Back to Journals » International Journal of General Medicine » Volume 17
Analysis of the Current Status of Outcome Indicators of Randomised Controlled Trials of Traditional Chinese Medicine for the Treatment of Qi and Yin Deficiency in Coronary Heart Disease
Authors Zhou M, Li J, Xiao X, Lim J ![]() , Xu Z
, Xu Z
Received 13 June 2024
Accepted for publication 13 August 2024
Published 16 August 2024 Volume 2024:17 Pages 3575—3590
DOI https://doi.org/10.2147/IJGM.S473899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Mi Zhou,1 Jieyun Li,1 Xinang Xiao,1 Jiekee Lim,1 Zhaoxia Xu1,2
1School of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Shanghai Key Laboratory of Health Identification and Assessment, Shanghai, People’s Republic of China
Correspondence: Zhaoxia Xu, Shanghai University of Traditional Chinese Medicine, 1200 Cailun Road, Pudong New Area, Shanghai, 201203, People’s Republic of China, Email [email protected]
Purpose: To analyse the current status of outcome indicators in randomised controlled trials (RCTs) of traditional Chinese medicine (TCM) for the treatment of coronary heart disease (CHD) with deficiency of qi and yin, and to provide a basis for constructing a core indicator set (COS) for TCM treatment of CHD.
Methods: We searched the database of China National Knowledge Infrastructure (CNKI), PubMed,etc. 8 databases in the last 5 years. RCTs of TCM for CHD included in core journals were evaluated for the risk of bias of the included studies, and the current status of the selection of outcome indicators was statistically analysed.
Results: A total of 39 RCTs with a sample size of 44~398 cases were included, and 164 outcome indicators were reported, with a frequency of 383 applications. The outcome indicators were categorised into 6 indicator domains according to their functional attributes, which were, in descending order, safety indicators, physicochemical examination, effective rate, economic assessment, disease evidence score, and quality of life. The top 3 indicators in terms of frequency of application of outcome indicators were safety indicators, physical and chemical examination indicators, and efficiency, among which electrocardiogram, inflammation indicators, and clinical efficacy were the most frequently used; there were many different types of measurement tools for outcome indicators, among which total efficiency and TCM symptom points were the most frequently used; the time point of measurement was not the same.
Conclusion: The RCTs of TCM for CHD in the last 5 years have many shortage in the selection of outcome indicators, and should actively promote the construction of the COS of TCM for CHD.
Keywords: Coronary heart disease, deficiency of qi and yin, TCM, randomised controlled trials, outcome indicators, core indicator set
Introduction
Coronary heart disease (CHD) refers to heart disease caused by atherosclerosis of coronary arteries resulting in narrowing or occlusion of the lumen, leading to myocardial ischemia, hypoxia or necrosis, also known as ischemic heart disease, which is the most common type of organ pathology caused by atherosclerosis.1 Although the overall number of deaths due to CHD has declined relatively by about 25% over the past decade, it is still the leading cause of death worldwide and carries a huge family and social burden.2,3 CHD is classified as “chest paralysis and heart pain” and “true heart pain” in TCM, and it is believed that chest paralysis is a symptomatic evidence of the underlying deficiencies. The main deficiency is the deficiency of qi, blood, yin and yang, and the underlying substance is stagnation of qi, phlegm, cold condensation and blood stasis. With the development of society, the pathogenesis of CHD has also evolved, and the underlying deficiency is more often manifested as a deficiency of qi and yin, while the underlying reality is mainly focused on phlegm and blood stasis, and the internalisation of evil heat.4
 |
Figure 1 Literature screening flowchart. |
The deficiency of qi and yin is the basis of CHD mechanism. There are many reasons for the formation of qi and yin deficiency: CHD in the population to middle-aged and old people, 《Huang Di Nei Jing》said: “Yin is halved from age 40” which indicates that the body’s internal organs function with the growth of age and decline, the essence of the substance of the lack of sources of biochemical production, resulting in the body to show a qi and yin deficiency of the state; CHD patients are often combined with hypertension, diabetes, hyperlipidaemia, etc., a longer course of disease, exhaustion and injury to the yin, over time the yin damage and become qi and yin deficiency; with the improvement of the standard of life, the consumption of fatty, sweet, thick and spicy food increase, resulting in dampness and heat, dry heat, injury to the yin and exhaustion of qi and become qi and yin deficiency; work pressure and emotional fluctuations so that people “turn their wills into fire”, and fire and heat are generated internally, which drains qi and hurts yin. After the formation of qi and yin deficiency, on the one hand, qi deficiency blood transport weakness, blood stasis, without circulation, there will be pain; on the other hand, heart veins are not moistened due to the heart yin insufficient, without nutrition, it hurts. The development of CHD is a complex pathological process of mixed pathology, with deficiency of qi and yin as the root of the disease and heat and phlegm as the symptom of the disease, while heat, blood stasis and phlegm are all pathological factors produced on the basis of deficiency of qi and yin. Clinical manifestations of qi and yin deficiency are common: vague pain in the heart and chest, which occurs sometimes and stops sometimes, shortness of breath with palpitation, which gets worse when moving, tiredness and weakness, low voice, easy to perspire, red tongue, thin white moss.5,6 Randomised controlled trials (RCTs) are the “gold standard” for evaluating clinical efficacy. Endpoint indicators are an important part of RCT study design, and the reasonable selection of endpoint indicators can reduce bias, improve study quality and enhance the application value of study results. Currently, there is no guideline for the selection of outcome indicators for RCTs of CHD treated with TCM.7 Scientific and standardised COS studies can reduce the heterogeneity of outcome indicators in related clinical trials, promote the standardisation and unification of the measurement time points and measurement tools for outcome indicators, and reduce the risk of selective reporting bias, highlighting the outcomes of concern to patients.8
The author’s team found that there are no guideline standards for the selection of outcome indicators for RCTs of TCM treatment of CHD with qi and yin deficiency, and there is a lack of outcome indicators reflecting the characteristics of TCM, which is not conducive to the comparative analyses of the same studies, and it is difficult to obtain high-quality evidence-based evidence.By analysing the current status of the selection of outcome indicators in RCTs of TCM for CHD in the last 5 years (2019–2024), this study provides a reference basis for the selection of outcome indicators in RCTs of TCM for CHD, and lays the foundation for the construction of a COS for TCM for CHD.
