Back to Journals » International Journal of General Medicine » Volume 18
Analysis of the Correlation Between Serum Procalcitonin (PCT), C-Reactive Protein (CRP) Levels and the Occurrence/Severity of Bronchopulmonary Dysplasia in ELBW/VLBW Neonates
Authors Wang J, Zhang S, Dong X, Chen J, Li M
Received 10 August 2025
Accepted for publication 15 November 2025
Published 23 December 2025 Volume 2025:18 Pages 7775—7783
DOI https://doi.org/10.2147/IJGM.S559764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Reynold Panettieri Jr
Jiaan Wang, Shu Zhang, Xian Dong, Jinwen Chen, Ming Li
Neonatal Department, Hefei Maternal and Child Health Hospital, Hefei, Anhui, 230000, People’s Republic of China
Correspondence: Ming Li, Email [email protected]
Objective: This study aimed to analyze the correlation between serum levels of Procalcitonin (PCT) and C-reactive protein (CRP) and the occurrence and severity of Bronchopulmonary Dysplasia (BPD) in Extremely Low Birth Weight (ELBW) and Very Low Birth Weight (VLBW) neonates, and to identify associated risk factors.
Methods: A retrospective analysis was conducted on 213 ELBW/VLBW neonates admitted between January 2021 and January 2024. According to BPD diagnosis, they were categorized into a control group (n=62, without BPD) and an observation group (n=151, with BPD). The observation group was further stratified by severity into mild (n=71), moderate (n=46), and severe (n=34) BPD. Serum PCT and CRP levels were compared across groups. The correlation between these biomarkers and BPD severity was analyzed, and risk factors for BPD were investigated.
Results: PCT and CRP levels were significantly higher in the observation group than in the control group (P< 0.05). A significant increasing trend in both PCT and CRP levels was observed with worsening BPD severity (P< 0.05). Spearman analysis confirmed positive correlations between BPD severity and PCT (r=0.354) and CRP (r=0.472) levels (P< 0.05). Multivariate logistic regression identified intrauterine infection, gestational age < 28 weeks, assisted ventilation > 2 weeks, infectious pneumonia, and FiO2 > 40% as independent risk factors for BPD (P< 0.05).
Conclusion: In this retrospective study, elevated serum PCT and CRP levels were positively associated with the severity of BPD in ELBW/VLBW neonates. The identified risk factors, including intrauterine infection, gestational age < 28 weeks, prolonged assisted ventilation, infectious pneumonia, and high FiO2, are independently associated with BPD. These findings suggest that monitoring these biomarkers and risk factors may warrant intensified clinical attention.
Keywords: extremely and very low birth weight neonates, PCT, CRP, bronchopulmonary dysplasia in children, correlation, risk factors
Introduction
Bronchopulmonary dysplasia (BPD) remains the most common chronic respiratory disease complicating the clinical course of extremely low birth weight (ELBW, <1000g) and very low birth weight (VLBW, <1500g) neonates. With advances in perinatal care and the widespread use of pulmonary surfactant and non-invasive ventilation, the survival rate of these fragile infants has significantly improved. However, this has led to a changing epidemiology of BPD, now characterized more by arrested alveolar and vascular development in extremely immature lungs, rather than the classic barotrauma and oxygen toxicity seen historically.1 Despite these advancements, BPD continues to affect approximately 40% of ELBW infants, representing a major cause of long-term pulmonary and neurodevelopmental morbidity.2,3
The pathogenesis of BPD is multifactorial, involving genetic predisposition, prenatal and postnatal insults, but inflammation is recognized as a central driving mechanism.4 Both antenatal factors such as chorioamnionitis and postnatal exposures including mechanical ventilation and infection can trigger a sustained pro-inflammatory cascade in the immature lung, disrupting normal signaling pathways critical for alveolarization and microvascular maturation.5
In this context, biomarkers capable of quantifying this inflammatory state are of great clinical interest. Procalcitonin (PCT) and C-reactive protein (CRP) are well-established serum biomarkers for diagnosing and monitoring bacterial infections. PCT, the prohormone of calcitonin, rises rapidly in response to pro-inflammatory stimuli, particularly of bacterial origin, while CRP is an acute-phase protein synthesized by the liver.6 Beyond their role in infection, accumulating evidence suggests that both biomarkers are elevated in non-infectious inflammatory states and may reflect the magnitude of systemic inflammation.7 A few preliminary studies have explored the potential link between these inflammatory markers and respiratory outcomes in preterm neonates. For instance, elevated CRP levels in the first week of life have been associated with an increased risk of BPD development, and PCT has been proposed as a marker for sepsis-associated lung injury.8,9 However, the existing literature is often limited by small sample sizes or a narrow focus solely on infection. A comprehensive analysis simultaneously evaluating the correlation of both PCT and CRP with the subsequent occurrence and, crucially, the graded severity of BPD in a well-defined ELBW/VLBW cohort is still lacking.
