Back to Journals » Patient Preference and Adherence » Volume 20
Analysis of Medication-Related Burden and Associated Factors Among Elderly Patients with Coronary Heart Disease: A Cross-Sectional Study
Authors Zhou Z, Zheng J, Wu M, Ren J, Zhang M, Qiu H, Mo N, Chen L, Li J, Wang Q, Li Z, Yang X, Bao M
Received 14 April 2026
Accepted for publication 29 June 2026
Published 10 July 2026 Volume 2026:20 616727
DOI https://doi.org/10.2147/PPA.S616727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Zhiqing Zhou,1,2,* Jinmin Zheng,1,2,* Mengyan Wu,1,2,* Juan Ren,2,* Miao Zhang,2 Huan Qiu,1,3 Nan Mo,2 Longju Chen,2 Juan Li,2 Qin Wang,2 Zhen Li,2 Xiyao Yang,2 Manzhen Bao1– 3
1School of Nursing, Anhui Medical University, Hefei, Anhui, People’s Republic of China; 2Department of Nursing, The Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China; 3Anhui Medical University Taikang Health Industry Research Institute, Hefei, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Manzhen Bao, Department of Nursing, The Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China, Tel +86 15305609462, Email [email protected] Xiyao Yang, Department of Nursing, The Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China, Email [email protected]
Purpose: This cross-sectional study sought to examine the current level of medication-related burden (MRB) in elderly individuals with coronary heart disease (CHD) and to explore its key determinants. The findings are intended to inform strategies for optimizing medication management, mitigating MRB, and enhancing treatment adherence.
Methods: A cross-sectional survey was conducted amongst 231 elderly patients diagnosed with CHD who were admitted to the cardiology ward of tertiary hospital in Hefei from January to March 2026. Data collection was performed using three assessment tools: the Chinese version of the Living with Medicines Questionnaire-3 (C-LMQ-3), the Chinese version of the Beliefs about Medicines Questionnaire (C-BMQ), and a reliable and valid Medication Literacy Scale. Statistical procedures included descriptive statistics, univariate tests, and multiple linear regression analyses.
Results: Mean overall scores from the C-LMQ-3 and Visual Analogue Scale (VAS) both indicated moderate MRB among participants. Regression analysis indicated that medication adverse reactions, utilization of medication assistance devices, acquisition of medication-related health education, medication beliefs, and medication literacy were independent predictors of MRB (all P < 0.05).
Conclusion: MRB levels among elderly CHD patients are moderate and are associated with various modifiable factors. Medical practitioners should implement holistic approaches to reduce MRB, with particular attention to enhancing medication literacy and addressing medication beliefs, alongside minimizing adverse drug events, encouraging the use of medication support tools, and reinforcing medication education.
Keywords: coronary heart disease in older adults, medication burden, medication literacy, influencing factors
Introduction
Coronary heart disease (CHD), or coronary atherosclerotic disease, is a highly prevalent chronic illness in older adults.1 Its extended disease trajectory, coupled with the necessity of sustained pharmacological therapy,2,3 makes CHD a significant public health concern that undermines the health status and quality of life of aging populations.4 As reported in the China Cardiovascular Health and Disease Report 2024,5 the estimated prevalence of CHD among elderly Chinese individuals is 27.8 per 1000, and this rate continues to rise with advancing age.
Pharmacotherapy is the cornerstone of secondary prevention for CHD.6 Elderly patients require long-term treatment with a variety of medications, including antiplatelet agents, lipid-lowering drugs, antihypertensives and anti-ischaemic agents.7 These complex treatment regimens and the need for long-term medication place a heavy medication-related burden (MRB) on elderly patients with CHD.8 MRB not only directly affects patients’ adherence to medication but may also lead to behaviours such as self-adjustment of doses, discontinuation of treatment and medication errors, thereby increasing the risk of adverse cardiovascular events and readmission, and further exacerbating the burden on the healthcare system and society.9–11 A recent cross-sectional study among elderly cardiovascular patients in Iran reported that polypharmacy affected 60.1% of participants and was significantly associated with lower medication knowledge, multimorbidity, and hospitalization history, highlighting the close link between complex medication regimens and adverse clinical outcomes.12 Higher medication burden not only impairs patients’ adherence but also negatively affects their health-related quality of life, making it a critical issue in the management of elderly CHD patients. Therefore, assessing the current status of patients’ medication-related behaviour and analysing its influencing factors can provide important strategies for promoting medication adherence and ensuring medication safety.
In recent years, the issue of MRB has gradually attracted attention in the field of clinical research, and studies have now been conducted in populations such as those with tuberculosis, type 2 diabetes and late-life depression.13–16 Most existing studies have used the LMQ-3 questionnaire to assess patients’ subjective MRB across dimensions such as difficulties in adherence, adverse reactions, financial burden and autonomy in medication use, and have found that income, educational attainment, type of medication and frequency of dosing are key factors associated with MRB.17 However, existing studies have primarily focused on general demographic characteristics, with little attention paid to key modifiable factors such as medication-related variables and beliefs regarding medication adherence; furthermore, there is a lack of MRB research specifically targeting elderly patients with CHD.
Accordingly, this study aimed to analyze the level of MRB and its associated factors in elderly patients with CHD, with a specific emphasis on the impacts of medication literacy and medication beliefs. In order to provide empirical support for optimizing clinical medication management, delivering personalized health guidance, and enhancing the long-term safety and efficacy of medication use in this population.
Materials and Methods
Population and Design
This study employed a cross-sectional design, and participants were enrolled through convenience sampling among elderly CHD patients admitted to four cardiology wards at the Second Affiliated Hospital of Anhui Medical University from January to March 2026. The eligibility criteria for inclusion were defined as follows: (1) Meeting the established diagnostic criteria for CHD.18 (2) Aged 60 years or older. (3) Has been prescribed and has been taking coronary heart disease-related medication (such as antiplatelet agents, statins, beta-blockers, etc) for at least three months. (4) Is alert, has no severe visual or hearing impairments, and is able to communicate normally. (5) Being fully informed of their condition and having voluntarily provided signed informed consent. (6) With stable clinical condition, and attending the cardiology department for either acute cardiac events or routine follow-up. Exclusion criteria were defined as follows: (1) History of severe cognitive impairment or mental illness, rendering the participant unable to cooperate with the questionnaire. Cognitive status was assessed using the Mini-Cog screening tool, and patients scoring ≤ 2 (out of 5) were excluded from the study.19 (2) Presence of major physical illnesses such as malignant tumours or severe liver or kidney failure, or a life expectancy of less than one year due to other conditions; Ethical approval for this research was obtained from the Medical Ethics Committee of the Second Affiliated Hospital of Anhui Medical University (Approval No. YX2025-307). All participants provided written informed consent before taking part in the survey.
