")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Analysis of the incidence of postintubation injuries in patients intubated in the prehospital or early hospital conditions of the hospital emergency department and the intensive care unit
Authors Cierniak M, Timler D, Sobczak R, Wieczorek A, Sekalski P, Borkowska N, Gaszynski T
Received 9 June 2015
Accepted for publication 17 July 2015
Published 1 October 2015 Volume 2015:11 Pages 1489—1496
DOI https://doi.org/10.2147/TCRM.S90181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh

Marcin Cierniak,1 Dariusz Timler,1 Renata Sobczak,1 Andrzej Wieczorek,2 Przemyslaw Sekalski,3 Natalia Borkowska,2 Tomasz Gaszynski1
1Department of Emergency Medicine and Disaster Medicine, Barlicki University Hospital, 2Department of Anesthesiology and Intensive Therapy, Medical University of Lodz, 3Department of Microelectronics and Computer Science, IT Centre, Lodz University of Technology, Lodz, Poland
Background: Intubation is still one of the best methods to secure the airway. In the case of prehospital or early hospital conditions when factors such as urgency, stress, or inaccuracy of the undertaken activities are involved, the risk of causing complications, for instance, edema or postintubation injuries, increases, especially while dealing with a difficult intubation. The risk of improper inflation of the endotracheal tube cuff also increases, which is considered in this study.
Objective: The aim of this study was to evaluate the prevalence of postintubation complications, such as postintubation injuries or edema, in a research sample, and to examine whether such complications occur more often, for example, while using a guidewire. In this study, we also evaluated the injuries associated with the inflation of the endotracheal tube cuff.
Materials and methods: This study was performed on a group of 153 patients intubated in prehospital conditions. The tests were carried out in three clinical sites that received patients from prehospital care. Postintubation injuries were revealed and photographed using videolaryngoscope, such as the C-MAC and the McGrath series 5. The endotracheal tube cuff pressure was measured using a pressure gage manual (VBM Medizintechnik GmbH). The quantitative analyses of differences between incidence of variables were assessed using χ2 test for P<0.05. Analyses have been carried out using the Statistica software.
Results: In the group of 153 patients, postintubation injuries occurred in 17% of cases. The dependency between using the guidewire and the occurrence of the hematomas and loss of mucosa was statistically significant (P<0.01). In nearly half (42%) of the patients the endotracheal tube cuff pressure was excessively inflated over 30 cm H2O, and in two cases, endotracheal tube displacement was observed on account of poor cuff inflation (<20 cm H2O).
Conclusion: The highest percentage of overfilled cuffs were observed in the admission room. In the other wards, it was observed in 25% of cases. Even though only six cases of poor cuff inflation were noticed, the relationship between the leakage and the clinical conditions of patients is worth examining. The results would help in taking additional measures to reduce the risk of complications.
