Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 16
Analysis of Primary Tooth Extractions and Associated Factors in 3 to 5-Year-Old Children in Kabul, Afghanistan: A Retrospective Study
Authors Fayaz Y ![]() , Ahmadi SU, Miri SAS
, Ahmadi SU, Miri SAS ![]() , Mohammadi H, Wikins WM, Nikzad NA
, Mohammadi H, Wikins WM, Nikzad NA
Received 30 July 2024
Accepted for publication 5 October 2024
Published 10 October 2024 Volume 2024:16 Pages 397—404
DOI https://doi.org/10.2147/CCIDE.S480120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Yahya Fayaz,1 Shahab Uddin Ahmadi,1 Said Ahmad Sorosh Miri,2 Hussain Mohammadi,1 Wakil Muhammad Wikins,3 Naseer Ahmad Nikzad3
1Department of Stomatology, Khatam AL Nabieen University, Kabul, Afghanistan; 2Department of Prosthodontics, Khatam AL Nabieen University, Kabul, Afghanistan; 3Department of Oral & Maxillofacial Surgery, National Curative and Specialized Stomatology Hospital, Kabul, Afghanistan
Correspondence: Yahya Fayaz, Department of Stomatology, Khatam AL Nabieen University, Kabul, Afghanistan, Tel +93706281798, Email [email protected]
Background/Objective: Understanding the patterns and reasons behind the extraction of children’s primary teeth is crucial for improving oral health outcomes. This retrospective investigation aimed to discern the patterns and factors contributing to primary tooth extraction among pediatric patients aged 3 to 5 years treated at the Pediatric Surgery Department of the National Curative and Specialized Stomatology Hospital in Kabul, Afghanistan.
Materials and Methods: Between January and May 2023, we conducted an extensive review of dental records, focusing on patients aged 3 to 5 years who had undergone primary tooth extraction. Data were collected on patients’ age, gender, specif tooth extracted, and reasons for tooth extraction. Statistical analysis was performed using SPSS Statistics version 25.
Results: Among 150 subjects reviewed, 53.3% were male. Primary first molars were the most commonly extracted teeth (29.3%). Dental caries was the leading cause of extraction (50%), followed by periodontitis (31.3%) and root resorption (18.7%). Mandibular extractions (58.6%) were more frequent than maxillary extractions (41.4%). No significant differences were found based on age or tooth type. Weak correlations were observed between specific tooth extractions, age, and etiology.
Conclusion: This study reveals a higher frequency of extractions in older children, primarily due to dental caries, periodontitis, and root resorption, with a slight male predominance. While no significant differences were noted in extraction patterns based on age or tooth type, understanding these trends is essential for improving pediatric dental care.
Keywords: dental extraction, dental caries, root resorption, primary teeth, Kabul
Introduction
Tooth extraction, commonly performed due to dental caries, trauma, or periodontal disease, involves removing a tooth from its alveolar socket.1,2 While tooth extraction is sometimes necessary for orthodontic purposes,3 it is most frequently performed in children when teeth become unrestorable due to severe decay. For pediatric patients, extractions may vary in complexity, from simple procedures using local anesthesia to more complex surgeries involving bone removal.4–6 However, beyond the extraction procedure itself, understanding the factors contributing to early tooth loss in children is critical to improving oral health outcomes.
Dental caries is the leading cause of tooth extractions in children and one of the most common chronic diseases globally.7 If untreated, caries can rapidly progress from affecting the crown to the root, leading to pain, infection, and eventual tooth loss. Early childhood caries (ECC), in particular, poses a significant public health challenge, especially in developing countries where access to preventive dental care is often limited.8 Globally, ECC is a major contributor to the premature loss of primary teeth, with significant consequences for children’s oral health, nutrition, and development.8
Despite the global impact of ECC,9 data on the prevalence of dental caries and tooth extractions in Afghan children remain limited. Previous studies from regions such as Chennai10 and Nigeria,11 India12 and Turkiye13 have shown that primary molars are often the most commonly extracted teeth in children, largely due to dental caries. However, research in Afghanistan has primarily focused on permanent teeth,14–16 leaving a gap in the literature regarding dental extractions in young children.
This study specifically examines patterns and factors associated with primary tooth extractions in 3- to 5-year-old children in Kabul, Afghanistan. By investigating the prevalence of dental caries, the types of teeth most frequently extracted, and the relationship between factors such as age, gender, and tooth location (mandibular vs maxillary), this research aims to provide new insights into pediatric oral health in Afghanistan.
In addition to filling a significant gap in the literature, this study holds important clinical relevance. Identifying the key reasons for tooth extraction in young children will aid in the development of targeted public health interventions aimed at reducing the burden of early childhood caries. The findings will also highlight the need for greater access to preventive care in Afghanistan and underscore the importance of early dental check-ups to prevent extensive decay and tooth loss.
This study is among the first of its kind to investigate primary tooth extractions in Kabul, and its results are expected to inform both clinical practices and public health policies aimed at improving pediatric dental care in the region.
