Back to Journals » Orthopedic Research and Reviews » Volume 17
Analysis of the Effect of Integrated Orthopedic Rehabilitation Programs on Elbow Joint Function Recovery After Ulnar Olecranon Fracture Surgery
Received 6 June 2025
Accepted for publication 17 November 2025
Published 6 December 2025 Volume 2025:17 Pages 573—581
DOI https://doi.org/10.2147/ORR.S545214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Xu Hu,1 Zhuojin Wu,2 Shangtuan Zheng1
1Department of Orthopedics, the Affiliated Nanping First Hospital of Fujian Medical University, Nanping, Fujian, 353000, People’s Republic of China; 2The 907th Hospital of the Joint Logistics Support Force, Nanping, Fujian, 353000, People’s Republic of China
Correspondence: Shangtuan Zheng, Email [email protected]
Objective: This study aimed to evaluate the effect of an integrated orthopedic rehabilitation program on elbow joint function recovery in patients after surgical treatment for ulnar olecranon fractures, compared to conventional rehabilitation.
Methods: A retrospective cohort study was conducted on 87 patients who underwent surgery for ulnar olecranon fractures. Based on the standard of care at the time of admission, patients were assigned to a control group (n=42) receiving conventional rehabilitation or an observation group (n=45) receiving an integrated rehabilitation program. The integrated program comprised preoperative education, standardized in-hospital training, a structured 24-week home-based protocol with phased goals, and monitored follow-up. The primary outcome was the Mayo Elbow Performance Score (MEPS). Secondary outcomes included elbow range of motion (ROM), Activities of Daily Living (ADL) score, Visual Analog Scale (VAS) for pain, and complication rates.
Results: The observation group showed a significantly higher rehabilitation effectiveness rate (97.78% vs 80.95%, p=0.026). They also achieved superior MEPS (75.31 vs 53.85, p< 0.001), ADL scores (62.64 vs 55.17, p< 0.001), and lower VAS scores (2.36 vs 4.36, p< 0.001). Elbow ROM improvements in flexion, extension, pronation, and supination were all significantly greater in the observation group (all p< 0.001). Complication rates did not differ significantly (6.67% vs 9.52%, p=0.924).
Conclusion: The integrated orthopedic rehabilitation program is superior to conventional rehabilitation in promoting functional recovery, improving range of motion, enhancing daily living activities, and alleviating pain in patients after ulnar olecranon fracture surgery. However, these findings should be interpreted with caution due to the limitations of a retrospective design and a modest sample size. Integrated rehabilitation represents a highly effective postoperative management strategy for these patients.
Keywords: integrated orthopedic rehabilitation, ulnar olecranon fracture, elbow joint, function recovery, role
Introduction
Ulnar olecranon fractures represent a prevalent orthopedic injury, accounting for approximately 10% of all fractures around the elbow.1 Given the subcutaneous location of the olecranon and its critical role in elbow stability and motion, these fractures often result from direct trauma or high-energy mechanisms, leading to significant functional impairment.2 While surgical intervention, such as tension band wiring or plate osteosynthesis, is the standard of care to restore joint anatomy and stability, the postoperative rehabilitation process is equally critical for determining long-term functional outcomes and patient quality of life.3
Conventional postoperative rehabilitation protocols typically follow a generalized, stepwise approach, focusing on early immobilization followed by gradual range-of-motion and strengthening exercises.4 Although these methods provide a foundational framework for recovery, they often lack the comprehensiveness and individualization required for optimal recovery. Limitations may include insufficient patient education, inadequate supervision during the critical home-based phase, and a lack of structured, phased goals, which can contribute to suboptimal outcomes such as persistent stiffness, pain, and diminished activities of daily living (ADL).5,6
In recent years, the concept of integrated orthopedic rehabilitation has emerged as a promising holistic approach. This model extends beyond the physical aspects of healing to encompass a multidisciplinary strategy, including preoperative education, supervised in-hospital training, structured home-based programs with clear phased goals, and continuous follow-up.7 By integrating these elements, the program aims to empower patients, enhance compliance, and provide a tailored rehabilitation pathway that adapts to the patient’s progress. Previous studies have suggested the potential benefits of such integrated care models in other musculoskeletal conditions, demonstrating improved functional scores and faster return to normal function.8,9
However, the specific application and efficacy of a comprehensive integrated rehabilitation program for patients undergoing surgery for ulnar olecranon fractures remain underexplored. There is a notable scarcity of comparative studies that systematically evaluate its impact on elbow joint function, range of motion, pain control, and daily living abilities against conventional protocols.
