Back to Journals » Risk Management and Healthcare Policy » Volume 16
Analysis of the Nursing Effect of Anesthesia Care Integration Combined with Preventive Nursing on Older Patients with Lumbar Disc Herniation During the Perioperative Period
Authors Liu H, Li P, Yu D, Ma Z, An Y, Li S, Cai L
Received 10 March 2023
Accepted for publication 17 May 2023
Published 9 June 2023 Volume 2023:16 Pages 1001—1009
DOI https://doi.org/10.2147/RMHP.S411885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Honghong Liu,1 Peng Li,1 Dan Yu,1 Zhongxi Ma,2 Yu An,1 Si Li,1 Lin Cai1
1Department of Anesthesiology, Wuhan Fourth Hospital, Wuhan, 430033, People’s Republic of China; 2Department of Spine Surgery, Wuhan Fourth Hospital, Wuhan, 430033, People’s Republic of China
Correspondence: Lin Cai, Department of Anesthesiology, Wuhan Fourth Hospital, No. 473, Hanzheng Street, Qiaokou District, Wuhan, 430033, People’s Republic of China, Tel +86 17764059606, Email [email protected]
Objective: This study explored the nursing effect of anesthesia care integration combined with preventive nursing on older patients with perioperative lumbar disc herniation (LDH).
Methods: Clinical data of 100 older patients with LDH who were admitted to our hospital between May 2017 and May 2022 were used, and there were no patients who had not had surgery between January and May 2020 because of the COVID-19 pandemic. Based on the different nursing methods, the patients were divided into control and observation groups, with 50 cases each. The control group received anesthesia care integration, whereas the observation group received anesthesia care integration combined with preventive nursing. Lumbar spine function, pain score, anesthesia recovery assessment, and nursing effects were compared between the two groups.
Results: The scores of the anesthesia recovery assessment of the two groups were compared, and the vital signs of the observation group during recovery from anesthesia were significantly better than those of the control group (P< 0.05). After nursing care, the Japanese Orthopaedic Association (JOA) score of the observation group was significantly higher than that of the control group; however, the numerical scale (NRS) score of the observation group was significantly lower than that of the control group (P< 0.05). After nursing care, the physical comfort, emotional state, psychological support, self-care ability, and pain scores were higher in the observation group than in the control group; however, the NRS score of the observation group was significantly lower than that of the control group (P< 0.05).
Conclusion: Anesthesia care integration combined with preventive nursing has a positive effect on older patients with perioperative LDH, and it significantly improves lumbar spine function, reduces pain, shortens recovery time, and benefits physical and mental health.
Keywords: anesthesia nursing, preventive nursing, lumbar disc herniation, nursing effect, lumbar spine function
Introduction
Lumbar disc herniation (LDH) is a common disease in orthopedics. The main clinical symptoms of the disease are lower back and radiating pain in the lower extremities. Most patients suffer from repeated illnesses and a long course of disease, which affects their normal work and life. When conservative management fails, patients usually require surgical treatment.1 Currently, the surgical treatment for LDH is mainly conventional surgery, and the curative effect is positive; however, the surgical trauma is large, and the postoperative recovery of patients is slow.2 Effective nursing interventions can optimize treatment effects and accelerate patient recovery.3 Anesthesia care integration management model is more efficient than routine care and has its own unique advantages.4 In addition, its’ implementation can effectively reduce overcare problems and enhance the pertinence of care. However, anesthesia care integration lacks pre-judgment of the patient’s condition, disease development, and risk factors based on the risk of prediction results.5,6 Studies have shown that the application of preventive nursing guidelines in orthopedic nursing is effective and can improve compliance, reduce complications, and improve patient self-care levels and nursing satisfaction.7 Preventive nursing comprehensively evaluates the patient’s condition, formulates and implements a scientific and reasonable nursing plan to intervene in the progression of the disease, promote patient recovery, and improve nursing satisfaction.8
Preventive nursing is a feature with pre-darkness and predictability that can prevent various clinical nursing risks and ensure the safe and effective recovery of patients by formulating scientific nursing plans.9 Preventive nursing intervention enhances patients’ awareness and understanding of LDH through education, prompts patients to actively cooperate, strengthens posture and lumbar spine function; training and nursing to prevent complications helps patients improve lumbar spine function, and promotes good recovery of their condition.10 Here, the safety of anesthesia care integration combined with preventive nursing in the recovery period of anesthetized patients is discussed, including clinical nursing practice through clinical trial research analysis to develop anesthesia care integration after anesthesia, thereby reducing the patient’s anxiety level. This study was performed to explore the nursing effect of Anesthesia care integration combined with Preventive Nursing on perioperative elderly patients with lumbar disc herniation.
