")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Analysis of Risk Factors for Otitis Media with Effusion in Children with Adenoid Hypertrophy
Authors Yang A, Jv M, Zhang J , Hu Y, Mi J, Hong H
Received 23 December 2022
Accepted for publication 17 February 2023
Published 28 February 2023 Volume 2023:16 Pages 301—308
DOI https://doi.org/10.2147/RMHP.S399499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Anni Yang,1,* Menglei Jv,2,* Jun Zhang,1,* Yuqi Hu,1 Jiaoping Mi,1 Haiyu Hong1
1Allergy Center, Department of Otolaryngology Head and Neck Surgery, The Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, People’s Republic of China; 2Department of Nephrology, The Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haiyu Hong, Allergy Center, Department of Otorhinolaryngology Hospital, The Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, People’s Republic of China, Email [email protected]
Objective: This study aimed to explore whether children with AH have a higher obesity prevalence and analyze the risk factors for otitis media with effusion(OME) in AH children.
Methods: AH patients aged 3– 12 years old that were hospitalized in our hospital for adenoidectomy from June 2020 to September 2022 were included in this study. Height and weight were measured to calculate the body mass index, weight for height and weight z-score to evaluate the development of AH children. Propensity score matching was applied to minimize patient selection bias and adjust for confounding factors to analyze the risk factors for OME in children with AH.
Results: A total of 887 children with AH were enrolled in this study. The prevalence of overweight or obesity was higher in children with AH than the control group. The size of adenoids is significantly different between AH children with and without OME. For children aged over 5, there are significantly higher counts of white blood cells, neutrophils, and monocytes in the AH children with OME than those without OME. More individuals represent to be atopic in children with OME than those without OME.
Conclusion: The obstruction of the Eustachian tube is the most important factor of OME in AH children. It seems that there is no apparent correlation between OME and atopic conditions in AH children. In addition to surgical resection of adenoids, active control of infection and inflammation are also important to prevent OME for AH children aged over 5.
Keywords: adenoid hypertrophy, otitis media with effusion, risk factors, atopic conditions
Introduction
Adenoid hypertrophy(AH), which is a natural response to increased immunologic activity in early life is the most common cause of upper airway obstruction in children and adolescents.1,2 Studies have shown that the prevalence of AH is about 42–70%.3 The high incidence of adenoid hypertrophy and a series of complications such as mouth breathing, obstructive sleep apnea, otitis media with effusion(OME), sinusitis, and craniofacial anomalies caused by severe upper airway obstruction make the parents pay more attention to it.4
The global prevalence of obesity has tripled over the past decade, both in adults and children.5,6 Previous studies6,7 have suggested a possible relationship between adenotonsillar hypertrophy and obesity rates. Nevertheless, considering the small sample size, the correlation between obesity and adenoid hypertrophy is worthy of further study.7 Meanwhile, as a common complication of adenoidal hypertrophy, related studies also point out that obesity is associated with the occurrence of OME.5 However, in AH children, whether obesity is associated with OME remains to be further analyzed. Some factors, such as allergy and infection, are thought to be involved in the development of OME.8 Therefore, atopic condition and infection are probably the risk factors of OME in children with AH and it is warranted to further study.
In this study, we aimed to evaluate the development of children with AH and whether the children with AH have a higher obesity prevalence. Propensity score matching(PSM), as a statistical method that offers certain advantages over more traditional regression methods to reduce confounding biases in observational studies9 was applied in this study in analyzing the risk factors of otitis media with effusion in children of adenoid hypertrophy.
Methods
This is a retrospective study conducted at the Fifth Affiliated Hospital of Sun Yat-sen University in southern china. AH patients aged 3–12 years old that were hospitalized in the hospital for adenoidectomy from June 2020 to September 2022 were included in this study. Children with any other chronic diseases, recurrent otitis media, recurrent tonsillitis, upper respiratory tract infection, a history of fever within two weeks, pneumonia, congenital diseases, and other infectious diseases were excluded. Children with OME who had myringotomy at the same time as the adenoidectomy were included in the OME group. The remaining patients were included in the NOME group. A variety of demographic information was collected, including sex, age, height, weight and disease duration. The size of the tonsils and adenoids was recorded prior to surgery. Tonsils were graded as follows:10 Grade I, tonsil confined to tonsillar fossa; Grade II, tonsils extending just outside the anterior pillars; Grade III, tonsils extending outside the posterior pillars but not meeting in the midline; and Grade IV, tonsils meeting in the midline and almost completely obstructing the airway. Size of the adenoids was graded based on the percentage of adenoid tissue occupying the rhinopharyngeal cavity: grade 1 (<25%); grade 2 (<50%); grade 3 (<75%); and grade 4 (>75%).11
To explore whether overweight and obesity are related to AH and the occurrence of OME in AH children, the height and weight of each child were measured to calculate the weight-for-age z-score(WAZ), height-for-age z-score (HAZ) and BMI-for-age z-score (BAZ) by the WHO anthro and anthroplus package in R 4.2.1 software.12 The BAZ of children reported in the study13 that investigated the BAZ of Chinese children all over the country were included in the control group. The BAZ ≥1 was defined as overweight, and BAZ ≥2 was defined as obesity.