Keywords: postintubation injuries, postintubation edema, endotracheal tube cuff pressure
Introduction
Endotracheal intubation is the most effective method of airway management. It provides the most effective protection against complications such as regurgitation or hypoxemia.1 Intubation performed in prehospital (at the site of the event) and early hospital conditions (the hospital emergency department or in the intensive care unit [ICU]) was our scope of interest. Immediate prehospital intubation is a well-known standard procedure, although it is related to a greater number of complications.2 It is not uncommon for medical rescue teams not to intubate the patient as patient’s condition did not require it at that particular moment. In such cases, intubation occurs in the hospital emergency department or in the admission room immediately upon the arrival of the patient, which also increases the risk of complications, including mechanical damage to the airways, hematomas, damage to the vocal cords, damage to teeth, and aspiration of gastric contents.3,4 Among the reasons for mechanical damage of the upper respiratory tract, we should enumerate several intubation attempts, using guidewires which because of incorrectly adjusted length may protrude outside the distal part of the tube as well as modifying the tube’s location without prior cuff’s deflation and using too large size of the endotracheal tube.5 The improper cuff inflation should also be taken into consideration. The optimal level of endotracheal tube cuff inflation monitored by the anesthetic care team is related to lower risk of complications related to intubation.6,7 Too low a air pressure level in the endotracheal tube cuff, ie, <20 cm H2O, can lead to unplanned extubation, movement of the endotracheal tube into one of the bronchi, or gastric content aspiration to the respiratory tract.8,9 Pressure >30 cm H2O may lead to ischemic damage of the tracheal mucosa, resulting in tracheal stenosis, tracheal rupture, tracheoesophageal fistula, or hemorrhage.7,10 During the intubation, the endotracheal tube sealing cuff is almost always inflated using the disposable syringes and the cuff pressure is controlled by subjective assessment of the pilot balloon inflation performed by the person who intubates the patient and assists. This may entail many threatening complications for the intubated patient. Cuff inflation should be monitored with a pressure gage manual or continuous monitoring of sealing cuff pressure.11–13 The aim of this study was to evaluate the prevalence of postintubation complications, such as injuries or edemas, in the research sample and to examine whether postintubation injuries occur more often while using the guidewire. An additional goal was to evaluate the sufficiency in endotracheal tube cuff inflation in the research sample. We have also examined if improper cuff inflation (eg, pressure <20 cm H2O) could cause alteration in the endotracheal tube position. In the case of any irregularities, they were corrected immediately.
Materials and methods
This study was approved by the Ethics Committee of the Medical University of Lodz. Approval number RNN/496/13/KB dated 16/07/2013. Correction to the title KB/818/14/P dated 23.09.2014. Informed consent was not obtained as the patients were unconscious. The study was conducted over the years 2013–2014. It was carried out on a group of 153 patients intubated by emergency medical service in prehospital conditions and in early hospital conditions. In these places, the performer is sometimes forced to intubate in a quick time frame and under emotional stress. This study was undertaken over three clinical sites in order to improve the reliability of the results. The first of these was at the emergency department of WSS Nicolas Copernicus Hospital in Lodz, Poland (33 patients). The second and third were from the admission room (50 patients) and ICU (70 patients), respectively, of the Barlicki University Hospital, Lodz. We have taken into consideration these sites as patients who have been intubated by a medical emergency team, or intubated shortly after admission to hospital (early hospital condition) will pass through these departments. In Poland in the aforementioned departments, intubation may only be performed by a physician. Intubated patients brought to the hospital by medical emergency teams in S-type ambulances, in which there are one physician and two paramedics, intubations were also performed by the physician. Differences in the number of patients included from each department is due to the different frequency of patients meeting inclusion criteria in the given period of time. The study was based on visualization of the laryngeal inlet performed by a person having the degree MD or PhD, at least a second degree of specialization in emergency medicine, anesthesiology, or intensive care with a minimum of 15 years work experience. In the course of investigation, different types of videolaryngoscopes were used (Table 1). These were done to compare the field of view of the laryngeal inlet in this study with that observed for other studies when the same test was performed. In order to avoid confusion between postintubation injuries and injuries that occurred due to a long-term placement of the endotracheal tube in the airway, the study was always performed within 36 hours after the intubation. Each hematoma and lesion visualized as a big local congestion of mucosa observed during videolaryngoscopy was classified as a postintubation injury. Laryngeal and esophagus edemas and also mild edema of the mucous membrane were qualified as edemas. Patients with craniofacial damage and penetrating neck injuries were excluded from the research sample because in case of such damage, a false impression of postintubation injuries could be made. After visualizing the laryngeal inlet, an assistant, ie, a member of the research team, took a photo of the laryngeal inlet and of any injuries or edemas if they had occurred. The documentation of the laryngeal inlet was created in order to compare the field of view of certain devices observed in this study with that obtained for other studies when the same test was performed. One of the parameters tested was measuring the endotracheal tube cuff inflation. Measurements were made using a pressure gage manual (VBM Medizintechnik GmbH, Sulz am Neckar, Germany) (Figure 1). The cuff pressure of 20–30 cm H2O was declared as sufficient. An additional benefit for patients was visualizing repeatedly residual foreign bodies that were not detected in the course of intubation or in standard care of upper respiratory tract. If improper endotracheal cuff inflation was noticed, it was adjusted to the correct value immediately. In addition, during each test, the patient was being suctioned from residual secretions. Quantitative differences in incidence of variables were assessed using χ2 test for P<0.05. Analyses have been carried out using the Statistica software.