Materials and Methods
Study Participants
This study used clinical data of 100 older patients with LDH who were admitted to our hospital between May 2017 and May 2022, and there were no patients who had not had surgery between January and May 2020 because of the COVID-19 pandemic. (This study was approved by the Ethics Committee of Wuhan No. 4 Hospital, Ethics No. KY2022-073-01.) Based on the different nursing methods, the patients were divided into control and observation groups, with 50 cases each. The diagnostic criteria for LDH1 were: (i) leg pain higher than lower back pain, mainly confined to the sciatic nerve or femoral innervation area; (ii) paresthesia in the dermatomes; and (iii) positive straight leg raising between a hip flexion angle of 30–70 degrees, and imaging features (CT or MRI) consistent with clinical manifestations. In addition, the incidence of LDH is associated with sedentary lifestyle, long-term driving, chronic cough, pregnancy, smoking, and heavy physical labor.
Eligibility Criteria
Inclusion criteria were as follows: (i) patients with typical symptoms of lower back and leg pain confirmed by frontal and lateral spine X-ray, CT, and magnetic resonance imaging (MRI); (ii) patients with ineffective conservative treatment or repeated attacks and those who were able to communicate normally; and (iii) complete clinical data. The exclusion criteria were as follows: (i) new onset intervertebral disc herniation, previous traditional interlaminar fenestration surgery, severe liver and kidney insufficiency, or abnormal coagulation mechanism; (ii) those who had undergone spinal fusion or internal fixation surgery, and those who were unwilling to do so; and (iii) those with traumatic fractures who underwent minimally invasive lumbar spine surgery. The treatment and nursing measures of the selected cases in this study were in line with ethical standards.
Intervention
The comparison group used anesthesia care integration, that is, the establishment of an anesthesia care management team. The basis for anesthesia care integration management is the nursing staff, and a team was established. Members of this team underwent professional training in anesthesia care, anesthesia resuscitation, and other related knowledge. They were familiar with operating room instruments, were skilled in the dosage and methods of drug use, and had professional nursing and resuscitation skills to handle special situations in surgery.
Pre-Operative Preparation
The surgical environment has an impact on the body temperature of patients; therefore, the temperature of the operating room is adjusted to 22°C~25°C. Patients entering the operating room are carefully checked for name, sex, operation name and site, anesthesia mode, and pre-anesthesia medication. It is verified whether the patient strictly followed the medical cheat sheet to ensure good personal pre-operative preparation and are strictly monitored for heart rate, blood pressure, and respiratory condition during pre-operative medication.
Anesthesia Care
Prior to anesthesia, traveling nurses establish intravenous channels for surgical anesthesia, intraoperative rehydration, blood transfusion, and drug resupply. During operation, nurses are agile, alert, and skilled in cooperating with the operation and in touring the operation room to ensure that supply and needs are met during the operation. Patients’ vital signs are monitored so that doctors can observe the changes in vital signs after anesthesia in a timely manner. As anesthetic drugs affect the patient’s middle and frame nervous and respiratory systems, the patient’s heart rate, blood pressure, respiration, and oxygen saturation should be closely monitored. In addition, blood loss of the patient is monitored, and rehydration or blood transfusion is performed when necessary.
Postoperative Care
Here, safe movement of the patient to the hospital bed after surgery is ensured to minimize vibration and prevent sudden changes in the patient’s blood pressure and dislodgement of various drains. Patients who undergo general anesthesia are prone to postoperative agitation; therefore, preparatory measures are made in advance to prevent patients from falling out of bed and ensuring their safety. In addition, anesthetic drugs have an effect on the patient’s thermoregulatory frame, and prolonged exposure of organs and large amounts of fluids during surgery can cause a drop in body temperature; therefore, the patient should be kept warm after surgery. For patients who are not yet awake, a ventilation catheter can be placed in the pharynx to ensure that the airway is open until the patient is awake, as the muscles in the lower collar joint area are relaxed and prone to obstruction of the pharyngeal passage. In this process, the patient’s head is tilted to one side with the pillow removed. In case of misaspiration, the patient’s head is lowered so that the vocal fissure is higher than the entrance of the esophagus, and the vomit can flow from the corner of the patient’s mouth after flowing to the nasopharyngeal cavity.
In the observation group, preventive nursing was implemented based on the comparison group, that is, patients were introduced to the ward environment layout and status of medical and nursing staff in a warm and gentle tone after admission to eliminate unfamiliarity and fear. Disease brochures were distributed to the patients, with emphasis on explaining about LDH, and videos were shown to deepen their impressions and allow them to understand the prevention and treatment measures and prognosis of the disease. To obtain a positive cooperative attitude, the patient’s cognitive level should be improved.