Standard laboratory procedures were used to collect blood samples from all participants for further analysis. The ImmunoCAP 100 (Uppsala, Sweden) was used to measure serum Immunoglobulin E(sIgE)specific to Dermatophagoides pteronyssinus, Dermatophagoides farinae, Penicillium notatum, Cladosporium herbarum, Aspergillus fumigatus, dog dander, cat epithelia, egg, milk, wheat flour, fish, peanut, soybean, common ragweed, mugwort sagebrush, willow, and poplar. It is considered to be positive when a sIgE value ≥0.35 kU/L. Individuals who are positive for at least one of these allergens are considered to be atopic.14
PSM was applied to minimize patient selection bias and adjust for confounding factors between patients in OME and NOME groups. One to two matched analyses using nearest-neighbor matching were performed with 0.03 standard deviations of the logit of the propensity score as the caliper value. Patients were then divided into two groups according to age to analyze the differences between OME and NOME groups in children of different ages.
Statistical analyses were carried out using SPSS 24.0 software (SPSS, Inc.; Chicago, IL, USA) and R 4.2.1 software. Continuous variables and categorical variables were presented as mean±standard deviation(SD) and percentage, respectively. For normally distributed and skewed variables, independent samples t-tests and Mann–Whitney U-tests were used to examine differences between the two groups. Chi-square test was performed to compare the categorical variables in two groups. Statistical significance was determined when p<0.05 for all statistical tests.
Results
Overweight and Obesity Rate Analysis of AH Children