The sample size was calculated based on the empirical rule for multiple regression analysis, which suggests that the minimum sample size should be 5–10 times the number of independent variables included in the model.20 Given that 18 independent variables were incorporated into the analysis, the initial minimum required sample size was estimated at 90 participants. To account for an expected 20% rate of invalid or incomplete questionnaires, the adjusted minimum sample size was set at 113 cases. A total of 244 questionnaires were distributed, and 13 were excluded due to missing data or obvious logical contradictions, resulting in a final valid sample of 231 participants.
Survey Tools
General Information Questionnaire
Compiled by the researchers, this included eight items of demographic and sociological data: gender, age, educational level, marital status, place of residence, Living conditions, average monthly household income and payment types; as well as eight items of data relating to medication for the condition, including the number of other chronic conditions, types of medication, occurrence of adverse drug reactions, whether medication has been adjusted, whether Percutaneous Coronary Intervention (PCI)or coronary artery bypass grafting (CABG)has been performed, duration of medication use, use of medication aids, and receipt of medication-related health education.
Chinese Version of the Living with Medicines Questionnaire Version 3 (C-LMQ-3)
MRB was measured with the Chinese version of the Living with Medicines Questionnaire Version 3 (C-LMQ-3), which has been culturally adapted and psychometrically validated for elderly Chinese individuals by Wang et al21 The C-LMQ-3 includes 8 subscales addressing different dimensions of MRB, consisting of 39 items in total. Each item is rated on a 5-point Likert scale, with responses from 1 (strongly disagree) to 5 (strongly agree). The C-LMQ-3 contains both positively and negatively worded items. For negatively worded items, responses were reverse‑coded prior to summation, so that higher scores consistently indicate higher MRB. A Visual Analogue Scale (VAS) from 0 (no burden) to 10 (extreme burden) was also employed to assess patients’ subjective feelings of MRB. For this scale, the Cronbach’s α was 0.855 for the total scale, with subscale α values ranging from 0.822 to 0.932. In our sample, the Cronbach’s α for the total C-LMQ-3 was 0.892, and the α values for the eight subscales ranged from 0.792 to 0.931, indicating good internal consistency.
Beliefs About Medicines Questionnaire (Chinese Version, C-BMQ)
This tool was translated and culturally adapted into Chinese by Si et al22 This instrument consists of two dimensions: beliefs concerning medication necessity and beliefs concerning medication-related concerns, each containing five items. Each item is rated on a 5-point Likert scale, ranging from “strongly disagree” to “strongly agree”, with scores assigned from 1 to 5. Elevated scores reflect stronger endorsement of the respective belief dimension. The overall score is calculated by subtracting the total score of the concerns subscale from the total score of the necessity subscale, which reflects the patient’s perceived balance between the benefits of treatment and potential risks. A C-BMQ total score > 0 indicates that the perceived necessity of pharmacotherapy outweighs associated worries, whereas a score≤ 0suggests that concerns regarding medication risks predominate over perceived clinical advantages. For this scale, The Cronbach’s α was 0.77 for the total scale, 0.92 for the necessity subscale, and 0.67 for the concerns subscale. In our study, the Cronbach’s α coefficient for the total C-BMQ was 0.893, with α values of 0.912 for the necessity subscale and 0.862 for the concerns subscale, indicating good internal consistency.
Chinese Version of Discharge Medication Literacy Questionnaire
This questionnaire was culturally adapted for use among Chinese residents by Zheng et al23 The scale evaluates patients’ capacity to comprehend, compute, and manage medication-related information, covering essential aspects such as medication name, dosage, administration frequency, therapeutic purpose, and major adverse effects. It consists of nine items in total, utilizing a binary scoring approach wherein a correct response receives 1 point and an incorrect response receives 0 points. Items 7 and 9 are excluded from scoring. The maximum attainable score is 7, with higher values reflecting superior medication literacy. The original validation study reported a Cronbach’s α of 0.85 for this questionnaire. In our sample, the KR-20 coefficient was 0.815, confirming good internal consistency. Based on the stratification employed by Jiao et al24 medication literacy scores were categorized into three levels: low (0–2 points), moderate (3–5 points), and high (6–7 points).
Data Collection and Quality Control
Data were collected via on-site questionnaire surveys, completed on the day of discharge for elderly patients with CHD. Prior to the survey, patients were informed of the study’s objectives, completion requirements and confidentiality principles. The survey was conducted only after obtaining informed consent. For patients with poor eyesight, difficulty writing or who were unable to complete the form independently, a researcher who had undergone standardised training read out each question and recorded the responses accurately; those unable to express themselves independently were excluded in accordance with the exclusion criteria. This study implemented standardised data management: following the return of questionnaires, their completeness was verified, and invalid questionnaires with more than three missing items or logical inconsistencies were excluded; Valid data were entered into EpiData 3.1 by two independent operators; the system performed automatic validation, with any inconsistencies verified and corrected by a third party; outliers and extreme values were addressed following discussion and verification against the original questionnaires; the entire process was documented to ensure data accuracy, reliability and traceability.
Statistical Analysis
SPSS version 27.0 was utilized for all data processing and statistical analyses in this study. Skewness and kurtosis tests were conducted to assess the normality of the distribution. Continuous data were considered to follow an approximately normal distribution if skewness ranged between −1 and 1 and kurtosis ranged between −2 and 2, and all variables met these criteria. To characterize the distribution patterns of variables, descriptive statistics were applied: categorical data were summarized using frequency counts and respective percentages, and continuous data were reported as mean ± standard deviation (SD). Between-group differences in the total C-LMQ-3 scores for elderly CHD patients were evaluated using independent-samples t-tests and one-way analysis of variance (ANOVA) where applicable. For variables with more than two groups, one‑way ANOVA was used, followed by Tukey’s HSD post‑hoc test for multiple pairwise comparisons. Following univariate analysis, variables with a P value less than 0.05 were entered simultaneously into a multiple linear regression model to identify factors independently associated with MRB and to adjust for potential confounding effects. Multicollinearity was assessed using variance inflation factor (VIF) and tolerance, and model assumptions (normality of residuals, homoscedasticity, and independence of residuals) were checked using residual plots and the Durbin-Watson test.