Prevention of Hypothermia
In the intraoperative infusion process, hypothermia may be caused by a large amount of abdominal irrigation and exposure of the abdominal cavity. Hypotensive patients can be warmed up by a heater after full implementation, and temperature monitoring can be performed to avoid agitation caused by stress reaction of the patient’s body owing to high or low temperatures. For patients who are clear or conscious, the medical staff should inform the patients whether the operation is successful so that the patients can be released from psychological pressure and avoid the increase in blood pressure owing to emotional excitement, thus, allowing patients to feel happy and relieved. Some patients may have elevated blood pressure because of pain, which may manifest as agitation and pain and may be treated with intravenous analgesic pumps or by following appropriate medical advice. If the patient’s blood pressure cannot be controlled, the anesthesiologist is informed immediately, and antihypertensive medication is prescribed for oral administration. During the recovery period from surgical anesthesia, the patient’s body position should be observed, allowing the patient to maintain a good psychological state by deep breathing to relieve tension and anxiety. Once awake, the patient should be given psychological comfort. Patients should be informed of possible complications and be allowed to spend the recovery period of anesthesia with medical staff. The body should be wiped with hot towels every day to promote local blood circulation.
Rehabilitation Exercise Care
Rehabilitation exercise care includes formulating a healthy diet for the patient, allowing the patient to practice the lumbar spine and abdominal muscles according to the patient’s physical recovery, helping the patient establish proper sleeping and sitting postures, practicing leg swinging, knee bending, prone head lifting, and foot-picking exercises, adopting a three- or five-point support method for the lumbar back to improve the function of the lumbar muscles, and strengthening the spinal balance function to promote stable rehabilitation of the lumbar spine.
Outcome Indicator
The evaluation of lumbar vertebrae function adopts the Japanese Orthopaedic Association (JOA) score for which the total score is 29; the higher the score, the better the functional recovery. The patient’s degree of pain was evaluated using the NRS, with scores ranging from 0—10, and an increase in the score indicated an increase in pain.
Nursing Effect
The Chinese version of the 40-item Postoperative Recovery Quality Questionnaire (QoR-40) was used to conduct a series of evaluations of the nursing effect on patients after recovery. The QoR-40 scale includes emotional state, pain status, physical comfort, psychological support, and physical independence. The QoR-40 uses a five-point Likert scale to edit the total score and its subscales (1 = none, 2 = occasionally, 3 = more time, 4 = most of the time, and 5 = always have). The total score for individual items was 40–200 points.
Statistical Analysis
SPSS 23.0 was used for all data in this study; the test level was α=0.05 and P<0.05, which was considered statistically significant. Measurement data were described by mean ± standard deviation, and independent samples t-test was used. Those that did not obey the normal distribution were described as the median (interquartile range) and obeyed the normal distribution. The paired-sample t-test was used for the comparison within groups, and the two independent sample t-tests were used for comparison between groups. If the normal distribution was not obeyed, the nonparametric Wilcoxon signed-rank test was used for intra-group comparisons, and the rank-sum test was used for between-group comparisons.
Results
Baseline Data Comparison
There were no significant differences in the average age, sex, basic illness, and body mass index between the two groups (P>0.05). See Table 1.
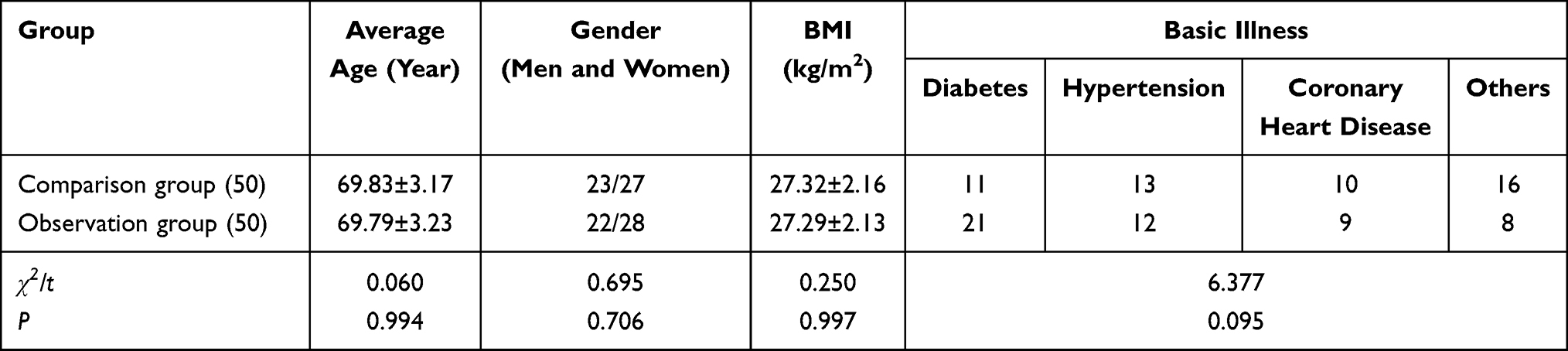 |
Table 1 Comparison of Baseline Data of Two Groups of Patients |
Anesthesia Recovery Assessment
Comparing the scores of anesthesia recovery evaluation of the two groups of patients, the vital signs of the two groups of patients during recovery from anesthesia were significantly better than those of the control group (P<0.05). See Figure 1.
