Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Analysis of Factors Related to Lymph Node Metastasis Following Neoadjuvant Chemotherapy for Breast Cancer: Correlation Between Plasma Exosomal Circular RNA and Metastasis
Authors Ma S, Huang Y, Yang Q, Liu X, Zhang Z, Yan B
Received 22 December 2025
Accepted for publication 12 March 2026
Published 9 April 2026 Volume 2026:18 588196
DOI https://doi.org/10.2147/BCTT.S588196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Sushuang Ma,1 Yanqiu Huang,2 Qingyan Yang,1 Xiaoyan Liu,1 Zhiqiang Zhang,1 Bing Yan1
1Department of Breast Surgery, Affiliated Hospital of Hebei Engineering University, Handan, Hebei, 056002, People’s Republic of China; 2Big Data Center, Affiliated Hospital of Hebei Engineering University, Handan, Hebei, 056002, People’s Republic of China
Correspondence: Bing Yan, Department of Breast Surgery, Affiliated Hospital of Hebei Engineering University, No. 81, Congtai Road, Congtai District, Handan, Hebei, 056002, People’s Republic of China, Tel +86 17320662026, Email [email protected]
Objective: To investigate the correlation between plasma exosomal circular RNA (circRNA) (non-invasive, dynamically monitorable) and lymph node metastasis following neoadjuvant chemotherapy in breast cancer and highlight its predictive superiority over traditional serum markers.
Methods: The clinicopathological data and follow-up data of 487 patients with breast cancer who received neoadjuvant therapy in our hospital between 1 January 2018 and 1 January 2020 were retrospectively collected using convenience sampling. Following screening, 379 patients who met the inclusion and exclusion criteria were included in the analysis. The patients’ data, including age, clinical TNM stage, tumour pathological type, tumour histological grade, tumour molecular typing, neoadjuvant regimen and course of treatment, were collected for analysis.
Results: Log rank test results showed that there were significant differences between the two groups in molecular typing (χ2 = 46.058, P < 0.001), neoadjuvant regimen (χ2 = 10.996, P < 0.001), axillary surgery (χ2 = 4.267, P = 0.039), histological grade (χ2 = 32.280, P < 0.001) and pathological complete response (pCR) (χ2 = 18.993, P < 0.001). The t-test results showed that the circRNA level was higher in the metastatic group than in the non-metastatic group (8.55 ± 2.12 vs 3.70 ± 1.81, t = 22.868, P < 0.001). The results of regression analysis showed that non-pCR (odds ratio [OR] = 2.320, 95% CI: 1.259– 4.276), molecular subtype HER2+ (OR = 1.747, 95% CI: 1.070– 2.852), histological grade II (OR = 3.159, 95% CI: 1.537– 6.491), histological grade III (OR = 2.606, 95% CI: 1.242– 5.466) and circRNA expression level (OR = 1.497, 95% CI: 1.398– 1.602) were risk factors for postoperative metastasis in patients with breast cancer. The level of circRNA has predictive value for the occurrence of postoperative metastasis in breast cancer. The area under the curve was 0.955 (95% CI: 0.933– 0.976), with a sensitivity of 87.4% and a specificity of 91.9%.
Conclusion: Molecular typing, pCR status, histological grade and plasma exosomal circRNA expression level are independent predictors of recurrence and metastasis following neoadjuvant therapy. Notably, plasma exosomal circRNA, with its non-invasive and dynamic monitoring advantages, shows promising predictive potential for lymph node metastasis, providing a novel and superior clinical tool for prognosis assessment.
Keywords: breast cancer, neoadjuvant treatment, prognosis, circular RNA
Introduction
Metastasis remains the primary driver of mortality in breast cancer.1 Although neoadjuvant therapy has become a cornerstone for locally advanced disease, the current tools for predicting metastatic recurrence – primarily pathological complete response (pCR) and residual cancer burden (RCB) – are static, postoperative assessments.2,3 This creates a critical gap: clinicians lack non-invasive, real-time biomarkers that capture the dynamic biological processes driving metastasis during treatment.4,5
Extracellular vesicles (EVs) are now recognised not merely as cellular debris but as central architects of the metastatic cascade.6 Emerging evidence positions EVs as the primary messengers in the tumour microenvironment, facilitating pre-metastatic niche formation, immune evasion and intercellular communication, all of which are essential for lymph node spread.7 Given that circulating biomarkers such as RNA are notoriously unstable in plasma, the EV compartment represents the most biologically plausible vehicle for stable tumour-derived genetic cargo.8 This biological rationale shifts the focus from purely statistical associations to a mechanistic understanding of how tumour-derived EVs “educate” distant sites.
Within this EV-driven framework, circular RNAs (circRNAs) have emerged as ideal liquid biopsy targets due to their covalently closed structure and enrichment within EVs.9 Although several EV-circRNAs have been proposed as diagnostic tools, few have been functionally contextualised within the specific genetic landscape of neoadjuvant-treated breast cancer,10 underscoring the criticality of biomarker discovery rooted in the genetic mechanisms driving EV-mediated metastasis.
This study focuses on hsa_circ_0000615 (circ-ZNF609). Although circ-ZNF609 has been implicated in cellular proliferation, its role as an EV-packaged communicator in the plasma of patients with breast cancer – particularly in predicting lymph node metastasis following neoadjuvant chemotherapy – remains unvalidated. This study bridges the gap between the broad EV-metastasis paradigm and the clinical need for dynamic prognostic tools by investigating plasma exosomal circ-ZNF609 as a non-invasive sentinel of residual disease.
Materials and Method
Study Participants
The clinicopathological and follow-up data of 487 patients with breast cancer who received neoadjuvant therapy in our hospital between 1 January 2018 and 1 January 2020 were retrospectively collected using convenience sampling. The inclusion criteria were female patients with breast cancer who were ≥18 years of age and undergoing neoadjuvant therapy. The exclusion criteria included patients (1) with newly diagnosed advanced (stage IV) breast cancer, (2) with bilateral breast cancer, (3) not receiving radical surgery and (4) with no complications with other malignant tumours. Following screening, 379 patients who met the inclusion and exclusion criteria were included in the analysis, including 108 patients with pCR and 271 patients with no pCR.
