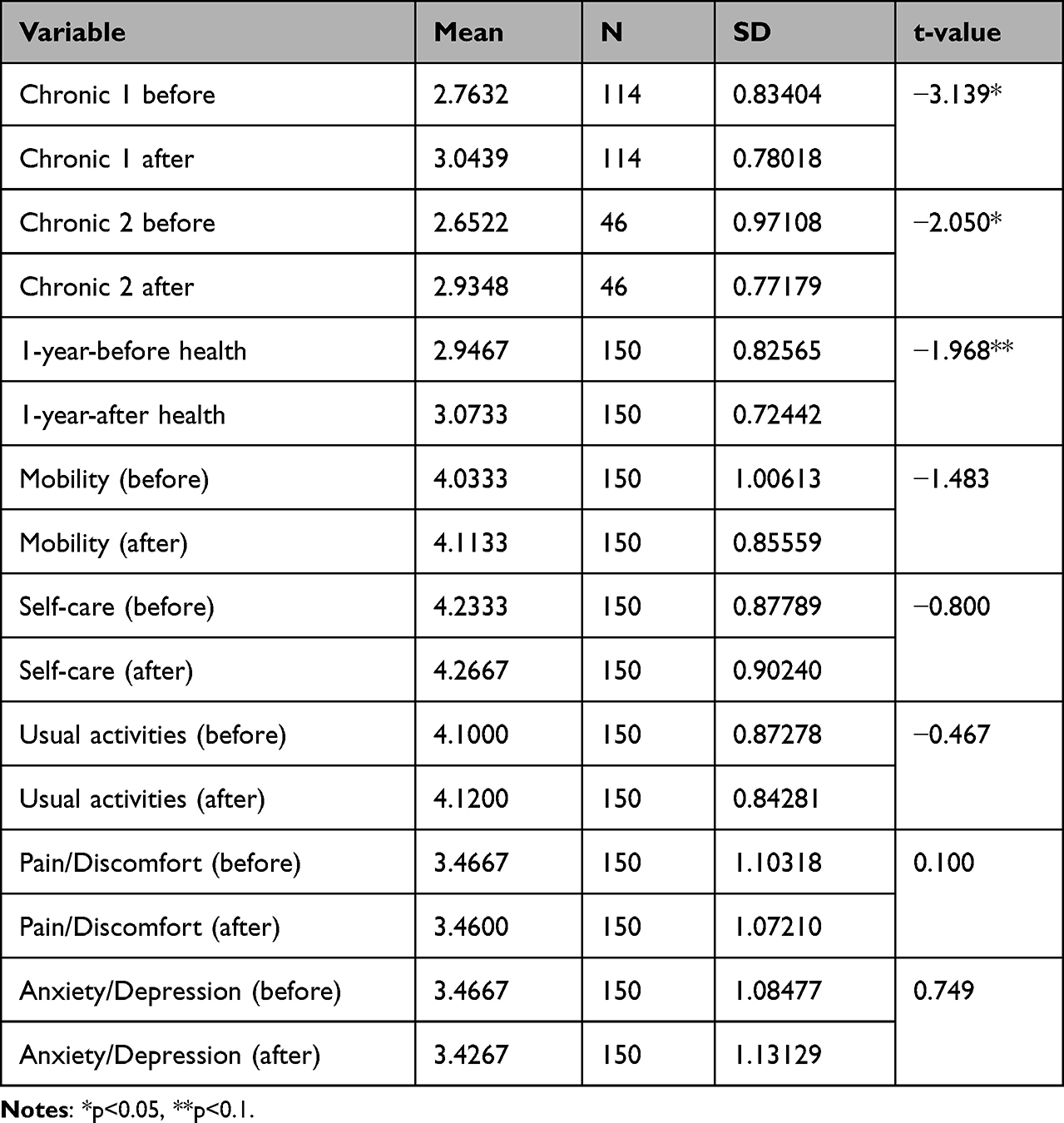 |
Table 7 Mean Difference Analysis with Regard to the Health Status of Post-Service Users |
Moreover, those who did not use the health checkup result-related data-linked post-services realized no improvement in any of their chronic diseases, health status, and health-related quality of life compared to their corresponding “one-year-ago” status. In other words, it implies that the health checkup result-related data-linked post-services in regional health and medical institutions were found to have a significant effect on their users. However, it is important to consider linking the service use with various other services (eg, exercise prescriptions, mental health, and so on) from the current focus on chronic diseases so that users’ health-related quality of life can also be improved (Table 8).
