Back to Journals » Risk Management and Healthcare Policy » Volume 18
Analyzing Radiation Protection Risks in Nuclear Medicine: Cause Investigation and WSR-Based Countermeasure Evaluation
Received 22 November 2024
Accepted for publication 21 January 2025
Published 4 February 2025 Volume 2025:18 Pages 329—337
DOI https://doi.org/10.2147/RMHP.S508013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Peng Sun,1 Guanting Li,2 Yunhe Zhu1
1Department of Nuclear Medicine, Renmin Hospital, Hubei University of Medicine, Shiyan, Hubei, People’s Republic of China; 2Research School of Physics, The Australian National University, Canberra, ACT, Australia
Correspondence: Yunhe Zhu, Email [email protected]
Objective: To analyze and investigate the causes of radiation protection safety risks in nuclear medicine diagnosis and treatment, formulate radiation protection safety management countermeasures, and evaluate their effectiveness.
Methods: In October 2020, the Department of Nuclear Medicine at our hospital established a radiation protection safety management team, utilizing association rules to investigate and analyze the causes of radiation protection safety risks. A Wuli-Shili-Renli (WSR) system management approach was implemented, addressing physical (Wuli), procedural (Shili), and human factors (Renli) to improve technical safeguards, optimize processes, and enhance personnel awareness. A total of 1200 patients receiving diagnosis and treatment were divided into two groups. The control group (600 cases) used standard inspection-based radiation protection, while the observation group (600 cases) adopted WSR system management in addition to standard measures. Radiation protection risk control effectiveness and safety control capability scores were compared between the two groups.
Results: The proportions of excessive diagnostic doses and additional radiation harm in the observation group were both lower than those in the control group (P < 0.05); the proportions of risk sources, including building environment, protective measures, dose monitoring, safety awareness, and waste disposal, in the observation group were all lower than those in the control group (P < 0.05). The observation group’s scores in radiation protection theory, practical risk management skills, and radiation protection safety literacy, as well as the total score, were higher than those of the control group (P < 0.05).
Conclusion: The WSR system management approach effectively reduces radiation protection safety risks, improves the diagnostic and therapeutic environment, minimizes radiation exposure to patients and staff, and enhances safety risk management levels in nuclear medicine departments.
Keywords: nuclear medicine, radiation protection, radiation safety, risk management, safety management, association rule learning, Wuli-Shili-Renli framework
Introduction
Nuclear medicine, as an important and rapidly developing branch of modern medicine, is widely applied in the diagnosis and treatment of clinical diseases, with its core technology relying on the use of radioactive drugs.1 The greatest advantage of nuclear medicine technology is its ability to achieve early detection and precise diagnosis of diseases through functional imaging techniques, as well as to utilize specific radioactive isotopes for targeted therapy.2 However, this advantage comes with the challenge of extensive radiation use, leading to exposure risks for patients, medical staff, and the environment. As a result, radiation safety protection has become one of the critical and challenging issues in the field of nuclear medicine.3 How to effectively reduce the potential health hazards of radiation while improving clinical diagnostic and therapeutic effects has become a key issue in nuclear medicine that needs to be urgently addressed.