This study was approved by the hospital’s ethics committee. Data were retrospectively collected with patient information concealed and confidential, thus informed consent was not required.
Study Method
Molecular Typing Determination
According to the guidelines for the detection of oestrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) recommended by the American Society of Clinical Oncology and the American Society of Pathologists.11,12 Oestrogen receptor/PR-positive was defined as ≥1% of the tumour cell nucleus staining positive,11 HER2-positive (HER2+) was defined as immunohistochemical detection of 3+ or fluorescence in situ hybridisation (FISH) detection of HER2 gene amplification; FISH amplification was defined as HER2/chromosome enumeration probe 17 ratio ≥2 or HER2 gene average copy number reference probe signal/nuclear ratio ≥6.12 Triple-negative breast cancer (TNBC) is defined as a type of breast cancer in which ER, PR and HER2 are all negative.11,12 Kiel (Ki)-67 index was calculated according to the percentage of positive nuclear staining, with Ki-67 < 20% defined as low expression and Ki-67 ≥ 20% as high expression. Non-pCR was defined as invasive cancer residue in primary breast lesions or regional lymph nodes following neoadjuvant therapy, that is, RCB > 0.
Histologic Grades
The histological grade was evaluated using haematoxylin and eosin staining of tissue sections and classified according to the Nottingham system. Classification was achieved by summing the scores for the three indices of glandular structure, nuclear pleomorphism and mitotic count as follows: if the total score was 3–5 points, the histological grade was grade I; if the total score was 6–7 points, the histological grade was grade II; if the total score was 8–9, the histological grade was grade III.
Follow-Up Method
All cases were followed up by telephone, outpatient review, inpatient medical record query and household registration search. The follow-up time was 5 years after the operation, and the follow-up endpoint was the follow-up date/date of loss to follow-up, along with the outcome event (recurrence, metastasis or death). Of the 379 enrolled patients, 19 were lost to follow-up over the 5-year period, for an overall loss-to-follow-up rate of 5.01% (19/379). The reasons for loss to follow-up were patient migration (n = 10), inability to contact due to phone number change (n = 6) and voluntary withdrawal (n = 3). No loss to follow-up was related to tumour progression or treatment outcomes.
Circular RNA-ZNF609 Determination
To specifically isolate and detect plasma exosomal circRNA (excluding free circulating RNA in plasma), 3–4 mL of fasting venous blood was collected from patients with breast cancer in ethylenediaminetetraacetic acid vacuum anticoagulant blood collection tubes. Whole blood samples were immediately placed on ice and processed via centrifugation within 2 h of collection to avoid exosome rupture and RNA degradation. The plasma was first separated via low-speed centrifugation (3000 × g, 10 min, 4°C) to remove blood cells and cell debris. The supernatant plasma was then subjected to high-speed ultracentrifugation (12,000 × g, 20 min, 4°C) to further remove microvesicles and residual impurities, ensuring the purity of the exosomal fraction. Total RNA exclusively from plasma exosomes was extracted using the TIANamp Virus RNA Kit (Tiangen Biotech, Beijing, China), a kit specifically optimised for exosomal RNA extraction with a silica-membrane adsorption method that effectively excludes free nucleic acids in the plasma matrix.
The extracted exosomal RNA was reverse transcribed into complementary (c)DNA using the First-Strand cDNA Synthesis Super Mix kit (TransGen Biotech, China) according to the manufacturer’s standard protocol, with random hexamers as reverse transcription primers to ensure the integrity of circRNA reverse transcription. The cDNA was amplified using real-time quantitative polymerase chain reaction (qPCR) with the SYBR® Green fluorescence method on a StepOnePlus Real-Time PCR System (Applied Biosystems, USA).
The hsa_circ_0000615-specific qPCR primers were designed across the back-splice junction (the core feature of circRNA) to ensure specific amplification of circRNA but not its linear host gene ZNF609, with the sequences as follows: upstream 5′-GCTGCTGAAGATGAAGCCAA-3′, downstream 5′-CCTTCTGCTGCTTCTTCTGG-3′; U6 small nuclear RNA was selected as the internal reference gene for exosomal RNA normalisation (upstream: 5′-CTCGCTTCGGCAGCACA-3′, downstream: 5′-AACGCTTCACGAATTTGCGT-3′). The specificity of the amplification product was verified using melting curve analysis (a single peak indicated specific amplification), and the relative expression level of plasma exosomal hsa_circ_0000615 was calculated using the 2−ΔΔCt method. Quantitative analysis of the initial exosomal RNA template was conducted by observing the real-time accumulation of fluorescence signals during qPCR amplification.
Postoperative Adjuvant Therapy Criteria
Postoperative adjuvant therapy was standardised for all enrolled patients in accordance with the Chinese Guidelines for the Diagnosis and Treatment of Breast Cancer (2019 version). All patients who were HER2+ received 1 year of trastuzumab targeted therapy (loading dose = 8 mg/kg, maintenance dose = 6 mg/kg, once every 3 weeks) regardless of pCR status. For patients who were non-pCR, capecitabine-based intensive chemotherapy was administered uniformly (1250 mg/m2 twice daily, days 1–14, with a 21-day cycle, for a total of 6–8 cycles). For patients with TNBC, adjuvant chemotherapy with an anthracycline–taxane regimen was routinely performed for 6–8 cycles following radical surgery. Patients who were hormone receptor-positive received standardised endocrine therapy according to their menopausal status. Adjuvant therapy was strictly consistent across groups, and the therapeutic course and drug dosage were standardised to ensure balance in postoperative adjuvant therapy among subgroups.