Result
Demographic and Medication-Related Characteristics
The demographic and clinical characteristics of the 231 participants included in this study are presented in Table 1. The age of the study population ranged from 60 to 84 years, with an average age of 70.31 ± 6.38 years. Male patients comprised the predominant group, representing 62.8% of the total sample, whilst those with an educational attainment of primary school or below were the largest group, accounting for 53.2%. Regarding income per month, 57.1% of patients had an average monthly income of 2000–4000 yuan. In terms of Living conditions, 58.0% of patients lived solely with their spouse, Regarding medication or treatment, 56.7% of patients had a history of PCI or CABG surgery. The largest proportion of patients (52.8%) had one comorbid chronic condition. The largest group of patients (42%) had been taking medication for 1–5 years. 28.6% of patients reported experiencing adverse drug reactions, and 30.3% had had their medication adjusted within the past year. Only 15.2% of patients used medication management tools. 48.9% of patients had received specific health education on medication. Regarding medication beliefs, 59.3% had a C-BMQ score >0, whilst 40.7% had a score ≤0; medication literacy was most commonly at a moderate level (45.0%), with 31.2% at a low level and 23.8% at a high level.
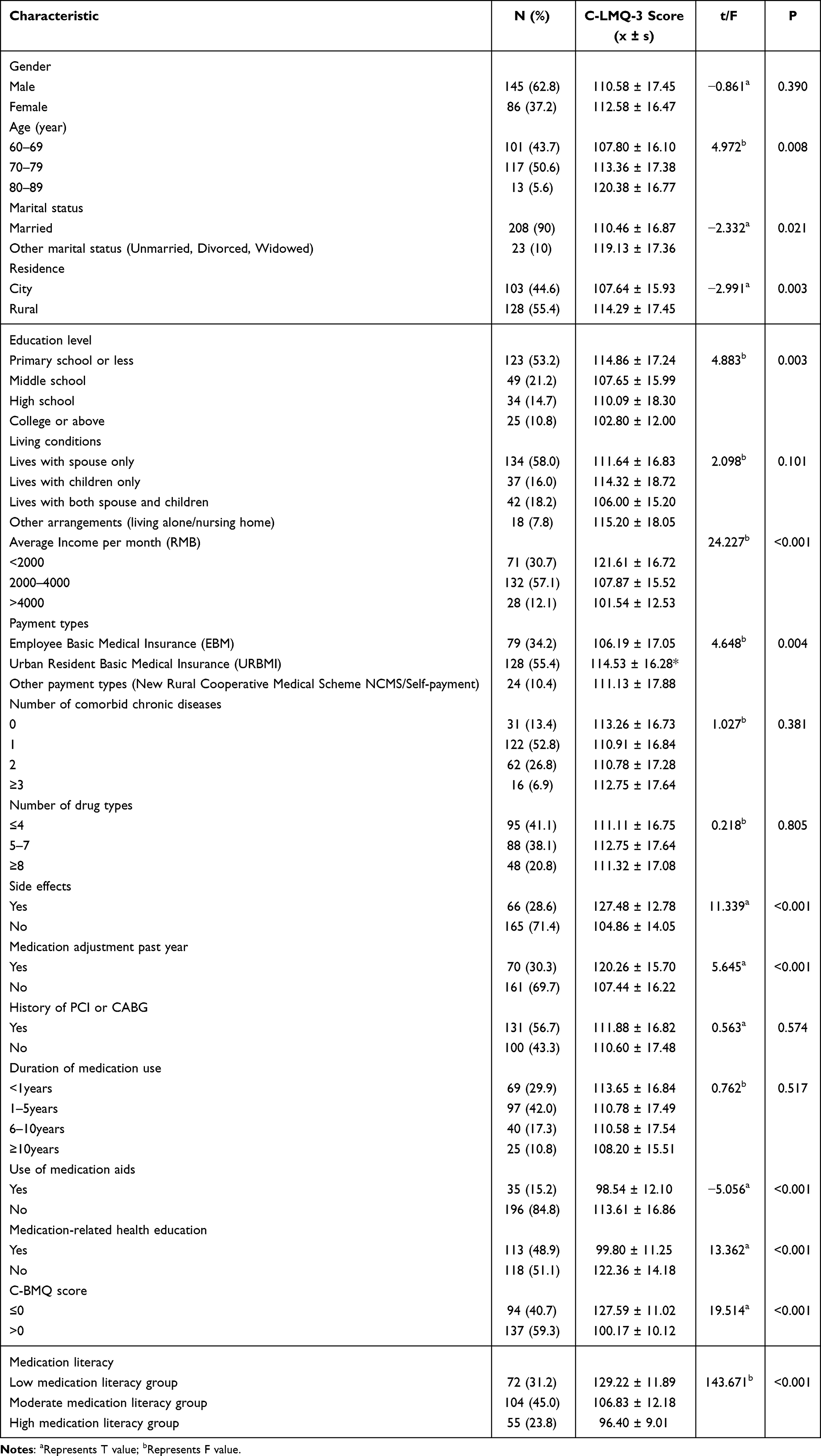 |
Table 1 Demographic Characteristics of Participants (n = 231) |
Assessing MRB Using the C-LMQ-3
Supplementary Table 1 presents the responses to the statements in the C-LMQ-3 and the scores for the eight domains. The total and dimensional scores of the C-LMQ-3 are presented in Table 2. The total C-LMQ-3 score follows an approximately normal distribution, with a mean of 111.32 (SD = 17.08) and a range of 75–153 (the maximum possible range being 39–195). VAS scores tended towards higher values, with a median (range) of 6 (0–10) and a mean of 5.58 (SD = 1.36). The top 10 items with the highest scores on the C-LMQ-3 are listed in Table 3.