Materials and Methods
Inclusion criteria: Studies that met the following criteria were included in this study.
Study subjects: patients with a clear diagnosis of CHD qi and yin deficiency syndrome and a clear report of Western medicine diagnostic criteria and TCM evidence diagnostic criteria, regardless of gender, age, race, and cause of illness;
Interventions: use of TCM alone or in combination; TCM treatments included TCM compounding, proprietary TCM, acupuncture, moxibustion, acupoint plasters and other treatments based on the guidance of TCM theory;
Control measures: no restriction;
Study type: Chinese and English RCT studies published between 2019 and 2024, Chinese literature will only be included if published in journals included in the China Science Citation Database (CSCD), Chinese core journals, and Chinese Science and Technology Paper Citation Database (CSTPCD). For duplicate studies, only the most complete and newly published studies were selected for inclusion.
Exclusion criteria: Studies that met the following criteria were excluded.
The research subjects were not Qi and Yin deficiency CHD; dissertations, conference papers; only involved “pathways”, “factors” and other mechanism of action related outcome indicators, no clinical efficacy related outcome indicators; literature ≤ 1 page; unable to obtain the full text.
Literature Search
Computerised searches of the China National Knowledge Infrastructure (CNKI), Wanfang data knowledge service platform (Wanfang data), Chongqing Weipu Chinese Journal Database (VIP), China Biomedical Literature Service System (SinoMed), PubMed, Web of Science, Embase, and Cochrane Library databases were conducted to collect RCTs of TCM for the treatment of CHD with a search timeframe of 1st January 2019 to 26th February 2024. In addition, Google Scholar and Chinese Medical Journal Full Text Database were also searched. Chinese search terms included “coronary heart disease”, “coronary atherosclerotic heart disease”, “stable heart disease”, “chronic heart disease ”, “acute coronary syndrome”, “unstable angina”, “myocardial infarction”, “CHD ”, “CAD”, “SCAD”, “ACS”, “evidence type ”, “Chinese medicine evidence type”, “qi and yin deficiency”; English search terms included “coronary heart disease”, “CHD”, “CAD”, “stable coronary artery disease”, “ Acute Coronary Syndromes”, “myocardial infarction”, “unstable angina”, “qi and yin deficiency”, etc. The search was performed using subject terms combined with free terms, and the search strategy was adjusted accordingly to the database.
Literature Screening and Data Extraction
Literature screening, data extraction and cross-checking were carried out independently by 2 researchers, and any differences were resolved by consulting the steering committee experts. Noteexpress software was used to manage the literature, and Excel 2016 software was used to extract and analyse the data. The extracted content included: basic information of the literature (first author, year and journal of publication, ethical review and registration); information of the study subjects (sample size, coronary angiography, disease duration, intervention, course of treatment); methodological characteristics (randomised method, allocation concealment, blinded method, etc).; and outcome indicators (name of the indicator and the indicator response status, time point of measurement, and measurement tool).
Risk of Bias Assessment
The Cochrane Risk of Bias Assessment Tool was used to assess the risk of bias of the included literature. Evaluation entries included random sequence generation, allocation concealment, blinding of patients and staff, blinding of outcome evaluators, incomplete outcome data, selective reporting of outcomes, and other biases, and each entry was assessed as “low risk of bias”, “uncertain risk of bias”, “high risk of bias”.
Statistical Analysis
All the extracted data were analysed using Excel 2016 software, and the identification and classification and outcome indicators of the included studies were standardised. Referring to the Technical Specification for the Development of Core Indicator Sets for Clinical Trials of Traditional Chinese Medicine,9 the outcome indicators were categorised into seven indicator domains according to their functional attributes, which were presented as a dendrogram, and the frequency of the use of each type of outcome indicator was statistically and descriptively analysed.
Results
Literature Screening Process
The preliminary search yielded 2734 pieces of literature, and 39 pieces of literature were finally included in the screening process according to the inclusion and exclusion criteria (39 pieces of literature are in Chinese) and the flow chart of the literature screening process is shown in Figure 1.10–48
Basic Characteristics of the Included Studies
Of the 39 Chinese literature included, 3 (0.77%) were published in CSCD, 1 (2.56%) was published in Chinese core journals, and 35 (89.74%) were published in Chinese science and technology core journals.
Sample Size
A total of 4061 patients were included, of which 2154 were in the experimental group and 1905 were in the control group, the sample size of a single study ranged from 56 to 240 cases, and the average sample size of the included studies was 104 cases.
Interventions and Control Measures
The types of interventions were mostly TCM compound soup, prepared prescription (TCM), and TCM injections combined with western medicines. Among them, there were 20 articles (51.28%) of TCM compound soup combined with conventional western medicine, 16 articles (41.03%) of prepared prescription (TCM) combined with conventional western medicine, and 3 articles (7.69%) of TCM injection combined with conventional western medicine. See Table 1.
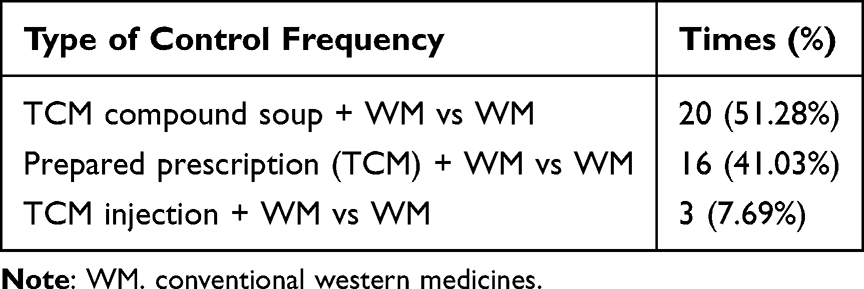 |
Table 1 Reported Types of TCM for CHD Control |
Specific Classification of Qi and Yin Deficiency Types
39 of the included RCTs reported specific TCM diagnostic typing of the study population, of which 13 (33.33%) reported ≥2 types of evidence. A total of 5 evidence types were reported in the included studies, and the specific reporting frequencies are shown in Table 2.
 |
Table 2 Reported TCM Evidence Typing for TCM Treatment of CHD |
Duration of Treatment and Follow-Up
The duration of treatment in the included studies ranged from 14 days to 3 months, with 4 (10.26%) having a duration of ≤14 days, 19 (48.72%) having a duration of 14 days to 1 month, and 16 (41.03%) having a duration of 1 to 3 months. None of the studies were followed up.