Materials and Methods
This retrospective study was conducted at the National Curative and Specialized Stomatology Hospital in Kabul, Afghanistan, selected for its strategic location and capacity to enroll a significant number of patients. Additionally, the hospital serves patients from various provinces across Afghanistan, often providing dental treatment services free of charge.
Study Period
This retrospective study included all pediatric patients who underwent primary tooth extraction between January 2023 and May 2023 at the Pediatric Surgery Department of the National Curative and Specialized Stomatology Hospital in Kabul, Afghanistan.
Inclusion criteria included: a) Pediatric patients aged 3 to 5 years who underwent primary tooth extraction during the specified study period. b) Complete records, including patient demographics, tooth type, and reason for extraction.
Exclusion criteria included: a) Cases with incomplete or missing essential registration data (eg, missing age, sex, or extraction details). A total of 5 patients were excluded from the study due to incomplete registration data.
Diagnosis and Reasons for Extraction
The reason for tooth extraction was determined based on the diagnosis documented by the dentist in the patient records. There was no access to X-rays, as they are not preserved within the National Curative and Specialized Stomatology Hospital, and remain with the patients. As a result, the documented diagnosis by the dentist was utilized as the primary basis for classifying the reasons for extraction.
Data Collection and Analysis
Comprehensive data were collected for each patient, including age, sex, type of tooth extracted (eg, primary molars, incisors), tooth location (mandibular vs maxillary), and the reason for extraction, which was determined based on the diagnosis documented by the dentist.
The data were analyzed using SPSS Statistics software version 25. Pearson’s contingency coefficient was utilized to examine associations between variables, such as the type of tooth extracted, location (facial side), age, and etiology of extraction. A frequency distribution analysis was performed, and the chi-square test was used to assess significance, with a p-value of <0.05 considered statistically significant.
Ethical Approval
Ethical approval for the study protocol was obtained from the Research Ethics Committee of Khatam-Al-Nabieen University (AF, knu.edu.af.rec 03, 15-Dec-2022), ensuring adherence to the principles outlined in the Helsinki Declaration (1964 and its subsequent revisions). Given the retrospective nature of the study, a waiver of informed consent was granted by the ethics committee, as the study involved minimal risk to participants and utilized anonymized data. All data were handled in accordance with ethical guidelines to ensure confidentiality and privacy.
Results
A tooth may be indicated for extraction due to various reasons, including dental caries rendering it unrestorable, trauma to the tooth, or periodontal disorder. This study analyzes the prevalence of primary tooth extraction in children aged 3 to 5 undergoing treatment under local anesthesia at a governmental hospital.
In our research, we retrospectively reviewed the records of 150 children who underwent primary tooth extraction procedures at the National Curative and Specialized Stomatology Hospital. Of these, 80 out of 150 (53.3%) were male, and the children’s ages ranged from 3 to 5 years.
The frequency of primary tooth extraction was higher in males (53.3%, 80 out of 150) compared to females (46.7%, 70 out of 150), although no statistical difference was observed (χ2 = 1.061, P > 0.05). When considering the distribution of extracted teeth across age groups, extractions were most common among children aged 5 years, while they were least common among 3-year-old children (46% and 21% respectively) (Table 1).
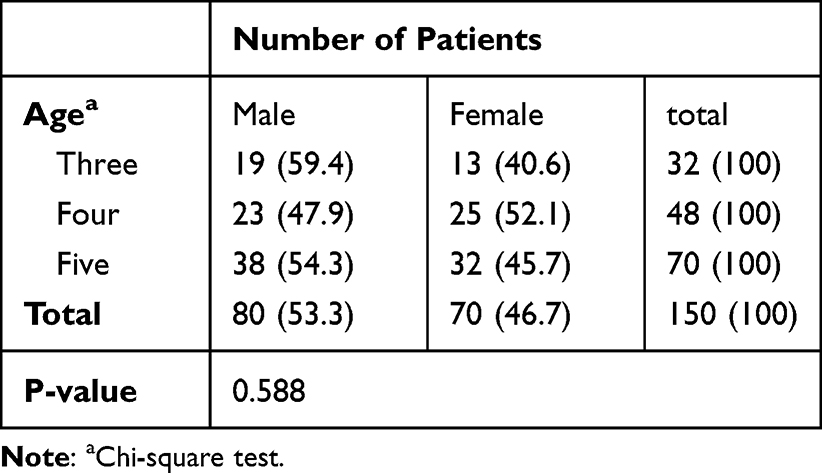 |
Table 1 Distribution of Children by Age and Gender, n (%) |
The primary first molar was the most frequently extracted tooth (29.3%, 44 out of 150), followed by the central and lateral incisors, each accounting for 24% (36 out of 150) of extractions. The canine represented the least frequently extracted primary tooth, accounting for only 2% of extractions (3 out of 150). Additionally, differences were noted in the extraction patterns among age groups and types of teeth. Among 3-year-old children, the lateral incisor (37.5%, 12 out of 32) was the most commonly extracted primary tooth, while the primary first molar (35.4%, 17 out of 48) was predominant among 4-year-olds, and molars (54.2%, 38 out of 70) were frequently extracted among 5-year-olds. There were no significant differences found between the type of tooth extracted and the age groups (χ2 = 9.898, P > 0.05) (Table 2).