Data Collection
Collected data included patient age, clinical TNM stage, tumour pathological type, tumour histological grade, tumour molecular typing, neoadjuvant regimen and course of treatment, breast and axillary surgery, puncture time, operation time, efficacy evaluation, adjuvant therapy, recurrence and metastasis, death and time, and last follow-up time.
Statistical Analysis
Statistical analysis was performed using IBM SPSS v26.0. The Kaplan–Meier (K–M) method, the Log rank test and the Cox regression model were used to analyse prognostic factors in breast cancer. The circRNA levels were expressed as mean ± standard deviation (x ± s), and an independent-samples t-test was used to compare groups. The receiver operating characteristic (ROC) curve was used to assess the predictive value of circRNA for lymph node metastasis following neoadjuvant chemotherapy in postoperative breast cancer. Only P < 0.1 in the K–M univariate survival analysis was considered statistically significant; P < 0.05 was considered significant in the remaining analyses.
Results
Univariate Analysis
There were 119 cases in the metastasis group and 260 cases in the non-metastasis group. Log rank test results showed that there were significant differences in molecular typing (χ2 = 46.058, P < 0.001), neoadjuvant regimen (χ2 = 10.996, P < 0.001), axillary surgery (χ2 = 4.267, P = 0.039), histological grade (χ2 = 32.280, P < 0.001) and pCR proportion (χ2 = 18.993, P < 0.001) between the two groups. The t-test results showed that the circRNA level was higher in the metastatic group than in the non-metastatic group (8.55 ± 2.12 vs 3.70 ± 1.81, t = 22.868, P < 0.001). Both groups achieved 100% completion of the postoperative adjuvant therapy. The statistical results are shown in Table 1, and the survival curve is shown in Figure 1.