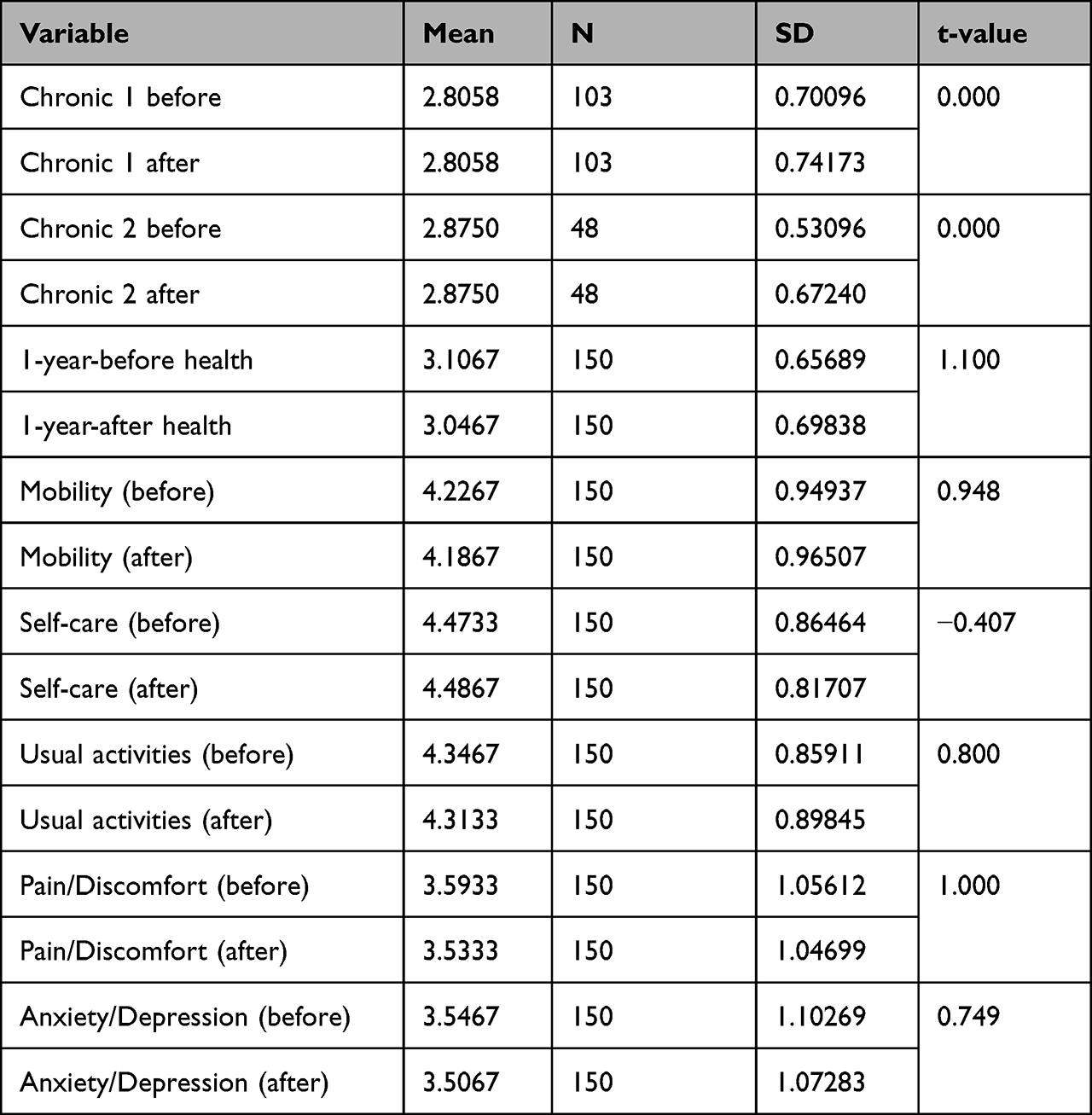 |
Table 8 Mean Difference Analysis in Health Status of Non-Users of Post-Services |
Finally, the differences in health status based on the number of individual users’ chronic diseases were investigated. The numbers of such chronic diseases were classified into cases of 0, 1, and 2 or more. First, regarding health satisfaction, a higher number of chronic diseases was perceived as indicating a worse level of health, thus suggesting a statistically significant difference. Furthermore, regarding awareness of “one-year-ago” health status, those suffering more chronic diseases perceived their health to be worse (Table 9).