Therefore, this study was designed to fill this knowledge gap. We hypothesized that an integrated orthopedic rehabilitation program would be superior to conventional rehabilitation in improving functional recovery, as measured by the Mayo Elbow Performance Score, increasing elbow range of motion, enhancing daily living abilities, and reducing pain levels in patients after ulnar olecranon fracture surgery. Through this comparative analysis, we aim to provide robust evidence to guide clinical practice and optimize postoperative care pathways for this patient population.
Materials and Methods
Study Subjects
A retrospective cohort study was conducted on 87 patients who underwent surgical treatment for ulnar olecranon fractures at the Affiliated Nanping First Hospital of Fujian Medical University between January 2021 and January 2023. This study was approved by the ethics committee of the Affiliated Nanping First Hospital of Fujian Medical University. Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki. Patients were assigned to the control group (n=42) or observation group (n=45) based on the standard rehabilitation protocol in use at the time of their admission. Specifically, the control group comprised patients admitted earlier in the study period who received the conventional rehabilitation program, while the observation group consisted of patients admitted later for whom the new integrated orthopedic rehabilitation program was implemented as the standard of care. This assignment was based on the timing of admission and protocol availability, not randomization. Inclusion criteria: ① Aged 15–65 years; ② Clear trauma history with elbow swelling, tenderness, impaired mobility, palpable crepitus, and confirmed fracture on X-ray/CT; ③ Surgery performed by the same orthopedic team; ④ Willing and able to comply with postoperative rehabilitation; ⑤ Complete clinical data. Exclusion criteria: ① Concomitant joint disorders; ② Fractures involving the coronoid process, severe comminution, multiple ipsilateral fractures, or pathological fractures; ③ History of elbow deformity; ④ Severe cardiac, hepatic, or renal dysfunction; ⑤ Severe infectious, autoimmune, or allergic diseases; ⑥ Lactating or pregnant women; ⑦ Severe allergic reactions during treatment; ⑧ Neurological or psychiatric disorders; ⑨ Inability to complete rehabilitation. All 87 patients completed the 24-week follow-up without dropouts.
Methods
Sample Size Consideration
The sample size for this retrospective study (n=87) was determined by the number of eligible patients presenting during the specified two-year period. While a formal a priori power analysis was not conducted for this retrospective cohort, a post-hoc power analysis was performed using G*Power software (version 3.1.9.7). With an effect size of 0.65, an alpha level of 0.05, and sample sizes of 42 and 45, the achieved power for detecting a significant difference in the primary outcome (Mayo Elbow Performance Score) was 82%, which is considered adequate.
Control Group
Patients in the control group received conventional rehabilitation interventions. Preoperatively, they underwent routine orthopedic treatment and care. During hospitalization post-surgery, they received standard orthopedic rehabilitation treatment, including limb elevation assistance, elbow fixation using plaster or adjustable braces, administration of anti-infection and pain relief measures, symptomatic supportive treatment, and rehabilitation training after fracture stabilization. Upon routine discharge guidance, patients engaged in active limb movement training, muscle strength exercises, and activities of daily living training. Patients were provided with a home rehabilitation manual and did not receive telephone rehabilitation guidance.