A total of 887 AH children were included in this study (550 boys and 337 girls). The mean age of the enrolled patients is 5.71±2.23 years. The Distributions of 3 scores (HAZ, WAZ, BAZ) of AH children are shown in Table 1. The overweight and obesity rates of AH children are 11.61% and 9.58%. The overweight rate of AH boys and girls is 12.55% and 10.09%, respectively. However, the obesity rate of AH boys and girls is 11.27% and 6.82%, respectively. The obesity rate of AH boys is much higher than AH girls.
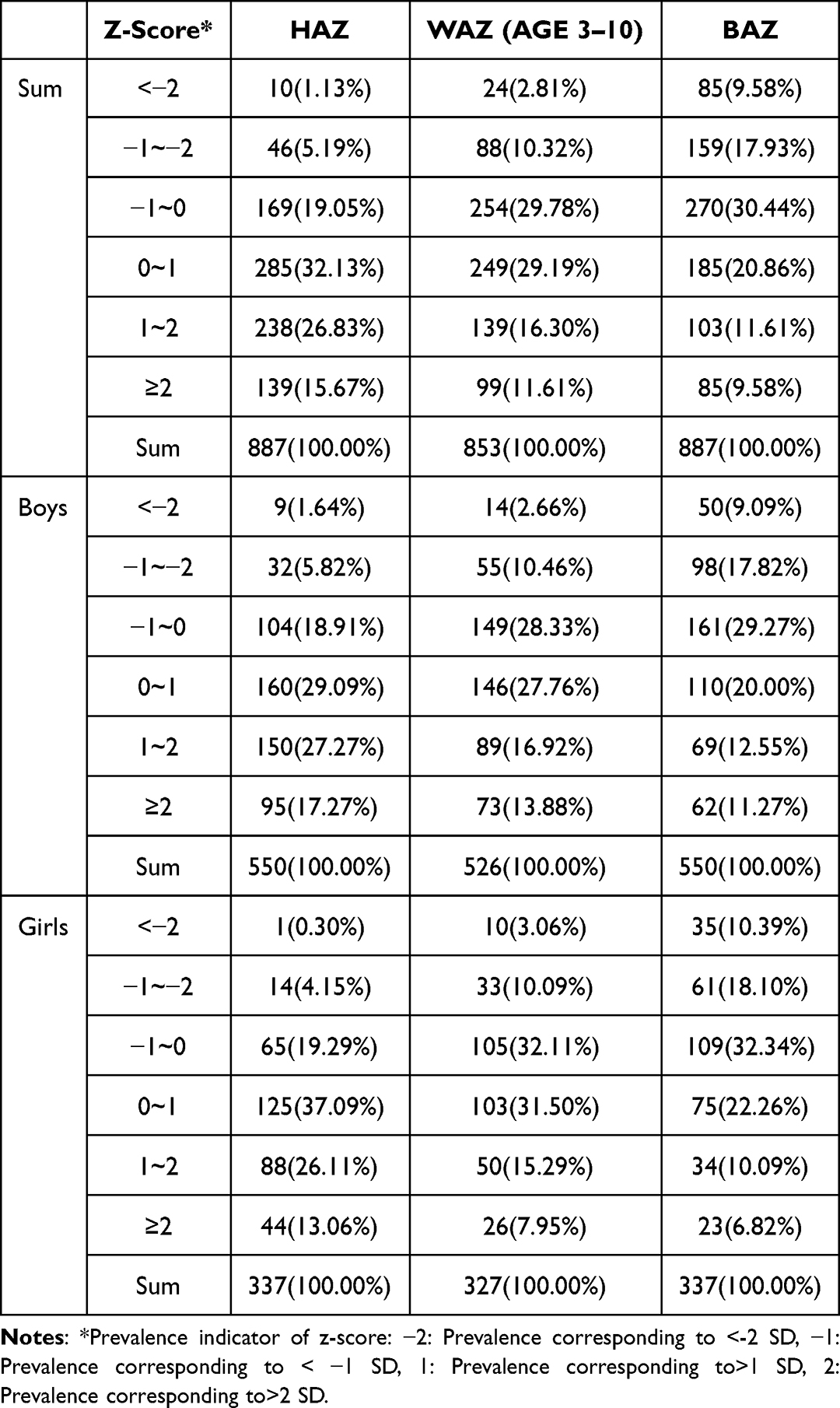 |
Table 1 Distributions of 3 Scores (HAZ, WAZ, BAZ) of AH Children |
The overweight and obesity rates of AH children are higher than those of Chinese children reported by the recent nationwide research13 (control group) (p<0.05). For AH girls, there is no significant difference in overweight and obesity rates compared with the reported prevalence. The obesity and overweight rates of AH boys are 11.27% and 12.55%, which are significantly higher than AH girls (p<0.05). Moreover, the obesity and overweight rates of AH boys are also significantly higher than those of boys in the control group (p<0.05). The details are in Table 2.
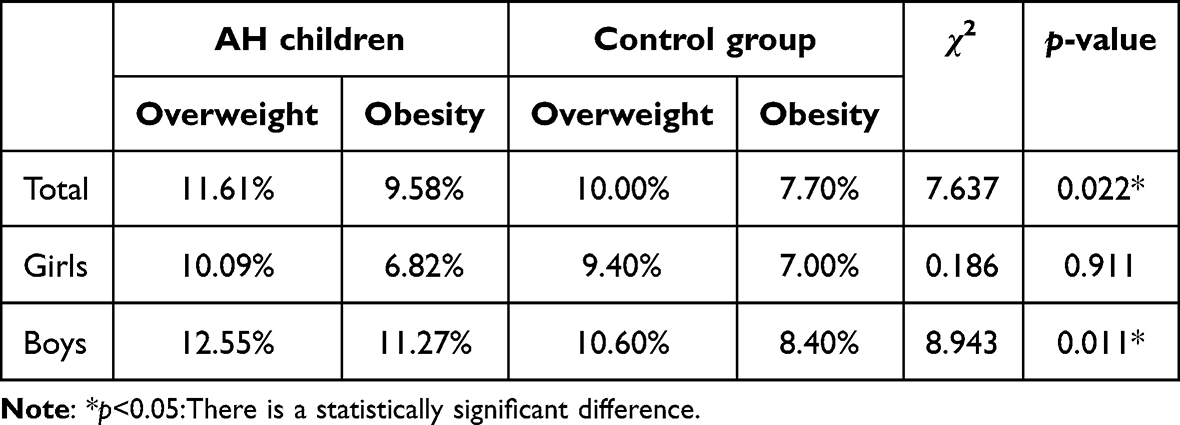 |
Table 2 Comparison of BAZ for AH Children and Control Group |
Patient Characteristics of AH Children with and without OME
Of the enrolled AH children, 626 patients were allergic to at least one allergen. 143 with OME and 744 without OME were included in the OME and NOME groups. As it is shown in Table 3, the age and the size of adenoids are significantly different between OME and NOME groups (p=0.008 and p=0.041, respectively). The age of OME group is older than the NOME group. Compared with the NOME group, more patients with adenoid hypertrophy of grade 4. There is no significant difference in gender, duration, BAZ, and the size of the tonsils. 142 and 275 patients with and without OME were selected after one to two nearest-neighbor matching PSM analyses. There is no significant difference in gender, age, duration, BAZ, tonsil size, and adenoid size after PSM.