 | Table 1 Examination of patients examined by using certain types of devices |
 | Figure 1 Manual pressure gage (VBM Medizintechnik GmbH, Sulz am Neckar, Germany). |
Results
The results are divided into sections according to the complications: injuries, postintubation edemas, and endotracheal tube cuff inflation.
Postintubation injuries
In the group of 153 patients, postintubation injuries occurred in 17% of all cases (26 people). We divided these injuries into four groups (Table 1). The most frequent postintubation injury was a single hematoma (Figure 2), which constituted more than a half of the injuries (Fraction [Fr] =0.54), and multiple hematomas constituting less than half of the injuries (Fr =0.38). The vast majority of the hematomas, (n=18, Fr =0.70), were localized on the soft palate close to or just on the uvula. A total of six hematomas occurred around the epiglottis. The rest of the injuries comprised of tooth damage (n=2), eg, dental extraction and upper lip damage with bleeding (Fr =0.04) (Table 2). Owing to the fact that the study was conducted at three clinical sites, the results were organized as three different groups (Figure 3). At the emergency department of Kopernik Hospital, 33 patients were examined and in only four cases did injuries occur (Fr =0.12). It was a single hematoma in all of these cases. In the ICU in Barlicki University Hospital, 70 patients were examined. The damage occurred in almost one-fifth of patients in the research group (Fr =0.23) (Figure 3). There were 16 cases, in which 12 were multi hematomas and four were single hematomas. In the admission room of Barlicki University Hospital, 50 patients were examined, with injuries occurring in six cases (Fr =0.12). There were four cases of single hematomas, a case of an extracted tooth, and a case where there was damage to the upper lip. The guidewire should be used only in the case of difficult intubation. There was not always an opportunity to contact the person who performed the intubation to check whether the guidewire was used. It was possible in 103 cases, and in other cases it was detected by the amount of equipment noted on the emergency exit card. It was not possible to verify whether the guidewire was seated properly or if it protruded outside the pipe, so the analysis about the guidewires was limited to whether it was used or not. From these 103 patients, it was discovered that there was a statistically significant relationship between the use of the guidewire and the occurrence of injuries. Test χ2=10.63 for critical values of −6.63 to 6.63 of P<0.01. Relating to the cases in which the guidewire was used, 80% of patients did not have any injuries, while in the group who operated with the guidewire, almost half of the patients (20 people) had injuries. The endotracheal tubes sized between 6 and 9 cm were used in the research group. Where the endotracheal tube size was 6.0, 6.5, and 7.0 cm, no postintubation injuries were detected. This is probably due to the fact that the smaller size tubes (6.0, 6.5, 7.0 cm) were rarely used. When endotracheal tubes of greater sizes were used, the postintubation injuries were found in 17%–25% of the patients. It may look like the tubes of a smaller size are safer, but during the analysis, there was no statistically significant dependency between the size of the endotracheal tube and the occurrence of injuries in the research group.