Therefore, this study aimed to bridge this gap by performing a retrospective analysis of ELBW/VLBW neonates in our institution. Our primary objective was to determine whether serum levels of PCT and CRP, measured in the early clinical course, are correlated with the subsequent development of BPD and its severity. Secondly, we sought to identify and consolidate other pertinent clinical risk factors for BPD within our population. We hypothesize that higher levels of these inflammatory markers are positively associated with more severe forms of BPD. The findings from this study may contribute to earlier identification of high-risk neonates, potentially allowing for more targeted monitoring and preventive strategies.
Materials and Methods
Ethical Statement
This study was approved by the Hefei Maternal and Child Health Hospital’s Medical Ethics Committee with a waiver for informed consent due to its retrospective nature. Patient data will not be shared with third parties. All the methods were carried out in accordance with the Declaration of Helsinki.
Study Design and Participants
A retrospective cohort study was conducted by reviewing the medical records of 213 extremely low birth weight (ELBW, <1000 g) and very low birth weight (VLBW, <1500 g) neonates admitted to our hospital between January 2021 and January 2024.
The diagnosis and severity grading of Bronchopulmonary Dysplasia (BPD) were established according to the National Institute of Child Health and Human Development (NICHD) criteria.10 BPD was defined as a persistent oxygen requirement (Fraction of Inspired Oxygen, FiO2 >21%) for at least 28 days. Severity was assessed at 36 weeks’ postmenstrual age (for infants born at <32 weeks) or at 28–56 days of age (for those born at ≥32 weeks), and was classified as mild, moderate, or severe based on the level of respiratory support required. Based on this, neonates were categorized into a control group (non-BPD, n=62) and an observation group (BPD, n=151). The Observation Group was further stratified by severity into mild (n=71), moderate (n=46), and severe (n=34) subgroups.
Inclusion and Exclusion Criteria
Inclusion criteria were: (1) Birth weight <1500 g; (2) Admitted to the neonatal intensive care unit within 7 days of birth and survived for at least 28 days; (3) Availability of complete clinical data, including at least one measurement of serum PCT and CRP levels during the first 28 days of life.
Exclusion criteria were designed to minimize confounding factors and included: (1) Clinical diagnosis of maternal chorioamnionitis with amniotic fluid contamination; (2) Maternal use of teratogenic or clinically prohibited medications during pregnancy; (3) Neonates with major congenital anomalies, chromosomal abnormalities, or severe organ dysfunction (eg, severe congenital heart disease requiring surgery); (4) Death or discharge against medical advice within the first 28 days of life.
Data Collection
Clinical data were extracted from electronic medical records. To address potential confounding, the following maternal and neonatal variables were collected for subsequent comparative and regression analyses:
Maternal factors: mode of delivery (vaginal vs cesarean section), conception method (natural vs assisted reproduction), intrauterine infection, gestational hypertension, and gestational diabetes.
Neonatal factors: gestational age (<28 weeks vs ≥28 weeks), sex, birth weight (<1000 g vs ≥1000 g), occurrence of hospital-acquired infection, duration of assisted ventilation (>14 days vs ≤14 days), diagnosis of infectious pneumonia, history of neonatal asphyxia, and exposure to FiO2 >40%.
Measurement of Serum PCT and CRP
Regarding the timing of biomarker measurement: due to the retrospective nature of the study, PCT and CRP levels were not measured at a single, standardized time point for all infants. Instead, the first available measurement taken within the first 28 days after birth, primarily for clinical suspicion of early-onset sepsis or routine monitoring in high-risk infants, was utilized for analysis. Fasting venous blood samples were collected and centrifuged at 3500 rpm for 15 minutes. Serum PCT levels were quantified using an electrochemiluminescence immunoassay kit (Getein Biotech, Inc). Serum CRP levels were measured using a Beckman automated special protein analyzer (Beckman Coulter). The laboratory personnel performing these assays were blinded to the clinical outcomes (BPD status) of the neonates.