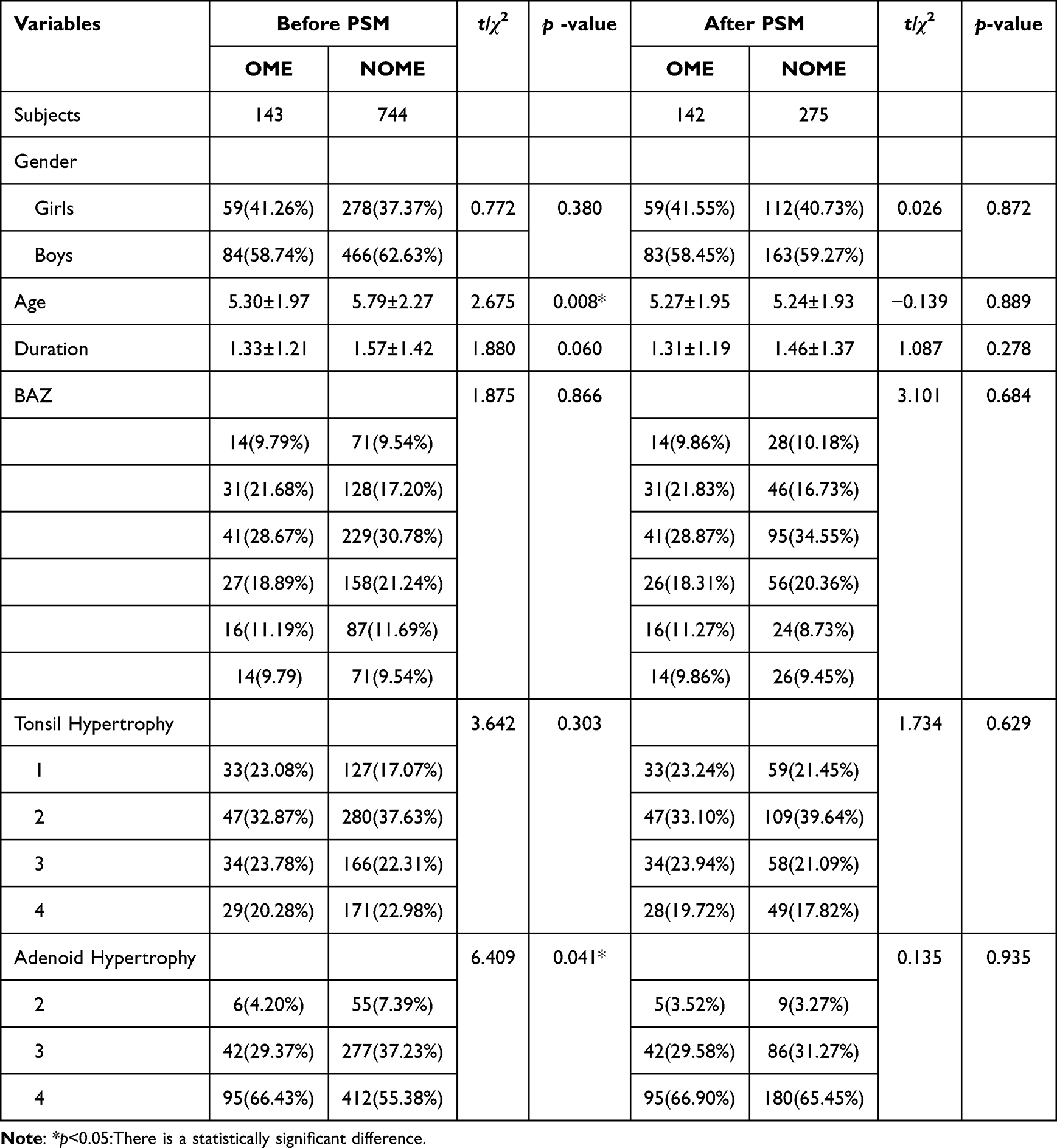 |
Table 3 Baselines of AH Children with and without OME Before PSM and After PSM |
Peripheral Blood Parameters Analysis
From the peripheral blood parameters analysis, the counts of white blood cells(WBC), Neutrophils, Neutrophils%, and monocytes are much higher in the OME group than in the NOME group (p<0.05). A greater proportion of patients in NOME group than that of OME group represent to be atopic (Table 4).