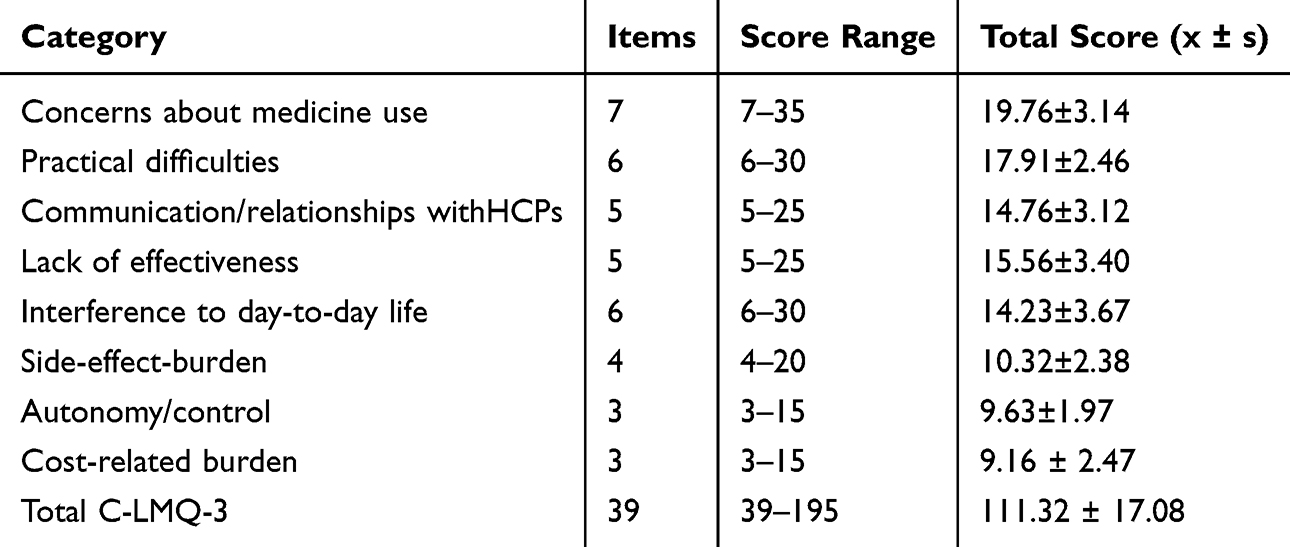 |
Table 2 Total and Dimensional Scores of the C-LMQ-3 Among Elderly Patients with CHD |
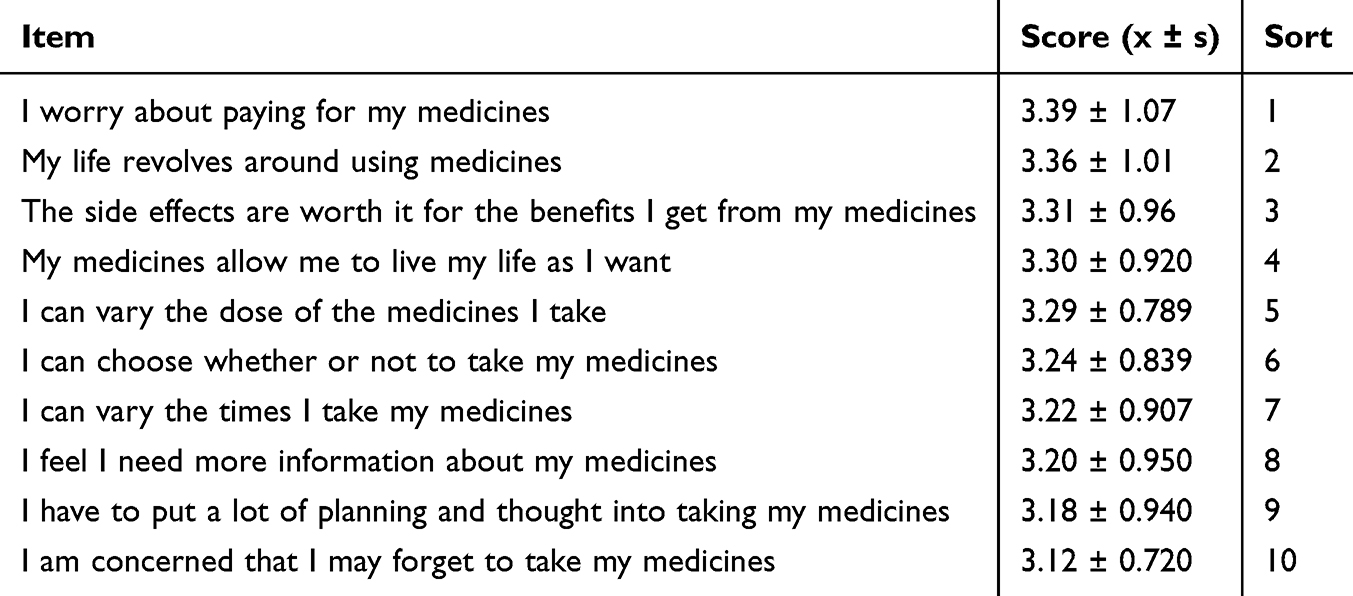 |
Table 3 The Top 10 Items with the Highest Scores in C-LMQ-3 |
Factors Influencing the MRB
Table 1 shows the results of differences in C-LMQ-3 scores between different groups of elderly CHD patients in relation to their demographic characteristics and medication-related practices. Analysis of the results revealed significant differences in the C-LMQ-3 total medication burden score across different age groups, marital status, place of residence, educational level, average monthly income, type of health insurance, medication side effects, whether medication had been adjusted in the past year, use of medication aids, receipt of medication health education, BMQ score and medication literacy (all P-values < 0.05). Post-hoc comparisons using Tukey’s HSD test showed that patients aged 60–69 years had significantly lower MRB than those aged 70–79 years (mean difference = –5.56, P = 0.041) and those aged 80–89 years (mean difference = –12.58, P = 0.031). Patients with primary school education or less had significantly higher MRB than those with college or above education (mean difference = 12.06, P = 0.006). Patients in the lowest income group (<2000 RMB) had significantly higher MRB than those in the middle (2000–4000 RMB) and highest (>4000 RMB) income groups (both P < 0.001). Patients with low medication literacy had significantly higher MRB than those with moderate or high literacy (both P < 0.001).
Taking the total C-LMQ-3 score as the dependent variable, only those variables that achieved a significance level of P<0.05 in the univariate screening were incorporated into the multiple linear regression model. The coding scheme for all independent variables included in the regression model is presented in Table 4. The results of the multiple linear regression analysis are presented in Table 5. The multiple linear regression model was significant (F = 62.230, P < 0.001) and explained 77.6% of the variance in MRB (adjusted R2 = 0.776). The Durbin-Watson statistic was 1.867, and all VIF values were below 3 (range: 1.109–2.237), indicating no multicollinearity and independence of residuals. The results showed that medication side effects, the use of medication support tools, whether medication health education was provided, medication beliefs, and medication literacy were independent factors associated with MRB in elderly CHD patients (all P < 0.05). Specifically, when compared to the reference group, patients experiencing medication side effects had a higher MRB, whereas patients using medication aids, having received medication health education, possessing stronger medication necessity beliefs, and having moderate or high levels of medication literacy had a lower MRB.