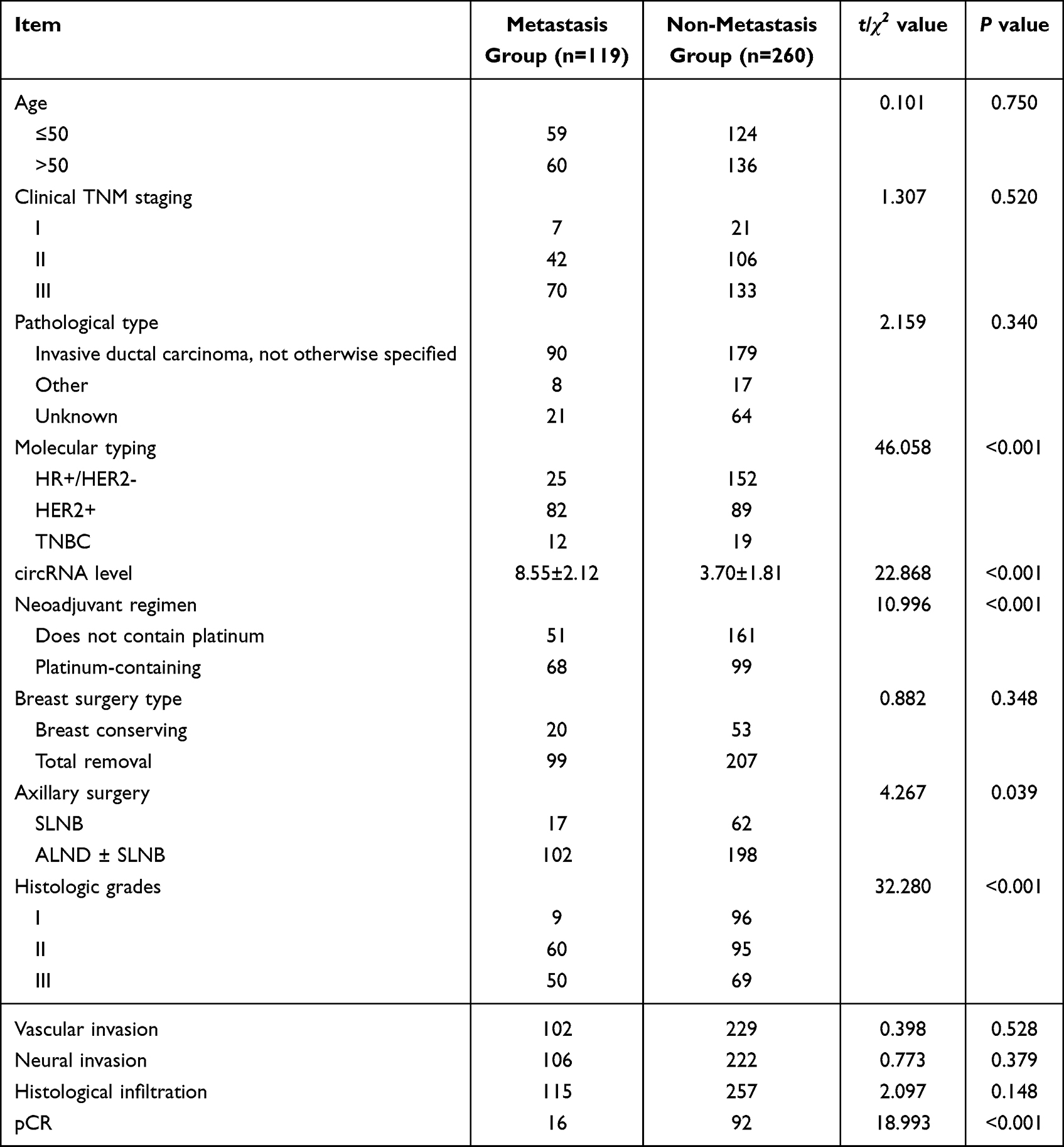 |
Table 1 Univariate Analysis |
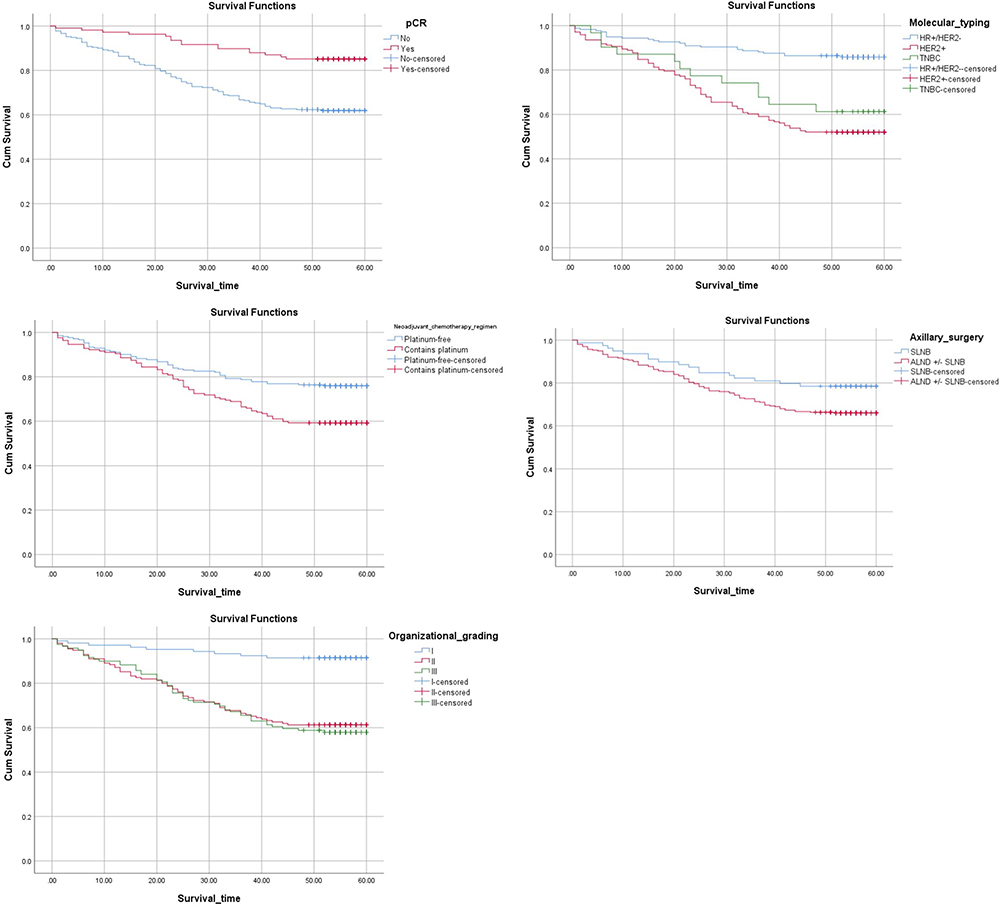 |
Figure 1 Survival curve. |
Multiple-Factor Analysis
The Cox regression model was constructed with tumour metastasis occurrence as the dependent variable (occurrence = 1, no occurrence = 0) and the statistically significant factors from the univariate analysis as independent variables. The variable grouping and coding are shown in Table 2. The results of the regression analysis showed that non-pCR (odds ratio [OR] = 2.320, 95% CI: 1.259–4.276), molecular subtype HER2+ (OR = 1.747, 95% CI: 1.070–2.852), histological grade II (OR = 3.159, 95% CI: 1.537–6.491), histological grade III (OR = 2.606, 95% CI: 1.242–5.466) and circRNA expression level (OR = 1.497, 95% CI: 1.398–1.602) were potential independent risk factors for postoperative metastasis in patients with breast cancer (see Table 3).
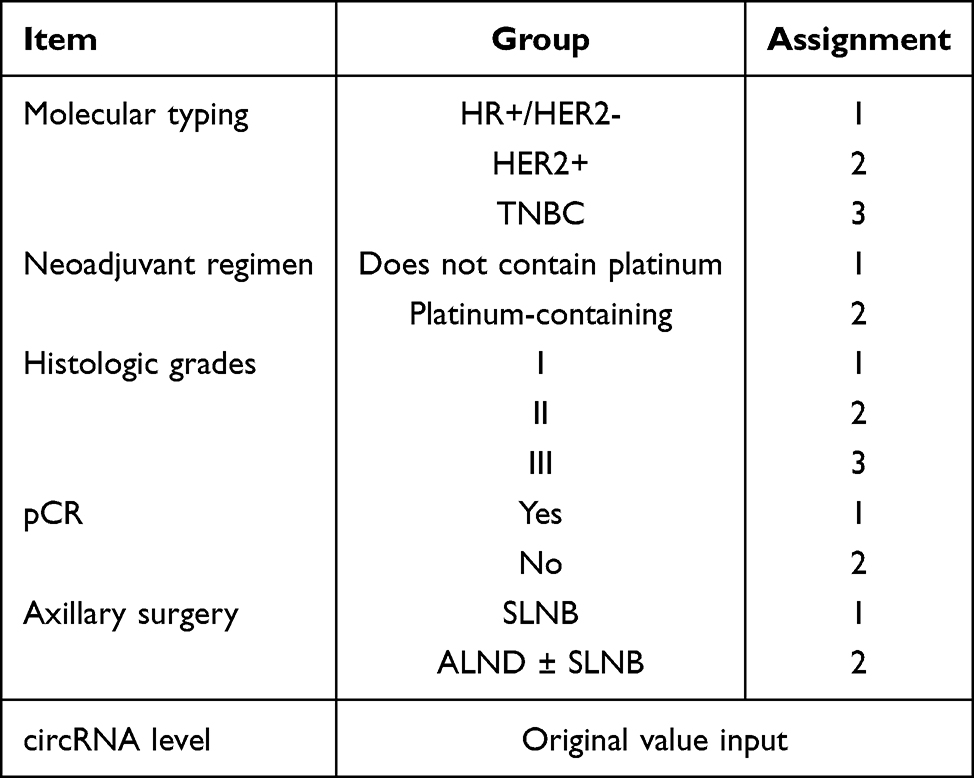 |
Table 2 Variable Grouping and Value Assignment |
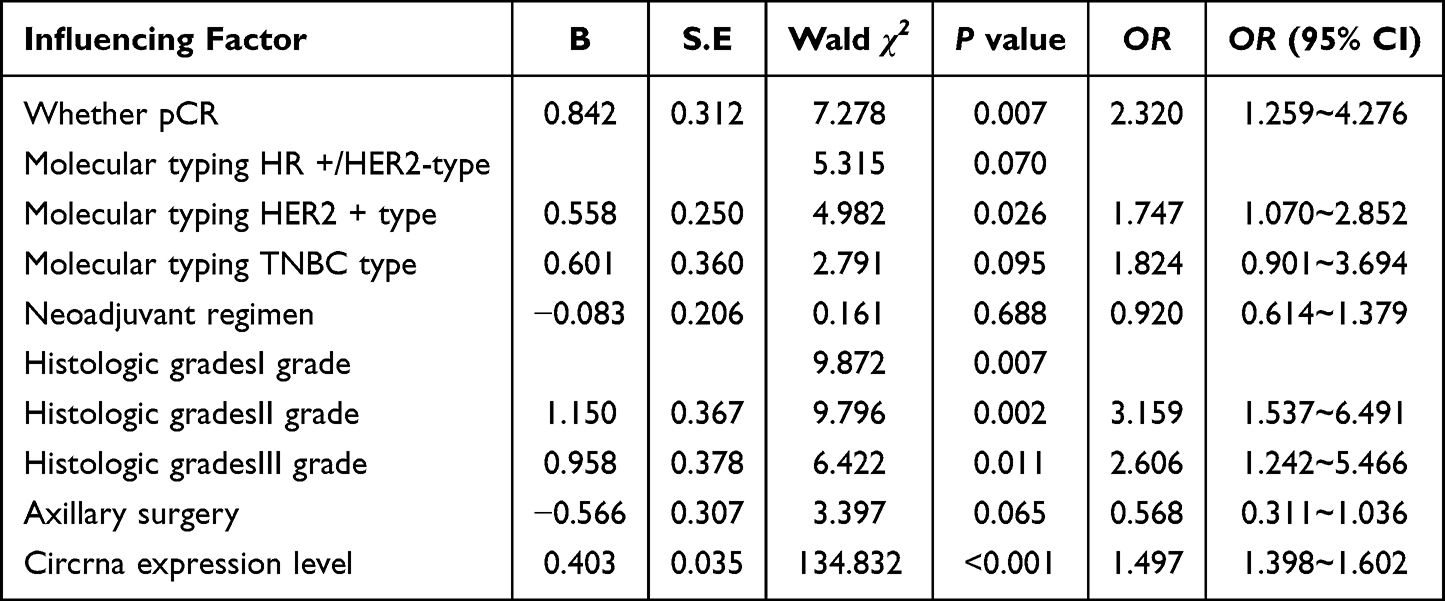 |
Table 3 COX Regression Analysis |
The Predictive Value of Circular RNA for Postoperative Metastasis of Breast Cancer
The results showed that circRNA level had considerable predictive performance for the occurrence of postoperative metastasis of breast cancer. The area under the curve was 0.955 (95% CI: 0.933–0.976), the sensitivity was 87.4%, and the specificity was 91.9%, as shown in Figure 2.
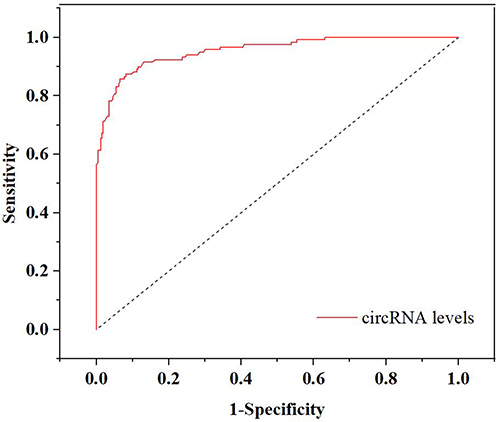 |
Figure 2 ROC curve of circRNA predictive value. |