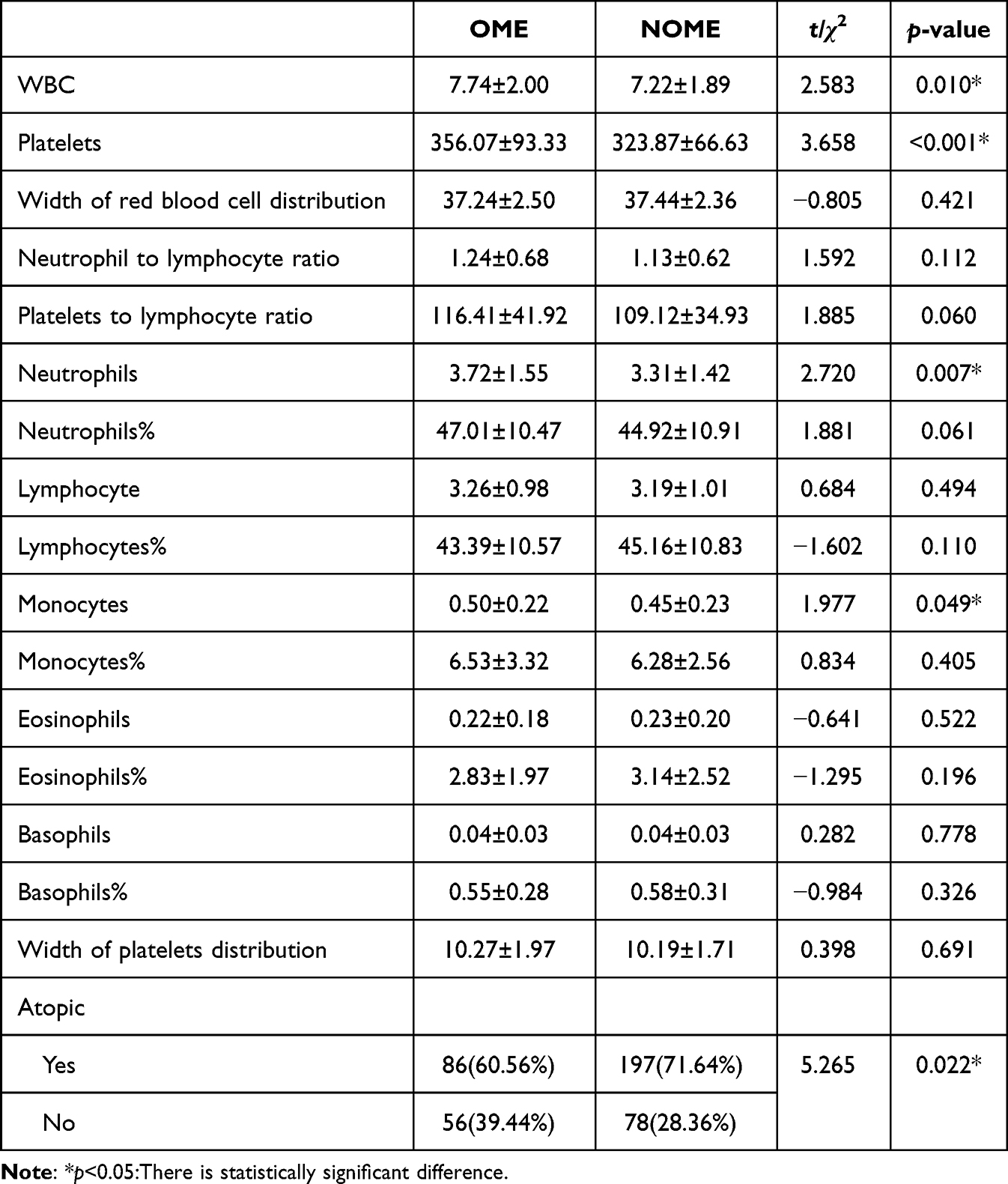 |
Table 4 The Peripheral Blood Parameters Analysis Between OME and NOME After PSM |
Peripheral Blood Parameters Analysis in Different Age Sub-Groups
To further analyze the differences between AH patients with and without OME in different age groups. We divided the propensity score-matched cohort into two age groups: ≤5 years (n=273) and >5 years (n=144) (Table 5). Only the count of Platelets and Neutrophil to lymphocyte ratio showed statistically significant results between OME and NOME groups in AH children under 5 years of age. For AH children older than 5 years, the counts of WBC, Platelets, Neutrophils, and monocytes exhibited a significant elevation in the OME group (p<0.05).
