Back to Journals » Infection and Drug Resistance » Volume 15
Analysis of the Protective Effect of Infection Controllers Supervising Third-Party Personnel Entering and Leaving Shanghai Fangcang Shelter Hospital
Authors Lei N, Li BX, Zhang KF, Bao H, Ding J, Wang Y
Received 4 September 2022
Accepted for publication 6 December 2022
Published 19 December 2022 Volume 2022:15 Pages 7519—7527
DOI https://doi.org/10.2147/IDR.S388707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Na Lei,1,* Bi-Xi Li,2,* Kai-Fen Zhang,3 Hui Bao,4 Jian Ding,1 Yan Wang1
1Department of Disinfection and Supply, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, People’s Republic of China; 2Department of Anesthesiology, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, People’s Republic of China; 3Department of Outpatient, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, People’s Republic of China; 4Department of Urology, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Ding; Yan Wang, Department of Disinfection and Supply, General Hospital of Central Theater Command of the People’s Liberation Army, 627#, Wuluo Road, Wuchang District, Wuhan, 430070, People’s Republic of China, Tel +86-18971123442, Fax +86-27-50772953, Email [email protected]; [email protected]
Objective: To analyze the impact of the new supervision and management methods of infection controllers on the protection of third-party personnel entering and leaving Shanghai Fangcang shelter hospital, to provide a reference for the management of third-party personnel in Fangcang shelter hospitals.
Methods: A total of 200 third-party personnel received with traditional supervision and management methods, and 156 received new supervision and management methods from the Fangcang shelter hospital of the Shanghai International Convention and Exhibition Center. The sociodemographic characteristics of third-party personnel, including gender, age, education level, work experience in fighting the epidemic with safety awareness, was analyzed. The effects of the two different management modes on the protection of third-party personnel were statistically analyzed by the Chi-square test or logistic regression analysis.
Results: There were statistically significant differences in the incidence of infection among third-party personnel in terms of age, education level, work experience in fighting the epidemic in traditional supervision and management group, and whether they accepted the new supervision and management model had statistically significant differences (p < 0.05). The main causes of incorrect put on and take off protective clothing, such as wrong way to detach the face screen, wrong way to remove goggles, wrong way to undress protective clothing, wrong way to take off the shoe cover, hand washing steps omitted, are that causes infection of third-party personnel (p < 0.05).
Conclusion: The new supervision and management model can reduce the infection rate of third-party personnel in Fangcang shelter hospitals through planned and purposeful training in terms of different age groups, education levels, work experience, and acceptance of protection knowledge.
Keywords: shelter hospital, third-party personnel, new supervision, infection rate, Fangcang hospital
Introduction
With the continuous mutation and evolution of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a variety of mutant strains, such as Alpha, Beta, Gamma, Delta, and Omicron, have emerged.1–6 In the COVID-19 pandemic, the Omicron virus quickly became the dominant strain, and its infection gradually showed new characteristics, including fast transmission, widespread, and strong occultation, but it also showed the characteristics of reduced pathogenicity and severe disease rate.7–9 In the face of the novel pneumonia epidemic, the Chinese government has established an emergency medical system for classified treatment and sent COVID-19 patients with mild or asymptomatic disease to designated quarantine centers with primary medical treatment capabilities.8,10 Fangcang shelter hospitals have been proven to be an effective strategy for responding to the outbreak of COVID-19 in the community.11,12 Under the condition of a shortage of medical resources, Fangcang shelter hospital of the Shanghai International Convention and Exhibition Center has adopted a new management model. Medical personnel are responsible for in-flight medical treatment, and a large amount of logistical support is handed over to third-party personnel. These third-party personnel mainly include cleaning, security, and maintenance personnel. They are responsible for the sanitation in the Fangcang shelter hospital and the transfer of the daily life necessities of the patients. Third-party personnel are not health care professionals and have never been educated or practiced in contact with infectious disease protection systems. Therefore, they have indifferent protection awareness, wear and take off protective clothing unprofessionally, have to wear protective clothing to perform a lot of manual labor and hence are more likely to be directly exposed to the source of infection. If they are infected, it will affect the livelihood of patients in Fangcang shelter hospital. So, an effective supervision and management model from medical staff is worth exploring to reduce the infection of third-party personnel.