Observation Group
Patients in the observation group underwent integrated orthopedic rehabilitation interventions, which were designed as a standardized protocol to ensure consistency. To minimize inter-provider variability, all rehabilitation physicians and nursing staff involved in delivering the intervention received standardized training on the protocol before the study period. A senior rehabilitation physician supervised the program to ensure adherence. The interventions included: (1) Preoperative Rehabilitation Education: Nursing staff provided detailed explanations to patients and their families regarding the surgical process, potential postoperative complications, and corresponding preventive measures to familiarize them with the rehabilitation plan. Patients were educated preoperatively on isometric muscle contraction exercises, active joint mobility training, and exercises involving unaffected joints. (2) In-Hospital Postoperative Period: Initially, patients underwent isometric contraction and proprioception training of the upper limb muscles. After discomfort subsided, they progressed to active and passive motion exercises, gradually increasing the range of motion of the affected elbow. Limb elevation was facilitated, and plaster or adjustable braces were used to fix the elbow in the flexed position. Normal function of the unaffected joints in the upper limb was maintained. (3) Pre-Discharge Guidance: Patients and their families were provided with a detailed home rehabilitation manual and instructed to follow it. Different rehabilitation objectives were set for each stage over a 24-week period: Stage 1 (from discharge to 4 weeks post-surgery): Non-weight-bearing activities for the limb, safe range-of-motion exercises for elbow flexion, extension, pronation, and supination, isometric muscle exercises, and unaffected joint activities. Stage 2 (5–8 weeks post-surgery): Building upon Stage 1, adding forearm rotation, encouraging patients to use the affected hand for simple daily activities without heavy lifting. Stage 3 (9–12 weeks post-surgery): Continuing previous exercises without weight-bearing, aiming for maximum passive elbow joint range of motion equivalent to active motion. Stage 4 (13–24 weeks post-surgery): Introducing light weight-bearing activities, continuing earlier training, incorporating moderate whole-body aerobic endurance exercises, focusing on strengthening crucial upper limb muscles, and striving for full range-of-motion elbow joint recovery to actively engage in daily life and leisure activities. (4) Other Interventions: Compliance with the home-based program was monitored through regular follow-up calls conducted by rehabilitation physicians, who also adjusted patient training plans promptly. For patients with inadequate telephone guidance or poor compliance, orthopedic or rehabilitation outpatient reviews or home visits by rehabilitation physicians were conducted for supervised rehabilitation to ensure effective patient recovery. Patient adherence to exercises was assessed during these follow-ups using a simple logbook provided to patients, where they recorded their daily exercise frequency and any difficulties encountered.
Outcome Measures
Rehabilitation Effectiveness
After 24 weeks of intervention, rehabilitation effectiveness was evaluated based on the patient’s elbow joint pain, swelling, and mobility. The clinicians assessing the outcomes were not blinded to the group allocation due to the retrospective nature of the study, which is a recognized limitation. Significant Improvement: Patients exhibited a recovery of elbow joint mobility to over 90% of normal levels post-intervention, with no significant pain or swelling. Effective: Patients achieved over 80% recovery in elbow joint mobility post-intervention, accompanied by noticeable alleviation of pain and swelling. Ineffective: Patients achieved less than 60% recovery in elbow joint mobility post-intervention, coupled with significant pain and swelling reactions.
Elbow Joint Function8
Before and after intervention, the Mayo Elbow Performance Score was used to assess patients’ elbow joint functional recovery. This scoring system involves pain (0–45 points), range of motion (0–20 points), stability (0–10 points), and daily living activities (0–25 points), with higher scores indicating better elbow joint functional recovery.
Elbow Joint Range of Motion
Before and after intervention, the elbow joint fracture motion measurement device was used to measure and record the range of motion of patients’ affected elbows concerning flexion, extension, pronation, and supination.
Activities of Daily Living9
Before and after intervention, the Activities of Daily Living (ADL) scale was employed to assess patients’ daily living abilities. The scale includes physical self-maintenance items such as dressing, toileting, eating, grooming, walking, bathing, and instrumental activities such as meal preparation, shopping, using the phone, housework, laundry, transportation, managing finances, and medication. Scores range from 0 to 100, with higher scores indicating stronger daily living abilities.
Pain Assessment10
Before and after intervention, the Visual Analog Scale (VAS) was used to evaluate the pain level of patients. Scores range from 0 to 10, with higher scores indicating more severe pain.