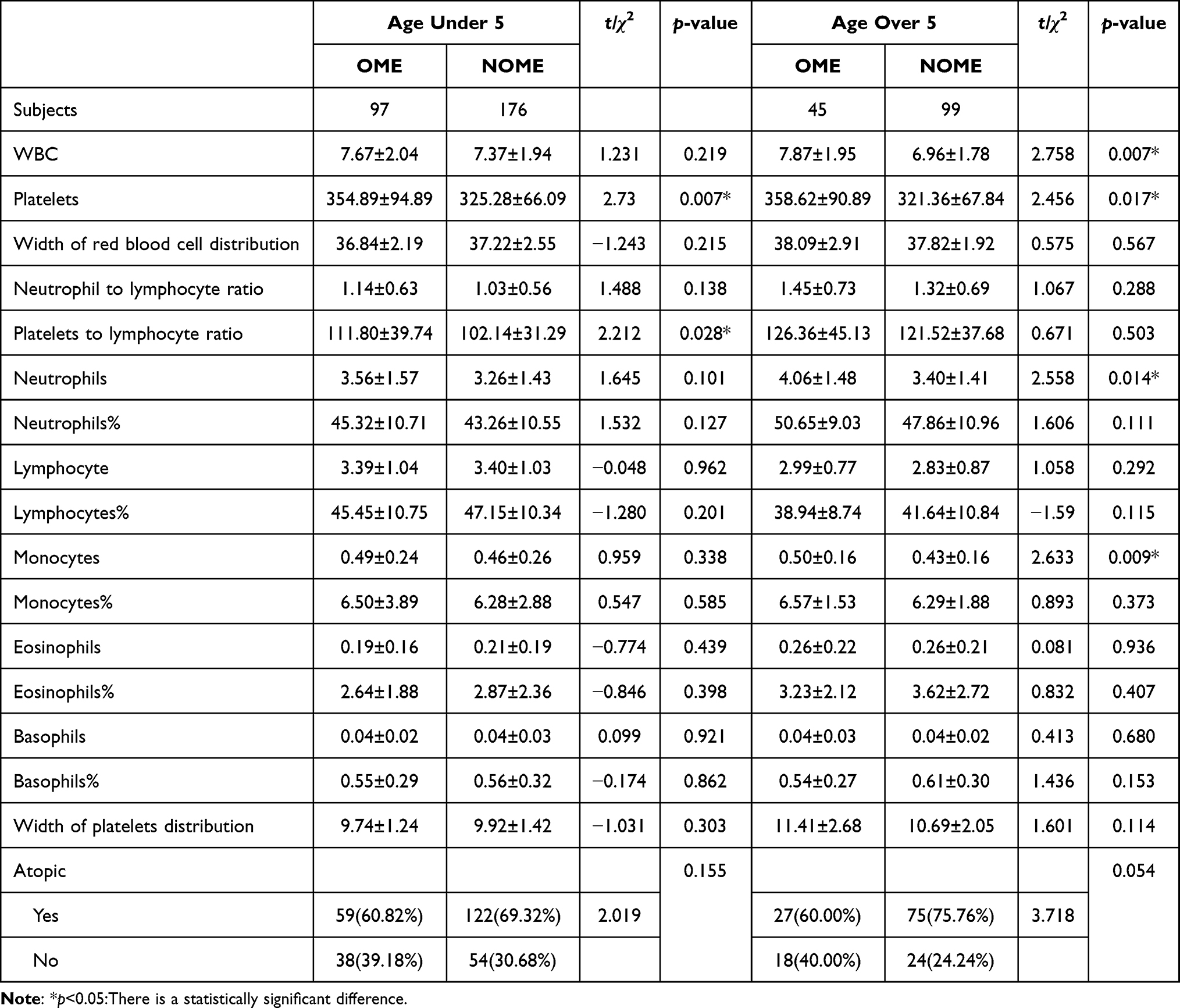 |
Table 5 Peripheral Blood Parameters Analysis in Different Age Sub-Groups |
Discussion
In this study, we analyzed growing development in children with AH according to the WHO criteria. And we compared the growing development data of AH patients with the national survey of children.13 The overweight and obesity rate of AH children was significantly higher than in the control group.13 This is consistent with the previous studies that have suggested a possible association between obesity and adenotonsillar hypertrophy.6,7 Adipose tissue deposited around the pharynx and neck, along with hypertrophic adenoids largely plays a part in obstructive sleep apnea(OSA) in obese children.7,15–17 Therefore, obese or overweight AH children are more likely to have symptoms such as snoring and open-mouth breathing getting their parents’ attention to accepting further treatment in the hospital. It is therefore important for obese or overweight children to be aware of nasal congestion, snoring, open-mouth breathing, as well as other symptoms of AH in order to receive early treatment to prevent serious OSA. The overweight and obesity rate of boys both in AH and the control group is higher than that of girls. A common phenomenon, parental son preference in China that makes families pay more attention to boys may be the reason for this difference.