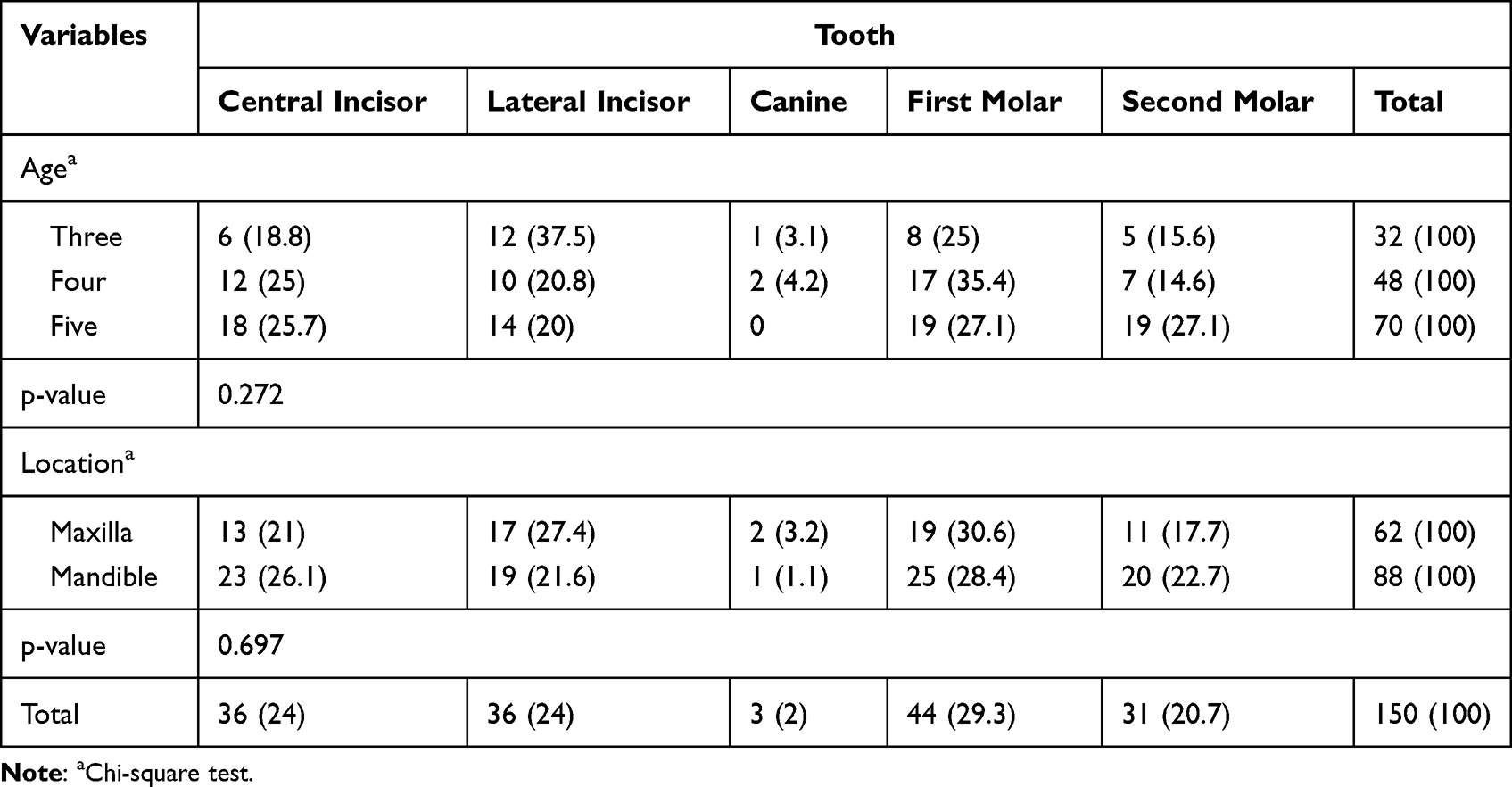 |
Table 2 Distribution of Extracted Primary Teeth Categorized by Tooth Type, Age, and Location, n (%) |
Regarding the jaw type, the extraction of mandibular teeth (58.7%, 88 out of 150) was more prevalent compared to the extraction of maxillary teeth (41.3%, 62 out of 150). The first molar was the most commonly extracted tooth in both the maxilla and mandible, accounting for 30.6% (19 out of 62) and 28.4% (25 out of 88) of extractions, respectively. The analysis of extracted primary teeth patterns in both jaws of dentition in relation to tooth type showed no significant difference (χ2 = 2.213, P > 0.05) (Table 2).