Incidence of Complications
Observed complications in this study include ectopic ossification, fracture displacement, joint stiffness, neurovascular injury, muscle or tendon injury, and were uniformly recorded by relevant medical staff in our hospital.
Statistical Analysis
Statistical analysis was performed using SPSS 22.0 and GraphPad Prism 8. Continuous variables were expressed as mean ± SD or median (IQR) after normality testing (Shapiro–Wilk). Between-group comparisons used t-tests or Mann–Whitney U-tests for continuous data, and chi-square or Fisher’s exact tests for categorical data. Analysis of covariance (ANCOVA) was used to compare the primary outcome (MEPS at 24 weeks), adjusting for potential confounders. A two-sided P < 0.05 was considered statistically significant.
Results
Baseline Data Comparison
The baseline characteristics of the two patient groups were comparable, showing no significant differences upon comparison (P > 0.05). Furthermore, an analysis of key comorbidities and baseline functional status (as reflected by the pre-intervention Mayo score, ADL, and VAS scores) also showed no significant differences between the groups (P > 0.05), suggesting that these potential confounding factors were balanced at baseline. Refer to Table 1 for details.
 |
Table 1 Baseline Data Comparison |
Comparison of Rehabilitation Outcomes
The rehabilitation effectiveness in the control group was 80.95%, while in the observation group, it was notably higher at 97.78% (P < 0.05). Refer to Table 2 for details.
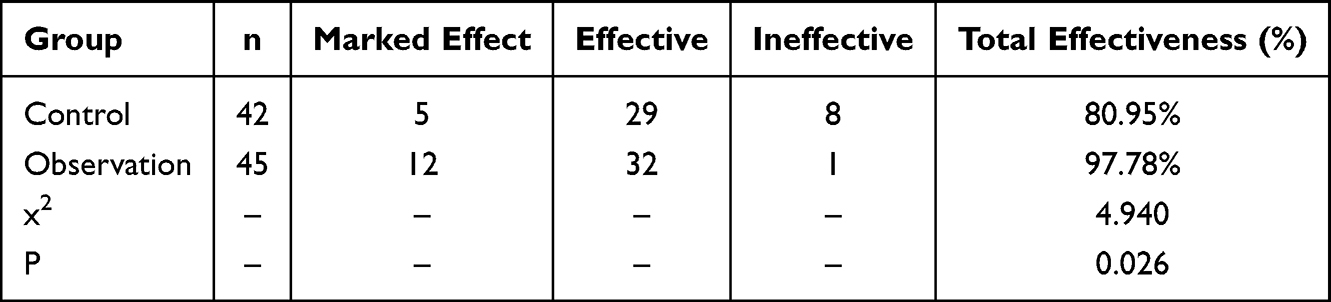 |
Table 2 Comparison of Rehabilitation Outcomes |
Comparison of Elbow Joint Function
As shown in Figure 1, before and after intervention, the pain scores in the control group were (11.57±2.85, 26.27±3.29), motion function scores were (7.89±1.64, 11.37±1.95), stability scores were (2.58±0.63, 5.32±0.81), and daily life scores were (6.25±1.27, 10.89±2.54). In the observation group, the pain scores were (11.53±2.82, 32.65±3.47), motion function scores were (7.82±1.75, 16.27±2.04), stability scores were (2.56±0.67, 7.74±0.85), and daily life scores were (6.32±1.19, 18.65±3.17). Before intervention, there was no significant difference in pain, motion function, stability, and daily life scores between the two groups (P > 0.05). After intervention, the observation group showed significantly higher scores in pain, motion function, stability, and daily life compared to the control group (P < 0.05).