Material
Inclusive Criteria
The third-party personnel (cleaning, security, and maintenance) from Shanghai Wanjie Company who worked in the Fangcang shelter hospital of the Shanghai International Convention and Exhibition Center from April to May 2022 were selected as the study subjects. A total of 200 third-party personnel received with traditional supervision and management methods, and 156 third-party personnel received the new supervision and management methods in May 2022. According to the requirements of minimize the infection of personnel by the health department, all of them received at least two doses of COVID-19 vaccine before entering the workforce, and the last one was given within three months. The sociodemographic characteristics of third-party personnel, including gender, age, education level, work experience in fighting the epidemic with safety awareness, was analyzed. The causes and times of errors made by third-party personnel in the process of wearing and removing protective clothing were counted.
Method
Infection Control Supervision and Management Methods
Traditional supervision and management methods as follows, the infection control supervision team is based on a shift system, and each shift sends a full-time infection control medical worker to supervise the third-party personnel out of the red zone buffer zone and guide them to put on and take off the protective equipment during the whole process. Irregularities were carefully explained. In the buffer zone, the first and second take off rooms, and finally to the clean area, there were strict inspections by infection control personnel (see Figure 1A).
 |
Figure 1 The third-party personnel take off the protective clothing. (A) Using the traditional supervision and management methods; (B) Using the new supervision and management methods. |
The new supervision and management methods as follows, infection control medical staff should full-time supervise the third-party personnel out of the red zone buffer zone and guide them to put on and take off the protective equipment during the whole process. What’s more, all third-party personnel on duty were scanned and registered, and their names, personnel categories (cleaning, security, maintenance), working hours and other related information were published and posted to facilitate subsequent epidemiological tracking (see Figure 1B). All third-party personnel protection theory training, on-site operation drills, repeated viewing of videos for consolidation, and simulation tests were added. To enter the Fangcang shelter hospital, a full score is required for the simulation. When entering the Fangcang shelter hospital, if the supervisor finds the problem of wearing and taking off protective clothing, he or she will conduct on-site correction and retraining and record the training time and improvement measures. At the same time, the cause of the error was studied by all employees. Specifically, it can be summarized as the learning-practice-examination-supervision model (see Figure 2).
 |
Figure 2 The process of procedures for management the third-party personnel with the new supervision and management method. |
Statistical Methods
All data were processed using SPSS 22.0 statistical software. Descriptive statistical analysis was used to analyze the gender, age, education level of the third-party personnel, whether they had combined underlying diseases, vaccine injection, whether they had work experience in fighting the epidemic, and the incidence of infection. In the analysis, the comparison between groups was performed using the χ2 test or logistic regression analysis. When p <0.05, the difference was considered statistically significant.
Results
General Information of Third-Party Personnel
Among the 200 third-party personnel (cleaning, security, and maintenance), who received with traditional supervision and management methods. Cleaning in the Fangcang shelter hospital, 153 were males and 47 were females. The results showed that the third-party personnel are in terms of age, education level, and whether they have work experience in fighting the epidemic had statistically significant differences in the incidence rates (p <0.05), while the differences in the incidence of infections in terms of gender was not statistically significant (p >0.05), as shown in Table 1.