During nuclear medicine diagnosis and treatment, radioactive drugs are introduced into the patient’s body via intravenous injection or other means. These radioactive substances distribute within the patient’s body and undergo decay, thereby producing diagnostic images or therapeutic effects.4 However, the use of radioactive substances inevitably carries radiation risks. Patients directly come into contact with the radiation source during treatment, and if the radiation dose is not properly controlled or the operational procedures are not rigorously followed, the patient may be exposed to radiation beyond the safe range, adversely affecting their health.5 Additionally, the medical staff in the nuclear medicine department, who are in long-term contact with radioactive substances, face the threat of occupational radiation exposure.6 Radioactive substances may also spread into the diagnostic environment through waste, excreta, and air, potentially affecting the surrounding environment and unrelated personnel.7 Controlling radiation exposure is crucial during nuclear medicine examinations and treatments. In this context, “radiation dose” refers specifically to the administered activity (measured in MBq), which plays a critical role in achieving accurate diagnostic imaging or therapeutic effects while minimizing unnecessary radiation exposure. However, in clinical practice, administered activities sometimes exceed recommended levels due to patient-specific variations or improper handling by medical personnel. Additionally, medical staff involved in the preparation and administration of radioactive drugs may lack sufficient awareness of radiation hazards. Combined with inadequate adherence to protective protocols, this oversight further heightens the risk of occupational exposure. The architectural design, equipment configuration, and completeness of protective facilities in nuclear medicine departments also directly affect the effectiveness of radiation protection; unreasonable layouts or insufficient shielding measures may lead to radioactive substance leakage, impacting the surrounding environment. Additionally, the daily generation of various types of radioactive waste poses potential threats to the environment and public health if not properly disposed of according to regulations. For this reason, the International Commission on Radiological Protection (ICRP)8 and medical regulatory bodies in various countries have established strict standards for radiation protection in nuclear medicine, covering aspects such as radiation dose limits, individual protective measures, and radioactive waste disposal. However, due to insufficient awareness among medical staff and varying levels of technical proficiency, there are still instances of inadequate protection in practice.
Traditional radiation protection in nuclear medicine mainly relies on regular inspections and basic technical measures for risk control, but this method is rather fragmented and difficult to form a comprehensive safety management system.9 To more effectively address the complex issues in radiation protection in nuclear medicine, systematic management thinking has gradually become a research focus in recent years. The Wuli-Shili-Renli (WSR) system10 management method has emerged as a new tool for enhancing radiation protection management levels in nuclear medicine. The WSR model builds a complete protection management framework from three dimensions: physical environment, operational processes, and personnel management. Physical management focuses on the optimization of equipment and environment in the nuclear medicine department; operational management emphasizes the establishment and enforcement of procedural norms; and personnel management aims at improving training and raising awareness of protection among staff. This multidimensional management model ensures that every aspect of nuclear medicine diagnosis and treatment is under effective control, thereby achieving better radiation protection results.
This study aims to identify the key risk factors in radiation protection using association rule analysis and to evaluate the effectiveness of the WSR management framework in improving radiation safety. By providing a multidimensional strategy, this research seeks to contribute to the advancement of safety standards in nuclear medicine, benefiting both patients and healthcare providers.
Materials and Methods
Study Design
This study is a retrospective comparative analysis conducted to evaluate the effectiveness of WSR-based radiation protection management in nuclear medicine. It compares two cohorts treated between January 2020 and February 2024. According to the different radiation protection safety management methods for patients and the medical staff involved in their diagnosis and treatment, 600 patients treated from January 2020 to December 2021 were included in the control group (where radiation protection safety of patients and medical staff was managed through regular detection), and 600 patients treated from January 2022 to February 2024 were included in the observation group (where radiation protection safety of patients and medical staff was managed using the WSR system). All patients provided informed consent for the study and signed relevant informed consent forms. The content of this study was reviewed and approved by the Renmin Hospital, Hubei University of Medicine ethics committee. All the methods were carried out in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Inclusion criteria: ① Complete clinical diagnosis and treatment data; ② Patients aged >35 years and <70 years, with no gender restriction. Exclusion criteria: ① Patients with interruptions during examination or treatment; ② Patients undergoing other medical imaging examinations and radiation therapy projects during examination or treatment.
Methods
Control Group
Patients in the control group received conventional radiation protection management. This involved compliance with national regulations, regular monitoring of equipment, building safety, and environmental radiation doses. Identified risks were addressed promptly, especially in high-risk areas.
Dose Monitoring Records: These records included administered radioactive activity, dose rates from patients, and environmental radiation levels.
Observation Group
The observation group adopted a WSR (Wu Li, Shi Li, Ren Li) system management approach, building upon the conventional management used in the control group.
