")
Back to Journals » Clinical Ophthalmology » Volume 17
Analysis of the Outcomes of the Screen-Time Reduction in Computer Vision Syndrome: A Cohort Comparative Study [Response to Letter]
Received 20 January 2023
Accepted for publication 20 January 2023
Published 25 January 2023 Volume 2023:17 Pages 361—363
Mohammed Iqbal, Ahmed Gad
Department of Ophthalmology, Faculty of Medicine, Sohag University, Sohag, Egypt
Correspondence: Mohammed Iqbal, Email [email protected]
View the original paper by Professor Iqbal and colleagues
This is in response to the Letter to the Editor
Dear editor
We thank both Dr. Abdelaziz K. and Dr. Shaheen M. for their interest in our study1 in computer vision syndrome (CVS) and the important issues and questions they raised. For more precision and clarity, we would like to respond to their concerns in this reply and discuss the issues they addressed.
First, we did not publish and/or analyze all study data as we previously stated in the Discussion section; however, Table 1 shows the correlation between the daily screen-hours’ differences and the differences in the other study outcome measures particularly uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), and multifocal electroretinogram (mfERG) Rings and Quadrants. Mathematically, we can simply define these differences as “the post-screen-time-reduction values – the pre-screen-time-reduction values”. We exhibited a negative correlation between the differences of the daily screen-hours and UDVA, i.e. the lower the daily screen-hours the better the UDVA (r=−0.61, P=<0.0001, Table 1). Furthermore, we also documented a positive correlation between the differences of the daily screen-hours reduction and mfERG Rings 1 and 2 with Quadrant 1, i.e. the more the daily screen-hours reduction the greater the foveal responses amplitude (amplitude density of the first foveal peak [P1 AD]) in R1, R2 and Q1 with more improved foveal peak close to normal (r=0.53, 0.51 and 0.38; P=0.0001, 0.0002 and 0.006, respectively; Table 1). Tables 2 and 3 summarize the correlation between UDVA and mfERG parameters, and CDVA and mfERG parameters, respectively. In short, there are negative correlations between many mfERG parameters and the mathematical “minus” sign of the logMAR units of pre- and post-screen-time reduction differences of both UDVA and CDVA, i.e. the more the improvements in the mfERG foveal responses, the more negative is the “–” sign of the logMAR differences’ units thus the better the improvements in both UDVA and CDVA (Tables 2 and 3). Therefore, we concluded that the improvements in the mfERG foveal responses were associated with corresponding improvements in the visual performances.