Statistical Methods
Statistics version 22.0 (IBM Corp). Prior to analysis, the baseline characteristics of the non-BPD and Observation Groups were compared to assess for significant differences in potential confounders, such as gestational age and birth weight. Normally distributed continuous data were presented as mean ± standard deviation and compared using the Independent-Samples t-test (for two groups) or one-way ANOVA (for multiple groups). Categorical data were expressed as numbers (percentages) and compared using the Chi-square test or Fisher’s exact test, as appropriate.
The correlation between BPD severity (ordinal scale: mild, moderate, severe) and serum PCT/CRP levels was evaluated using Spearman’s rank correlation coefficient. A Spearman correlation coefficient (r) of 0.3–0.5 is generally interpreted as a moderate association, which we considered clinically relevant for identifying a biological trend between inflammation and disease severity. Univariate and multivariate logistic regression analyses were performed to identify independent risk factors for BPD occurrence. Variables with a P-value < 0.05 in the univariate analysis were entered into the multivariate model. A formal sample size calculation was not performed a priori as this was a retrospective cases during the specified period. However, a post-hoc power analysis was conducted, which indicated that our sample size provided over 80% power to detect the observed differences in PCT and CRP between groups, with an alpha of 0.05. A two-tailed P-value < 0.05 was considered statistically significant for all tests.
Results
Baseline Characteristics of the Study Population