WSR System Overview:
1. Technical (Wu Li)
The Technical dimension of the WSR system focuses on improving the physical infrastructure and environmental factors that contribute to radiation safety. A critical aspect of this dimension is Site Selection. The location of nuclear medicine facilities and diagnostic rooms is carefully chosen to minimize radiation exposure to both staff and patients. Proximity to high-risk areas is minimized, and radiation shielding is strategically planned to provide effective protection. Another key area is Structural Protection. This involves ensuring that the building and facility comply with national radiation safety regulations (eg, GBZ120-2020).11 Structural shielding for walls, doors, and windows is implemented to prevent radiation leakage. Particular focus is placed on high-traffic areas, such as waiting rooms and corridors, which might be near radioactive materials, ensuring that the public and staff are adequately shielded from radiation risks. Personal Protective Equipment (PPE) is another vital component in radiation safety. Adequate protective gear, including lead aprons, thyroid shields, and gloves, is provided to staff and patients. Regular checks are made to ensure the protective equipment is up-to-date and well-maintained, and faulty equipment is replaced promptly to maintain safety standards. In terms of Waste Disposal, proper protocols for handling, storing, and disposing of radioactive waste are established. This includes the use of dedicated containers for radioactive materials, clear labeling of waste, and transportation to secure disposal sites. Staff members are trained in handling radioactive waste safely to reduce the risk of contamination and ensure compliance with safety guidelines. These technical measures are all aimed at improving radiation protection and minimizing exposure risks.12
2. Procedural (Shi Li)
The Procedural dimension of the WSR system focuses on establishing and standardizing processes that minimize radiation exposure risks. One of the primary components is Risk Control Processes. Detailed protocols are developed for every step of the diagnostic and therapeutic process, from patient preparation to post-treatment monitoring. These protocols ensure that radiation exposure is kept within acceptable limits, and any deviations from standard procedures are promptly identified and corrected. Another critical procedural measure is Patient Treatment Schedules. Optimizing the scheduling of patient treatments is a strategy to minimize cumulative radiation exposure. High-risk procedures are scheduled during low-traffic periods to limit exposure, while treatment plans are structured to reduce unnecessary repeat scans or therapies, ensuring that radiation exposure is minimized. Radiation Monitoring is a key part of the procedural approach, where regular audits and monitoring of radiation exposure levels are conducted to ensure compliance with safety standards. This includes checks of environmental radiation levels, personal dose monitoring for staff, and measurement of patient exposure during procedures. If anomalies are detected, they are addressed immediately to maintain safe working conditions. Additionally, Compliance Audits are performed regularly to ensure that radiation safety protocols are being adhered to. Internal and external audits help identify any non-compliance issues, and corrective actions are swiftly taken to align the system with safety standards. These measures ensure that procedural steps are continuously followed to mitigate radiation exposure risks.13
3. Human Factors (Ren Li)
The Human Factors dimension of the WSR system focuses on the importance of training, safety culture, and adherence to protocols among the staff. One key component is Staff Training, where regular programs are implemented to ensure that all staff members are updated with the latest radiation safety practices. These training sessions cover the proper use of personal protective equipment (PPE), handling of radioactive materials, and emergency procedures in case of a radiation spill or exposure incident. Building a Safety Culture is another integral element of the human factors approach. The team emphasizes the importance of vigilance and reporting of potential safety hazards. A safety-conscious environment is fostered where staff feel a shared responsibility for each other’s safety. Employees are encouraged to participate in safety initiatives and contribute to process improvements, ensuring a proactive approach to safety. Finally, the system ensures Adherence to Protocols through continuous education and periodic assessments. Regular drills and reminders reinforce the importance of following established safety guidelines to minimize radiation exposure. The team also uses the PDCA (Plan-Do-Check-Act)14 cycle to continuously improve radiation protection practices, fostering an environment where feedback is integrated into ongoing risk management and safety protocols. This iterative process helps ensure that staff continuously improve their skills and knowledge, ensuring the safety of all stakeholders.14
Management Framework: In October 2020, the hospital’s Department of Nuclear Medicine initiated the radiation safety management project. An interdisciplinary team was formed, including experts in radiation quality control, nuclear medicine technicians, physicians, engineers, nurses, and IT specialists. Their responsibilities and goals are detailed in Appendix A.
Observation and Evaluation Indicators
(1) Safety risk control effects: Including both risks and risk sources, the proportion of 600 patients in each group who experienced excessive radiation dosage, and the proportion of medical staff or patients’ family members exposed to additional radiation, were recorded. The proportion of risk sources related to the building environment, protective measures, dose monitoring, safety awareness, and radioactive medical waste disposal was also calculated. Trigger levels for radiation dose were defined as exceeding 20 mSv/year for staff or local reference levels for patients.