Risk of Bias Assessment
The risk of bias of the included studies was evaluated according to the Cochrane Risk of Bias Assessment Tool: (i) Generation of random sequences: 33 studies referred to ”random”, of which 24 (62.00%) were grouped by the ”Randomised Numeric Table Method”, evaluated as ”low risk of bias”,and 6 items (15.00%) were evaluated as ”high risk of bias”, 2 (5%) of them were grouped by ”treatment method”, 2 (5%) were grouped by ”order of admission”, 1 (3%) was grouped by ”CHD or not”, and 1(3%) did not mention the specific group. (ii) Distribution concealment: 3 items (8.00%) were evaluated as ”low risk of bias”, and distribution concealment was performed by ”envelope sealing”. (iii) Blinding of patients and staff: 3 items (7%) were ”double-blinded” and evaluated as ”low risk of bias”; the remaining 36 items (82%) explicitly did not mention ”blinding” and were evaluated as ”low risk of bias”. The remaining 36 (82%) were evaluated as ”uncertain risk of bias” without explicit reference to the implementation of ”blinding”. (iiii) Blinding of outcome evaluators: 1 item (3%) explicitly mentioned ”blinding” and was evaluated as ”low risk of bias. (v) Incomplete outcome data: 7 cases (16%) explicitly reported that patients were discharged, of which 5 cases (13%) accounted for <10% of the total sample size and were evaluated as ”low risk of bias”, and 2 cases (5%) accounted for >10% of the total sample size and were evaluated as ”high risk of bias”; 32 cases (82%) did not explicitly report whether or not a patient was discharged, so they were evaluated as ”uncertain risk of bias”. (vi) Selective reporting of outcomes: 3 (8%) were provided with the protocol of the previous study and all outcome indicators were reported according to the study protocol, which was evaluated as ”low risk of bias”; 36 (92%) were not provided with the protocol of the previous study, and comparisons of the outcome indicators could not be made, which was evaluated as ”uncertain risk of bias”; (vii) Other bias: 13 (33%) were evaluated as ”uncertain risk of bias” because the source of bias, such as fund support and conflict of interest, could not be determined, and the remaining 26 (67%) were evaluated as ”low risk of bias”. The results of risk of bias evaluation of the included studies are shown in Figure 2.
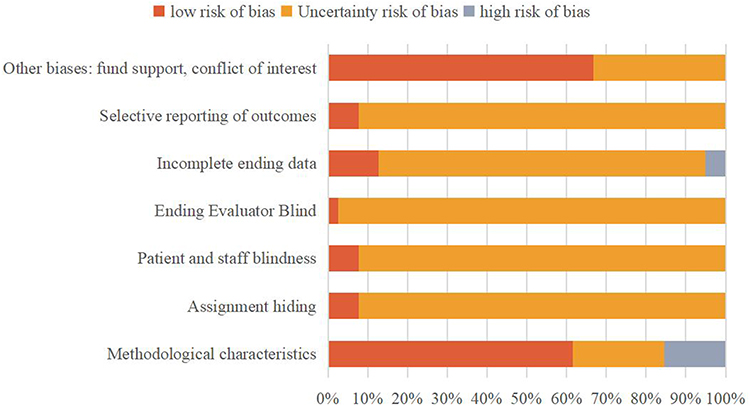 |
Figure 2 Results of bias risk assessment of included RCT. |
Outcome Indicators
Indicator Domain
A total of 136 outcome indicators were reported by the 39 RCTs included, with a total of 383 indicator application frequencies. The minimum number of indicators reported by a single RCT was 3, and the maximum number was 9, with an average of 9 indicators reported per RCT. The outcome indicators were grouped into 6 indicator domains according to the functional attributes of the indicators, and in order of frequency of application, they were safety indicators 139 times (36.29%), biochemical examinations 107 times (27.94%), effective rate 53 times (13.84%), economic assessment 39 times (10.18%), disease score 29 times (7.57%), and quality of life 16 times (6.60%). Among them, physical and chemical examination was divided into 8 categories, safety indicators were divided into 7 categories, the efficiency indicators are divided into 5 categories, the quality indicators into 3 categories, the disease score into 2 categories, and the economics assessment category into 1 category as shown in Figure 3.
 |
Figure 3 Reported TCM for CHD qi and yin deficiency syndrome control types. |
Indicator Application Frequency
The application frequency of 136 outcome indicators was counted, and the top 3 indicators in application frequency were safety indicators, physical and chemical examination indicators, and effective rate, among which ECG, inflammation indicators, and clinical efficacy had the highest application frequency, which were 44 times (11.49%), 44 times (11.49%), and 30 times (7.83%), respectively. The outcome indicators with application frequency ≥2 times in each indicator domain are shown in Table 3.
 |
Table 3 Outcome Indicators of TCM Treatment of CHD with Qi and Yin Deficiency Syndrome with Application Frequency ≥2 Times in Each Index Domain |
Measurement Tools
There was a wide variety of measurement tools for the 136 outcome indicators, with the total effectiveness rate and TCM evidence score leading the list, with 14 and 8 measurement tools respectively.