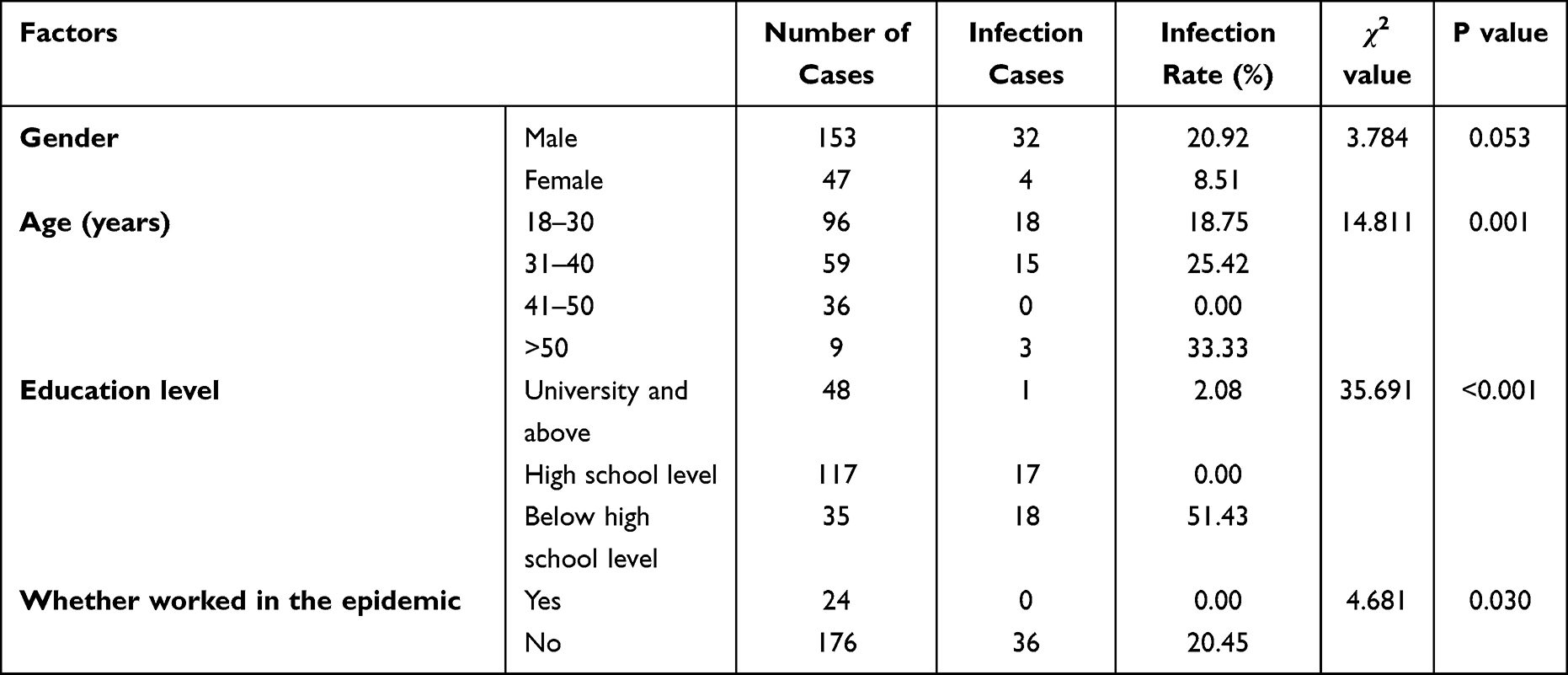 |
Table 1 Analysis of Risk Factors for Infection in Third-Party Personnel |
The Frequency of Errors in the Removal the Protective Equipment of Two Different Supervision and Management Methods
After implementing the new supervision and management methods, the frequency of errors in the removal of protective equipment continued to decline, and the safety awareness of third-party personnel gradually increased (Figure 3). In terms of common error removal of protective equipment, the supervision and management methods were significantly less than the traditional supervision and management methods (statistically significant), with wrong order of the face screen and the protective gown excluded.