A total of 213 ELBW/VLBW neonates were included in this retrospective analysis, comprising 62 in the control group and 151 in the observation group. The baseline demographic and clinical characteristics of both groups are summarized in Table 1. There were no statistically significant differences between the two groups in terms of maternal mode of delivery, conception method, incidence of gestational hypertension or diabetes, birth weight distribution, rate of hospital-acquired infection, or history of neonatal asphyxia (all P > 0.05). However, as expected, the Observation Group had a significantly higher proportion of neonates with gestational age <28 weeks, intrauterine infection, prolonged assisted ventilation (>2 weeks), infectious pneumonia, and exposure to high oxygen (FiO2 >40%) (all P < 0.05).
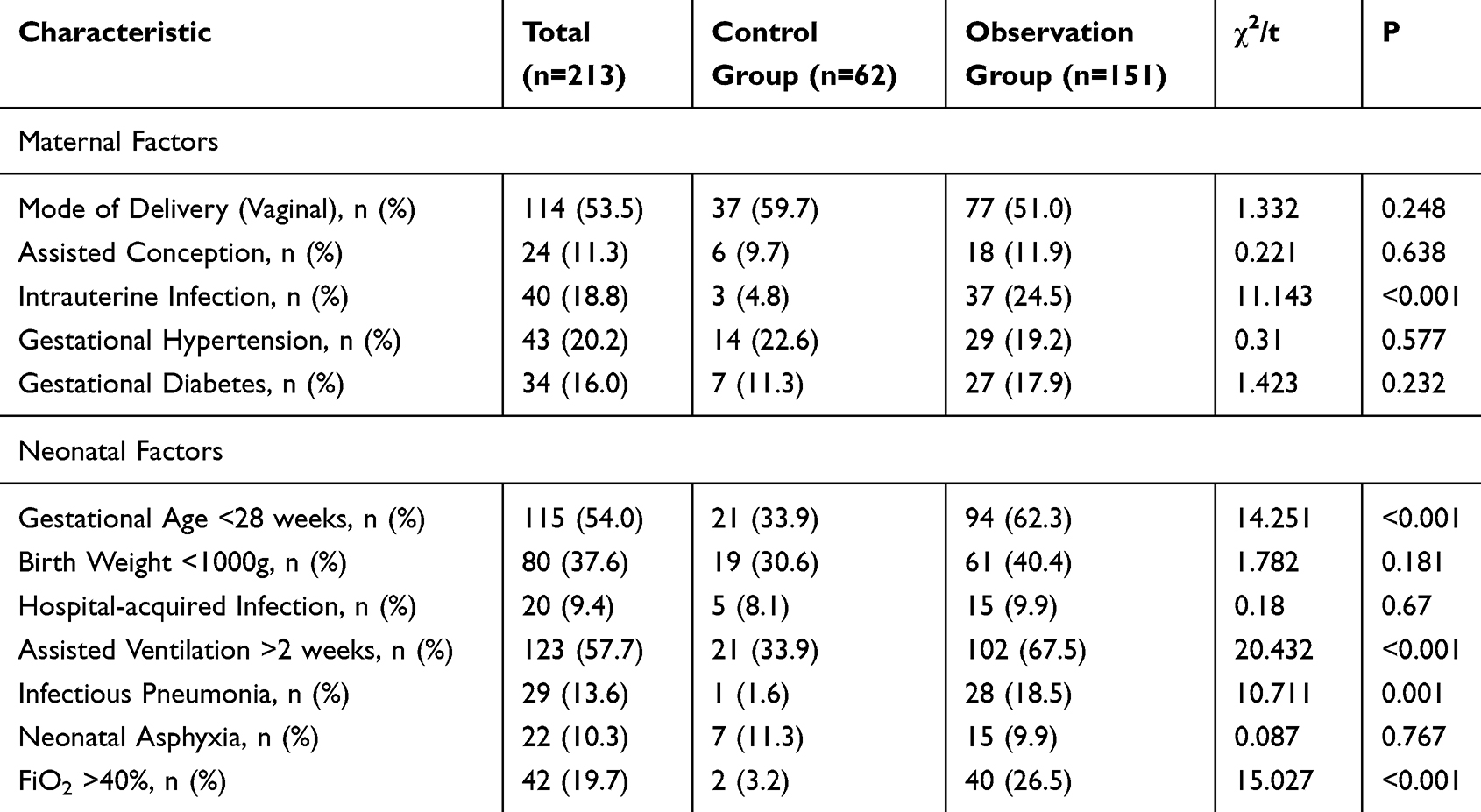 |
Table 1 Baseline Characteristics Between Groups |
Comparison of Serum PCT and CRP Levels Between Control Group and Observation Group
Compared with the control group, the levels of PCT and CRP in the observation group were significantly increased (P < 0.05), as shown in Table 2.
 |
Table 2 Comparison of Serum PCT and CRP Levels |
Comparison of Serum PCT and CRP Levels in Neonates with BPD of Different Severity
One-way ANOVA showed that as the severity of neonatal BPD increased, serum PCT and CRP levels exhibited a clear upward trend (P < 0.05), as shown in Table 3.
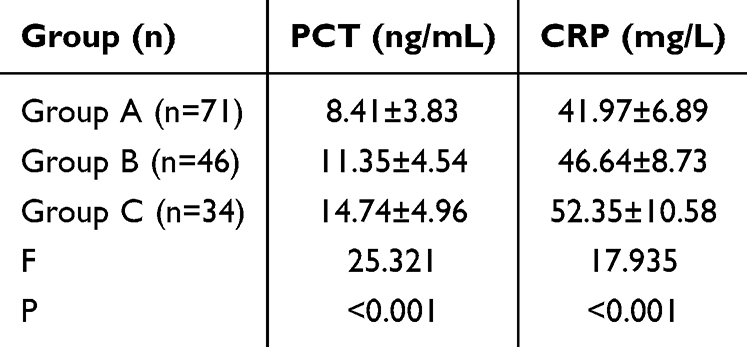 |
Table 3 Comparison of Serum PCT and CRP Levels in Neonates with BPD of Different Severity ( |

Correlation Analysis Between Serum PCT, CRP Levels and Severity of BPD
As shown in Figure 1, PCT and CRP levels were positively correlated with the severity of neonatal BPD (r = 0.354, 0.472; P < 0.05).
 |
Figure 1 Correlation Analysis between Serum PCT, CRP Levels and Severity of BPD. |
Univariate Analysis
Univariate analysis showed that intrauterine infection, gestational age <28 weeks, assisted ventilation >2 weeks, infectious pneumonia, FiO2 >40%, and extremely/very low birth weight were associated with the occurrence of BPD in neonates (P < 0.05), as shown in Table 4.