Total Effectiveness Rate
32 RCTs reported total effectiveness rates, with “clinical efficacy”, “comparative efficacy”, “comprehensive efficacy” and “TCM symptomatic efficacy” appearing in the literature, and so on. There were a total of 14 measurement tools for total efficacy, and 3 RCTs had ≥2 measurement tools, among which the <Guidelines for Clinical Research of New Chinese Medicines> was the most frequently used. The use of total effectiveness measurement tools in the included studies is shown in Table 4.
 |
Table 4 Measurement Tools for the Total Effectiveness Rate of TCM in Treating CHD |
TCM Evidence Score
29 RCTs reported TCM evidence score, and there were a total of 8 measurement tools, 3 RCTs had ≥2 measurement tools, of which the frequency of application of the Guiding Principles for Clinical Research of New Traditional Chinese Medicines was in the first place, and the use of the measurement tools for TCM evidence score in the included studies is shown in Table 5.
 |
Table 5 Measurement Tools for TCM Evidence Score in TCM Treatment of CHD |
Measurement Time Points
The measurement time points for each type of outcome indicator varied, of which the top 2 indicators in terms of frequency of application were the total effectiveness rate and TCM evidence score, with 16 and 18 measurement time points, respectively.
Total Effective Rate
All 34 RCTs reported the measurement time points, which spanned from 2 weeks to 3 months, with the most reported measurement time point being 4 weeks of treatment (13 times, 38.23%). The time points of measurement for total effectiveness in the included studies are shown in Table 6.
 |
Table 6 Measurement Time Points for Overall Effectiveness of TCM in Treating CHD |
TCM Evidence Score
The time point of measurement was reported in all 29 RCTs, with the most frequently reported time point of measurement being pre-treatment versus 4 mouth of treatment (29 times, 44.83%). The time points of measurement of TCM evidence score in the included studies are shown in Table 7.
 |
Table 7 Measurement Time Points of TCM Evidence Points in TCM Treatment of CHD |
Discussion
The outcome indicator is one of the important elements of clinical research design, and is an important means of measuring and evaluating the effectiveness and safety of interventions. In clinical studies of TCM, problems such as wide variation in the selection of outcome indicators and irregular reporting are common, which will have an impact on secondary studies to a certain extent and reduce the quality and grade of research evidence.49 In this study, we systematically searched 8 major databases for all RCTs of TCM treatment of CHD with qi and yin deficiency from 2019 to 2024, and finally included 39 studies that reported 136 types of outcome indicators, classified the indicators into 6 indicator domains: safety indicators, physicochemical examination, efficiency, economic assessment, disease score, and quality of life, and preliminarily counted the frequency of the application of the outcome indicators, the measurement tools, measurement time point, etc., and found that there were more deficiencies in the reporting of outcome indicators, which are analysed as follows.
Current Situation and Thoughts on the Design and Reporting of RCT Trials of TCM for CHD
Incomplete Study Registration and Ethical Review
Research registration is an important part of making research transparent, allowing the sharing of study design and implementation progress, and avoiding or reducing publication bias and selective reporting.50 Ethics is a moral code that guides and evaluates actors,51 and the Law of the People’s Republic of China on Basic Medical Care and Health Promotion, promulgated in 2019, stipulates that all biomedical research involving human beings should be subjected to review by an ethics committee.52 Of the 39 RCTs included in this study, 22 (56.41%) did not report study registration information, and 7 (17.94%) did not report specific information on ethical review, which is related to the relatively lax requirements of some academic journals in China. Therefore, this study suggests registering with a recognised registration platform at home and abroad and obtaining ethical approvals before formally carrying out the study, updating the progress of the study in a timely manner during the course of the study, and disclosing the information on registration and ethical review when the research results are published, so as to ensure the scientific and transparent nature of the study.
Lack of Uniform Symptom Names and Dialectical Criteria
Among the 39 RCTs on CHD with qi and yin deficiency, there were multiple related TCM syndromes with qi and yin deficiency as the core, and the following problems existed: ① the syndromes with the same meaning had different names, such as qi and yin deficiency, deficiency of both qi and yin; ② multifactorial syndromes were expressed arbitrarily, such as qi and yin deficiency and stasis, qi and yin deficiency and blood stasis, qi and yin deficiency with blood stasis and phlegm obstruction, and so on; TCM syndromes are the identification of the cause, location, and location of the disease at a certain stage. The TCM pattern is a high degree of generalisation of the essence of the disease such as the cause, location, nature and situation of the disease at a certain stage, which guides the establishment of the treatment, and the subtle differences in the pattern have very different meanings; and secondly, the diagnostic criteria of the pattern are different, which also affects the promotion and application of the results of the study. Therefore, it is recommended to standardise the diagnostic criteria of TCM evidence for CHD, in order to lay the foundation for further optimising and standardising the clinical research of TCM for CHD.
Risk of Bias in Literature Assessment
Of the 39 RCTs included in this study, only 1 (2.56%) was blinded to outcome evaluators, only 3 (7.69%) were blinded to patients and staff, only 3 (7.69%) reported allocation of hidden relevant information, only 3 (7.69%) were given access to prior study protocols and evaluated as low risk of reporting bias, 26 (66.67%) reported grant funding, and the other bias rated as uncertain risk, and the remaining 13 (33.33%) RCTs other sources of bias could not be judged and rated as uncertain risk. The overall methodological quality of the included studies was poor. Therefore, it is recommended that in the design and implementation of clinical trials of TCM in the future, blinding should be implemented as much as possible, and the whole process of quality control should be carried out, so as to avoid or reduce the bias that may occur in the course of the study as much as possible.
Problems and Considerations in the Selection of Outcome Indicators for CHD Treatment in TCM
Wide Variety of Indicators, Large Differences in the Number of Indicators and Frequency of Application
First of all, the 39 RCTs reported a total of 136 types of outcome indicators, and the frequency of their application varied greatly, for example, “adverse reactions” was reported 19 times, and “cardiac efficacy” was reported only once, and this difference also existed in the same indicator domain. This difference also exists in the same indicator domain, such as “clinical efficacy”, which was reported 16 times, whereas “heart failure efficacy” and other 62 indicators were reported only 9 times. Secondly, the non-specific indicators used in the included studies were more diverse, with more studies on “blood glucose”, “adhesion molecules”, “electrocardiogram”, “ blood rheology levels”, and other indicators of cardiac function were used infrequently, which is less practical. Thirdly, the specificity of cardiac function and inflammation-related indexes selected in some studies is not high, and they cannot be used as reliable “alternative indexes” to evaluate the treatment effect. Fourth, the number of outcome indicators reported in a single RCT varied widely, from a minimum of 3 to a maximum of 9, and too few or too many indicators may affect the evaluation of the efficacy of the intervention. Therefore, choosing the right number of indicators with reliability not only reduces the waste of research and medical resources, but also improves the level of evidence of the study.