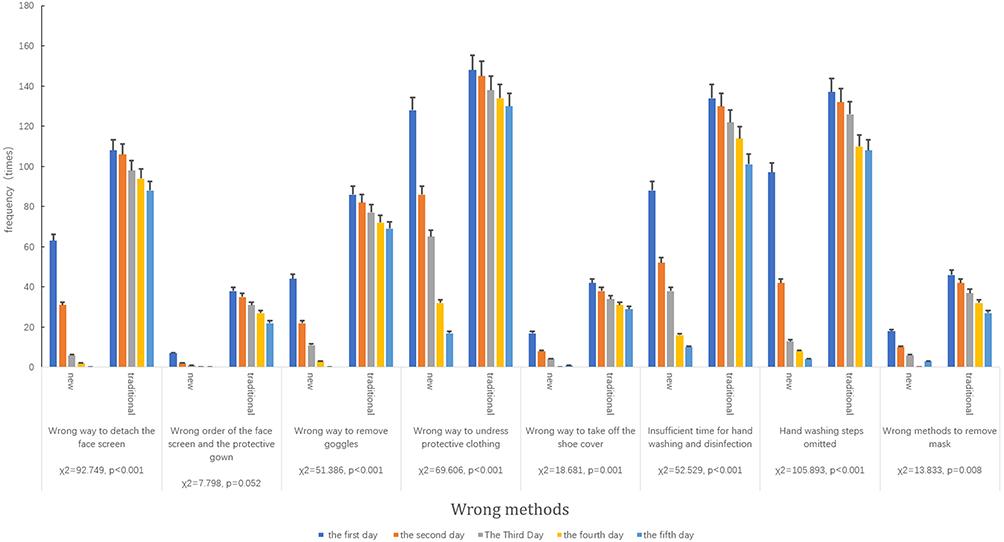 |
Figure 3 Comparison the errors frequency of two different methods with supervision and management of removal the protective equipment. |
Infection of Third-Party Personnel
During the operation stage of traditional supervision and management models, a total of 200 third-party personnel had infected 36 cases, including 32 males and 4 females. 18 cases were 18 to 30 years old, 15 cases were 31 to 40 years old, and 3 cases were over 40 years old. After the same number of days after the new supervision and management models, only 2 cases infected with the infection rate was 1.28%. The difference in the incidence of infection was statistically significant (p<0.05), see Table 2 for details.
 |
Table 2 Analysis of Infection of Third-Party Personnel with Different Supervision and Management Model |
The Main Causes of Incorrect Put on and Take off Protective Clothing That Causes Infection of Third-Party Personnel
The main causes of incorrect put on and take off protective clothing that causes infection of third-party personnel. Wrong way to detach the face screen, wrong way to remove goggles, wrong way to undress protective clothing, wrong way to take off the shoe cover, hand washing steps omitted are the main causes of incorrect put on and take off protective clothing that causes infection of third-party personnel (p <0.05), see Table 3 for details.
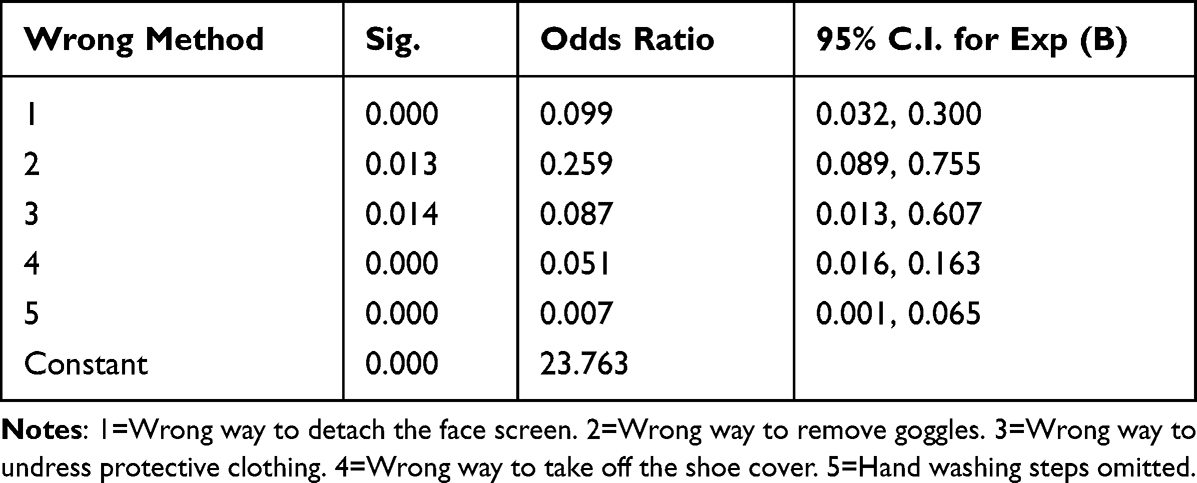 |
Table 3 Results of Errors in the Removal of Protective Equipment with Logistic Regression Analysis with Variables in the Equation (n = 356) |
Discussion
Compared with the traditional supervision and management mode, the new supervision and management mode is in terms of personnel management. One infection control officer is responsible for the supervision and management of a group of full-time infection control personnel who are responsible for supervising the third-party personnel to leave the red zone buffer zone and guide them to put on and take off the protective equipment. Therefore, it avoids the situation that in the traditional model, the personnel are scattered, and the problems that cannot be solved on duty are not implemented. Develop a roster of all personnel to go to work, check in with real names according to the shift, and check the health code to ensure that all personnel entering and leaving the passageway of the wear and tear area are safe and controllable personnel and to avoid the entry and exit of other factories and halls that bring bacteria and viruses in. In terms of training management, this mode targeted training based on the basic situation of third-party personnel. After multiple multistep training sessions, the frequency of third-party personnel taking off the protective equipment gradually decreased, and safety awareness gradually increased. In terms of quality control management, continuous improvement measures are proposed for problems, and continuous improvement is implemented to form a virtuous circle.13–15 In terms of effective communication, to ensure that all communication can be fed back to the people for the first time, the reported problems are solved in a timely manner.