Non-compliance metrics included incomplete protective measures or deviations from standard operating procedures.
(2) Safety risk control ability: This refers to the assessment scores of medical staff’s theoretical knowledge of radiation protection, practical risk management ability, and radiation protection safety literacy. The hospital conducted assessments in June each year. The assessment consisted of three components with the following point allocation: 30 points for theoretical knowledge of radiation protection, 50 points for practical risk management ability, and 20 points for radiation protection safety literacy, totaling 100 points. Each component was evaluated using a specific set of criteria, including (1) theoretical knowledge assessments through written tests or quizzes, (2) practical risk management evaluated through simulated scenarios or case studies, and (3) safety literacy based on adherence to protocols and participation in safety-related activities. A higher score indicates a greater level of competence in radiation protection and safety management.
Statistical Analysis
Data were processed using SPSS 22.0 software. Count data were expressed as percentages (%), and analyzed with the χ²-test; measurement data were expressed as ( ) and compared using independent sample t-tests or paired t-tests. A P value of <0.05 indicated statistically significant differences.
) and compared using independent sample t-tests or paired t-tests. A P value of <0.05 indicated statistically significant differences.
Results
Example of Radiation Protection Safety Risk Data Assignment in Nuclear Medicine Diagnosis
To systematically quantify and analyze radiation safety risks in nuclear medicine diagnostics, the project team conducted data preprocessing and assignment. Preprocessing involved cleaning, standardizing, and converting raw data to ensure completeness and consistency, including addressing missing values, removing inaccuracies, consolidating duplicates, and protecting personal information. In the assignment stage, qualitative data, such as the presence of safety risks, were coded as “1” for “yes” and “0” for “no”, while quantitative data, like the frequency and duration of risks, were recorded as actual values and normalized for uniformity. This structured approach ensured the data’s reliability and suitability for analyzing trends and informing radiation safety management strategies (Table 1).
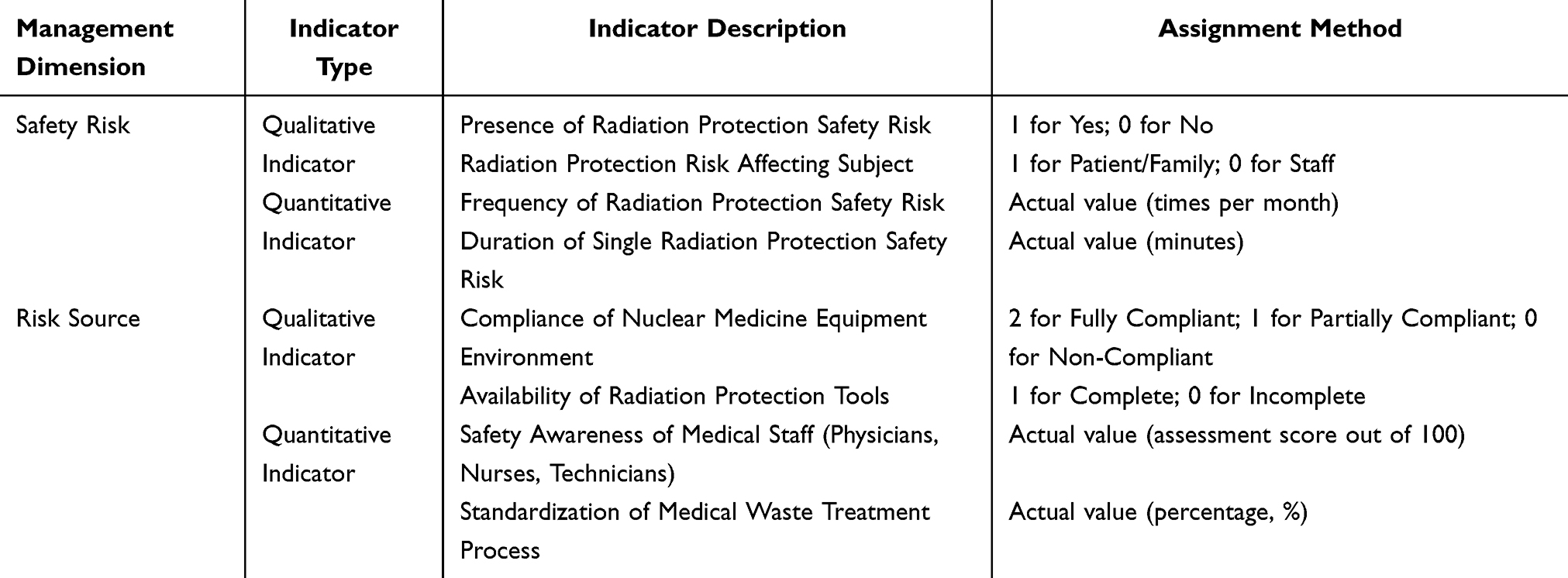 |
Table 1 Example of Radiation Protection Safety Risk Data Assignment in Nuclear Medicine Diagnosis |
Classification of Radiation Protection Safety Risk Management Levels in Nuclear Medicine Diagnosis
To ensure an effective and structured approach to managing radiation protection safety risks, the project team classified risks into six levels based on metrics such as support, confidence, and lift (L). These metrics were derived through association rule analysis, with support reflecting the frequency of a risk factor, confidence indicating its likelihood of leading to a safety issue, and lift (L) demonstrating the strength of the association between a risk factor and its source. Risk levels range from high risk, requiring immediate corrective action, to no risk, allowing for the continuation of normal operations. Table 2 provides a detailed overview of the classification criteria and corresponding management plans.
 |
Table 2 Classification of Radiation Protection Safety Risk Management Levels in Nuclear Medicine Diagnosis |
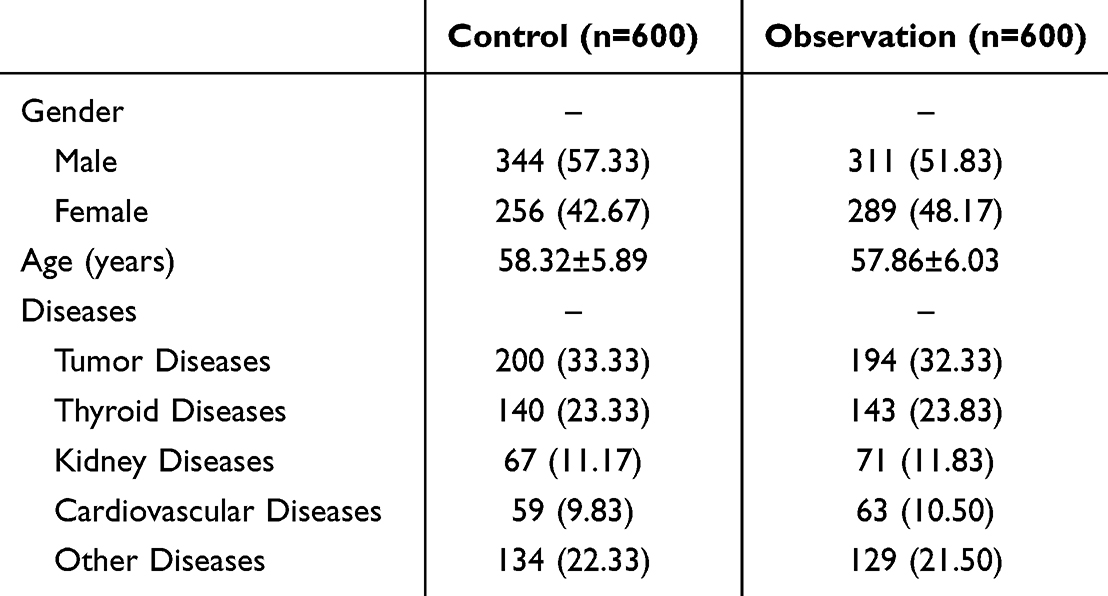
Comparison of Basic Data
There were no statistically significant differences in the basic data of the patients, the medical staff involved, and the equipment used between the two groups (P>0.05). The basic information of the patients is shown in Table 3 below.