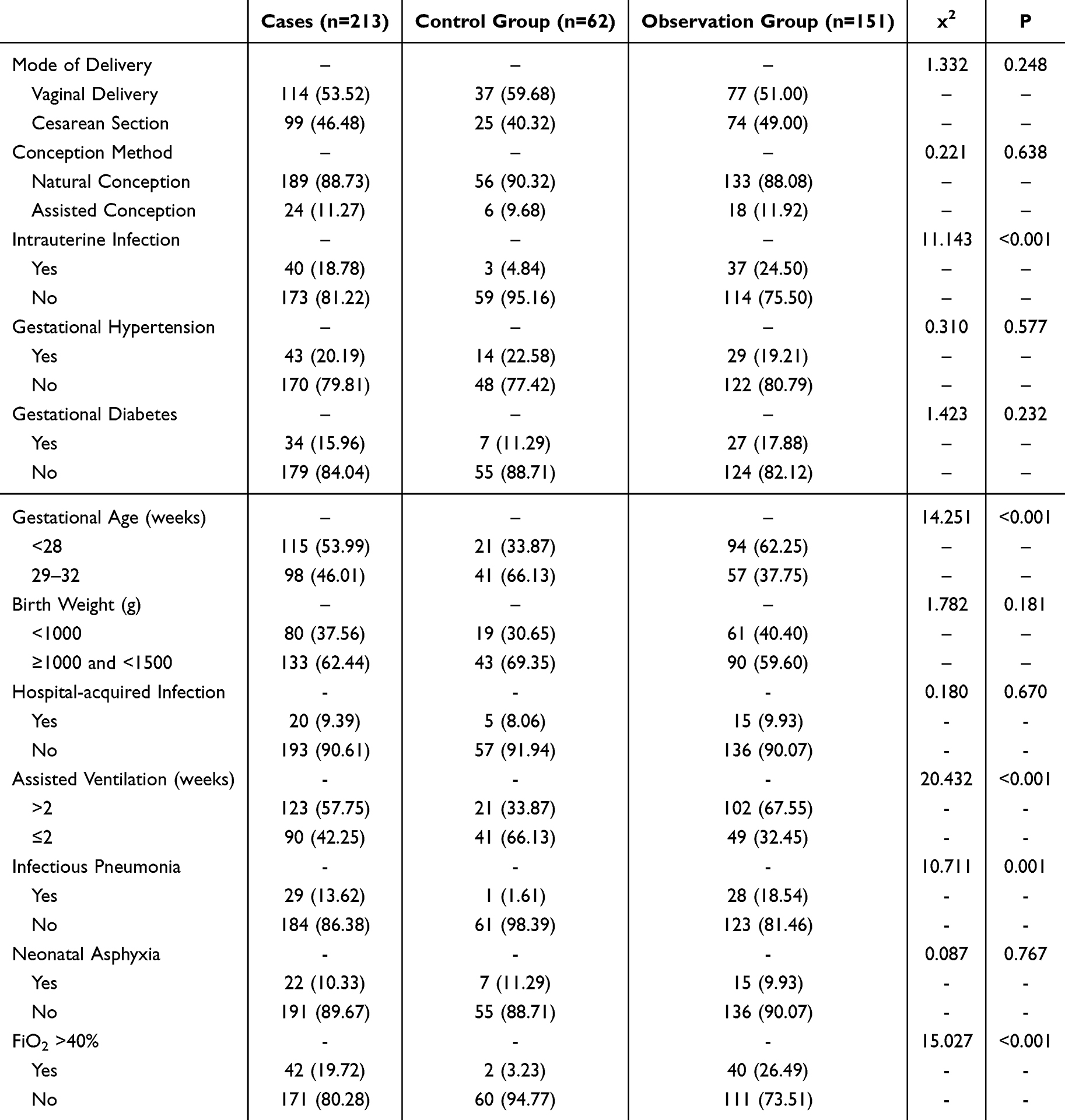 |
Table 4 Univariate Analysis [n (%)] |
Multivariate Logistic Regression Analysis
Taking the occurrence of BPD in neonates as the dependent variable, factors with statistical significance in univariate analysis were included as independent variables in multivariate logistic regression analysis. Variable assignments are shown in Table 5. The multivariate logistic regression analysis showed that intrauterine infection, gestational age <28 weeks, assisted ventilation >2 weeks, infectious pneumonia, and FiO2 >40% were all independent risk factors for the occurrence of BPD in extremely and very low birth weight neonates (P < 0.05), as shown in Table 6.