Unstandardised Names for the Same Indicators, Diverse Measurement Tools and Confusing Measurement Time Points
Among the 39 RCTs included, the same evaluation indicators were expressed in various ways. For example, 32 RCTs reported the total effective rate, and different expressions such as “clinical efficacy”, “comparative efficacy”, “comprehensive efficacy”, “TCM efficacy”, etc. appeared in the literature. In the literature, there are different expressions such as “clinical efficacy”, “comparative efficacy”, “comprehensive efficacy”, “TCM efficacy”, etc. In the physicochemical examination, there are even more diverse expressions for the indicators of inflammation and myocardial damage. In addition, statistics on the measurement tools and time points of the most frequently used outcome indicators showed that there were 14 measurement tools and 8 measurement time points for “total effectiveness”, and 8 measurement tools and 7 measurement time points for “TCM evidence score”. Different forms of expression, measurement tools and time points for the same indicator will affect the consolidation of the indicator data and the generation of high quality evidence in the secondary study.
Mixed Primary and Secondary Indicators, Random Combination of Primary and Objective Indicators
Primary outcome indicators refer to the indicators that can provide the most clinically relevant and credible evidence for the primary purpose of the trial, and secondary outcome indicators refer to the indicators that are related to the primary or secondary purpose of the trial and can support the primary purpose.53 In general, a clinical study needs to provide one primary indicator, and the number of secondary indicators needs to be appropriate, in order to prevent the mixing of indicators from leading to inconsistency in the final point of the study and affecting the evaluation of the study results. Of the 39 RCTs included in this study, only 2 distinguished between primary and secondary outcome indicators. At the same time, there was also the problem of arbitrary combination of primary and objective indicators in the included studies, for example, the evaluation of “total efficiency” mainly included “clinical symptoms”, “electrocardiogram and cardiac function tests”. The mixing of primary and secondary indicators and the arbitrary combination of primary and objective indicators will affect the objectivity and reliability of the results of the studies, as well as the level of evidence for similar studies and their secondary studies.
Unstandardised Indicators of TCM Characteristics
As evidence-based treatment is the foundation and essence of TCM theory, clinical research on TCM should attach great importance to the application of indicators of TCM characteristics, reflecting the characteristics and advantages of TCM treatment, and based on which TCM can be inherited and carried forward. Among the 39 RCTs included, 24 RCTs (61.54%) reported “TCM disease indicators”, indicating that most of the researchers attached great importance to the characteristic indicators of TCM, however, after summarisation, it was found that there were five different ways of expression in the “TCM disease score”. For example, “TCM syndrome score” includes “symptoms”, “signs”, “tongue” and “pulse”, which is difficult to be counted due to the large individualised differences, and we look forward to conducting in-depth statistical analyses in the future. Therefore, although the frequency of application of “indicators of TCM” ranks third, the frequency of application of individual indicators is not high, so the construction of a core set of CHD indicators with TCM characteristics can effectively solve this problem.
Neglecting Patient-Reported Outcome Indicators, Long-Term Prognosis and Economic Indicators
Patient-reported outcomes (PROs) are indicators related to one’s own health that must be reported by patients, including data such as quality of survival evaluation, patient symptoms and satisfaction.54 Of the 39 RCTs included, a part of patients’ quality of life was reported; of the 136 indicators, the frequency of reporting on patient mental health indicators accounted for 1.5%. CHD is known as one of the major diseases threatening the lives and health of the people in China,55 and the prevalence and mortality rate are still on the rise each year, so long-term prognosis needs to be paid great attention to, and there was no post-treatment follow-up in any of the included studies. The progression of CHD affects the quality of life of patients, and its treatment period is relatively long, and the cost of treatment is not low. Prognosis and economic factors are the key concerns of patients. Therefore, it is necessary to pay attention to the application of PROs, long-term prognosis and economic indicators in clinical trials, so as to enrich the dimensions of the efficacy evaluation of CHD treatment with TCM, and to provide users of evidence with evidence that is more relevant to the needs of clinical practice.
Inadequate Reporting of Safety Indicators
The safety evaluation of interventions is of high concern to patients and is also an important guarantee for the promotion and application of interventions. TCM treatment follows the principles of holistic concept and evidence-based treatment, which are not exactly the same for different individuals and may result in unanticipated adverse events, and detailed and standardised safety evaluation is the basis for promoting the development of TCM application.56 Of the 39 RCTs included, 19 (48.72%) explicitly evaluated the safety of the intervention, such as adverse events, and were relatively simple to report. In addition, factors such as “follow-up” should be taken into account when reporting safety indicators, and none of the trials had post-treatment follow-up, so long-term safety could not be evaluated. It is recommended that researchers should refer to the “Harms” section in the statement of the Consolidated Standards of Reporting of Randomised Controlled Trials (CONSORT) to report the safety-related outcomes of RCTs,57 and report the names of the adverse reactions and events, their occurrence and duration, frequency, severity, time to remission and improvement, and treatment modalities in detail. If no adverse events occurred, they also need to be reported truthfully. In addition, the duration of long-term follow-up can be appropriately extended to observe the long-term safety after treatment.