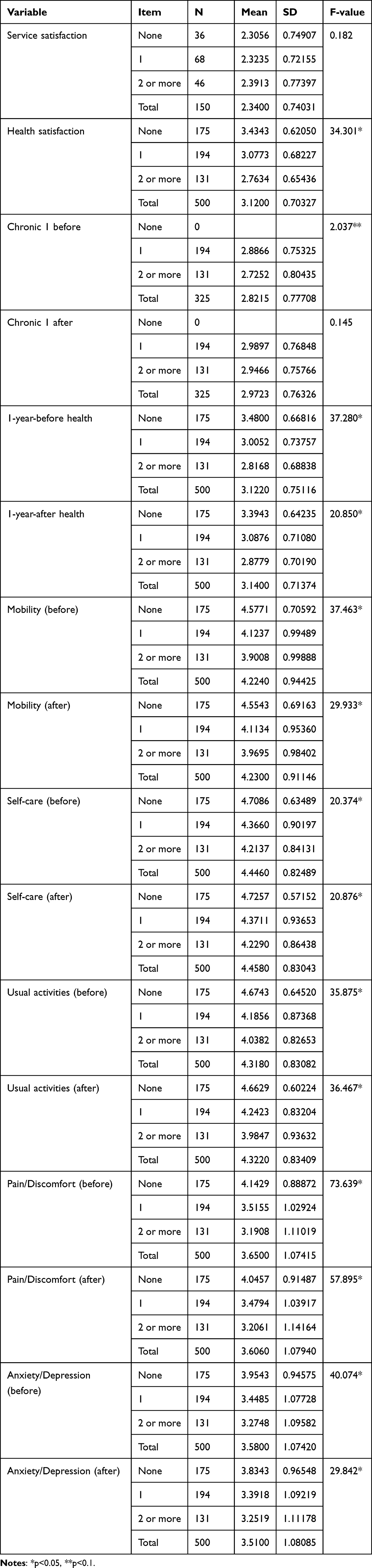 |
Table 9 Mean Difference Analysis Based on the Number of Chronic Diseases |
In terms of the health-related quality of life, as the number of chronic diseases increased in the one-year-before mobility, current usual activities, and one-year-before and current pain/discomfort, they perceived their health as worse. Moreover, with regard to current mobility, one-year-ago and current self-care, one-year-ago usual activities, and one-year-ago and current anxiety/depression, it was found that those without chronic diseases were healthier compared to those with one or more chronic diseases. This indicates a statistically significant difference between the two camps. In other words, it suggests that those who did not have chronic diseases perceived better health than those who had chronic diseases.