 |
Figure 1 Mayo Elbow Performance Score (MEPS) components before and after intervention. Data are presented as mean ± SD. Between-group comparisons of post-intervention scores were analyzed using independent samples t-tests. *P < 0.05 indicates a statistically significant difference vs the control group. |
Comparison of Elbow Joint Range of Motion
As depicted in Figure 2, the range of motion in the control group before and after intervention was as follows: flexion (41.64±7.35, 86.59±9.23), extension (−13.27±3.45, 1.63±0.29), pronation (24.39±5.23, 41.56±5.87), and supination (29.57±6.14, 48.52±5.89). In the observation group, the range of motion before and after intervention was: flexion (42.18±7.16, 111.37±11.65), extension (−13.43±3.32, 4.84±0.81), pronation (23.65±5.61, 64.04±7.39), and supination (29.27±6.35, 57.26±6.03). Before intervention, there was no significant difference in the range of motion in flexion, extension, pronation, and supination between the two groups (P > 0.05). After intervention, the observation group exhibited significantly higher range of motion in flexion, extension, pronation, and supination compared to the control group (P < 0.05).
 |
Figure 2 Active range of motion of the elbow joint before and after intervention. Data are presented as mean ± SD. Between-group comparisons of post-intervention scores were analyzed using independent samples t-tests. *P < 0.05 indicates a statistically significant difference vs the control group. |
Comparison of Daily Life Ability and Pain Condition
As illustrated in Figure 3, before and after intervention, the ADL scores in the control group were (42.57±4.89, 55.17±4.06), and VAS scores were (7.89±0.94, 4.36±1.09). In the observation group, the ADL scores were (42.27±4.34, 62.64±5.23), and VAS scores were (8.21±0.89, 2.36±0.91). Before intervention, there was no significant difference in ADL scores and VAS scores between the two groups (P > 0.05). After intervention, the observation group showed significantly higher ADL scores and notably lower VAS scores than the control group (P < 0.05).
 |
Figure 3 Activities of Daily Living (ADL) and pain (VAS) scores before and after intervention. Data are presented as mean ± SD. Between-group comparisons of post-intervention scores were analyzed using independent samples t-tests. *P< 0.05 indicates a statistically significant difference vs the control group. |
Comparison of Complications Occurrence
The complication occurrence rate was 9.52% (4/42) in the control group and 6.67% (3/45) in the observation group. The comparison of complication occurrence rates between the two groups showed no significant difference (P > 0.05). The lack of a statistically significant difference in complication rates, despite clear differences in functional outcomes, may be attributed to the overall low incidence of complications and the study’s limited sample size, which was not powered to detect differences in rare adverse events. Please refer to Table 3 for details.
 |
Table 3 Comparison of Complication Occurrence |
Discussion
Principal Findings
This retrospective cohort study demonstrates that an integrated orthopedic rehabilitation program significantly enhances functional recovery following surgical treatment of ulnar olecranon fractures. Compared to conventional rehabilitation, the integrated approach yielded superior outcomes, as evidenced by significantly higher Mayo Elbow Performance Scores, greater range of motion in all planes (flexion, extension, pronation, and supination), improved activities of daily living, and reduced pain levels at the 24-week follow-up. Crucially, these functional benefits were achieved without a significant increase in complication rates, suggesting that the integrated program is a safe and effective strategy for postoperative management.
Interpretation of Results and Comparison with Literature
The superior functional outcomes observed in the observation group align with the core principles of the integrated model. While conventional rehabilitation provides a foundational framework for recovery,11–16 its generalized approach may lack the structure and support needed for optimal patient engagement and progression. The success of the integrated program can likely be attributed to several key components. First, preoperative education sets realistic expectations and mentally prepares patients for the recovery journey, potentially reducing anxiety and improving cooperation.17 Second, the structured, phased home-based protocol with clear goals provides patients with a tangible roadmap, which may enhance adherence and ensure that exercises are progressed appropriately based on healing phases, rather than time alone. Finally, the active monitoring and follow-up by rehabilitation physicians allow for timely adjustments to the training plan and address patient concerns promptly, preventing deviations from the rehabilitation pathway.
Our findings of improved MEPS and ROM are consistent with the proposed benefits of comprehensive rehabilitation models. For instance, a study by Smith et al18 also emphasized that structured rehabilitation significantly impacts final elbow function post-fracture, primarily through effective pain management and early, guided mobilization. The significant reduction in VAS scores and concurrent improvement in ADL scores in our observation group further substantiate this. We postulate that the early incorporation of isometric exercises and controlled motion within a supported framework stimulates blood flow and reduces inflammatory mediator release without compromising fracture stability, thereby alleviating pain and facilitating a quicker return to functional independence.