This study also identified the reasons for the extraction of primary teeth across various age groups, sex and location of extracted tooth. In a thorough analysis of reasons for primary tooth extractions, caries and its sequelae were identified as the primary cause (50%, 75 out of 150), followed by periodontitis (31.3%, 47 out of 150; potentially indicating periapical periodontitis, given the age group), and root resorption (18.7%, 28 out of 150). The diagnoses of periodontitis and root resorption were based on documented data from the patients’ records, which may have included both clinical evaluations and radiographic assessments. Significant differences were noted between the reason for tooth extraction and the location of the extracted tooth (χ2 = 7.508, P < 0.05) (Table 3).
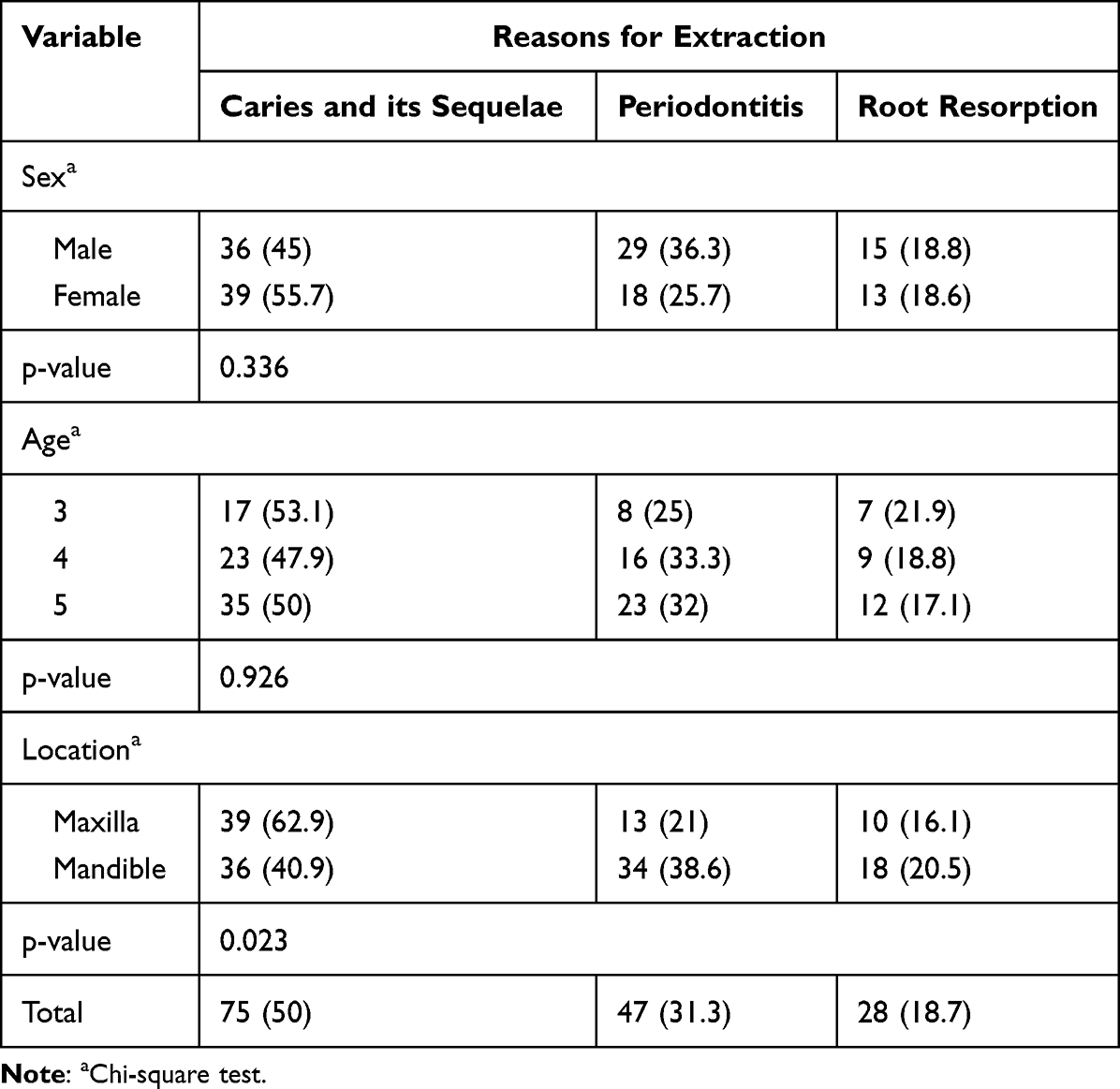 |
Table 3 Distribution of Extracted Primary Teeth Categorized by Reason, Sex, Age, and Location, n (%) |
The correlation between the specific type of tooth and the location of the extracted tooth, facial sides, age, and etiology of extractions was analyzed (Table 4). The results revealed a weak but significant correlation between lateral incisor extraction and age 3 years (r = −0.165, P = 0.044), lateral incisor extraction and periodontitis (r = −0.178, P = 0.030), as well as canine extraction and root resorption (r = 0.175, P = 0.031).