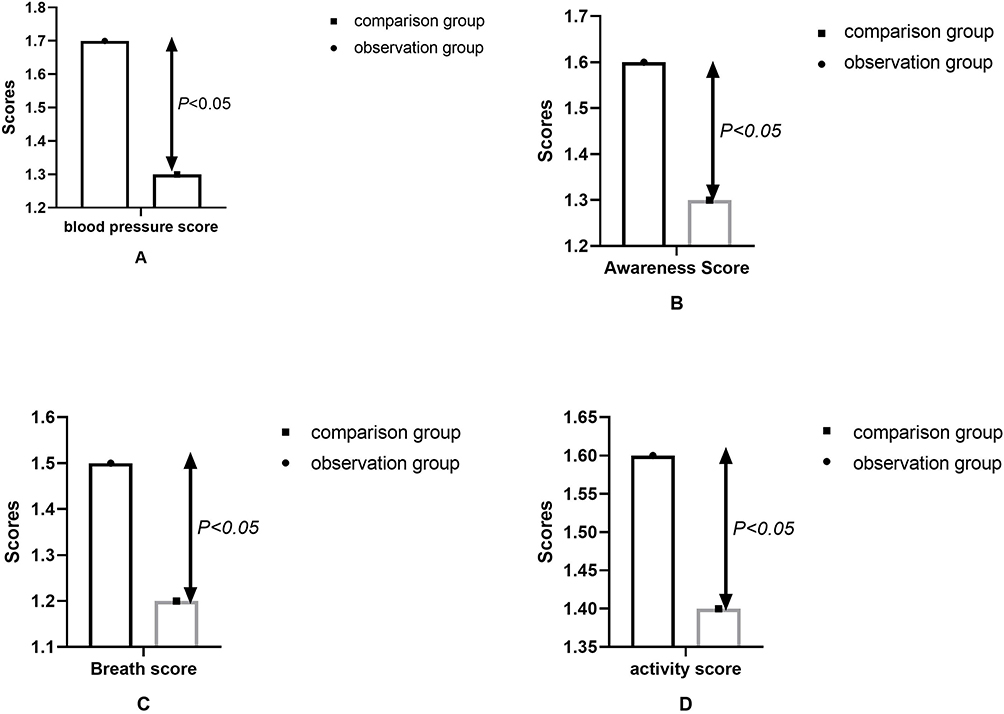 |
Figure 1 Anesthesia recovery assessment. This study uses SPSS 23.0 statistical software to conduct statistical analysis and calculation of anesthesia recovery assessment data. Measurement data are expressed as mean ± standard deviation, and an independent sample t-test is used. It is found that in the anesthesia recovery assessment of the two groups of patients, the vital signs of the patients in the observation groups were significantly better than those in the control group. In addition, the blood pressure, consciousness, and breathing and activity scores of the observation group were significantly higher than those of the control group (P<0.05). |
Comparison of Lumbar Spine Function and Pain Level
Prior to nursing care, there was no significant difference in lumbar spine function and the degree of pain between the two groups (P>0.05). After nursing care, the JOA score of the observation group was higher than that of the control group; however, the NRS score of the observation group was significantly lower than that of the control group (P<0.05). See Figure 2.