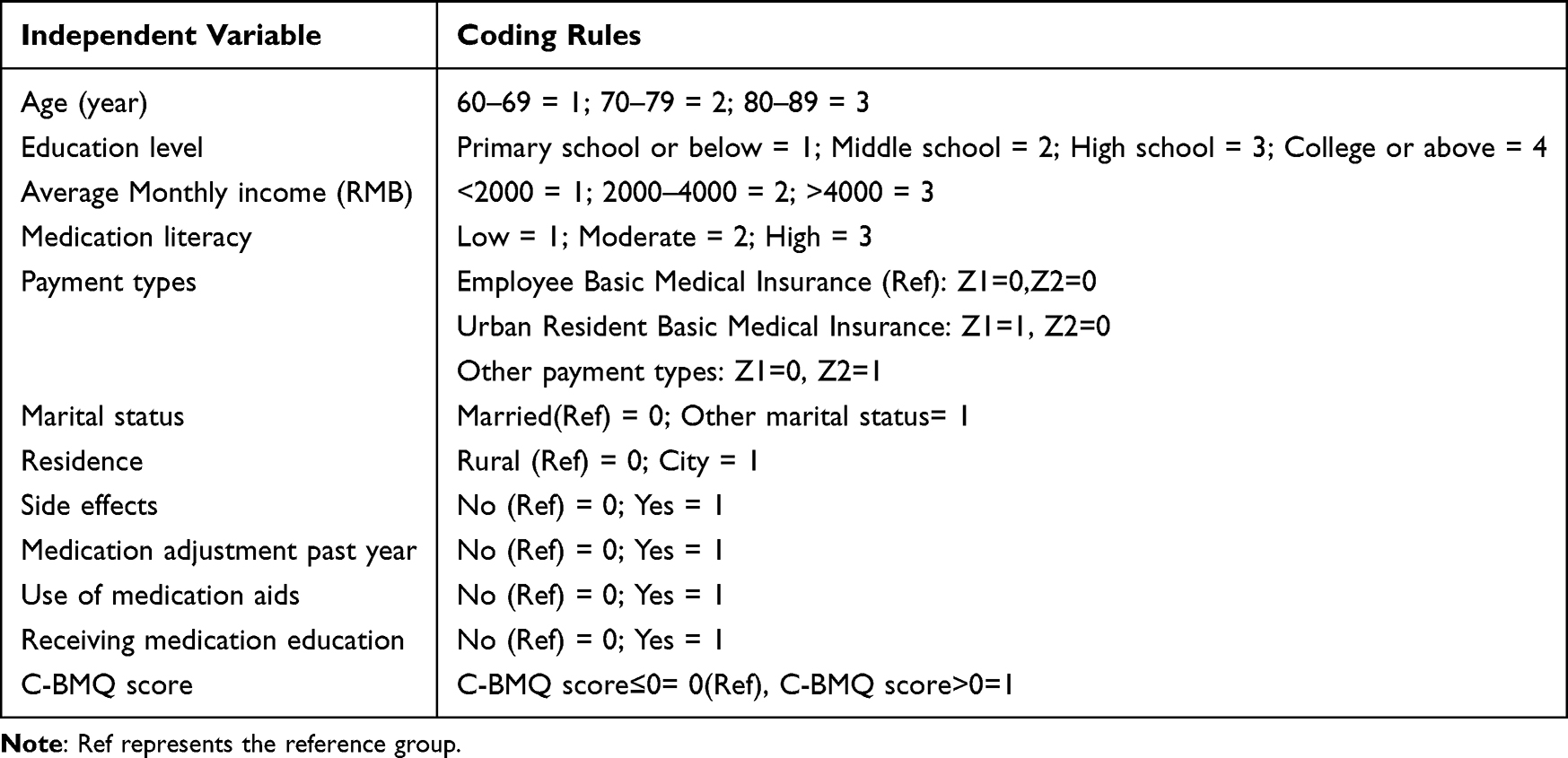 |
Table 4 Coding Scheme for Independent Variables |
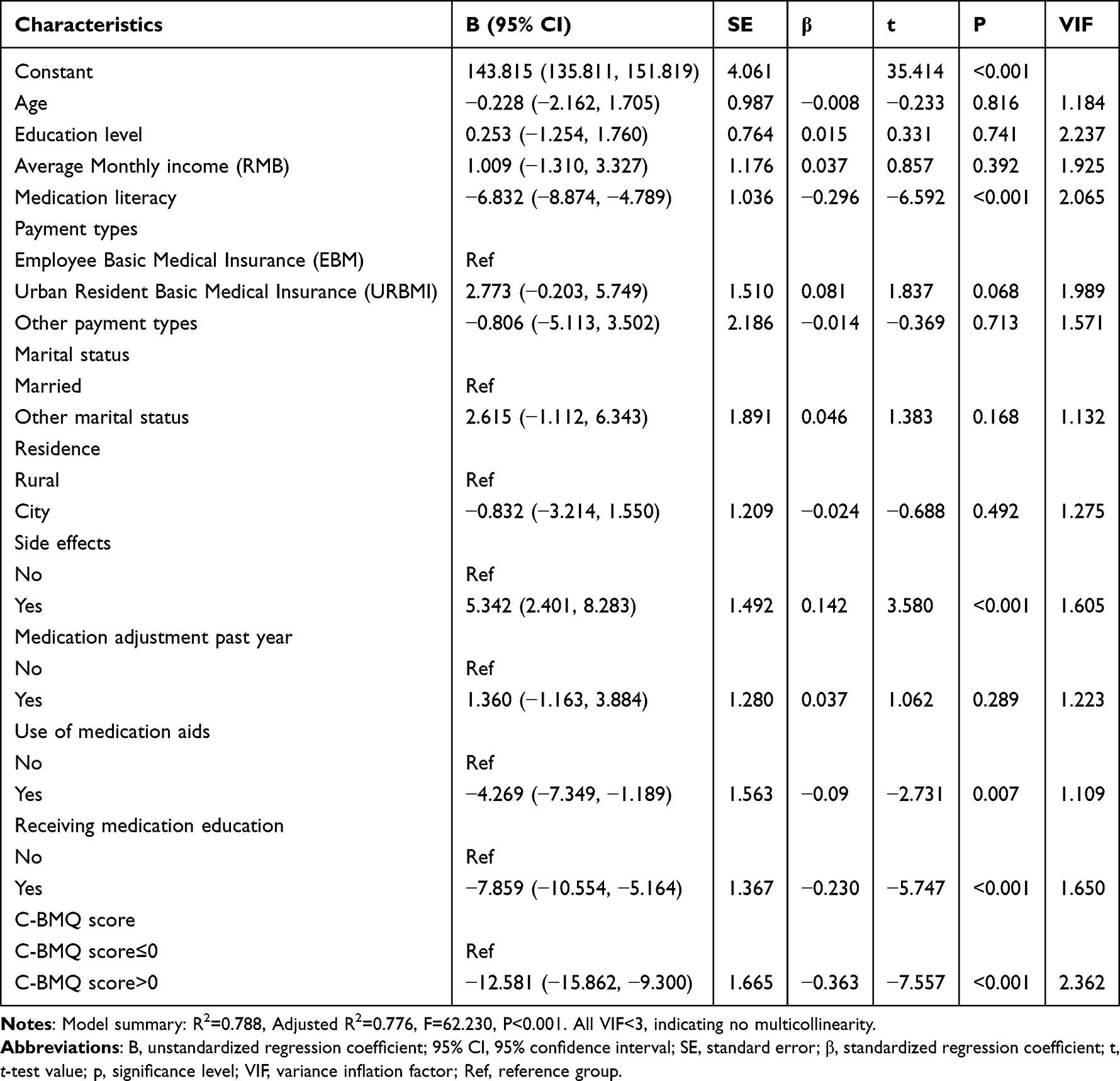 |
Table 5 Multivariable Linear Model Analysis for the Association with the MRB Among Patients with CHD (n=231) |
Discussion
In this research, the C-LMQ-3 scale was employed to evaluate the MRB of 231 elderly CHD patients. The findings revealed that the overall C-LMQ-3 score was 111.32 ± 17.08, which reflected a moderate level of medication burden in this cohort. These results were comparable to those reported in a previous Chinese study (112.9 ± 11.3)17 and elderly patients with chronic diseases in Kuwait [median 112 (interquartile range 21) in the LMQ-3],25 but were higher than those reported in New Zealand (101.8 ± 21)26 and among adults in South East England (99.7 ± 19.8).27 These differences may be related to factors such as the type of disease, age structure, regional economic development, healthcare system and cultural background of the study population. Currently, research focusing on MRB in elderly CHD patients remains relatively limited, and the outcomes of this study offer an important reference for the assessment of MRB in this group.