More specifically, we investigated the difference regarding the “one-year-ago” status and current awareness of health status between those who had two or more chronic diseases. Those with two or more chronic diseases perceived their current condition (2.95) to have improved compared to what it was year ago (2.73) in the case of at least one chronic disease. The health status of those with one chronic disease improved in terms of usual activities compared to what it had been one year ago. That is, it had improved from 4.19 one year ago to 4.24 at present, thus suggesting a statistically significant difference. Those without chronic diseases perceived that their current health status had worsened in terms of health satisfaction, pain/discomfort, anxiety/depression, and so on compared to what it had been one year ago. This indicated that, because the health checkup result-related data-linked post-services from regional health and medical institutions were effective in treating those with chronic diseases, it would be necessary to make efforts to improve health status through the life-cycle management—even for those without chronic diseases (Table 10).
 |
Table 10 Mean Difference Analysis in Health Status Based on the Number of Chronic Diseases |
Discussion
This study analyzed the effectiveness when the local health and medical institutions link the health checkup result data of the National Health Insurance Corporation to the service so as to promote the health of local residents. To measure the effectiveness, the survey subjects were classified according to whether or not they had the usage experience of the public health center, and then among the local residents using the health centers, the subjects were divided and verified according to whether to have used the data-linked service.32
Despite their relatively lower health-related quality of life, those who had experienced the use of public health centers recognized that their chronic diseases had improved than those who had not used. Therefore, they were sympathizing more with the necessity of linking with the health checkup result data of the National Health Insurance Corporation.
Among the public health center users, those who had experienced the use of the health checkup result data-linked services perceived that their health conditions had improved compared to a year ago, particularly where they considered that their chronic diseases were improved. It was found that the health level had been improved when services were provided using the health checkup result data rather than in the case of those who simply used public health centers. Accordingly, the effectiveness of the data-linked service was verified to be valid.33,34
Conclusion
Based on the research results provided, policy recommendations for activating health checkup result-related data-linked post-service in regional health and medical institutions may be examined as follows. First, the project’s effectiveness was ensured if the health checkup data of other institutions were linked and utilized during implementations of health promotion projects in regional health and medical institutions. Accordingly, to link the regional medical information system (PHIS) with other systems, it is necessary to enact or revise certain guidelines. That is, it is necessary to use appropriate guidelines to define the projects that are linkable between systems. Second, project linking of health data in regional health and medical institutions as well as other institutions must be expanded. Furthermore, it is important to utilize it in “visiting health” projects, which directly take services to users, and other projects, beyond the service methods centered on counseling and users’ visits. Third, if health promotion projects in regional health and medical institutions are linked with medical checkup results of the National Health Insurance Corporation, it will be necessary to classify the relevant health levels into various stages to enable customized services. It is difficult to provide services tailored to each subject’s characteristics when only the current information to represent whether a disease can be presented as a medical checkup result is available. Fourth, to enhance the effectiveness of the health checkup result-related data-linked post-service, it is necessary to strengthen education regarding the use of ICT mobile devices so that data can be linked in real time to relevant personnel (eg, visiting nurses, who provide the direct visiting services). Fifth, dedicated manpower is needed to link regional medical information systems (PHIS) with health data of other institutions; therefore, a sufficient project budget must be secured to successfully activate and maintain such data-linked services. Comparable processes of a scale are taking place in People’s Republic of China and Japan providing the developmental mile stones for a large number of LMICs countries across the Global South.1,35,36