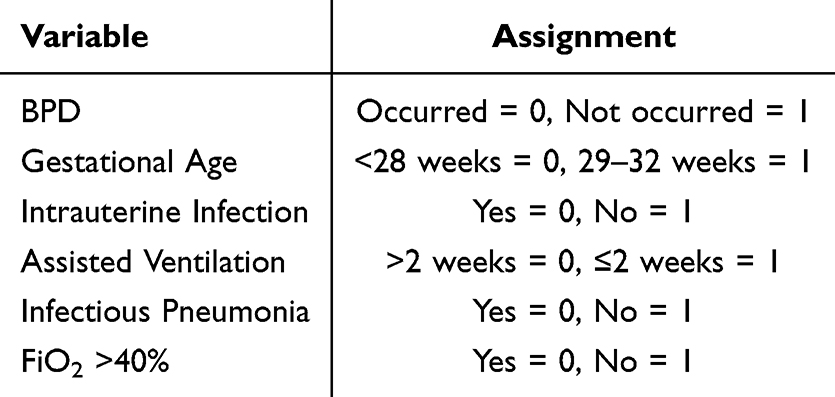 |
Table 5 Variable Assignment |
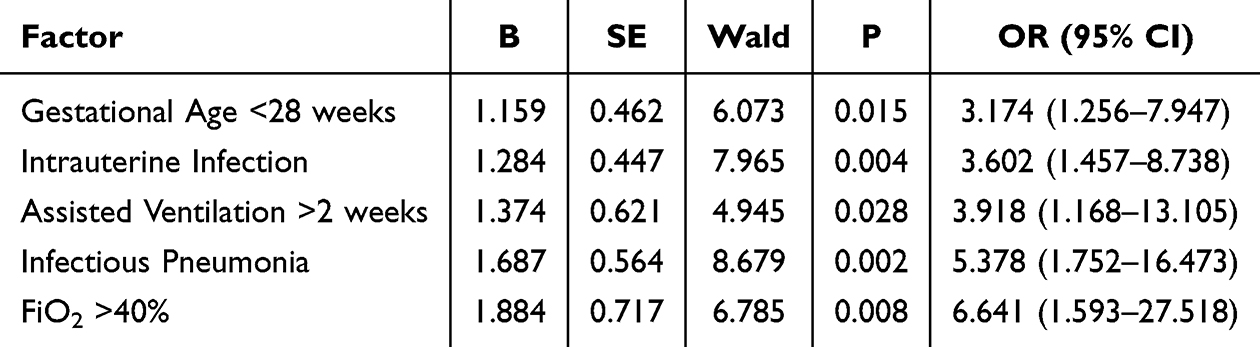 |
Table 6 Multivariate Logistic Regression Analysis |
Discussion
This retrospective study demonstrates that elevated serum levels of PCT and CRP are significantly associated with both the presence and increasing severity of BPD in ELBW and VLBW neonates. Furthermore, we identified intrauterine infection, gestational age <28 weeks, prolonged assisted ventilation, infectious pneumonia, and high oxygen exposure (FiO2 >40%) as independent risk factors for BPD development.
The central role of inflammation in the pathogenesis of BPD is well-established.11–13 Our findings align with this paradigm, showing that neonates who developed BPD had significantly higher levels of the inflammatory biomarkers PCT and CRP compared to the non-BPD group. This observation is consistent with previous literature. For instance, a study by Yang et al14 similarly reported elevated PCT and CRP in preterm infants with BPD, suggesting a sustained systemic inflammatory state. More importantly, we observed a clear gradient: serum levels of both biomarkers rose progressively with the severity of BPD, from mild to moderate to severe. The positive correlations, while modest (r=0.354 for PCT and r=0.472 for CRP), were statistically significant and indicate a measurable biological trend. In a multifactorial disease like BPD, where numerous genetic and environmental factors interplay, a moderate correlation from a single time-point measurement is clinically relevant. It suggests that the intensity of the inflammatory response, as captured by these biomarkers, is proportionally linked to the degree of subsequent lung injury and dysplastic repair.
The clinical implication of our findings lies in the potential of PCT and CRP to serve as adjunct, objective measures for risk stratification. While the diagnosis of BPD is clinical, quantifying this underlying inflammatory burden could help identify a subgroup of infants with a more pronounced “inflammatory phenotype” who might be at the highest risk for severe, long-term sequelae. Therefore, integrating serial PCT and CRP monitoring into the broader management strategy—which includes optimizing nutrition for lung growth, implementing lung-protective ventilation to minimize volutrauma/barotrauma, and rigorous infection control—could provide a more dynamic assessment of an infant’s trajectory. An upward trend might prompt clinicians to intensify supportive measures, such as a more aggressive weaning from mechanical ventilation or a thorough search for a subclinical infectious focus. However, caution is warranted in interpretation. As noted by Bianco et al,15 the physiological rise of PCT in the first days of life and the potential for blunted CRP response due to hepatic immaturity in ELBW infants mean that these biomarkers should not be used in isolation. They are pieces of a larger puzzle, to be interpreted in the full clinical context.