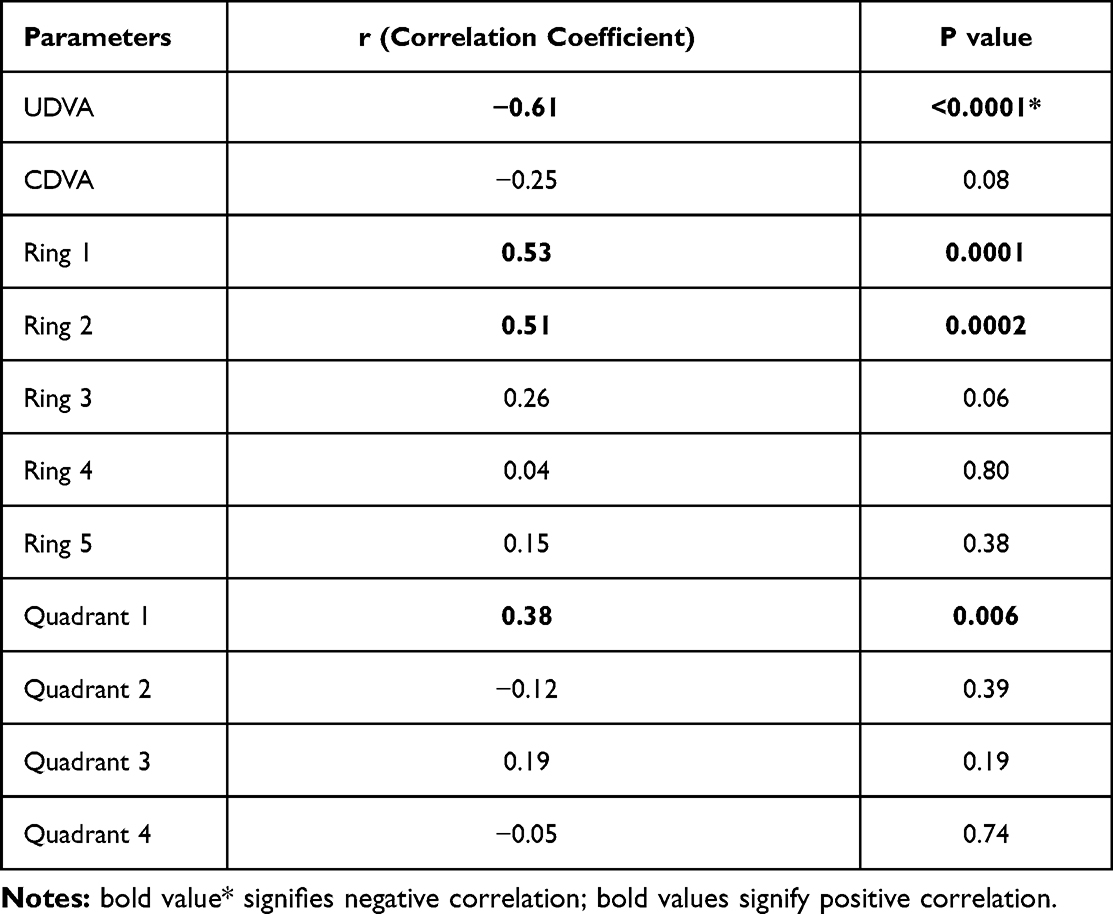 |
Table 1 Correlation Between Differences in Daily Screen-Hours and Study Parameters |
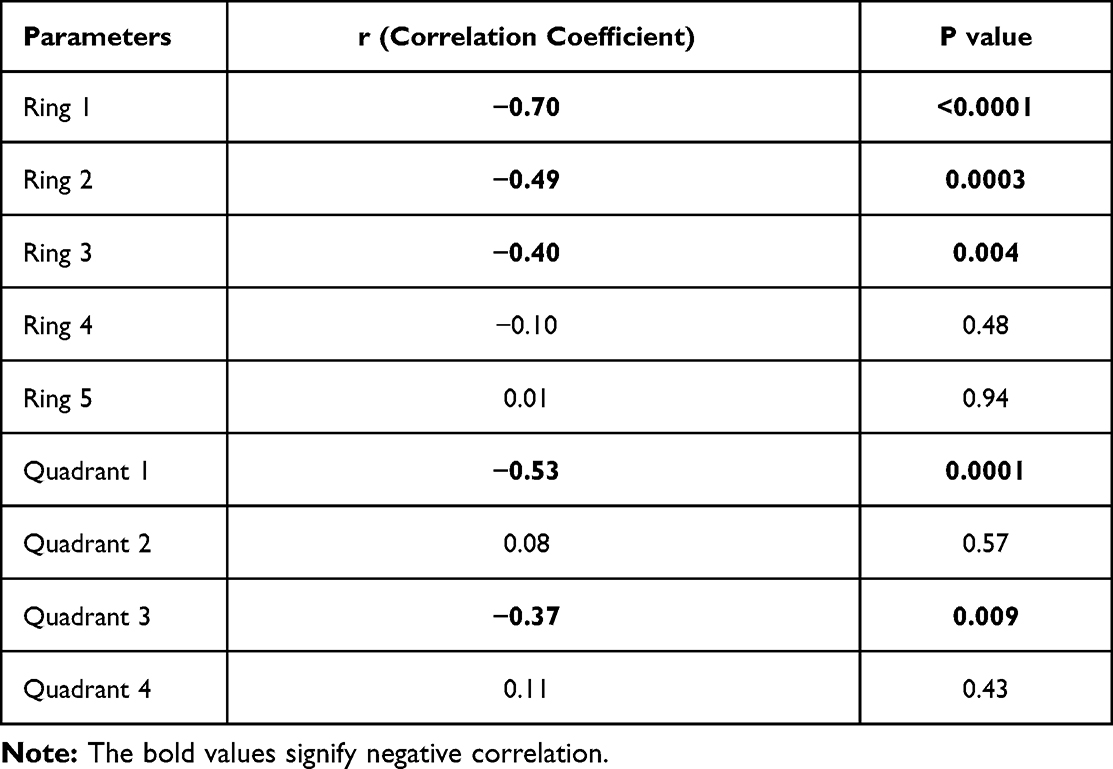 |
Table 2 Correlation between Differences in UDVA and mfERG Parameters |
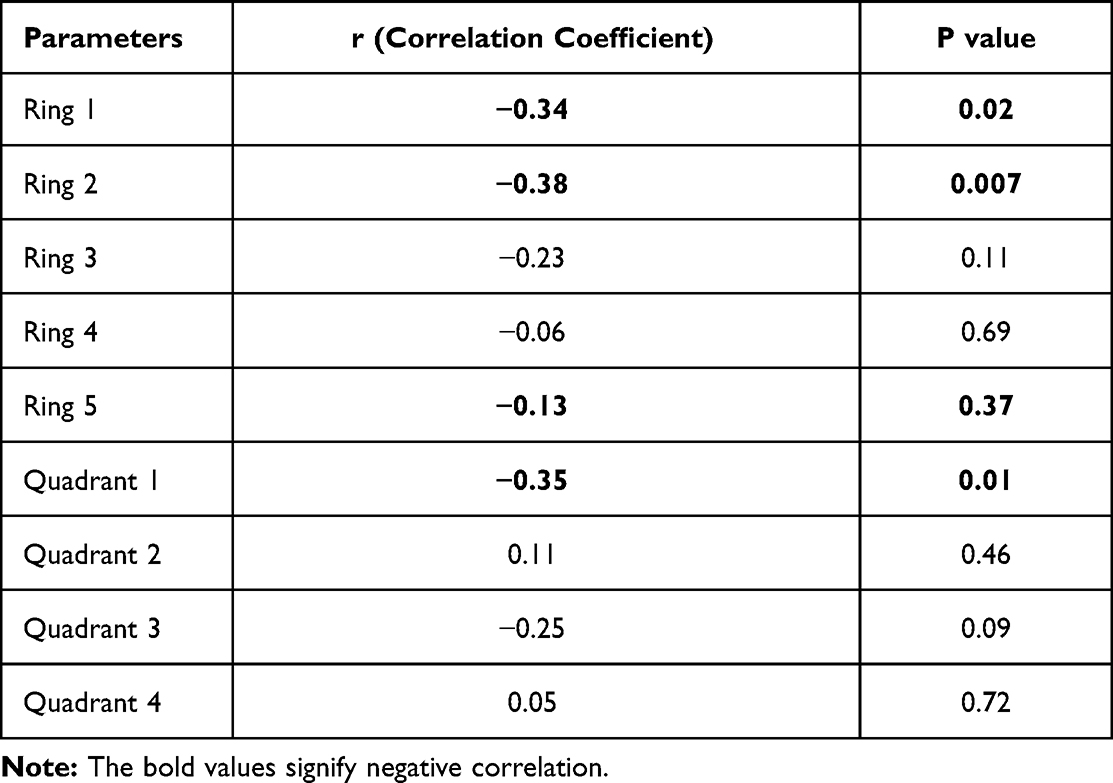 |
Table 3 Correlation Between Differences in CDVA and mfERG Parameters |
Second, regarding the concerns how we managed to observe these students, we definitely did not use surveillance cameras or observe them at their homes or colleges 24/7; however, we observed their objective outcomes that exhibited great improvements at the end of the study. Moreover, the students were free to quit at any time without trial completion. Therefore, we found no reason why the students did not follow our instructions especially if they were free to quit the trial anytime they wanted. Nevertheless, the improvement in their objective outcomes (UDVA, CDVA and mfERG foveal responses) at the end of the study coincided with the fact that they limited their screen-time to one hour daily for four weeks. Another similar example, when a doctor prescribes a diet regimen for an obese patient, the doctor cannot observe exactly what the patient eats at home or elsewhere; however the doctor measures the objective outcomes by observing the patient weight; once the patient follow the instructions, he/she starts to lose weight. Furthermore, as we mentioned in the Discussion section, all participants responded to the CVS-F3 questionnaire,1–3 (Supplementary Material) twice at the beginning and the end of the study. Most of these participants reported marked improvements in their subjective CVS complaints especially with improvement of the visual blur and relieved eyestrain, headache, neck and shoulder pain. These subjective findings also proved the fact that the participants managed to reduce their screen-time to one screen-hour daily for four weeks. Nevertheless, we advised the participants to watch the TV screen from a proper distance of 5−6 meters and wear their spectacles if they had ones.