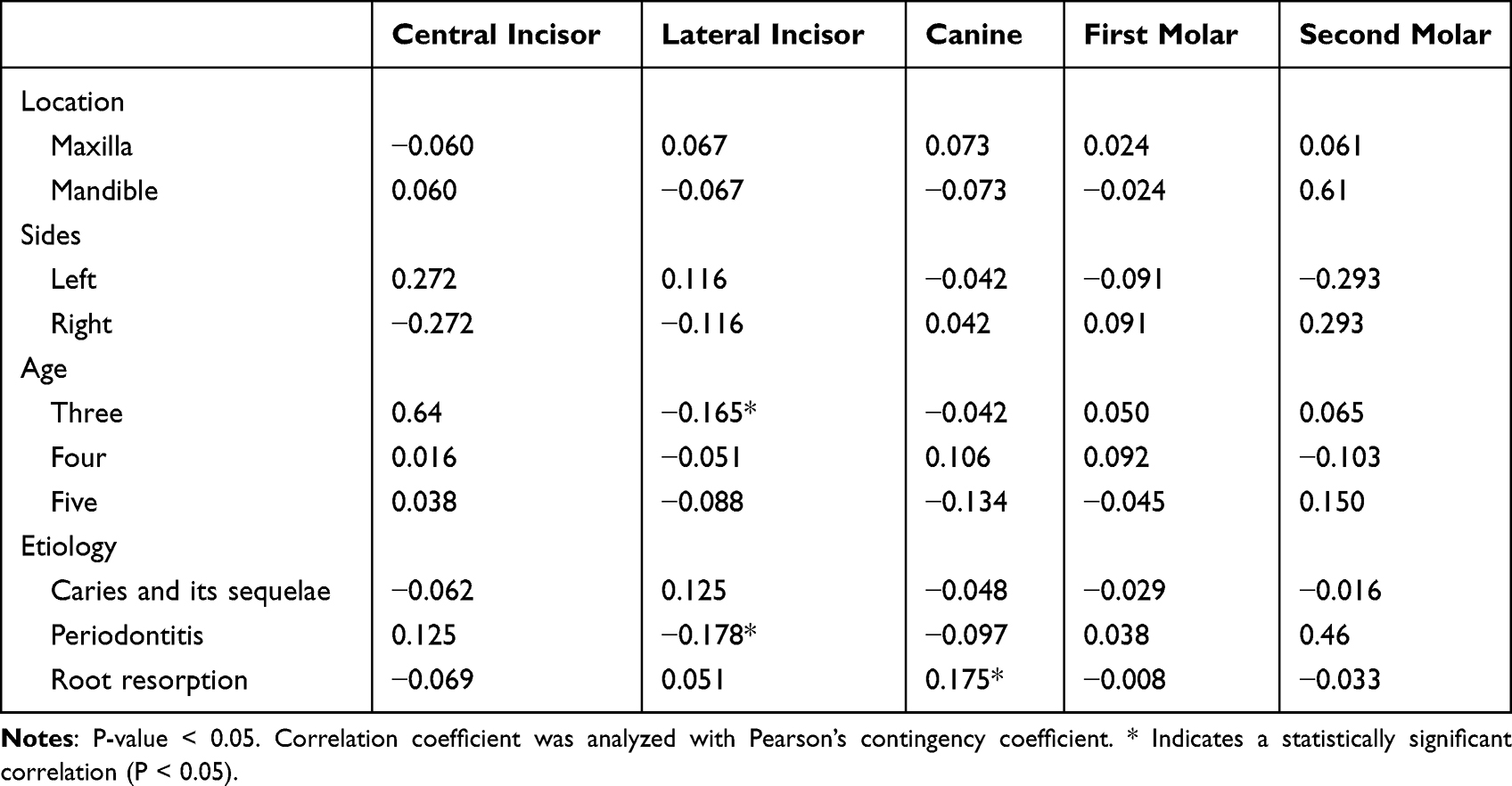 |
Table 4 Pearson’s Correlation Analysis of Extracted Deciduous Teeth Characteristics by Location, Sides, Age, and Etiology |
Discussion
This research focused on analyzing the dental records of preschool-aged children, aged 3 to 5 years, who had received primary tooth extraction while under local anesthesia between January and March 2023. The primary goal was to investigate the patterns of extractions in this age group and uncover the reasons behind these procedures. This understanding is vital for dental professionals as it helps improve services and enhance oral health outcomes within the community. Notably, there is a lack of studies on primary tooth extraction patterns among Afghan children.
In our study, primary tooth extractions were slightly more common in males (53.3%) than females (46.7%), though the difference was not statistically significant. This finding is consistent with previous studies, such as those by Taşsöker et al,17 Ashiwaju et al18 which also reported a male predominance in tooth extractions. Although there was a slight male predominance, no statistically significant gender differences were observed in the types of teeth extracted. Both males and females exhibited a similar pattern of first molar and incisor extractions. However, further research could investigate subtle differences in tooth extraction patterns by gender, as seen in other countries17,19,20 where oral hygiene habits and dietary factors sometimes show gender-based disparities.