The new type of supervision and management model provides purposeful and planned training based on the age, education level of third-party personnel, and whether they have work experience in fighting the epidemic that is statistically significant in reducing the number of infections and intervenes and evaluates existing problems at any time. Improved effectiveness and timely adjustment of training programs ultimately increased safety awareness and reduced the rate of infections, which greatly reduced the infection rate of third-party personnel in shelter hospitals.16
The age of the third-party personnel had statistical significance in reducing the rate of infections. This suggests that younger people are more likely to learn and accept the complex and professional work of putting on and taking off protective equipment.17–19 Besides, the undressing process needs to be completed independently and is prone to errors. Young people are willing to admit mistakes, accept criticism and help from the supervision and management from medical staff, and they are more willing to communicate with others to learn and improve together.
The education level of third-party personnel was statistically significant in reducing the number of infections. In this epidemic, the COVID-19 virus was extremely contagious. We should fully study its biological characteristics to be better protected ourself at work. Even the training content is limited to the steps of the process of putting on and taking off protective equipment, personnel with a high level of education can combine theoretical knowledge and practice to master the specific steps of putting on and taking off masks, protective clothing, goggles, and visors.20,21 Highly educated personnel are better able to understand the significance of each step of putting on and taking off protective clothing, and better understand the consequences of putting on and taking off protective clothing incorrectly. As a result, they are better able to prevent mistakes from happening, and better able to accept with remedial measures after mistakes. Although third-party personnel do clean and security work, the risk factors are higher. Therefore, it is recommended that third-party personnel try to recruit personnel with higher education levels. The higher the overall education level is, the lower the risk of infection.
Third-party personnel with work experience fighting the epidemic had statistical significance in reducing the number of infections. Possessing work experience in fighting the epidemic has important guiding significance for this type of epidemic work.22,23 Protection is the key point in the work of the epidemic. The personnel with such work experience pay more attention to the details of protection when wearing protective equipment than other personnel when performing hygiene, such as avoiding pollution. It can prevent sharp objects from scratching the gloves, and the mask needs to be replaced urgently after sweating so that it can respond urgently and have a stronger awareness of safety protection.24 At the same time, serving as the monitor and group leader in the team, dispersed in each group. Entering and exiting the Fangcang shelter hospital at the same time as other third-party personnel can guide and help the colleagues around him at any time, improve the overall protection level, and reduce the rate of infections.
Putting on and taking off protective clothing is a very professional working for medical staff, who are often not standardized in this daily work.2,24–27 It is even more difficult for non-professional third-party personnel. Third-party personnel not only need to face COVID-19 patients, but also need to handle the extremely high amount SARS-CoV-2 of medical waste.28 This study preliminarily discussed how to guide the third-party personnel in Fangcang shelter hospitals to wear and remove protective clothing. The main causes of incorrect put on and take off protective clothing, such as wrong way to detach the face screen, wrong way to remove goggles, wrong way to undress protective clothing, wrong way to take off the shoe cover, hand washing steps omitted, are that causes infection of third-party personnel. So, these errors need to strengthen the correction.
As the first study to raise this issue, it also has some limitations and shortcomings. Firstly, this study is a retrospective study with small sample size, which may have statistical bias. Secondly, the two different supervision and management methods are carried out in different periods of time, which may be interfered by other hidden factors, such as the latter may obtain more learning opportunities for epidemic prevention knowledge. However, we believe that this study can bring some enlightenment to the anti-epidemic work. Firstly, the anti-epidemic work can give full play to the strength of third-party personnel and reduce the pressure on medical resources. Secondly, reasonable supervision and management methods can reduce the infection rate of non-medical staff in high-infection wards. Thirdly, this study provides some effective measures to guide non-medical staff to wear and remove protective clothing.