Age and the size of adenoid are found to be significantly different between AH children with and without OME in our study. The age of AH children with OME is significantly lower than that of AH children without NOME. Compared to the NOME group, more patients in the OME group with grade 4 adenoid hypertrophy with statistical significance. Thereby, young children with low immunity and the hypertrophic adenoids compress or obstruct the Eustachian tube ostium are the main risk factors for OME in AH patients. Previous studies have suggested that being overweight and obese are the risk factors for OME.5,18 However, our results indicated that there were no significant differences in the rates of obesity and overweight between OME and NOME groups. This difference is probably due to AH in children not being included in the risk factors analysis. Therefore, obesity or being overweight is probably not the risk factor for OME in children with AH.
Then, PSM analysis was applied to exclude the confounding factors to analyze the difference of indicators in the peripheral blood between the OME and NOME groups. In this study, statistically significant elevated WBC, neutrophils, and monocytes counts were founded in the OME group compared to the NOME group (p<0.05).
The current study showed that 70.57% (626/887) AH children were sensitive to at least one allergen, which is in agreement with the previous study19 that reported 66.8% adenoidal hypertrophy children with atopy. A study20 investigated the allergic sensitization of children in southern China found that 59.70% of children were allergic to at least one allergen. This result is consistent with the previous studies,19–22 indicating this is a close association between AH and allergy. Interestingly, previous studies have indicated that there is an independent relationship between allergic responses and OME.23,24 However, our results show that there are more atopic individuals in the NOME group. There was no significant difference in allergy-related indicators25–27 such as the count of eosinophils and basophils in the two groups. In previous studies, the obstruction of the Eustachian tube caused by AH has not been included in the analysis.23,24 For this reason, we propose that for AH children, the atopic response is not the critical risk factor for the occurrence of OME. Furthermore, the risk factors of OME are found to be different in the two age-subgroups. In children aged under 5, no statistically significant difference in meaningful indicators was seen in the peripheral blood parameters between the OME and NOME groups. Nevertheless, for children aged over 5, this study showed significantly higher counts of WBC, neutrophils, and monocytes in the OME group compared to the NOME group. Thus, these results demonstrated that for AH children aged under 5, the obstruction of the Eustachian tube caused by AH is the main risk factor of OME; and for AH children aged over 5, infection and the immune response are the critical risk factors of OME in addition to the obstruction of the Eustachian tube caused by AH.
Our study had several limitations. Indicators of infection or inflammation such as C-reactive protein and procalcitonin were not included in this study. Another limitation is that this is a single-center study. A multicenter study with more subjects should be conducted for further research.
Conclusion
Overall, obesity or being overweight is not a risk factor for OME in AH children. The obstruction of the Eustachian tube is the main risk factor of OME in AH children under 5. The infection and immune response are also involved in the occurrence of OME in AH children over 5. In addition to surgical resection of adenoids, active control of infection and inflammation are also important to prevent OME for AH children age over 5. And it seems that there is no apparent correlation between OME and atopic conditions in AH children.
Ethics Statement
This study followed the guidelines outlined in the Declaration of Helsinki and was approved by the Ethics Committee of the Fifth Affiliated Hospital of Sun Yat-sen university. Since this is a retrospective study in addition only clinical data and completed test results were collected. An exemption for informed consent was applied and approved by the Ethics Committee.
Acknowledgments
This study is supported by the National Natural Science Foundation of China (82071018).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brambilla I, Pusateri A, Pagella F, et al. Adenoids in children: advances in immunology, diagnosis, and surgery. Clin Anat. 2014;27(3):346–352. doi:10.1002/ca.22373
2. Feng X, Li G, Qu Z, et al. Comparative analysis of upper airway volume with lateral cephalograms and cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2015;147(2):197–204. doi:10.1016/j.ajodo.2014.10.025
3. Pereira L, Monyror J, Almeida FT, et al. Prevalence of adenoid hypertrophy: a systematic review and meta-analysis. Sleep Med Rev. 2018;38:101–112. doi:10.1016/j.smrv.2017.06.001
4. Scadding G. Non-surgical treatment of adenoidal hypertrophy: the role of treating IgE-mediated inflammation. Pediatr Allergy Immunol. 2010;21(8):1095–1106. doi:10.1111/j.1399-3038.2010.01012.x
5. Kaya S, Selimoglu E, Cureoglu S, et al. Relationship between chronic otitis media with effusion and overweight or obesity in children. J Laryngol Otol. 2017;131(10):866–870. doi:10.1017/S002221511700161X
6. Zatonski T, Pazdro-Zastawny K, Kolator M, et al. A study on health and the association between overweight/obesity and otorhinolaryngological diseases in 6- to 17-year-old children from Wroclaw, Poland. Arch Med Sci. 2022;18(2):413–421. doi:10.5114/aoms.2020.97285
7. Daar G, Sari K, Gencer ZK, et al. The relation between childhood obesity and adenotonsillar hypertrophy. Eur Arch Otorhinolaryngol. 2016;273(2):505–509. doi:10.1007/s00405-015-3554-4
8. Cantone E, Gallo S, Torretta S, et al. The role of allergen-specific immunotherapy in ENT diseases: a systematic review. J Pers Med. 2022;12(6):946. doi:10.3390/jpm12060946
9. Liang J, Hu Z, Zhan C, et al. Using propensity score matching to balance the baseline characteristics. J Thorac Oncol. 2021;16(6):e45–e46. doi:10.1016/j.jtho.2020.11.030
10. Bokov P, Boujemla I, Matrot B, et al. Oropharyngeal obstruction and respiratory system compliance are linked to ventilatory control parameters in pediatric obstructive sleep apnea syndrome. Sci Rep. 2022;12(1):17340. doi:10.1038/s41598-022-22236-7
11. Acharya K, Bhusal CL, Guragain RP. Endoscopic grading of adenoid in otitis media with effusion. JNMA J Nepal Med Assoc. 2010;49(177):47–51.