 |

Comparison of the Safety Risk Control Effects of Radiation Protection in Nuclear Medicine Between the Two Groups
The proportions of patients in the observation group with excessive diagnostic dosages and additional radiation exposure were lower than those in the control group (P<0.05). The proportions of risk sources related to the building environment, protective measures, dose monitoring, safety awareness, and waste disposal were also lower in the observation group than in the control group (P<0.05), as shown in Table 4 below.
 |
Table 4 Comparison of the Safety Risk Control Effects of Radiation Protection in Nuclear Medicine Between the Two Groups (n [%]) |
Comparison of the Safety Risk Control Ability Scores of Radiation Protection in Nuclear Medicine Between the Two Groups
The scores for theoretical knowledge of radiation protection, practical risk management ability, radiation protection safety literacy, and the total scores of medical staff in the observation group were all higher than those in the control group (P<0.05), as shown in Table 5 below.
 |
Table 5 Comparison of the Safety Risk Control Ability Scores of Radiation Protection in Nuclear Medicine Between the Two Groups ( |

Discussion
The rapid development of nuclear medicine diagnostic and therapeutic technologies has provided irreplaceable tools for the diagnosis and treatment of clinical diseases, particularly in the fields of cardiovascular diseases, oncology, and neurology, where their application value is increasingly prominent.15,16 However, despite the rapid development of nuclear medicine departments in many medical institutions in China in recent years, there remain significant deficiencies in radiation protection management systems. These shortcomings are primarily due to the late development of nuclear medicine in the country, the technical complexity involved, and the substantial capital investments required. Specifically, the execution of relevant standards and implementation of supporting systems remain inconsistent, unsystematic, and insufficiently refined.17 These challenges make it easier for radiation protection safety management in nuclear medicine departments to develop vulnerabilities, leading to unnecessary radiation exposure for patients, medical staff, and the surrounding environment.
The diagnostic and therapeutic application of radiopharmaceuticals in nuclear medicine inevitably exposes patients to certain levels of radiation. Although most medical institutions have relatively strict operational protocols to control the activity of radiopharmaceuticals administered (measured in MBq), there are no specific regulatory mandates for the radiation dose (measured in rem) that patients may receive.18 Dose overexposure, therefore, can occur due to various factors, including equipment aging, operator error, or suboptimal environmental layouts. Moreover, incorrect administration—such as delivering the wrong radiopharmaceutical, to the wrong patient, by the wrong route, or with the wrong activity—can significantly contribute to radiation overexposure risks. While this study primarily focuses on systemic and operational risk factors, these additional causes should be considered in future investigations.19
Physical space protection measures in nuclear medicine departments, such as shielding walls, ventilation systems, and waste disposal facilities, are critical in mitigating risks. However, inadequate design or maintenance of these facilities can increase the likelihood of radioactive substance leakage, posing potential threats to hospital personnel and public health. To better control radiation protection risks in nuclear medicine diagnostics, association rule algorithms were used to systematically analyze risk sources. This technology identifies various potential risk factors in radiation protection and reveals their internal relationships. Compared to traditional risk assessment methods, association rule algorithms mine hidden patterns and trends from large and complex management data, providing managers with more targeted protective strategies.20 Through this analytical method, hospitals can clearly identify major loopholes in the daily management of nuclear medicine departments—such as untimely equipment maintenance, non-standard operating procedures, and improper waste disposal—and provide scientific evidence for optimizing radiation protection.