The primary first molar was the most frequently extracted tooth (29.3%), a pattern observed in studies by Ashiwaju et al18 and Jayachandar et al21 which indicate that molars are often more susceptible to caries due to early eruption and prolonged exposure to cariogenic factors. Additionally, we found mandibular extractions (58.6%) to be more prevalent than maxillary extractions (41.4%), aligning with the findings of Jayachandar et al21 and Murshid et al,22 who attributed this to anatomical differences and the higher risk of caries in mandibular teeth.
The primary reasons for extracting primary teeth across all age groups were dental caries and its consequences, alongside periodontal disease. This trend is attributed to behavioral challenges, as many children tend to be uncooperative during dental procedures. The rapid progression of dental caries can lead to pulp involvement and periapical lesions, underscoring the urgency of extractions. Our findings align with studies conducted in countries with varying socioeconomic and healthcare systems, such as Iraq,23,24 Nigeria,25 Egypt,26 Mexico,27 Jordan,28 Turkey29 that have reported similar patterns of primary tooth extraction, with dental caries being the primary reason. Socioeconomic factors and healthcare access likely influence tooth extraction patterns in different countries. In countries like Iraq and Nigeria, where access to dental care may be limited, delayed treatment often results in higher rates of extractions due to advanced decay. Understanding how cultural attitudes toward dental care and socioeconomic status influence tooth extraction trends globally can help tailor public health interventions aimed at reducing childhood caries and extractions.
In cases of severe early childhood caries among children under six, extraction may be preferred over restoration, especially when parents are aware of the poor prognosis for badly decayed teeth. This decision is influenced by the understanding that these primary teeth will eventually be replaced by permanent adult teeth, consistent with findings from other studies.30,31 Delayed visits for routine checkups may contribute to the high prevalence of caries, highlighting the importance of early dental examinations and enhancing parental awareness.
Root resorption was noted as a contributing factor to tooth extraction, though it was less common compared to caries and periodontal disease. Nutritional deficiencies, particularly in calcium, vitamin D, and vitamin C, have been consistently linked to poor tooth development and increased susceptibility to dental caries globally. Studies have shown that malnutrition exacerbates dental caries, leading to early tooth extractions.32,33 Additionally, poor nutrition in early childhood can weaken the immune system, increasing susceptibility to infections and periodontal diseases. Understanding the interplay between tooth development, oral health, and nutrition in this age group is crucial for developing effective preventive strategies.34 Further research into specific nutritional influences on dental health in young children is necessary to fully understand these associations.
In addition to the prevalence of primary first molar extractions, distinct patterns were observed across different age groups. In 3-year-old children, lateral incisor extractions were most common (37.5%), while first molar extractions predominated in 4-year-olds (35.4%). Among 5-year-olds, molars represented the majority of extractions (54.2%). These trends align with the timing of tooth eruption and suggest that younger children may experience more extractions of incisors, likely due to their earlier eruption and prolonged exposure to cariogenic environments. Similar patterns have been observed in other countries,17,23 where younger children tend to lose anterior teeth, while older children lose posterior teeth, highlighting developmental differences in susceptibility to caries.
Our findings indicate that primary first molars (29.3%) were the most frequently extracted teeth. This is consistent with studies from other regions, including Iraq24 and Turkey,29 and India30 which have reported similar patterns in the prevalence of primary first molar extractions. The loss of primary first molars at an early age may influence the normal development of occlusion and increase the need for future orthodontic treatment.35
To further explore these trends, we utilized Pearson’s contingency coefficient to examine the correlation between the specific tooth (central incisor, lateral incisor, canine, first molar, second molar) and the extraction site (maxilla, mandible), facial sides (left, right), age (three, four, five), and the cause of extraction (caries and its consequences, periodontitis, root resorption) (Table 4). Our findings revealed a correlation between the presence of periodontitis and extraction of the lateral incisor, as well as between root resorption and extraction of the canine. The susceptibility of lateral incisor and canine teeth to periodontal issues or root resorption may be influenced by nutritional factors. Deficiencies in essential nutrients like calcium, vitamin D, and vitamin C can impact tooth development and enamel formation, increasing the risk of dental conditions.
Furthermore, poor nutrition in early childhood can weaken the immune system and oral defenses, heightening susceptibility to infections and periodontal diseases. Alongside developmental and early dental history factors, nutritional status is crucial in determining vulnerability to periodontitis or root resorption in primary teeth. Understanding the interplay between tooth development, oral health, and nutrition in this age group is vital for effective preventive strategies.30 Further research into specific nutritional influences on dental health in young children is necessary to fully grasp these associations.