Analysis of the scores for each item of the C-LMQ-3 revealed that items associated with a higher MRB were primarily concentrated in the areas of financial burden, disruption to daily life caused by medication, autonomy in medication use, need for medication information, and medication-related concerns. Among these, the item “concerns about medication costs” received the highest score (3.39 ± 1.07), suggesting that the financial burden of medication is the primary source of MRB for elderly patients with CHD. This result is in line with the findings reported by Wang et al on elderly patients with chronic diseases.17 This may be linked to the limited financial resources of elderly patients and inadequate health insurance coverage.28 Consequently, health authorities and healthcare providers can alleviate patients’ out-of-pocket costs through measures such as prioritising the use of medicines listed in the National Reimbursement Drug List, implementing policies for long-term prescriptions for chronic conditions and high reimbursement rates, and providing advice on medication costs. This was followed by “Taking medication has become a major part of my life” (3.36 ± 1.01), reflecting the impact of long-term, regular medication on patients’ daily routines and their dependence on medication. Furthermore, items such as “ability to adjust dosage independently”, “ability to decide independently whether to take medication”, and “ability to adjust the timing of medication” also scored highly, indicating that patients lack autonomy in their medication regimens; This finding is in accordance with the conclusions drawn by Liu et al in their investigation of older adults with depressive disorders.16 This suggests that in clinical practice, when formulating treatment regimens, due consideration should be given to patients’ preferences, allowing them reasonable scope for self-adjustment. At the same time, items such as “need for more information about medication”, “requires considerable effort to plan medication”, and “concern about forgetting to take medication” also ranked highly, indicating that elderly patients with CHD commonly face issues such as insufficient information about their medication, difficulties in managing their medication, and concerns about forgetting to take it.
This study found that patients experiencing adverse drug reactions was associated with higher MRB, a finding that aligns closely with the results reported by Liu et al in their study of elderly patients with depression16 Approximately 28.6% of patients reported adverse drug reactions, indicating that such reactions are relatively common among elderly patients with CHD. This patient population often requires long-term treatment with antiplatelet agents, lipid-lowering drugs and antihypertensive agents. Among these, aspirin may increase the risk of bleeding and cause gastrointestinal discomfort, whilst statins may lead to abnormal liver function and muscle pain,29 these adverse reactions may be associated with a greater MRB and affect treatment adherence.30,31 It is possible that adverse reactions are related to increased fear and anxiety regarding medication, thereby undermining their confidence in treatment.32 Healthcare professionals should therefore conduct a comprehensive assessment of patients’ liver and kidney function, bleeding risk and concomitant medication prior to prescribing; select the type and dose of medication on an individual basis; inform patients of the potential adverse reactions; and strengthen the monitoring and management of adverse drug reactions, with a view to reducing the MRB on patients.
Research also indicates that patients who use medication aids such as pill boxes tend to experience milder medication-related behavioural problems. This may be because these tools help standardise medication routines, reduce missed and incorrect doses, and relieve memory pressure, thereby easing the overall medication management burden. This may also be because the use of medication aids may be associated with better medication management and lower MRB. Previous studies have found that simple medication aids can alleviate medication-related behavioural problems in patients.33,34 In this study, only 15.2% of patients used medication management aids, suggesting that the uptake of such tools in clinical practice remains low. In future clinical practice, both traditional and smart medication management aids should be promoted, taking into account the cognitive and practical abilities of elderly patients, and personalised guidance should be provided to simplify the medication process and reduce the administrative burden.
Furthermore, patients who have received medication education and possess a higher level of medication literacy tend to experience milder MRB. Proper medication education is associated with better understanding of patients’ condition and treatment plan, while higher medication literacy is associated with knowledge of medication efficacy, adverse reactions, and precautions. Both may be related to lower burdens caused by lack of information.35–37 Consequently, clinicians should prioritise and enhance medication support and interventions for elderly patients with CHD. They should provide standardised, personalised medication education during the initial consultation and follow-up appointments, and utilise digital tools to assist patients in acquiring medication knowledge, broaden their access to information, and clarify drug administration, dosages and therapeutic effects, thereby improving their medication literacy.
At the same time, this study also found that stronger medication necessity beliefs are associated with lower MRB. This is primarily because stronger medication necessity beliefs make patients more receptive to long-term medication regimens and more proactive in adhering to medication management, thereby reducing the subjective burden and management pressure caused by psychological resistance, cognitive biases and excessive anxiety.38,39 A meta-analysis found40 that the stronger a patient’s positive belief in the necessity of drug treatment and the fewer their concerns about taking medication, the higher their long-term adherence to the treatment. Clinical healthcare professionals should therefore provide more positive guidance to help patients form a positive attitude towards medication. By thoroughly discussing the benefits of treatment with patients and promptly clarifying misconceptions about medication, they can help patients develop a rational and positive understanding of medication, thereby reducing unnecessary concerns and resistance, and consequently alleviating the psychological and management burdens associated with medication.