Countermeasures and Suggestions
Actively Constructing a Core Indicator Set for TCM Treatment of CHD with Qi and Yin Deficiency
Core indicator set (COS) refers to the smallest collection of indicators that must be reported for clinical research in a specific area of health or health care, with the characteristics of being the most important, standardised, consensus, primary and secondary.COS can effectively solve the problem of indicator selection in clinical research and promote the comparison of clinical research results in the same area, thus improving the quality of clinical trial research and reducing unnecessary waste of resources. Therefore, in strict accordance with the COS development and reporting specifications, on the basis of standardising the TCM syndrome of CHD, the COS of CHD with qi and yin deficiency with TCM characteristics should be constructed, so as to improve the clinical efficacy evaluation index system of TCM in treating CHD with qi and yin deficiency.58
Standardise the Study Design, Implementation and Reporting of Clinical Trials
It is recommended that researchers standardise the study design of RCTs according to the purpose of the study before conducting a clinical trial of TCM, and make comprehensive considerations in terms of patient recruitment, sample size, randomised grouping, blind selection, implementation of interventions, assessment of efficacy, quality control and statistical analysis, etc., and learn about and solve problems that may be encountered in the study as early as possible by conducting a pre-trial. At the same time, it is also recommended that researchers register the trial on the clinical trial registration platform and make the study protocol public. During the course of the trial, they should strictly control the process and details of the trial, record the trial data in detail, keep the original records, and conduct regular monitoring and quality control to minimise or avoid possible bias in the course of the study. After the completion of the study, it is suggested that researchers should refer to the CONSORT statement to report the results of the RCT study, attach importance to the outcome indicators reported by patients, long-term prognosis and economic indicators, and standardize the measuring tools and measuring time points of the outcome indicators to ensure the feasibility, scientific, normative and authenticity of the study implementation.
Conclusion
This study analysed the current status of RCT outcome indicators of TCM for treating CHD with qi and yin deficiency from 2019 to 2024, and found that in the selection of outcome indicators, there were a wide variety of indicators, irregular reporting of names, lack of a clear distinction between primary and secondary, arbitrary combinations of subjective and objective indicators, neglecting of patient-reported outcome indicators, neglecting of long-term prognostic, safety Inadequate reporting of indicators, non-uniformity of measurement tools and time points, which will directly affect the quality of primary and secondary research. The lack of uniform standards for outcome indicators is the main reason for the above problems, and the construction of COS of TCM for CHD (COS-TCM-CHD) is an effective way to solve this problem. The establishment of COS-TCM-CHD can obtain a uniform minimum set of outcome indicators that should be reported in clinical trials of TCM treatment of CHD, combine the characteristics of TCM with clinical research, provide researchers with the most reasonable and effective core outcome indicators and the best measurement tools and time points, control the risk of bias, further standardise the clinical research of TCM treatment of CHD, improve the quality of the research, and increase the recognition and application value of the research results. It will further standardise the clinical research on CHD treatment with TCM, improve the quality of research, and increase the recognition and application value of the research results.
Discussion
In terms of the included studies, this study only included publicly published English literature or Chinese core journal literature from 2019–2024, with strict inclusion and exclusion criteria, and did not search for relevant RCT study protocols in the clinical trial registration platform. In terms of the analysis of results, this study did not conduct a comprehensive horizontal comparison of the selection of indicators for different treatment modalities and different populations, did not conduct a longitudinal comparison of the selection of indicators for different periods of time, and did not statistically analyse the mode of measurement and the time point of measurement of all indicators. Therefore, the results of the analyses in this study are limited in time and scope, and the next step is to carry out more comprehensive and in-depth exploratory analyses and to construct a core set of indicators for the treatment of CHD with TCM.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by the National Natural Science Foundation of China (No. 82374336, No. 82074333) and the Shanghai Key Laboratory of Health Identification and Assessment (NO.21DZ2271000).
Disclosure
The authors of this paper declare that they have no conflict of interest.
References
1. Wang ZW, Ma ZY. Expert consensus on primary coronary heart disease and ischaemic stroke co-morbidity management 2022[J]. Cardiovas & Cerebrovas Dis Control. 2022;22(4):1–19.
2. Yangjin WANG, Fang LIANG. Guidelines for chronic disease management of coronary heart disease in the elderly[J]. Chin and West Med Res. 2023;15(01):30–42.
3. Virani SS, Newby LK, Arnold SV, et al. AHA/ACC/ACCP/ ASPC/NLA/PCNA Guideline for the management of patients with chronic coronary disease: a report of the American Heart Association/American College of Cardiology joint committee on clinical practice guidelines. Circulation. 2023;148(9):e9–e119. 10.1161/CIR.0000000000001168
4. Mao JY, Wu YJ, Shi DZ. Guidelines for clinical application of proprietary Chinese medicines in the treatment of coronary heart disease (2020)[J]. J Integr Cardiovas & Cerebrovas Dis. 2021;19(09):1409–1435.
5. WANG J, Guang CHEN. Expert consensus on Chinese medicine diagnosis and treatment of stable angina in coronary heart disease[J]. J Trad Chin Med. 2018;59(05):447–450.
6. Yangjin WANG, Fang LIANG. Guidelines for chronic disease management of coronary heart disease in the elderly[J]. Integr Med Res. 2023;15(01):30–42.
7. Jie Z, Yaxi S, Qingrui Y, et al. Current analysis of outcome indicators of randomised controlled trials of Chinese medicine for chronic atrophic gastritis[J/OL]. Chin J Experimen. 2024;30(17):93–202.
8. Huan CHEN, Jinzhi LU, Jiaqi WANG, et al. Analysis of the current status of outcome indicators in randomised controlled trials of Chinese medicine for functional dyspepsia[J]. World J Integr Med. 2024;19(01):28–35.
9. Mingyan Z, Junhua Z, Boli Z,et al. Technical Specification for the Development of the Core Indicator Set for the Clinical Trials of Chinese Medicine. Chin J Trad Chin Med. 2021;36(2):924–928.
10. Chen WF. Clinical study of Dengzhan Shengmai capsule combined with conventional Western medicine in the treatment of stable angina pectoris of coronary heart disease [J]. New Chin Med. 2023;55(04):40–45.
11. Tengfei L, Dawei Z, Wei T, et al. Effects of Tiaomai mixture on heart rate variability and atrial fibrillation load in patients with atrial fibrillation complicated with stable coronary heart disease [J]. Modern Chin Med Clinical. 2023;30(05):35–39.