Abbreviations
PHIS, Personalized Hospital Information System; EQ-5D-5L, European Quality of Life 5 Dimensions 5 Level Version; ED-5D-3L, European Quality of Life 5 Dimensions 3 Level Version; ICT, Information & Communications Technology; LMIC, Low- and Middle-Income Countries.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We are grateful to the journal editors and anonymous reviewers for their time and helpful comments to improve the paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2021R1I1A4A01057428) and Bio-convergence Technology Education Program through the Korea Institute for Advancement Technology (KIAT) funded by the Ministry of Trade, Industry and Energy (No. P0017805).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Jakovljevic M, Liu Y, Cerda A, et al. The Global South political economy of health financing and spending landscape–history and presence. J Med Econ. 2021;24(sup1):25–33. doi:10.1080/13696998.2021.2007691
2. Jakovljevic M, Sugahara T, Timofeyev Y, Rancic N. Predictors of (in) efficiencies of healthcare expenditure among the leading asian economies–comparison of OECD and non-OECD nations. Risk Manag Healthc Policy. 2020;13:2261. doi:10.2147/RMHP.S266386
3. Dupre ME, Moody J, Nelson A, et al. Place-based initiatives to improve health in disadvantaged communities: cross-sector characteristics and networks of local actors in North Carolina. Am J Public Health. 2016;106(9):1548–1555. doi:10.2105/AJPH.2016.303265
4. Pakhnenko OM, Kulibaba V, Palienko M. Health care provision in state institutions in the context of COVID-19. Health Econom Manag Rev. 2022;3(2):17–25. doi:10.21272/hem.2022.2-02
5. Park G, Yoon K, Lee M. Regional factors influencing non-take-up for social support in Korea using a spatial regression model. SAGE Open. 2021;11(4):21582440211061562. doi:10.1177/21582440211061562
6. Kim J-S, S-H O. Current status of work performance and support plan for public health doctors in the COVID-19 QUARANTINE. J Digital Conver. 2022;20(3):367–376.
7. Young-Woo Seo PC, Young-Hee P. Health care system recognition and influential factors of health care experiences. Korean J Health Serv Manag. 2018;12(4):59–72.
8. Youn H-M, Yun C, Kang SH, et al. A study on regional differences in healthcare in Korea: using position value for relative comparison index. Health Policy Manag. 2021;31(4):491–507.
9. Yoon K, Lee M. Comparative analysis of factors affecting quality of community-based care services in Korea. Int J Environ Res Public Health. 2022;19(8):4641. doi:10.3390/ijerph19084641
10. Min-Jung Kang MSL. Positive relationship between citizens’ perception of community qualities, awareness of community issues, and their sense of community for promoting community health. Korean J Health Educ Promot. 2021;38(5):e012.
11. Sohn J-I, Pillay Y, Alinier G. Current status and challenges for public health care governance in South Korea. Qatar Med J. 2022;2022(9):50–75. doi:10.5339/qmj.2022.50
12. Kaplan RM, Hays RD. Health-related quality of life measurement in public health. Annu Rev Public Health. 2022;43:355–373. doi:10.1146/annurev-publhealth-052120-012811
13. Saigí-Rubió F, Pereyra-Rodríguez JJ, Torrent-Sellens J, Eguia H, Azzopardi-Muscat N, Novillo-Ortiz D. Routine health information systems in the European context: a systematic review of systematic reviews. Int J Environ Research Public Health. 2021;18(9):4622. doi:10.3390/ijerph18094622
14. Zhao Y, Liu L, Qi Y, Lou F, Zhang J, Ma W. Evaluation and design of public health information management system for primary health care units based on medical and health information. J Infect Public Health. 2020;13(4):491–496. doi:10.1016/j.jiph.2019.11.004
15. Sahay S, Nielsen P, Latifov M. Grand challenges of public health: how can health information systems support facing them? Health Policy Technol. 2018;7(1):81–87. doi:10.1016/j.hlpt.2018.01.009
16. Lee M. Comparison of community rehabilitation services for the elderly in South Korea and Japan: focusing on the long-term care insurance system. J Physical Therapy Korea. 2022;29(2):94–105. doi:10.12674/ptk.2022.29.2.94
17. Lim JY, Kim J, Kim S. Case analysis of visiting nursing center for improving efficiencies: based on business management consulting. J Korean Acad Soc Home Health Care Nurs. 2021;28(2):111–123.