The present study investigated the level of MRB and its associated factors among older patients with CHD. Amid the global population ageing trend, the prevalence of CHD in the elderly is continuously increasing, and long-term polypharmacy has become a common clinical practice. Nevertheless, systematic studies focusing on MRB in this specific patient group are still relatively limited. Through evaluating patients’ MRB and its influencing factors, this study enhances our in-depth understanding of the real-world experiences and challenges encountered by elderly CHD patients during long-term pharmacotherapy, and provides a reference for clinical healthcare professionals and health policymakers. Against the backdrop of China’s accelerating population ageing, addressing and improving MRB among elderly patients with CHD is of great significance for optimising medication management, enhancing treatment adherence and improving patient health outcomes.
Based on our findings, clinicians should consider routine MRB assessment, personalized medication education, promotion of medication aids, active monitoring of adverse drug reactions, and enhancement of medication literacy to reduce MRB in elderly CHD patients. However, these suggestions are based on associational findings and require further validation in future interventional studies. Given the cross-sectional design, we cannot fully exclude the possibility of confounding by these or other unmeasured variables.
The current study possesses certain inherent limitations. To elaborate, the cross-sectional research design precludes the establishment of causal relationships among the investigated variables. Despite adjusting for all variables that reached statistical significance in univariate analysis, we cannot exclude the possibility of residual confounding by unmeasured factors, such as social support, disease severity, cognitive function, or health literacy. Secondly, the study sample was drawn from a relatively concentrated source and the sample size was limited, which may limit the external validity of the findings, making it difficult to apply them to populations of elderly CHD patients in different geographical areas or with varying levels of healthcare resources. Additionally, the evaluation of MRB and its associated determinants was based exclusively on patient self-reporting, which is potentially prone to recall bias or subjective reporting biases. Fourth, data were collected on the day of discharge, when patients may experience stress that could affect self-reported MRB. Future studies could enhance the representativeness of the findings by increasing the sample size and conducting multicentre studies, thereby providing a more reliable basis for optimising intervention strategies for MRB in elderly patients with CHD.
Conclusion
In this study, the MRB among elderly patients with CHD was found to be moderate, primarily reflected in dimensions such as financial burden and disruption to daily life. The MRB experienced by elderly patients with CHD is associated with a range of different factors, including drug side effects, the use of medication support tools, medication health education, medication beliefs and medication literacy. Notably, our findings highlight the novel and clinically relevant roles of medication beliefs and medication literacy as key modifiable factors associated with MRB in elderly CHD patients. Healthcare professionals should consider implementing targeted, standardised medication education to enhance patients’ medication knowledge and self-management skills, whilst providing positive guidance on medication beliefs to alleviate unnecessary concerns. Furthermore, strategies such as promoting the use of medication aids, reducing the incidence of adverse drug reactions, and optimising individualised medication regimens can further alleviate patients’ MRB.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by Second Affiliated Hospital of Anhui Medical University (Approval No. YX2025-307). Written informed consent was obtained.
Acknowledgments
We would like to thank all the faculty members in the Nursing Department of the Cardiovascular Medicine Division at the Second Affiliated Hospital of Anhui Medical University for their support of our work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Anhui Medical University School Clinical Science Fund Project [grant number 2020xkj197]; Nursing Project of Anhui Institute of Translational Medicine [grant number 2025zhyx-hl-A20]; 2026 Anhui Medical University School of Nursing Postgraduate Youth Training Project [grant number Hlqm22025101].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wu N, Xie X, Cai M, Han Y, Wu S. Trends in health service needs, utilization, and non-communicable chronic diseases burden of older adults in China: evidence from the 1993 to 2018 National Health Service Survey. Int J Equity Health. 2023;22(1):169. doi:10.1186/s12939-023-01983-7
2. Yang L, Xing Y, Gao X, Guo C, Wu D. Burden of ageing spectrum of diseases in China, 1990-2021: a systematic analysis of global burden of disease study 2021. Front Public Health. 2025;13:1611901. doi:10.3389/fpubh.2025.1611901
3. Fadah K, Hechanova A, Mukherjee D. Epidemiology, pathophysiology, and management of coronary artery disease in the elderly. Int J Angiol. 2022;31(4):244–12. doi:10.1055/s-0042-1751234
4. Xu S, Liu Z, Tang M, Xu C. Burden, risk factors, and projections of ischemic heart disease in China (1990-2021): findings from the 2021 GBD study. Front Cardiovasc Med. 2025;12:1549147. doi:10.3389/fcvm.2025.1549147
5. National Center for Cardiovascular Diseases C. Annual report on cardiovascular health and diseases in China 2024. Peking Union Medical College Press; 2025.