Conclusion
The main causes of incorrect put on and take off protective clothing, such as wrong way to detach the face screen, wrong way to remove goggles, wrong way to undress protective clothing, wrong way to take off the shoe cover, hand washing steps omitted, are that causes infection of third-party personnel. The new supervision and management methods are more comprehensive and meticulous in personnel management, training management, and quality management than the traditional management model. This greatly reduces the number of third-party personnel infected and reduces the infection rate of third-party personnel in shelter hospitals. Compared with the traditional supervision and management methods, it is more suitable for the protection and management of third-party personnel in Fangcang shelter hospital, which is worthy of recommendation. We hope that by spreading this experience, more people will be able to participate in the fight against COVID-19 without becoming susceptible to infection.
Ethics Statement
This study complies with the guidelines for public studies and is in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patients and/or the public in accordance with the Declaration of Helsinki for the purpose of publication of the present report and any relevant images. This is a public health management experience report; thus, no medical ethics statement is needed according the Ethics Review Committee of General Hospital of Central Theater Command of the Chinese People’s Liberation Army.
Patient and Public Involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors do not declare a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mann C, Hoyle JS, Downard KM. Detection of SARS CoV-2 coronavirus omicron variant with mass spectrometry. Analyst. 2022;147(6):1181–1190. doi:10.1039/d2an00028h
2. Zhang X, Wang H, Wang Y, et al. Epidemiological and clinical based study on four passages of COVID-19 patients: intervention at asymptomatic period contributes to early recovery. BMC Infect Dis. 2020;20(1):855. doi:10.1186/s12879-020-05570-x
3. Zhu J, Huang WC, Huang B, et al. Clinical characteristics and prognosis of COVID-19 patients with initial presentation of lung lesions confined to a single pulmonary lobe. Am J Transl Res. 2020;12(11):7501–7509.
4. Wolfe M, Hughes B, Duong D, et al. Detection of SARS-CoV-2 variants mu, beta, gamma, lambda, delta, alpha, and omicron in wastewater settled solids using mutation-specific assays is associated with regional detection of variants in clinical samples. Appl Environ Microbiol. 2022;88(8):e0004522. doi:10.1128/aem.00045-22
5. Zhu J, Zhang Y, Gao XH, Xi EP. Coronavirus disease 2019 or lung cancer: a differential diagnostic experience and management model from Wuhan. J Thorac Oncol. 2020;15(8):e141–e142. doi:10.1016/j.jtho.2020.04.030
6. Zinatizadeh MR, Zarandi PK, Zinatizadeh M et al. Efficacy of mRNA, adenoviral vector, and perfusion protein COVID-19 vaccines. Biomed Pharmacother. 2022;146:112527. doi:10.1016/j.biopha.2021.112527
7. Liu Y, Yu Y, Zhao Y, He D. Reduction in the infection fatality rate of Omicron variant compared with previous variants in South Africa. Int J Infect Dis. 2022;120:146–149. doi:10.1016/j.ijid.2022.04.029
8. Zhang X, Zhang W, Chen S. Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic. Lancet. 2022;399(10340):2011–2012. doi:10.1016/S0140-6736(22)00838-8
9. Liu M, Shi L, Chen H, et al. Comparison between China and Brazil in the two waves of COVID-19 prevention and control. J Epidemiol Glob Health. 2022;12(2):168–181. doi:10.1007/s44197-022-00036-6
10. Liu P, Zhang H, Long X, et al. Management of COVID-19 patients in Fangcang shelter hospital: clinical practice and effectiveness analysis. Clin Respir J. 2021;15(3):280–286. doi:10.1111/crj.13293