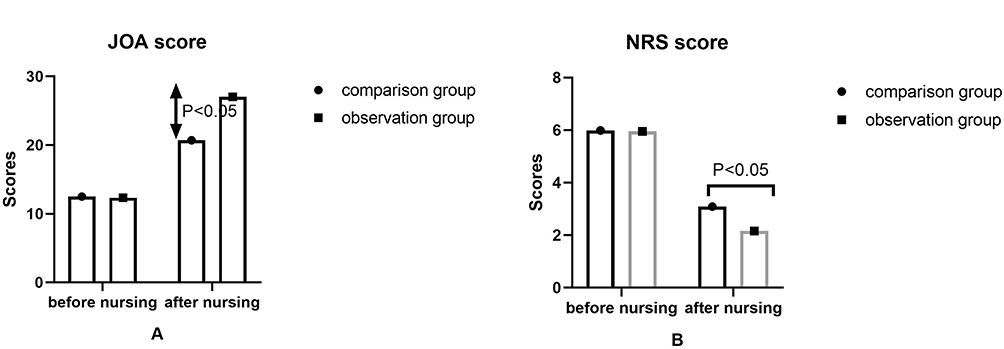 |
Figure 2 Comparison of lumbar spine function and pain level. This study uses SPSS 23.0 statistical software to conduct statistical analysis and calculation on the comparison data of lumbar spine function and pain level. Measurement data are expressed as mean ± standard deviation, and independent sample t-test is used. Before nursing care, there was no significant difference in lumbar spine function and degree of pain between the two groups (P>0.05). After nursing care, the JOA score of the observation group was significantly higher than that of the control group; however, the NRS score of the observation group was significantly lower than that of the control group (P<0.05). |
Nursing Effect Analysis
Prior to nursing care, there was no significant difference in the nursing effect scores between the two groups (P>0.05). After nursing care, the physical comfort, emotional state, psychological support, self-care ability, and pain scores were higher in the observation group than in the control group; however, the NRS score of the observation group was significantly lower than that of the control group (P<0.05). See Figure 3.
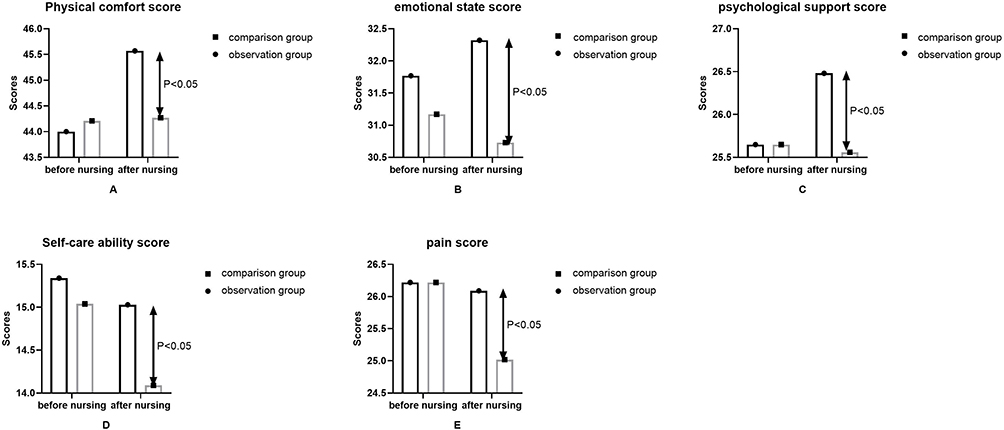 |
Figure 3 Nursing effect analysis. This study uses SPSS 23.0 statistical software to conduct statistical analysis and calculation on the nursing effect analysis data. Measurement data are expressed as mean ± standard deviation, and independent sample t-test is used. There was no statistical difference in the effect scores (P>0.05). After nursing care, the physical comfort, emotional state, psychological support, self-care ability, and pain scores of the observation group were significantly higher than those of the control group; however, the NRS score of the observation group was significantly lower than that of the control group (P<0.05). |
Discussion
LDH is a common orthopedic disease. The main clinical symptoms of the disease are lower back and radiating pain in the lower extremities. Most patients suffer from repeated illnesses and a long course of disease, which affects their normal work and life. These patients usually require surgical treatment.11 The incidence of LDH increases with the age of the population, and its pathogenesis includes a series of lumbar symptoms and diseases due to the rupture and degeneration of the intervertebral disc, herniation of the nucleus pulposus lamina, and pressing and chasing other tissues.12 Damage to the lumbar spine leads to limited physical activity.13 Changes in the spinal curve can only alleviate the condition and correct the deformed spine, even with the best treatment plan.14 At present, the surgical treatment method for LDH is mainly conventional surgery, and the curative effect is positive; however, the surgical trauma is large, and the postoperative recovery of patients is slow.15 Preventive nursing refers to the use of professional knowledge by nurses to conduct an overall assessment of the patient during or prior to nursing work and to predict the patient’s condition, disease development, and risk factors.16 According to the degree of risk of the predicted results, preventive nursing also includes providing targeted care, nursing measures in line with clinical prediction as soon as possible, minimizing the risk index of patients, improving nursing efficiency, and achieving the nursing goal of prevention before disease.17 In addition, preventive nursing intervention is a method of predicting potential risks and proposing effective nursing programs based on the laws of disease development and change.18 Preventive nursing interventions contribute to the health of patients transform the status of nursing work from passive into active, stimulate the work motivation of nursing staff, and highlight the independent value of nursing work.19 In addition, preventive nursing interventions improve the pertinence of nurses’ work and help reduce medical costs. Preventive nursing interventions change the concept of clinical nursing from an ideological perspective and promote high-quality service.20 Through the management of preventive nursing interventions during the entire operation, itinerant nurses provide a more humanized communication method, soothe the patient’s emotions, and improve the sense of security and trust.21 In preventive nursing intervention, there should be preoperative psychological adjustment to reduce the patient’s nervousness about surgery and shorten the distance between nurses and patients, which helps achieve the ideal effect of the interventions.22