Discussion
This study is retrospective. The clinicopathological data and prognosis of patients with breast cancer receiving neoadjuvant therapy were analysed using univariate and multivariate regression analysis. The pCR rate of patients with breast cancer in this study was 28%, which was in line with the pCR rate range reported in the current literature (pCR rate: 17–66%).2 The results of this study showed that pCR, molecular typing, histological grade and circRNA expression level were associated with postoperative metastasis.
According to the literature, the prognosis of patients with TNBC is worse than that of those with other subtypes.13 However, in this study, the risk of TNBC (39%) was lower than that of HER2+ (47%) but higher than that of ER+/HER2− (14%). This result differs from previous results, which may be due to the lower proportion of patients in the HER2+ group receiving intensive treatment in this study. A meta-analysis published in 202014 included 25 studies and analysed 4330 patients with TNBC who received neoadjuvant chemotherapy. The results showed that additional adjuvant chemotherapy improved disease-free survival (DFS) and overall survival (OS) in the patients, regardless of pCR status. Although there is no reliable evidence for the effect of intensive neoadjuvant therapy on the prognosis of patients with TNBC and small tumours and low lymph node staging,15,16 residual tumours following neoadjuvant chemotherapy are considered resistant to it. Therefore, changing the chemotherapy regimen for intensive treatment may alter the tumour’s sensitivity to chemotherapy, thereby reducing the risk of tumour recurrence.