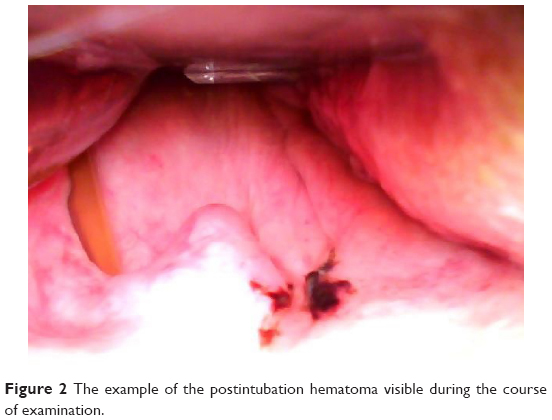 | Figure 2 The example of the postintubation hematoma visible during the course of examination. |
 | Table 2 The types and frequency of the examined postintubation injuries |
 | Figure 3 The sites where the study was conducted. |
Edemas
Almost all (except one) detected cases of edemas (n=26) occurred when previous postintubation injuries were discovered. Only in one case of edema was there no relation to prior injuries, though a statistically significant dependency between postintubation injuries and the later occurrence of edemas was shown (Figure 4), χ2 =139 (df=1), P<0.001. Other statistical tests are almost identical with those concerning injuries; hence, we will not describe further statistics on edemas here. However, it is worth noting that in five cases the residual foreign body that was not removed earlier by the medical personnel could be a possible reason that led to edemas (Figure 5). The edema occurred simultaneously in three out of the five cases. The research group was too small to carry out statistical analyses and draw statistically significant conclusions. In all of these five cases, patients were examined during the first 24 hours after intubation, and those having an edema were also diagnosed with hematomas and some lesions in the mucous membrane at the same time. There is no evidence to treat a foreign body as a reason for edema. All of the recorded foreign bodies were of organic origin, and we believed it was the last meal of the patient before intubation. No cultures were performed.
 | Figure 4 The example of postintubation edema visible during the course of the examination. |
 | Figure 5 The example of the foreign body (arrow), probably of organic origin, visible during the course of examination. |
Endotracheal tube cuff inflation
All of the 153 examined patients were divided into three groups. The first group included patients (n=6, 4%) whose air pressure in the endotracheal tube cuff was insufficient (<20 cm H2O). Among these six patients, there were two cases of endotracheal tube displacement (Figure 6), which could result in leakages. However, the number of cases was too little in order to carry out any statistical analysis. The second group consisted of patients whose air pressure was maintained within the range established as the norm (20–30 cm H2O). It constituted of more than half (54%) of the patients (n=83). The third group consisted of patients with the endotracheal tube cuff inflated with air pressure of >30 cm H2O (n= 64, 42%). The medical staff inflated the cuff with an average air pressure of 34.9±17.4 cm H2O. In the group of patients with an overinflated cuff, the medical staff used an average air pressure of 49.3±18.2 cm H2O. From the results over the individual departments, 33 patients were examined in the hospital emergency department and the vast majority of them (Fr =0.72) had correctly inflated cuffs with an air pressure value of 20–30 cm H2O. The vast minority of cuffs was inflated incorrectly. The other values present as follows. The values >30 cm H2O, Fr=0.24, and values of <20 cm H2O were Fr=0.03. A total of 70 patients were examined in the ICU, and in a greater number of these cases, the cuffs were inflated correctly (Fr =0.62). Meanwhile, in the admission room of the same hospital, 50 patients were examined and only in one case (Fr =0.02), the cuff was not sufficiently inflated (15 cm H2O), while the vast majority of patients (Fr =0.8) had overinflated cuffs (average 56.3±19.5 cm H2O). Only a small fraction (Fr =0.18) had a cuff with air pressure within the accepted normal range (Figure 7).