12. Wang L, Ping L, Chai Y, et al. Curative effect of Shenguining Xin Mixture on Qi-Yin deficiency combined with stasis syndrome of stable angina pectoris of coronary heart disease [J]. Shaanxi Trad Chin Med. 2022;43(12):1691–1693.
13. Shenghua D, Jing F, Xiaoning C. Effect of Qidongyixin Granule combined with trimetazidine on exercise tolerance in patients with stable coronary heart disease with Qi-Yin deficiency syndrome [J]. Clinl Misdiagnosis and Treatment. 2022;35(07):23–27.
14. Wen Z, Jingjing S, Mingchao W, et al. Effect of Shenmai Injection on angina pectoris of Qi-Yin deficiency coronary heart disease and its influence on hemorheology and electrocardiogram [J]. World J Integr Chin and West Med. 2022;17(06):1238–1241.
15. Shulin S, Lu Y. Effects of Wenxin Granule combined with Western Medicine on cardiac function and serum N-terminal B-type brain natriuretic peptide precursors in patients with coronary heart failure of Qi-Yin deficiency and ventricular premature beat [J]. World J Integr Chin and West Med. 2022;17(04):737–742.
16. Guobang F, Zhenlian L, Fangxu F. Effect of Dingtong Jiexin Decoction on coronary heart disease with Qi-Yin deficiency Syndrome and changes of electrocardiogram and autonomic nervous function [J]. Sichuan Trad Chin Med. 2022;40(03):81–84.
17. Haiyan W, Boqing S, Xinghai Z, et al. Taohong Siwu Decoction and Qiwei Baizhu Powder treating 50 cases of diabetes complicated with coronary heart disease [J]. HUNAN J of TRAD CHIN MED. 2022;38(10):17–21.
18. Yuejiao HAO, Dandan S, Jing S. Effect of Yangyin Anshen Jianpi Decoction on stable angina pectoris of Qi-Yin deficiency Coronary Heart disease and its Influence on TCM syndrome and heart function [J]. Shi Zhen Chin Med. 2021;32(07):1676–1679.
19. Feng J, Yaolong R, Baiyao Z, et al. Application of Shenmai Injection in patients with ST-segment elevation myocardial infarction with Qi-Yin deficiency [J]. World Trad Chin Med. 2021;16(04):643–647.
20. Jianzhong P, Yang J, Shanfu C, et al. Effect of Tongmai Yangxin Pill on stable angina pectoris with Qi-Yin deficiency [J]. J Mod Integr Chin and West Med. 2021;30(23):2513–2517+2544.
21. Qing J, Limei L. Clinical study of Shenmai Injection combined with Western medicine in the treatment of coronary heart disease complicated with chronic heart failure syndrome of Qi-Yin deficiency [J]. New Chin Med. 2021;53(24):61–64.
22. Linlin R. Clinical study of Yiqi Fumai Decoction combined with metoprolol in the treatment of arrhythmia in coronary heart disease with deficiency of Qi and Yin [J]. New Chin Med. 2021;53(13):68–71.
23. Yao H, Mei D, Hongxu L, et al. Clinical effect of Tiaomai mixture on ventricular precontraction of coronary heart disease with Qi and Yin deficiency combined with blood stasis and heat [J]. Chin J Exp Formul. 2021;27(19):118–125.
24. Jianzhong P, Yang J, Shanfu C, et al. Clinical study of Tongmai Yangxin Pill for treating Qi-Yin deficiency syndrome of stable angina pectoris [J]. Liaoning J Trad Chin Med. 2021;48(10):115–119.
25. Wei N, Nuo T, Jimei G, et al. Clinical observation of Shuxinyin combined with conventional Western medicine in the treatment of coronary arteriosclerotic heart disease complicated with chronic heart failure [J]. J Shanghai Univer Trad Chin Med. 2021;35(03):17–22.
26. Li Mingzi CAIQ, Yuxin S. Clinical observation of Yiqi Yangyin Huayu Decoction in treating stable angina pectoris of coronary heart disease (syndrome of Qi Yin deficiency combined with blood stasis) [J]. Chin J Emerg Med. 2020;29(12):2186–2189.
27. L SG, Liu F, Wan Z, et al. Yangxin Tongluo Decoction treating chronic stable coronary heart disease with Qi and Yin deficiency and blood stasis and phlegm obstruction [J]. World of Chin Med. 2020;15(08):1162–1166.
28. Tao J, Huiying W, Chunling Z, et al. Effect of Qiling Ningxin Decoction on autonomic nervous function of patients with Qi-Yin deficiency syndrome of coronary heart disease [J]. J Cardio-Cerebrovas Dis of Integr Chin and West Med. 2019;18(03):478–482+502.
29. Yan C, Tao J, Xianjun Y.Clinical observation of Dendrobitongbi Decoction combined with acupoint application in the treatment of angina pectoris of type 2 diabetic coronary heart disease [J]. Chin Med Science and Tech. 2019;27(06):898–900.
30. Yilan X, Shan G, Bing D, et al. Clinical and biochemical basis of Tongmai Yangxin Pill in treating stable angina pectoris with coronary heart disease [J]. Tianjin Chin Med. 2019;36(01):18–22.
31. Chang D, Tong L. Clinical study of Shenqi Huoxue Decoction in treating unstable angina pectoris of Qi Yin deficiency combined with blood stasis [J]. Asian and Pacific Trad Med. 2019;15(02):152–154.
32. Hui C, Liming Y. 75 cases of angina pectoris of coronary heart disease with Qi-Yin deficiency combined with Chinese and Western Medicine [J]. West Chin Med. 2019;32(08):98–100.
33. Huiying W, Song C, Lanxun H, et al. Effect of Wushen oral liquid on autonomic nervous function of patients with Qi-Yin deficiency myocardial infarction after PCI [J]. Shanghai J Trad Chin Med. 2019;53(03):47–50.
34. Dong Z, Yunsu W, Linlin Y, et al. Effect of Tongmai Yangxin pill on ventricular precontraction of coronary heart disease with Qi and Yin deficiency [J]. J Cardio-Cerebrovas Dis in Integr Chin and West Med. 2019;17(21):3368–3370.