The molecular subtypes of tumours may affect the choice of intensive treatment options and their efficacy. In the CREATE-X study, capecitabine improved the DFS and OS in patients with TNBC more than in those with hormone receptor-positive tumours.3 However, the results of the GEICAM/2003-11_CIBOMA/2004-01 trial showed that DFS and OS were not significantly prolonged in the capecitabine group compared with the observation group in patients with TNBC tumours who received standard neoadjuvant anthracycline- and/or taxane-based chemotherapy.15 The inconsistent results may be due to differences in tumour recurrence risk among the patients studied in the two trials. In the CREATE-X trial, the 5-year DFS of patients with TNBC in the control group was 56.1%, compared with 76.8% in the control group in the GEICAM/200311_CIBOMA/2004-01 trial.3,15 These results suggest that, compared with molecular subtypes, tumour recurrence risk better predicts whether patients will benefit from intensive treatment. Therefore, patients with positive hormone receptors who are at high risk may also benefit from intensive capecitabine therapy.
The current literature reports recurrence and metastasis rates of 10–25% in patients with pCR.17,18 In this study, the 5-year tumour recurrence rate in patients with pCR was 15%, which is similar to rates reported in related studies. Some studies have focused on the prognostic value of clinicopathological parameters in patients with pCR. The results showed that the higher the clinical stage is, the higher the recurrence and metastasis rates in patients with pCR,19,20 consistent with the conclusion of this study. These results suggest that, even if pCR is achieved following neoadjuvant therapy, the greater the tumour load before neoadjuvant therapy is, the higher the risk of recurrence and metastasis, and that it may be necessary to reduce this risk through postoperative intensive adjuvant therapy.
At present, the sensitivity of the serum markers, cancer antigen (CA)-125, CA-153 and carcinoembryonic antigen (CEA), used in clinical breast cancer, is low. They are generally used in recurrent and metastatic breast cancer, and the ability to distinguish early breast cancer is poor. Therefore, identifying molecular markers in body fluids that can serve as therapeutic monitoring markers for non-invasive diagnosis, prognosis and cancer management is among the most practical challenges in oncology research. The increased use of new methods such as second-generation sequencing, single-cell sequencing, RT-qPCR and other non-invasive biomarker research methods has greatly increased the potential for research to be translated into clinical applications. In recent years, many studies have identified differentially expressed circRNAs in blood,21 saliva22 and other body fluids,23 indicating that circRNAs can serve as biomarkers for a variety of diseases. However, the current research on circRNA in breast cancer mainly focuses on its potential functional mechanism, and the clinical diagnostic value in breast cancer remains largely unknown; the study of circRNA in breast cancer plasma is especially rare. Yin et al24 found that the expression level of hsa-circ-0001785 in the plasma of patients with breast cancer was significantly higher than that in the healthy control group, and that high plasma hsa-circ-0001785 expression was closely related to histological grade, TNM stage and distant metastasis. More importantly, the diagnostic value of hsa-circ-0001785 for breast cancer is higher than other tumour biomarkers such as CA-153 and CEA. Hu et al25 found that the expression of plasma cell-free hsa_circ_0008673 in patients with breast cancer was up-regulated, which was associated with poor prognosis and could promote tumour proliferation and metastasis; Hsa_circ_0008673 is a promising biomarker for tumour diagnosis and prognosis evaluation in patients with breast cancer. The ROC results of this study also showed that circRNA had a high predictive value for postoperative metastasis of patients with breast cancer. The present study further validates the clinical value of plasma exosomal circRNA as a prognostic biomarker for breast cancer lymph node metastasis, and its potential biological relevance to tumour metastatic behaviour is further elaborated as follows.
Our study found that plasma exosomal circ-ZNF609 expression was significantly elevated in patients with breast cancer and lymph node metastasis following neoadjuvant chemotherapy, with the level in the metastatic group more than twice that in the non-metastatic group. High circ-ZNF609 expression was significantly associated with lymph node metastasis, suggesting an underlying biological association between the two.25 Elevated exosomal circ-ZNF609 expression may be correlated with enhanced migratory and invasive capacities of breast cancer cells, which represent the core biological processes driving lymph node metastasis of tumours.4,5 All enrolled patients in this study completed standardised postoperative adjuvant therapy as prescribed, thereby eliminating confounding interference from inconsistent adjuvant treatment regimens and enhancing the reliability of the observed association between circ-ZNF609 expression and lymph node metastasis. Emerging preclinical evidence indicates that the regulatory effect of circ-ZNF609 on tumour cell migration and invasion is closely linked to the epithelial-mesenchymal transition (EMT) pathway,4 providing a critical molecular entry point for further exploration of the biological mechanism of circ-ZNF609 in breast cancer lymph node metastasis.5,25
Plasma exosomal hsa_circ_0000615 overexpression in patients with breast cancer complicated by lymph node metastasis is closely linked to the competitive endogenous RNA (ceRNA) network and exosomal secretion, jointly boosting cancer cell migration and invasion.4,5 With a closed-loop structure, it exhibits high plasma stability and RNase resistance,4 enabling stable exosomal packaging and secretion into peripheral blood, resulting in detectable high expression. In the ceRNA network, hsa_circ_0000615 may act as a molecular sponge for tumour-suppressive microRNAs (eg. miR-145-5p, miR-206),4,25 relieving their inhibition of metastasis-related genes (eg. SNAI1, VIM) and activating the EMT pathway.3,8 Notably, exosomal hsa_circ_0000615 can mediate crosstalk between breast tumour cells and cancer-associated fibroblasts (CAFs) in the tumour microenvironment,26,27 transferring the ceRNA network to CAFs to reshape their pro-metastatic phenotype, thereby further promoting pre-metastatic niche formation in axillary lymph nodes and accelerating lymph node metastasis. Thus, hsa_circ_0000615 is both a metastasis biomarker and a potential regulator via the ceRNA mechanism, verifying the biological rationality of its predictive value.