Third, we stated in the Methods section that the first step in recruitment of the students was to respond to our CVS-F3 questionnaire,1–3 (Supplementary Material) which includes an important question “Are you willing to decrease your screen hours to guard against CVS?” The students, who admitted that they were willing to decrease their screen-hours, were interviewed to convince them to participate in our trial to investigate the potential effect of the screen-time reduction in improving the screen-induced foveal dysfunction and visual performances. Therefore, although a large number of students responded to our CVS-F3 and we anticipated their participation, yet unfortunately only small number of them responded “Yes” as an answer to the later question. Among this small number, only students that fulfilled Iqbal’s four major diagnostic criteria for accurate CVS diagnosis,2,4 were included in the CVS group of the study.
Fourth, we think that our described instructions are generally applicable for all cases suffering from CVS complaints provided that they are really willing to reduce their screen-time.
Finally, we are grateful for the Editor-in-Chief and the Editorial Board for giving us the opportunity for this reply to respond to the concerns and issues addressed by Dr. Abdelaziz K and Dr. Shaheen M.
Acknowledgments
We are grateful for Professor Fouad Metry, the mathematician expert who analyzed the statistics in this reply.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this communication.
References
1. Iqbal M, Soliman A, Ibrahim O, Gad A. Analysis of the outcomes of the screen-time reduction in computer vision syndrome: a cohort comparative study. Clin Ophthalmol. 2023;17:123–134. doi:10.2147/OPTH.S399044
2. Iqbal M, Said O, Ibrahim O, Soliman A. Visual sequelae of computer vision syndrome: a cross-sectional case-control study. J Ophthalmol. 2021;2021:6630286. doi:10.1155/2021/6630286
3. Iqbal M, Elzembely H, El-Massry A. Computer vision syndrome prevalence and ocular sequelae among medical students: a university-wide study on a marginalized visual security issue. Open Ophthalmol J. 2021;15:156–170. doi:10.2174/1874364102115010156
4. Iqbal M, Ibrahim Elzembely H, Said OM. Letter to the editor: “Self-reported student awareness and prevalence of computer vision syndrome during COVID-19 pandemic at Al-Baha University” [Letter]. Clin Optom. 2022;14:193–194. doi:10.2147/OPTO.S391171
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.