18. Park S, Kim H-K, Lee M. An analytic hierarchy process analysis for reinforcing doctor–patient communication. BMC Primary Care. 2023;24(1):1–11. doi:10.1186/s12875-023-01972-3
19. Molella RG, Murad AL, Sherden M, et al. Community health needs assessment data and community recovery from COVID-19. Am J Prev Med. 2022;63(2):273–276. doi:10.1016/j.amepre.2022.02.010
20. Hwang EJ. Comparison of demographic characteristics and health promotion activities among older adults with dementia, older adults with Subjective Mild Cognitive Impairment (MCI), and healthy older adults residence in community. J Korea Acad Industr Cooperat Soc. 2022;23(7):152–160. doi:10.5762/KAIS.2022.23.7.152
21. Lee J, Lee HS, Park Y, Hwang R. An empirical study on tele-consultation in home-visit nursing care setting under Korean long-term care insurance system. J Korean Gerontol Nurs. 2021;23(3):249–260. doi:10.17079/jkgn.2021.23.3.249
22. Yoon K, Lee M. Factors influencing the health satisfaction of users of public health and medical institutions in South Korea. Front Public Health. 2022;10:1079347. doi:10.3389/fpubh.2022.1079347
23. Park S, Yoon K, Lee M. Healthy City Project: an application of data envelopment analysis. Risk Manag Healthc Policy. 2021;14:4991–5003. doi:10.2147/RMHP.S325825
24. Lee Y, Kim E, Lee D. Comparative study on the national health screening programs according to the health insurance system. Health Policy Manag. 2021;31(3):272–279.
25. Ark TK, Kesselring S, Hills B, McGrail K. Population Data BC: supporting population data science in British Columbia. Int J Popul Data Sci. 2019;4(2):1133.
26. Kornelsen J, Carthew C, Míguez K, et al. Rural citizen-patient priorities for healthcare in British Columbia, Canada: findings from a mixed methods study. BMC Health Serv Res. 2021;21(1):1–12. doi:10.1186/s12913-021-06933-z
27. Relova S, Joffres Y, Rasali D, Zhang LR, McKee G, Janjua N. British Columbia’s Index of multiple deprivation for community health service areas. Data. 2022;7(2):24. doi:10.3390/data7020024
28. Park S, Kim H-K, Choi M, Lee M, Kielbassa AM. Factors affecting revisit intention for medical services at dental clinics. PLoS One. 2021;16(5):e0250546. doi:10.1371/journal.pone.0250546
29. Jakovljevic M, Wu W, Merrick J, Cerda A, Varjacic M, Sugahara T. Asian innovation in pharmaceutical and medical device industry–beyond tomorrow. J Med Econ. 2021;24(sup1):42–50. doi:10.1080/13696998.2021.2013675
30. Jakovljevic M. Therapeutic Innovations: The Future of Health Economics and Outcomes Research–Increasing Role of the Asia-Pacific. Taylor & Francis; 2021:(i)–(iii).
31. Sapkota B, Palaian S, Shrestha S, Ozaki A, Mohamed Ibrahim MI, Jakovljevic M. Gap analysis in manufacturing, innovation and marketing of medical devices in the Asia-Pacific region. Expert Rev Pharmacoecon Outcomes Res. 2022;22(7):1043–1050. doi:10.1080/14737167.2022.2086122
32. Park Y, Park S, Lee M. Digital health care industry ecosystem: network analysis. J Med Internet Res. 2022;24(8):e37622. doi:10.2196/37622
33. Jakovljevic M, Sharma T, Kumagai N, Ogura S. NCDs–core challenge of modern day health care establishments. Front Public Health. 2021;9:692926.
34. Jakovljevic M, Jakab M, Gerdtham U, et al. Comparative financing analysis and political economy of noncommunicable diseases. J Med Econ. 2019;22(8):722–727. doi:10.1080/13696998.2019.1600523
35. Jakovljevic MM. Comparison of historical medical spending patterns among the BRICS and G7. J Med Econ. 2016;19(1):70–76. doi:10.3111/13696998.2015.1093493
36. Yoon K, Choi M, Lee M. Policy network analysis the legislation process for medical privatization in Korea. Health Policy Technol. 2022;11(3):100654. doi:10.1016/j.hlpt.2022.100654
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.