In the practice of radiation protection management, the WSR (Wuli-Shili-Renli) system management method offers a new, multi-dimensional framework for addressing issues in nuclear medicine departments. Compared to traditional methods of regular inspections and supervision, WSR system management combines the physical environment, operating procedures, and personnel management, effectively enhancing the overall radiation protection management level through comprehensive measures. The physical facilities of the nuclear medicine department form the foundation of radiation protection. WSR system management ensures the standardization of building layouts, equipment protection, and radiation source control. For example, regular inspections and maintenance of the shielding performance of radioactive equipment ensure that radioactive substances are effectively contained in designated areas, reducing their impact on the surrounding environment and personnel.21 Shili management emphasizes optimizing management systems and operational procedures. WSR system management establishes comprehensive systems and standardized operating procedures to ensure systematic execution, reducing radiation overexposure caused by human error. Additionally, it includes the standardization of radioactive waste disposal to ensure the safe and effective handling of radioactive substances. Renli management focuses on improving medical staff’s radiation protection awareness and operational skills. By organizing regular radiation protection training, WSR system management enhances staff proficiency in using protective equipment and following operational standards, thereby reducing occupational exposure risks.22
The application of WSR system management in nuclear medicine radiation protection has demonstrated significant advantages. Research data indicate that the observation group utilizing WSR system management outperformed the control group using traditional management methods across all aspects of radiation protection. Specifically, WSR system management effectively reduced radiation overexposure and unnecessary radiation injuries during diagnostics and treatments. Improvements in building environments and protective facilities also significantly reduced the impact of radioactive substances on external environments.23 Furthermore, WSR system management substantially improved the radiation protection capabilities and risk management levels of medical staff. Systematic training and assessments enabled the observation group to achieve higher scores in theoretical knowledge, operational skills, and safety awareness than the control group, highlighting the importance of personnel coordination in ensuring radiation protection. Additionally, the overall safety management level of nuclear medicine departments was significantly enhanced, with fewer management loopholes and greater diagnostic safety.24
Despite these achievements, there are areas for improvement. As nuclear medicine technology continues to advance, new radiopharmaceuticals and equipment emerge, requiring updated protective management strategies. WSR system management should further integrate intelligent technologies, such as big data analysis and AI-assisted diagnostics, to enhance efficiency and precision in radiation protection. Additionally, cultivating a strong culture of radiation protection is critical to making safety awareness a norm for all staff, ultimately achieving comprehensive and sustainable safety management goals.
Conclusion and Limitations
This study systematically analyzed radiation protection risks in nuclear medicine diagnostics and treatments, using association rule analysis to identify key risk factors and proposing WSR system management as a countermeasure. The results demonstrated that WSR system management effectively reduces safety risks, enhances the radiation protection knowledge and skills of medical staff, and improves the diagnostic environment by lowering radiation exposure for patients and staff. Compared to the widely known Plan-Do-Check-Act (PDCA) cycle, the WSR methodology offers a more holistic framework that integrates physical infrastructure, operational procedures, and personnel management, providing multi-dimensional risk control. However, limitations such as sample size, time span, and the lack of integration with advanced technologies like AI and big data must be addressed in future research. By addressing these gaps, the WSR methodology can be further refined to advance radiation safety in nuclear medicine and offer a model for other healthcare domains.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mankoff D. The future of nuclear medicine. J Nucl Med. 2023;64(9):1329–1330. doi:10.2967/jnumed.123.266448
2. Gonzalez-Montoro A, Vera‐Donoso CD, Konstantinou G, et al. Nuclear-medicine probes: where we are and where we are going. Med Phys. 2022;49(7):4372–4390. doi:10.1002/mp.15690