Regarding safety, our study found no statistically significant difference in complication rates between the two groups. This finding appears to contrast with some previous literature,19,20 which suggested that high-quality postoperative rehabilitation could significantly lower complication risks. The discrepancy may not solely be due to our modest sample size, which was underpowered to detect differences in rare adverse events, but could also be influenced by factors such as the consistent surgical technique employed by a single orthopedic team in our study, which might have established a low baseline complication rate. Furthermore, the integrated program’s emphasis on proper technique and supervised progression may have prevented the aggressive mobilization that sometimes leads to complications, thereby achieving excellent function without increasing risk.
Limitations
The interpretation of our encouraging results must be tempered by the acknowledgment of several study limitations. First, the retrospective, non-randomized design introduces the potential for selection and information bias. Although baseline characteristics were comparable, unmeasured confounders could have influenced the outcomes. Second, the single-center nature and relatively small sample size limit the generalizability of our findings and the statistical power for subgroup analyses, such as by age or fracture type. The broad age range (15–65 years) is a particular limitation, as functional recovery expectations and physiological responses likely differ between adolescents and older adults; future studies with larger samples should consider stratified analyses. Third, the absence of assessor blinding could have introduced observer bias in outcome assessments, though the use of objective measures like goniometry for ROM may have mitigated this for some endpoints. Finally, the 24-week follow-up period is sufficient to assess short-to-medium term functional recovery but is inadequate to evaluate long-term outcomes, such as the risk of post-traumatic osteoarthritis or sustained functional benefits.
Implications and Future Directions
Despite these limitations, our study provides compelling preliminary evidence for the effectiveness of an integrated rehabilitation model. Future research should prioritize a prospective, randomized controlled trial with a larger, multi-center cohort to confirm these findings and establish causality. Longer-term follow-up extending to one or two years is essential to assess the durability of the functional improvements. Additionally, investigating the cost-effectiveness of this integrated model and identifying which specific components (eg, preoperative education, structured home program, or follow-up calls) contribute most to its success would be valuable for optimizing resource allocation.
Conclusion
In patients with ulnar olecranon fractures, the integrated orthopedic rehabilitation program leads to superior outcomes in elbow joint function, range of motion, pain relief, and activities of daily living compared to conventional rehabilitation at 24-week follow-up. However, these findings should be interpreted with caution considering the study’s limitations, including its retrospective design and modest sample size. The integrated approach represents a promising and effective strategy for postoperative management. Further validation through larger, prospective randomized controlled trials is recommended to confirm its benefits and support broader clinical implementation.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethical Approval Statement
This study was approved by the ethics committee of the Affiliated Nanping First Hospital of Fujian Medical University. Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki.
Funding
This study was supported by Fujian Provincial Natural Science Foundation of China (Grant number:2023J011870).
Disclosure
The authors declare that they have no competing interests.