Histological grading is another widely used parameter that helps determine the prognosis of patients with invasive breast cancer. The Nottingham grading system is used for invasive breast cancer and assigns a composite score based on three tissue factors: glandular structure, nuclear pleomorphism and mitotic count.28 In 2017, the Nottingham grading system was adopted by the American Joint Committee on Cancer for breast cancer prognostic staging.29 In a large histological grading prognostic study, all cases were treated according to standard protocols at a single institution. After long-term follow-up, it was found that histological grade was closely related to breast cancer-specific survival (BCSS) and DFS, and was an independent predictor of BCSS and DFS in patients with breast cancer. It is also closely related to tumour size (T1 and T2) and N stages. The survival rate of patients with breast cancer with different histological grades also varies.30 The results of this study also show that histological grade is an independent risk factor for the prognosis of patients with breast cancer, consistent with the above.
In the era of individualised breast cancer therapy, our identified predictors (non-pCR, HER2+ status and high plasma exosomal hsa_circ_0000615) provide a robust basis for post-neoadjuvant risk stratification. This combined risk stratification strategy is also supported by recent studies,31,32 which confirmed that integrating circRNA biomarkers with molecular subtype and pCR status can optimise the identification of patients with breast cancer at high risk and guide the formulation of individualised intensive therapy. Aligned with the clinical need for intensive treatment, the high-risk subgroup (non-pCR + HER2-positive + high circRNA expression) warrants escalated adjuvant therapy. In contrast, patients at low risk (pCR + low circRNA) may benefit from de-escalation. Notably, the non-invasive, dynamically monitorable nature of exosomal hsa_circ_0000615 enables real-time risk re-stratification, making it a practical complement to static pathological indicators such as pCR in clinical practice.
This study also has some limitations. The study used convenience sampling and enrolled patients only from the Affiliated Hospital of Hebei Engineering University. This single-centre retrospective design introduces obvious regional and population limitations, reducing sample representativeness and affecting the extrapolation of the results to the general breast cancer population. In addition, the included patients are limited to a single medical institution, with a small sample size, a short research period, and a limited population scope. It is necessary to conduct multicentre, large-sample prospective cohort studies in the future to verify the study results. The study is a retrospective study, which has some shortcomings to a certain extent, such as potential flaws in the inclusion criteria, clinical data selection, data processing and causal association determination. Notably, the overall loss-to-follow-up rate in this study was only 5.01%, well below the 20% critical value, and loss to follow-up was not associated with study outcomes, indicating it did not cause selective bias or substantially affect the core conclusions.
Conclusion
In summary, non-pCR status, HER2+ molecular subtype, histological grade and plasma exosomal circ-ZNF609 expression are independent predictors of lymph node metastasis following neoadjuvant chemotherapy for breast cancer. With its EV-mediated stability and potential regulatory role in tumour cell motility and tumour-stroma crosstalk, plasma exosomal circ-ZNF609 exhibits excellent predictive value for lymph node metastasis and offers the unique advantage of non-invasive, dynamic monitoring. This study bridges the gap between clinical prognostic needs and biological mechanisms of breast cancer metastasis, providing a novel functional liquid biopsy biomarker for clinical risk stratification and individualised adjuvant therapy. Notably, the proposed regulatory mechanisms of circ-ZNF609 require further in vitro and in vivo validation to confirm their direct functional role in breast cancer metastasis.
Data Sharing Statement
All data generated or analyzed during this study are included in the article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Affiliated Hospital of Hebei Engineering University (No. 2023[K]055). Since this study was a retrospective study, the Medical Ethics Committee waived the need for informed consent from patients.
Funding
Handan City Science and Technology Research and Development Plan (NO. 23422083355).
Disclosure
None of the authors have any personal, financial, commercial, or academic conflicts of interest.
References
1. Kerr AJ, Dodwell D, McGale P, et al. Adjuvant and neoadjuvant breast cancer treatments: a systematic review of their effects on mortality. Cancer Treat Rev. 2022;105:102375. doi:10.1016/j.ctrv.2022.102375
2. Schneeweiss A, Chia S, Hickish T, et al. Long-term efficacy analysis of the randomised, Phase II TRYPHAENA cardiac safety study: evaluating pertuzumab and trastuzumab plus standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer. Eur J Cancer. 2018;89:27–11. doi:10.1016/j.ejca.2017.10.021
3. Masuda N, Lee SJ, Ohtani S, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med. 2017;376(22):2147–2159. doi:10.1056/NEJMoa1612645
4. Su M, Xiao Y, Ma J, et al. Circular RNAs in cancer: emerging functions in hallmarks, stemness, resistance and roles as potential biomarkers. Mol Cancer. 2019;18(1):90. doi:10.1186/s12943-019-1002-6
5. Pardini B, Sabo AA, Birolo G, et al. Noncoding RNAs in extracellular fluids as cancer biomarkers: the new frontier of liquid biopsies. Cancers. 2019;11(8):1170. doi:10.3390/cancers11081170
6. Seibold T, Waldenmaier M, Seufferlein T, Eiseler T. Small extracellular vesicles and metastasis-blame the messenger. Cancers. 2021;13(17):4380. doi:10.3390/cancers13174380 PMID: 34503190; PMCID: PMC8431296.
7. Jahangiri L. The impact of extracellular vesicles on breast cancer metastasis and therapeutics: genetic considerations. Cancer Genet. 2025;298–299:1–9. PMID: 40818418. doi:10.1016/j.cancergen.2025.08.003
8. Zhang C, Qin C, Dewanjee S, et al. Tumor-derived small extracellular vesicles in cancer invasion and metastasis: molecular mechanisms, and clinical significance. Mol Cancer. 2024;23(1):18. doi:10.1186/s12943-024-01932-0 PMID: 38243280; PMCID: PMC10797874.
9. Zhang F, Jiang J, Qian H, Yan Y, Xu W. Exosomal circRNA: emerging insights into cancer progression and clinical application potential. J Hematol Oncol. 2023;16(1):67. doi:10.1186/s13045-023-01452-2 PMID: 37365670; PMCID: PMC10294326.
10. Qurtam AA. CircRNAs in extracellular vesicles associated with triple-negative breast cancer. Cell Mol Biol. 2025;70(12):99–109. doi:10.14715/cmb/2024.70.12.14 PMID: 39799490.