 | Figure 6 The endotracheal tube displacement probably due to the insufficient cuff inflation. |
 | Figure 7 The air pressure in the endotracheal tube cuff depending on the department. |
Discussion
Injuries and edemas
The vast majority of injuries detected in our study were the single esophageal hematoma and mucous membranes lesions. This is a known complication of intubation, but rarely described in the literature.14,15 While searching for literature, we found that the extensive studies focused on minor injuries, such as small hematomas and mucous membranes lesions. Most of the considered injury literature was based on case reports. Esophageal hematomas may arise spontaneously, but more often they appear as a result of injuries, particularly iatrogenic.16,17 The lack of knowledge and experience in intubation was indicated to have a direct impact on the quantity of injuries.3,18 It was not possible to check the number of years work experience for each person performing intubation, but we were able to confirm that all the operators were doctors working in the units mentioned earlier, or were doctors from the emergency medical services team. Despite the fact that it was not possible to collect all the data from the 153 patients for our study, the use of the guidewire was indicated as a statistically significant variable. We were unable to determine the exact cause of this relationship. However, it should be noted that in the course of intubation performed in emergency conditions, there is a risk of the guidewire being positioned improperly in the tube due to stress, urgency, or sometimes even due to the hostile environment at the site of the event.19 Accompanied by such factors, it is possible that the guidewire positioned incorrectly may protrude slightly beyond the tube, which can lead to additional risk.5,18 The improper use of the guidewire and the possible displacement of the endotracheal tube without prior cuff deflation are indicated in the literature as the causes of the mucosal damage.20 It is suggested in the literature that the difficult intubation increases the risk of injuries depending on the endotracheal tube size.21 There was no such dependency observed in our research sample. In literature referring to the occurrence of edemas, there were some single-case reports describing the esophageal edema caused by the residual foreign body, which was food that the patient had recently eaten.22,23 In five cases in the research group, foreign bodies of organic origin were found. We have not done inoculation, and the sample was too small to determine the dependency between edema and the detected foreign bodies. There was edema observed in three out of five cases. Simultaneously, it appeared with losses in the mucosa caused by intubation. Therefore, there is no basis for the inference that it was a foreign body that resulted in edema in such a short time after intubation (<24 hours). Owing to the fact that in almost every case of injury or loss in the mucous membrane resulted in edema, it can be assumed that the injuries actually led to edema in the research group.
Pressure in the endotracheal tube cuff
In the literature, there are plenty of studies confirming the fact that there is a relationship between the air pressure in the endotracheal tube cuff and the incidence of postintubation complications.10,24–25,28 The insufficient inflation off the endotracheal tube cuff may increase the risk of various complications, among which are losses in tracheal mucosa and its inlet.20 In our study, we noted two cases of the endotracheal tube spontaneous movement due to insufficient inflation of the endotracheal tube cuff (Figure 6). Inflating the cuff with pressure <20 cm H2O increases the risk of the endotracheal tube displacement in the airway.8,9 There were too few cases to carry out any statistical analysis. Owing to the nature of the study, we were not able to assess whether there was any damage to the mucosa distal from the entrance to the larynx. In this trial, less than a half of the cuffs (42%) were filled with pressure exceeding the upper limit of normal. Published studies confirm the tendency to overinflate the cuff by medical personnel.12,29,30 This phenomenon bears significant consequences in long-term intubation, but it is also dangerous in the case of short-term intubation. Irreversible complications are possible in both cases.6,10,28 In our study, the highest percentage of overinflated cuff was observed in the admission room, the place where patients are either brought to by medical rescue teams or intubated shortly after arrival. In both cases, when factors such as stress and rushed conditions should be considered, the cuff palpation is very difficult.3,4,31 It is known that if the assessment of the endotracheal tube cuff inflation performed by the medical staff is based only on palpation, it is much harder to obtain the correct air pressure. Monitoring the correct pressure is definitely easier while using a manometer manual or continuous monitoring.12,13,26,27,32–34 Taking this fact into consideration, and above all, bearing the safety of the intubated patient in mind, we believe that it would be worthwhile to check the air pressure gage manually after each successful attempt at intubation. Perhaps this would help to avoid dangerous health complications.
Limitations
One of the limitations could be the fact that due to the use of the videolaryngoscopes, there was no opportunity to assess postintubation injuries located below the laryngeal inlet. For this purpose, bronchoscopes ought to be used, but they were not taken into consideration during the planning of this research because we wanted to concentrate on videolaryngoscopes. It is also possible that some part of the mucous membrane lesions, hematomas, and edemas occurred as a result of insufficient suction. If such insufficient suction had taken place before our study, we would not be able to determine whether this was indeed the injury after intubation or if it was caused by another reason. It was not possible to verify whether the guidewire protruded outside the endotracheal tube, so the analysis about the guidewires was limited up to the fact of whether it was used or not.