6. Ma TT, Wong ICK, Man KKC, et al. Effect of evidence-based therapy for secondary prevention of cardiovascular disease: systematic review and meta-analysis. PLoS One. 2019;14(1):e0210988. doi:10.1371/journal.pone.0210988
7. Dornbrook-Lavender KA, Roth MT, Pieper JA. Secondary prevention of coronary heart disease in the elderly. Ann Pharmacother. 2003;37(12):1867–1876. doi:10.1345/aph.1D026
8. van der Laan DM, Elders PJM, Boons C, Nijpels G, Krska J, Hugtenburg JG. The impact of cardiovascular medication use on patients’ daily lives: a cross-sectional study. Int J Clin Pharm. 2018;40(2):412–420. doi:10.1007/s11096-018-0601-4
9. Schreiner N, DiGennaro S, Harwell C, Burant C, Daly B, Douglas S. Treatment burden as a predictor of self-management adherence within the primary care population. Appl Nurs Res. 2020;54:151301. doi:10.1016/j.apnr.2020.151301
10. Dagnew SB, Moges TA, Tarekegn GY, et al. Treatment burden and medication adherence among older patients in comprehensive specialised hospitals in the Amhara Region in Ethiopia: a multicentre, cross-sectional study. BMJ Open. 2025;15(6):e095666. doi:10.1136/bmjopen-2024-095666
11. Baah-Nyarkoh E, Alhassan Y, Dwomoh AK, Kretchy IA. Medicated-related burden and adherence in patients with co-morbid type 2 diabetes mellitus and hypertension. Heliyon. 2023;9(4):e15448. doi:10.1016/j.heliyon.2023.e15448
12. Faramarzi Nasab N, Rezaeian S, Ezadi S, Khatony A. Prevalence and determinants of polypharmacy: a cross-sectional study among elderly patients with cardiovascular diseases in outpatient clinics. Scientifica. 2025;2025:6641747. doi:10.1155/sci5/6641747
13. Wang Y, Jian S, Huang Z, Chen H, Hu Y, Fang S. Medication-related burden and its association with medication adherence among elderly tuberculosis patients in Guizhou, China: a cross-sectional study. Front Pharmacol. 2024;15:1416005. doi:10.3389/fphar.2024.1416005
14. Le MH, Le ND, Le TTN, Nguyen MC, Tran V. Psychosocial factors associated with medication burden among patients with type 2 diabetes mellitus: a cross-sectional study. J Diabetes Res. 2025;2025:8885209. doi:10.1155/jdr/8885209
15. Li Y, Yu Q, Yao R, et al. Latent profile analysis and influencing factors of medication-related burden in multidrug-resistant tuberculosis patients in Chengdu, China. Patient Prefer Adherence. 2025;19:3387–3397. doi:10.2147/ppa.S558068
16. Liu D, Qiu L, Han L, et al. Prevalence and influencing factors of medication-related burden among patients with late-life depression in typical city of eastern China: a cross-sectional study. BMC Public Health. 2024;24(1):3521. doi:10.1186/s12889-024-20939-2
17. Wang Y, Li X, Jia D, et al. Exploring polypharmacy burden among elderly patients with chronic diseases in Chinese community: a cross-sectional study. BMC Geriatr. 2021;21(1):308. doi:10.1186/s12877-021-02247-1
18. Chinese guidelines for the diagnosis and management of patients with chronic coronary syndrome. Zhonghua Xin Xue Guan Bing Za Zhi. 2024;52(6):589–614. doi:10.3760/cma.j.cn112148-20240325-00168
19. Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The mini-cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry. 2000;15(11):1021–1027. doi:10.1002/1099-1166(200011)15:11<1021::aid-gps234>3.0.co;2-6
20. Norman G, Monteiro S, Salama S. Sample size calculations: should the emperor’s clothes be off the peg or made to measure? BMJ. 2012;345:e5278. doi:10.1136/bmj.e5278
21. Wang Y, Krska J, Lin B, et al. Cross-cultural adaptation and reliability testing of Chinese version of the living with medicines questionnaire in elderly patients with chronic diseases. Patient Prefer Adherence. 2020;14:2477–2487. doi:10.2147/ppa.S275006
22. Si ZZ, Min, Cao GQ. Reliability and validity of the Chinese version of Beliefs about Medicines Questionnaire-Specific among patients on warfarin therapy after mechanical heart-valve replacement. J Nurs Sci. 2013;28(4):20–23.
23. Zheng FD, Siqing, Zhong Z, Pan C, Xie J, Qin C. Investigation on status quo of discharged patients’ medication literacy after coronary artery stent implantation. Chin Nurs res. 2015;29(5B):1732–1734. doi:10.3969/j.issn.1009-6493.2015.14.024
24. Jiao AH, Xianna, He D, Chen Y. Investigation on medication literacy in patients with coronary heart disease after PCI and analysis of influencing factors. Clin Med. 2023;43(11):25–36. doi:10.19528/j.issn.1003-3548.2023.11.018
25. Awad A, Alhadab A, Albassam A. Medication-related burden and medication adherence among geriatric patients in Kuwait: a cross-sectional study. Front Pharmacol. 2020;11:1296. doi:10.3389/fphar.2020.01296
26. Tordoff JM, Brenkley C, Krska J, Smith A. Exploring medicines burden among adults in New Zealand: a cross-sectional survey. Patient Prefer Adherence. 2019;13:2171–2184. doi:10.2147/ppa.S231202
27. Krska J, Katusiime B, Corlett SA. Patient experiences of the burden of using medicines for long-term conditions and factors affecting burden: a cross-sectional survey. Health Soc Care Community. 2018;26(6):946–959. doi:10.1111/hsc.12624
28. Ma M, Tian W, Kang J, et al. Does the medical insurance system play a real role in reducing catastrophic economic burden in elderly patients with cardiovascular disease in China? Implication for accurately targeting vulnerable characteristics. Global Health. 2021;17(1):36. doi:10.1186/s12992-021-00683-7
29. Montgomery S, Miedema MD, Dodson JA. Aspirin and statin therapy for primary prevention of cardiovascular disease in older adults. Heart. 2022;108(14):1090–1097. doi:10.1136/heartjnl-2021-320154
30. Insani WN, Wei L, Abdulah R, et al. Exploring the association of adverse drug reactions with medication adherence and quality of life among hypertensive patients: a cross-sectional study. Int J Clin Pharm. 2025;47(2):354–364. doi:10.1007/s11096-024-01832-9
31. Gil-Guillen VF, Balsa A, Bernárdez B, et al. Medication non-adherence in rheumatology, oncology and cardiology: a review of the literature of risk factors and potential interventions. Int J Environ Res Public Health. 2022;19(19):12036. doi:10.3390/ijerph191912036
32. Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet. 2000;356(9237):1255–1259. doi:10.1016/s0140-6736(00)02799-9
33. Lecouturier J, Cunningham B, Campbell D, Copeland R. Medication compliance aids: a qualitative study of users’ views. Br J Gen Pract. 2011;61(583):93–100. doi:10.3399/bjgp11X556191
34. Wang Y, Wong EL, Qiu H, Cheung AW, Tang KS, Yeoh EK. The influence of written medication reminder on patient experience among older adult patients: a repeat cross-sectional study. BMC Geriatr. 2024;24(1):662. doi:10.1186/s12877-024-05253-1
35. Qu W, Wang X, Zhang S, et al. Factors related to the treatment burden of patients with coronary heart disease: a cross-sectional study. Heart Lung. 2025;70:141–146. doi:10.1016/j.hrtlng.2024.11.019
36. Martin D, Kripalani S, Durapau VJ. Improving medication management among at-risk older adults. J Gerontol Nurs. 2012;38(6):24–34;quiz36–7. doi:10.3928/00989134-20120509-01
37. Gentizon J, Bovet E, Rapp E, Mabire C. Medication literacy in hospitalized older adults: concept development. Health Lit Res Pract. 2022;6(2):e70–e83. doi:10.3928/24748307-20220309-02
38. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/s0022-3999(99)00057-4
39. Russell J, Kazantzis N. Medication beliefs and adherence to antidepressants in primary care. N Z Med J. 2008;121(1286):14–20.
40. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the Necessity-Concerns Framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Literacy and Home Medication Behaviors Among Older Chinese Patients with Chronic Diseases: A National Cross-Sectional Study

Shi X, Cheng H, Mutalifu M, Zhao Z, Wu M
Clinical Interventions in Aging 2026, 21:593700
Published Date: 6 May 2026