Our multivariate analysis reaffirms several well-documented risk factors for BPD. The strong association with lower gestational age (<28 weeks) underscores that the greatest risk factor for BPD is lung immaturity itself.14,16,17 The lungs of these extremely preterm infants are often in the late canalicular or early saccular stage, highly vulnerable to any postnatal insult. Similarly, the identification of prolonged assisted ventilation (>2 weeks) and FiO2 >40% as independent risk factors highlights the critical iatrogenic component of BPD pathogenesis, often termed “the new BPD”. Mechanical ventilation, while life-saving, can cause volutrauma and barotrauma, initiating a pro-inflammatory cascade.18–20 Concurrently, high-concentration oxygen therapy contributes to oxidative stress, overwhelming the underdeveloped antioxidant defenses of the preterm neonate and leading to further cellular injury.21 Our findings strongly support the clinical imperative to pursue non-invasive respiratory support whenever possible and to meticulously titrate oxygen delivery to the lowest sufficient level.
Furthermore, the role of infection and inflammation is highlighted by our results showing that both intrauterine infection and postnatal infectious pneumonia are potent independent risk factors. Antenatal inflammation can prime the fetal lung, making it hyper-responsive to postnatal insults,22–24 while postnatal pneumonia directly fuels the inflammatory fire in the lung parenchyma. This reinforces the importance of maternal antibiotic treatment for intrauterine infection and stringent infection prevention and control measures in the NICU.
Limitations
This study has several limitations that should be considered when interpreting the results. First, its retrospective and single-center nature may introduce selection bias and limits the generalizability of our findings. Second, as a retrospective study, we could not standardize the timing of PCT and CRP measurements. The use of a single measurement within the first 28 days precludes any analysis of the dynamic changes and predictive value of these biomarkers at specific, critical early time points (eg, the first 72 hours vs the third week of life). Future prospective studies should include serial measurements at predefined time points to establish more precise temporal relationships. Third, while we identified significant associations, the modest correlation coefficients remind us that PCT and CRP are part of a complex picture and not the sole determinants of BPD severity. Finally, our study elucidates associations but cannot prove causality, and the underlying molecular mechanisms linking PCT and CRP to aberrant lung development remain an area for future mechanistic investigation.
Conclusion
In conclusion, this study demonstrates that serum PCT and CRP levels are significantly associated with the presence and graded severity of BPD in ELBW and VLBW neonates. These inflammatory biomarkers may serve as valuable clinical tools for identifying high-risk infants and monitoring disease progression. Furthermore, we have confirmed that intrauterine infection, gestational age <28 weeks, prolonged assisted ventilation (>2 weeks), infectious pneumonia, and FiO2 >40% are independent risk factors for BPD in this vulnerable population.
Our findings underscore the central role of inflammation in BPD pathogenesis and highlight the importance of targeting modifiable risk factors. A comprehensive clinical strategy that integrates vigilant monitoring of inflammatory biomarkers with aggressive prevention of infections, strict lung-protective ventilation protocols, and cautious oxygen management is essential to mitigate the risk and burden of BPD.
Funding
‘Maternal and infant nutrition and health research project’ of maternal and child health care center of China Center for Disease Control and prevention in 2022 (Project No.: 2022fyh007).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Devyaltovskaya MG, Nikitchanko DY, Potapnev MP, et al. The first experience of application the umbilical cord-derived human autologous mesenchymal stromal cells for the rehabilitation therapy of premature infants with extremely low body weight and hypoxic-ischemic encephalopathy. Bull Exp Biol Med. 2022;174(1):142–146. doi:10.1007/s10517-022-05663-4
2. McEvoy CT, Schilling D, Go MD, et al. Pulmonary function in extremely low birth weight infants with bronchopulmonary dysplasia before hospital discharge. J Perinatol. 2021;41(1):77–83. doi:10.1038/s41372-020-00856-z