This study found that the scores of the two groups of patients in the anesthesia recovery assessment were significantly better than those of the control group, and the blood pressure, consciousness, breathing, and activity scores of the observation group were higher than those of the control group. The results showed that anesthesia care integration combined with preventive nursing intervention can slow down the cardiovascular response of surgical patients due to stress, reduce fluctuations in blood pressure and heart rate, and stabilize postoperative indicators and vital signs. Studies have found that surgery can lead to anxiety, restlessness, tension, and other negative emotions in patients, resulting in sympathetic-adrenal stress, which increases the excitability of the midframe nervous system.23–27 It manifests as increased blood pressure, increased heart rate, and, in severe cases, arrhythmia and hypertension, resulting in increased postoperative instability.28 Predictive nursing requires nurses to determine the influencing factors and causes of a patient’s condition according to the actual situation of the patient after analyzing the patient’s condition as a whole, predict nursing problems that will likely occur, and provide a scientific and reasonable nursing plan.29 In specific nursing operations, in addition to implementing nursing routines and related medical fraud, nurses should interact with patients, focus on their psychological conditions, and at the same time publicize and guide relevant knowledge of the disease to improve patients’ self-protection awareness.30
Furthermore, this study found that the JOA score of the observation group after nursing care was higher than that of the control group; however, the NRS score of the observation group was lower than that of the control group. This indicates that the nursing staff had implemented preventive nursing measures for the patients in the observation group, which not only effectively reduced the pain of the patients but also improved their lumbar spine function. The QoR-40 scale achieved satisfactory results, and it has been further upgraded.31 Relevant studies have verified that the QoR-40 questionnaire can help measure the recovery of postoperative anesthesia in clinical practice.32,33 Some scholars reviewed the use, effect, and discrimination of the questionnaire and believed that it was a relatively thorough psychological measurement tool, which had certain guiding and clinical values.34,35
This study has several limitations. The number of samples selected in the study is relatively small, and all cases are from the same medical institution. The study and follow-up time are short. Data of the study are obtained from the collection and arrangement of the scale, results of blood sample testing, and ultrasound diagnosis, which may have unpredictable influence of other subjective and objective factors.
Conclusions
Anesthesia care integration combined with preventive nursing has a significant effect on patients with perioperative LDH. It significantly improves lumbar spine function, reduces pain, and helps shorten the recovery time. Furthermore, it is beneficial to the physical and mental health of patients.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Wuhan Fourth Hospital ethics approval and consent (No. KY2022-073-01). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Kim JH, van Rijn RM, van Tulder MW, et al. Diagnostic accuracy of diagnostic imaging for lumbar disc herniation in adults with low back pain or sciatica is unknown; a systematic review. Chiropr Man Therap. 2018;26:37. PMID: 30151119; PMCID: PMC6102824. doi:10.1186/s12998-018-0207-x
2. Yan S, Taotao T, Shunwei Y, Haitao L, Cheng C, Khalaf OI. Cervical spondylopathy and lumbar intervertebral disc herniation coexist in free radical metabolism and focus separation in the body. J Healthc Eng. 2021;2021:1480282. PMID: 34873436; PMCID: PMC8643231. doi:10.1155/2021/1480282