References
1. Luengo-Alonso G, García Lamas L, Jiménez Díaz V, et al. Trans-olecranon fracture dislocations: how should we treat them? Injury. 2021;52(Suppl 4):S131–s136. doi:10.1016/j.injury.2021.02.058
2. Cain EL, Moroski NM. Elbow surgery in athletes. Sports Med Arthrosc Rev. 2018;26(4):181–184. doi:10.1097/JSA.0000000000000227
3. Luchetti TJ, Abbott EE, Baratz ME. Elbow fracture-dislocations: determining treatment strategies. Hand Clin. 2020;36(4):495–510. doi:10.1016/j.hcl.2020.07.011
4. Griffith TB, Kercher J, Clifton Willimon S, et al. Elbow injuries in the adolescent thrower. Curr Rev Musculoskelet Med. 2018;11(1):35–47. doi:10.1007/s12178-018-9457-4
5. Awad MAH, Mbogori M, Lalani A, Badre A. Outcomes of suture tension band technique for fixation of olecranon fractures: a retrospective case series. JSES Int. 2025;9(5:1825–1832. doi:10.1016/j.jseint.2025.04.032
6. Tunalı O, Erşen A, Pehlivanoğlu T, Bayram S, Atalar AC, Demirhan M. Evaluation of risk factors for stiffness after distal humerus plating. Int Orthop. 2018;42(4):921–926. doi:10.1007/s00264-018-3792-3
7. Greising SM, Corona BT, Call JA. Musculoskeletal regeneration, rehabilitation, and plasticity following traumatic injury. Int J Sports Med. 2020;41(8):495–504. doi:10.1055/a-1128-7128
8. Cusick MC, Bonnaig NS, Azar FM, et al. Accuracy and reliability of the mayo elbow performance score. J Hand Surg Am. 2014;39(6):1146–1150. doi:10.1016/j.jhsa.2014.01.041
9. Pashmdarfard M, Azad A. Assessment tools to evaluate activities of daily living (ADL) and instrumental activities of daily living (IADL) in older adults: a systematic review. Med J Islam Repub Iran. 2020;34:33. doi:10.34171/mjiri.34.33
10. Talaski GM, Yazdanpanah S, Smith MS, Cassidy BP, Satalich JR, Vanderbeck J. Short-term complications of open reduction and internal fixation of olecranon fractures: a national database study. JSES International. 2025;9(6):2156–2160. doi:10.1016/j.jseint.2025.06.017
11. Arnold MJ, Moody AL. Common running injuries: evaluation and management. Am Fam Physician. 2018;97(8):510–516.
12. Pinto D, Alshahrani M, Chapurlat R, et al. The global approach to rehabilitation following an osteoporotic fragility fracture: a review of the rehabilitation working group of the International Osteoporosis Foundation (IOF) committee of scientific advisors. Osteoporos Int. 2022;33(3):527–540. doi:10.1007/s00198-021-06240-7
13. Kakehi S, Wakabayashi H, Inuma H, et al. Rehabilitation nutrition and exercise therapy for sarcopenia. World J Mens Health. 2022;40(1):1–10. doi:10.5534/wjmh.200190
14. Fairhall NJ, Dyer SM, Mak JC, et al. Interventions for improving mobility after Hip fracture surgery in adults. Cochrane Database Syst Rev. 2022;9(9):Cd001704. doi:10.1002/14651858.CD001704.pub5
15. Stanghelle B, Bentzen H, Giangregorio L, et al. Effects of a resistance and balance exercise programme on physical fitness, health-related quality of life and fear of falling in older women with osteoporosis and vertebral fracture: a randomized controlled trial. Osteoporos Int. 2020;31(6):1069–1078. doi:10.1007/s00198-019-05256-4
16. Reid SA, Andersen JM, Vicenzino B. Adding mobilisation with movement to exercise and advice hastens the improvement in range, pain and function after non-operative cast immobilisation for distal radius fracture: a multicentre, randomised trial. J Physiother. 2020;66(2):105–112. doi:10.1016/j.jphys.2020.03.010
17. Gokeler A, Neuhaus D, Benjaminse A, et al. Principles of motor learning to support neuroplasticity after ACL injury: implications for optimizing performance and reducing risk of second ACL injury. Sports Med. 2019;49(6):853–865. doi:10.1007/s40279-019-01058-0
18. Ho W, Yao SH, Chen CH. Loop anchor tension band fixation for olecranon fractures and chevron olecranon osteotomy. Tech Hand up Extrem Surg. 2022;26(4):250–256. doi:10.1097/BTH.0000000000000394
19. Fan J, Ji JQ, Zhang X, et al. Operative effect and treatment strategies for the low distal humerus fracture. Zhonghua Wai Ke Za Zhi. 2020;58(3):213–219. doi:10.3760/cma.j.issn.0529-5815.2020.03.009
20. Arif E, Larion A. Rebuilding elbows: tech-driven recovery after olecranon fractures. Balneo and PRM. Research Journal. 2025;16(3):857.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.