Despite offering valuable insights, this study is constrained by several limitations. Its single-center design raises concerns about the generalizability of the findings. Although correlations between specific teeth and extraction reasons were established, the study did not delve into underlying mechanisms or consider potential confounding factors, such as socioeconomic status or nutritional influences on dental health outcomes. Additionally, medical histories and previous tooth extractions were not consistently recorded in the hospital’s records, limiting our ability to assess the influence of underlying conditions on dental health.
Furthermore, due to time constraints in accessing additional documentation, we were unable to expand the study’s timeline. It is important to note that the diagnoses of periodontitis and root resorption were based on documented data from the patients’ records, which may have included both clinical evaluations and radiographic assessments conducted by the treating dentists. However, the limited access to x-ray imaging for confirmation of these diagnoses remains a significant constraint in our analysis.
Importantly, this study is among the first of its kind to investigate primary tooth extractions in Kabul, and its results are expected to inform both clinical practices and public health policies aimed at improving pediatric dental care in the region. Future research should aim to include multi-center designs to enhance generalizability, incorporate detailed medical histories, and extend the study timeline to better understand the broader factors influencing dental health outcomes in preschool-aged children.
Conclusion
This study reveals a slightly higher frequency of primary tooth extractions among males (53.3%) and a trend of increasing extractions with age, particularly in 5-year-olds. The primary first molars were the most commonly extracted teeth, accounting for 29.3% of extractions, primarily due to dental caries (50%), followed by periodontitis (31.3%) and root resorption (18.7%).
These results underscore the urgent need for preventive measures targeting dental caries, especially given its significant role in pediatric extractions. Although no significant differences were found based on age or tooth type, the weak correlations between specific teeth and extraction reasons highlight the complex interplay of factors influencing dental health.
This study contributes to understanding primary tooth extraction patterns in Afghanistan, providing a basis for improving pediatric dental care. Future research should incorporate multi-center designs and explore socioeconomic and nutritional influences on dental health to better inform public health interventions.
Data Sharing Statement
Data are available from the corresponding author upon request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. van Waes H. Tooth extraction. Manag Dental Emerg Children Adolescents. 2019;159–162.
2. Hughes C, Alsheneifi T. Reasons for dental extractions in children. Pediatr Dent. 2001;23(2):109–112.
3. Suljkanovic N, Balic D, Begic N, Begic N. Supernumerary and supplementary teeth in a non-syndromic patients. Med Archives. 2021;75(1):78. doi:10.5455/medarh.2021.75.-78-81
4. Coulter W, Coffey A, Saunders I, Emmerson A. Bacteremia in children following dental extraction. J Dental Res. 1990;69(10):1691–1695. doi:10.1177/00220345900690101201
5. Dörfer CE, Staehle HJ, Wolff D. Three-year randomized study of manual and power toothbrush effects on pre-existing gingival recession. J Clin Periodontol. 2016;43(6):512–519. doi:10.1111/jcpe.12518
6. Johnson R, Baldwin DC. Relationship of maternal anxiety to the behavior of young children undergoing dental extraction. J Dental Res. 1968;47(5):801–805. doi:10.1177/00220345680470052201
7. Bernabe E, Marcenes W, Hernandez C, Bailey J, Abreu L, Arora A. GBD 2017 oral disorders collaborators. global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: a systematic analysis for the global burden of disease 2017 study. J Dent Res. 2020;99(4):362–373. doi:10.1177/0022034520908533
8. Abdelrahman M, Hsu KL, Melo MA, Dhar V, Tinanoff N. Mapping evidence on early childhood caries prevalence: complexity of worldwide data reporting. Int J Clin Pediatric Dent. 2021;14(1):1–7. doi:10.5005/jp-journals-10005-1882
9. Foláyan MNO, Schroth RJ, Duangthip D, et al. A scoping review on the association between early childhood caries and life on land: the sustainable development goal 15. PLoS One. 2024;19(7):e0304523. doi:10.1371/journal.pone.0304523
10. Harini B, Gurunathan D, Padmapriya S. Prevalence of class I caries in the second maxillary primary molar in 3–6-year-old children: a retrospective study. J Adv Pharmaceut Technol Res. 2022;13(Suppl 1):S190–S193. doi:10.4103/japtr.japtr_185_22
11. Olatosi O, Sote E. Causes and pattern of tooth loss in children and adolescents in a Nigerian tertiary hospital. Nig Q J Hosp Med. 2012;22(4).
12. Mukhopadhyay S, Roy P. Extraction of primary teeth in children: an observational study. J Craniomaxillofac Surg. 2015;4(1):57–61.
13. Koruyucu M, Bayram M, Bekiroglu N, Seymen F. Reasons for tooth extraction in 3-8 year-old Turkish children. Trauma. 2017;1:0–7.