3. Chu ECP, Wong AYL. Chronic orchialgia stemming from lumbar disc herniation: a case report and brief review. Am J Mens Health. 2021;15(3):15579883211018431. PMID: 34027733; PMCID: PMC8141999. doi:10.1177/15579883211018431
4. Postacchini F, Postacchini R. Operative management of lumbar disc herniation: the evolution of knowledge and surgical techniques in the last century. Acta Neurochir Suppl. 2011;108:17–21. PMID: 21107933. doi:10.1007/978-3-211-99370-5_4
5. Yang S, Shao Y, Yan Q, Wu C, Yang H, Zou J. Differential diagnosis strategy between lower extremity arterial occlusive disease and lumbar disc herniation. Biomed Res Int. 2021;2021:6653579. PMID: 33884268; PMCID: PMC8041544. doi:10.1155/2021/6653579
6. van der Windt DA, Simons E, Riphagen II, et al. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst Rev. 2010;2:CD007431. PMID: 20166095. doi:10.1002/14651858.CD007431.pub2
7. Huang CY, Tsai HW, Liu CY, et al. The predictive and prognostic role of hematologic and biochemical parameters in the emergency department among coronavirus disease 2019 patients. Chin J Physiol. 2021;64(6):306–311. PMID: 34975124. doi:10.4103/cjp.cjp_77_21
8. Wang L, Chen J, Zhao J, et al. The predictive role of lymphocyte subsets and laboratory measurements in COVID-19 disease: a retrospective study. Ther Adv Respir Dis. 2021;15:17534666211049739. PMID: 34632871; PMCID: PMC8512232. doi:10.1177/17534666211049739
9. Marais LC, Bertie J, Rodseth R, Sartorius B, Ferreira N. Pre-treatment serum lactate dehydrogenase and alkaline phosphatase as predictors of metastases in extremity osteosarcoma. J Bone Oncol. 2015;4(3):80–84. PMID: 26587373; PMCID: PMC4648997. doi:10.1016/j.jbo.2015.09.002
10. Zhang J, Zhang F, Zhang F, Wu H, Zhang B, Wu X. Correlation between promoter methylation of the LDH-C4 gene and DNMT expression in breast cancer and their prognostic significance. Oncol Lett. 2022;23(1):35. PMID: 34966451; PMCID: PMC8669647. doi:10.3892/ol.2021.13153
11. Al Nezari NH, Schneiders AG, Hendrick PA. Neurological examination of the peripheral nervous system to diagnose lumbar spinal disc herniation with suspected radiculopathy: a systematic review and meta-analysis. Spine J. 2013;13(6):657–674. PMID: 23499340. doi:10.1016/j.spinee.2013.02.007
12. Karimi N, Akbarov P, Rahnama L. Effects of segmental traction therapy on lumbar disc herniation in patients with acute low back pain measured by magnetic resonance imaging: a single arm clinical trial. J Back Musculoskelet Rehabil. 2017;30(2):247–253. PMID: 27636836. doi:10.3233/BMR-160741
13. Xu J, Ding X, Wu J, et al. A randomized controlled study for the treatment of middle-aged and old-aged lumbar disc herniation by Shis spine balance manipulation combined with bone and muscle guidance. Medicine. 2020;99(51):e23812. PMID: 33371159; PMCID: PMC7748321. doi:10.1097/MD.0000000000023812
14. Zhang R, Zhang SJ, Wang XJ. Postoperative functional exercise for patients who underwent percutaneous transforaminal endoscopic discectomy for lumbar disc herniation. Eur Rev Med Pharmacol Sci. 2018;22(1 Suppl):15–22. PMID: 30004565. doi:10.26355/eurrev_201807_15354
15. Wang L, He T, Liu J, et al. Revealing the immune infiltration landscape and identifying diagnostic biomarkers for lumbar disc herniation. Front Immunol. 2021;12:666355. PMID: 34122424; PMCID: PMC8190407. doi:10.3389/fimmu.2021.666355
16. Demirel A, Yorubulut M, Ergun N. Regression of lumbar disc herniation by physiotherapy. Does non-surgical spinal decompression therapy make a difference? Double-blind randomized controlled trial. J Back Musculoskelet Rehabil. 2017;30(5):1015–1022. PMID: 28505956. doi:10.3233/BMR-169581
17. Rogerson A, Aidlen J, Jenis LG. Persistent radiculopathy after surgical treatment for lumbar disc herniation: causes and treatment options. Int Orthop. 2019;43(4):969–973. PMID: 30498910. doi:10.1007/s00264-018-4246-7
18. Yang B, Wang X, Li Y, et al. A newly established severity scoring system in predicting the prognosis of patients with severe fever with thrombocytopenia syndrome. Tohoku J Exp Med. 2017;242(1):19–25. PMID: 28496029. doi:10.1620/tjem.242.19
19. Lv B, Zhang Y, Yuan G, et al. Establishment of a nomogram model for predicting adverse outcomes in advanced-age pregnant women with preterm preeclampsia. BMC Pregnancy Childbirth. 2022;22(1):221. PMID: 35305610; PMCID: PMC8933958. doi:10.1186/s12884-022-04537-x