3. Wagner JB. Radiation Protection and Safety in Interventional Radiology. Radiol Technol. 2020;91(5):431–442.
4. Magrini SM, Pasinetti N, Belgioia L, et al. Applying radiation protection and safety in radiotherapy. Radiol Med. 2019;124(8):777–782. doi:10.1007/s11547-019-01043-7
5. Maina PM, Motto JA, Hazell LJ. Investigation of radiation protection and safety measures in Rwandan public hospitals: readiness for the implementation of the new regulations. J Med Imaging Radiat Sci. 2020;51(4):629–638. doi:10.1016/j.jmir.2020.07.056
6. Thomadsen B. Radiation protection responsibility in Brachytherapy. Health Phys. 2019;116(2):189–204. doi:10.1097/HP.0000000000001005
7. Aizer A, Qiu JK, Cheng AV, et al. Utilization of a radiation safety time-out reduces radiation exposure during electrophysiology procedures. JACC Clin Electrophysiol. 2019;5(5):626–634. doi:10.1016/j.jacep.2018.12.002
8. Rühm W, Clement C, Cool D, et al. Summary of the 2021 ICRP workshop on the future of radiological protection. J Radiol Prot. 2022;42(2):023002. PMID: 35417898. doi:10.1088/1361-6498/ac670e
9. Esfahani AJ, Cheraghi S. Radiation protection evaluation of medical X-ray imaging centers in Qazvin. Iran Health Phys. 2021;121(5):454–462. doi:10.1097/HP.0000000000001453
10. Lang DK, Singh H, Arora A, et al. Radioprotectors: nature’s Boon. Mini Rev Med Chem. 2021;21(20):3074–3096. doi:10.2174/1389557521666210120112814
11. Jian H, Hao H, Haize P, et al. Research on brownfield redevelopment based on Wuli-Shili-Renli system theory and catastrophe progression method. PLoS One. 2022;17(11):e0277324.PMID: 36395184; PMCID: PMC9671343. doi:10.1371/journal.pone.0277324
12. Xiangyong F. Analysis and evaluation of the layout of diagnostic workplaces in Nuclear Medicine Departments Based on GBZ 120-2020 radiation protection requirements for nuclear medicine. Chin J Health Supervision. 2021;28(4):368–371. doi:10.3969/j.issn.1007-6131.2021.04.013
13. Goodman TR, Mustafa A, Rowe E. Pediatric CT radiation exposure: where we were, and where we are now. Pediatr Radiol. 2019;49(4):469–478. doi:10.1007/s00247-018-4281-y
14. Singh VK, Seed TM. Entolimod as a radiation countermeasure for acute radiation syndrome. Drug Discov Today. 2021;26(1):17–30. doi:10.1016/j.drudis.2020.10.003
15. Liu C, Liu Y, Tian Y, et al. Application of the PDCA cycle for standardized nursing management in sepsis bundles. BMC Anesthesiol. 2022;22(1):39. doi:10.1186/s12871-022-01570-3
16. Breunig J, Hernandez S, Lin J, et al. A system for continual quality improvement of normal tissue delineation for radiation therapy treatment planning. Int J Radiat Oncol Biol Phys. 2012;83(5):e703–8.PMID: 22583604. doi:10.1016/j.ijrobp.2012.02.003
17. Herrmann K, Veit-Haibach P, Weber WA. Driving the future of nuclear medicine. J Nucl Med. 2019;60(Suppl 2):1s–2s. doi:10.2967/jnumed.119.232264
18. Mairinger S, Hernández-Lozano I, Zeitlinger M, et al. Nuclear medicine imaging methods as novel tools in the assessment of pulmonary drug disposition. Expert Opin Drug Deliv. 2022;19(12):1561–1575. doi:10.1080/17425247.2022.2137143
19. Jaschke W, Bartal G, Martin CJ, et al. Unintended and accidental exposures, significant dose events and trigger levels in interventional radiology. Cardiovasc Intervent Radiol. 2020;43(8):1114–1121. doi:10.1007/s00270-020-02517-2
20. Hussey P, Wu I, Johnston T. 2018 ACC/HRS/NASCI/SCAI/SCCT expert consensus document on optimal use of ionizing radiation in cardiovascular imaging: best practices for safety and effectiveness–a review for the cardiac anesthesiologist. J Cardiothorac Vasc Anesth. 2019;33(11):2902–2908. doi:10.1053/j.jvca.2019.01.006
21. Wei S, Zhou C, Huang L. Occupational health and safety: measurement and analysis of the electromagnetic radiation produced by radiofrequency devices for rejuvenation. Lasers Med Sci. 2022;38(1):25. doi:10.1007/s10103-022-03669-y
22. Peng M, Lee S, D’Souza AG, et al. Development and validation of data quality rules in administrative health data using association rule mining. BMC Med Inform Decis Mak. 2020;20(1):75. doi:10.1186/s12911-020-1089-0
23. Emery RJ, Gutierrez JM, Zwick MK. A compendium of radiation safety practices that can complement organizational worker well-being initiatives. Health Phys. 2024;127(4):539–542. doi:10.1097/HP.0000000000001835
24. Buda KG, Megaly MS, Omer M, et al. Use of radiation protection measures in live percutaneous coronary interventions cases at interventional scientific meetings. JACC Cardiovasc Interv. 2020;13(7):905–906. doi:10.1016/j.jcin.2019.11.036
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.