11. Hammond ME, Hayes DF, Wolff AC, et al. American society of clinical oncology/college of American pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Oncol Pract. 2010;6(4):195–197. doi:10.1200/JOP.777003
12. Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med. 2007;131(1):18–43. doi:10.5858/2007-131-18-ASOCCO
13. Kuroi K, Toi M, Ohno S, et al. Prognostic significance of subtype and pathologic response in operable breast cancer; a pooled analysis of prospective neoadjuvant studies of JBCRG. Breast Cancer. 2015;22(5):486–495. doi:10.1007/s12282-013-0511-1
14. Huang M, O’Shaughnessy J, Zhao J, et al. Association of pathologic complete response with long-term survival outcomes in triple-negative breast cancer: a meta-analysis. Cancer Res. 2020;80(24):5427–5434. doi:10.1158/0008-5472.CAN-20-1792
15. Lluch A, Barrios CH, Torrecillas L, et al. Phase III trial of adjuvant capecitabine after standard neo-/adjuvant chemotherapy in patients with early triple-negative breast cancer (GEICAM/2003-11_CIBOMA/2004-01). J Clin Oncol. 2020;38(3):203–213. Erratum in: J Clin Oncol. 2020 Mar 10;38(8):847. doi: 10.1200/JCO.20.00164. doi:10.1200/JCO.19.00904
16. Piroth MD, Krug D, Sedlmayer F, et al. Post-neoadjuvant treatment with capecitabine and trastuzumab emtansine in breast cancer patients-sequentially, or better simultaneously? Strahlenther Onkol. 2021;197(1):1–7. doi:10.1007/s00066-020-01667-z
17. Kuerer HM, Newman LA, Smith TL, et al. Clinical course of breast cancer patients with complete pathologic primary tumor and axillary lymph node response to doxorubicin-based neoadjuvant chemotherapy. J Clin Oncol. 1999;17(2):460–469. doi:10.1200/JCO.1999.17.2.460
18. Fei F, Messina C, Slaets L, et al. Tumour size is the only predictive factor of distant recurrence after pathological complete response to neoadjuvant chemotherapy in patients with large operable or locally advanced breast cancers: a sub-study of EORTC 10994/BIG 1-00 phase III trial. Eur J Cancer. 2015;51(3):301–309. doi:10.1016/j.ejca.2014.11.023
19. O’Shaughnessy J, Robert N, Annavarapu S, et al. Recurrence rates in patients with HER2+ breast cancer who achieved a pathological complete response after neoadjuvant pertuzumab plus trastuzumab followed by adjuvant trastuzumab: a real-world evidence study. Breast Cancer Res Treat. 2021;187(3):903–913. doi:10.1007/s10549-021-06137-3
20. Chaudry M, Lei X, Gonzalez-Angulo AM, et al. Recurrence and survival among breast cancer patients achieving a pathological complete response to neoadjuvant chemotherapy. Breast Cancer Res Treat. 2015;153(2):417–423. doi:10.1007/s10549-015-3533-x
21. Zhang YG, Yang HL, Long Y, et al. Circular RNA in blood corpuscles combined with plasma protein factor for early prediction of pre-eclampsia. BJOG. 2016;123(13):2113–2118. doi:10.1111/1471-0528.13897
22. Bahn JH, Zhang Q, Li F, et al. The landscape of microRNA, Piwi-interacting RNA, and circular RNA in human saliva. Clin Chem. 2015;61(1):221–230. doi:10.1373/clinchem.2014.230433
23. Qu S, Zhong Y, Shang R, et al. The emerging landscape of circular RNA in life processes. RNA Biol. 2017;14(8):992–999. doi:10.1080/15476286.2016.1220473
24. Yin WB, Yan MG, Fang X, et al. Circulating circular RNA hsa_circ_0001785 acts as a diagnostic biomarker for breast cancer detection. Clin Chim Acta. 2018;487:363–368. doi:10.1016/j.cca.2017.10.011
25. Hu Y, Song Q, Zhao J, et al. Identification of plasma hsa_circ_0008673 expression as a potential biomarker and tumor regulator of breast cancer. J Clin Lab Anal. 2020;34(9):e23393. doi:10.1002/jcla.23393
26. Li C, Yang C, Yang Q. The role of miRNAs in the extracellular vesicle-mediated interplay between breast tumor cells and cancer-associated fibroblasts. J Cancer Metastasis Treat. 2024;10:27. doi:10.20517/2394-4722.2024.76
27. Liu H, Hamaia SW, Dobson L, et al. The voltage-gated sodium channel β3 subunit modulates C6 glioma cell motility independently of channel activity. Biochim Biophys Acta Mol Basis Dis. 2025;1871(6):167844. PMID: 40245999. doi:10.1016/j.bbadis.2025.167844
28. Bloom HJ, Richardson WW. Histological grading and prognosis in breast cancer; a study of 1409 cases of which 359 have been followed for 15 years. Br J Cancer. 1957;11(3):359–377. doi:10.1038/bjc.1957.43
29. Giuliano AE, Connolly JL, Edge SB, et al. Breast cancer-major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(4):290–303. doi:10.3322/caac.21393
30. Rakha EA, El-Sayed ME, Lee AH, et al. Prognostic significance of Nottingham histologic grade in invasive breast carcinoma. J Clin Oncol. 2008;26(19):3153–3158. doi:10.1200/JCO.2007.15.5986
31. Jing Y, Huang X, Wang Y, et al. Diagnostic value of 5 miRNAs combined detection for breast cancer. Front Genet. 2024;15:1482927. PMID: 39655225; PMCID: PMC11625769. doi:10.3389/fgene.2024.1482927
32. Li Y, Wang Y, Jing Y, et al. Visualization analysis of breast cancer-related ubiquitination modifications over the past two decades. Discov Oncol. 2025;16(1):431. PMID: 40163091; PMCID: PMC11958930. doi:10.1007/s12672-025-02032-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.