35. Dongfeng W, Jie Y. Observation on curative effect of Shengmai Powder combined with Xuefu Zhuyu Decoction in treating Qi Yin deficiency and blood stasis syndrome of coronary heart disease [J]. Chin Prim Health Care. 2019;33(02):76–77.
36. Junlong L, Jin Zheng PIJ. Effect of Yixin Huoxue Pill on the clinical efficacy and cardiac function of patients with acute ST segment elevation myocardial infarction in Qi-Yin deficiency syndrome after percutaneous coronary intervention [J]. J Trad Chin Med. 2019;60(11):949–953.
37. Chunhong L, Xinli Y, Haixia Y, et al. Effect of Bufei Yangxin Decoction on Traditional Chinese Medicine syndrome, heart function index and life quality score of patients with coronary heart failure (Qi Yin deficiency combined with blood stasis syndrome) [J]. Sichuan Chin Med. 2019;37(05):84–86.
38. Chen JM, Han P. Effect of self-prepared Baosheng Decoction on acute myocardial infarction with Qi and Yin deficiency [J]. Sichuan J Trad Chin Med. 2019;37(08):78–80.
39. Jing C, Jin K, Hui H. Effects of Yiqi Yangyin Quyu Formula on Lp-PLA2 and myocardial injury markers in patients with stable angina pectoris [J]. Sichuan Chin Med. 2019;41(12):107–110.
40. Wu J, Q CC, H WJ, et al. Clinical study of Yangxin Shengmai Granules in treating patients with stable angina pectoris of coronary heart disease [J]. World J Integr Med. 2019;18(09):1870–1873+1886.
41. Yunxia Z, Xiaojing C, Wenying L, et al. Effect of Shiwei Wendan Decoction combined with metoprolol on heart rate variability in patients with arrhythmia caused by deficiency of Qi and Yin combined with excessive phlegm turbidity [J]. Jilin Trad Chin Med. 2021;41(08):1050–1053.
42. Jingchun Z, Yue L, Shuyan L, et al. A multicentre, randomized, double-blind, placebo-controlled clinical study of Zhenyuan Capsule in the treatment of stable angina pectoris with abnormal glucose and lipid metabolism in Qi-Yin deficiency syndrome [J]. J Trad Chin Med. 2019;61(06):502–508.
43. Wei L, Huijun N, Jing W, et al. Clinical effect of Shengan Guanxin Mixture on patients with chronic heart failure with Qi-Yin deficiency [J]. Chin Patent Med. 2023;45(06):1854–1857.
44. Yongji H, Xueshan L, Mingqiu W, et al. Effect of Shengmai Fulv Decoction in the adjuvant treatment of non-ST-segment elevation myocardial infarction complicated with premature ventricular beat and its influence on holter electrocardiogram index, serum NF-κB and IL-6 levels [J]. Chin J Trad Chin Med. 2022;40(11):235–238.
45. Shengbo LIANG, Wu Jingjing TAOY. Effect of Anding Decoction on stable angina pectoris of coronary heart disease (Qi Yin deficiency combined with blood stasis) [J]. Chin Emerg Med. 2021;30(11):1996–1998.
46. Wanjiang T.Effect of Simvastatin combined with Shengmai Powder combined with Xuefu Zhuyu Decoction on coronary heart disease [J]. Chinese J Mod Appl Pharm. 20;37(04):478–482.
47. Yingwei W, Yanan L, Wang B, et al. Effect of Yiqi Yangyin Tongmai prescription on stable angina pectoris of coronary heart disease and its effect on Hcy [J]. Liaon J Trad Chin Med. 2019;47(02):110–112.
48. Yunchao L, Xiaojing L, Hao N, et al. Effect of Yiqi Huoxue prescription combined with high-dose atorvastatin on levels of hs-CRP, Hcy, cTnI and cTnT in patients with unstable angina pectoris [J]. J Hebei Med. 2019;41(14):2104–2108.
49. Chen JX, Zhou QX, Yu WJ, et al. Current analysis of outcome indicators of randomised controlled trial of kidney tonifying and blood activating method for treatment of knee osteoarthritis[J/OL]. Chin J Trad Chin, 2024;49(6):1661–1672.
50. Kai-Yang LI, Cai-Yu HUANG, SHI S, et al. Analysis of the current status of clinical research registries for systemic lupus erythematosus in China [J/OL]. Chin J Dermatol and Venereol. 2024;38(7):724–730.
51. Xin L, Yan X, Yazhong Z. Common problems and analysis of ethical review of drug clinical trials [J]. China Pharma Affair. 2023;37(12):1369–1374.
52. Rong H, Yue Z, Si-Nan T, et al. Discussion on issues related to the legal responsibility of Article 102 of the Law of the People’s Republic of China on Basic Medical Care and Health Promotion [J]. Chin J Health Supervision. 2022;29(01):9–12.
53. Andrade C. The primary outcome measure and its importance in clinical trials. J Clin Psychiatry. 2015;76(10):e1320–3. doi:10.4088/JCP.15f10377
54. Zou Y, Zhang HL, Chen YY, et al. Visualisation and analysis of hotspots in domestic patient-reported outcome research [J/OL]. J Nurse Advance. 2024;39(5):552–557.
55. Juju SHANG, Hongxu LIU, Heung LI. Guideline/consensus-based discussion on the progress of Chinese medicine/combined Chinese and Western medicine in the prevention and treatment of coronary heart disease[J]. Beijing Trad Chin Med. 2023;42(09):939–942.
56. Wang H. Clinical rationality and safety evaluation of oxaliplatin [J]. J Clin Rational Use of Drugs. 2022;15(01):151–154.
57. Wan-Xin WEN, Jing-Min LU, Li-Ming LU, et al. Analysis of the current status of applying CONSORT and STRICTA to evaluate RCT in China [J]. J Trad Chin Med. 2015;56(18):1559–1563.
58. Xingying Q, Tang Q, Wencong C, et al. Literature quality assessment of Chinese medicine-related core outcome indicator set studies [J]. Chinese J Evidence-Based Med. 2024;24(02):192–201.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.