14. Da’ameh DA. Reasons for permanent tooth extraction in the North of Afghanistan. J Dent. 2006;34(1):48–51. doi:10.1016/j.jdent.2005.02.009
15. Fayaz Y, Ahmadi NA, Ahmadi SU, Atiq MA. Common reasons for permanent tooth extraction and its correlation with demographical factors in Kabul, Afghanistan. Clin Cosmetic Invest Dent. 2024;Volume 16:25–31. doi:10.2147/CCIDE.S442179
16. Safari S, Mohebi MM, Nazhand NA, Mazaher N. Reasons for permanent tooth extraction in the west of Kabul. J Biosci Med. 2020;8(5):54–63. doi:10.4236/jbm.2020.85006
17. Taşsöker M, Menziletoğlu D, Baştürk F, Karabekiroğlu S, Şener S. Investigation of tooth extraction reasons in patients who applied to a dental faculty. Meandros Med Dental J. 2018;19(3):219–225. doi:10.4274/meandros.40085
18. Ashiwaju M, Folayan M, Sote E, Isikwe M. Pattern of tooth extraction in children attending tertiary health care centers in Nigeria: a prospective study. J Clin Pediatr Dent. 2011;36(1):107–110. doi:10.17796/jcpd.36.1.3616j76286616672
19. Candan M, Buldur B. Primary tooth extraction pattern among Turkish children with severe early childhood caries treated under general anesthesia. Pesquisa Brasileira em Odontopediatria e Clínica Integrada. 2020;20:e5382. doi:10.1590/pboci.2020.030
20. Mekete G, Mulualem Belay G, Kassa SF. Prevalence of primary tooth extraction and its associated factors among under-five-year-old children in Debre Tabor town, north-central Ethiopia: community-based cross-sectional study. Int J Gene Med. 2023;Volume 16:837–846. doi:10.2147/IJGM.S383048
21. Jayachandar D, Gurunathan D, Jeevanandan G. Prevalence of early loss of primary molars among children aged 5–10 years in Chennai: a cross-sectional study. J Indian Soc Pedodontics Preventive Dent. 2019;37(2):115–119. doi:10.4103/1319-2442.261340
22. Murshid SA, Al-Labani MA, Aldhorae KA, Rodis OM. Prevalence of prematurely lost primary teeth in 5–10-year-old children in Thamar city, Yemen: a cross-sectional study. J Int Soc Preventive Commun Dent. 2016;6(Suppl 2):S126–S130. doi:10.4103/2231-0762.189739
23. Al-Assadi AH. Patterns and causes of teeth extraction among children attending Baghdad dental teaching hospital. Int J Med Res Health Sci. 2018;7(5):88–95.
24. Mohammed AG. Causes of primary and permanent teeth extraction in children aged 3–12 years in Mosul city. Al-Rafidain Dental J. 2008;8(2):238–245. doi:10.33899/rden.2008.9065
25. Folayan MO, Otuyemi OD, Esan TA, Adeleke AA, Adedigba MA. Pattern of dental extraction in children in a Nigerian tertiary hospital. J Contemp Dent Pract. 2005;6(2):80–90. doi:10.5005/jcdp-6-2-80
26. Abdel Latif A, Omran A. Reasons of primary teeth extraction in Egyptian children. EDJ-Egyptian Dental J. 2002;48(2 Part II):823–828.
27. Galicia-Sosa A, Hernández-Guerrero JC, Jiménez-Farfán M, Ledesma-Montes C. Reasons for primary teeth extraction in Mexican children. Boletin Medico-Hospital Infantil De Mexico. 2003;60(2):184–188.
28. Nsour HF, Masarweh NA. Reasons for extraction of primary teeth in Jordan-a study. Pakistan Oral Dental J. 2013;33(2):336–339.
29. Bani M, Akal N, Bodur H, et al. The reasons for extractions of primary teeth in Turkish children. Eur J Paediatr Dent. 2015;16(3):187–190.
30. Bansal M, Gupta N, Gupta P, Arora V, Thakar S. Reasons for extraction in primary teeth among 5-12 years school children in Haryana, India-A cross-sectional study. J Clin Experimental Dent. 2017;9(4):e545.
31. Hussein AS, Abu-Hassan MI, Schroth RJ, Ghanim AM. Parent’s perception on the importance of their children’s first dental visit (a cross-sectional pilot study in Malaysia). J Oral Res. 2013;1(1):17–25.
32. Vieira KA, Rosa-Júnior LS, Souza MAV, Santos NB, Florêncio T, Bussadori SK. Chronic malnutrition and oral health status in children aged 1 to 5 years: an observational study. Medicine. 2020;99(18):e19595. doi:10.1097/MD.0000000000019595
33. Batista LRV, Moreira EAM, Corso ACT. Alimentação, estado nutricional e condição bucal da criança. Revista de Nutrição. 2007;20(2):191–196. Portuguese. doi:10.1590/S1415-52732007000200008
34. Harokopakis-Hajishengallis E. Physiologic root resorption in primary teeth: molecular and histological events. J Oral Sci. 2007;49(1):1–12. doi:10.2334/josnusd.49.1
35. Pedersen J, Stensgaard K, Melsen B. Prevalence of malocclusion in relation to premature loss of primary teeth. Comm Dentist Oral Epidemiol. 1978;6(4):204–209. doi:10.1111/j.1600-0528.1978.tb01151.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.