12. Chan B. Data analysis using r programming. Adv Exp Med Biol. 2018;1082:47–122.
13. Yang Y, Zhang M, Yu J, et al. Nationwide trends of pediatric obesity and BMI z-score from 2017–2021 in China: comparable findings from real-world mobile- and hospital-based data. Front Endocrinol. 2022;13:859245. doi:10.3389/fendo.2022.859245
14. Johansson SG, Hourihane JO, Bousquet J, et al. A revised nomenclature for allergy. An EAACI position statement from the EAACI nomenclature task force. Allergy. 2001;56(9):813–824. doi:10.1034/j.1398-9995.2001.t01-1-00001.x
15. Perez C. Obstructive sleep apnea syndrome in children. Gen Dent. 2018;66(6):46–50.
16. Kang KT, Lee PL, Weng WC, et al. Body weight status and obstructive sleep apnea in children. Int J Obes. 2012;36(7):920–924. doi:10.1038/ijo.2012.5
17. Hsu WC, Kang KT, Weng WC, et al. Impacts of body weight after surgery for obstructive sleep apnea in children. Int J Obes. 2013;37(4):527–531. doi:10.1038/ijo.2012.194
18. Kim SH, Park DC, Byun JY, et al. The relationship between overweight and otitis media with effusion in children. Int J Obes. 2011;35(2):279–282. doi:10.1038/ijo.2010.144
19. Zhang YJ, Yuan F, Liu YH, et al. 腺样体肥大儿童的变应原检测及病因探讨 [Allergen detection and etiological study of adenoidal hypertrophy in children]. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017;31(7):549–551. Chinese. doi:10.13201/j.issn.1001-1781.2017.07.014
20. Liu T, Lai SY, Li WS, et al. Prevalence of food allergen and aeroallergen sensitization among children in Sichuan province. Medicine. 2020;99(27):e21055. doi:10.1097/MD.0000000000021055
21. Sadeghi-Shabestari M, Jabbari MY, Ghaharri H. Is there any correlation between allergy and adenotonsillar tissue hypertrophy? Int J Pediatr Otorhinolaryngol. 2011;75(4):589–591. doi:10.1016/j.ijporl.2011.01.026
22. Evcimik MF, Dogru M, Cirik AA, et al. Adenoid hypertrophy in children with allergic disease and influential factors. Int J Pediatr Otorhinolaryngol. 2015;79(5):694–697. doi:10.1016/j.ijporl.2015.02.017
23. Byeon H. The association between allergic rhinitis and otitis media: a national representative sample of in South Korean children. Sci Rep. 2019;9(1):1610. doi:10.1038/s41598-018-38369-7
24. Norhafizah S, Salina H, Goh BS. Prevalence of allergic rhinitis in children with otitis media with effusion. Eur Ann Allergy Clin Immunol. 2020;52(3):121–130. doi:10.23822/EurAnnACI.1764-1489.119
25. Hemmings O, Kwok M, McKendry R, et al. Basophil activation test: old and new applications in allergy. Curr Allergy Asthma Rep. 2018;18(12):77. doi:10.1007/s11882-018-0831-5
26. O’Sullivan JA, Bochner BS. Eosinophils and eosinophil-associated diseases: an update. J Allergy Clin Immunol. 2018;141(2):505–517. doi:10.1016/j.jaci.2017.09.022
27. Zou J, Yang Y, Fu Q, et al. Eosinophils are more strongly relevant to allergic sensitization than basophils in pediatric adenotonsillar hypertrophy. Front Pediatr. 2021;9:598063. doi:10.3389/fped.2021.598063
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.