Conclusion
Each medical personnel should try to reduce postintubation injuries. The percentage of 17 for the injuries and swellings among the tested samples is distressingly high even if prehospital or early hospital intubations were considered. Medical personnel have had a tendency to overinflate the endotracheal tube cuff. Almost half (42%) of the patients had overinflated cuffs. Mean values achieved were 34.9±17.4 cm H2O, and the maximum was close to 74 cm H2O, which increases the risk of complications. The highest percentage of overfilled cuffs were observed in the admission room. Appropriate actions should be taken to reduce the risk of complications occurring in prehospital intubation, taking into consideration every examined aspect.
Despite detecting only two cases of displacement of the endotracheal tube, most likely caused by insufficient inflation of the endotracheal tube cuff, it would be worthwhile to carry out further tests in order to check whether the resulting leakages did not affect the clinical status of patients.
Acknowledgment
Work was conducted by Medical University of Lodz, Poland, grant no. 502-03/6-010-02/502-64-077.
Disclosure
The authors report no conflicts of interest in this work.
References
Raum M, Buchheisler B. The role of prehospital hypotension and respiratory dysfunction – results of epidemiological study. Abstracts of the 5th International Neurotrauma Symposium 2000. Rest Neurol Neurosci. 2000;16:265. | ||
Block E, Cheatham M, Parrish G, Nelson L. Ingested endotracheal tube in an adult following intubation attempt for head injury. Am Surg. 1999;65:1134–1136. | ||
Nolan J. Prehospital and resuscitative airway care: should the gold standard be reassessed? Curr Opin Crit Care. 2001;7:413–421. | ||
Murphy MF, Walls RM. The Difficult and Failed Airway. Manual of Emergency Airway Management. Philadelphia: Lippincott Williams and Wilkins; 2000:31–39. | ||
Weissbrod PA, Merati AL. Reducing injury during video-assisted endotracheal intubation: the “smart stylet” concept. Laryngoscope. 2011;121(11):2391–2393. | ||
Spittle N, McCluskey A. Tracheal stenosis after intubation. BMJ. 2000;321:1000–1002. | ||
Curiel Garcia JA, Guerrero-Romero F, Rodriguez-Moran M. Cuff pressure in endotracheal intubation: should it be routinely measured? Gac Med Mex. 2000;137:179–182. | ||
Hameed AA, Hasan M, Motasem AM. Acquired tracheoesophageal fistula due to high intracuff pressure. Ann Thorac Med. 2008;3: 23–25. | ||
Nseir S, Brisson H, Marquette CH, et al. Variations in endotracheal cuff pressure in intubated critically ill patients: prevalence and risk factors. Eur J Anaesthesiol. 2009;26:229–234. | ||
De S, De S. Post intubation tracheal stenosis. Indian J Crit Care Med. 2008;12:194–197. | ||
Sole ML, Aragon D, Bennett M, Johnson RL. Continuous measurement of endotracheal tube cuff pressure: how difficult can it be? AACN Adv Crit Care. 2008;19:235–243. | ||
Sengupta P, Sessler DI, Maglinger P, et al. Endotracheal tube cuff pressure in three hospitals, and the volume required to produce an appropriate cuff pressure. BMC Anesthesiol. 2004;4:8. | ||
Sole ML, Penoyer DA, Su X, et al. Assessment of endotracheal cuff pressure by continuous monitoring: a pilot study. Am J Crit Care. 2009;18:133–143. | ||
Wang AY, Riordan RD, Yang N, Hiew CY. Intramural hematoma of the esophagus presenting as an unusual complication of endotracheal intubation. Australas Radiol. 2007;51:260–264. | ||