20. Cole A, Arthur A, Seymour J. Comparing the predictive ability of the Revised Minimum Dataset Mortality Risk Index (MMRI-R) with nurses’ predictions of mortality among frail older people: a cohort study. Age Ageing. 2019;48(3):394–400. PMID: 30806455. doi:10.1093/ageing/afz011
21. Kirchberg FF, Grote V, Gruszfeld D, et al.; European Childhood Obesity Trial Study Group. Are all breast-fed infants equal? Clustering metabolomics data to identify predictive risk clusters for childhood obesity. J Pediatr Gastroenterol Nutr. 2019;68(3):408–415. PMID: 30358737. doi:10.1097/MPG.0000000000002184
22. Ballesta-Castillejos A, Gómez-Salgado J, Rodríguez-Almagro J, Hernández-Martínez A. Development and validation of a predictive model of exclusive breastfeeding at hospital discharge: retrospective cohort study. Int J Nurs Stud. 2021;117:103898. PMID: 33636452. doi:10.1016/j.ijnurstu.2021.103898
23. Gabay ZP, Gondwe KW, Topaz M. Predicting risk for early breastfeeding cessation in Israel. Matern Child Health J. 2022;26(6):1261–1272. PMID: 34855056. doi:10.1007/s10995-021-03292-3
24. Yokota S, Ohe K. Construction and evaluation of FiND, a fall risk prediction model of inpatients from nursing data. Jpn J Nurs Sci. 2016;13(2):247–255. PMID: 27040735. doi:10.1111/jjns.12103
25. Rossello X, Dorresteijn JA, Janssen A, et al. Risk prediction tools in cardiovascular disease prevention: a report from the ESC Prevention of CVD Programme led by the European Association of Preventive Cardiology (EAPC) in collaboration with the Acute Cardiovascular Care Association (ACCA) and the Association of Cardiovascular Nursing and Allied Professions (ACNAP). Eur J Cardiovasc Nurs. 2019;18(7):534–544. PMID: 31234638. doi:10.1177/1474515119856207
26. Song W, Kang MJ, Zhang L, et al. Predicting pressure injury using nursing assessment phenotypes and machine learning methods. J Am Med Inform Assoc. 2021;28(4):759–765. PMID: 33517452; PMCID: PMC7973453. doi:10.1093/jamia/ocaa336
27. Naberhuis J, Wetzel C, Tappenden KA. A novel neonatal feeding intolerance and necrotizing enterocolitis risk-scoring tool is easy to use and valued by nursing staff. Adv Neonatal Care. 2016;16(3):239–244. PMID: 26825014. doi:10.1097/ANC.0000000000000250
28. Lee EO, Ahn SH, You C, et al. Determining the main risk factors and high-risk groups of breast cancer using a predictive model for breast cancer risk assessment in South Korea. Cancer Nurs. 2004;27(5):400–406. PMID: 15525868. doi:10.1097/00002820-200409000-00010
29. Breckenridge DM, Wolf ZR, Roszkowski MJ. Risk assessment profile and strategies for success instrument: determining prelicensure nursing students’ risk for academic success. J Nurs Educ. 2012;51(3):160–166. PMID: 22233161. doi:10.3928/01484834-20120113-03
30. Harris J, Purssell E, Ream E, Jones A, Armes J, Cornelius V. How to develop statistical predictive risk models in oncology nursing to enhance psychosocial and supportive care. Semin Oncol Nurs. 2020;36(6):151089. PMID: 33223408. doi:10.1016/j.soncn.2020.151089
31. Bayramoğlu BG, Akyüz N. Investigation of preoperative fasting time and preoperative and postoperative well-being of patients. Florence Nightingale J Nurs. 2022;30(1):33–39. PMID: 35635345; PMCID: PMC8958228. doi:10.5152/FNJN.2022.21047
32. Kamiya Y, Hasegawa M, Yoshida T, Takamatsu M, Koyama Y. Impact of pectoral nerve block on postoperative pain and quality of recovery in patients undergoing breast cancer surgery: a randomised controlled trial. Eur J Anaesthesiol. 2018;35(3):215–223. PMID: 29227351. doi:10.1097/EJA.0000000000000762
33. Araya K, Fukuda M, Mihara T, Goto T, Akase T. Association between anxiety and depressive symptoms during prehospitalization waiting period and quality of recovery at postoperative day 3 in perioperative cancer patients. J Perianesth Nurs. 2022;37(5):654–661. PMID: 35589499. doi:10.1016/j.jopan.2021.11.007
34. Yun S, Jo Y, Sim S, et al. Comparison of continuous and single interscalene block for quality of recovery score following arthroscopic rotator cuff repair. J Orthop Surg. 2021;29(1):2309. PMID: 33745379. doi:10.1177/23094990211000142
35. Gümüs K. The effects of preoperative and postoperative anxiety on the quality of recovery in patients undergoing abdominal surgery. J Perianesth Nurs. 2021;36(2):174–178. PMID: 33640291. doi:10.1016/j.jopan.2020.08.016
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.