11. Fang D, Pan S, Li Z, et al. Large-scale public venues as medical emergency sites in disasters: lessons from COVID-19 and the use of Fangcang shelter hospitals in Wuhan, China. BMJ Glob Health. 2020;5(6):e002815. doi:10.1136/bmjgh-2020-002815
12. Rosecrans AM, Moen MA, Harris RE, et al. Implementation of Baltimore City’s COVID-19 isolation hotel. Am J Public Health. 2022;112(6):876–880. doi:10.2105/AJPH.2022.306778
13. Li J, Yuan P, Heffernan J, et al. Fangcang shelter hospitals during the COVID-19 epidemic, Wuhan, China. Bull World Health Organ. 2020;98(12):830–841D. doi:10.2471/BLT.20.258152
14. Alderden J, Kennerly SM, Cox J, Yap TL. Pressure injury risk assessment and prevention in patients with COVID-19 in the intensive care unit. AACN Adv Crit Care. 2022;33(2):173–185. doi:10.4037/aacnacc2022335
15. Zhou L, Rong X, Fan M, et al. Modeling and evaluation of the joint prevention and control mechanism for curbing COVID-19 in Wuhan. Bull Math Biol. 2022;84(2):28. doi:10.1007/s11538-021-00983-4
16. Windisch O, Zamberg I, Zanella MC, et al. Using mHealth to increase the reach of local guidance to health professionals as part of an institutional response plan to the COVID-19 outbreak: usage analysis study. JMIR Mhealth Uhealth. 2020;8(8):e20025. doi:10.2196/20025
17. Arévalo A, Simoes E, Petinati F, Lepski G. What does the general public know (or not) about neuroscience? Effects of age, region and profession in Brazil. Front Hum Neurosci. 2022;16:798967. doi:10.3389/fnhum.2022.798967
18. Khatib M, Sheikh Muhammad A, Hadid S et al. Correlates of hookah smoking among Arab adults in Israel identified by a machine learning algorithm. Isr Med Assoc J. 2022;24(4):246–252.
19. Murphy DH, Castel AD. The role of attention and ageing in the retrieval dynamics of value-directed remembering. Q J Exp Psychol. 2022;75(5):954–968. doi:10.1177/17470218211046612
20. Dow AW, DiPiro JT, Giddens J et al. Emerging from the COVID-19 crisis with a stronger health care workforce. Acad Med. 2020;95(12):1823–1826. doi:10.1097/ACM.0000000000003656
21. Peterson WJ, Munzer BW, Tucker RV, et al. Rapid dissemination of a COVID-19 airway management simulation using a train-the-trainers curriculum. Acad Med. 2021;96(10):1414–1418. doi:10.1097/ACM.0000000000004120
22. Rao A, Ma H, Moloney G, et al. A disproportionate epidemic: COVID-19 cases and deaths among essential workers in Toronto, Canada. Ann Epidemiol. 2021;63:63–67. doi:10.1016/j.annepidem.2021.07.010
23. Hsu YT, Lan FY, Wei CF, et al. Comparison of COVID-19 mitigation and decompression strategies among homeless shelters: a prospective cohort study. Ann Epidemiol. 2021;64:96–101. doi:10.1016/j.annepidem.2021.08.023
24. Yang Y, Wang H, Chen K et al. Shelter hospital mode: how do we prevent COVID-19 hospital-acquired infection? Infect Control Hosp Epidemiol. 2020;41(7):872–873. doi:10.1017/ice.2020.97
25. Zhu J, Jiang CY, Huang B, et al. Cylindrical tube stethoscopes: the value of practical equipment in the management of patients with infectious diseases. Infect Drug Resist. 2022;15:3611–3618. doi:10.2147/IDR.S369305
26. Keum H, Kim D, Whang CH, et al. Impeding the medical protective clothing contamination by a spray coating of trifunctional polymers. ACS Omega. 2022;7(12):10526–10538. doi:10.1021/acsomega
27. Kahveci Z, Kilinc-Balci FS, Yorio PL. A simulation study to assess fluid leakage through the glove-gown interface in isolation settings. Am J Infect Control. 2021;49(12):1481–1487. doi:10.1016/j.ajic.2021.08.013
28. Seif F, Noorimotlagh Z, Mirzaee SA, et al. The SARS-CoV-2 (COVID-19) pandemic in hospital: an insight into environmental surfaces contamination, disinfectants’ efficiency, and estimation of plastic waste production. Environ Res. 2021;202:111809. doi:10.1016/j.envres.2021.111809
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.