Hrvoje I, Marina PI. Intramural esophageal hematoma: an unusual complication of endotracheal intubation. J Emerg Med. 2013;44(1):89–90. | ||
Younes Z, Johnson D. The spectrum of spontaneous and iatrogenic esophageal injury: perforations. J Clin Gastroenterol. 1999;29:306–317. | ||
Cullen SN, McIntyre AS. Dissecting intramural hematoma of the esophagus. Eur J Gastroenterol Hepatol. 2000;12:1151–1162. | ||
Jougon J, Ballester M, Choukroun E, Dubrez J, Reboul G, Velly JF. Conservative treatment for postintubation tracheobronchial rupture. Ann Thorac Surg. 2000;69:216–220. | ||
Eckstein M, Chan L, Schneir A, Palmer R. Effect of prehospital advanced life support on outcomes of major trauma patients. J Trauma. 2000;48:643–648. | ||
Marty-Ané CH, Picard E, Jonquet O, Mary H. Membranous tracheal rupture after endotracheal intubation. Ann Thorac Surg. 1995;60(5):1367–1371. | ||
Horton CL, Brown CA, Raja AS. Trauma airway management. J Emerg Med. 2014;46(6):814–820. | ||
Canji K, Mitrović SM, Jovancević L. Complicated hypopharyngeal perforation caused by a foreign body. Med Pregl. 2007;60(7–8):391–396. | ||
Asif M, Shah SA, Khan F, Ghani R. Foreign body inhalation site of impaction and efficacy of rigid bronchoscopy. J Ayub Med Coll Abbottabad. 2007;19(2):46–48. | ||
Akadiri OA, Olusanya AA, Sotunmbi P. Predictive variables for difficult intubations in oral and maxillofacial surgery. J Maxillofac Oral Surg. 2009;8(2):154–159. | ||
Biro P, Weiss M, Gerber A, Pasch T. Comparison of a new video-optical intubation stylet versus the conventional malleable stylet in simulated difficult tracheal intubation. Anaesthesia. 2000;55(9):886–889. | ||
Reed MJ. Can an airway assessment score predict difficulty at intubation in the emergency department? Emerg Med J. 2005;22:99–102. | ||
Peter B. A topographically oriented, simple and informative formula to describe a difficult airway: F.R.O.N.T. Anaesthesiol Rescue Med. 2012;6:182–187. | ||
Silva MJ, Aparício J, Mota T, Spratley J, Ribeiro A. Ischemic subglottic damage following a short-time intubation. Eur J Emerg Med. 2008;15:351–353. | ||
Wujtewicz MA, Sawicka W, Bukowska A, Owczuk R, Wujtewicz M. Relation of the pressure in the cuff of endotracheal tube vs time in practice and experience of anaesthetist. Anaesthesiol Rescue Med. 2003;35:281–284. | ||
Wujtewicz MA, Sawicka W, Owczuk R, Dylczyk-Sommer A, Wujtewicz M. Tracheal tube cuff pressure depends on the anaesthesiologist’s experience. A follow-up study. Anaesthesiol Rescue Med. 2009;41: 205–208. | ||
Maboudi A, Abtahi H, Hosseini M, Tamadon A, Safavi E. Accuracy of endotracheal tube cuff pressure adjustment by fingertip palpation after training of intensive care unit nurses. Iran Red Crescent Med J. 2013;15(5):381–384. | ||
Galinski M, Treoux V, Garrigue B, Lapostolle F, Borron SW, Adnet F. Intracuff pressure of endotracheal tubes in the management of airway emergencies: the need for pressure monitoring. Ann Emerg Med. 2006;47:545–547. | ||
Hoffman RJ, Parwani V, Hahn I. Experienced emergency medicine physicians cannot safely inflate or estimate endotracheal tube cuff pressure using standard techniques. Am J Emerg Med. 2006;24:139–143. | ||
Duguet A, D’Amico L, Biondi G, Prodanovic H, Gonzalez-Bermejo J, Similowski T. Control of tracheal cuff pressure: a pilot study using a pneumatic device. Intensive Care Med. 2007;33:128–132. | ||
Gaszynski T. Clinical experience with the C-Mac videolaryngoscope in morbidly obese patients. Anaesthesiol Intensive Ther. 2014;46(1):14–16. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.