3. Lalitha R, Bitar E, Hicks M, et al. Pulmonary artery dopplers for early prediction of risk for bronchopulmonary dysplasia in extremely low birth weight babies. J Clin Ultrasound. 2022;50(3):385–392. doi:10.1002/jcu.23161
4. Bonadies L, Cavicchiolo ME, Priante E, et al. Prematurity and BPD: what general pediatricians should know. Eur J Pediatr. 2023;182(4):1505–1516. doi:10.1007/s00431-022-04797-x
5. Li Y, Min L, Zhang X. Usefulness of procalcitonin (PCT), C-reactive protein (CRP), and white blood cell (WBC) levels in the differential diagnosis of acute bacterial, viral, and mycoplasmal respiratory tract infections in children. BMC Pulm Med. 2021;21(1):386. doi:10.1186/s12890-021-01756-4
6. Liang P, Yu F. Value of CRP, PCT, and NLR in prediction of severity and prognosis of patients with bloodstream infections and sepsis. Front Surg. 2022;9:857218. doi:10.3389/fsurg.2022.857218
7. Jensen EA, Laughon MM, DeMauro SB, et al. Contributions of the NICHD neonatal research network to the diagnosis, prevention, and treatment of bronchopulmonary dysplasia. Semin Perinatol. 2022;46(7):151638. doi:10.1016/j.semperi.2022.151638
8. Savoy CD, Schmidt LA, McGowan PO, et al. Extremely low birth weight influences the relationship between stress and telomere length in adulthood. J Dev Orig Health Dis. 2021;12(2):328–334. doi:10.1017/S2040174420000409
9. Dini G, Ceccarelli S, Celi F. Strategies for the prevention of bronchopulmonary dysplasia. Front Pediatr. 2024;12:1439265. doi:10.3389/fped.2024.1439265
10. Bårdsen T, Røksund OD, Benestad MR, et al. Tracking of lung function from 10 to 35 years after being born extremely preterm or with extremely low birth weight. Thorax. 2022;77(8):790–798. doi:10.1136/thoraxjnl-2021-218400
11. Cho HY, Wang X, Campbell MR, et al. Prospective epigenome and transcriptome analyses of cord and peripheral blood from preterm infants at risk of bronchopulmonary dysplasia. Sci Rep. 2023;13(1):12262. doi:10.1038/s41598-023-39313-0
12. Zhang L, Bai X, Yan W. LncRNA-MALAT1, as a biomarker of neonatal BPD, exacerbates the pathogenesis of BPD by targeting miR-206. Am J Transl Res. 2021;13(2):462–479.
13. Callahan C, Haas L, Smith LT and Stewart MF. Multifaceted roles of nursing in the care of patients receiving car T-cell therapy for pediatric refractory or relapsed acute lymphoblastic leukemia. J Mod Nurs Pract Res. 2025;5(1):2. doi:10.53964/jmnpr.2025002.
14. Yang Y, Li J, Mao J. Early diagnostic value of C-reactive protein as an inflammatory marker for moderate-to-severe bronchopulmonary dysplasia in premature infants with birth weight less than 1500 g. Int Immunopharmacol. 2022;103:108462. doi:10.1016/j.intimp.2021.108462
15. Bianco B, François-Garret B, Butin M, et al. Procalcitonin in preterm neonates: a different threshold and prolonged interpretation. Front Pediatr. 2021;9:623043. doi:10.3389/fped.2021.623043
16. Kurata H, Ochiai M, Inoue H, et al. Inflammation in the neonatal period and intrauterine growth restriction aggravate bronchopulmonary dysplasia. Pediatr Neonatol. 2019;60(5):496–503. doi:10.1016/j.pedneo.2018.11.007
17. Straňák Z, Berka I, Širc J, et al. Role of umbilical interleukin-6, procalcitonin and C-reactive protein measurement in the diagnosis of fetal inflammatory response syndrome. Ceska Gynekol. 2021;86(2):80–85. doi:10.48095/cccg202180
18. Gilfillan M, Bhandari A, Bhandari V. Diagnosis and management of bronchopulmonary dysplasia. BMJ. 2021;375:n1974. doi:10.1136/bmj.n1974
19. Mahmoud RA, Schmalisch G, Oswal A, et al. Non-invasive ventilatory support in neonates: an evidence-based update. Paediatr Respir Rev. 2022;44:11–18. doi:10.1016/j.prrv.2022.09.001
20. Kim YH, Kim KW, Eun HS, et al. Small for gestational age birth may increase airflow limitation in bronchopulmonary dysplasia. Pediatr Pulmonol. 2020;55(2):346–353. doi:10.1002/ppul.24580
21. Huang J, Lin X-Z, Zheng Z, et al. [Influencing factors for the development and severity of bronchopulmonary dysplasia in preterm infants with a gestational age of <32 weeks and a birth weight of <1 500 g]. Zhongguo Dang Dai Er Ke Za Zhi. 2022;24(12):1326–1333. Xhosa. doi:10.7499/j.issn.1008-8830.2207013
22. Homan TD, Nayak RP. Short- and long-term complications of bronchopulmonary dysplasia. Respir Care. 2021;66(10):1618–1629. doi:10.4187/respcare.08401
23. Hennelly M, Greenberg RG, Aleem S. An update on the prevention and management of bronchopulmonary dysplasia. Pediatric Health Med Ther. 2021;12:405–419. doi:10.2147/PHMT.S287693
24. Daskalakis G, Psarris A, Koutras A, et al. Maternal infection and preterm birth: from molecular basis to clinical implications. Children. 2023;10(5). doi:10.3390/children10050907
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.